Back to Journals » Journal of Inflammation Research » Volume 19
Association Between Perioperative Inflammatory Trajectories and Postoperative Hirschsprung-Associated Enterocolitis: Insights from Group-Based Trajectory Modeling
Authors Jiang Z ![]() , Feng W, Hu H, Wei X, Jiang Y, Hou J, Wang Y
, Feng W, Hu H, Wei X, Jiang Y, Hou J, Wang Y
Received 21 January 2026
Accepted for publication 15 May 2026
Published 11 June 2026 Volume 2026:19 594201
DOI https://doi.org/10.2147/JIR.S594201
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alberto Caminero
Zhengxing Jiang, Wei Feng, Hongtao Hu, Xiaoping Wei, Yinuo Jiang, Jinping Hou, Yi Wang
Department of General and Neonatal Surgery, Children’s Hospital of Chongqing Medical University; National Clinical Research Center for Child Health and Disorders; Ministry of Education Key Laboratory of Child Development and Disorders; Chongqing Key Laboratory of Structural Birth Defect and Reconstruction, Chongqing, People’s Republic of China
Correspondence: Wei Feng; Yi Wang, Department of General and Neonatal Surgery, Children’s Hospital of Chongqing Medical University, 20 Jinyu Avenue, Yubei District, Chongqing, People’s Republic of China, Tel +86 15123495318 ; +86 18523442781, Email [email protected]; [email protected]
Purpose: This retrospective cohort study aimed to delineate the dynamic change trajectories of perioperative inflammatory markers in pediatric patients with Hirschsprung disease (HSCR) who underwent one-stage laparoscopic-assisted pull-through surgery at a single tertiary pediatric center using Group-Based Trajectory Modeling (GBTM), and to explore the association between different trajectory patterns and the risk of postoperative Hirschsprung-associated enterocolitis (HAEC).
Methods: This study enrolled HSCR patients who underwent surgical treatment. Blood samples were collected at four perioperative time points (preoperative, postoperative days 1, 4, and 7) to calculate composite inflammatory markers such as the systemic inflammation response index (SIRI) and pan-immune inflammation value (PIV), as well as individual markers like white blood cell (WBC) and neutrophil counts. GBTM was employed to identify subgroups with similar inflammatory marker change trajectories. Multivariable logistic regression analysis was used to assess the association between different inflammatory trajectories and postoperative HAEC occurring within several years after surgery.
Results: A total of 400 patients were included, of which 133 (33.3%) developed postoperative HAEC. Each inflammatory marker was categorized into 2– 3 significantly distinct trajectory groups via GBTM. Multivariable logistic regression analysis revealed that for SIRI and PIV, compared to trajectory group 1 (low baseline with mild rise), patients in trajectory group 2 (moderate baseline with sharp rise and slow decline; SIRI: OR = 5.20, P = 0.011; PIV: OR = 4.75, P = 0.007) and trajectory group 3 (high baseline with sharp rise and slow decline; SIRI: OR = 4.73, P = 0.025; PIV: OR = 5.63, P = 0.008) had a significantly increased risk of postoperative HAEC. For WBC and neutrophils, trajectory group 2 (WBC: persistently high; neutrophils: low baseline with sharp rise and rapid decline) was an independent risk factor for postoperative HAEC (WBC: OR = 2.49, P = 0.004; neutrophils: OR = 2.53, P = 0.001).
Conclusion: Specific rising trajectories of SIRI, PIV, WBC, and neutrophils may serve as novel biomarkers for early identification of children at high risk for HAEC.
Keywords: Hirschsprung-associated enterocolitis, group-based trajectory modeling, Hirschsprung disease, inflammatory markers, systemic inflammation response index, pan-immune inflammation value
Introduction
Hirschsprung disease (HSCR) is a congenital developmental anomaly of the enteric nervous system, characterized by the absence of ganglion cells in the distal affected bowel, leading to functional intestinal obstruction proximal to the aganglionic segment.1 Surgery is the only curative treatment, involving resection of the aganglionic bowel segment and anastomosis of the normally innervated bowel to the anal canal to restore intestinal function. Despite continuous advancements in current surgical techniques, approximately one-third of patients still develop postoperative complications.2
Among them, Hirschsprung-associated enterocolitis (HAEC) is the most common and severe complication of HSCR and the leading cause of mortality in affected patients.3 Currently, the diagnosis of HAEC mainly relies on clinical symptoms and signs, but the diagnostic criteria vary considerably across different studies, and the onset time of postoperative HAEC can range from immediately after surgery to several years postoperatively.4 The incidence of postoperative HAEC has been reported to be approximately 25 ~ 37%.3 Although previous studies have explored the relationship between factors such as surgical approach, pathological classification, nutritional status, and the risk of postoperative HAEC development, there remains a clinical lack of simple, convenient, and quantifiable biological indicators for risk stratification in patients with HSCR.5 The pathophysiological mechanism of HAEC is complex, involving multiple aspects including intestinal mucosal barrier disruption, dysbiosis, and abnormal immune responses. Notably, regardless of the initiating factors, inflammatory response represents a common pathway in the development of HAEC.6 Systemic inflammatory markers from routine blood tests, including neutrophils, monocytes, lymphocytes, and platelets, are key participants in this process. Composite indicators derived from these markers can theoretically reflect the systemic “inflammation-immunity-coagulation” imbalance that parallels the intestinal inflammatory state in HAEC, thereby providing clues for predicting HAEC.
Among numerous inflammatory markers, white blood cells (WBC), neutrophils, monocytes, lymphocytes, platelets and their derived systemic inflammatory response index (SIRI), pan-immune inflammatory value (PIV), systemic immune-inflammatory index (SII), etc, have been widely used in clinical practice due to their advantages of low cost, convenient detection, and rapid reporting. These indicators have demonstrated significant predictive value in areas such as gastric ulcer, cardiovascular diseases, and prognostic assessment of various tumors.7–10 However, most studies have focused solely on the association between inflammatory markers at a single time point and disease prognosis, failing to capture the dynamic changes in systemic inflammatory status and potentially overlooking critical information contained therein. Currently, the association between longitudinal dynamic changes in perioperative systemic inflammatory markers and the risk of HAEC has not been reported. Furthermore, whether different trajectory patterns of inflammatory markers can be used for postoperative HAEC risk stratification in HSCR patients remains unknown. This limitation underscores the importance of longitudinal research. Group-based trajectory modeling (GBTM), as a statistical method for longitudinal data, can effectively identify subgroups of individuals with similar change trajectories over time.11 Compared to static inflammatory markers measured at a single time point, GBTM can capture the dynamic evolution of perioperative inflammatory markers, thereby revealing distinct trajectory phenotypes that may reflect differences in evolution among patients and the risk of adverse outcomes.
This study aims to use GBTM to identify the change trajectories of inflammatory markers during the perioperative period in patients with HSCR and to further explore the association between different trajectory patterns and the risk of postoperative HAEC development. We hope to identify potential biomarkers by understanding the temporal evolution trends of different inflammatory markers, ultimately achieving precise risk stratification for HAEC high-risk patients, and providing a basis for early intervention and improving prognosis.
Materials and Methods
Relationship to Prior Work and Statement of Novelty
This study is part of an ongoing, broader research program at our institution, which systematically investigates the associations between perioperative factors and long-term outcomes in patients with HSCR. While utilizing a retrospective patient cohort similar to that in our previously published work, the present study addresses a distinct scientific question. Prior research primarily focused on the relationship between short-term postoperative complications and long-term bowel function.12 In contrast, this study introduces GBTM for the first time, revealing the dynamic and longitudinal inflammatory trajectory during the perioperative period and its association with the risk of postoperative HAEC from a novel perspective. Specifically, the innovations of this study include: (1) the first description of the dynamic evolution of composite and routine inflammatory markers during the perioperative period in HSCR patients, and (2) the first investigation into the correlation between these inflammatory trajectories and postoperative HAEC risk. Therefore, this study differs from previous work in its analytical method (GBTM for longitudinal data), its core exposure variable (dynamic inflammatory trajectories), and its study outcome (postoperative HAEC). It provides novel insights for understanding the pathogenesis of HAEC and enabling early prediction based on perioperative inflammatory dynamic patterns.
Study Approval
This study was approved by the Institutional Research Ethics Board of Children’s Hospital affiliated Chongqing Medical University (Date: 2023/No: 01) and complies with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Because this study was retrospective, the requirement for informed consent was waived. This study was conducted and reported in accordance with the RECORD guidelines.
