Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Association Between Serum Bicarbonate Levels and Prediabetes and Subclinical Inflammation in Young Healthy Adults: A Cross-sectional Study
Authors Omar AA ![]() , Radwani KJ, Al Thani MK, Abouzeid NH, Qabeel YE, Al Shamari M, Chivese T, Zughaier SM
, Radwani KJ, Al Thani MK, Abouzeid NH, Qabeel YE, Al Shamari M, Chivese T, Zughaier SM ![]()
Received 19 December 2022
Accepted for publication 25 March 2023
Published 4 April 2023 Volume 2023:16 Pages 969—977
DOI https://doi.org/10.2147/DMSO.S402037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Abeer A Omar, Khadija J Radwani, Maryam K Al Thani, Nadin H Abouzeid, Yousef E Qabeel, Manwa Al Shamari, Tawanda Chivese, Susu M Zughaier
College of Medicine, QU Health, Qatar University, Doha, Qatar
Correspondence: Susu M Zughaier, College of Medicine, QU Health, Qatar University, Tel +974 4403 7859, Email [email protected]
Purpose: Low bicarbonate, a hallmark of metabolic acidosis is associated with various diseases. This study investigated associations between bicarbonate levels with prediabetes and subclinical inflammation among healthy young adults in Qatar.
Patients and Methods: A cross-sectional study was carried out with 825 participants aged 18– 40 years, devoid of any known comorbidities, using data from the Qatar Biobank. For each participant, blood samples were taken for measurements of bicarbonate, prediabetes, and subclinical inflammation biomarkers. Prediabetes was defined using HbA1c between 5.7 and 6.4% and subclinical inflammation was defined using monocyte to high density lipoprotein (HDL) cholesterol ratio (MHR). Associations between bicarbonate levels and the outcomes were analyzed using multivariable linear and logistic regression and then stratified by gender.
Results: A total of 825 participants with mean age 29.2 years (5.9) of which 365 (44.2%) were males. After multivariable logistic regression, each unit increase in serum bicarbonate was associated with a 17% decreased risk of prediabetes (OR: 0.83, 95%CI: 0.70– 0.99, p=0.034), in males but no association was observed for females. Similarly, after multivariable linear regression, a unit increase in serum bicarbonate was associated with a 0.18 unit decrease in MHR (beta − 0.18, 95%CI: − 0.29, − 0.07, p=0.002), again with no association observed in females.
Conclusion: In a healthy young adult population, higher serum bicarbonate levels were inversely associated with both prediabetes and subclinical inflammation in males, but not in females.
Keywords: bicarbonate, prediabetes, subclinical inflammation, males, females, Qatar
Introduction
Prediabetes or intermediate hyperglycemia is a high-risk state for developing diabetes with annualized conversion rate of 5–10% and is linked with the simultaneous presence of insulin resistance and β-cell dysfunction that begin before the glucose changes are measurable. People with prediabetes are asymptomatic but have increased risk of both microvascular diseases such as nephropathy, retinopathy, and macrovascular disease such as cardiovascular diseases.1 Qatar currently is one of the countries with high prevalence of prediabetes and diabetes at 11.9%2 and 16.4%,3 respectively, and more research is needed to identify risk factors and preventive factors for both diabetes and prediabetes.
