Back to Journals » International Journal of Women's Health » Volume 17
Association Between Oxidative Balance Score and Gynecological Cancer Using NHANES 2011–2018 Data
Received 17 July 2025
Accepted for publication 6 November 2025
Published 3 December 2025 Volume 2025:17 Pages 5129—5139
DOI https://doi.org/10.2147/IJWH.S554574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yu’ e Yang,1 Chunfang Ha2
1The First Clinical Medical College of Ningxia Medical University, Yinchuan, Ningxia Hui Autonomous Region 750000 People’s Republic of China; 2General Hospital of Ningxia Medical University, Yinchuan, Ningxia Hui Autonomous Region 750000 People’s Republic of China
Correspondence: Chunfang Ha, General Hospital of Ningxia Medical University, 804 Shengli Street, Xingqing District, Yinchuan, Ningxia Hui Autonomous Region, 750000, People’s Republic of China, Email [email protected]
Background: Oxidative stress has been implicated in the pathogenesis of various malignancies, including gynecological cancers (GC). This study aimed to evaluate the association between oxidative balance score (OBS) and GC prevalence using data from the National Health and Nutrition Examination Survey (NHANES) 2011– 2018.
Methods: A total of 7816 adult female participants were included, of whom 195 reported a history of GC (cervical, endometrial, or ovarian). OBS was computed from 20 components: 15 antioxidants and five pro-oxidants from dietary and lifestyle sources. Multivariable logistic regression models were used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for GC according to the OBS tertiles and per-unit increases, adjusting for covariates.
Results: Higher total OBS was associated with significantly lower odds of GC (adjusted OR per unit increase = 0.92; 95% CI: 0.86– 0.97). Participants in the highest OBS tertile had 34% lower odds of developing GC than those in the lowest tertile. This association was more pronounced among women aged ≥ 60 years, non-smokers, and those with normal body mass index (BMI).
Conclusion: Greater antioxidant exposure, as reflected by higher OBS, was inversely associated with GC risk. These findings support dietary and lifestyle interventions aimed at improving oxidative balance.
Keywords: oxidative stress, gynecologic neoplasms, diet, lifestyle, antioxidants
Introduction
Gynecological cancers (GC), including malignancies of the cervix, endometrium (uterus), and ovaries, impose a substantial global health burden.1 These cancers account for approximately 40% of cancer cases and 30% of cancer-related deaths among women worldwide.1 For example, in 2020, cervical cancer alone caused an estimated 0.6 million new cases and 342,000 deaths globally.2 Ovarian cancer similarly imposed a heavy burden (314,000 new cases in 2020),3 and uterine (endometrial) cancer ranks among the most common female cancers.3
Human papillomavirus (HPV) infection is widely recognized as the principal etiologic factor in cervical carcinogenesis.4 Hormonal factors play a substantial role in the risk of gynecologic cancers, particularly endometrial and ovarian malignancies.5 In addition to HPV infection and hormonal factors, growing evidence implicates the microbiota of the female reproductive tract and gut in the etiology and progression of gynecologic cancers. Microbial dysbiosis may influence carcinogenesis via immune modulation, chronic inflammation, altered estrogen metabolism, and effects on the tumor microenvironment.6 For example, a disrupted vaginal microbiome has been associated with HPV persistence and cervical neoplasia, while uterine and gut microbial profiles have also been linked to endometrial and ovarian tumorigenesis.7
Despite advances in screening, vaccination (for HPV), and treatment, the incidence and mortality rates of these diseases remain high or are increasing in some populations. A key contributor is that many cases are diagnosed at advanced stages when tumors are more aggressive or disseminated. Moreover, resistance to standard treatments (eg chemotherapy or radiotherapy) frequently develops during the disease course, partly mediated by dysregulation in signaling pathways such as the Nuclear Factor Erythroid 2-Related Factor 2 (NRF2)/Kelch Like ECH Associated Protein 1 (KEAP1) (NRF2/KEAP1) axis.8 The large and growing incidence of cervical, endometrial, and ovarian cancers underscores the urgent need to identify modifiable risk factors that could reduce cancer burden.9
Oxidative stress is a state in which pro-oxidant forces (eg, reactive oxygen species, ROS) overwhelm antioxidant defenses, leading to damage to DNA, lipids, and proteins.10 Chronic oxidative damage can activate inflammatory and oncogenic pathways that link persistent oxidative stress to cancer initiation and progression.11 The Oxidative Balance Score (OBS) is a composite index that quantifies an individual’s net exposure to pro-oxidant and antioxidant factors.12,13 OBS is calculated by combining multiple dietary nutrients and lifestyle factors into a single score, with higher OBS values reflecting relatively greater antioxidant exposure.12,13 Previous epidemiological studies have found inverse associations between a higher OBS and the risk of several common cancers. In a recent meta-analysis of observational studies, individuals with higher OBS had significantly lower odds of colorectal, breast, prostate, and gastric cancers (pooled odds ratio roughly 0.3–0.7, for highest versus lowest OBS).14 These findings suggest biological plausibility for cancer prevention: maintaining a more favorable oxidative balance through diet and lifestyle may reduce the risk of malignancy. However, to date, no large population-based study has examined OBS in relation to GC (cervical, endometrial, or ovarian). However, the potential link between oxidative balance and female-specific cancers remains unclear.
To address this gap, we used data from the 2011 to 2018 National Health and Nutrition Examination Survey (NHANES) cycles 2011–2018. The NHANES is a nationwide, cross-sectional survey designed to evaluate the health and nutritional status of the US population. In summary, the present study aimed to determine whether a higher (more antioxidant‐favorable) oxidative balance score is associated with a reduced prevalence of GC among women in the NHANES 2011–2018 data. We will compute a composite OBS from dietary nutrient intake and lifestyle factors (smoking, alcohol use, body mass index, etc.) and assess its relationship with self‐reported cervical, endometrial, and ovarian cancers. This analysis will fill an important knowledge gap by providing the first large-scale population-based assessment of the relationship between oxidative balance and GC risk.
