Back to Journals » Journal of Inflammation Research » Volume 16
Association Between Systemic Immune Inflammation Level and Poor Prognosis Across Different Glucose Metabolism Status in Coronary Artery Disease Patients
Authors Xu X, Xie Y, Gu X, Zhou Y, Kang Y, Liu J, Lai W, Lu H, Chen S, Xu J ![]() , Lin F, Liu Y
, Lin F, Liu Y
Received 11 June 2023
Accepted for publication 2 September 2023
Published 12 September 2023 Volume 2023:16 Pages 4031—4042
DOI https://doi.org/10.2147/JIR.S425189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xiayan Xu,1– 3,* Yun Xie,2– 4,* Xia Gu,5– 7,* Yang Zhou,2,3 Yu Kang,2,3,8 Jin Liu,2,3 Wenguang Lai,2– 4 Hongyu Lu,2,3 Shiqun Chen,2,3 Jun-yan Xu,2,3,9 Feng Lin,10 Yong Liu1– 3
1School of Medicine, South China University of Technology, Guangzhou, 510006, People’s Republic of China; 2Department of Cardiology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, 510080, People’s Republic of China; 3Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, 510080, People’s Republic of China; 4School of Biology and Biological Engineering South China University of Technology, Guangzhou, 510006, People’s Republic of China; 5Department of Cardiology, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, 150086, People’s Republic of China; 6The Key Laboratory of Myocardial Ischemia, Chinese Ministry of Education, Harbin, Heilongjiang, 150086, People’s Republic of China; 7Cardiovascular Imaging Center, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, 150086, People’s Republic of China; 8Shantou University Medical College, Shantou, 515041, People’s Republic of China; 9Ministry of Education, Key Laboratory of Hainan Trauma and Disaster Rescue, College of Emergency and Trauma, Hainan Medical University, Haikou, 571199, People’s Republic of China; 10Shenzhen People’s Hospital, Shenzhen, 518020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng Lin, Shenzhen People’s Hospital, Shenzhen, 518020, People’s Republic of China, Email [email protected] Yong Liu, South China University of Technology, No. 382, Waihuan East Road, University City, Panyu District, Guangzhou, Guangdong Province, People’s Republic of China, Tel +86 2083827812-10528, Fax +86 2083851483, Email [email protected]
Background: Blood glucose levels significantly affect the clinical prognosis of patients with coronary artery disease (CAD), and systemic immune inflammation is a common risk factor for both CAD and diabetes. However, the relationship between immune inflammation levels and poor prognosis in patients with CAD with different glucose metabolic statuses remains unclear.
Methods: Between January 2007 and December 2020, we recruited 84,645 patients with CAD. The systemic immune inflammation index (SII) was used to comprehensively reflect the immune and inflammatory levels of patients and was calculated using the following formula: neutrophils × platelets/lymphocytes. The patients were classified into nine groups according to their glucose metabolism status (diabetes mellitus [DM], pre-diabetes mellitus [pre-DM], and normal glucose regulation [NGR]). Cox regression models and competing risk Fine and Gray models were used to investigate the association between SII and clinical outcomes.
Results: During the follow-up period, 12,578 patients died, including 5857 cardiovascular-related and 1251 cancer-related deaths. The risk of all-cause and cause-specific mortality increased with increasing SII tertiles in CAD patients with NGR, pre-DM, and DM. When considering glucose metabolism status, the multivariate cox regression revealed that CAD patients with DM and SII-H levels had the highest risk of all-cause mortality (1.69 [1.56– 1.83]), cardiovascular mortality (2.29 [2.02– 2.59]), and cancer mortality (1.29 [1.01– 1.66]). Moreover, incorporating the SII into traditional risk factor models significantly improved the C-index for predicting all-cause and cardiovascular mortality.
Conclusion: Systemic immune inflammation levels on admission were correlated with a higher risk of all-cause and cause-specific mortality in patients with CAD, particularly in those with DM.
Keywords: systemic immune inflammation index, coronary artery disease, type 2 diabetes, prognosis, mortality
Introduction
Coronary artery disease (CAD), a leading global cause of death, primarily because of its widespread prevalence, represents 32.7% of the global burden of cardiovascular disease.1–3 Research has shown a significant correlation between elevated blood glucose levels in individuals with CAD and a heightened risk of all-cause, and cardiovascular mortality.4 Independent of other traditional risk factors, diabetes mellitus (DM) roughly doubles the risk of CAD, according to a meta-analysis of 690,000 individuals.5 Pre-diabetes mellitus (pre-DM) is a metabolic condition that falls between normal glucose regulation (NGR) and DM, serving as an intermediate stage. It is expected to affect over 470 million people by 2030.5 In the absence of intervention, pre-diabetes frequently evolves into DM and is associated with a higher risk of cardiovascular disease.6,7 The risk of negative clinical outcomes varies widely among patients with different glucose metabolism statuses. According to the most recent guidelines from the American Diabetes Association, the European Association for the Study of Diabetes, and the European Society of Cardiology, treatment for different glucose metabolism statuses is greatly influenced by the existence of cardiovascular disease.8–10 Therefore, identifying new tools for stratifying glucose metabolism in patients with CAD is of great value for risk assessment.
As a common precursor of CAD, immunity and inflammation are crucial factors in the onset and progression of CAD.11,12 DM, a common comorbidity of CAD, also creates an immune-inflammatory environment that further damages cardiac structure and function.13 The systemic immune inflammation index (SII) is an emerging indicator proposed in recent years that integrates information on neutrophil, lymphocyte, and platelet counts into one variable and is a more powerful tool than traditional inflammatory indicators.14,15 The SII comprehensively reflects the immune and inflammatory status of patients and is associated with CAD.16 Previous research has provided evidence that SII serves as a robust predictor of the advancement of coronary atherosclerosis. Furthermore, it has been identified as an independent predictor of cardiovascular events, including cardiovascular mortality, nonfatal myocardial infarction, nonfatal stroke, and hospitalization for heart failure, in patients with STEMI.17,18 Nevertheless, to date, no studies have provided evidence regarding the relationship between the SII and prognosis in CAD patients with different glucose metabolism statuses.
Therefore, this large cohort study aimed to investigate the association between systemic immune inflammation and all-cause and cause-specific mortality in CAD patients across different glucose metabolism statuses.
