Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Association Between Physical Activity and Anxiety in A Rural Chinese Middle-Aged and Older Cohort
Authors Ding Z, Liu Z, Liu C ![]() , Yan Z, Yan J
, Yan Z, Yan J
Received 30 March 2026
Accepted for publication 4 June 2026
Published 10 June 2026 Volume 2026:19 613184
DOI https://doi.org/10.2147/JMDH.S613184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Zifan Ding,1,* Zhuoqi Liu,2,* Chong Liu,1 Zhaoying Yan,1 Jun Yan1
1College of Physical Education, Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China; 2Department of Gastroenterology, The Affiliated Hospital of Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Yan, College of Physical Education, Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China, Email [email protected]
Background: As China’s population ages, the burden of anxiety is increasing. Physical activity (PA) is a cost-effective lifestyle factor, but its associations with mental health differ by domain and volume.
Methods: This cross-sectional study included 4394 rural middle-aged and older adults (mean age 56.67± 8.73 years) from the Yangzhou Upper Gastrointestinal Disease Screening Cohort. PA was assessed using a questionnaire based on the International Physical Activity Questionnaire (IPAQ), and anxiety was measured with the 7-item Generalized Anxiety Disorder Scale (GAD-7). Logistic regression and restricted cubic spline (RCS) models were used to examine associations and nonlinear patterns. Sensitivity analyses assessed robustness.
Results: Domain-specific associations with anxiety were observed. After confounder adjustment, each 1-SD increase in total physical activity (TPA) and occupational physical activity (OPA) was associated with 22% higher odds of anxiety (both OR=1.22, 95% CI: 1.11– 1.34, P< 0.001). Household physical activity (HPA) showed a marginally positive association (OR=1.10, 95% CI: 1.00– 1.21, P=0.050), whereas leisure-time physical activity (LTPA) was inversely associated (OR=0.88, 95% CI: 0.80– 0.96, P=0.004). RCS analysis further revealed reverse L-shaped dose-response relationships for TPA and OPA, with inflection points at 7098.72 and 4200.11 MET-min/week, respectively.
Conclusion: We found that the relationship between PA and anxiety was domain-specific. OPA was positively associated with anxiety above a certain threshold, whereas LTPA was inversely associated. HPA showed only a weak positive association. Public health strategies should distinguish between activity domains and population characteristics, and implement targeted interventions for anxiety.
Keywords: physical activity, anxiety, domain-specific, occupational physical activity, leisure-time physical activity, household physical activity
Introduction
The prevalence of anxiety disorders increases in China, driven by population growth and demographic aging.1,2 Anxiety is associated with psychological distress, multi-system dysfunction, and more often than not this is accompanied by comorbidity with chronic physical conditions which can cause a reduction in the quality of life and social functioning.3–7 There is growing support in the field of clinical practice to incorporate lifestyle intervention with conventional treatment.8 Regular physical activity (PA) is a cost-effective cornerstone of mental health lifestyle interventions through integrated psychobiological pathways.9,10
The connection between PA and anxiety is complicated and controversial particularly in terms of domains and quantity of activities. To start with, the physical activity paradox has found that:11–13 autonomous, enjoyable leisure-time physical activity (LTPA) is associated with lower anxiety, whereas occupational physical activity (OPA) is associated with increased fatigue and higher anxiety risk.14–16 OPA is predominantly governed by external regulation such as financial reward, constraining autonomy over the nature and intensity of exertion. Conversely, LTPA is fueled by intrinsic motivation, marked by high self-determination and hedonic enjoyment.17,18 Notably, the physical activity paradox framework has predominantly centered on the dichotomy between LTPA and OPA, largely overlooking household physical activity (HPA) as an independent domain. HPA is a part of daily movement and is explicitly recognized as a distinct dimension in widely used instruments such as the International Physical Activity Questionnaire (IPAQ). Existing evidence regarding the relationship between HPA and anxiety remains sparse and equivocal.11,19 Second, the relationship between anxiety and PA volume is nonlinear.20,21 With excessive intensity or prolonged duration, the association may weaken or reverse, and may be associated with negative effects due to an inability to adapt and recover.22 This highlights the need to identify domain-specific turning points to define the safe and effective PA range for anxiety management.
Rural middle-aged and older adults in China represent an ideal population for examining the physical activity paradox. Unlike their urban counterparts, who are predominantly engaged in sedentary or discretionary occupations, rural older adults often continue to perform heavy agricultural labor well into old age, rendering their OPA largely obligatory and associated with insufficient recovery time.23,24 At the same time, this population faces unique psychosocial stressors, including poor access to mental health services, a high prevalence of the empty-nest syndrome resulting from adult children migrating to cities, and economic vulnerability.25–27 Each of these factors may be associated with a higher baseline risk of anxiety. In addition, cultural background is associated with the expression of anxiety symptoms, pointing to the value of local evidence.28 Against this background, the present study systematically examined domain-specific associations and nonlinear relationships between PA and anxiety in a rural middle-aged and older adult population. We propose the following hypotheses. First, based on the physical activity paradox, we hypothesize that LTPA is inversely associated with anxiety, whereas OPA is positively associated with anxiety. Second, given the inconsistent evidence on HPA and its limited investigation in this population, we do not prespecify a directional hypothesis and instead treat this association as exploratory. Third, we hypothesize that the dose-response relationship between OPA and anxiety is nonlinear, with an inflection point beyond which the risk pattern changes. By integrating activity domains and individual characteristics, this study aims to provide targeted evidence for public health guidance on anxiety prevention in China.
Materials and Methods
Study Design and Participants
This study was based on data from the Yangzhou Upper Gastrointestinal Disease Screening Cohort, which enrolled participants from 2017 to 2024 in Jiangsu Province. Of the 4904 enrolled participants, 510 were excluded due to missing covariates or prior cancer, yielding a final cohort of 4394 individuals (Figure 1). No imputation was performed for missing covariate data.