Methods
Study Design and Population
This cross-sectional study utilized data from the NHANES, a continuous, nationally representative survey of the non-institutionalized US population. We analyzed combined data from four NHANES cycles: 2011–2012, 2013–2014, 2015–2016, and 2017–2018. The NHANES employs a complex, multistage probability sampling design to ensure national representation, including the oversampling of certain population subgroups (https://wwwn.cdc.gov/nchs/nhanes).
The present analysis included female participants aged ≥ 20 years with complete data on dietary intake, lifestyle behaviors, and a self-reported history of GC. Participants were excluded if they (1) were pregnant at the time of the survey, (2) had missing or unreliable dietary recall data, or (3) lacked complete information regarding the key variables used to compute the OBS or covariates.
NHANES protocols were approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board. Written informed consent was obtained from all the participants.15 This study used publicly available, de-identified data and was deemed exempt from institutional review board supervision.
Outcome Ascertainment
History of GC was ascertained through self-reported responses to the question, “Have you ever been told by a doctor or other health professional that you had cancer or a malignancy of any kind?” Participants who responded “yes” were asked to specify the type(s) of cancer. Women who reported cervical, uterine (endometrial), or ovarian cancers were classified as having GC. All other female respondents, including those without a history of cancer and those reporting other types of cancer, were categorized as non-GC participants.
Oxidative Balance Score
The OBS was constructed based on 20 components, including 16 dietary nutrients and 4 lifestyle factors, adapted from previously validated methods with modifications specific to the NHANES dataset.16 Pro-oxidants (n = 5) included smoking status, alcohol consumption, body mass index (BMI), total dietary fat, and total iron intake. Antioxidants (n = 15) included dietary fiber, selenium, copper, zinc, magnesium, calcium, vitamin E, vitamin C, vitamin B12, total folate, vitamin B6, niacin, riboflavin, beta-carotene, and vitamin A (retinol activity equivalents). All dietary components were derived from the average of two 24-hour dietary recalls and adjusted for total energy intake using the residual method. Smoking, alcohol consumption, BMI, and physical activity were assessed using NHANES questionnaire data and laboratory values, where applicable.
Each dietary and lifestyle variable was categorized into tertiles based on its distribution among women in the analytic sample. For antioxidant components, participants in the lowest tertile received a score of 0, those in the middle tertile received a score of 1, and those in the highest tertile received a score of 2. For the pro-oxidant components, the scoring was reversed; participants in the highest tertile received a score of 0, the middle tertile received 1 point, and the lowest tertile received 2 points. Alcohol consumption was categorized according to the sex-specific thresholds used in previous studies. For women, non-drinkers were assigned 2 points, moderate drinkers (0–15 g/day) received 1 point, and heavy drinkers (≥15 g/day) received 0 point. Smoking status was determined using a combination of self-reported data and serum cotinine levels. Never smokers or those with cotinine levels <1 ng/mL were assigned 2 points; former smokers or those with levels between 1 and 10 ng/mL received 1 point; and current smokers or those with cotinine levels ≥10 ng/mL were assigned 0 points. BMI was categorized using standard WHO classifications: normal weight (<25 kg/m2) received 2 points, overweight (25–29.9 kg/m2) received 1 point, and obesity (≥30 kg/m2) received 0 points. Physical activity was included as a lifestyle factor influencing oxidative status and was scored based on the total weekly metabolic equivalent (MET) minutes. Participants in the highest quartile received 2 points, those in the middle 50% received 1 point, and those in the lowest quartile received 0 points.
The total OBS score was calculated by summing the scores for all individual components, resulting in a possible range of 0 (maximum pro-oxidant exposure) to 40 (maximum antioxidant exposure). For categorical analyses, OBS was divided into tertiles: Q1 (low OBS) was defined as a score of less than 16, Q2 (moderate OBS) as a score between 16 and 23, and Q3 (high OBS) as a score of 24 or higher. These cut-off points were derived from the tertile distribution of OBS in the combined female NHANES sample from 2011 to 2018.16
Covariates
Potential confounders included age (years), race/ethnicity (non-Hispanic white, non-Hispanic Black, Hispanic, and others), poverty-income ratio (PIR), educational attainment, marital status, health insurance coverage, hypertension (yes/no), diabetes (yes/no), and total energy intake (kcal/day). All covariates were self-reported or measured using standardized NHANES procedures.
Statistical Analysis
Survey weights, strata, and primary sampling units were applied to account for the NHANES complex sampling design, thereby enabling nationally representative estimates. Descriptive statistics were used to compare baseline characteristics between participants with and without GC using chi-square tests for categorical variables and t-tests or Wilcoxon rank-sum tests for continuous variables. Multivariable logistic regression models were used to estimate the association between OBS (continuous and tertiles) and the odds of GC. The models were adjusted progressively: model 1 was unadjusted; model 2 was adjusted for age, race/ethnicity, and PIR; and model 3 was further adjusted for education, marital status, hypertension, diabetes, and total energy intake. Trend tests were conducted across tertiles by modeling the median value of each tertile as a continuous variable. Subgroup analyses were stratified by age (<60 vs ≥60 years), smoking status, diabetes status, and BMI category (<25 vs ≥25 kg/m2), and the interaction terms were tested. All analyses were performed using Stata version 17.0 (StataCorp LLC, College Station, TX, USA), with statistical significance set at p < 0.05.
Results
Baseline Characteristics of Participants
Baseline characteristics of the study participants are presented in Table 1. A total of 7816 female participants with a mean age of 46.1 years (SD: 15.8). Among them, 195 women were identified as having a history of GC, including cervical, endometrial, and ovarian cancers, whereas the remaining 7621 participants did not report any cancer diagnosis. Statistically significant differences were observed between the two groups in terms of age, PIR, ethnicity, and smoking status (p < 0.05). Additionally, the prevalence of hypertension was markedly higher among GC participants compared to those without (52.3% vs 30.0%).