Materials and Methods
Study Population
The Cardiorenal Improvement II (CIN-II) study, a multicenter cohort of patients recruited at five significant tertiary hospitals in China from January 2007 to December 2020 (Cardiorenal Improvement II, ClinicalTrials.gov NCT05050877), provided data for this cohort analysis. A total of 99, 699 patients diagnosed with CAD undergoing coronary angiography (CAG) upon admission were enrolled. The exclusion criteria were as follows: a) age <18 years (n=638); b) missing survival information (n=2923); c) missing following parameters - platelet count, lymphocyte count, and neutrophil count (n=11,153); and d) missing baseline fasting plasma glucose (FPG) and hemoglobin A1c (HbA1c) parameters (n=340). Finally, 84,645 patients were included in the analysis (Figure 1). This study was approved by the Ethics Committee of Guangdong Provincial People’s Hospital (No.GDREC2019-555H-2). To protect patient privacy, all traceable personal identifiers were deleted from the analytical dataset, and all participating sites received approval from their respective institutional review boards and ethics committees. As this study was retrospective, no further intervention was used, and all patient information was anonymized to ensure confidentiality. Therefore, informed consent was not required. This study was conducted in accordance with the principles of the Declaration of Helsinki.
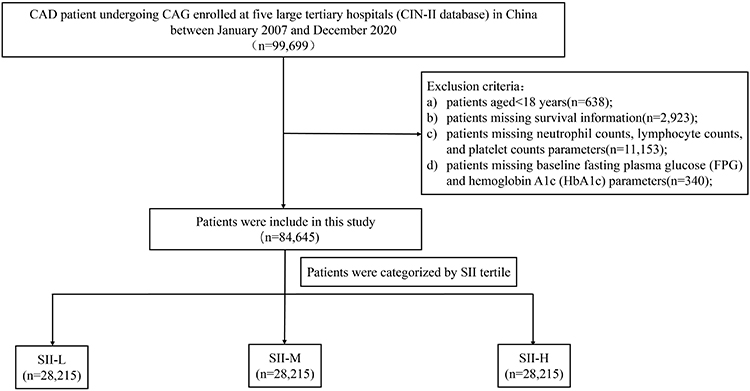 |
Figure 1 Flowchart of study participants. Abbreviations: CAD, coronary artery disease; CAG, coronary angiography; SII, systemic immune inflammation index. |
Baseline Data Collection
Patient information was extracted from the electronic clinical management system. All primary and secondary care records were obtained. Baseline information encompassed a wide range of data including demographic characteristics, comorbidities, medical procedures, laboratory test results, and medications prescribed at the time of discharge. Platelets, neutrophils, lymphocytes, FPG, glycated hemoglobin, and other biochemical indicators were measured upon admission. Survival data were collected from a cause-specific surveillance dataset at the Regional Centers for Disease Control and Prevention (CDC).
Clinical Definition and Endpoint
The endpoints of this study were all-cause, cardiovascular, and cancer mortality. The SII was defined as multiplying the total platelet count with the neutrophil to lymphocyte ratio measured at the time of admission. Based on the guidelines provided by the American Diabetes Association,8 DM was defined as FPG of ≥ 7.0 mmol/L or (HbA1c) of ≥ 6.5% or the current use of hypoglycemic medications. Pre-DM was defined as FPG levels within the range of 5.6 mmol/L to < 7.0 mmol/L or HbA1c levels within the range of 5.7% to < 6.5%. NGR was considered for patients who did not meet the criteria for pre-DM or DM. Anemia was defined as a hematocrit of 39% for males and 36% for females. The estimated glomerular filtration rate (eGFR) was determined using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation,19 and chronic kidney disease (CKD) was defined as an eGFR < 60mL/min/1.73 m2.20 Acute myocardial infarction (AMI) and hypertension (HT) adhered to the guidelines according to the ICD-10 guidelines.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) or median (interquartile range [IQR]), and post hoc multiple comparisons among groups were analyzed by analysis of variance or the Kruskal–Wallis test. Categorical variables were reported as numbers (percentages) and compared using the χ2 test. To establish a dose-response association between SII and the risk of endpoints, restricted cubic spline analyses were performed. The time-to-event data for all-cause mortality among the groups were illustrated by the Kaplan–Meier plots and analyzed using the Log rank test. Cumulative incidence function (CIF) curves for cardiovascular and cancer mortality were used to describe competing hazards, and Gray’s test was used to evaluate group differences. Cox regression models and Fine and Grey models, both of which are presented as adjusted hazard ratios (HR) with 95% confidence intervals (CI), were used to evaluate the SII and endpoints. Baseline variables exhibiting a p-value < 0.0001 or those with clinical significance were incorporated into Cox regression models. Multivariate models were developed using stepwise selection methods. A variance inflation factor <5 was used as the threshold to assess the presence of multicollinearity. The following adjustments were made for age, sex, CKD, HT, AMI, stroke, anemia, atrial fibrillation (AF), congestive heart failure (CHF), and low-density lipoprotein cholesterol (LDLC). The C-index was developed to assess the change in the long-term mortality prediction accuracy following the inclusion of the SII in the original clinical risk factor model. R version 4.2.2 was used to analyze the data. Statistical significance was defined at p-value <0.05.
Results
Baseline Characteristics
This study consisted of 31,084 participants with NGR, 23,914 with pre-DM, and 29,647 with DM (weighted prevalence 35.0%). The entire population was classified into three groups based on the SII tertiles: SII-L (≤443.5), SII-M (443.5 to ≤772.6), SII-H (>772.6), and further into nine groups based on glucose metabolic status (NGR, Pre-DM, DM) (Table 1). Patients with higher SII were older, less frequently female, and had a higher prevalence of concomitant diseases, including AMI, HT, CHF, CKD, stroke, and anemia. The pre-DM proportion was lower in patients with higher SII, whereas the proportion of patients undergoing percutaneous coronary intervention (PCI) and drug metal stent (DES) increased with higher SII. Individuals with higher SII levels also had higher LDLC and HbA1C levels but lower eGFR and hemoglobin levels than those with low SII levels.