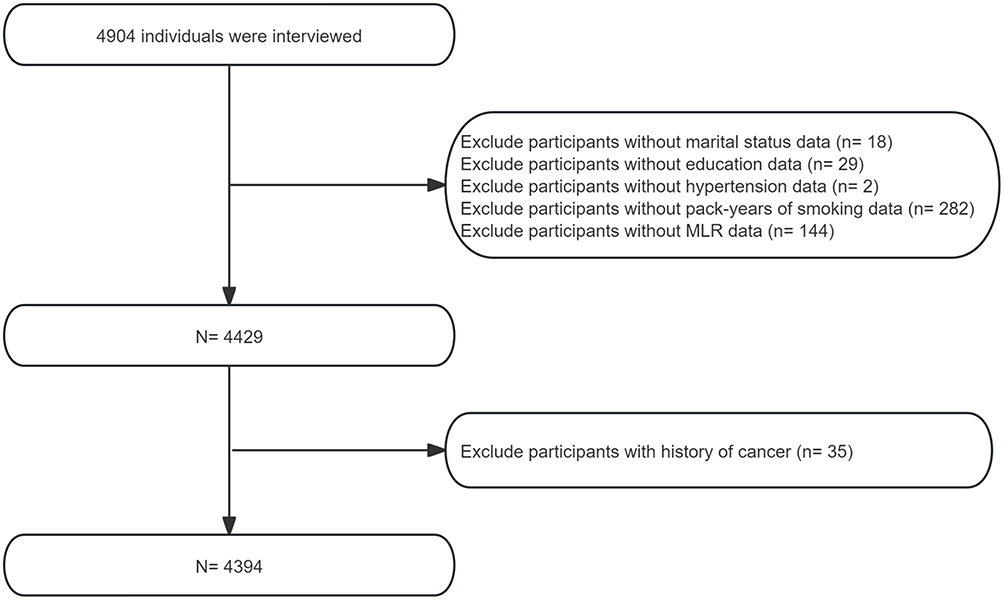 |
Figure 1 Flow chart for inclusion and exclusion criteria of the study population. |
All participants underwent standardized questionnaires, physical examinations, fasting laboratory tests, and upper gastrointestinal endoscopy. Our research has been ethically approved by the Ethics Review Committee of Yangzhou University Affiliated Hospital. All procedures were performed in accordance with the Helsinki Declaration, and written informed consent was obtained from all participants before enrollment.
Assessment of PA
Self-reported PA was assessed using a questionnaire based on the IPAQ.29 The questionnaire captured occupational, leisure-time, and household activities, recording key parameters for each: type, intensity, weekly frequency, session duration, and cumulative years of engagement. Commuting-related activities were excluded from the total physical activity (TPA) calculation because the predominant modes (motor vehicle/electric bicycle) in the study population involved energy expenditure comparable to sedentary levels. HPA was classified as light-intensity physical activity (LPA).
For quantitative analysis, PA volume was computed through MET values, which were assigned based on the intensity of each activity:30,31 3.3 METs for LPA (such as walking, light household chores), 4.0 METs for moderate-intensity PA (MPA, such as brisk walking, Tai Chi), and 8.0 METs for vigorous-intensity PA (VPA, such as running, heavy manual labor). The weekly PA volume for each domain d (occupational, leisure-time, or household) was calculated as:

where METi, Frequencyi, and Durationi represent the assigned MET value, weekly session days, and session duration in minutes for activity i, respectively.
No observations were excluded from the main analysis. IQR‑based outlier removal was used only in sensitivity analyses to test robustness.
Assessment of Anxiety
Anxiety was evaluated through the 7-item Generalized Anxiety Disorder Scale (GAD-7).32 On this scale, participants rated each symptom’s two-week frequency from 0 to 3, with a score ≥5 indicating the presence of anxiety symptoms.33
Covariates
Sociodemographic and health-related data were collected through standardized questionnaires and physical examinations. Marital status was categorized as married or unmarried/living alone. Education was categorized as ≤9 years, 9–12 years, and >12 years of schooling. BMI was classified into <25 kg/m2, 25–30 kg/m2, and ≥30 kg/m2. Length of sleep was classified as short (<6 h/day), suitable (6–8 h/day), and long (>8 h/day). Cumulative smoking exposure was quantified in pack-years and categorized as never, light-to-moderate (<20 pack-years), or heavy (≥20 pack-years). Alcohol drinking was defined as current (≥1 standard drink per week on average over the past year) versus non-use (never or former drinking). Based on their self-reported psychological stress over the past month, participants were categorized into low, moderate, and high groups. Hypertension was defined as self-reported diagnosis or SBP≥140 mmHg and/or DBP≥90 mmHg. Diabetes was defined as self-reported diagnosis or current use of glucose-lowering medication. Heart disease was defined as physician-confirmed coronary heart disease, myocardial infarction, or heart failure. Gastric disease was defined as present if endoscopy and histopathology showed atrophy, intestinal metaplasia, dysplasia, or cancer, and absent if normal mucosa or non-atrophic gastritis was found. Three inflammation-based composite indices were computed from the complete blood count: the neutrophil-to-lymphocyte ratio (NLR) and the monocyte-to-lymphocyte ratio (MLR) were calculated as the ratios of absolute neutrophil or monocyte counts to the absolute lymphocyte count, respectively; the systemic immune-inflammation index (SII) was calculated as platelet count × neutrophil count/lymphocyte count.34,35 Pepsinogen ratio (PGR) was computed as serum pepsinogen I divided by pepsinogen II (PG I/PG II).36
Statistical Analysis
Continuous variables were presented as means ± standard deviations, while categorical variables were reported as frequencies and corresponding percentages. Multivariable logistic regression was applied to quantify the association between PA and anxiety, yielding adjusted odds ratios (ORs) with 95% confidence intervals (CIs). Three hierarchical logistic regression models were fitted: Crude (unadjusted); Model 1 (adjusted age and sex); Model 2 (additionally adjusted marital status, education, BMI, length of sleep, pack-years of smoking, alcohol drinking, psychological stress, hypertension, diabetes, heart disease and MLR). PA was analyzed as a continuous variable (per 1-SD increase in MET-min/week) and in tertiles. We used restricted cubic splines (RCS) fitted with four knots (at the 5th, 35th, 65th, and 95th percentiles) to model potential nonlinear relationships. Subgroup analyses were conducted according to age, sex, BMI, length of sleep, pack-years of smoking, and alcohol drinking. To assess the robustness of our main findings, we performed a sensitivity analysis in which TPA outliers identified by the IQR method (observations below Q1−1.5×IQR or above Q3+1.5×IQR) were excluded. Finally, the Boruta algorithm was employed to identify factors significantly associated with anxiety.