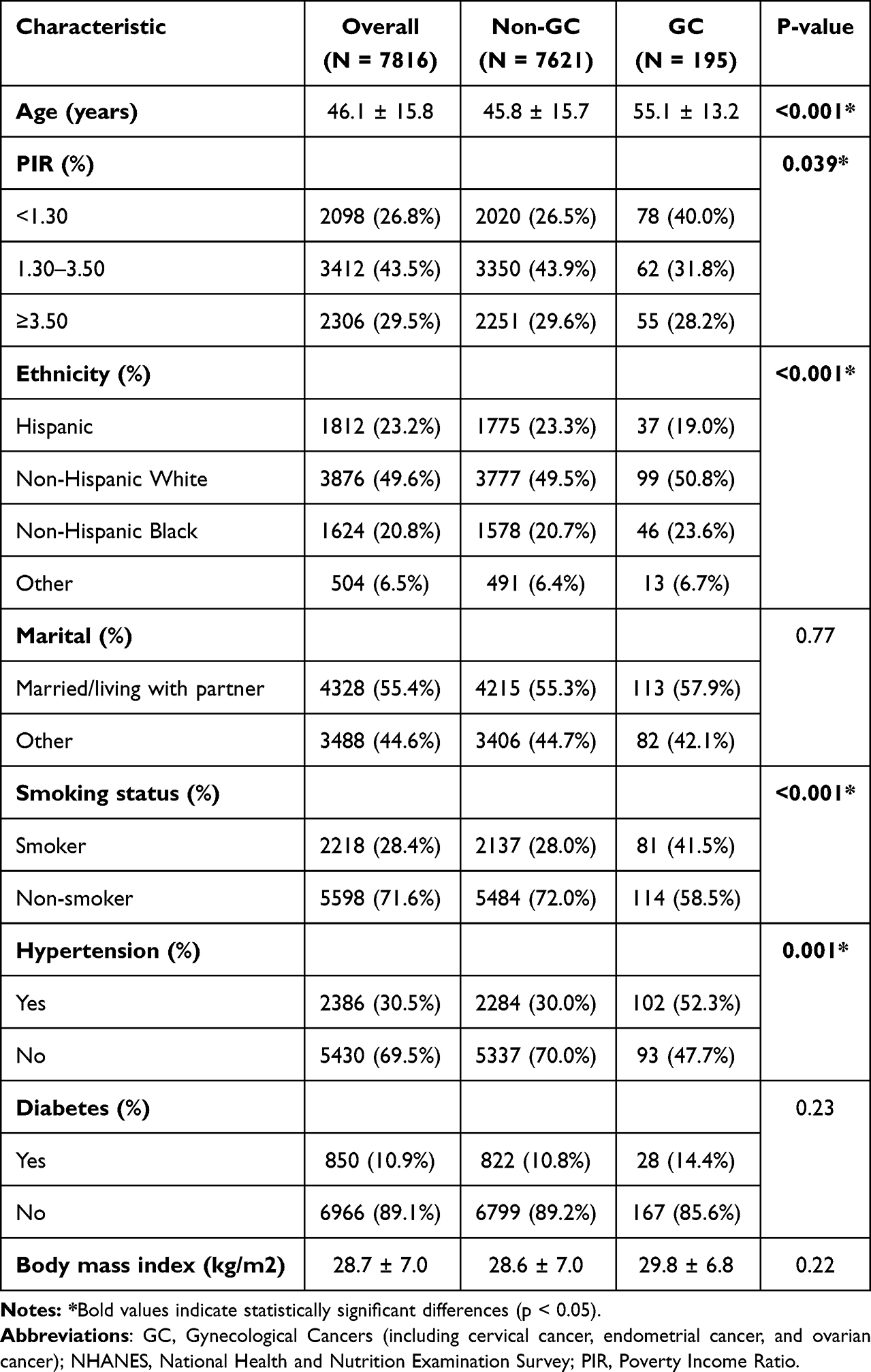 |
Table 1 Characteristics of the Study Participants, NHANES (2011–2018) |
Dietary Characteristics of Participants
As shown in Table 2, mean total OBS and both its dietary and lifestyle components were significantly lower in the GC group compared to non-GC participants (Total OBS: 16.8 ± 5.1 vs 18.4 ± 5.0; Dietary OBS: 10.4 ± 3.4 vs 11.2 ± 3.6; Lifestyle OBS: 6.3 ± 2.5 vs 7.2 ± 2.4). Among dietary components, women with GC had significantly lower intakes of dietary fiber, niacin, vitamin B6, folate, zinc, and several antioxidants, including vitamin E, selenium, and iron. Physical activity levels were lower (1950 ± 1080 vs 2320 ± 1020), and cotinine levels was higher (36.8 ± 16.8 vs 29.5 ± 14.5) among GC participants.