Study Population
We retrospectively reviewed the medical records of HSCR patients who underwent surgical treatment in the Department of General and Neonatal Surgery at Children’s Hospital of Chongqing Medical University (a tertiary pediatric hospital and National Clinical Research Center for Child Health and Disorders in China) between January 2015 and July 2021. The inclusion criteria for this study were as follows: (1) Confirmed diagnosis of HSCR based on histopathology; (2) Received one-stage Laparoscopicassisted pull-through surgery (modified Swenson technique by the experienced team, the surgical procedure was described in detail in our previous report);13 (3) Had complete blood count results from ≥ 3 time points; (4) Had complete clinical data. It should be noted that some patients with long segment HSCR (L-HSCR) and total colonic aganglionosis (TCA) who underwent temporary enterostomy were not included in this study to maintain high homogeneity of the surgical cohort. Exclusion criteria were: (1) Occurrence of postoperative HAEC during hospitalization (the occurrence of HAEC might elevate the relevant inflammatory markers, potentially creating a bidirectional causal relationship that would preclude an accurate assessment of the impact of perioperative inflammatory trajectories on the outcome); (2) Presence of other systemic diseases affecting inflammatory markers; (3) Development of severe postoperative complications (grade III and IV complications according to Clavien-Dindo Classification System); (4) Presence of severe concomitant malformations affecting HSCR treatment; (5) Presence of cognitive impairment (especially Down syndrome; Figure 1). All patients were managed according to a standardized institutional protocol. Bowel preparation was initiated 2 weeks before surgery, including rectal irrigations, and the diet was changed to a liquid diet 3–5 days before surgery. Postoperatively, third-generation cephalosporins were routinely administered for anti-infection for one week (the course was extended if white blood cell or C-reactive protein levels remained elevated, or the antibiotic was escalated). An analgesic pump was routinely used (except for children younger than 1 year or weighing less than 10 kg), and patients were kept on a fasting regimen (no food or water) for five days while receiving parenteral nutrition support. Oral probiotics were started after the resumption of enteral feeding. All patients received standardized and systematic follow-up by telephone, internet, or clinic visit.
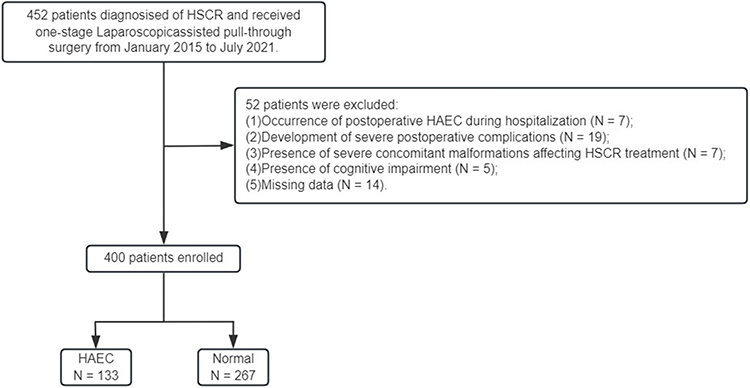 |
Figure 1 Flow chart of the study population. Abbreviations: HAEC, Hirschsprung-associated enterocolitis; HSCR, Hirschsprung disease. |
Exposure Variable and Covariates
Peripheral venous blood count data were retrieved from the electronic medical records for four prespecified perioperative time points:
- T1: The most recent preoperative sample (≤ 7 days before surgery);
- T2: Postoperative day 1;
- T3: Postoperative day 4 (± 1 day);
- T4: Postoperative day 7 (± 1 day).
Based on the complete blood count results, we obtained the counts of WBC, neutrophils (N), monocytes (M), lymphocytes (L), and platelets (PLT), and calculated the following composite inflammatory markers:
- Systemic Inflammatory Response Index (SIRI = N × M/L);
- Systemic Immune-Inflammation Index (SII = PLT × N/L);
- Pan-Immune Inflammation Value (PIV = PLT × N × M/L);
- Platelet-to-Lymphocyte Ratio (PLR = PLT/L);
- Monocyte-to-Lymphocyte Ratio (MLR = M/L);
- Neutrophil-to-Lymphocyte Ratio (NLR = N/L);
- Lymphocyte-to-Monocyte Ratio (LMR = L/M).
Based on relevant literature and clinical experience, we retrospectively included the following covariates as potential confounding variables for postoperative HAEC: (1) demographic information: sex, gestational age, birth weight, feeding method and surgical age; (2) preoperative comorbidities: preoperative nutritional status, preoperative HAEC, preoperative hypoalbuminemia and associated congenital anomalies; (3) social determinants of health: residence, relationship of caregivers, educational level of caregivers and insurance type; (4) postoperative findings: pathological type of HSCR, surgical time, length of hospital stay and mild postoperative complications (grade I and II complications according to Clavien-Dindo Classification System). Among them, preoperative hypoalbuminemia was defined as serum albumin < 2.5 g/dL in infants < 7 months of age, and < 3.5 g/dL in older children. Preoperative nutritional status was assessed using height-for-age (HAZ) and weight-for-age (WAZ) z-scores; malnutrition was defined as HAZ and/or WAZ < –2, and risk of malnutrition as HAZ and/or WAZ between –2 and –1. Patients meeting neither criterion were considered normal.12
Definition of Outcome Variables
Currently, the diagnostic criteria for HAEC are not standardized. At our center, the diagnosis of suspected HAEC is primarily based on clinical symptoms. Our definition of HAEC onset is as follows: (1) vomiting or explosive diarrhea; (2) abdominal distension; (3) fever (core body temperature ≥ 38.5°C) and/or (4) leukocytosis and imaging findings. As these manifestations are consistently present across various diagnostic scoring systems, a diagnosis of HAEC was made when all four criteria were satisfied.4,14 Antibiotic therapy was routinely initiated upon clinical suspicion and diagnosis of HAEC. During postoperative follow-up, researchers systematically tracked the occurrence of HAEC according to a standardized schedule: outpatient assessments were performed at 2 weeks, 1 month, 3 months, 6 months, 1 year, and 2 years after surgery, and follow-up was conducted beyond 3 years postoperatively via telephone or regular outpatient visits. HAEC events were confirmed through systematic review of hospital readmission records, outpatient medical records, and caregiver reports obtained via standardized telephone or outpatient follow-up. All suspected HAEC events were adjudicated by two senior pediatric surgeons (Wei Feng and Yi Wang) through independent review of clinical records. Finally, events meeting the diagnostic criteria during the postoperative follow-up period of more than 3 years were recorded as the primary outcome (HAEC events were counted regardless of whether they were first or recurrent episodes).
Statistical Analysis
HSCR patients were stratified into two groups based on the occurrence of postoperative HAEC. Categorical variables were expressed as frequency and percentage (%), and comparisons of baseline characteristics between the two groups were performed using the Chi-square test. Continuous variables were first assessed for normality using the Shapiro–Wilk test: those conforming to a normal distribution were described as mean ± standard deviation, and between-group comparisons were performed using the t-test; those not conforming to a normal distribution were described as median (interquartile range), and between-group comparisons were performed using the Kruskal–Wallis test.
To explore the dynamic change trajectories of perioperative inflammatory markers (SIRI, SII, PIV, PLR, MLR, NLR, and LMR), we employed GBTM for modeling (using the traj package in STATA, version 18.0). This model aims to identify latent subgroups with similar trajectories of inflammatory marker changes. It should be noted that the aforementioned inflammatory markers exhibited a severely right-skewed distribution. To meet the basic assumptions of the GBTM model and improve the stability of model fitting, we applied a natural logarithm (ln) transformation to all inflammatory marker values. The transformed markers approximately conformed to a normal distribution and were suitable for trajectory modeling.15 Additionally, we employed GBTM to model the trajectory of WBC, neutrophils, monocytes, lymphocytes, and platelets (all demonstrating normal distribution, thus requiring no further data processing). To determine the optimal GBTM model, we sequentially fitted models with 2 to 5 trajectory groups. Simultaneously, we attempted polynomial functions of different orders (linear, quadratic, and cubic) for each trajectory group to ensure a significance level of P ≤ 0.05 for each group.16 The selection of the best trajectory model was based on a comprehensive assessment of the following criteria: (1) Bayesian Information Criterion (BIC): the model with the largest BIC value (or smallest absolute value) was selected; the Akaike Information Criterion (AIC) and log-likelihood (LL) also aided in selecting the best model, with BIC being our primary reference; (2) Average Posterior Probability (AvePP): each trajectory group required an AvePP > 0.7, with higher values indicating greater model classification accuracy; (3) Group proportion: the estimated number of individuals in each group should exceed 5% to ensure the clinical representativeness and stability of each group.17 As a retrospective cohort study, the sample size was determined by the number of eligible patients during the study period. According to the above inclusion criteria, we constructed models with either 2 or 3 trajectory groups for each inflammatory marker (Table S1).