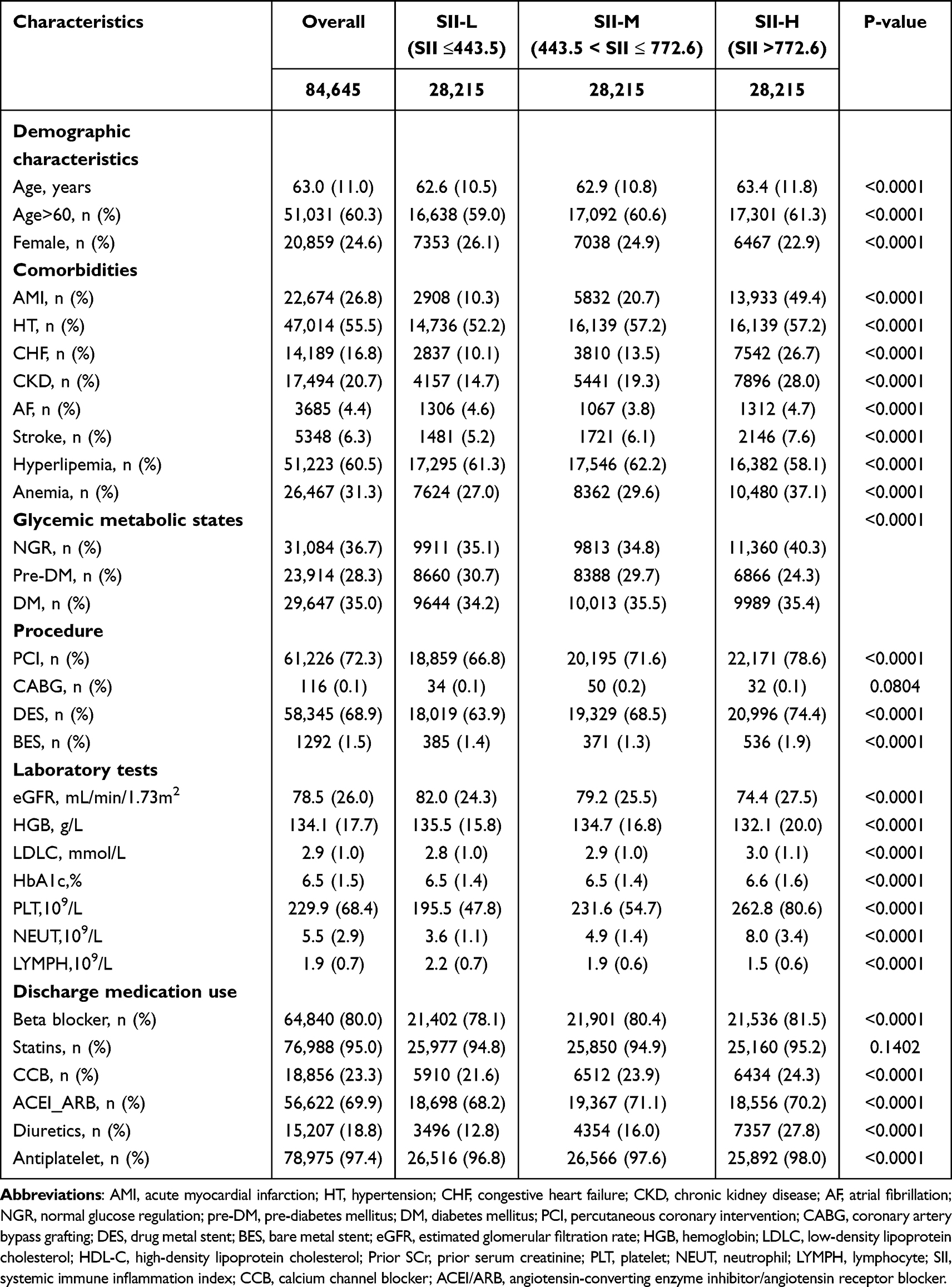 |
Table 1 Baseline Characteristics of the Study Population According to Systemic Immune Inflammation Index (SII) Levels |
Among individuals with different glucose metabolic states, those with DM exhibited significantly higher rates of all-cause and cardiovascular mortality than those in the NGR group (Table 2). Moreover, in our overall study population, the proportion of patients with a higher SII was significantly higher than that in the SII-L group for all-cause and cause-specific mortality (Table 3).
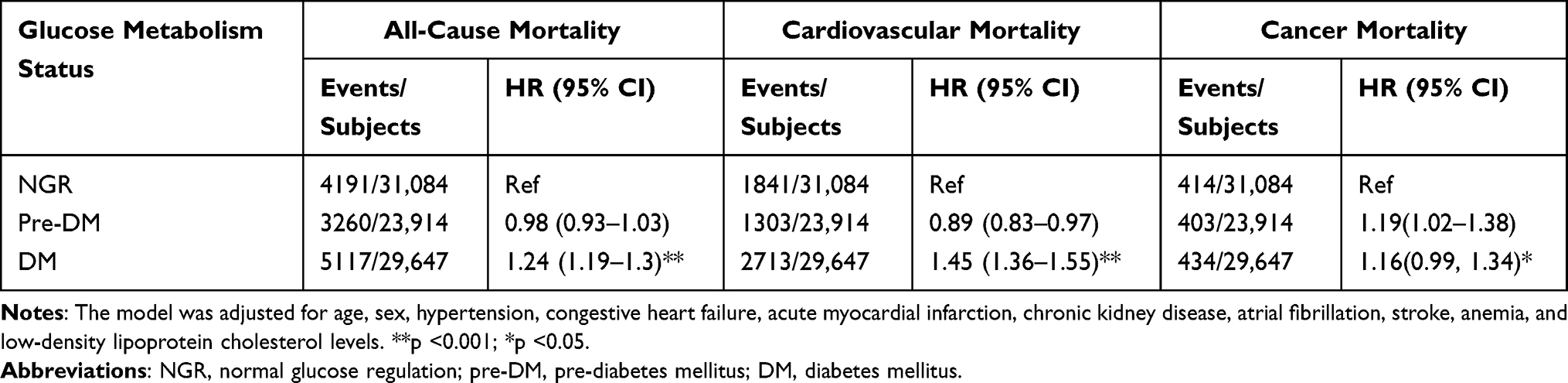 |
Table 2 Clinical Outcomes in Different Glucose Metabolism Status of the Study Participants |
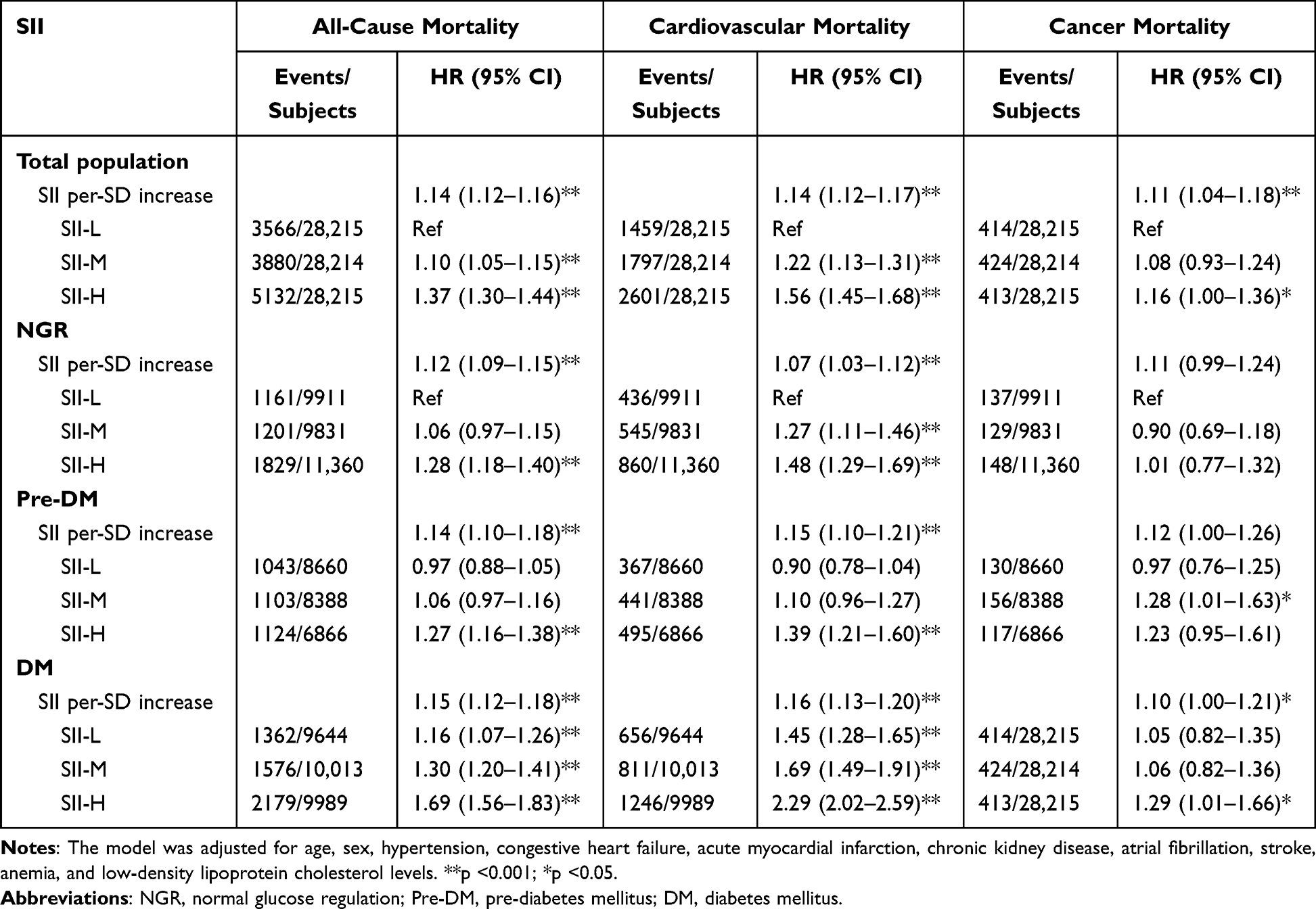 |
Table 3 SII Levels in Relation to All-Cause, Cardiovascular and Cancer Mortality in Patients with Different Glucose Metabolism Status |
Glucose Metabolism Status, SII Levels and Clinical Outcomes
During the 4.47-year median follow-up period, 12,578 (14.9%) participants died (5857 (6.9%) had cardiovascular causes, 1251 (1.5%) had cancer). Kaplan–Meier curves for all-cause mortality showed that patients with DM displayed the highest cumulative event rate among the three groups (p < 0.001). Patients with SII-H were most likely to have all-cause mortality events (p < 0.001), and the SII-H group also had a significantly higher risk of all-cause mortality than the reference group (NGR plus SII-L) across all glucose metabolism statuses. Additionally, the DM + SII-L, pre-DM + SII-M, and NGR + SII-H groups had significantly higher cumulative event rates than the reference group (NGR + SII-L) (Figure 2). Cardiovascular mortality showed a consistent trend (Figure 3), whereas cancer mortality did not differ significantly (Supplementary Figure 1). Furthermore, analysis using restricted cubic splines highlighted a non-linear association between all-cause, cardiovascular, and cancer mortality (all non-linear p<0.05) and SII levels; as the SII levels increased, the risk of mortality was significantly elevated, particularly at relatively higher levels (Figure 4).