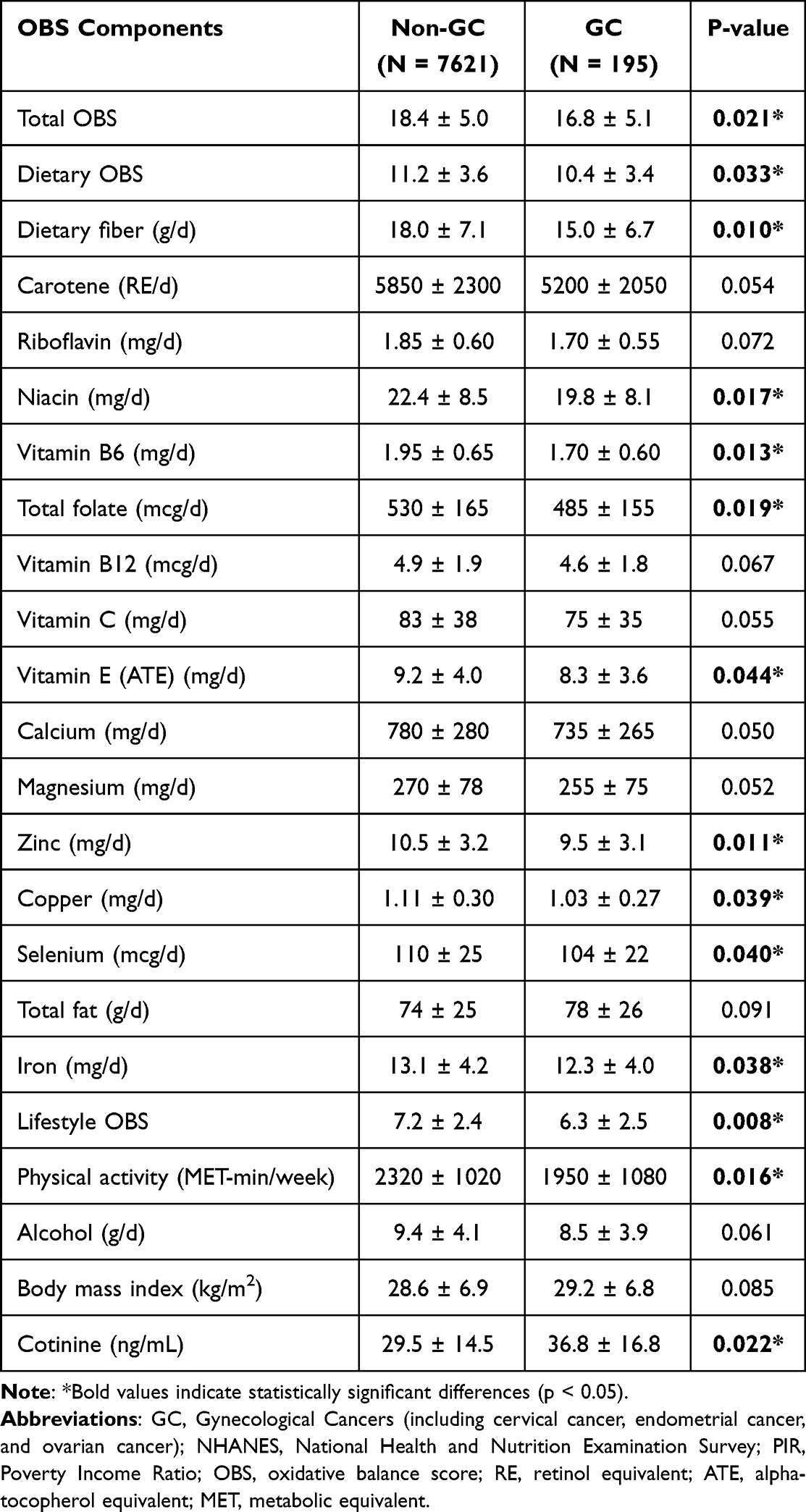 |
Table 2 Comparison of OBS and Its Component Scores Between Gynecological Cancer and Control Groups, NHANES (2011–2018) |
Association Between OBS and GC
Table 3 shows the association between OBS and GC. In the fully adjusted models, a one-unit increase in total OBS was associated with 8% lower odds of GC (odds ratio (OR) = 0.92; 95% confidence interval (CI): 0.86–0.97). Compared to the lowest tertile, participants in the highest tertile of total OBS had significantly reduced odds of GC (OR = 0.66; 95% CI: 0.47–0.93). Although the association with dietary OBS was modest and borderline significant in the highest tertile (OR = 0.77; 95% CI: 0.55–1.09), lifestyle OBS showed a stronger and independent inverse association with GC (OR per unit increase = 0.89; 95% CI: 0.83–0.96; highest vs lowest tertile OR = 0.64; 95% CI: 0.45–0.92).
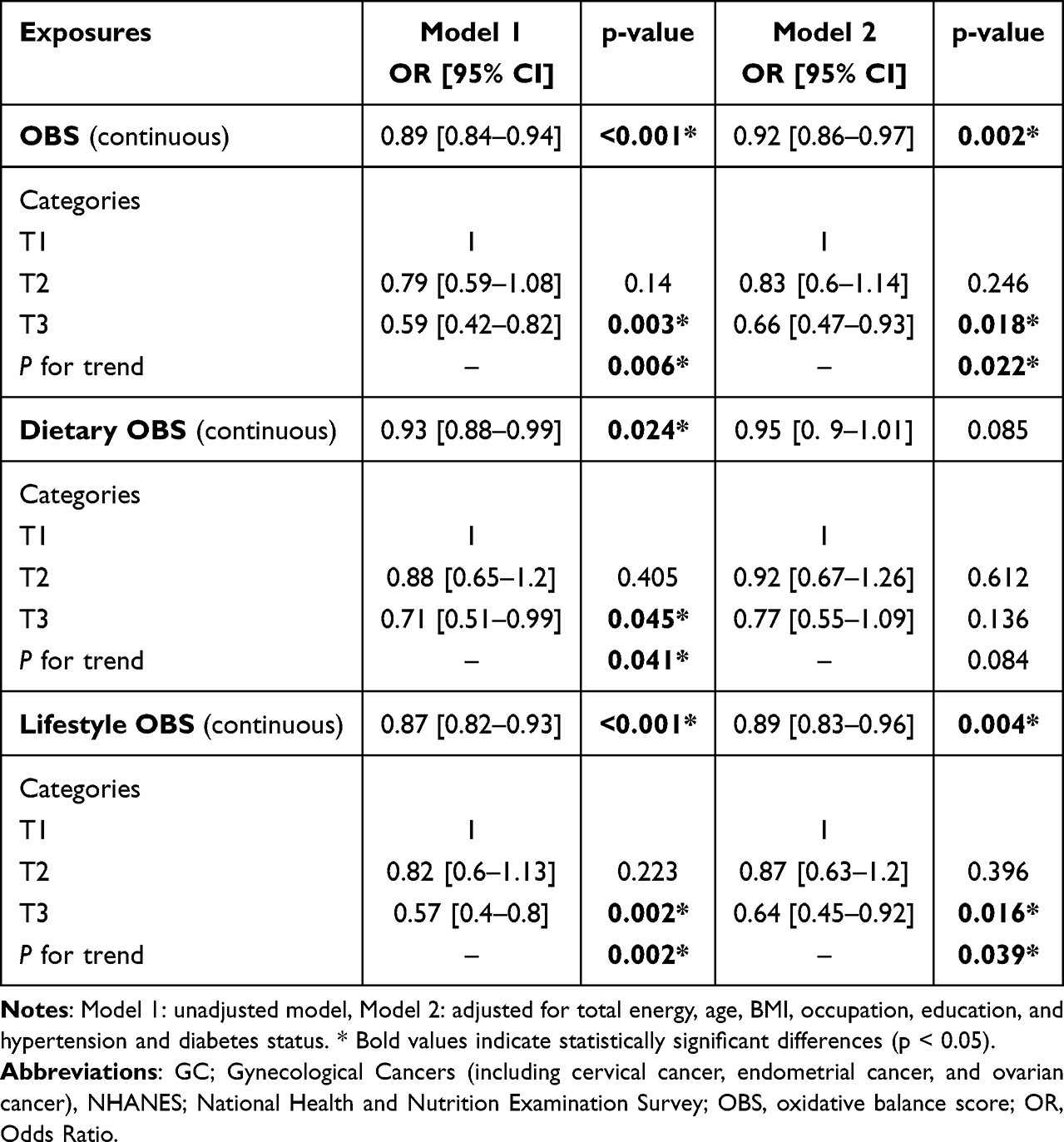 |
Table 3 The Association Between Tertiles of OBS Components and Gynecological Cancer (Odds Ratio and 95% Confidence Interval) |
Subgroup Analysis
Subgroup analysis revealed (Table 4) that the inverse association between total OBS and GC was more pronounced among women aged ≥60 years (OR = 0.60; 95% CI: 0.41–0.89) and non-smokers (OR = 0.62; 95% CI: 0.44–0.87) (Table 4). The protective association was also stronger in participants without diabetes (OR = 0.67; 95% CI: 0.48–0.92) and in those with a BMI <25 kg/m2 (OR = 0.58; 95% CI: 0.34–0.97).
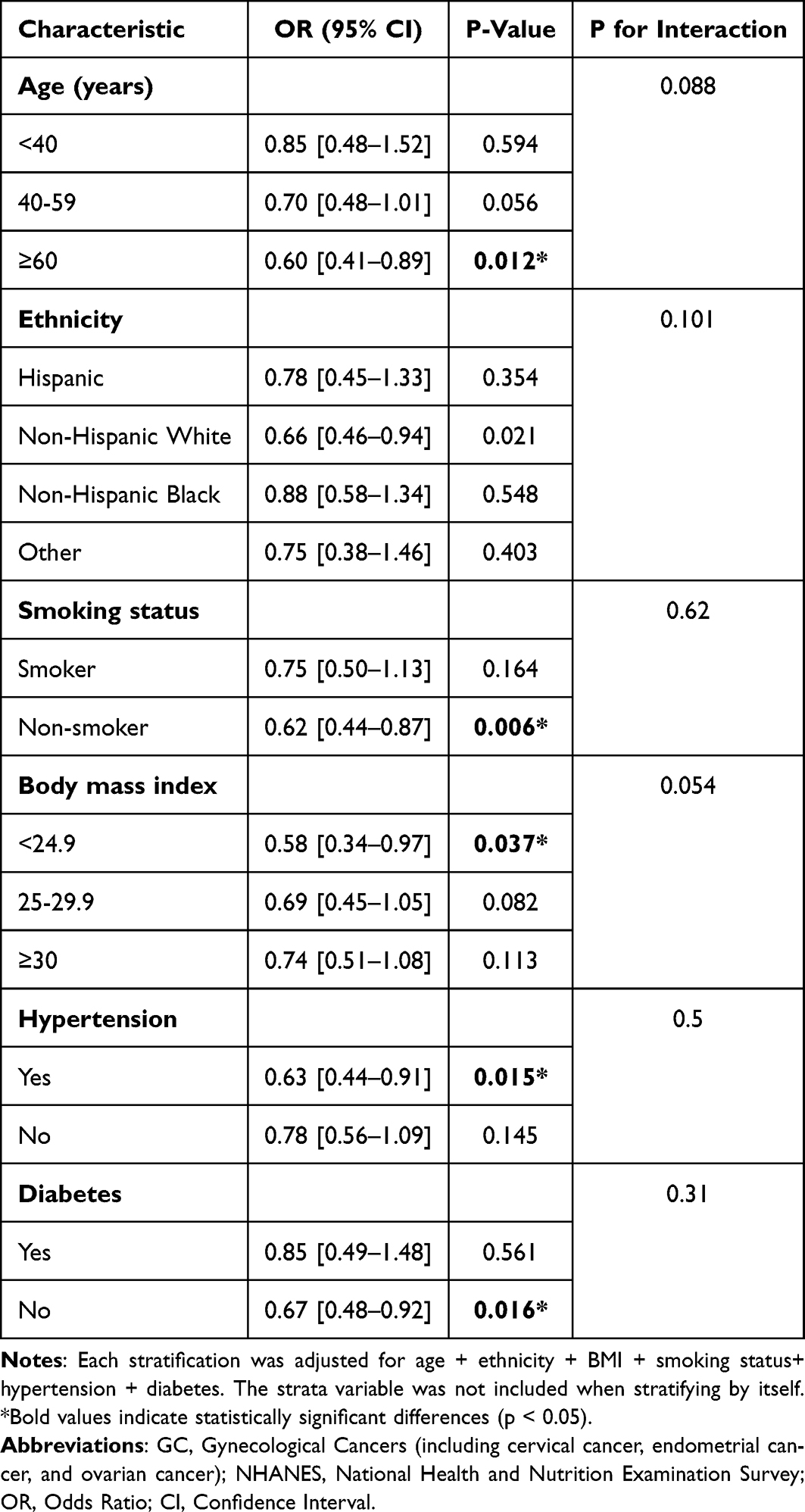 |
Table 4 Associations Between OBS and Gynecological Cancers, Stratified by Selected Factors, NHANES 2011–2018 |
Discussion
In our analysis of NHANES 2011–2018 data, a higher OBS was consistently associated with a lower prevalence of GC. Women in the highest OBS categories (total, dietary, and lifestyle subscores) had substantially reduced odds of having a reported gynecological malignancy compared to those in the lowest categories, even after adjusting for demographics and lifestyle covariates. For example, in fully adjusted logistic models controlling for age, race/ethnicity, BMI, smoking, and other factors, each incremental increase in the total OBS score corresponded to a significant decrease in GC odds. Similar inverse trends were observed for dietary OBS (reflecting antioxidant-rich diet) and lifestyle OBS (reflecting behaviors such as non-smoking, moderate alcohol intake, and physical activity) components. Subgroup analyses suggested that the protective association of high OBS was particularly evident in postmenopausal women and those without diabetes, whereas it was weaker among younger women and those with obesity, which may reflect differences in hormone exposure and metabolic risk. The inverse relationships persisted across most multivariable models, indicating that the OBS–cancer link was not explained by measured confounders. Overall, our findings support a dose–response interpretation; thus, greater antioxidant exposure (higher OBS) is linked to substantially lower GC prevalence among women in the US.
