Back to Journals » Journal of Inflammation Research » Volume 18
Association Between the Systemic Immune-Inflammation Index and 24-week Outcomes in Patients with HIV-Associated Cryptococcal Meningitis: Secondary Analysis of a Prospective Multicenter Cohort Study
Authors Zhao T, Wang X, Song Y, Harypursat V ![]() , Chen Y
, Chen Y
Received 6 August 2025
Accepted for publication 15 November 2025
Published 3 December 2025 Volume 2025:18 Pages 16991—17003
DOI https://doi.org/10.2147/JIR.S555540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Ting Zhao,1,2,* Xiaohong Wang,1,* Yuxia Song,3 Vijay Harypursat,2,4 Yaokai Chen2,4
1Department of Pharmacology, Chongqing Public Health Medical Center, Chongqing, People’s Republic of China; 2Clinical Research Center, Chongqing Public Health Medical Center, Chongqing, People’s Republic of China; 3Department of Infectious Diseases, The Sixth People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, People’s Republic of China; 4Department of Infectious Diseases, Chongqing Public Health Medical Center, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaokai Chen, Department of Infectious Diseases; Clinical Research Center, Chongqing Public Health Medical Center, 109 Baoyu Road, Shapingba District, Chongqing, 400036, People’s Republic of China, Tel +86 23 65231256, Fax +86 23 65481658, Email [email protected]
Objective: The systemic immune-inflammation index (SII) represents a promising yet underexplored biomarker in HIV-associated cryptococcal meningitis (HCM). The study aimed to assess the association between SII levels before and during treatment, and 24-week outcomes in HCM patients, as well as its potential for predicting mortality.
Methods: This was a secondary analysis of a prospective multicenter study involving HIV patients with newly diagnosed cryptococcal meningitis (CM). SII was measured at baseline, and at weeks 2 and 4 following initiation of induction antifungal therapy. Correlations between baseline SII levels and clinicopathological factors were analyzed. We also investigated the relationship that baseline and on-treatment SII levels may have on patient cumulative mortality.
Results: In total, 21.8% (54/248) of HCM patients succumbed within the 24-week follow-up period. Baseline SII levels were significantly higher in HCM patients compared to those with HIV without CM (p< 0.0001). In patients with HCM, SII levels during treatment were significantly higher in non-survivors than in survivors. Furthermore, a negative correlation was observed between SII levels and CD4+ T-cell counts in HCM patients (r=− 0.245, p< 0.001). After adjusting for potential confounders, elevated SII levels at weeks 2 and 4 remained independently associated with a 2.5-fold and 5.5-fold increased risk of mortality, respectively [adjusted hazard ratio (95% CI): 2.51 (1.09— 5.76), p=0.03; 5.47 (2.38— 12.6), p< 0.001, respectively]. Moreover, the combination of SII levels at weeks 2 and 4, as well as their integration with impaired consciousness (IC) status, effectively predicted poor outcomes within 24 weeks.
Conclusion: Elevated SII levels during treatment are independently associated with increased 24-week mortality in HCM patients, suggesting the potential of SII as an effective prognostic biomarker. The integration of the SII into IC indicators for risk stratification further improves prognostic accuracy.
Keywords: HIV, cryptococcal meningitis, systemic immune-inflammation index, biomarkers, prognostic analysis
Introduction
Cryptococcal meningitis (CM) is a life-threatening central nervous system (CNS) disease caused by the invasion of Cryptococcus into the meninges and/or brain parenchyma. It is recognized as a common opportunistic infection among human immunodeficiency virus- (HIV-) infected individuals, and remains one of the significant causes of acquired immunodeficiency syndrome (AIDS)-related mortality. Although effective treatment has greatly improved the prognosis of patients with HIV-associated cryptococcal meningitis (HCM), the overall mortality rate for these patients remains high, accounting for 19% of AIDS-related deaths.1 As a result, the early identification of this high-risk population is imperative in order to improve clinical outcomes of patients with HCM.
The hallmark of Cryptococcus infection is immunosuppression, characterized by impaired T-cell-mediated immunity and a dysregulated inflammatory response,2 which may contribute to disease severity and poor outcomes. Clinically, immune profiling in antiretroviral therapy (ART)-naïve HCM patients reveals that elevated interleukin (IL)-4 and IL-17 levels, along with reduced tumor necrosis factor (TNF)-α, interferon-gamma (IFN)-γ, and CD4+ T-cells, are associated with an increased risk of the emergence of immune reconstitution inflammatory syndrome (IRIS) in these patients.3,4 Furthermore, Scriven et al, have identified an immune signature linked to fatal outcomes in HCM patients, marked by increased inflammation [increased levels of serum immune activation markers (IL-6 and CXCL10), higher concentrations of anti-inflammatory mediators (IL-10), and increased neutrophil counts], monocyte deactivation (reduced HLA-DR expression and TNF-α response to lipopolysaccharide), and downregulated T-helper cell type 1 response (reduced IL-12 and IFN-γ production).5 Notably, non-surviving HCM patients also exhibit significantly higher levels of circulating inflammatory markers [neutrophil-to-lymphocyte ratio (NLR), white blood cell count (WBC), and C-reactive protein (CRP)] as well as reduced CD4+ T-cell counts,6–8 possibly due to modulation of the host immune response by Cryptococcus. The preceding observations collectively highlight the prognostic potential of the immunological and inflammatory biomarkers present in peripheral blood in predicting the clinical trajectory of cryptococcosis.
The systemic immune-inflammation index (SII), derived from neutrophil, platelet, and lymphocyte counts, has recently emerged as a prognostic marker in inflammatory diseases and various cancers.9 It is also recognized as an independent risk factor for mortality in systemic infections, such as COVID-19, sepsis, and infective endocarditis.10–12 Furthermore, SII can be integrated with other biomarkers to improve predictive models and support clinical decision-making.13,14 However, its prognostic value in HCM remains unclear. Given that Cryptococcus infection is characterized by its systemic and disseminated nature, and frequently coexists with systemic inflammation and immune dysregulation, dynamic changes in peripheral immune and inflammatory factors during induction therapy phase may hold clinical significance. Therefore, SII was measured at admission and at weeks 2 and 4 following antifungal therapy to establish baseline status and assess early treatment response. Subsequently, we further explored the association between SII dynamics and 24-week outcomes in those patients with HCM, aiming to assess its potential as a readily accessible peripheral biomarker for monitoring treatment response.