Subsequently, using the first trajectory group of each inflammatory marker as the reference, we constructed a multivariable logistic regression model. In this process, we performed univariable logistic regression analyses on the previously mentioned covariates. Variables with a significance level of P < 0.05 in the univariable analyses were then incorporated into the multivariable logistic regression model. This was to ensure that the ratio of outcome events to covariates in the final multivariable model was no less than 10, thereby reducing the risk of overfitting while still allowing adjustment for key clinical confounders. Additionally, we conducted collinearity diagnostics for the variables in the model. A variance inflation factor (VIF) ≥ 5 was considered indicative of collinearity among variables (none was found in this study, Table S2). In the final model, we evaluated the independent predictive value of the different inflammatory marker trajectory groups for postoperative HAEC.
All statistical analyses in this study were performed using Stata 18 MP. Two-sided p-values less than 0.05 were considered statistically significant.
Results
Baseline Characteristics
A total of 400 HSCR patients meeting the inclusion/exclusion criteria were enrolled in this study (S-HSCR: 356, L-HSCR: 44), comprising 336 males and 64 females. Among them, 133 patients (33.3%) developed postoperative HAEC (Table 1). Between-group comparison of the postoperative HAEC and non-HAEC groups revealed that feeding method, surgical age, preoperative nutritional status, preoperative HAEC, preoperative hypoalbuminemia, residence, relationship of caregivers, type of HSCR, and mild postoperative complications were significantly associated with postoperative HAEC (P < 0.05). Table 2 provides detailed information on the inflammatory markers.
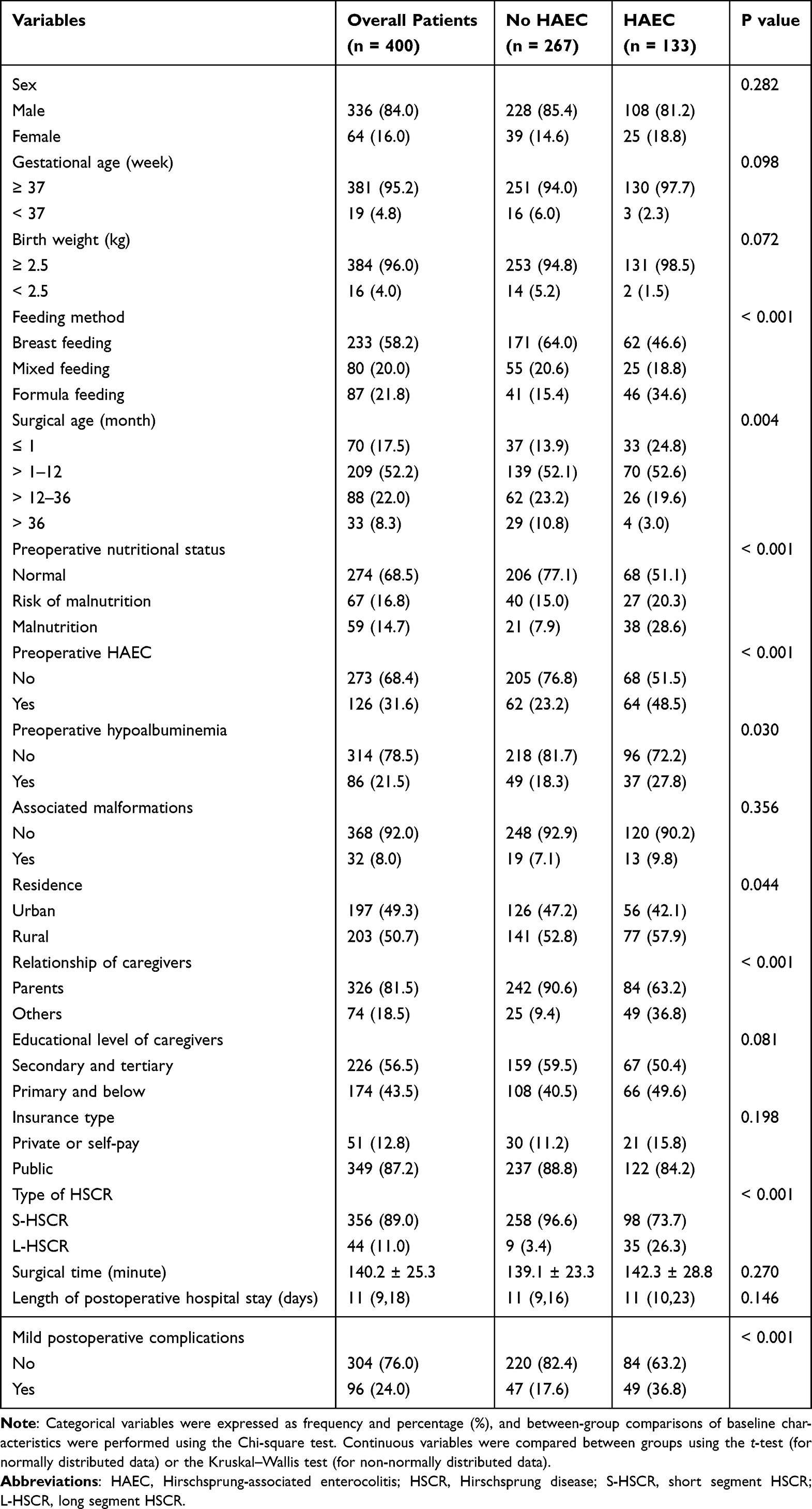 |
Table 1 Baseline Characteristics According to Postoperative HAEC Occurrence |
 |
Table 2 Distribution of Inflammatory Markers According to Postoperative HAEC Occurrence |
Univariate/Multivariate Logistic Regression Analyses of Covariate and Postoperative HAEC
Univariable logistic regression analysis revealed that risk factors for postoperative HAEC included formula feeding (OR = 3.09, 95% CI, 1.86 ~ 5.16, P < 0.001), preoperative nutritional status (malnutrition risk: OR = 2.04, 95% CI, 1.17 ~ 3.58, P = 0.012; malnutrition: OR = 5.48, 95% CI, 3.01 ~ 9.98, P < 0.001), preoperative HAEC (OR = 3.11, 95% CI, 2.00 ~ 4.85, P < 0.001), preoperative hypoalbuminemia (OR = 1.71, 95% CI, 1.05 ~ 2.80, P = 0.031), rural residents (OR = 1.54, 95% CI, 1.01 ~ 2.34, P = 0.044), non-parental care (OR = 5.65, 95% CI, 3.28 ~ 9.71, P < 0.001), L-HSCR (OR = 10.24, 95% CI, 4.75 ~ 22.08, P < 0.001) and mild postoperative complications (OR = 2.73, 95% CI, 1.70 ~ 4.38, P < 0.001). Surgical age served as a protective factor against postoperative HAEC (> 1–12 months: OR = 0.56, 95% CI, 0.33 ~ 0.98, P = 0.042; > 12–36 months: OR = 0.47, 95% CI, 0.24 ~ 0.91, P = 0.024; > 36 months: OR = 0.15, 95% CI, 0.05 ~ 0.49, P = 0.001). Inclusion of the aforementioned variables in a multivariable logistic regression model identified malnutrition (OR = 3.16, 95% CI, 1.52 ~ 6.55, P = 0.002), preoperative HAEC (OR = 2.26, 95% CI, 1.31 ~ 3.90, P = 0.003), non-parental care (OR = 4.15, 95% CI, 2.17 ~ 7.93, P < 0.001), L-HSCR (OR = 5.28, 95% CI, 2.14 ~ 13.01, P < 0.001) and mild postoperative complications (OR = 2.58, 95% CI, 1.45 ~ 4.57, P = 0.001) as independent risk factors for postoperative HAEC (Table 3).