Results
Baseline Characteristics
The study included 4394 participants, with 622 (14.2%) screening positive for anxiety symptoms. The mean age of the cohort was 56.67±8.73 years, and 41.1% were male. TPA averaged 5853.03±2283.28 MET-min/week, driven mainly by OPA (3224.48±1964.73 MET-min/week), followed by HPA (1797.13±1326.12 MET-min/week) and LTPA (831.43±265.52 MET-min/week). Anxiety was significantly more prevalent among females, younger individuals, short sleepers, non-drinkers, lighter smokers, and those with higher psychological stress, heart disease, or lower MLR (Table 1).
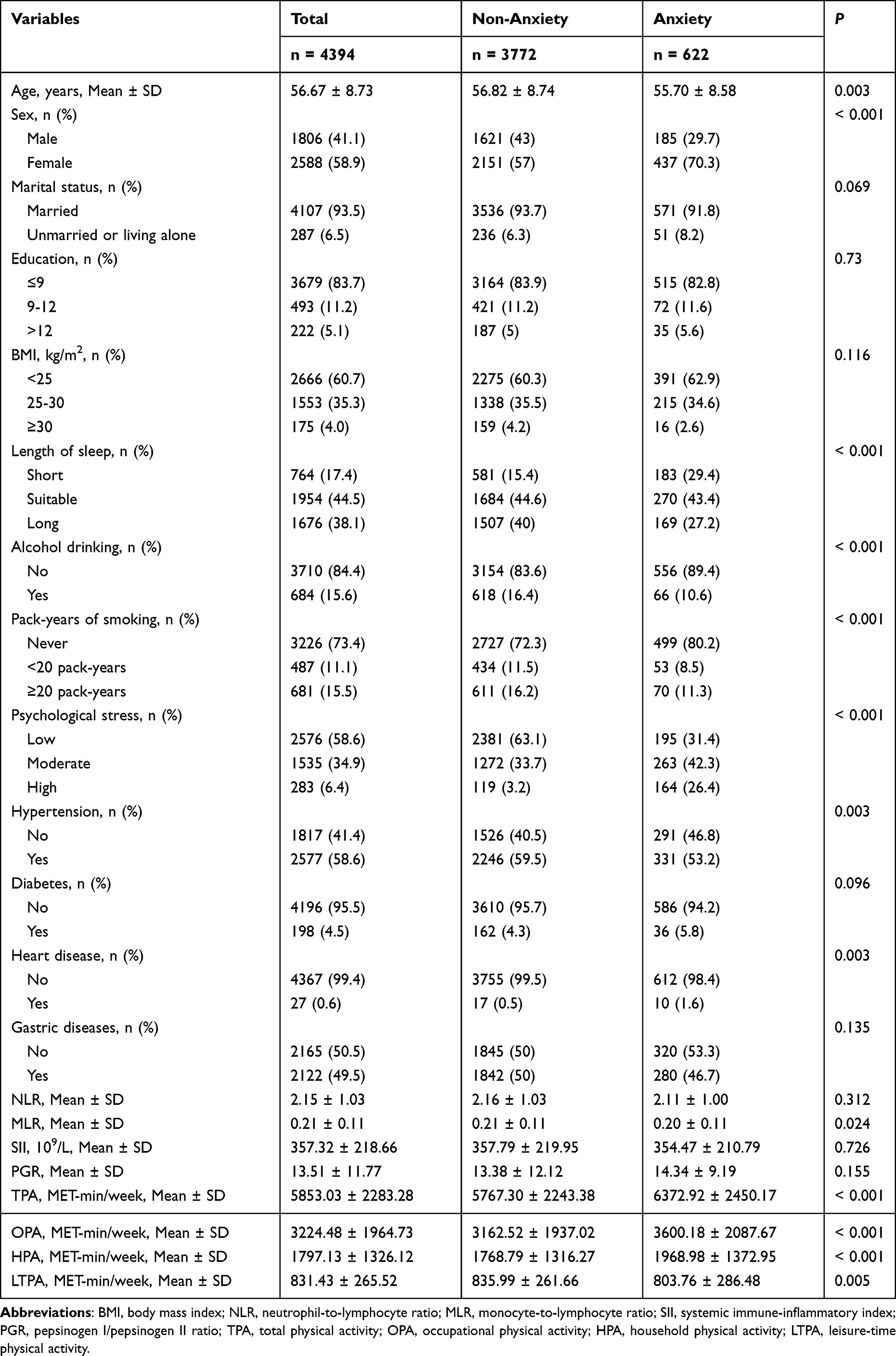 |
Table 1 Baseline Characteristics of Participants |
Associations Between PA and Anxiety
Logistic regression analysis showed domain-specific associations between PA and anxiety (Table 2). In the fully adjusted model, TPA and OPA were positively associated with anxiety risk. Specifically, each 1-SD increment in TPA or OPA was associated with an OR of 1.22 for anxiety (95% CI: 1.11–1.34, P<0.001). When analyzed by tertiles, participants in the highest TPA tertile (T3) had higher odds compared with the lowest tertile (T1) (OR=1.35, 95% CI: 1.07–1.70, P=0.010); for OPA, the T3 versus T1 comparison was not statistically significant (OR=1.22, 95% CI: 0.98–1.53, P=0.078). HPA showed a marginally significant positive association with anxiety in the fully adjusted model (OR=1.10, 95% CI: 1.00–1.21, P=0.050). LTPA exhibited an inverse association with anxiety: each 1-SD increment was associated with an OR of 0.88 (95% CI: 0.80–0.96, P=0.004), and the T3 versus T1 comparison yielded an OR of 0.74 (95% CI: 0.59–0.94, P=0.012).