Methods
Study Design and Participants
This study is a secondary analysis of data gathered from participants that were enrolled in a prospective multicenter clinical trial registered in China between from January 1st 2019 and December 30th 2020 (Registration No. ChiCTR1900021195). The patients included in this study were from 15 medical institutions across China, viz., Chongqing Public Health Medical Center, Harbin Medical University, Guangxi Longtan Hospital of Guangxi Zhuang Autonomous Region, The First Affiliated Hospital of Zhejiang University, Liuzhou General Hospital, the Third People’s Hospital of Guilin, the First Hospital of Changsha, the Fourth People’s Hospital of Nanning, Kunming Third People’s Hospital, Public Health Clinical Center of Chengdu, Guiyang Public Health Clinical Center, Xixi Hospital of Hangzhou, Beijing Youan Hospital of Capital Medical University, the Third People’s Hospital of Shenzhen, and Tianjin Second People’s Hospital. This study was approved by the Ethics Committee of Chongqing Public Health Medical Center (Approval No. 2019–003-02-KY), as well as by the individual institutional ethics committees of each of the other 14 hospitals involved in this study. Written informed consent was obtained from all participants. When patients were unable to provide written informed consent, their legal representative was asked to sign the consent form on their behalf. The research was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2008.
Eligible participants were individuals with HIV aged 18 years or older who experienced the first episode of microbiologically confirmed CM, as diagnosed by positive cerebrospinal fluid (CSF) culture, CSF microscopy, or CSF cryptococcal antigen (CrAg) detection. Patients were excluded if they were allergic or intolerant to any of the therapeutic drugs, were pregnant or lactating, had severe concurrent CNS infections, or had other serious coexisting conditions. Finally, a total of 248 patients with HCM were included in this study. To assess the impact of HIV infection on SII levels, an additional cohort of 236 people with HIV who tested negative for CM was recruited to serve as the control group. Access to this dataset was approved by the Ethics Review Committee of Chongqing Public Health Medical Center (Approval No. 2020-008-02-KY). The two principal options for CM induction therapy include amphotericin B (AmB) combined with flucytosine and AmB combined with fluconazole, and decisions with respect to choice of either of these options are based on clinical patient characteristics, and direction from the 2010 Infectious Diseases Society of America guidelines15 and Chinese expert consensus documents.16 All patients were followed up until 24 weeks or death either via inpatient stay, outpatient visits, or telephone calls.
Data Acquisition
Study data were collected for all participants, and included demographics, symptoms and signs, laboratory examination findings, and information regarding prior HIV diagnosis, prior and current ART, diagnosis of opportunistic infections at admission, and combination antifungal treatment after diagnosis of CM. The complete blood count (CBC) included the platelet count, neutrophil count, and lymphocyte count. The composite biomarker, the SII, calculated using the formula  ,17 was longitudinally evaluated at three key time points, ie, 1) the pre-treatment baseline (W0), 2) post-treatment week 2 (W2), and 3) post-treatment week 4 (W4) during antifungal therapy. The SII values at these respective time points are denoted as SII-W0, SII-W2, and SII-W4.
,17 was longitudinally evaluated at three key time points, ie, 1) the pre-treatment baseline (W0), 2) post-treatment week 2 (W2), and 3) post-treatment week 4 (W4) during antifungal therapy. The SII values at these respective time points are denoted as SII-W0, SII-W2, and SII-W4.
Statistical Analysis
Baseline characteristics and outcomes were summarized using frequency and percentages for categorical variables, and means with standard deviations (SD) or medians with interquartile ranges (IQR) for continuous variables. Propensity score matching was used to obtain matched 1:1 samples of HIV patients who had CM or not, using sex and age as covariates. The Mann–Whitney U-test was used to analyze the distributions of SII levels between distinct groups. Correlation was measured using Spearman correlation coefficient between two non-normally distributed continuous variables and using the point-biserial correlation coefficient between a binary and a continuous variable. Receiver operating characteristic (ROC) curves were used to determine the optimal cutoff of SII-W2 and SII-W4, and the participants were categorized into high and low groups accordingly. Further risk stratification of participants was based on the combination of SII-W2 and SII-W4, and their combination with state of consciousness at admission, respectively. Potential prognostic factors were initially assessed using univariable Cox regression, and those with significance (p<0.05) were further analyzed via multivariable Cox proportional hazards models. Survival analysis was performed by the Kaplan–Meier (KM) method, and the differences were compared using the Log-rank (Mantel-Cox) test. Survival predictive accuracy of prognostic models was assessed based on a time-dependent ROC analysis and Harrell’s concordance index (C-index) analysis. Data analyses were performed using GraphPad Software Version 9.5 (GraphPad Prism, La Jolla, California, USA), Statistical Package for the Social Sciences (SPSS) software, Version 27 [IBM SPSS Statistics for Windows, version 27 (IBM Corp., Armonk, N.Y., USA)], and R statistical software package (version 4.3.1). A p-value of <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 322 patients were evaluated for eligibility, and 248 of these patients were eventually selected for inclusion (Figure 1). The median patient age across the study cohort was 44 years (range, 34—53 years), and participants were predominantly male [186 (75%)]. Typical patient symptoms were fever (61.7%), headache (66.5%), and nausea or vomiting (48.8%). The most common comorbidities present in the study cohort were oral candidiasis, tuberculosis, and cytomegalovirus infection, seen in >15% of patients. In total, 22.6% of patients were taking or had previously taken ART. The median CD4+ T-cell count was 33 cells/μL (IQR, 14—53) at enrollment, and 8.9% of patients had an HIV viral load of <200 copies/mL. The majority (67.7%) of patients received an AmB-based combination antifungal regimen. The study cohort was also characterized by elevated CSF protein levels, reduced CSF glucose levels, and increased CSF intracranial pressure (ICP). Overall mortality was 21.8% (54/248) within 24 weeks. Patient characteristics and mortality are provided in Table 1.