Our results align with a growing body of literature showing inverse associations between OBS (related antioxidant measures) and cancer risk in various populations. For instance, Chang et al (2024) reported in a large UK Biobank cohort that higher OBS was significantly associated with reduced colorectal cancer incidence.13 Likewise, Bentyaghoob et al (2023) found that Iranian women in the top tertile of the OBS had markedly lower odds of colorectal cancer.17 Although there have been few studies on gynecological tumors, some evidence is consistent. Slattery et al (2013) examined the dietary oxidative balance and observed a significant trend toward reduced breast cancer risk with a higher dietary oxidative balance.18 Xu et al (2025) analyzed US cancer survivors and found that a higher OBS strongly predicted lower all-cause and cancer-specific mortality,19 suggesting that even after diagnosis, better oxidative balance confers a survival advantage. A recent systematic review and meta-analysis by Hasani et al (2023) synthesized multiple case–control and cohort studies and found that, on average, higher OBS was associated with a 35–40% reduction in cancer odds (pooled OR = 0.64) in retrospective studies; cohort results were less consistent but showed a protective trend in women (pooled HR = 0.74).14 These findings broadly support our conclusion that a pro-antioxidant profile appears to lower the risk of cancer. Some discrepancies exist in the literature; for example, Gifkins et al (2012) in a US ovarian cancer case–control study reported that higher dietary selenium (an antioxidant) was associated with reduced ovarian cancer risk, but they found no clear association for total antioxidant capacity indices.20 This indicated that individual antioxidant nutrients may have variable effects. Overall, our results are consistent with those of previous research showing that antioxidant-rich diets and lifestyles tend to be linked to reduced cancer incidence in both women and men.17
Emerging molecular insights have shed light on how oxidative balance influences gynecological tumorigenesis. Chronic oxidative stress can induce DNA mutations, lipid peroxidation, and pro-inflammatory signaling, all of which promote cancer development. In normal cells, antioxidant systems and repair enzymes buffer ROS; however, when overwhelmed, ROS reacts with DNA and lipids. Calaf et al (2018) emphasized that ROS can mediate carcinogen activation and directly cause DNA strand