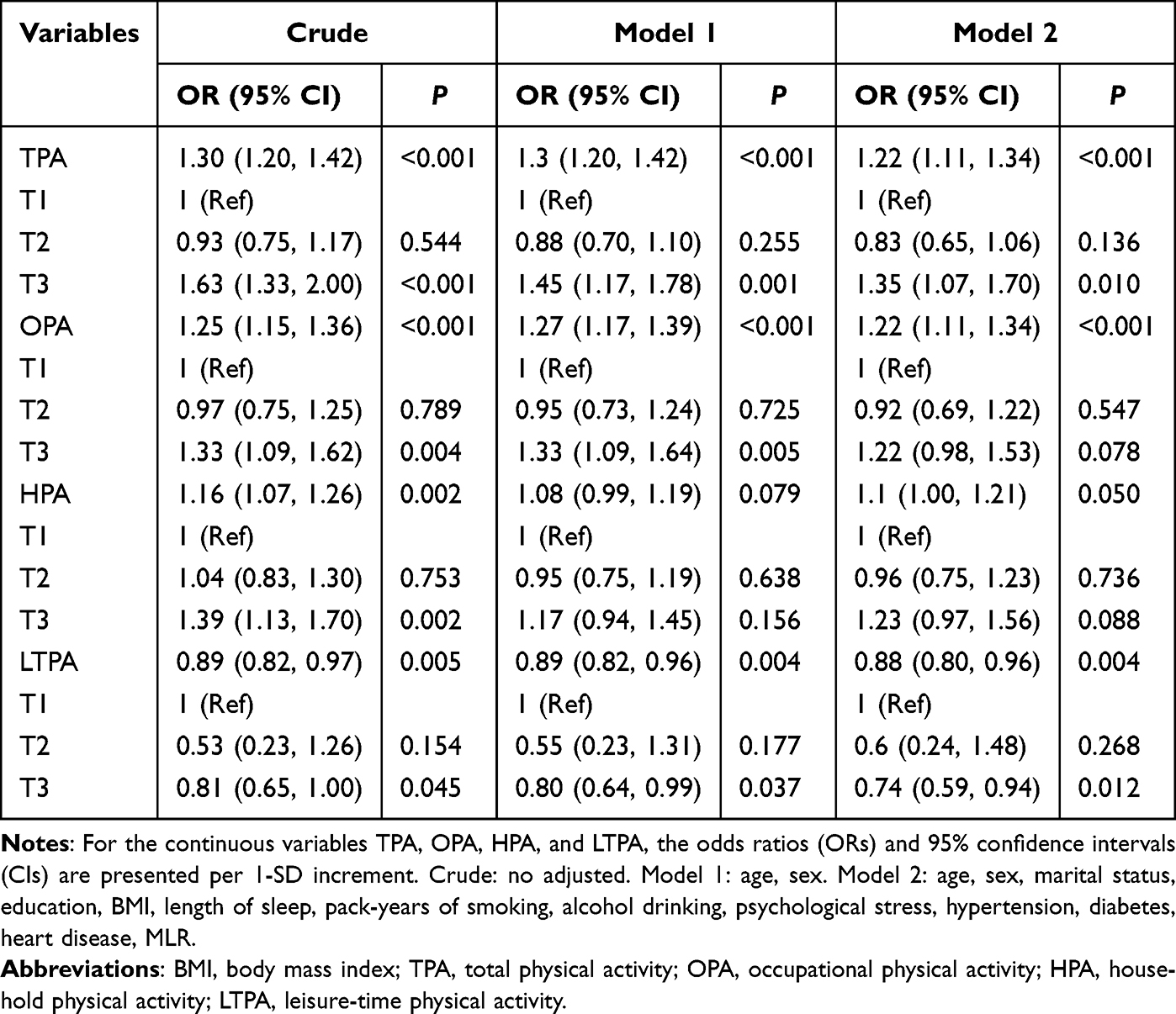 |
Table 2 Associations Between PA and Anxiety |
RCS analysis showed reverse L-shaped nonlinear associations with anxiety symptoms for both TPA (inflection point: 7098.72 MET-min/week) and OPA (inflection point: 4200.11 MET-min/week) (Figure 2). Below these thresholds, the associations were not statistically significant (P>0.05). Above the thresholds, each 100 MET-min/week increase in TPA and OPA was associated with higher anxiety odds (OR=1.02, 95% CI: 1.01–1.03, P=0.001 for TPA; OR=1.02, 95% CI: 1.01–1.04, P=0.003 for OPA). In contrast, HPA and LTPA showed no significant nonlinear associations with anxiety (Table 3 and Table 4).
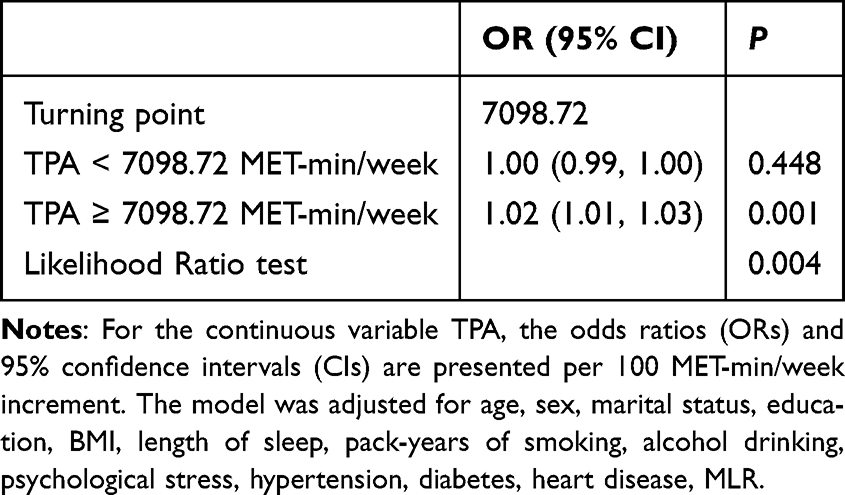 |
Table 3 Association Between TPA and Anxiety Using Two-Piecewise Regression Models |
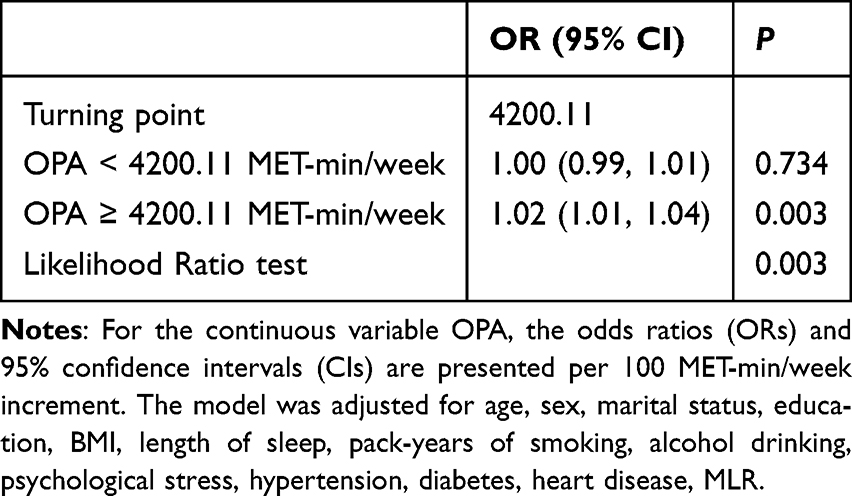 |
Table 4 Association Between OPA and Anxiety Using Two-Piecewise Regression Models |
 |
Figure 2 Restricted cubic spline analysis of the association between PA and anxiety. (A) total physical activity (TPA), (B) occupational physical activity (OPA), (C) household physical activity (HPA), (D) leisure-time physical activity (LTPA). |
Sensitivity Analysis
Subgroup analyses by age, sex, BMI, sleep duration, pack-years of smoking, and alcohol drinking showed that the associations of TPA, OPA, and HPA with anxiety remained stable across all strata (Figures 3 and S1–S3). Although the P value for the LTPA–smoking interaction was below 0.05, this finding should be interpreted with caution given multiple testing. Furthermore, the results remained robust after excluding IQR-defined outliers (Table S1). As shown in Figure 4, the Boruta algorithm identified 11 variables as the strongest predictors of anxiety after 500 iterations. Ranked by their z-scores, these variables were: psychological stress, sex, sleep duration, OPA, HPA, pack-years of smoking, age, heart disease, education, MLR, and LTPA.