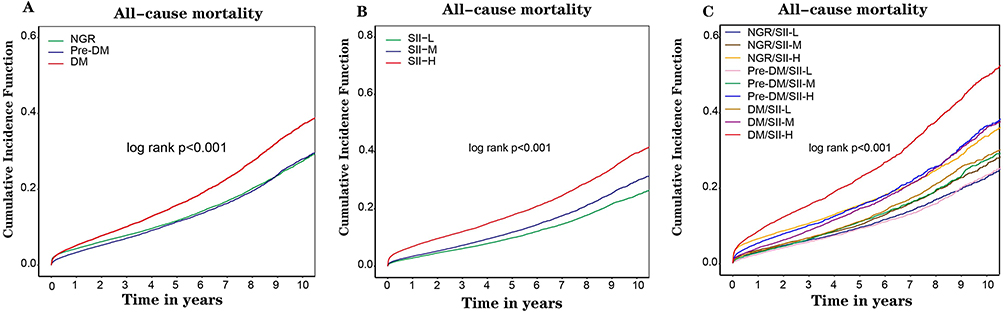 |
Figure 2 Kaplan–Meier analysis of all-cause mortality according to (A) different glucose metabolism status; (B) different SII levels; (C) both status of SII levels and glucose metabolism. |
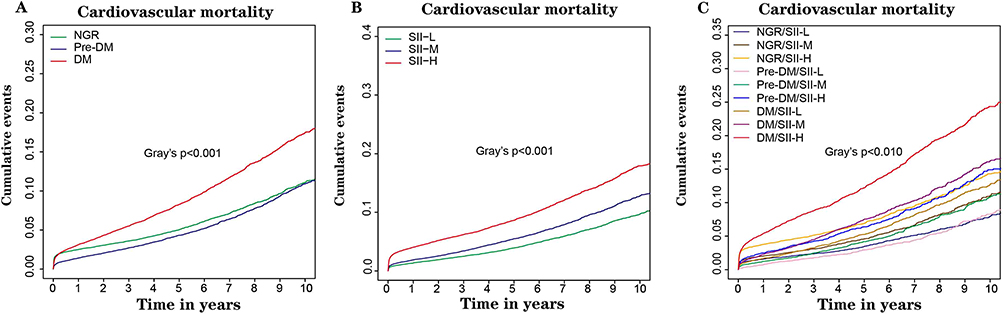 |
Figure 3 Cumulative incidence function (CIF) curves of cardiovascular mortality according to (A) different glucose metabolism status; (B) different SII levels; (C) both status of SII levels and glucose metabolism. |
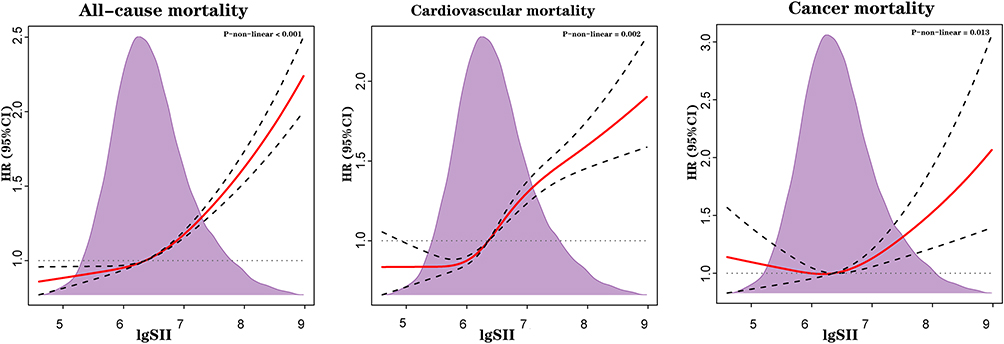 |
Figure 4 Hazard ratios for the all-cause, cardiovascular, and cancer mortality based on restricted cubic spine function for lgSII. |
As depicted in Table 2, patients with DM had 1.24-fold (95% CI 1.19–1.30), 1.45-fold (95% CI 1.36–1.55), and 1.16-fold (95% CI 1.01–1.34) the risk of all-cause, cardiovascular and cancer mortality, respectively, compared to NGR group. However, no significant difference in mortality risk was observed for individuals with pre-DM. Furthermore, the multivariable cox regression analysis showed that SII-H was associated with 37%, 56% and 16% increased risk of all-cause, cardiovascular and cancer mortality, respectively, and these risks significantly increased with the SII tertiles across the NGR, pre-DM, and DM groups. Moreover, for patients with DM, per 1-SD change in SII was associated with 1.15-fold (95% CI 1.12–1.18), 1.16-fold (95% CI 1.13–1.20), and 1.10-fold (95% CI 1.00–1.21) highest risks of all-cause, cardiovascular, and cancer mortality, respectively. Additionally, when considering both glucose metabolism and SII levels, multivariate cox regression studies showed that compared to the reference group (NGR/SII-L), the SII-H group with DM had 1.69-fold (95% CI 1.56–1.83), 2.29-fold (95% CI 2.02–2.59) and 1.29-fold (95% CI 1.01–1.66) highest risk of all-cause, cardiovascular and cancer mortality (Table 3).