breaks or base modifications, thereby driving tumor initiation.21 For example, estrogen metabolism in breast and endometrial tissues generates catechol-estrogens and ROS that form DNA adducts (Cavalieri model), linking hormonal exposure to oxidative DNA damage.22 Lipid peroxidation is a key pathway in this process. Barrera (2012) noted that ROS attack polyunsaturated fatty acids to form products such as 4-hydroxynonenal (4-HNE), which can further damage DNA and proteins, and that high 4-HNE levels can induce cancer cell apoptosis under oxidative overload.23 Inflammation also interacts with the redox balance; chronic inflammatory cytokines (eg, TNF-α and IL-1β) induce ROS production, which in turn activates Nuclear Factor-Kappa-B (NF-κB) signaling, creating a self-perpetuating tumorigenic loop. Antioxidant defense mechanisms modulate these effects. The Kelch-like ECH-associated protein 1-nuclear factor erythroid 2-related factor 2 (Keap1–Nrf2) pathway, a master regulator of cellular antioxidants, is being increasingly recognized in cancer. Under normal conditions, Nrf2 upregulates the genes encoding glutathione synthesis, superoxide dismutase, and other enzymes to neutralize ROS.24 While physiological Nrf2 activity protects healthy cells from oxidative mutagenesis, many tumors exploit constitutive Nrf2 activation to survive in pro-oxidant environments and to resist chemotherapy.24 Thus, OBS may partly capture the balance of these processes. A high OBS implies a milieu where pro-oxidant exposures (such as smoking or high iron) are limited and antioxidants (from diet or endogenous systems) are ample, reducing DNA damage and oncogenic signaling. In addition to the oxidative stress and inflammatory pathways discussed above, there is growing evidence that shifts in microbiota composition and the ensuing immune responses may influence cancer risk and progression. Dysbiosis in the gut, oral cavity, or female reproductive tract can contribute to a proinflammatory milieu, mucosal barrier disruption, and altered metabolite profiles (eg short-chain fatty acids, bile acids) that may promote genotoxic stress and tumorigenesis.25 Moreover, the gut microbiota has been shown to modulate systemic antitumor immunity: pathogenic taxa may suppress effective immune surveillance, while commensals like Lactobacillus or Bifidobacterium can enhance T cell, NK cell, and dendritic cell functions (eg via influencing cytokine milieu or antigen presentation).26 Given the known links between oxidative balance and immune‐oxidative interactions, it is plausible that individuals with higher oxidative balance scores might also maintain a more favorable microbiome composition and more robust antitumor immunity, thus reducing risk of gynecologic cancers.