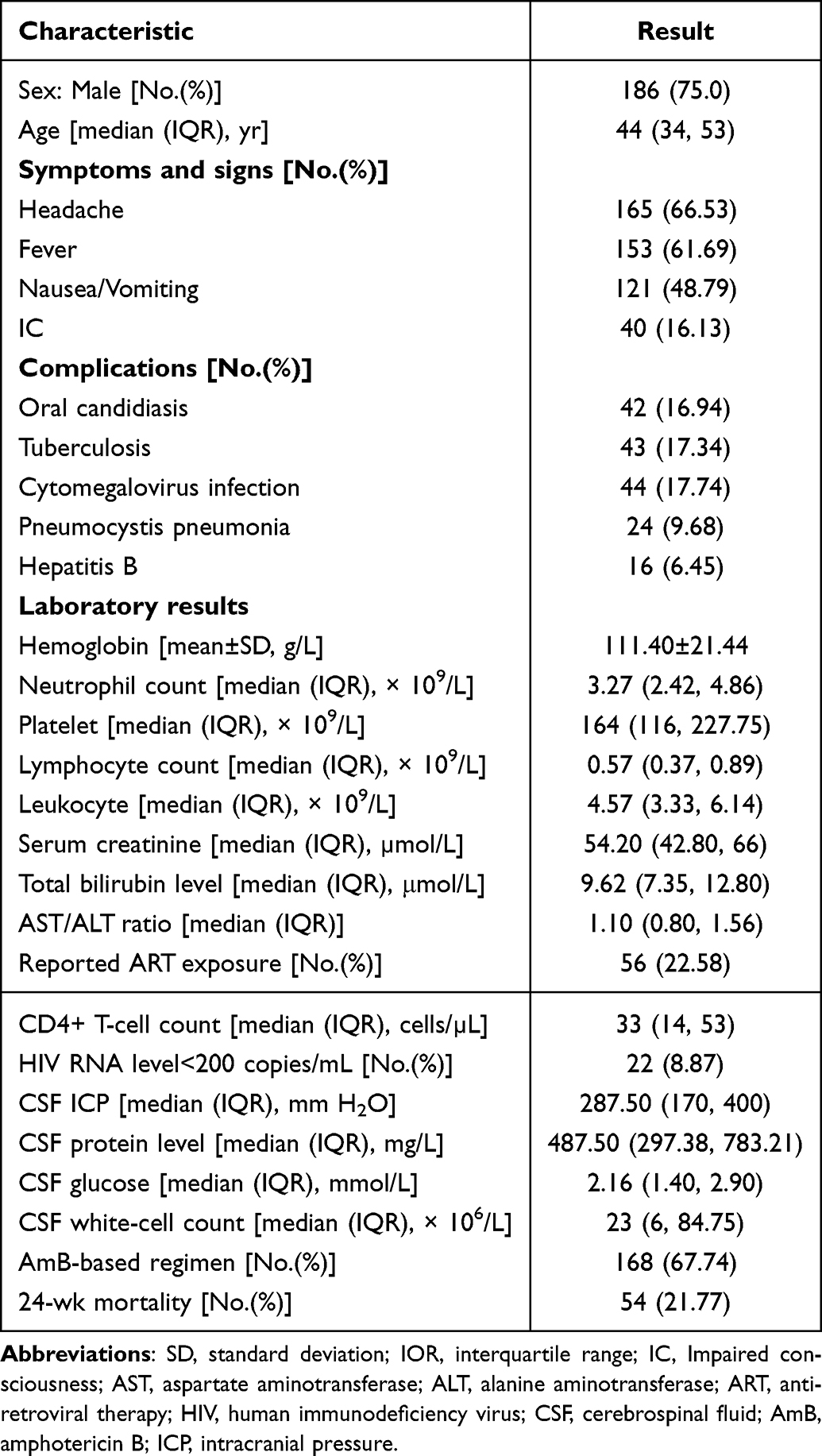 |
Table 1 Characteristics of Included Participants |
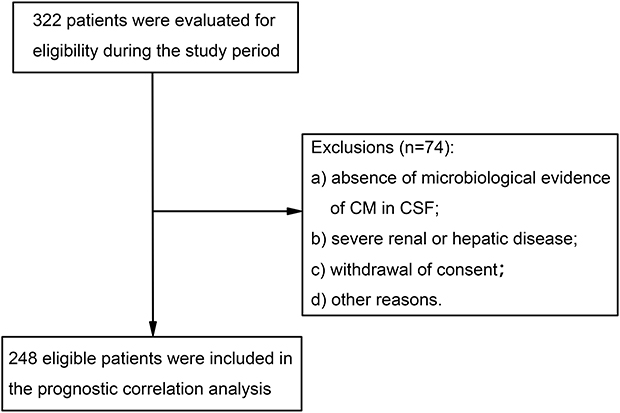 |
Figure 1 Study flowchart of patient inclusion and exclusion criteria for the analysis. Abbreviations: CM, cryptococcal meningitis; CSF, cerebrospinal fluid. |
Comparison of SII Levels in Different Populations
To delineate the specific impact of HIV infection on SII levels, we recruited an additional cohort of 236 individuals with HIV without CM as controls. Subsequently, a propensity score-matched cohort comprising 209 matched pairs (418 patients) was constructed, with each pair containing one HIV-infected individual with no CM and one HCM patient. The baseline SII levels in HCM patients were significantly higher than those in HIV-infected individuals not having CM (median [IQR], 1019.7×109/L [499.9—1873.2×109/L] vs 425.5×109/L [211.5—963.7×109/L], respectively, p<0.0001) (Figure 2a). We further performed a comparative analysis of SII levels at each follow-up time point for HCM patients with different clinical outcomes (Figure 2b). SII levels were significantly elevated in non-survivors compared to survivors at week 2 (median [IQR], 1236.6×109/L [565.5—1998.5×109/L] vs 571.8×109/L [238.9—1123.2×109/L], respectively, p<0.001) and also at week 4 (median [IQR], 1096.4×109/L [505.9—1955.4×109/L] vs 385.1×109/L [205.4—625.4×109/L], p<0.0001). However, no significant difference was observed in baseline SII levels between participants who succumbed from HCM and those who survived from HCM (median [IQR], 1190.7×109/L [437.8—2013.3×109/L] vs 951.9×109/L [501.7—1763.5×109/L], respectively, p=0.382).
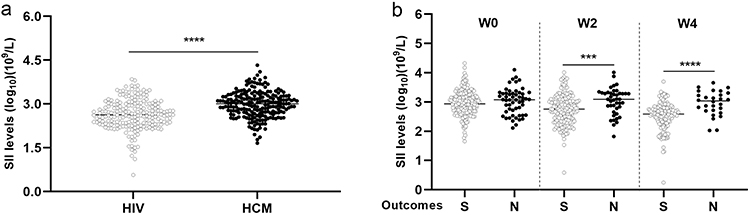 |
Figure 2 SII levels according to different populations. (a) Differences in baseline SII levels between matched HIV patients (n=209) and HCM patients (n=209). (b) Differences in SII levels at W0 (n=248), W2 (n=236), and W4 (n=199) between survivors and non-survivors in the HCM cohort. (note: “***” means p<0.001; “****” means p<0.0001). Abbreviations: SII, systemic immune-inflammation index; HCM, HIV-associated cryptococcal meningitis; S, survivors; N, non-survivors, W0, pre-treatment baseline; W2, post-treatment week 2, W4, post-treatment week 4. |
Correlation Between Baseline SII Levels and Clinical Characteristics
The median (range) SII level at baseline was 1010.5×109/L (498.1—1850.8×109/L). A statistically significant, albeit weak, negative correlation was observed between SII levels and CD4+ T-cell counts (r=−0.245, p<0.001, Figure 3). CD4+ T-cell counts serve as an indicator of HIV/AIDS progression. Therefore, elevated SII levels may suggest inflammatory activation of the immune system and declining immune function in HCM patients, which in turn negatively affects CD4+ T-cell counts and reflects disease progression. The remaining correlations between other variables and SII levels did not reach statistical significance, as shown in Supplementary Table 1.