Clinical Outcome Risk Prediction in Different Glucose Metabolism Groups
Finally, we assessed the predictive impact of the SII on the risk of all-cause, cardiovascular, and cancer mortality across different glucose metabolism statuses. The addition of the SII to the traditional risk model (including age, sex, CKD, HT, AMI, CHF, AF, stroke, anemia, and LDLC) significantly improved the C-index of all-cause and cardiovascular mortality in patients with NGR, pre-DM, and DM. The C-index values of cancer mortality significantly improved the predictive power for NGR but not for pre-DM and DM patients. All values were significantly higher than neutrophil to lymphocyte ratio (NLR) (Table 4).
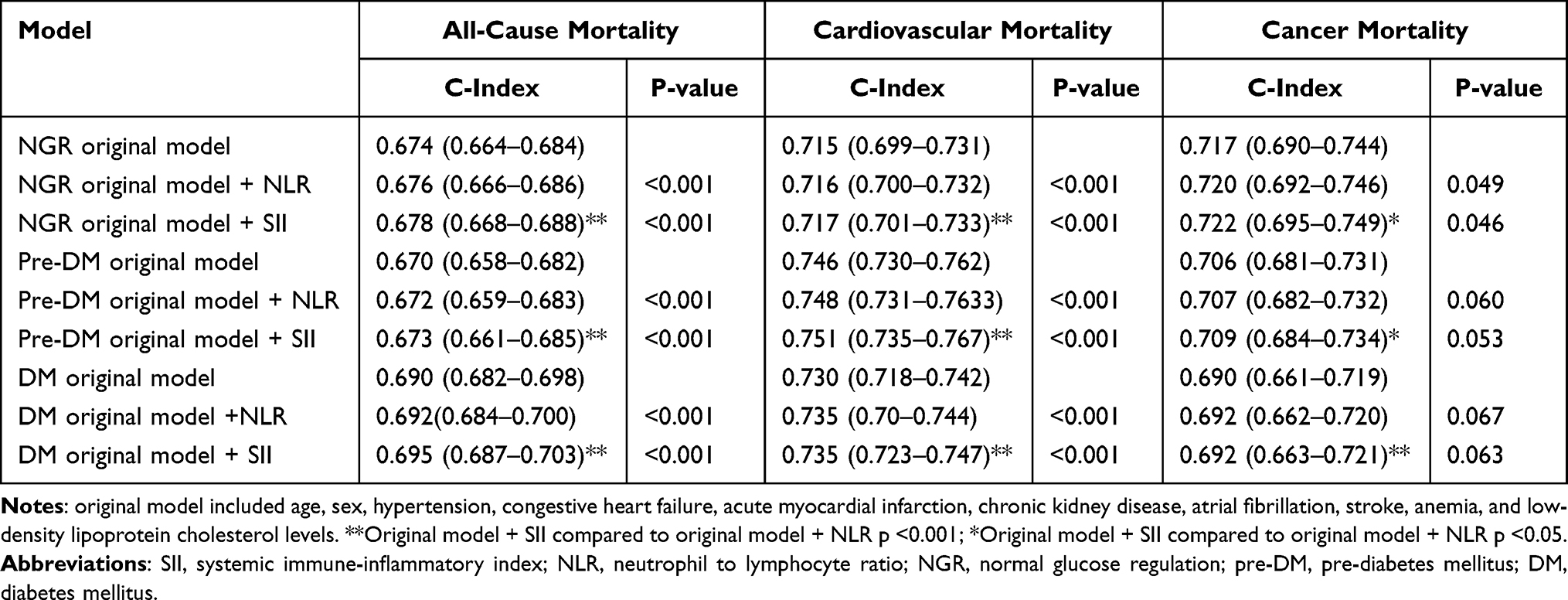 |
Table 4 C-Index of SII for Predicting Mortality in Subjects with Different Glucose Metabolism Status |
Discussion
This was a real-world, large-scale, observational cohort study that explored the correlation between SII levels and mortality in patients with CAD across different glucose metabolism statuses. The major results of this research are as follows. First, the SII was an independent risk factor for all-cause and cardiovascular mortality in patients with CAD during a median follow-up of 4.47 years. Second, when grouped according to glucose metabolism status, patients with DM were found to have a higher risk of all-cause and cardiovascular mortality compared to those in the NGR group. Interestingly, when patients were stratified according to both glucose metabolism status and SII levels, elevated blood glucose levels amplified the association between SII levels and the risk of all-cause, cardiovascular, and cancer mortality in patients with CAD. The SII-H group showed 1.69-fold, 2.29-fold, and 1.29-fold increases in the risk of all-cause, cardiovascular, and cancer mortality in DM, respectively. Adding the SII to traditional risk models improved the risk prediction for all-cause and cardiovascular mortality in the NGR, pre-DM, and DM groups, as well as the risk prediction for cancer mortality in the NGR group.