In gynecological tissues, hormones intersect with oxidative mechanisms. Estrogen and progesterone receptor signaling can influence cellular antioxidant capacity (for instance, via the modulation of mitochondrial function and antioxidant enzyme expression). Some studies have reported that estrogen itself can sensitize breast and ovarian cells to oxidative DNA damage via estrogen receptor–mediated pathways. Moreover, oxidative stress can trigger epigenetic changes, and ROS may alter DNA methylation and miRNA profiles that regulate tumor suppressors or oncogenes. These complex interactions are the subject of active research, but they collectively suggest that maintaining redox homeostasis is crucial for genomic stability in hormone-responsive tissues.21,24 Our observed protective effect of high OBS is therefore biologically plausible; by minimizing ROS-mediated DNA lesions and dampening chronic inflammation, a higher antioxidant balance may interrupt key steps in the carcinogenic process.
The primary strengths of this study include its use of NHANES data, which are broadly representative of the US population and involve rigorous standardized data collection. The multi-cycle NHANES sample (2011–2018) provided a large cohort of adult women with detailed dietary, lifestyle, and health information. We computed a comprehensive OBS incorporating multiple validated dietary antioxidants (eg, vitamins C, E, and β-carotene) and pro-oxidant factors (eg, alcohol, iron, and smoking) based on established methods. Crucially, we adjusted for a wide range of potential confounders (eg, age, BMI, race/ethnicity, education, and smoking status) to isolate the independent association between OBS and cancer prevalence.
Nevertheless, this study had several limitations that warrant caution. The cross-sectional design of the NHANES means that we cannot infer temporal causality. It is possible that women with cancer may have changed their diet or behaviors (reverse causation) or that healthier survivors remain in the sample. Gynecological cancer status was based on self-reported physician diagnoses, which may have introduced a misclassification or recall bias and the number of cases in subgroup analyses may be limited. The OBS components rely on self-reported dietary and lifestyle questionnaires, which are subject to measurement errors and reporting bias. Although we adjusted for many covariates, residual confounding was possible; for example, we lacked data on family cancer history, specific gynecological cancer subtypes (ovarian vs endometrial), and HPV status for cervical cancer. Additionally, the NHANES assesses cancer prevalence, not incidence or stage, and the number of cases in subgroups (eg, rare uterine cancers) was modest, limiting the power of stratified analysis. Finally, OBS is a summary metric that may obscure the effects of individual antioxidants or pro-oxidants.
Conclusion
In this nationally representative cross-sectional analysis of US women using the NHANES 2011–2018 data, a higher OBS was significantly associated with a lower prevalence of gynecological cancers. This inverse relationship persisted across multiple OBS formulations (total, dietary, and lifestyle) and remained robust after adjusting for a wide range of demographic, behavioral, and metabolic covariates. These findings suggest that an antioxidant-rich diet, combined with healthy lifestyle behaviors, may offer protective effects against the development of gynecological malignancies.
Data Sharing Statement
The original contributions of this study are included in the article, and further inquiries can be directed to the corresponding authors.
Ethics Statement
The study protocol of NHANES was approved by the NCHS Research Ethics Review Board (ERB), and all participants provided written informed consent prior to participation (https://www.cdc.gov/nchs/nhanes/irba98.htm). The study was conducted in accordance with the Declaration of Helsinki. In accordance with the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023, China), Article 32, Items 1 and 2, our analysis is exempt from additional ethical approval since it is based on publicly available and anonymized data.
The relevant legislation specifies:
Article 32: Research involving human data or biological samples, where no harm is caused to individuals and no sensitive personal information or commercial interests are involved, may be exempt from ethical review. This provision is intended to reduce unnecessary burdens on researchers and facilitate the progress of life science and medical research involving humans.
- Research using publicly available data that has been legally obtained, or data generated through non-interfering observation of public behavior.
- Research using anonymized data.
Author Contributions
All authors substantially contributed to the work reported, including the conception, study design, data acquisition, analysis, and interpretation; participated in drafting, revising, or critically reviewing the manuscript; approved the final version for publication; agreed on the target journal; and accept responsibility for all aspects of the work.
Funding
This work and Rapid Service Fee were supported by the Project supported by National Natural Science Foundation of China (No.82460304), Ningxia Natural Science Foundation (No.2023AAC03589, 2023AAC03570), Ningxia Hui Autonomous Region Key Research and Development Plan Project (No.2023BEG01001, No.2023BEG02037).
Disclosure
The authors declare that this research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview. Int J Cancer. 2021;149(4):778–789.