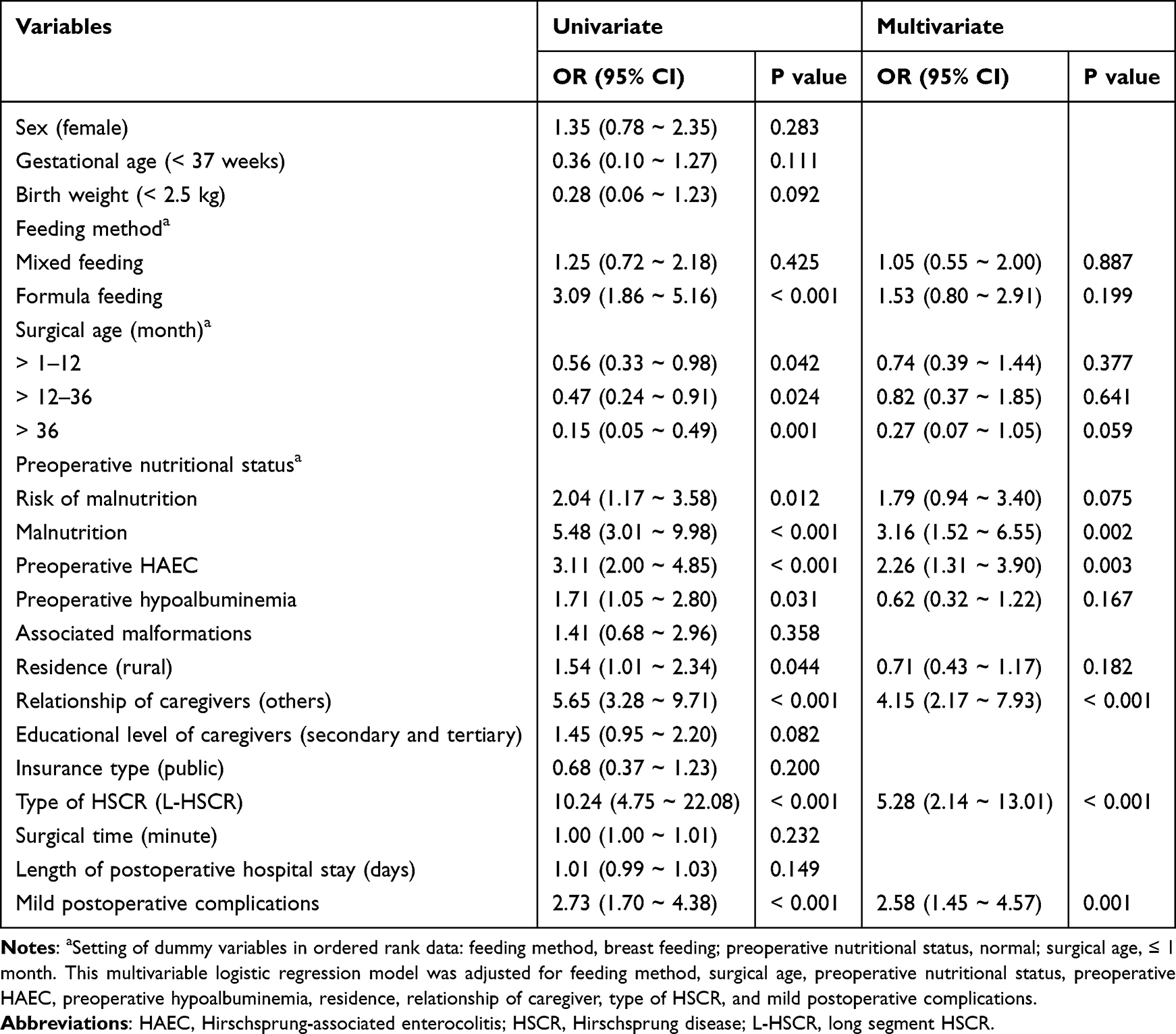 |
Table 3 Univariate/Multivariate Logistic Regression Analyses of Covariate for Postoperative HAEC |
Trajectories of Inflammatory Markers
Based on the GBTM model, we fitted perioperative change trajectories for each inflammatory marker and categorized each marker into two or three distinct trajectory groups with significant differences (Figure 2). The AvePP for each group exceeded 0.7, and the population proportion was greater than 5%, indicating the stability of the trajectory model (Table S1). For SIRI, SII, PIV, and NLR, we fitted three trajectory groups: low preoperative baseline with mild postoperative increase (trajectory group 1), moderate preoperative baseline with significant postoperative increase followed by a slow decline (trajectory group 2), and high preoperative baseline with significant postoperative increase followed by a slow decline (trajectory group 3). For PLR, MLR, LMR, monocytes, lymphocytes, and platelets, we also fitted three trajectory groups: consistently low levels (trajectory group 1), consistently moderate levels (Trajectory group 2), and consistently high levels (trajectory group 3). For WBC, we fitted two trajectory groups: consistently low levels (trajectory group 1) and consistently high levels (trajectory group 2). Finally, for neutrophils, we fitted two trajectory groups: low preoperative baseline with a mild postoperative increase followed by a slow decline (trajectory group 1) and low preoperative baseline with a significant postoperative increase followed by a rapid decline (trajectory group 2). Comparison of the inflammatory marker trajectory groups based on the occurrence of postoperative HAEC revealed that different change trajectories of SIRI, PIV, PLR, WBC, neutrophils, monocytes, and lymphocytes were significantly associated with postoperative HAEC (P < 0.05) (Table 4). Table S3 shows the univariate logistic regression analysis of inflammatory marker trajectories for postoperative HAEC.
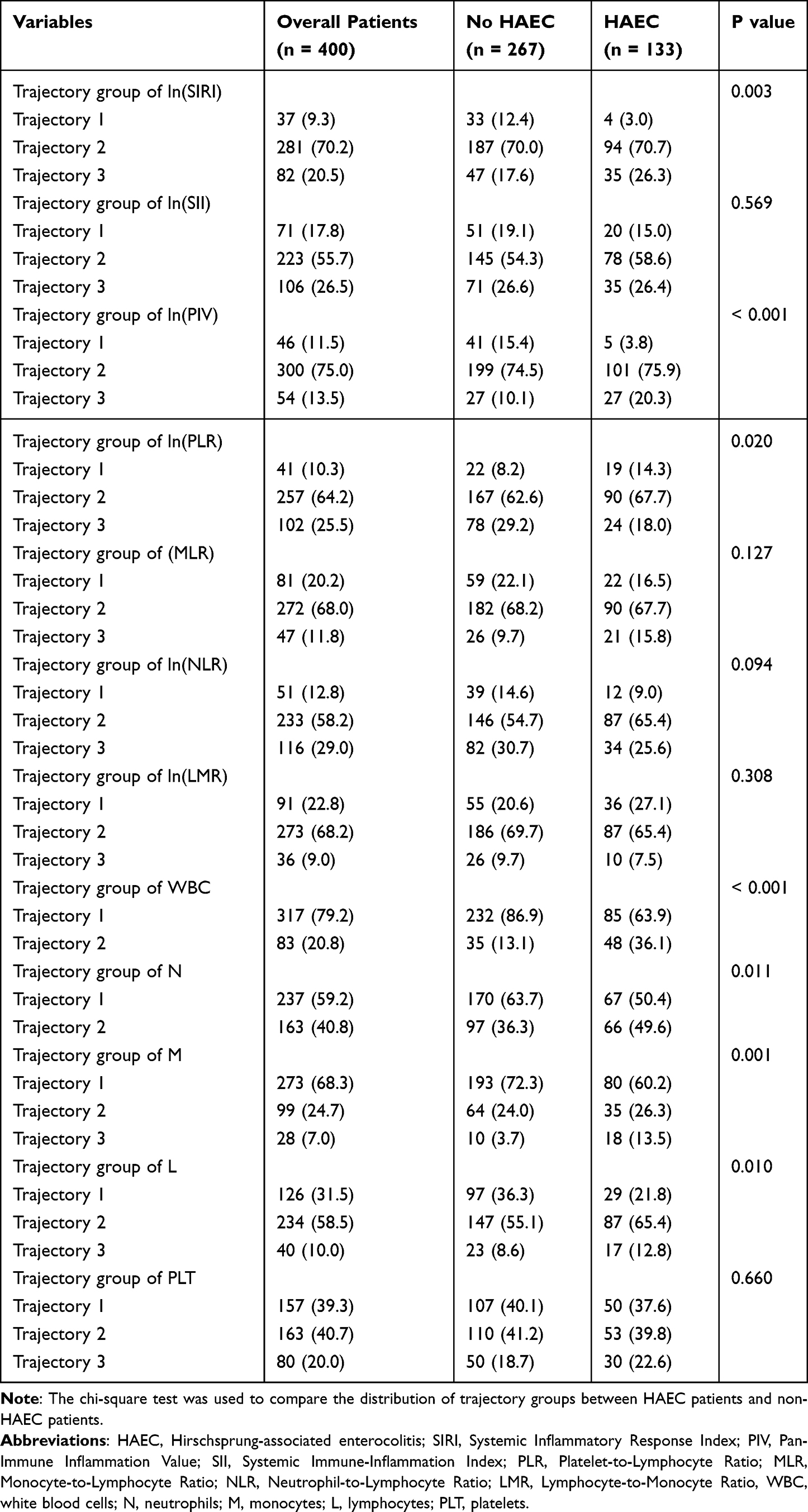 |
Table 4 Trajectory Groups of Inflammatory Markers |
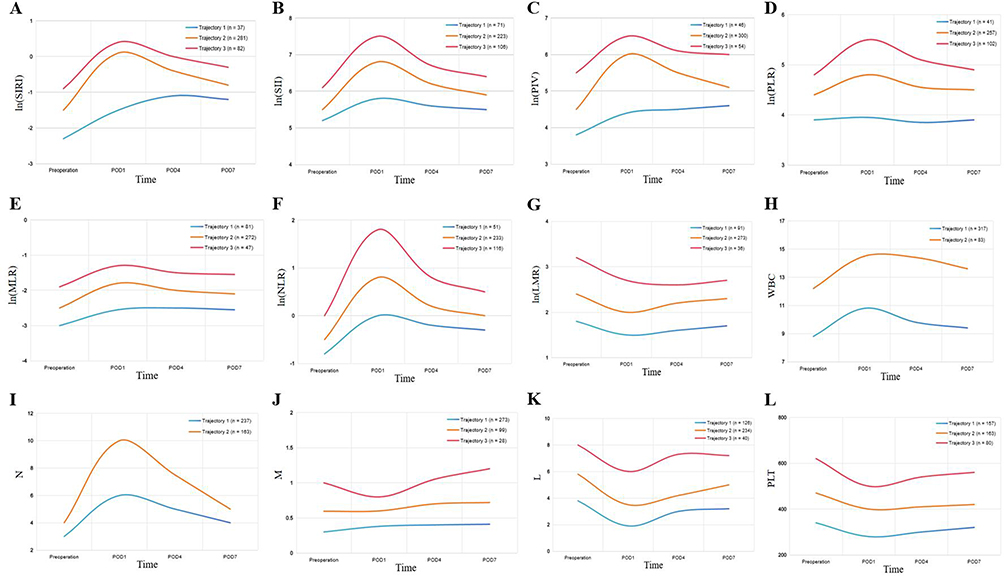 |
Figure 2 Trajectories of inflammatory markers. (A) Trajectory of ln(SIRI); (B) Trajectory of ln(SII); (C) Trajectory of ln(PIV); (D) Trajectory of ln(PLR); (E) Trajectory of ln(MLR); (F) Trajectory of ln(NLR); (G) Trajectory of ln(LMR); (H) Trajectory of WBC; (I) Trajectory of neutrophils; (J) Trajectory of monocytes; (K) Trajectory of lymphocytes; (L) Trajectory of platelets. Abbreviations: SIRI, Systemic Inflammatory Response Index; PIV, Pan-Immune Inflammation Value; SII, Systemic Immune-Inflammation Index; PLR, Platelet-to-Lymphocyte Ratio; MLR, Monocyte-to-Lymphocyte Ratio; NLR, Neutrophil-to-Lymphocyte Ratio; LMR, Lymphocyte-to-Monocyte Ratio, WBC, white blood cells; N, neutrophils; M, monocytes; L, lymphocytes; PLT, platelets. |