There is evidence that low grade metabolic acidosis maybe associated with insulin resistance and diabetes mellitus.4 Bicarbonate, produced by the stomach and the pancreas,5 serves as the main buffering system that maintains pH in the normal range between 7.35 and 7.45, and is fundamental for the optimum functioning of organs.6 Lower levels of bicarbonate are a marker of chronic low-grade metabolic acidosis and have been linked with decreased insulin sensitivity and diabetes mellitus, although findings are not conclusive.7,8 Higher levels of inflammatory biomarkers (subclinical inflammation) are associated with the development of chronic diseases and increase in mortality.9 The elevation of pro-inflammatory proteins is predictive of type 2 diabetes.10 In addition, there is growing evidence suggesting that acidosis has profound effects on the host, particularly in immune function, which may explain the inflammation observed in diabetes, renal and cardiovascular disease.11 A previous study has shown that lower bicarbonate levels were associated with higher levels of inflammatory markers (C-reactive proteins) in a healthy population.9 Apart from overt inflammation, subclinical inflammation has also been observed in people with diabetes.12 Several biomarkers such as monocyte to high density cholesterol ratio (MHR), a novel marker, ferritin, and albumin are also known to reflect subclinical inflammation.12,13 Research on the association between subclinical inflammation and bicarbonate levels remains limited.
Low grade acidosis maybe increasing in prevalence due to diets that consist of highly processed foods, which are consumed by an increasing number of people worldwide. This unvaried diet was shown to induce chronic low-grade metabolic acidosis in healthy adults.14 Studies have shown that the dietary acid load is linked with worsening insulin sensitivity and increased risk of developing type 2 diabetes.15–19
Previous research has suggested that bicarbonate has a differential effect in athletes, where male athletes respond well to bicarbonate supplements while female athletes do not show an effect.20 We hypothesized that a similar effect may be present in the association between bicarbonate and prediabetes. To our knowledge, research is scarce on the effect of bicarbonate on the risk of prediabetes and subclinical inflammation in the Middle East and North African region. Hence, this study aimed to investigate the associations between bicarbonate levels and prediabetes and subclinical inflammation among healthy young adults in Qatar followed by investigating the same associations in males and females separately. Further, we sought to investigate the associations between bicarbonate and other markers of inflammation and insulin resistance in males and females, separately.
Materials and Methods
This study is a cross-sectional study of participants, aged between 18 and 40 years without any known diseases, from the Qatar Biobank (QBB) whose data were collected between 2012 and 2017.21 For unfunded projects, the QBB gives a maximum number of 1,000 participants. A total of 874 participants were initially included but participants with comorbidities such as cardiovascular disease, diabetes (HbA1c ≥6.5), hypertension, morbid obesity (BMI >40), cancer and any kidney diseases were excluded leaving a total of 825 participants. For each participant, a questionnaire was administered, anthropometry measured, and blood samples were taken for the assessment of bicarbonate and measures of prediabetes and subclinical inflammation.
Variable Measurements
All variables used in this study were collected using Qatar Biobank established protocol.22 Data collected included sociodemographic data and past medical history, anthropometry, blood pressure and laboratory assessments of clinical markers of interest. Laboratory assessments were measured at Hamad Medical Corporation (HMC) laboratories, Department of Laboratory Medicine, and Pathology (DLMP) that holds College of American Pathologist (CAP) accreditation.
Exposure – Bicarbonate
Bicarbonate (HCO3−) levels were measured for each participant from serum in (mmol/L) having a normal range of 22–28 mmol/L.23 Bicarbonate and lipids profiles including HDL-c were measured using the microvolume automated Roche Cobas 6000 biochemical analyser.
Outcomes – Prediabetes and Subclinical Inflammation
For each participant HbA1c was measured from whole blood using latex agglutination inhibition with spectrophotometry (Siemens DCA vantage device). A normal level was defined as HbA1c <5.7 and prediabetes as HbA1c of (5.7–6.4), using the prediabetes criteria of the American Diabetes Association.24 Other markers of glycemic control assessed were fasting blood glucose and c-peptide. We also assessed insulin resistance defined using a homeostatic model of insulin resistance (HOMA-IR). The Oxford University calculator was used to calculate (HOMA-IR2)25 using C-peptide as it is more stable than insulin.26
Complete blood count and WBC differential was performed at the same laboratories using microcuvette technology using HemoCue WBC DIFF analyser. WBC differential counts included monocytes percentage. The monocyte percentage to HDL ratio (MHR) level, calculated by dividing monocyte percentage on HDL-c concentration, was used as a marker of subclinical inflammation and oxidative stress to assess the association between low levels of HCO3− and inflammation.27 Other markers of inflammation assessed were albumin, ferritin.