 |
Figure 3 Association between TPA and anxiety. Each stratification was adjusted for age, sex, marital status, education, BMI, length of sleep, pack-years of smoking, alcohol drinking, psychological stress, hypertension, diabetes, heart disease, MLR except the stratification factor itself. Bold font indicates the overall effect and each subgroup itself. |
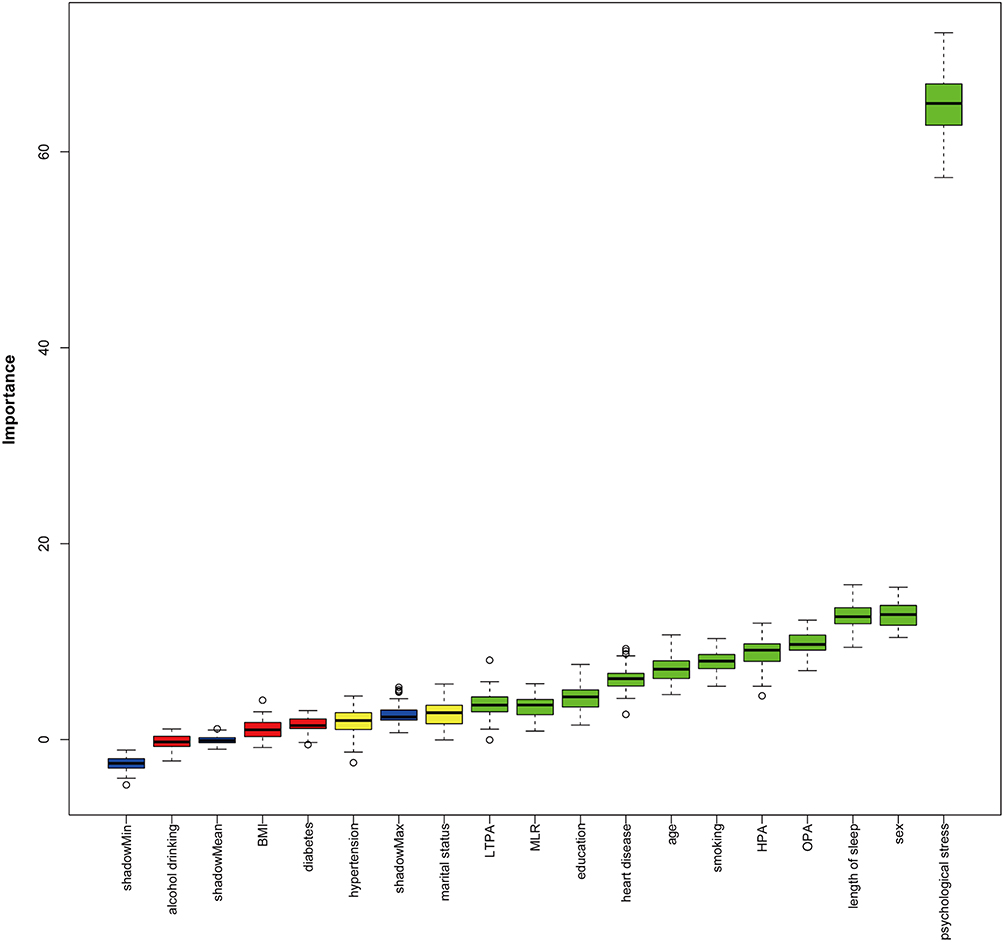 |
Figure 4 Feature selection results of the Boruta algorithm. Predictor importance for anxiety according to the Boruta algorithm. The blue box plots indicate the Z-scores of the shadow attributes; the red, yellow, and green box plots represent the rejected, tentative, and confirmed scoring attributes, respectively. A predictor is deemed important (green) if its mean importance Z-score is significantly higher than the maximum value of the shadow variables, and excluded (red) if significantly lower than the maximum value of the shadow variables. Predictors marked in yellow are classified as tentative, indicating that their importance remains uncertain and requires further evaluation. |
Discussion
The study examined domain-specific associations of PA with anxiety based on the Yangzhou Upper Gastrointestinal Disease Screening Cohort, providing local empirical support for the physical activity paradox. The main findings were as follows: TPA was positively associated with anxiety; OPA was positively associated, LTPA negatively associated, and HPA weakly positively associated. Furthermore, RCS analysis indicated reverse L-shaped associations of both TPA and OPA with anxiety.