Multivariable Logistic Regression Analysis of Inflammatory Marker Trajectories for Postoperative HAEC
To investigate the association between different inflammatory trajectories and the risk of postoperative HAEC, we incorporated the inflammatory marker trajectory groups into a multivariable logistic regression analysis (the model was adjusted for feeding method, surgical age, preoperative nutritional status, preoperative HAEC, preoperative hypoalbuminemia, residence, relationship of caregiver, type of HSCR and mild postoperative complications). The results showed that different trajectories of SIRI, PIV, WBC, and neutrophils were independently associated with postoperative HAECFigure 3. Specifically, for SIRI, compared with trajectory group 1, trajectory group 2 (OR = 5.20, 95% CI, 1.46 ~ 18.45, P = 0.011) and trajectory group 3 (OR = 4.73, 95% CI, 1.22 ~ 18.37, P = 0.025) were associated with a significantly increased risk of postoperative HAEC. For PIV, trajectory group 2 (OR = 4.75, 95% CI, 1.54 ~ 14.63, P = 0.007) and trajectory group 3 (OR = 5.63, 95% CI, 1.56 ~ 20.26, P = 0.008) were also independently associated with a significantly increased HAEC risk. For both WBC and neutrophils, compared with trajectory group 1, trajectory group 2 (WBC: OR = 2.49, 95% CI, 1.35 ~ 4.59, P = 0.004; neutrophils: OR = 2.53, 95% CI, 1.50 ~ 4.28, P = 0.001) similarly demonstrated a significantly higher risk. The distribution of clinical characteristics based on different trajectory groups of above inflammatory markers is shown in Tables S4–S7. However, for the remaining inflammatory markers, we found no association between the trajectory groups and postoperative HAEC (P > 0.05).
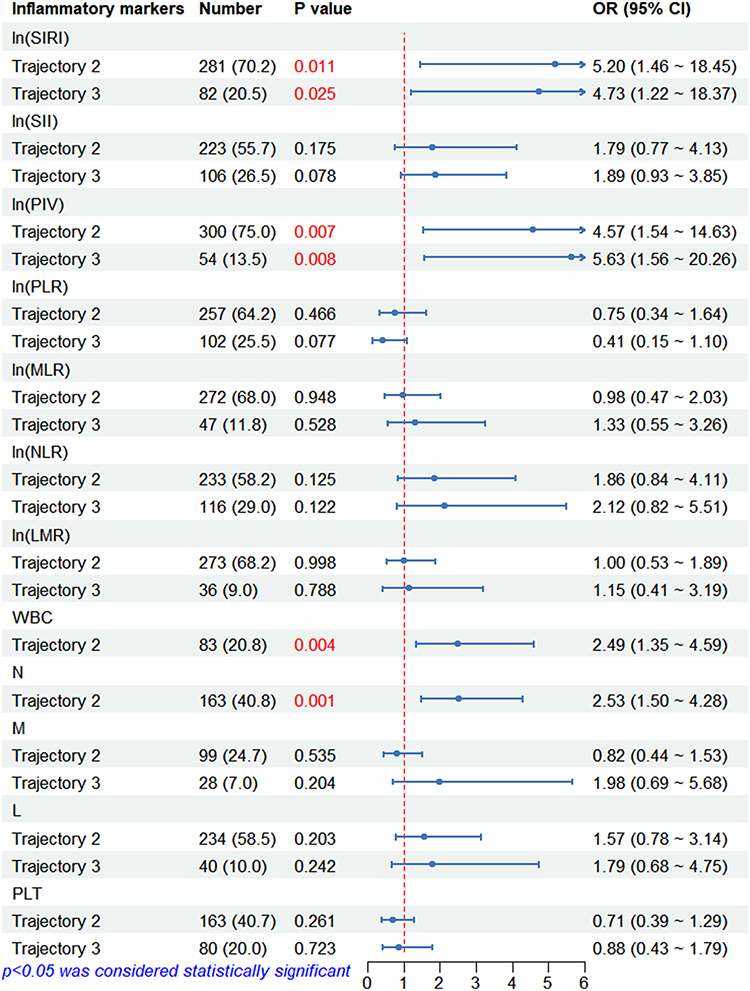 |
Figure 3 Multivariable logistic regression analysis of inflammatory marker trajectories for postoperative HAEC (this model was adjusted for feeding method, surgical age, preoperative nutritional status, preoperative HAEC, preoperative hypoalbuminemia, residence, relationship of caregiver, type of HSCR and mild postoperative complications). P values shown in red indicate statistical significance (P < 0.05). Abbreviations: N, neutrophils; M, monocytes; L, lymphocytes; PLT, platelets; OR, odds ratio. |
Discussion
HAEC is the most severe postoperative complication of HSCR. Previous studies have largely focused on the association between static patient characteristics (such as HSCR type, nutritional status, and Down syndrome) and HAEC.18,19 However, the relationship between perioperatively dynamically evolving inflammatory markers (reflecting real-time systemic inflammatory status) and the risk of HAEC has not been fully investigated.