Statistical Analysis
Normality of variables distribution was assessed by generating histograms. For normally distributed variables, means (SD) while median (IQR) was reported for abnormally distributed variables. For categorical variables, frequency tables were used to report frequency and percentages. Box plots were used to compare bicarbonate levels in both genders. For prediabetes, we categorized HbA1c. Linear regression was used to compute unadjusted beta coefficients for the association between bicarbonate and MHR. Logistic regression was used to compute unadjusted odds ratios (OR) for the association between bicarbonate and the following categorical outcome: prediabetes by HbA1c and for insulin resistance, we categorized HOMA-IR according to its upper quartile (75th percentile), with values above 75th percentile (a cut-off of 1.89) considered as high.
Multivariable linear regression was used to compute adjusted beta coefficients for the association between bicarbonate and MHR. Multivariable logistic regression was used to compute adjusted ORs for the association between bicarbonate and prediabetes by HbA1c. In each model, we adjusted age and BMI as confounders. Age was categorized into two categories (18–29) and (30–40). BMI was further categorized into normal <25, overweight 25–29.9, and obese ≥30. Stratified analysis by gender was performed for all the outcomes to test for possible effect modification. Exact p-values were reported, and 95%CIs reported for ORs and beta coefficients. We used residual vs predictor plots to assess for homoscedasticity in linear regressions and the link test was used to check for model specification. To investigate the possible cut-off point for bicarbonate associated with prediabetes, we used the Liu method,28 which tries to find the cut-off point that corresponds to the maximum of the product of the sensitivity and specificity of a test. In Stata, this was done using the “cutpt” module. All analyses were carried out using Stata statistical software package 16 (STATA 16), (Stata Corp, College Station, TX, USA).