We found a significant positive association between PA and anxiety among rural middle-aged and older adults engaged in heavy labor. While seemingly at odds with the consensus that “exercise promotes mental health”,37,38 this finding highlighted the critical domain-specific associations of PA. In this cohort, PA was predominantly comprised of OPA, which was characterized by high psychological pressure, low autonomy, and inadequate recovery.12,39 Functioning as a chronic passive stressor rather than an intrinsically motivated health behavior, OPA may be associated with attenuated or even negated protective associations.40–42 At a biological level, prolonged occupational exertion is linked to anxiety risk through sustained sympathetic overactivation and dysregulation of the HPA axis feedback,43,44 reduced BDNF synthesis, and elevated systemic inflammation.45,46 To explore whether inflammation is involved in the above association, we calculated NLR, MLR, and SII. The results did not support this hypothesis: there were no differences in NLR or SII between the anxiety and non-anxiety groups, while MLR was unexpectedly lower in the anxiety group. This counterintuitive finding is unlikely to reflect immunosuppression; rather, it is more likely attributable to baseline characteristics of the anxiety group, including a higher proportion of females and lower rates of smoking and alcohol consumption. Thus, the inflammatory pathway was not supported in our cohort, and psychosocial factors may be more strongly associated with anxiety.
In contrast, LTPA is associated with better mental health, possibly through fulfilling the basic psychological needs for autonomy, relatedness and competence.11,18,47 This positive engagement parallels the neurobiological findings of moderate exercise—which upregulates neurotrophic factors (IGF-1, BDNF, VEGF) to support neuroplasticity and cerebrovascular health,48,49 modulates monoamine and endogenous opioid systems for emotion regulation,50–52 and improves cerebral blood flow and metabolism.53,54
Notably, HPA showed a marginally significant positive association with anxiety. While an early meta-analysis (over 640,000 participants) found no significant association with mental health,11 a 2025 meta-analysis (over 3.3 million participants) reported a weak positive association with mental health.19 This shift may reflect lifestyle changes: more people now engage in enjoyable, autonomous household activities like gardening or parent-child play, rather than only traditional chores.17,19 In our cohort, the persistently weak positive association suggests that rural middle-aged and older adults perform traditional, livelihood-oriented, duty-driven household activities. Although such activities may provide daily structure and a sense of family role identity, their autonomy is far lower than that of LTPA, and they often entail minor burdens such as time pressure and fatigue. These characteristics likely explain the weak positive association.
Our RCS analysis indicated a reverse L-shaped relationship between PA and anxiety risk, with an inflection point at 7098.72 MET-min/week. This finding aligned with existing research in confirming a complicated relationship between PA and anxiety, while highlighting the significant moderating roles of population characteristics and activity domains. For instance, a study of 30054 Chinese adults revealed an inverse J-shaped relationship, with benefits peaking at 903 MET-min/week;55 this lower threshold was thought to reflect the optimal mental health benefit zone in general populations dominated by LTPA. In contrast, the substantially higher inflection point identified in our study may represent a critical point of psychophysiological tolerance in a population primarily engaged in OPA. We posit that long-term adaptation to high-intensity labor elevates this statistical threshold. However, this very adaptation implies a sustained high-load physiological state; consequently, exposure beyond this critical point may be associated with acute homeostatic overload and higher anxiety risk.56 This pattern is further contextualized by a study of a primarily urban, younger Japanese population, which reported a U-shaped relationship with the lowest anxiety at an intermediate threshold of 5277 MET-min/week,21 bridging the gap between the leisure-focused Chinese cohort and our occupationally active sample. Taken together, these comparisons suggest that anxiety-related PA thresholds are not fixed values but exist along a dynamic gradient, mediated by the dominant domain of activity and socio-demographic settings.
This study has several limitations. First, its cross-sectional design precludes causal inference and cannot rule out reverse causality—preexisting anxiety or economic hardship may drive excessive OPA, while psychological barriers may limit LTPA. Longitudinal data are needed to clarify temporal relationships. Second, PA was self-reported, introducing potential recall bias; although the questionnaire followed the IPAQ guidelines and drew on validated Chinese cohort instruments, it lacked formal psychometric validation. Third, commuting activities were excluded (due to predominant motor vehicle/electric bicycle), which may have underestimated TPA for walkers or cyclists—future studies should capture detailed commuting modes. Fourth, we used psychological stress as a proxy for broader psychological distress, and residual confounding by depression or unmeasured economic pressure remains possible. Notably, direct socioeconomic indicators were not included in the analysis due to low response rates and reporting bias—this may overestimate the observed association between OPA and anxiety. Finally, the findings are based on rural, middle-aged and older manual workers in Yangzhou, which limits their generalizability to other populations or regions.
Conclusion
In this rural, occupation-dominated middle-aged and older population, we identified significant domain-specific associations between physical activity and anxiety. OPA exhibited a reverse L-shaped nonlinear relationship: no significant association below a specific threshold, but higher odds of anxiety above that threshold. LTPA showed a linear inverse association. HPA presented a marginally significant positive association. For rural adults engaged in heavy occupational labor, these results suggest that avoiding excessive OPA and engagement in LTPA are associated with more favorable anxiety profiles than following the general recommendation to exercise more. Future public health guidelines may need to distinguish between activity domains and account for population characteristics in order to inform more precise intervention strategies.
Data Sharing Statement
The data from this study are available from the corresponding author upon reasonable request. Please contact Jun Yan, Email [email protected].