Although studies exploring the association between inflammatory markers and HAEC are relatively scarce, such markers have demonstrated significant predictive value in the diagnosis and prognosis of pediatric surgical and gastrointestinal-related diseases. A meta-analysis involving 5974 pediatric patients evaluated the diagnostic value of NLR in acute appendicitis, indicating its favorable diagnostic performance.20 Emerging markers like PIV have also shown excellent predictive potential in acute appendicitis.21 Other studies have indicated that preoperative WBC levels are significantly correlated with the degree of postoperative pain and recovery progress in appendicitis.22 Necrotizing enterocolitis (NEC) is the most common and severe gastrointestinal emergency in newborns, sharing clinical features and pathophysiological mechanisms with HAEC.23 Research by Luo et al found that the combined detection of high-sensitivity C-reactive protein, WBC, and interleukin-6 significantly improved the accuracy of early NEC diagnosis.24 Our previous study confirmed that SII is an important marker for assessing the need for surgical intervention and predicting mortality in NEC patients.25 Furthermore, NLR and PLR have also been proven to be valuable tools for diagnosing and determining the severity of inflammatory bowel disease (IBD) in children.26 This collective evidence suggests that systemic inflammatory markers are sensitive indicators for diagnosing and reflecting the severity of gastrointestinal-related diseases. Based on this rationale, we apply this logic to the risk prediction of postoperative HAEC and introduce a dynamic evolution analytical perspective. By monitoring the sequential changes of inflammatory markers, we aim to provide novel insights for identifying patients at high risk for HAEC.
This study represents the first application of GBTM to systematically delineate the dynamic trajectories of twelve inflammatory markers during the perioperative period and to explore their associations with postoperative HAEC. We found that specific rising trajectories of SIRI, PIV, WBC, and neutrophils were independently associated with increased HAEC risk. For SIRI and PIV, both the “moderate baseline with sharp rise and slow decline” (group 2) and “high baseline with sharp rise and slow decline” (group 3) trajectories conferred significantly elevated risk compared with the “low baseline with mild rise” (group 1). For WBC and neutrophils, the higher-level trajectory groups similarly predicted greater HAEC incidence. All associations persisted after multivariable adjustment.
SIRI and PIV are two novel composite inflammatory markers whose dynamic change trajectories demonstrate excellent predictive value for postoperative HAEC. It is well established that monocytes, lymphocytes, neutrophils, and platelets are all core participants in the inflammatory response. SIRI integrates the combined information from monocytes, lymphocytes, and neutrophils, while PIV further incorporates the coordinated role of platelets on this basis. Compared to single indicators, composite indicators can more precisely capture the imbalanced state of the “inflammation-immunity-coagulation” network, which is a critical component in the pathogenesis of HAEC. Macrophages are the terminally differentiated form of monocytes within the tissue microenvironment and can polarize into different phenotypes based on microenvironmental cues: classically activated M1 and alternatively activated M2 types. In the early stages of inflammation, M1 macrophages dominate, driving the inflammatory response by releasing inflammatory mediators, while M2 macrophages promote inflammation resolution and tissue repair in later phases.27 Significant infiltration of M1 macrophages, accompanied by markedly elevated tumor necrosis factor-α (TNF-α) levels, has been observed in the proximal dilated colon of HAEC patients and in 3-week-old endothelin receptor B targeted-null mice (Ednrb–/–).28 TNF-α is a key pro-inflammatory cytokine and immunomodulator primarily produced by M1 macrophages. Zhan et al further revealed that lipopolysaccharides from V. parvula can activate M1 macrophages via the Toll-like receptor 4 (TLR4) pathway, promoting the release of inflammatory factors such as TNF-α. These inflammatory factors impair intestinal motility, exacerbate gut dysbiosis, and thereby promote the development of HAEC.29 Lymphocytes, as the core component of the immune system, mediate specific immune responses by recognizing antigens and play a crucial role in maintaining intestinal mucosal homeostasis. Keck et al found a reduced number of regulatory T cells (Treg) and an increased proportion of T helper 17 cells (Th17) in the colonic tissues of HAEC patients, and this Treg/Th17 immune imbalance was significantly associated with an increased risk of HAEC occurrence.30 Gosain et al discovered through mouse models that defective B lymphocyte maturation and reduced numbers might promote HAEC development.31 The Frykman team further supplemented that Ednrb–/– mice developing HAEC exhibited significantly reduced thymic size and T cell numbers, accompanied by suppressed B lymphocyte production, the degree of which correlated closely with HAEC severity.32 These findings suggest that reduced lymphocyte numbers or functional deficits may weaken specific intestinal immune responses, thereby increasing susceptibility to HAEC. In intestinal inflammation, platelets are not only involved in coagulation but also act as key amplifiers of the inflammatory response, exacerbating local injury through multiple pathways. Studies indicate that colonic inflammation is closely associated with reactive thrombocytosis, which increases the risk of microthrombus formation, potentially leading to intestinal mucosal microcirculatory disturbances and aggravating tissue ischemia and local damage.33 Activated platelets can bind to white blood cells, forming circulating platelet-leukocyte aggregates (PLAs), which significantly amplify inflammatory effects.34 For example, platelet binding to neutrophils enhances their superoxide production, worsening oxidative stress and tissue injury, while platelet binding to monocytes enhances their migratory capacity.35,36 Furthermore, studies have found that platelets can exacerbate intestinal inflammation by inhibiting lymphangiogenesis.37 In summary, the “inflammation-immunity-coagulation” imbalance mediated by the concerted action of these inflammatory mediators may be a key pathway driving HAEC.
Following the discussion of the synergistic roles of monocytes, lymphocytes and platelets, special attention must be given to neutrophils, the first responders in innate immunity. Neutrophil is not only a critical component in the calculation formulas for SIRI and PIV but also constitutes the predominant subset of WBC. Our study reveals that the intrinsic dynamic trajectory of neutrophils can independently predict HAEC risk, highlighting its dominant role in driving early inflammation. During the initial inflammatory phase, inflamed intestinal mucosal epithelial cells release recruitment signals, prompting neutrophils to rapidly migrate to the site of inflammation. Once recruited to the intestinal tissue, neutrophils exacerbate inflammation by releasing high levels of reactive oxygen species (ROS), cytotoxic intracellular granular contents, and neutrophil extracellular traps (NETs).38 ROS can damage cell membranes and activate redox-sensitive inflammatory pathways.39 Dysregulated NETosis further aggravates epithelial injury, disrupts the intestinal barrier, contributes to microbial imbalance, and increases thrombotic risk.40 Additionally, α-defensins and calprotectin produced by neutrophils further enhance the recruitment of neutrophils, monocytes and T cells to the inflammatory site, amplifying the immune response and causing more severe mucosal damage.41,42 However, recent research points to the dual role of neutrophils in intestinal inflammation. Although their overactivation can lead to chronic inflammation and tissue damage, they are also crucial for maintaining the intestinal barrier, host defense, and promoting inflammation resolution.43 Future fundamental research is still needed to elucidate the specific roles and regulatory mechanisms of neutrophils in HAEC. Notably, various HAEC diagnostic scoring systems incorporate elevated WBC as a diagnostic criterion. This study further confirms and extends this association, identifying persistently high perioperative WBC levels as an independent risk factor for postoperative HAEC.44,45
It is worth noting that after multivariable adjustment, the associations between trajectory groups of monocytes, lymphocytes, and PLR and the risk of HAEC were no longer statistically significant. We believe this is mainly because the information carried by these inflammatory markers is largely encompassed by the stronger clinical risk factors in the multivariable model, such as L-HSCR, preoperative HAEC, and malnutrition. These risk factors have been established as independent predictors of postoperative HAEC and may influence the postoperative systemic inflammatory response. In other words, patients with more severe baseline clinical conditions may exhibit higher or more aberrant monocyte and lymphocyte counts postoperatively. Once these clinical variables are included in the model, the independent associations between monocyte, lymphocyte, or PLR trajectories and HAEC are no longer significant. This suggests that changes in these specific markers may be an indirect reflection of the patient’s underlying disease status rather than independent drivers of HAEC. In contrast, SIRI, PIV, WBC, and neutrophils remained significant and robust predictors after equally stringent adjustment, highlighting their unique predictive ability. They appear to capture deeper signals of host inflammatory dysregulation that are not fully accounted for by the aforementioned clinical characteristics.