Previous studies have highlighted the significance of immune and inflammatory factors in the development and progression of CAD.21 SII has emerged as a novel indicator of immune inflammation in various diseases.22–24 Rinde et al have reported that patients with CAD have an elevated risk of developing cancer, probably due to shared risk factors like inflammation.25 Additionally, there is emerging evidence that tumors themselves can induce a pro-inflammatory state and that there is a positive correlation between SII and adverse outcomes across various types of cancer.26 Notably, the SII has demonstrated superior predictive accuracy for CAD development and progression compared to other inflammatory markers such as NLR, PLR, and C-reactive protein (CRP).14,27 Previous research has found that a high SII elevates the risk of major cardiovascular events by 1.4- to 2-fold in patients with CAD after coronary intervention, as well as short-term poor prognosis in patients with acute ischemic stroke and has better predictive efficacy than traditional risk factor.15 In our study, participants with the highest tertile of SII (≥772.6) typically had neutropenia, lymphopenia, and thrombocytosis, suggesting a concurrent presence of non-specific inflammation, and compromised adaptive immune response.28 The connection between the SII and CAD becomes clearer when considering the roles of the three distinct cell types. This highlights the significance of platelet-leukocyte interactions at atherosclerotic plaque sites in CAD. This understanding could potentially shed light on the inflammatory processes occurring within vessel walls, which are commonly linked to poor prognosis.29 More importantly, the SII is more accessible as an indicator in both inpatient and outpatient scenarios than other inflammatory biomarkers like CRP.30 In this study, we conducted a comprehensive analysis by screening a population with CAD undergoing angiography at five tertiary hospitals in China. The findings fully elucidate the correlation between the SII and all-cause mortality as well as cardiovascular and cancer mortality in patients with CAD. Our study further strengthens the notion that SII is independently correlated with poor clinical outcomes in patients with CAD, providing a more comprehensive understanding of its prognostic significance.
Globally, pre-DM will affect roughly 470 million patients worldwide by 2030, which is considered a primary risk factor in the Framingham Study.25 It affects approximately 50% of patients with CAD and 25% of these patients have impaired glucose regulation.26,27 CAD is a common comorbidity in patients with DM and a leading cause of death in this population.31 Both diabetes and pre-diabetes are associated with worse outcomes in patients with CAD. A potential link between immune inflammation levels and the disruption of glucose metabolism, contributing to the development of pre-DM or DM is suggested.32,33 In type 2 diabetes, the levels of inflammatory markers such as plasminogen activator inhibitor-1, tumor necrosis factor (TNF)-α, and CRP play a significant role in increasing insulin resistance and may lead to the loss of insulin-secreting function in pancreatic islet cells,34,35 in turn resulting in higher blood glucose levels. The presence of inflammatory markers in type 2 diabetes may contribute to the progression of insulin resistance and disrupt glucose regulation in the body. Hyperglycemia causes increased hematopoiesis and ROS-producing neutrophils, which leads to the development of atherosclerosis during pre-DM.36 Moreover, extracellular vesicles in pre-diabetic patients carry specific species of miRNAs that promote atherosclerosis through hematopoiesis and inflammation.37 Mojiminiyi et al found higher concentrations of inflammatory markers in DM patients with CAD than in age- and sex-matched subjects without CAD, suggesting that inflammatory markers are strong discriminators for detecting CAD in DM patients.38 Furthermore, inflammatory markers (eg, CRP, WBC, FAR, and FIB) are also predictors of mortality from CAD in subjects with DM.39–42
A combined assessment of immune-inflammatory markers may help in the risk stratification of patients with CAD and DM.43,44 CRP, FAR, and FIB have all been found to be correlated with the prognosis of patients with CAD and DM.41,42,45 Higher NLR in type 2 DM predicts a worse prognosis in patients undergoing PCI.46 SII provides more clinical information than NLR and PLR, and studying the combined effects of SII and different levels of glucose metabolism may offer new insights into the assessment of cardiovascular and metabolic risks. However, there are no studies on the combined effects of the SII and glucose metabolism status on mortality risk in patients with CAD. To the best of our knowledge, this is the first study to demonstrate a significant association between elevated SII levels and an increased risk of all-cause, cardiovascular, and cancer mortality in patients with CAD undergoing CAG with DM and pre-DM status. In this study, we focused on the prognosis of CAD patients receiving CAG at different SII levels and also examined the combined effect of different SII levels in conjunction with pre-DM or DM status on all-cause, cardiovascular, and cancer mortality outcomes. As a primary novel discovery in our study, among individuals with pre-DM and higher SII, the risks of all-cause and cardiovascular mortality were found to be 1.27-fold and 1.39-fold higher, respectively. Moreover, individuals with DM and high SII levels had 1.69-fold and 2.29-fold higher risks of all-cause and cardiovascular mortality, respectively. These findings highlight the significant association between elevated SII levels and heightened risks of mortality across different causes, underscoring the potential of the SII as a valuable prognostic indicator in patients with both pre-DM and DM. Notably, DM patients with high SII levels exhibited worse prognosis than those with high SII levels alone, highlighting the clinical significance of SII assessment in patients with impaired glucose metabolism. However, when exploring the association between SII and cancer mortality in patients with CAD, we found significantly higher cancer mortality in the SII-H population with CAD, and its predictive value needs to be further explored in future studies. Upon stratification by different glucose metabolism statuses, elevated SII was associated with significantly higher cancer mortality in DM patients, but not in the NGR and pre-DM populations, suggesting a possible role of immune inflammation as a contributor to cancer mortality in DM populations, which is in line with a previous study.47 Furthermore, by adding SII to the conventional risk model under different glucose metabolism statuses, the efficiency of predicting poor clinical outcomes in patients with CAD improved, with the DM group having the highest predictive efficacy.
Study Limitations
This study has several limitations. First, being a retrospective study, it was not possible to establish a causal relationship between the variables under investigation. Second, we failed to exclude subjects with systemic inflammatory disorders and recent glucocorticosteroid therapy, which might obscure or attenuate the true relationship between the SII and outcomes. This study included only Chinese patients with CAD. Therefore, the generalizability of these findings to a broader population remains unclear. Third, we measured the SII only at baseline, and the potential clinical relevance of SII levels during the follow-up period remains unknown. Additionally, given the relatively extended duration of patient recruitment, we did not consider the potential impact of seasonal fluctuations on the blood cell ratios. Fourth, being an observational study, potential confounding factors may not have been fully accounted for. Further research is required to validate the results obtained in this study.
Conclusion
In conclusion, elevated SII is an independent risk factor for all-cause and cardiovascular mortality. Specifically, patients with DM and higher SII have a significantly increased risk of all-cause and cause-specific mortality, suggesting that SII can serve as a more accurate tool for stratifying glucose metabolism in patients with CAD.