Results
Baseline Characteristics
This cohort comprised of 825 young Qatari participants. Male participants were 365 (44.2%) whereas female participants were 460 (55.8%). In male participants, the mean age was 29.8 years, the mean bicarbonate 26.7 mmol/L, mean HbA1c was 5.2 and mean MHR was 6.7. In female participants the mean age was 28.8, mean bicarbonate was 25.2 mmol/L, mean HbA1c was 5.2 and mean MHR was 4.7 (Table 1). Males had significantly higher mean age, BMI, MHR, bicarbonate, and HOMA-IR, compared to females (Table 1, Figure 1).
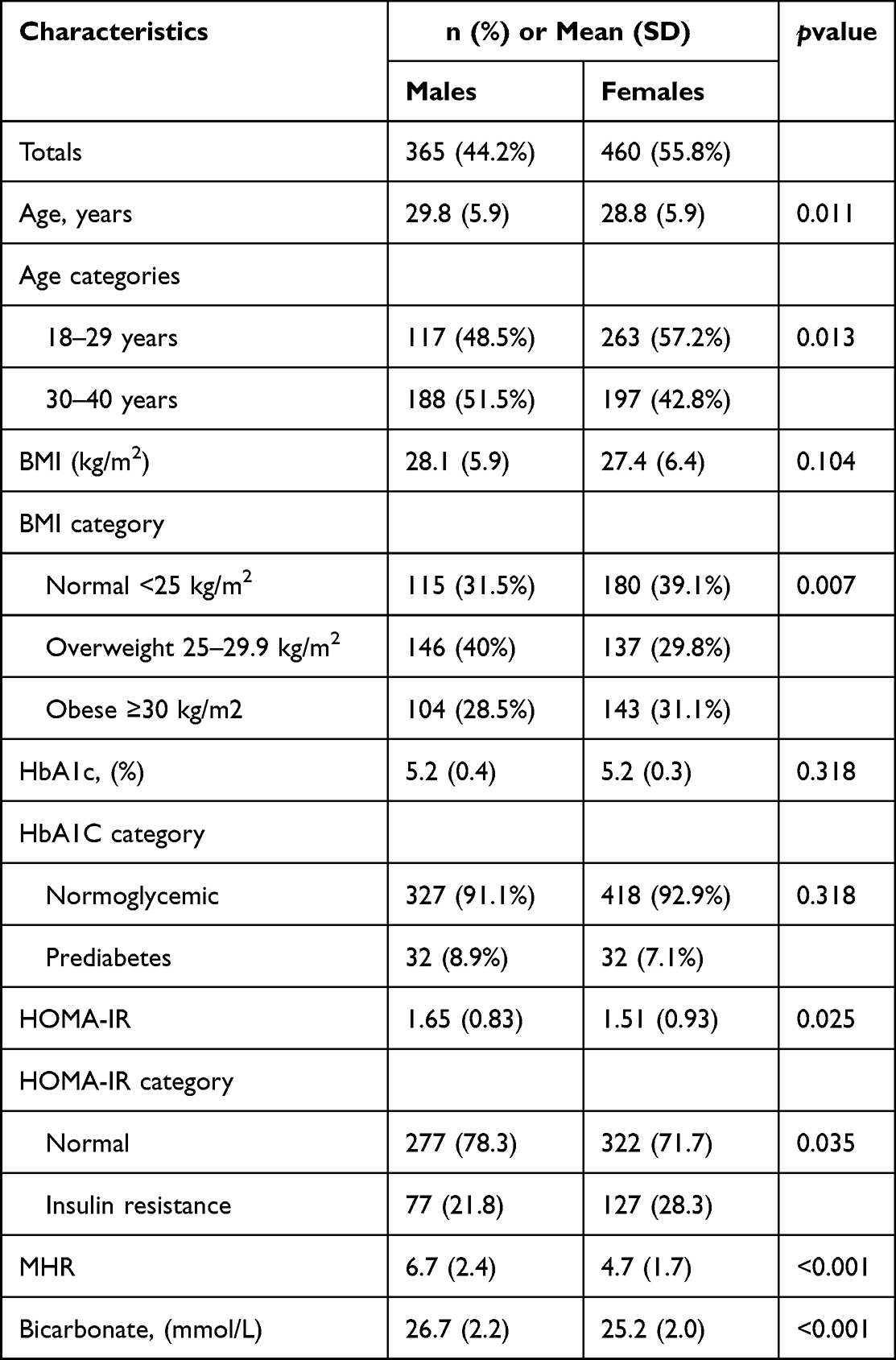 |
Table 1 Baseline Characteristics of Included Participants |
 |
Figure 1 Box plot of serum bicarbonate levels (mmol/L) (females n=460, males n=365). |
Associations between Bicarbonate Levels and Prediabetes
The proportion of participants with prediabetes was slightly higher in males (8.9%) in males than in females (7.1%) (Table 1). After multivariable logistic regression, bicarbonate was associated with a 17% decreased risk of prediabetes in males (OR: 0.83, 95%CI: 0.70, 0.99, p=0.034). There was no significant association between bicarbonate and prediabetes in females (Figure 2). The same pattern (ie the inverse association between bicarbonate in males and no effect in females) was observed when the analysis was repeated in both genders separately in the age groups of 18–29 years and 30–40 years (Supplementary Tables 1–4). Further analysis showed that the cut-off point for bicarbonate for increased odds of prediabetes was 26.75 in males. This cut-off point had a sensitivity of 54%, a specificity of 63% and an area under the receiver operating curve of 0.59, indicating that bicarbonate alone is insufficient in diagnosing or screening for prediabetes. The cut-off was not investigated in females as there were no clinical and statistically significant associations between bicarbonate and prediabetes in females.