From a clinical translation perspective, this study represents the first application of GBTM to analyze the dynamic trajectories of inflammatory markers during the perioperative period in patients with HSCR, overcoming the limitations inherent in traditional cross-sectional studies. We systematically evaluated the predictive value of multiple novel composite inflammatory markers as well as individual inflammatory markers for postoperative HAEC, identifying that specific rising trajectories of SIRI, PIV, WBC, and neutrophils are significantly associated with an increased risk of HAEC. It is worth noting that differences between low-risk and high-risk inflammatory trajectories emerged as early as postoperative days 1–4, while the day 7 measurement remains essential for clinical discharge decisions and also helps to more completely delineate the shape of the inflammatory trajectory. Therefore, we recommend perioperative trajectory monitoring of SIRI, PIV, WBC, and neutrophils, which holds promise for the early and precise identification of patients at high risk for HAEC. Since routine postoperative blood cell counts are already completed during the standard hospital stay, this method does not add extra laboratory workload. The trajectory-based stratified management strategy enables risk-adapted interventions: for high-risk patients, health education, enhanced follow-up monitoring, or other preventive measures can be intensified; whereas low-risk patients can be managed according to the routine clinical pathway. This method can help to achieve early risk stratification and may provide a reference basis for intervention strategies targeting high-risk patients. Furthermore, this study found that preoperative malnutrition, preoperative HAEC, non-parental caregivers, L-HSCR, and mild postoperative complications were independent risk factors for postoperative HAEC. These conclusions have been confirmed in our previous studies.46
However, this study has several potential limitations. First, this study only included HSCR patients who underwent one-stage laparoscopic-assisted pull-through surgery. Due to the small sample size and inconsistent surgical strategies, especially as TCA may be more prone to postoperative HAEC, patients who underwent staged surgery were excluded.47 Second, as severe postoperative complications and Down syndrome are risk factors for HAEC, excluding these patients may have underestimated the incidence risk of HAEC.5,46 Third, GBTM is an exploratory, data-driven method, and the number and shape of the trajectory groups it identifies are influenced by the study population and data distribution. Although we strictly adhered to the selection criteria, the reproducibility of the optimal trajectories in other independent populations requires validation. Finally, given the current lack of unified diagnostic criteria for HAEC, the diagnosis in this study was based on typical clinical symptoms and objective laboratory/radiological findings (see the Methods section for details). Although these diagnostic criteria are consistent with the core components of existing scoring systems, there is a lack of standardized diagnostic protocols across different centers. This may introduce bias into the observed incidence of HAEC and limit direct comparability with other cohorts. Therefore, multicenter prospective studies using a uniform definition of HAEC are needed to further validate the generalizability of the inflammation-trajectory-based risk stratification approach proposed in this study.
Conclusion
In summary, this study through GBTM analysis identified distinct perioperative trajectories of systemic inflammatory markers in pediatric HSCR patients. Specifically, three trajectory patterns emerged for SIRI and PIV: low baseline with mild rise, moderate baseline with sharp rise and slow decline, and high baseline with sharp rise and slow decline, while WBC and neutrophils exhibited two distinct trajectories. Adverse trajectories (sharp-rise patterns for SIRI/PIV and persistently high or steep-rise patterns for WBC/neutrophils) were independently associated with the development of postoperative HAEC. This indicates that the dynamic evolution patterns of the systemic inflammatory response during the perioperative period are closely associated with the occurrence of HAEC. Monitoring the dynamic changes in perioperative inflammatory markers aids in the early identification of patients at high risk for HAEC, providing information for future research aimed at developing risk-stratified surveillance and intervention strategies.
Data Sharing Statement
Data can be made available on request to corresponding author.
Ethics Statement
This study was approved by the ethics committee of the Children’s Hospital of Chongqing Medical University (Date: 2023/No: 01). All procedures in the study were carried out in accordance with national ethical guidelines for medical and health research involving human subjects, as well as the 1964 Helsinki Declaration and its subsequent amendments. Because of the retrospective nature of the study, the need for informed consent to participate was specifically waived by the Institutional Research Ethics Board of Children’s Hospital affiliated Chongqing Medical University.
Acknowledgments
We would like to express our sincere gratitude to the National Clinical Key Specialty Construction Project.
Author Contributions
Zhengxing Jiang: Writing - original draft, Software, Methodology, Formal analysis, Conceptualization. Wei Feng: Writing - original draft, Funding acquisition, Software, Methodology. Hongtao Hu: Writing - original draft, Investigation, Data curation. Xiaoping Wei: Writing - original draft, Visualization, Investigation. Yinuo Jiang: Writing - original draft, Conceptualization. Jinping Hou: Writing - review & editing, Visualization, Investigation. Yi Wang: Writing - review & editing, Supervision, Resources, Project administration, Funding acquisition, Conceptualization. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by research grants from Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau, No.2025QNXM028), Mechanistic Study of miRNA-124-3p Regulating Enteric Nervous System Development in Anorectal Malformations via Targeting the PAX3/p53 Pathway (No.KJZD-M202500401), and Program for Youth Innovation in Future Medicine, Chongqing Medical University (No.W0125).
Disclosure
The authors declare no competing interests.
References
1. Montalva L, Cheng LS, Kapur R, et al. Hirschsprung disease. Nat Rev Dis Primers. 2023;9(1):54. doi:10.1038/s41572-023-00465-y
2. El-Sawaf M, Siddiqui S, Mahmoud M, Drongowski R, Teitelbaum DH. Probiotic prophylaxis after pullthrough for Hirschsprung disease to reduce incidence of enterocolitis: a prospective, randomized, double-blind, placebo-controlled, multicenter trial. J Pediatr Surg. 2013;48(1):111–17. doi:10.1016/j.jpedsurg.2012.10.028
3. Mei F, Wu M, Zhao L, et al. Probiotics for the prevention of Hirschsprung-associated enterocolitis. Cochrane Database Syst Rev. 2022;4(4):CD13714. doi:10.1002/14651858.CD013714.pub2
4. Gosain A, Frykman PK, Cowles RA, et al. Guidelines for the diagnosis and management of Hirschsprung-associated enterocolitis. Pediatr Surg Int. 2017;33(5):517–521. doi:10.1007/s00383-017-4065-8
5. Zhang X, Sun D, Xu Q, et al. Risk factors for Hirschsprung disease-associated enterocolitis: a systematic review and meta-analysis. Int J Surg. 2023;109(8):2509–2524. doi:10.1097/JS9.0000000000000473
6. Li S, Zhang Y, Li K, et al. Update on the pathogenesis of the Hirschsprung-associated enterocolitis. Int J Mol Sci. 2023;24(5). doi:10.3390/ijms24054602
7. Shen Q, Sun Z, Xu Y, Hu Q, Zhang W, Huang S. Associations between complete-blood-count-derived inflammatory markers and gastric ulcer: a cross-sectional study. World J Gastroenterol. 2025;31(38):111298. doi:10.3748/wjg.v31.i38.111298
8. Zheng H, Wu K, Zheng H, et al. High systemic inflammation response index and increased cardiovascular risk and mortality in MASLD: a prospective cohort study. JHEP Rep. 2025;7(12):101602. doi:10.1016/j.jhepr.2025.101602
9. Kishimoto M, Koinuma M, Tokunaga J. Exploratory investigation of predictive factors for reducing adverse effects in CapeOX therapy for colorectal cancer patients. Cureus. 2025;17(10):e95702. doi:10.7759/cureus.95702