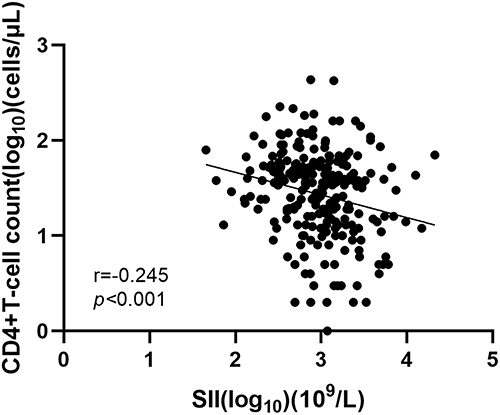 |
Figure 3 Correlation analysis of the SII with CD4+ T-cell count in HCM patients (n=245). Abbreviation: SII, systemic immune-inflammation index. |
Prognostic Factors in Univariate and Multivariate Analyses
The optimal cut-off values of SII levels for prediction of survival were determined through ROC analysis (Supplementary Figure 1) as follows: SII-W0 was 1122.16×109/L [area under the curve (AUC) = 0.539; 95% CI, 0.475—0.602]; SII-W2 was 1049.30×109/L (AUC = 0.676; 95% CI, 0.612—0.735); and SII-W4 was 725.42×109/L (AUC = 0.791; 95% CI, 0.728—0.845). Based on the optimal cutoff values, patients were stratified into two groups (the low inflammatory index group and the high inflammatory index group). The respective corresponding sensitivities and specificities were 55.6% and 59.3% for SII-W0, 57.1% and 73.7% for SII-W2, and 68.8% and 81.9% for SII-W4 (Supplementary Table 2).
We assessed the prognostic factors that might affect the survival of HCM individuals (Table 2). In the univariate analyses, we observed that SII-W2 ≥1049.3×109/L (hazard ratio [95% CI]; 3.11 [1.69—5.73], p<0.001), SII-W4 ≥725.42×109/L (6.43 [2.96—13.94], p<0.001), age ≥50 years (2.15 [1.26—3.67], p=0.005), headache (0.56 [0.33—0.96], p=0.035), nausea/vomiting (1.94 [1.12—3.37], p=0.019), impaired consciousness (IC) (2.30 [1.27—4.17], p=0.006), and non-AmB treatment (1.78×109/L [1.04—3.05], p=0.035) were closely associated with mortality outcomes within 24 weeks. Moreover, although not statistically significant (p=0.059), patients in the low SII-W0 group had numerically higher overall survival rates than those in the high SII-W0 group. Multivariate analyses confirmed the independent prognostic role of SII-W2 ≥1049.3×109/L (adjusted hazard ratio [95% CI]: 2.51 [1.09—5.76], p=0.03), SII-W4 ≥725.42×109/L (5.47 [2.38—12.6], p<0.001), and IC (2.97 [1.25—7.03], p=0.014) for 24-week mortality, after adjustment for potential confounders (see Table 2).
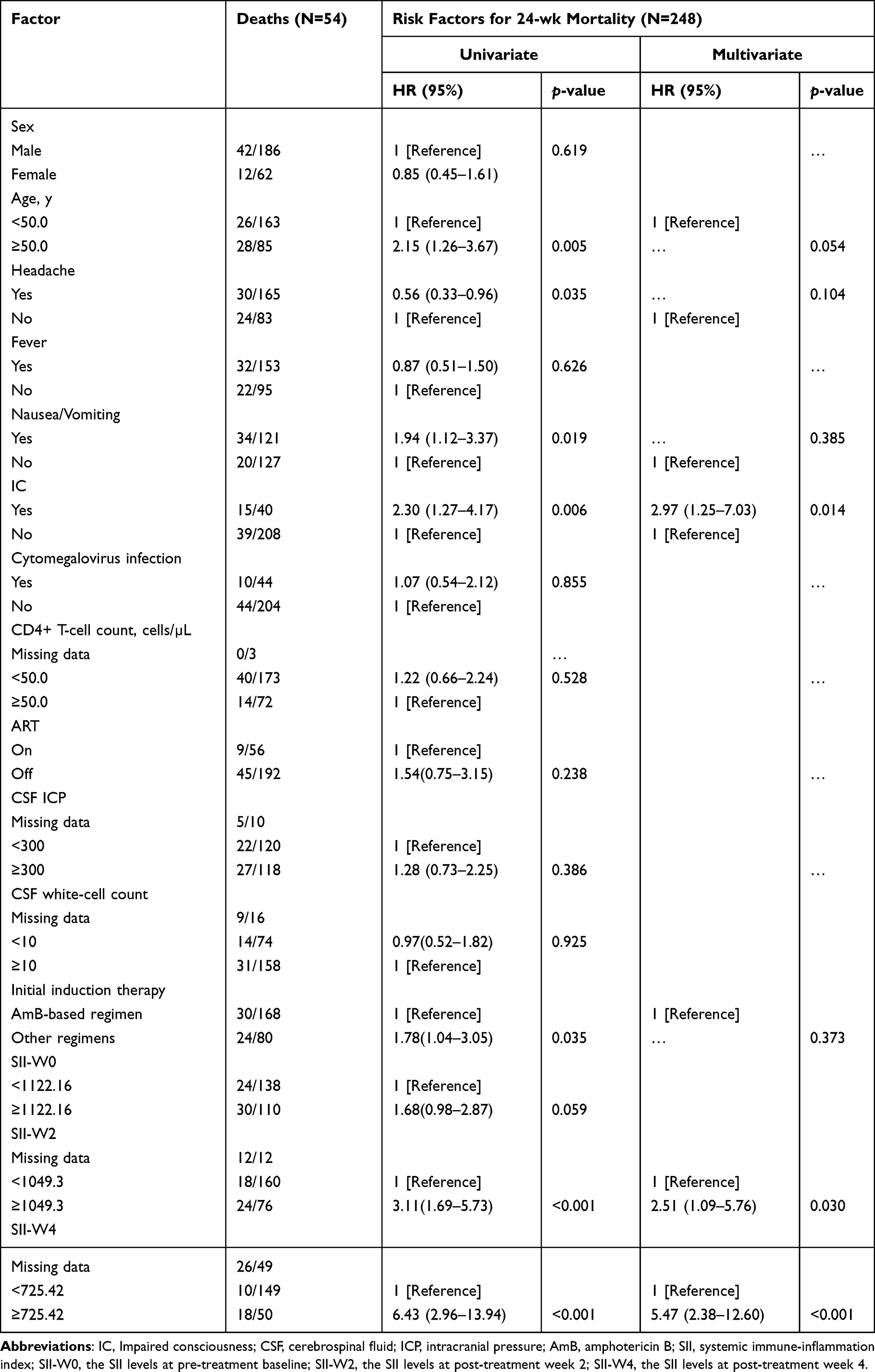 |
Table 2 Risk Factors for 24-week Mortality in HCM Patients in Univariate/Multivariate Cox Regression Analysis |
Kaplan–Meier analysis highlighted a significant association between elevated levels of SII after antifungal therapy and poor outcomes in patients with HCM (Figure 4a and b). Cumulative survival was significantly lower in HCM patients with high levels of SII (ie, SII-W2 ≥1049.3×109/L) compared with patients with low levels of SII (ie, SII-W2 <1049.3×109/L), and the difference between the two groups was calculated to be statistically significant (log-rank p=0.0001, Figure 4a). Comparable results were observed after four weeks of antifungal therapy, with a lower cumulative survival rate in patients with SII-W4 ≥725.42×109/L than in patients with SII-W4 <725.42×109/L (log-rank p<0.0001, Figure 4b). Furthermore, we observed a significant difference in 24-week survival rates between patients with and without IC at admission, with patients without IC showing significantly higher cumulative survival rates compared to those with IC (log-rank p=0.0048, Figure 4c).