 |
Figure 2 Forest plot showing association between bicarbonate and prediabetes by gender stratification. Adjusted for age and BMI. |
Associations between Bicarbonate Levels and Subclinical Inflammation
After multivariable linear regression, there was an inverse association between bicarbonate and MHR in both genders (beta −0.12, 95%CI: −0.18, −0.05, p=0.001). However, after stratification, the association was stronger in males, where a unit mmol/L increase in bicarbonate was significantly associated with 0.18 decrease in MHR (beta −0.18, 95%CI −0.29, −0.07, p=002) but no significant association was observed in females (Figure 3). In the age groups, there was no association between bicarbonate in both males and females aged 18–29 years (Supplementary Tables 5 and 6), but bicarbonate appeared to be protective against subclinical inflammation (higher MHR) in both males and females aged 30–40 years, again with a stronger effect in males (Supplementary Tables 7 and 8).
 |
Figure 3 Forest plot showing association between bicarbonate levels and subclinical inflammation marker MHR using multivariable linear regression by gender stratification. Adjusted for age and BMI. |
Associations between Bicarbonate Levels and Other Markers of Inflammation and Insulin Resistance
In secondary analysis, we observed no association between bicarbonate and ferritin in both genders (Supplementary Tables 9 and 10). However, bicarbonate showed a strong association with higher levels of albumin in males (Supplementary Table 11) and a weaker and nonstatistically significant association with an increase in albumin in females (Supplementary Table 12). A consistent pattern was also observed for HOMA-IR, with bicarbonate showing an inverse association with an increase in HOMA-IR in males but no association in females (Supplementary Tables 13 and 14). However, when HOMA-IR was categorized, there was no association with bicarbonate in both genders (Supplementary Tables 15 and 16). This was also the case with c-peptide (Supplementary Tables 17 and 18) and glucose (Supplementary Tables 19 and 20).
Discussion
In this study, we found that higher levels of serum bicarbonate were inversely associated with both prediabetes and subclinical inflammation in young males but not in young females suggesting a protective effect of higher levels of bicarbonate in males. We found that males had 17% decreased odds of developing prediabetes with every 1 mmol/L increase in bicarbonate levels. Conversely, there were no significant associations in females. Not many studies have been performed to assess the gender stratified associations of bicarbonate and prediabetes. Findings from one nested case control study4 among nurses aged 30–55 years showed that higher bicarbonate levels were associated with lower odds of getting type 2 diabetes. Women with plasma bicarbonate above the median level had lower odds of diabetes (OR: 0.76, 95%CI: 0.60–0.96).4 However, this study had not included males, and the endpoint was diabetes, different from our endpoint of prediabetes. Another difference between the two studies is that we included only healthy participants, without any known comorbidities. The mechanism by which bicarbonate exerts a protective effect in either diabetes or prediabetes is not completely understood. In the present study, it is also not clear why there is a differential effect, stronger in men and very weak in women. However, like our study, gender differences have been observed in one study before, in response to bicarbonate supplementation, where male athletes showed strong beneficial responses in several performance indicators while there were no observed benefits in women athletes.20 We also observed similar gender-stratified associations between bicarbonate and HOMA-IR but none with the categorized insulin resistance, c-peptide, and glucose. Various factors may explain why bicarbonate decreased the odds of prediabetes in males only. A possible explanation could be related to the differences in pancreatic fluid excretion, which is involved in secreting bicarbonate between the two genders. Males have greater output volume of pancreatic bicarbonate fluid 20% more than females and this is due to the body size where males have greater body size compared to females not necessarily that there is a gender difference in the pancreas itself.29 Therefore, the higher levels of bicarbonate could be more protective in males compared to females since lower bicarbonate a marker of chronic low grade metabolic acidosis is independently associated with decreased insulin sensitivity and higher levels of inflammatory markers.7,9