10. Bayram S, Alemdar MS, Tatli AM, Ozdogan M. Predictive value of tumor marker index for pathological complete response following neoadjuvant chemoradiotherapy in locally advanced rectal cancer. World J Surg Oncol. 2025;24(1). doi:10.1186/s12957-025-04081-w
11. Jha RM, Elmer J, Zusman BE, et al. Intracranial pressure trajectories: a novel approach to informing severe traumatic brain injury phenotypes. Crit Care Med. 2018;46(11):1792–1802. doi:10.1097/CCM.0000000000003361
12. Jiang Z, Hou J, Die X, et al. The association between short-term postoperative complications and bowel function after surgery for Hirschsprung disease. BMC Pediatr. 2025;25(1):514. doi:10.1186/s12887-025-05861-9
13. Feng W, Liu Y, Die X, et al. Sex differences in postoperative outcomes of hirschsprung disease: propensity score matching analysis. J Pediatr Surg. 2025;60(12):162655. doi:10.1016/j.jpedsurg.2025.162655
14. Frykman PK, Kim S, Wester T, et al. Critical evaluation of the Hirschsprung-associated enterocolitis (HAEC) score: a multicenter study of 116 children with Hirschsprung disease. J Pediatr Surg. 2018;53(4):708–717. doi:10.1016/j.jpedsurg.2017.07.009
15. Tang Z, Liao C, Zhuang Z, Xu Z, Liu M, Xu H. Trajectories of systemic immune inflammation index and mortality risk in patients with moderate-to-severe traumatic brain injury: a retrospective cohort study. Front Neurol. 2024;15:1439318. doi:10.3389/fneur.2024.1439318
16. Herle M, Micali N, Abdulkadir M, et al. Identifying typical trajectories in longitudinal data: modelling strategies and interpretations. Eur J Epidemiol. 2020;35(3):205–222. doi:10.1007/s10654-020-00615-6
17. Li X, Sun L, He Y, et al. HDL-C as a novel predictor of immune reconstitution in people living with HIV: insights from a baseline-to-dynamic change cohort study in China, 2005–2022. Front Immunol. 2025;16:1520615. doi:10.3389/fimmu.2025.1520615
18. Yulianda D, Sati AI, Makhmudi A. Risk factors of preoperative Hirschsprung-associated enterocolitis. BMC Proc. 2019;13(Suppl 11):18. doi:10.1186/s12919-019-0172-y
19. Taylor MA, Bucher BT, Reeder RW, et al. Comparison of Hirschsprung disease characteristics between those with a history of postoperative enterocolitis and those without: results from the pediatric colorectal and pelvic learning consortium. Eur J Pediatr Surg. 2021;31(3):207–213. doi:10.1055/s-0040-1716876
20. Eun S, Ho IG, Bae GE, et al. Neutrophil-to-lymphocyte ratio for the diagnosis of pediatric acute appendicitis: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2021;25(22):7097–7107. doi:10.26355/eurrev_202111_27263
21. Çoşkun N, Metin M, Doğan G, Ipek H, Demir E, Afşarlar ÇE. PAN-Immune inflammation value: a new biomarker for diagnosing appendicitis in children? BMC Pediatr. 2025;25(1):165. doi:10.1186/s12887-025-05544-5
22. Li X, Gong S, Ding Y, Chen Y, Yu Z. Preoperative inflammatory markers in pediatric appendicitis: associations with disease severity, postoperative recovery, pain, and surgical outcomes. BMC Pediatr. 2025;25(1):597. doi:10.1186/s12887-025-05941-w
23. Roberts AG, Younge N, Greenberg RG. Neonatal necrotizing enterocolitis: an update on pathophysiology, treatment, and prevention. Paediatr Drugs. 2024;26(3):259–275. doi:10.1007/s40272-024-00626-w
24. Luo R, Zhang J, Li X, Peng F, Zhang A, Zhang P. Adoption value of serum hematological inflammatory markers in early diagnosis of necrotising enterocolitis. J Med Biochem. 2025;44(2):244–249. doi:10.5937/jomb2502244L
25. Feng W, Hou J, Xiang C, et al. Correlation of systemic immune-inflammation Index with surgical necrotizing enterocolitis. Front Pediatr. 2022;10:1044449. doi:10.3389/fped.2022.1044449
26. Zahmatkesh A, Sohouli MH, Hosseini SME, Rohani P. The role of platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in the diagnosis and severity of inflammatory bowel disease in children. Eur J Pediatr. 2023;182(9):4263–4270. doi:10.1007/s00431-023-05110-0
27. Murray PJ. Macrophage Polarization. Annu Rev Physiol. 2017;79:541–566. doi:10.1146/annurev-physiol-022516-034339
28. Chen X, Meng X, Zhang H, et al. Intestinal proinflammatory macrophages induce a phenotypic switch in interstitial cells of Cajal. J Clin Invest. 2020;130(12):6443–6456. doi:10.1172/JCI126584
29. Zhan Z, Liu W, Pan L, Bao Y, Yan Z, Hong L. Overabundance of Veillonella parvula promotes intestinal inflammation by activating macrophages via LPS-TLR4 pathway. Cell Death Discov. 2022;8(1):251. doi:10.1038/s41420-022-01015-3
30. Keck S, Galati-Fournier V, Kym U, et al. Lack of mucosal cholinergic innervation is associated with increased risk of enterocolitis in Hirschsprung’s disease. Cell Mol Gastroenterol Hepatol. 2021;12(2):507–545. doi:10.1016/j.jcmgh.2021.03.004
31. Gosain A, Barlow-Anacker AJ, Erickson CS, et al. Impaired cellular immunity in the murine neural crest conditional deletion of endothelin receptor-B model of Hirschsprung’s disease. PLoS One. 2015;10(6):e128822. doi:10.1371/journal.pone.0128822
32. Frykman PK, Cheng Z, Wang X, Dhall D. Enterocolitis causes profound lymphoid depletion in endothelin receptor B- and endothelin 3-null mouse models of Hirschsprung-associated enterocolitis. Eur J Immunol. 2015;45(3):807–817. doi:10.1002/eji.201444737
33. Heits F, Stahl M, Ludwig D, Stange EF, Jelkmann W. Elevated serum thrombopoietin and interleukin-6 concentrations in thrombocytosis associated with inflammatory bowel disease. J Interferon Cytokine Res. 1999;19(7):757–760. doi:10.1089/107999099313604
34. Yan SLS, Russell J, Harris NR, Senchenkova EY, Yildirim A, Granger DN. Platelet abnormalities during colonic inflammation. Inflamm Bowel Dis. 2013;19(6):1245–1253. doi:10.1097/MIB.0b013e318281f3df
35. Polanowska-Grabowska R, Wallace K, Field JJ, et al. P-selectin-mediated platelet-neutrophil aggregate formation activates neutrophils in mouse and human sickle cell disease. Arterioscler Thromb Vasc Biol. 2010;30(12):2392–2399. doi:10.1161/ATVBAHA.110.211615
36. Huo Y, Schober A, Forlow SB, et al. Circulating activated platelets exacerbate atherosclerosis in mice deficient in apolipoprotein E. Nat Med. 2003;9(1):61–67. doi:10.1038/nm810
37. Sato H, Higashiyama M, Hozumi H, et al. Platelet interaction with lymphatics aggravates intestinal inflammation by suppressing lymphangiogenesis. Am J Physiol Gastrointest Liver Physiol. 2016;311(2):G276–G285. doi:10.1152/ajpgi.00455.2015
38. Kang L, Fang X, Song Y, et al. Neutrophil-epithelial crosstalk during intestinal inflammation. Cell Mol Gastroenterol Hepatol. 2022;14(6):1257–1267. doi:10.1016/j.jcmgh.2022.09.002
39. Denson LA, Jurickova I, Karns R, et al. Clinical and genomic correlates of neutrophil reactive oxygen species production in pediatric patients with Crohn’s disease. Gastroenterology. 2018;154(8):2097–2110. doi:10.1053/j.gastro.2018.02.016
40. Ortega-Zapero M, Gomez-Bris R, Pascual-Laguna I, Saez A, Gonzalez-Granado JM. Neutrophils and NETs in pathophysiology and treatment of inflammatory bowel disease. Int J Mol Sci. 2025;26(15):7098. doi:10.3390/ijms26157098
41. Yang D, Chen Q, Chertov O, Oppenheim JJ. Human neutrophil defensins selectively chemoattract naive T and immature dendritic cells. J Leukoc Biol. 2000;68(1):9–14. doi:10.1189/jlb.68.1.9
42. Wang S, Song R, Wang Z, Jing Z, Wang S, Ma J. S100A8/A9 in inflammation. Front Immunol. 2018;9:1298. doi:10.3389/fimmu.2018.01298
43. Danne C, Skerniskyte J, Marteyn B, Sokol H. Neutrophils: from IBD to the gut microbiota. Nat Rev Gastroenterol Hepatol. 2024;21(3):184–197. doi:10.1038/s41575-023-00871-3
44. Pastor AC, Osman F, Teitelbaum DH, Caty MG, Langer JC. Development of a standardized definition for Hirschsprung’s-associated enterocolitis: a Delphi analysis. J Pediatr Surg. 2009;44(1):251–256. doi:10.1016/j.jpedsurg.2008.10.052
45. Lewit RA, Veras LV, Cowles RA, et al. Reducing underdiagnosis of Hirschsprung-associated enterocolitis: a novel scoring system. J Surg Res. 2021;261:253–260. doi:10.1016/j.jss.2020.12.030
46. Feng W, Zhang B, Fan L, et al. Clinical characteristics and influence of postoperative Hirschsprung-associated enterocolitis: retrospective study at a tertiary children’s hospital. Pediatr Surg Int. 2024;40(1):106. doi:10.1007/s00383-024-05688-y
47. Chantakhow S, Tepmalai K, Tantraworasin A, Khorana J. Development of prediction model for Hirschsprung-Associated Enterocolitis (HAEC) in postoperative Hirschsprung patients. J Pediatr Surg. 2024;59(12):161696. doi:10.1016/j.jpedsurg.2024.161696
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.