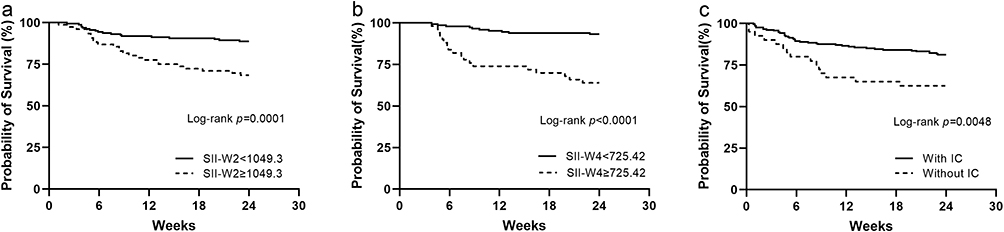 |
Figure 4 Kaplan-Meier survival curves for 24-week outcomes in patients with HCM. Kaplan-Meier curves of cumulative survival in HCM patients according to SII-W2 (n=236), (a), SII-W4 (n=199), (b), and IC (n=248), (c). Each p-value was calculated by Log rank testing. Abbreviations: SII, systemic immune-inflammation index; SII-W2, the SII levels at post-treatment week 2; SII-W4, the SII levels at post-treatment week 4; IC, impaired consciousness. |
Predictive Ability of Combined SII-W2 and SII-W4 for Survival Outcomes
In order to facilitate further validation, patients were categorized into four groups [(SII-W2 ≥1049.3×109/L and SII-W2 <1049.3×109/L) and (SII-W4 ≥725.42×109/L and SII-W4 <725.42×109/L)] based on SII levels measured at both two and four weeks following antifungal treatment. The combination of two prognostic factors was observed to improve the risk stratification for 24-week survival (p<0.0001). In this analysis, patients in the SII-W4 <725.42×109/L and the SII-W2 <1049.3×109/L groups were observed to have the best prognosis, with a survival rate of 95.7%. For patients with SII-W4 ≥725.42×109/L or SII-W2 ≥1049.3×109/L, the survival rate was intermediate. Specifically, survival rates in the SII-W4 ≥725.42×109/L and SII-W2 <1049.3×109/L groups were observed to be 71.4%, which was lower than the 87.1% observed in the SII-W4 <725.42×109/L and the SII-W2 ≥1049.3×109/L groups. However, patients in the high SII-W4 ≥725.42×109/L and SII-W2 ≥1049.3×109/L group were observed to have the poorest survival data (Figure 5a).
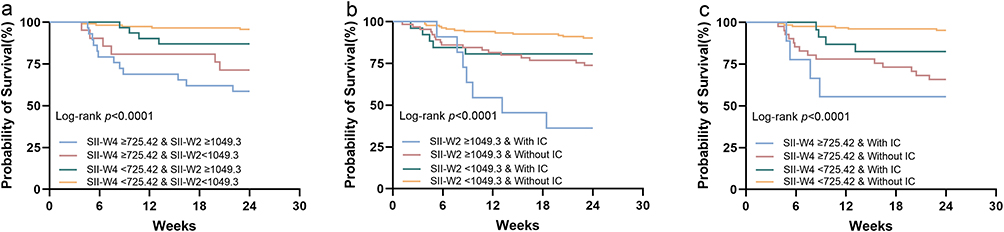 |
Figure 5 Kaplan-Meier survival curves for 24-week survival based on combinations of (a) SII-W2 and SII-W4, (b) SII-W2 and IC status, and (c) SII-W4 and IC status. Sample sizes for each variable were n=236 for SII-W2, n=199 for SII-W4, and n=248 for IC. Abbreviations: SII, systemic immune-inflammation index; SII-W2, the SII levels at post-treatment week 2; SII-W4, the SII levels at post-treatment week 4; IC, impaired consciousness. |
The Combination of IC and SII-W2 or SII-W4 May Better Predict Survival Outcomes
The results of our analysis indicate that SII levels following antifungal therapy may serve as an independent prognostic marker for cumulative survival in HCM patients. Additionally, given the established role of IC as a predictive marker for patient prognosis, we investigated the combined effect of SII levels together with IC at hospital admission in the quest to improve the accuracy of survival outcome prediction. To this end, patients were categorized into risk groups based on their state of consciousness and SII-W2 or SII-W4 levels, aiming to determine whether the resultant prognostic value is additive.
When stratified according to SII-W2 levels and IC status, patients with both elevated SII-W2 (≥1049.3×109/L) and IC demonstrated significantly lower cumulative survival rates compared to the other groups (p<0.0001, Figure 5b), indicating a synergistic adverse effect. Similarly, classification based on SII-W4 and IC status yielded enhanced discrimination of survival risk. Patients with SII-W4 <725.42×109/L and without IC exhibited the most favorable prognosis. Those with either SII-W4 ≥725.42×109/L or IC alone showed intermediate survival outcomes. Consistent with the observations for SII-W2, patients with SII-W4 ≥725.42×109/L and concomitant IC were observed to be associated with an extremely high risk of mortality (Figure 5c). These results underscore the potential clinical utility of integrating levels of markers of systemic inflammation together with clinicopathologic features to refine risk stratification, and guide early therapeutic decision-making in HCM management.
To further quantify the discriminatory power of this combination, we evaluated the predictive performance of a model incorporating both SII-W4 and IC. The model exhibited favorable predictive accuracy, with a C-index of 0.771 (95% CI: 0.684–0.857). We subsequently investigated whether the inclusion of CD4+ T-cell counts may improve model performance; however, no significant enhancement was observed (C-index: 0.773, 95% CI: 0.685–0.861; p=0.738). Furthermore, time-dependent ROC analysis at 24 weeks revealed highly similar AUC values for both models (0.796 vs 0.798; Supplementary Figure 2), underscoring the robust prognostic utility of combining SII-W4 with IC.
Discussion
This study investigated the relationship between SII levels and short-term clinical outcomes in patients with HCM. Our observations indicate that SII levels at presentation are significantly higher in patients with HCM compared to those with HIV without CM. Importantly, elevated SII levels during treatment are independently associated with an increased risk of mortality in the HCM cohort. Interestingly, a significant negative correlation was observed between SII levels and CD4+ T-cell counts. Additionally, the outcomes of this study suggest that monitoring SII-W2 and SII-W4 levels and combining these indices in assessment and prognostic analyses may assist in the early identification of high-risk individuals. Furthermore, the combination of each of these two SII risk indicators with IC status improves the prognostic significance. Thus, SII may serve as a valuable surrogate for prediction of clinical outcomes following antifungal therapy in HCM patients.