We found an (inverse) association between higher bicarbonate levels and two markers of subclinical inflammation, again with the association being observed in males but not in females. In males, a decrease in 0.18 in MHR was observed for every 1 mmol/L increase in bicarbonate, and similar associations observed for albumin with a beta of −0.26 in males. For females, both MHR and albumin showed diminished nonsignificant associations with bicarbonate. We found no studies which investigated the association between bicarbonate and these subclinical inflammation markers, especially MHR, due to its novel nature. Again, it is not clear why bicarbonate had a stronger and protective effect in males than in females in our study. The previously mentioned research suggested that males may respond more, physiologically, to bicarbonate supplementation, compared to females, and this may explain some of our observed findings for subclinical inflammation too.20 This could possibly stem from physiological differences like females have smaller type II muscle fibers compared to men which rely mainly on glycolytic energy system. Males have shown to have greater glycolytic capacity.20 The glycolytic state is linked to increase lactate and hydrogen ions through anaerobic respiration which results in decreased pH. Bicarbonate then increases and acts as a buffer through the process called bicarbonate loading.30 Therefore, in this study comprising of young healthy adults, males could be responding more to an alkaline diet or supplements than females which may explain why males had decreased odds of prediabetes and decreased risk of subclinical inflammation. Alternatively, estradiol, although not well proven, is believed to stimulate duodenal bicarbonate secretion through intracellular calcium mobilization and stimulation of Cl−/HCO3− anion exchange.31 One study showed that estrogen receptors are expressed in the duodenal mucosa which stimulates duodenal bicarbonate secretion explaining the lower prevalence of duodenal ulcers in premenopausal women compared to men.32
Bicarbonate has generally been disregarded as therapeutic use in treating critically ill people with severe metabolic acidosis. According to a systemic review, limited benefits were seen in using bicarbonate as therapy to severe acidosis in ICU, but may offer effective outcomes in carefully selected populations.33
Whether bicarbonate supplementation reduces the risk of prediabetes or insulin sensitivity is still not clear, as randomized controlled trials have yielded conflicting results. One study showed bicarbonate supplementation improves insulin resistance (HOMA index) in individuals with chronic kidney disease and type 2 diabetes34 while a three-month randomized control trial performed in nondiabetic older adults 50 years and above, who used bicarbonate supplementation to improve bone function, showed no improvement in insulin sensitivity or glucose control.35 These findings suggest a need for more research.
A strength of this study is it provides tentative findings on a research area that is under researched, and that we have carried out a robust and exhaustive analysis in a sample of healthy adults. This study has several limitations. This study was a cross-sectional study thus, no temporality between bicarbonate and various markers could be inferred and hence no inferences about causality can be made from the study. Data on possible confounders such as diets or supplements of the participants were not available. There were no data for arterial pH, venous pH, and urinary pH, which limited the ability to categorize the acidity status of participants. However, since this was a healthy cohort devoid of any known comorbidities, it was unlikely to find participants with clinical metabolic acidosis.
Conclusion
In a healthy young population, higher serum bicarbonate levels are inversely associated with both prediabetes and subclinical inflammation in males but not in females. Our findings could suggest a possible protective effect of higher serum bicarbonate levels against metabolic diseases such as prediabetes and subclinical inflammation in young men but not in young women. Further research is required to explore these findings in other population studies, to explain the mechanism by which this occurs, and to explore the effect of increased alkaline diet or oral supplemental bicarbonate on inflammatory biomarkers, prediabetes, and type 2 diabetes mellitus.
Data Sharing Statement
The data used in the current study are obtained under Material Transfer Agreement from Qatar Biobank repository in Doha, Qatar (https://www.qatarbiobank.org.qa/) therefore are not publicly available.
Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Qatar Biobank (QBB IRB (Ref- RES-ACC-0200-0121). At the QBB, all participants provided informed, written informed consent before participation.
Consent to Publication
Written informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors thank Qatar Biobank (https://www.qatarbiobank.org.qa/) and the participants of the QBB, for providing the cohort data for this study.
Disclosure
The authors report no conflict of interest in this work.