Ethics Statement
The studies involving humans were approved by Affiliated Hospital of Yangzhou University. The ethic number was 2020-YKL010-015. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Acknowledgments
We gratefully thank all patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Postgraduate Research and Practice Innovation Program of Jiangsu Province (KYCX24_3732).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–13. doi:10.1016/s2215-0366(18)30511-x
2. Tian W, Yan G, Xiong S, et al. Burden of depressive and anxiety disorders in China and its provinces, 1990-2021: findings from the global burden of disease study 2021. British J Psychiatry. 2025:1–11. doi:10.1192/bjp.2024.267
3. Vinkers CH, Kuzminskaite E, Lamers F, Giltay EJ, Penninx B. An integrated approach to understand biological stress system dysregulation across depressive and anxiety disorders. J Affect Disord. 2021;283:139–146. doi:10.1016/j.jad.2021.01.051
4. Sudhir PM, Sharma MP, Mariamma P, Subbakrishna DK. Quality of life in anxiety disorders: its relation to work and social functioning and dysfunctional cognitions: an exploratory study from India. Asian J Psychiatry. 2012;5(4):309–314. doi:10.1016/j.ajp.2012.05.006
5. Risal A, Manandhar K, Holen A, Steiner TJ, Linde M. Comorbidities of psychiatric and headache disorders in Nepal: implications from a nationwide population-based study. J Headache Pain. 2016;17(1):45. doi:10.1186/s10194-016-0635-8
6. Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primary care patients with chronic pain. General Hospital Psychiatr. 2013;35(4):359–365. doi:10.1016/j.genhosppsych.2013.03.020
7. Lim LL, Jones S, Cikomola JC, Hivert MF, Misra S. Understanding the drivers and consequences of early-onset type 2 diabetes. Lancet. 2025;405(10497):2327–2340. doi:10.1016/s0140-6736(25)01012-8
8. Firth J, Solmi M, Wootton RE, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–380. doi:10.1002/wps.20773
9. Singh B, Olds T, Curtis R, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. 2023;57(18):1203–1209. doi:10.1136/bjsports-2022-106195
10. Peluso MA, Guerra de Andrade LH. Physical activity and mental health: the association between exercise and mood. Clinics. 2005;60(1):61–70. doi:10.1590/s1807-59322005000100012
11. White RL, Babic MJ, Parker PD, Lubans DR, Astell-Burt T, Lonsdale C. Domain-specific physical activity and mental health: a meta-analysis. Am J Preventive Med. 2017;52(5):653–666. doi:10.1016/j.amepre.2016.12.008
12. Holtermann A, Krause N, van der Beek AJ, Straker L. The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med. 2018;52(3):149–150. doi:10.1136/bjsports-2017-097965
13. Mizrahi D, Swain CTV, Bruinsma F, Hodge A, Taylor N, Lynch BM. The relationship between psychological distress and physical activity is non-linear and differs by domain: a cross-sectional study. Int J Behav Med. 2023;30(5):673–681. doi:10.1007/s12529-022-10130-5
14. de Vries JD, Bakker AB. The physical activity paradox: a longitudinal study of the implications for burnout. Int Archiv Occupational Environm Health. 2022;95(5):965–979. doi:10.1007/s00420-021-01759-y
15. Cillekens B, Lang M, van Mechelen W, et al. How does occupational physical activity influence health? An umbrella review of 23 health outcomes across 158 observational studies. Br J Sports Med. 2020;54(24):1474–1481. doi:10.1136/bjsports-2020-102587
16. Heesch KC, Burton NW, Brown WJ. Concurrent and prospective associations between physical activity, walking and mental health in older women. J Epidemiol Community Health. 2011;65(9):807–813. doi:10.1136/jech.2009.103077
17. Salvo D, Jáuregui A, Adlakha D, Sarmiento OL, Reis RS. When moving is the only option: the role of necessity versus choice for understanding and promoting physical activity in low- and middle-income countries. Annu Rev Public Health. 2023;44(1):151–169. doi:10.1146/annurev-publhealth-071321-042211
18. Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutrition Phys Activity. 2012;9(1):78. doi:10.1186/1479-5868-9-78
19. Teychenne M, Sousa GM, Baker T, et al. Domain-specific physical activity and mental health: an updated systematic review and multilevel meta-analysis in a combined sample of 3.3 million people. Br J Sports Med. 2025;59(9):659–666. doi:10.1136/bjsports-2025-109806
20. Li X, Chen W, Zhang Z, et al. Association between physical activity and risk of anxiety: a dose-response meta-analysis of 11 international cohorts. EClinicalMedicine. 2025;84:103285. doi:10.1016/j.eclinm.2025.103285
21. Shimura A, Masuya J, Yokoi K, et al. Too much is too little: estimating the optimal physical activity level for a healthy mental state. Front Psychol. 2022;13:1044988. doi:10.3389/fpsyg.2022.1044988
22. Colledge F, Sattler I, Schilling H, Gerber M, Pühse U, Walter M. Mental disorders in individuals at risk for exercise addiction - A systematic review. Addict Behav Rep. 2020;12:100314. doi:10.1016/j.abrep.2020.100314
23. Zhao Y, Hou G, Gu Y, et al. Labour-type physical activity, alcohol use and hypertension in rural older adults in Northeast China. Front Public Health. 2026;14:1748721. doi:10.3389/fpubh.2026.1748721
24. Zeng Y, Zhang S, Li D, Liao A. Community environment and physical activity participation among rural older adults in China: evidence from the China longitudinal aging social survey. Front Public Health. 2026;14:1753599. doi:10.3389/fpubh.2026.1753599
25. Jiang Z, Ren H, Sun Q, Zhang H, Zhou S. Attitude towards aging and anxiety in the relationship between social alienation and depression in Chinese rural empty-nest older adults: a chained mediation modeling analysis. BMC Public Health. 2025;25(1):1435. doi:10.1186/s12889-025-22712-5
26. Wang L, Shentu Q, Xu B, Liang Y. The prevalence of anxiety on the empty-nest elders in China. J Health Psychol. 2020;25(2):152–160. doi:10.1177/1359105318776727
27. Xie J, Liu M, Ding S, et al. Attitudes toward depression among rural primary healthcare providers in hunan areas, China: a cross sectional study. BMC Med Educ. 2023;23(1):226. doi:10.1186/s12909-023-04197-1
28. Jovanović V, Adams S, Aritio-Solana R, et al. Positive and negative emotional experiences in adolescents across 32 countries: cross-national and gender differences. Appl Res Qual Life. 2025;20(4):1731–1757. doi:10.1007/s11482-025-10486-2
29. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exercise. 2003;35(8):1381–1395. doi:10.1249/01.Mss.0000078924.61453.Fb