The clinical outcome of cryptococcal infection depends on a precarious balance between the virulence of the pathogen and host immune responses and immune regulation.18,19 Lymphocytes are well-established as critical components of the immune defense against pathogenic microorganisms. A reduced peripheral lymphocyte count has been identified as a poor prognostic predictor for CM patients with connective tissue disease.20 Notably, the profound depletion of CD4+ T-cells is a hallmark of HCM, with lower CD4+ T-cell counts being independently associated with CM recurrence or mortality in HCM patients.8 In addition to adaptive immunity, innate immune responses, especially those involving neutrophils, also contribute significantly to disease progression.21 The “priming” of neutrophils by bacteria and fungi acts as a double-edged sword, promoting effective pathogen clearance while potentially inducing immunopathology though the release of reactive oxygen species (ROS) and neutrophil extracellular traps (NETs).21 Interestingly, one murine model of pulmonary cryptococcosis demonstrated improved survival in neutropenic mice compared to immunocompetent controls, suggesting that excessive neutrophil activity may be detrimental in certain contexts.22 Clinically, elevated neutrophil counts in HCM patients have been associated with increased mortality.6 The NLR serves as a diagnostic and prognostic marker of disease severity in patients with inflammatory conditions, reflecting the balance between innate and adaptive immunity.6 An increasing NLR during antifungal therapy has been proposed as a potential indicator of treatment failure in patients with CM.23 Furthermore, elevated neutrophil and NLR levels, alongside reduced lymphocyte, and monocyte counts, have been identified as risk factors for cryptococcal dissemination.24 Platelets have been shown to facilitate the recruitment of pathogenic eosinophils and exacerbate disease progression during cryptococcal infection.25 In addition, the platelet-to-lymphocyte ratio (PLR) and NLR have been proposed as indicators of the severity of systemic disturbances in the inflammatory and coagulation processes, which may contribute to increased mortality in people with HIV.26
The systemic immune-inflammation index (SII) biomarker is derived from peripheral neutrophil, lymphocyte, and platelet counts, and serves as a composite marker reflecting both inflammatory and immunological status. Prior research has established its substantial predictive value across various diseases, such as COVID-19, acute ischemic stroke, and malignant tumors;10,27,28 however, its utility in the context of HCM remains to be determined. In our study, SII was measured at admission and at weeks 2 and 4 to capture baseline status and early treatment response during the induction phase, a period critical for fungal clearance and survival. Mortality was then monitored over a 24-week follow-up term, which encompasses the early high-risk period and short-term outcomes while maintaining feasible follow-up. We observed that elevated SII values at 2 and 4 weeks following antifungal treatment were associated significantly with increased cumulative mortality. Notably, patients with SII levels exceeding an identified threshold exhibited a 2.5- to 5.5-fold higher risk of death compared to those with lower SII levels. These observations suggest that SII may serve as a surrogate marker of systemic inflammatory response and immune dysregulation, with a potential utility in prognostic risk stratification among patients with HCM.
Currently, there is a lack of clarity regarding the specific fundamental mechanisms responsible for increased SII levels in patients with HCM. One potential factor for this is the fact that HIV infection may directly alter hematological parameters via its effects on bone marrow, which in turn lead to elevated SII levels. One recent study observed that SII levels are significantly higher in ART-naïve HIV patients compared with those on ART, and while SII levels of ART-naïve HIV patients were also numerically elevated compared against non-HIV controls, this difference does not achieve statistical significance.29 Interestingly, another report showed that virologically suppressed HIV patients had lower SII levels than those without HIV,30 perhaps benefiting from the effect of ART on specific hematological parameters. Lower CD4+ T-cell counts (particularly <200 cells/µL) are associated with an increased likelihood of hematological abnormalities,31,32 and this is consistent with our observation that higher SII negatively correlates with lower CD4+ T-cell counts in HCM patients. Secondly, immunological perturbations and inflammatory responses driven by the cryptococcal organism and their antigens might influence SII levels. Cryptococcal infection is a hallmark of HIV disease progression, and its co-infection has been shown to alter the host immune system.33 Additionally, Li et al, have demonstrated the presence of a predominantly pro-inflammatory microenvironment characterized by elevated levels of cytokines (IL-4 and TNF-α) in patients with HIV co-infection with Cryptococcus.34 In the present study, we observed that SII levels were significantly higher in HIV patients with Cryptococcus co-infection than in those with HIV alone, suggesting that Cryptococcus co-infection may affect SII levels by materially altering the systemic immunological and inflammatory status.
IC that is observed at the time of CM diagnosis is associated with increased mortality risk in HCM patients.35 This relationship has also been observed in HIV-negative CM patients, where IC not only serves as an independent prognostic factor but also correlates significantly with survival duration.36 Consistent with these clinical findings, our cohort analysis revealed that non-survivors were significantly more likely to present with IC at baseline, compared to survivors. Furthermore, altered mental status [Glasgow Coma Scale (GCS) <15] at presentation has been linked to an elevated risk of neurocognitive impairment at 12 weeks post-treatment among HCM patients.37 In our study, further analysis showed that the combination of an elevated SII together with IC had significant prognostic predictive value for poor outcomes, suggesting that the synergistic effect of peripheral and central immune-inflammatory responses may exacerbate mortality risk. This result is consistent with the outcomes of a risk stratification model for HCM that has been previously designed and created by our team,35 which identified IC as a significant risk factor contributing to mortality, and collectively emphasizes the predictive and prognostic “early warning” value of IC in the clinical management of HCM.
Limitations across the present study include: i) the relatively limited sample size and potential unmeasured confounders (eg, concurrent infections, steroid therapy, or other triggers of stress) may have influenced the dynamics of SII. In addition, the prognostic utility of SII observed in our cohort has not yet been externally validated, which limits generalizability; ii) some clinical parameters such as GCS scores, body mass index (BMI), and inflammatory markers [including C-reactive protein (CRP) and procalcitonin (PCT) levels] were not available, limiting the depth of our clinical correlational analysis. Moreover, we were unable to perform cytokine profiling (eg, IL-6, IL-10) or to include fungal burden data, which would have provided a deeper understanding of the inflammatory drivers underlying SII; iii) The optimal monitoring duration of SII beyond week 4 remains unclear, and the clinical applicability and predictive value of SII should be further confirmed in larger, prospective cohorts.
Overall, our study suggests that elevated SII values at 2- and 4-weeks following antifungal therapy are independently associated with poor 24-week outcomes in patients with HCM. The SII may serve as a potential and readily accessible prognostic biomarker, which alone or in combination with IC status may also facilitate the early identification of high-risk populations. Further well-designed in-depth studies are required to evaluate the impact of the SII on survival in the HCM population, and its predictive and prognostic potential in clinical settings.
Data Sharing Statement
Supplementary material is available at Journal of Inflammation Research online. Consisting of data provided by the authors to benefit the reader, the posted material has been professionally copyedited, and is the sole responsibility of the authors. Questions or comments should thus be addressed to the corresponding author.