References
1. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. doi:10.1016/S0140-6736(12)60283-9
2. Al-Thani MH, Al-Thani AAM, Cheema S, et al. Prevalence and determinants of metabolic syndrome in Qatar: results from a national health survey. BMJ Open. 2016;6(9):e009514. doi:10.1136/bmjopen-2015-009514
3. Awad SF, O’Flaherty M, El-Nahas KG, et al. Preventing type 2 diabetes mellitus in Qatar by reducing obesity, smoking, and physical inactivity: mathematical modeling analyses. Popul Health Metrics. 2019;17:20. doi:10.1186/s12963-019-0200-1
4. Mandel EI, Curhan GC, Hu FB, Taylor EN. Plasma bicarbonate and risk of type 2 diabetes mellitus. Cmaj. 2012;184(13):E719–25. doi:10.1503/cmaj.120438
5. McGuckin E, Cade JE, Hanison J. The pancreas. Anaesth Intensive Care Med. 2020;21(11):604–610. doi:10.1016/j.mpaic.2020.08.005
6. Burger MK, Schaller DJ. Physiology, Acidosis, Metabolic. In: StatPearls. StatPearls Publishing StatPearls Publishing LLC; 2019.
7. Farwell WR, Taylor EN. Serum bicarbonate, anion gap and insulin resistance in the national health and nutrition examination survey. Diabet Med. 2008;25(7):798–804. doi:10.1111/j.1464-5491.2008.02471.x
8. Li J, Ni J, Wu Y, et al. Sex differences in the prevalence, awareness, treatment, and control of diabetes mellitus among adults aged 45 years and older in rural areas of northern china: a cross-sectional, population-based study. Front Endocrinol. 2019;10:147. doi:10.3389/fendo.2019.00147
9. Farwell WR, Taylor EN. Serum anion gap, bicarbonate and biomarkers of inflammation in healthy individuals in a national survey. Can Med Assoc J. 2010;182(2):137–141. doi:10.1503/cmaj.090329
10. Festa A, Hanley AJ, Tracy RP, D’Agostino R
11. de Nadai TR, de Nadai MN, Albuquerque AAS, de Carvalho MTM, Celotto AC, Evora PRB. Metabolic acidosis treatment as part of a strategy to curb inflammation. Int J Inflam. 2013;2013:601424. doi:10.1155/2013/601424
12. Chang DC, Xu X, Ferrante AW
13. Sciacqua AA-O, Ventura E, Tripepi G, et al. Ferritin modifies the relationship between inflammation and arterial stiffness in hypertensive patients with different glucose tolerance. Cardiovasc Diabetol. 2020;19:1. doi:10.1186/s12933-020-01102-8
14. Rylander R, Remer T, Berkemeyer S, Vormann J. Acid-base status affects renal magnesium losses in healthy, elderly persons. J Nutr. 2006;136(9):2374–2377. doi:10.1093/jn/136.9.2374
15. Xu H, Jia T, Huang X, et al. Dietary acid load, insulin sensitivity and risk of type 2 diabetes in community-dwelling older men. Diabetologia. 2014;57:1561–1568. doi:10.1007/s00125-014-3275-z
16. Kiefte-de Jong JC, Li Y, Chen M, et al. Diet-dependent acid load and type 2 diabetes: pooled results from three prospective cohort studies. Diabetologia. 2017;60(2):270–279. doi:10.1007/s00125-016-4153-7
17. Fagherazzi G, Vilier A, Bonnet F, et al. Dietary acid load and risk of type 2 diabetes: the E3N-EPIC cohort study. Diabetologia. 2014;57:313–320. doi:10.1007/s00125-013-3100-0
18. Akter S, Eguchi M, Kuwahara K, et al. High dietary acid load is associated with insulin resistance: the furukawa nutrition and health study. Clin Nutr. 2016;35(2):453–459. doi:10.1016/j.clnu.2015.03.008