30. Li X, Zhang W, Zhang W, et al. Level of physical activity among middle-aged and older Chinese people: evidence from the China health and retirement longitudinal study. BMC public Health. 2020;20(1):1682. doi:10.1186/s12889-020-09671-9
31. Zhou Z, Tian X. Prevalence and association of sleep duration and different volumes of physical activity with type 2 diabetes: the first evidence from CHARLS. BMC Public Health. 2024;24(1):3331. doi:10.1186/s12889-024-20743-y
32. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archiv Internal Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
33. Kroenke K, Spitzer RL, Williams JB, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Internal Med. 2007;146(5):317–325. doi:10.7326/0003-4819-146-5-200703060-00004
34. Fang JW, She Q, Xia JL, et al. A nomogram combining platelet to lymphocyte ratio (PLR) and systemic inflammatory response index (SIRI) to predict patients with H. pylori -positive gastric dysplasia. J Multidisciplinary Healthc. 2025;18:6795–6809. doi:10.2147/jmdh.S538329
35. Guo B, Liu X, Si Q, et al. Associations of CBC-Derived inflammatory indicators with sarcopenia and mortality in adults: evidence from Nhanes 1999 ∼ 2006. BMC Geriatr. 2024;24(1):432. doi:10.1186/s12877-024-05012-2
36. Chi Y, Tian H, Shi C, et al. Enhancing diagnostic accuracy: role of stomach-specific serum biomarkers in real-world risk-based sequential screening for malignant gastric lesions. Chinese J Cancer Res. 2025;37(2):154–164. doi:10.21147/j.issn.1000-9604.2025.02.03
37. Fiuza-Luces C, Garatachea N, Berger NA, Lucia A. Exercise is the real polypill. Physiology. 2013;28(5):330–358. doi:10.1152/physiol.00019.2013
38. Smith PJ, Merwin RM. The role of exercise in management of mental health disorders: an integrative review. Ann Rev Med. 2021;72(1):45–62. doi:10.1146/annurev-med-060619-022943
39. Ketels M, Belligh T, De Bacquer D, Clays E. Are psychosocial resources buffering the relation between physical work behaviors and need for recovery? Int J Public Health. 2022;67:1604787. doi:10.3389/ijph.2022.1604787
40. Abe T, Okuyama K, Motohiro A, Shiratsuchi D, Isomura M. Combined associations of regular exercise and work-related moderate-to-vigorous physical activity with occupational stress responses: a cross-sectional study. Front Sport Active Liv. 2024;6:1386775. doi:10.3389/fspor.2024.1386775
41. Sothmann MS, Buckworth J, Claytor RP, Cox RH, White-Welkley JE, Dishman RK. Exercise training and the cross-stressor adaptation hypothesis. Exer Sport Sci Rev. 1996;24:267–287. doi:10.1249/00003677-199600240-00011
42. Abe T, Okuyama K, Motohiro A, Shiratsuchi D, Isomura M. Association between different types of physical activity and occupational stress in Japanese workers: a cross-sectional study. Industrial Health. 2024;62(4):227–236. doi:10.2486/indhealth.2023-0092
43. Swaab DF, Bao AM, Lucassen PJ. The stress system in the human brain in depression and neurodegeneration. Ageing Res Rev. 2005;4(2):141–194. doi:10.1016/j.arr.2005.03.003
44. Angeli A, Minetto M, Dovio A, Paccotti P. The overtraining syndrome in athletes: a stress-related disorder. J Endocrinol Invest. 2004;27(6):603–612. doi:10.1007/bf03347487
45. Dadkhah M, Baziar M, Rezaei N. The regulatory role of BDNF in neuroimmune axis function and neuroinflammation induced by chronic stress: a new therapeutic strategies for neurodegenerative disorders. Cytokine. 2023;174:156477. doi:10.1016/j.cyto.2023.156477
46. Lee J, Kim H-R, Jang T-W, Lee D-W, Lee YM, Kang M-Y. Occupational physical activity, not leisure-time physical activity, is associated with increased high-sensitivity C reactive protein levels. Occup Environ Med. 2021;78(2):86–91. doi:10.1136/oemed-2020-106753
47. Ryan RM, Deci EL. Intrinsic and extrinsic motivation from a self-determination theory perspective: definitions, theory, practices, and future directions. Contemp Educ Psychol. 2020;61:101860. doi:10.1016/j.cedpsych.2020.101860
48. Cotman CW, Berchtold NC, Christie LA. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci. 2007;30(9):464–472. doi:10.1016/j.tins.2007.06.011
49. Voss MW, Erickson KI, Prakash RS, et al. Neurobiological markers of exercise-related brain plasticity in older adults. Brain Behav Immun. 2013;28:90–99. doi:10.1016/j.bbi.2012.10.021
50. Chaouloff F. Physical exercise and brain monoamines: a review. Acta Physiol Scand. 1989;137(1):1–13. doi:10.1111/j.1748-1716.1989.tb08715.x
51. Xue P, Du X, Kong J. Age-dependent mechanisms of exercise in the treatment of depression: a comprehensive review of physiological and psychological pathways. Front Psychol. 2025;16:1562434. doi:10.3389/fpsyg.2025.1562434
52. Chen Z, Lan W, Yang G, et al. Exercise intervention in treatment of neuropsychological diseases: a review. Front Psychol. 2020;11:569206. doi:10.3389/fpsyg.2020.569206
53. Kleinloog JPD, Mensink RP, Ivanov D, Adam JJ, Uludağ K, Joris PJ. Aerobic exercise training improves cerebral blood flow and executive function: a randomized, controlled cross-over trial in sedentary older men. Front Aging Neurosci. 2019;11:333. doi:10.3389/fnagi.2019.00333
54. Renke MB, Marcinkowska AB, Kujach S, Winklewski PJ. A systematic review of the impact of physical exercise-induced increased resting cerebral blood flow on cognitive functions. Front Aging Neurosci. 2022;14:803332. doi:10.3389/fnagi.2022.803332
55. Zhou H, Jiang F, Liu H, Wu Y, Tang YL. Dose-dependent association between physical activity and mental health, and mitigation effects on risk behaviors. iScience. 2025;28(2):111866. doi:10.1016/j.isci.2025.111866
56. McEwen BS. Neurobiological and systemic effects of chronic stress. Chronic Stress. 2017;1:2470547017692328. doi:10.1177/2470547017692328.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Physical Activity on Anxiety: The Mediating Role of Subjective Well-Being and the Moderating Role of Gender
Tian J, Yu H, Austin L
Psychology Research and Behavior Management 2022, 15:3167-3178
Published Date: 27 October 2022
Association Between Emotional Eating, Sociodemographic Characteristics, Physical Activity, Sleep Duration, and Mental and Physical Health in Young Adults
Calderón-Asenjo RE, Jalk-Muñoz MC, Calizaya-Milla YE, Calizaya-Milla SE, Ramos-Vera C, Saintila J
Journal of Multidisciplinary Healthcare 2022, 15:2845-2859
Published Date: 13 December 2022
Mental Health, Sleep, and Physical Activity Among Young Saudi Women During Ramadan: A Comparative Cohort Study
Balasubramanian K, Sanjeevi RR, Alshehri MM, Alothman SA
Nature and Science of Sleep 2026, 18:583610
Published Date: 11 June 2026