Acknowledgments
We would like to thank all the patients and healthcare workers of the 15 hospitals from around China that were involved in this study, viz., Chongqing Public Health Medical Center, Harbin Medical University, Guangxi Longtan Hospital of Guangxi Zhuang Autonomous Region, The First Affiliated Hospital of Zhejiang University, Liuzhou General Hospital, the Third People’s Hospital of Guilin, the First Hospital of Changsha, the Fourth People’s Hospital of Nanning, Kunming Third People’s Hospital, Public Health Clinical Center of Chengdu, Guiyang Public Health Clinical Center, Xixi Hospital of Hangzhou, Beijing Youan Hospital of Capital Medical University, the Third People’s Hospital of Shenzhen, and Tianjin Second People’s Hospital.
Funding
The work was supported by the Joint Medical Research Projects of Chongqing Municipal Health Committee and Chongqing Municipal Science and Technology Bureau (2024MSXM088, 2022QNXM032, 2024ZDXM015), the Chongqing AIDS Medical Research Center Construction Program, the Chongqing Disease Prevention and Public Health Research Center Construction Program, the Chongqing Key Public Health Disciplines Improvement Project, and the Xinjiang Uighur Autonomous Region Natural Science Foundation (2021D01A128). The funding bodies have had no role in the trial design, trial execution, collection and interpretation of data, manuscript writing and editing, or decision to submit for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rajasingham R, Govender NP, Jordan A, et al. The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. Lancet Infect Dis. 2022;22(12):1748–1755. Erratum in: Lancet Infect Dis. 2023 Jan;23(1):e1. doi: 10.1016/S1473-3099(22)00597-7. PMID: 36049486; PMCID: PMC9701154. doi:10.1016/S1473-3099(22)00499-6
2. Li YN, Wang ZW, Li F, et al. Inhibition of myeloid-derived suppressor cell arginase-1 production enhances T-cell-based immunotherapy against Cryptococcus neoformans infection. Nat Commun. 2022;13(1):4074. PMID: 35835754; PMCID: PMC9283461. doi:10.1038/s41467-022-31723-4
3. Boulware DR, Meya DB, Bergemann TL, et al. Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: a prospective cohort study. PLoS Med. 2010;7(12):e1000384. PMID: 21253011; PMCID: PMC3014618. doi:10.1371/journal.pmed.1000384
4. Chang CC, Lim A, Omarjee S, et al. Cryptococcosis-IRIS is associated with lower cryptococcus-specific IFN-γ responses before antiretroviral therapy but not higher T-cell responses during therapy. J Infect Dis. 2013;208(6):898–906. Epub 2013 Jun 12. PMID: 23766525; PMCID: PMC3749010. doi:10.1093/infdis/jit271
5. Scriven JE, Graham LM, Schutz C, et al. A glucuronoxylomannan-associated immune signature, characterized by monocyte deactivation and an increased interleukin 10 level, is a predictor of death in cryptococcal meningitis. J Infect Dis. 2016;213(11):1725–1734. Epub 2016 Jan 14. PMID: 26768248; PMCID: PMC4857465. doi:10.1093/infdis/jiw007
6. Musubire AK, Meya DB, Rhein J, COAT and ASTRO trial teams, et al. Blood neutrophil counts in HIV-infected patients with cryptococcal meningitis: association with mortality. PLoS One. 2018;13(12):e0209337. PMID: 30596708; PMCID: PMC6312212. doi:10.1371/journal.pone.0209337
7. Chesdachai S, Engen NW, Rhein J, et al. Baseline Serum C-reactive protein level predicts mortality in cryptococcal meningitis. Open Forum Infect Dis. 2020;7(12):ofaa530. PMID: 33335936; PMCID: PMC7727340. doi:10.1093/ofid/ofaa530
8. Li Y, Lu Y, Nie J, et al. Potential predictors and survival analysis of the relapse of HIV-associated cryptococcal meningitis: a retrospective study. Front Med (Lausanne). 2021;8:626266. PMID: 34041249; PMCID: PMC8141581. doi:10.3389/fmed.2021.626266
9. Yang R, Chang Q, Meng X, Gao N, Wang W. Prognostic value of systemic immune-inflammation index in cancer: a meta-analysis. J Cancer. 2018;9(18):3295–3302. PMID: 30271489; PMCID: PMC6160683. doi:10.7150/jca.25691
10. Fois AG, Paliogiannis P, Scano V, et al. The systemic inflammation index on admission predicts in-hospital mortality in COVID-19 patients. Molecules. 2020;25(23):5725. PMID: 33291581; PMCID: PMC7731255. doi:10.3390/molecules25235725
11. Mangalesh S, Dudani S, Malik A. The systemic immune-inflammation index in predicting sepsis mortality. Postgrad Med. 2023;135(4):345–351. Epub 2022 Nov 8. PMID: 36287784. doi:10.1080/00325481.2022.2140535
12. Agus HZ, Kahraman S, Arslan C, et al. Systemic immune-inflammation index predicts mortality in infective endocarditis. J Saudi Heart Assoc. 2020;32(1):58–64. PMID: 33154893; PMCID: PMC7640593. doi:10.37616/2212-5043.1010
13. Li L, Yang L, Yuan Z, Wu Q, Lyu X. The combination of systemic immune-inflammation index and serum procalcitonin has high auxiliary predictive value for short-term adverse prognosis in septic shock patients. J Emerg Med. 2024;67(4):e357–e367. Epub 2024 May 17. PMID: 39183119. doi:10.1016/j.jemermed.2024.05.005
14. Zheng J, Zheng L, Wang X, et al. The clinical value of the combined detection of Systemic Immune-Inflammation Index (SII), Systemic Inflammation Response Index (SIRI), and Prognostic Nutritional Index (PNI) in early diagnosis of gastric cancer. J Inflamm Res. 2025;18:813–826. PMID: 39845022; PMCID: PMC11752871. doi:10.2147/JIR.S496703
15. Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2010;50(3):291–322. PMID: 20047480; PMCID: PMC5826644. doi:10.1086/649858
16. Liu ZY, Wang GQ, Zhu LP, et al. Society of infectious diseases, Chinese Medical Association. [Expert consensus on the diagnosis and treatment of cryptococcal meningitis]. Zhonghua Nei Ke Za Zhi. 2018. 57(5):317–323. Chinese. PMID: 29747285. doi:10.3760/cma.j.issn.0578-1426.2018.05.003
17. Huang S, Zhou Z, Yang D, et al. Persistent white matter changes in recovered COVID-19 patients at the 1-year follow-up. Brain. 2022;145(5):1830–1838. PMID: 34918020; PMCID: PMC8754808. doi:10.1093/brain/awab435