Abbreviations
CAD, Coronary artery disease; DM, Diabetes mellitus; Pre‑DM, Pre-diabetes mellitus; NGR, Normal glucose regulation; SII, Systemic immune inflammation index; CAG, coronary angiography; AMI, acute myocardial infarction; HT, hypertension; CHF, congestive heart failure; CKD, chronic kidney disease; AF, atrial fibrillation; PCI, percutaneous coronary intervention; CABG, Coronary artery bypass grafting; DES, drug metal stent; BES, Bare metal stent; eGFR, estimated glomerular filtration rate; HGB, hemoglobin; LDLC, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; Prior SCr, Prior serum creatinine; PLT, platelet; NEUT, neutrophil; LYMPH, lymphocyte; SII, systemic immune inflammation index; CCB, calcium channel blocker; ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker.
Data Sharing Statement
Data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Guangdong Provincial People’s Hospital (No.GDREC2019-555H-2). All traceable personal identifiers were removed from the analytical dataset to protect patient privacy. All participating sites received approval from their respective institutional review boards and ethics committees. Our database is not open to the public to protect the privacy of the participants. Because our research included retrospective cases, there was no additional intervention, information on all patients was desensitized, and no informed consent was required. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We would like to thank Editage for English language editing.
Author Contributions
All authors have made significant contributions to the reported work, including contributions to the conception, study design, data acquisition, analysis, interpretation, and execution or in all these aspects. They have been involved in drafting, revising, and critically reviewing the manuscript. All authors have provided their final approval for the version to be published; have reached an agreement on the journal to which the article has been submitted; and have committed to being accountable for all aspects of the work.
Funding
This research was funded and supported by the Guangdong Provincial Science and Technology Project (2020B1111170011), Guangdong Provincial Science and Technology Project (KJ022021049), and National Science Foundation for Young Scientists of China (grant no.82070360). Key Laboratory of Emergency and Trauma, Ministry of Education (Hainan Medical University) (grant no. KLET-202116). NSFC Incubation Project of Guangdong Provincial People’s Hospital (KY0120220041). The funders had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Roth GA, Forouzanfar MH, Moran AE, et al. Demographic and epidemiologic drivers of global cardiovascular mortality. N Engl J Med. 2015;372(14):1333–1341. doi:10.1056/NEJMoa1406656
2. Collaborators GCoD. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
3. Collaborators GDaIIaP. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
4. Ding D, Qiu J, Li X, et al. Hyperglycemia and mortality among patients with coronary artery disease. Diabetes Care. 2014;37(2):546–554. doi:10.2337/dc13-1387
5. Sarwar N, Gao P; Emerging Risk Factors C. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–2222. doi:10.1016/S0140-6736(10)60484-9
6. Cai X, Zhang Y, Li M, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297. doi:10.1136/bmj.m2297
7. Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953. doi:10.1136/bmj.i5953
8. American Diabetes Association Professional Practice C. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–S38. doi:10.2337/dc22-S002
9. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323. doi:10.1093/eurheartj/ehz486
10. Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2022;65(12):1925–1966. doi:10.1007/s00125-022-05787-2
11. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. doi:10.1056/NEJMra043430
12. Fioranelli M, Bottaccioli AG, Bottaccioli F, Bianchi M, Rovesti M, Roccia MG. Stress and inflammation in coronary artery disease: a review psychoneuroendocrineimmunology-based. Front Immunol. 2018;9:2031. doi:10.3389/fimmu.2018.02031
13. Odegaard AO, Jacobs DR Jr, Sanchez OA, Goff DC Jr, Reiner AP, Gross MD. Oxidative stress, inflammation, endothelial dysfunction and incidence of type 2 diabetes. Cardiovasc Diabetol. 2016;15(1):51. doi:10.1186/s12933-016-0369-6
14. Liu Y, Ye T, Chen L, et al. Systemic immune-inflammation index predicts the severity of coronary stenosis in patients with coronary heart disease. Coron Artery Dis. 2021;32(8):715–720. doi:10.1097/MCA.0000000000001037
15. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
16. Candemir M, Kiziltunc E, Nurkoc S, Sahinarslan A. Relationship between systemic immune-inflammation index (SII) and the severity of stable coronary artery disease. Angiology. 2021;72(6):575–581. doi:10.1177/0003319720987743
17. Saylik F, Akbulut T. Systemic immune-inflammation index predicts major cardiovascular adverse events in patients with ST-segment elevated myocardial infarction. Arq Bras Cardiol. 2022;119(1):14–22. doi:10.36660/abc.20210412
18. Xu M, Chen R, Liu L, et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: the Dongfeng-Tongji cohort study. Atherosclerosis. 2021;323:20–29. doi:10.1016/j.atherosclerosis.2021.02.012
19. Aguiar-Souto P, Ferrante G, Del Furia F, Barlis P, Khurana R, Di Mario C. Frequency and predictors of contrast-induced nephropathy after angioplasty for chronic total occlusions. Int J Cardiol. 2010;139(1):68–74. doi:10.1016/j.ijcard.2008.10.006
20. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D; Modification of Diet in Renal Disease Study Group. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999;130(6):461–470. doi:10.7326/0003-4819-130-6-199903160-00002
21. Agrawal H, Choy HK, Liu J, Auyoung M, Albert MA. Coronary artery disease. Arterioscler Thromb Vasc Biol. 2020;40(7):e185–e192. doi:10.1161/ATVBAHA.120.313608
22. Lai W, Xie Y, Zhao X, et al. Elevated systemic immune inflammation level increases the risk of total and cause-specific mortality among patients with chronic kidney disease: a large multi-center longitudinal study. Inflamm Res. 2023;72(1):149–158. doi:10.1007/s00011-022-01659-y
23. Lai W, Zhao X, Huang Z, et al. Elevation of preprocedural systemic immune inflammation level increases the risk of contrast-associated acute kidney injury following coronary angiography: a Multicenter Cohort Study. J Inflamm Res. 2022;15:2959–2969. doi:10.2147/JIR.S364915
24. Zhou YX, Li WC, Xia SH, et al. Predictive value of the systemic immune inflammation index for adverse outcomes in patients with acute ischemic stroke. Front Neurol. 2022;13:836595. doi:10.3389/fneur.2022.836595
25. Rinde LB, Småbrekke B, Hald EM, et al. Myocardial infarction and future risk of cancer in the general population-The Tromsø Study. Eur J Epidemiol. 2017;32(3):193–201. doi:10.1007/s10654-017-0231-5
26. Nøst TH, Alcala K, Urbarova I, et al. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol. 2021;36(8):841–848. doi:10.1007/s10654-021-00752-6
27. Kiorpes AL, Clayton MK. Moment analysis of multibreath nitrogen washout in healthy female goats and calves. Am J Vet Res. 1988;49(4):543–547.