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
4. Jensen JE, Becker GL, Jackson JB, Rysavy MB. Human papillomavirus and associated cancers: a review. Viruses. 2024;16(5):680. doi:10.3390/v16050680
5. Katagiri R, Iwasaki M, Abe SK, et al. Reproductive factors and endometrial cancer risk among women. JAMA Network Open. 2023;6(9):e2332296–e2332296. doi:10.1001/jamanetworkopen.2023.32296
6. Maleki V, Faghfouri AH, Pourteymour Fard Tabrizi F et al. Mechanistic and therapeutic insight into the effects of cinnamon in polycystic ovary syndrome: a systematic review. J Ovarian Res. 2021;14(1):130. doi:10.1186/s13048-021-00870-5
7. Yalvaç ES, Ateş Ç, Bakırcı M, et al. Composition of the vaginal microbiota in relation to cervical intraepithelial lesions. Turk J Obstet Gynecol. 2025;22(3):220–229. doi:10.4274/tjod.galenos.2025.09803
8. Fantone S, Marzioni D, Tossetta G. NRF2/KEAP1 signaling inhibitors in gynecologic cancers. Expert Rev Anticancer Ther. 2024;24(12):1191–1194. doi:10.1080/14737140.2024.2438951
9. Priyadarshini S, Swain PK, Agarwal K, Jena D, Padhee S. Trends in gynecological cancer incidence, mortality, and survival among elderly women: a SEER study. Aging Med. 2024;7(2):179–188. doi:10.1002/agm2.12297
10. Ďuračková Z. Some current insights into oxidative stress. Physiol Res. 2010;59(4):459–469.
11. Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB. Oxidative stress, inflammation, and cancer: how are they linked? Free Radic Biol Med. 2010;49(11):1603–1616. doi:10.1016/j.freeradbiomed.2010.09.006
12. Zhou Z, Han Y. Association between oxidative balance score and hearing loss: a cross-sectional study from the NHANES database. Front Nutr. 2024;11:1375545. doi:10.3389/fnut.2024.1375545
13. Chang Y, Li F, Wang Z, et al. Oxidative balance score: a potential tool for reducing the risk of colorectal cancer and its subsites incidences. Front Endocrinol. 2024;15. doi:10.3389/fendo.2024.1397512
14. Hasani M, Alinia SP, Khazdouz M, et al. Oxidative balance score and risk of cancer: a systematic review and meta-analysis of observational studies. BMC Cancer. 2023;23(1):1143. doi:10.1186/s12885-023-11657-w
15. Terry AL, Chiappa MM, McAllister J, Woodwell DA, Graber JE. Plan and operations of the national health and nutrition examination survey, august 2021-august 2023. Vital Health Stat. 2024;2024(66):1–21.
16. Zhang W, Peng SF, Chen L, Chen HM, Cheng XE, Tang YH. Association between the oxidative balance score and telomere length from the national health and nutrition examination survey 1999-2002. Oxid Med Cell Longev. 2022;2022:1345071. doi:10.1155/2022/1345071
17. Bentyaghoob S, Dehghani F, Alimohammadi A, et al. Oxidative balance score and dietary phytochemical index can reduce the risk of colorectal cancer in Iranian population. BMC Gastroenterol. 2023;23(1):183. doi:10.1186/s12876-023-02826-z
18. Slattery ML, John EM, Torres-Mejia G, et al. Angiogenesis genes, dietary oxidative balance and breast cancer risk and progression: the breast cancer health disparities study. Int J Cancer. 2014;134(3):629–644. doi:10.1002/ijc.28377
19. He R, Zhu Q, Ye Y, et al. The association between oxidative balance scores and all-cause mortality and cancer-specific mortality in cancer survivors: a retrospective cohort study. Front Nutr. 2025;12:1522048.
20. Gifkins D, Olson SH, Paddock L, et al. Total and individual antioxidant intake and risk of epithelial ovarian cancer. BMC Cancer. 2012;12:211. doi:10.1186/1471-2407-12-211
21. Calaf GM, Urzua U, Termini L, Aguayo F. Oxidative stress in female cancers. Oncotarget. 2018;9(34):23824–23842. doi:10.18632/oncotarget.25323
22. Cavalieri E, Chakravarti D, Guttenplan J, et al. Catechol estrogen quinones as initiators of breast and other human cancers: implications for biomarkers of susceptibility and cancer prevention. Biochimica et Biophysica Acta. 2006;1766(1):63–78.
23. Barrera G. Oxidative stress and lipid peroxidation products in cancer progression and therapy. ISRN Oncol. 2012;2012:137289. doi:10.5402/2012/137289
24. Zimta AA, Cenariu D, Irimie A, et al. The role of Nrf2 activity in cancer development and progression. Cancers. 2019;11(11). doi:10.3390/cancers11111755.
25. Wu J, Li J, Yan M, Xiang Z. Gut and oral microbiota in gynecological cancers: interaction, mechanism, and therapeutic value. NPJ Biofilms Microbiomes. 2024;10(1):104. doi:10.1038/s41522-024-00577-7
26. Xie M, Li X, Lau -HC-H, Yu J. The gut microbiota in cancer immunity and immunotherapy. Cell Mol Immunol. 2025;22(9):1012–1031. doi:10.1038/s41423-025-01326-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Redox Biomarkers – An Effective Tool for Diagnosing COVID-19 Patients and Convalescents
Wolszczak-Biedrzycka B, Dorf J, Matowicka-Karna J, Dymicka-Piekarska V, Wojewódzka-Żeleźniakowicz M, Żukowski P, Zalewska A, Dąbrowski Ł, Maciejczyk M
Journal of Inflammation Research 2024, 17:2589-2607
Published Date: 26 April 2024
A Narrative Review of the Reciprocal Relationship Between Sleep Deprivation and Chronic Pain: The Role of Oxidative Stress
Chen S, Xie Y, Liang Z, Lu Y, Wang J, Xing F, Mao Y, Wei X, Wang Z, Yang J, Yuan J
Journal of Pain Research 2024, 17:1785-1792
Published Date: 20 May 2024
Emodin, a Phytotherapeutic Anthraquinone, Potently Attenuates Synaptic Redox Pathology in Aged Rats
Saha P, Ahmad F
Degenerative Neurological and Neuromuscular Disease 2026, 16:570320
Published Date: 20 February 2026