18. Shourian M, Qureshi ST. Resistance and tolerance to cryptococcal infection: an intricate balance that controls the development of disease. Front Immunol. 2019;10:66. PMID: 30761136; PMCID: PMC6361814. doi:10.3389/fimmu.2019.00066
19. Tenforde MW, Scriven JE, Harrison TS, Jarvis JN. Immune correlates of HIV-associated cryptococcal meningitis. PLoS Pathog. 2017;13(3):e1006207. PMID: 28334020; PMCID: PMC5363984. doi:10.1371/journal.ppat.1006207
20. Liu S, Hu S, Jiang Y, Zuo X, Zhou Y. Clinical characteristics for connective tissue disease complicated with cryptococcal meningitis. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2019. 44(8):905–910. Chinese. PMID: 31570678. doi:10.11817/j.issn.1672-7347.2019.190082
21. Pillai PS, Molony RD, Martinod K, et al. Mx1 reveals innate pathways to antiviral resistance and lethal influenza disease. Science. 2016;352(6284):463–466. PMID: 27102485; PMCID: PMC5465864. doi:10.1126/science.aaf3926
22. Mednick AJ, Feldmesser M, Rivera J, Casadevall A. Neutropenia alters lung cytokine production in mice and reduces their susceptibility to pulmonary cryptococcosis. Eur J Immunol. 2003;33(6):1744–1753. PMID: 12778493. doi:10.1002/eji.200323626
23. Zhang K, Li H, Zhang L, et al. The change in the neutrophil/lymphocyte ratio predicts the prognosis of patients with cryptococcal meningitis. Mycopathologia. 2021;186(6):857–862. Epub 2021 Aug 31. PMID: 34467475. doi:10.1007/s11046-021-00553-1
24. Tao Z, Pu Q, Shen Y, et al. Clinical characteristics and prognostic factors of pulmonary and extrapulmonary cryptococcosis. BMC Infect Dis. 2024;24(1):1018. PMID: 39304813; PMCID: PMC11414175. doi:10.1186/s12879-024-09895-9
25. De Giovanni M, Dang EV, Chen KY, An J, Madhani HD, Cyster JG. Platelets and mast cells promote pathogenic eosinophil recruitment during invasive fungal infection via the 5-HIAA-GPR35 ligand-receptor system. Immunity. 2023;56(7):1548–1560.e5. Epub 2023 Jun 5. PMID: 37279752; PMCID: PMC10360074. doi:10.1016/j.immuni.2023.05.006
26. Raffetti E, Donato F, Casari S, et al. Systemic inflammation-based scores and mortality for all causes in HIV-infected patients: a MASTER cohort study. BMC Infect Dis. 2017;17(1):193. PMID: 28264665; PMCID: PMC5339992. doi:10.1186/s12879-017-2280-5
27. Ma F, Li L, Xu L, et al. The relationship between systemic inflammation index, systemic immune-inflammatory index, and inflammatory prognostic index and 90-day outcomes in acute ischemic stroke patients treated with intravenous thrombolysis. J Neuroinflammation. 2023;20(1):220. PMID: 37777768; PMCID: PMC10543872. doi:10.1186/s12974-023-02890-y
28. Li J, Cao D, Huang Y, et al. The prognostic and clinicopathological significance of systemic immune-inflammation index in bladder cancer. Front Immunol. 2022;13:865643. PMID: 35572533; PMCID: PMC9097688. doi:10.3389/fimmu.2022.865643
29. Aikpitanyi-Iduitua GA, Idemudia NL, Aikpitanyi-Iduitua RO, Omoregie R. Correlation of selected inflammatory markers with cardiovascular diseases markers among HIV patients in Benin City, Nigeria. New Zealand Journal of Medical Laboratory Science. 2023;77(1):33–37. doi:10.3316/informit.925139987911545
30. Wang CX, Letendre SL, Hong S, Andalibi M, Iudicello JE, Ellis RJ. Differential systemic immune-inflammation index levels in people with and without HIV infection. AIDS. 2025;39(5):554–559. Epub 2024 Dec 12. PMID: 39668666; PMCID: PMC12005313. doi:10.1097/QAD.0000000000004088
31. Vaswani PPM, Senga-Tang IR, Catapia JRM, Abad CLR, Dumagay TE. The hematologic profile of Filipino HIV-infected individuals and its association with CD4 counts. Hematol Transfus Cell Ther. 2022;44(3):307–313. Epub 2021 Jan 3. PMID: 33431267; PMCID: PMC9477755. doi:10.1016/j.htct.2020.10.964
32. Parinitha S, Kulkarni M. Haematological changes in HIV infection with correlation to CD4 cell count. Australas Med J. 2012;5(3):157–162. Epub 2012 Mar 31. PMID: 22952560; PMCID: PMC3433730. doi:10.4066/AMJ.20121008
33. Chen J, Shao J, Dai M, Fang W, Yang YL. Adaptive immunology of Cryptococcus neoformans infections-an update. Front Immunol. 2023;14:1174967. PMID: 37251371; PMCID: PMC10213923. doi:10.3389/fimmu.2023.1174967
34. Linyu L, Ali Abuderman AW, Muzaheed, Acharya S, Divakar DD. Modulation of host immune status by cryptococcus co-infection during HIV-1 pathogenesis and its impact on CD+4 cell and cytokines environment. Microb Pathog. 2020;139:103864. Epub 2019 Nov 9. PMID: 31715319. doi:10.1016/j.micpath.2019.103864
35. Zhao T, Xu XL, Nie JM, et al. Establishment of a novel scoring model for mortality risk prediction in HIV-infected patients with cryptococcal meningitis. BMC Infect Dis. 2021;21(1):786. PMID: 34376147; PMCID: PMC8353436. doi:10.1186/s12879-021-06417-9
36. Zheng H, Chen Q, Xie Z, et al. A retrospective research of HIV-negative cryptococcal meningoencephalitis patients with acute/subacute onset. Eur J Clin Microbiol Infect Dis. 2016;35(2):299–303. Epub 2016 Jan 20. PMID: 26792138. doi:10.1007/s10096-015-2545-0
37. Nsangi L, Hullsiek KH, Dai B, et al. Neurocognitive impairment among cryptococcal meningitis survivors in Uganda, a Prospective Cohort Study. Open Forum Infect Dis. 2025;12(2):ofaf054. PMID: 40008306; PMCID: PMC11850114. doi:10.1093/ofid/ofaf054
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Systemic Immune-Inflammation Index: A Promising, Non-Invasive Biomarker for Crohn’s Disease Activity and Severity Assessment
Deng Y, Fu T, Gao D, Zhou J, Nie X, Wang F, Yu Q
International Journal of General Medicine 2025, 18:483-496
Published Date: 30 January 2025
The Influence of Characteristics and Indexes (NLR, PNI, and SII) Evaluated at Admission on the Mortality Prediction of Infectious Endocarditis Patients
Sezen AI, Ozdemir YE, Borcak D, Goklu BN, Bilgin Z, Turkyilmaz G, Caglar FNT, Gedik H, Kart Yasar K
International Journal of General Medicine 2025, 18:5617-5627
Published Date: 18 September 2025