28. Li J, Cao D, Huang Y, et al. The prognostic and clinicopathological significance of systemic immune-inflammation index in bladder cancer. Front Immunol. 2022;13:865643. doi:10.3389/fimmu.2022.865643
29. May AE, Langer H, Seizer P, Bigalke B, Lindemann S, Gawaz M. Platelet-leukocyte interactions in inflammation and atherothrombosis. Semin Thromb Hemost. 2007;33(2):123–127. doi:10.1055/s-2007-969023
30. Shah AD, Denaxas S, Nicholas O, Hingorani AD, Hemingway H. Neutrophil counts and initial presentation of 12 cardiovascular diseases: a CALIBER Cohort Study. J Am Coll Cardiol. 2017;69(9):1160–1169. doi:10.1016/j.jacc.2016.12.022
31. Naito R, Miyauchi K. Coronary artery disease and type 2 diabetes mellitus. Int Heart J. 2017;58(4):475–480. doi:10.1536/ihj.17-191
32. Lontchi-Yimagou E, Sobngwi E, Matsha TE, Kengne AP. Diabetes mellitus and inflammation. Curr Diab Rep. 2013;13(3):435–444. doi:10.1007/s11892-013-0375-y
33. Prasad M, Chen EW, Toh SA, Gascoigne NRJ. Autoimmune responses and inflammation in type 2 diabetes. J Leukoc Biol. 2020;107(5):739–748. doi:10.1002/JLB.3MR0220-243R
34. King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol. 2008;79(8 Suppl):1527–1534. doi:10.1902/jop.2008.080246
35. Calle MC, Fernandez ML. Inflammation and type 2 diabetes. Diabetes Metab. 2012;38(3):183–191. doi:10.1016/j.diabet.2011.11.006
36. Katakami N. Mechanism of development of atherosclerosis and cardiovascular disease in diabetes mellitus. J Atheroscler Thromb. 2018;25(1):27–39. doi:10.5551/jat.RV17014
37. Liang Y, Wang M, Wang C, Liu Y, Naruse K, Takahashi K. The mechanisms of the development of atherosclerosis in prediabetes. Int J Mol Sci. 2021;22(8). doi:10.3390/ijms22084108
38. Mojiminiyi OA, Abdella N, Moussa MA, Akanji AO, Al Mohammedi H, Zaki M. Association of C-reactive protein with coronary heart disease risk factors in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2002;58(1):37–44. doi:10.1016/S0168-8227(02)00101-8
39. Soinio M, Marniemi J, Laakso M, Lehto S, Ronnemaa T. High-sensitivity C-reactive protein and coronary heart disease mortality in patients with type 2 diabetes: a 7-year follow-up study. Diabetes Care. 2006;29(2):329–333. doi:10.2337/diacare.29.02.06.dc05-1700
40. Sabatine MS, Morrow DA, Cannon CP, et al. Relationship between baseline white blood cell count and degree of coronary artery disease and mortality in patients with acute coronary syndromes: a TACTICS-TIMI 18 (Treat Angina with Aggrastat and determine Cost of Therapy with an Invasive or Conservative Strategy- Thrombolysis in Myocardial Infarction 18 trial)substudy. J Am Coll Cardiol. 2002;40(10):1761–1768.
41. Liu SL, Wu NQ, Shi HW, et al. Fibrinogen is associated with glucose metabolism and cardiovascular outcomes in patients with coronary artery disease. Cardiovasc Diabetol. 2020;19(1):36. doi:10.1186/s12933-020-01012-9
42. Wang P, Yuan D, Zhang C, et al. High fibrinogen-to-albumin ratio with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention: 5-year findings from a large cohort. Cardiovasc Diabetol. 2022;21(1):46. doi:10.1186/s12933-022-01477-w
43. Huang X, Yang S, Zhao Q, et al. Predictive value of non-high-density lipoprotein cholesterol and neutrophil-lymphocyte ratio for coronary artery vulnerable plaques in type 2 diabetes mellitus. Front Cardiovasc Med. 2022;9:927768. doi:10.3389/fcvm.2022.927768
44. Mugabo Y, Li L, Renier G. The connection between C-reactive protein (CRP) and diabetic vasculopathy. Focus on preclinical findings. Curr Diabetes Rev. 2010;6(1):27–34. doi:10.2174/157339910790442628
45. Haffner SM. The metabolic syndrome: inflammation, diabetes mellitus, and cardiovascular disease. Am J Cardiol. 2006;97(2A):3A–11A. doi:10.1016/j.amjcard.2005.11.010
46. He J, Bian X, Song C, et al. High neutrophil to lymphocyte ratio with type 2 diabetes mellitus predicts poor prognosis in patients undergoing percutaneous coronary intervention: a large-scale cohort study. Cardiovasc Diabetol. 2022;21(1):156. doi:10.1186/s12933-022-01583-9
47. Koene RJ, Prizment AE, Blaes A, Konety SH. Shared risk factors in cardiovascular disease and cancer. Circulation. 2016;133(11):1104–1114. doi:10.1161/CIRCULATIONAHA.115.020406
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Discordance Between Neutrophil to Lymphocyte Ratio and High Sensitivity C-Reactive Protein to Predict Clinical Events in Patients with Stable Coronary Artery Disease: A Large-Scale Cohort Study
He J, Song C, Zhang R, Yuan S, Li J, Dou K
Journal of Inflammation Research 2023, 16:5439-5450
Published Date: 20 November 2023
Exploring the Correlation Between the Systemic Immune Inflammation Index (SII), Systemic Inflammatory Response Index (SIRI), and Type 2 Diabetic Retinopathy

Wang S, Pan X, Jia B, Chen S
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3827-3836
Published Date: 24 November 2023
Serum FGF23 and DPP4 Levels as Biomarkers for Coronary Artery Disease Severity in Type 2 Diabetic Patients with Coronary Heart Disease
Zhong X, Liang Z, Liao H, Zhan Y, Li G, Wu H, Li J
International Journal of General Medicine 2025, 18:1757-1764
Published Date: 28 March 2025
The Prognostic Role of Naples Prognostic Score in Patients with Coronary Artery Disease
Jiang Y, Chen Y, Lu W, Peng Y, Chen L, Lin Y
Journal of Inflammation Research 2025, 18:6999-7012
Published Date: 30 May 2025
Association Between Systemic Inflammation Response Index, Worsening of Left Ventricular Systolic Function and Prognosis in Patients with Coronary Artery Disease
Ruan H, Lu X, Lu H, Huang H, Huang Z, Tang S, Yuan Z, Jiang R, Xin J, Tang T, Liu J, Liu Y, Tan N
Journal of Inflammation Research 2026, 19:577895
Published Date: 1 May 2026