19. Schulze MB, Hoffmann K, Manson JE, et al. Dietary pattern, inflammation, and incidence of type 2 diabetes in women. Am J Clin Nutr. 2005;82(3):675–684. doi:10.1093/ajcn/82.3.675
20. Durkalec-Michalski K, Zawieja EE, Zawieja BE, Michałowska P, Podgórski T. The gender dependent influence of sodium bicarbonate supplementation on anaerobic power and specific performance in female and male wrestlers. Sci Rep. 2020;10(1):1878. doi:10.1038/s41598-020-57590-x
21. Al Thani A, Fthenou E, Paparrodopoulos S, et al. Qatar biobank cohort study: study design and first results. Am J Epidemiol. 2019;188(8):1420–1433. doi:10.1093/aje/kwz084
22. Al Kuwari H, Al Thani A, Al Marri A, et al. The Qatar Biobank: background and methods. BMC Public Health. 2015;15:1–9. doi:10.1186/s12889-015-2522-7
23. Dhondup T, Qian Q. Electrolyte and acid-base disorders in chronic kidney disease and end-stage kidney failure. Blood Purif. 2017;43(1–3):179–188. doi:10.1159/000452725
24. de Veciana M, Major CA, Morgan MA, et al. Classification and diagnosis of diabetes: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl1):S13–s27. doi:10.2337/dc18-S002
25. Oxford Uo. HOMA2 Calculator. University of Oxford Diabetes Trials Unit. Available from: https://www.dtu.ox.ac.uk/homacalculator/.
26. Jones AG, Hattersley AT. The clinical utility of C-peptide measurement in the care of patients with diabetes. Diabet Med. 2013;30(7):803–817. doi:10.1111/dme.12159
27. Canpolat U, Çetin EH, Cetin S, et al. Association of Monocyte-to-HDL cholesterol ratio with slow coronary flow is linked to systemic inflammation. Clin Appl Thromb Hemost. 2016;22(5):476–482. doi:10.1177/1076029615594002
28. Liu X. Classification accuracy and cut point selection. Stat Med. 2012;31(23):2676–2686. doi:10.1002/sim.4509
29. Gaia E, Andriulli A, Tappero G, et al. Influence of sex and body size on pancreatic bicarbonate and enzyme output. J Clin Gastroenterol. 1984;6(5):429–433. doi:10.1097/00004836-198410000-00007
30. Calvo JL, Xu HA-O, Mon-López D, Pareja-Galeano H, Jiménez SL. Effect of sodium bicarbonate contribution on energy metabolism during exercise: a systematic review and meta-analysis. J Int Soc Sports Nutr. 2021;18(1):11. doi:10.1186/s12970-021-00410-y
31. Smith A, Contreras C, Ko KH, et al. Gender-specific protection of estrogen against gastric acid-induced duodenal injury: stimulation of duodenal mucosal bicarbonate secretion. Endocrinology. 2008;149(9):4554–4566. doi:10.1210/en.2007-1597
32. Tuo B, Wen G, Wei J, et al. Estrogen regulation of duodenal bicarbonate secretion and sex-specific protection of human duodenum. Gastroenterology. 2011;141(3):854–863. doi:10.1053/j.gastro.2011.05.044
33. Ghauri SK, Javaeed A, Mustafa KJ, Podlasek A, Khan AS. Bicarbonate therapy for critically Ill patients with metabolic acidosis: a systematic review. Cureus. 2019;11:3.
34. Bellasi A, Di Micco L, Santoro D, et al. Correction of metabolic acidosis improves insulin resistance in chronic kidney disease. BMC Nephrol. 2016;17:1. doi:10.1186/s12882-016-0372-x
35. Harris SS, Dawson-Hughes B. No effect of bicarbonate treatment on insulin sensitivity and glucose control in non-diabetic older adults. Endocrine. 2010;38:221–226. doi:10.1007/s12020-010-9377-6
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.