Back to Journals » Journal of Pain Research » Volume 19
Association Between Long-Term ACEI/ARB Use and Postoperative Pain in Hypertensive Patients: A Retrospective Cohort Study and Genetic Validation
Received 26 June 2025
Accepted for publication 24 March 2026
Published 8 April 2026 Volume 2026:19 549864
DOI https://doi.org/10.2147/JPR.S549864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Xinrui Li, Lu Che, Le Shen
Department of Anesthesiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Le Shen, Department of Anesthesiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, No. 1 Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-10-6915-2021, Email [email protected]
Background: Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are commonly used for hypertension management. Emerging evidence suggests that these agents may influence pain perception through neuroinflammatory and hormonal pathways. However, their impact on acute postoperative pain has not been well characterized.
Aim: This study aimed to explore the hypothesis that long-term ACEI/ARB use is associated with reduced acute postoperative pain in hypertensive patients undergoing non-cardiac surgery.
Methods: We conducted a hybrid study combining a retrospective cohort analysis with a drug-target Mendelian randomization approach. A total of 1206 hypertensive patients who underwent general anesthesia and received patient-controlled intravenous analgesia were included. The primary outcome was the presence of moderate-to-severe postoperative pain, which was defined as a numerical rating scale (NRS) score ≥ 4 on postoperative days (PODs) 1 and 3. Secondary outcomes included opioid consumption measured in morphine milligram equivalents. Confounders were adjusted using inverse probability of treatment weighting. Missing data was treated by multiple imputation with chained equation, as 37.3% of POD3 NRS missing. Genetic validation was performed using expression quantitative trait loci for ACEI/ARB target genes and genome-wide association data on multisite chronic pain.
Results: Patients receiving ACEIs/ARBs had significantly lower rates of moderate-to-severe pain on postoperative day 1 (OR 0.74, 95% CI 0.57– 0.94; ARR 6.87%; NNT 14.6) but had no significance on day 3 (OR 0.77, 95% CI 0.57– 1.04), despite similar opioid consumption on both days. Genetic validation found associations between several ACEI/ARB target genes and reduced chronic pain risk, directionally consistent with our clinical observations.
Conclusion: Long-term ACEI/ARB use may offer potential analgesic benefits for surgical patients with hypertension. These preliminary findings provide a foundation for future research to explore their potential role in perioperative pain management.
Keywords: ACE inhibitors, angiotensin receptor blockers, postoperative pain, hypertension, Mendelian randomization, perioperative analgesia
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ke has been published for this article.
Introduction
Hypertension is one of the most prevalent chronic conditions worldwide.1 Hypertension may increase the risk of chronic pain through impaired cardiovascular regulation.2,3 Commonly prescribed antihypertensive agents include angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), β-blockers (BBs), calcium channel blockers (CCBs), and diuretics. ACEIs and ARBs are among the most commonly used agents and are often used in combination therapy due to their efficacy and tolerability.4 With the increase of global surgical volume,5,6 a large number of patients with hypertension need to undergo surgery and are confronted with the important clinical issue of postoperative pain. Postoperative pain is common for surgical patients.7,8 Postoperative pain is a common and often underappreciated complication following surgery, and it may lead to delayed recovery, increased opioid consumption, and in some cases, chronic postsurgical pain (CPSP).9 Multimodal analgesia conduces to relief acute pain and reduces chronic postoperative pain. Understanding how chronic use of common medications such as antihypertensives influences postoperative pain is essential for optimizing perioperative care.
Beyond their primary cardiovascular effects, ACEIs and ARBs may also influence pain modulation. These agents act on the renin–angiotensin–aldosterone system (RAAS) and can modulate inflammatory responses by inhibiting angiotensin II and aldosterone signaling, both of which are implicated in pain sensitization pathways.10,11 Preclinical studies have suggested that RAAS components (eg, AT1 and AT2 receptors) are involved in the perception and regulation of pain through both central and peripheral mechanisms.12,13 Whereas AT1 receptor activation drives neuroinflammation and central sensitization via pro-inflammatory cytokines, AT2 receptor stimulation promotes opioidergic analgesia and anti-inflammatory effects, demonstrating opposing roles in pain modulation.14 Moreover, previous studies also indicated the pain-inducing action of ACEIs, which associated with their interference with metabolism of bradykinin and substance P.14 This dichotomy is particularly relevant to postoperative pain, which involves both inflammatory and neuropathic components. Role of RAAS and relevant agents on different types of pain deserved further investigation, especially from clinical perspective. However, evidence on the clinical implications of ACEI/ARB use on pain perception, particularly in the postoperative period, remains sparse and inconsistent. Very few clinical studies have been conducted for examining the relationship between ACEI/ARB use and postoperative pain outcomes.
We hypothesized that long-term use of ACEIs or ARBs may reduce the risk of acute postoperative pain in patients with hypertension, which has not been supported by previous clinical studies. To address this, we designed a hybrid study combining a single-center retrospective cohort analysis with drug-target Mendelian randomization (MR).15 The retrospective cohort provided real-world clinical data to assess associations between ACEI/ARB use and postoperative pain intensity. MR, using genetic proxies for ACEI/ARB target gene expression, allowed us to investigate the potential causal link between drug target modulation and pain risk, particularly chronic multisite pain (MCP), using large-scale genome-wide association summary data. By integrating clinical and genetic epidemiology, this study aims to provide both observational and mechanistic insights into the potential analgesic effects of ACEIs and ARBs. These findings may help inform personalized perioperative medication management in hypertensive patients and stimulate further investigation into the non-cardiovascular benefits of RAAS-targeting drugs.
Methods
Study Design
This is a hybrid study combining a single-center retrospective cohort analysis with drug-target MR to investigate the association between ACEI/ARB use and postoperative pain in hypertensive patients. The study was approved by the Ethics Committee of Peking Union Medical College Hospital with inform consent waived. The retrospective cohort study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)-Cohort reporting guidelines and MR study followed the STROBE–MR reporting guidelines.
Retrospective Cohort
Study Population
We included adult patients (aged ≥18 years) with a diagnosis of hypertension who underwent non-cardiac surgery under general anesthesia at Peking Union Medical College Hospital (PUMCH) between July 1, 2023, and July 31, 2024. Eligible patients received postoperative patient-controlled intravenous analgesia (PCIA). Patients who were <18 years old, or underwent emergency surgery, or had incomplete medical records were excluded. For patients with multiple surgeries, only the first surgery was included. The flowchart is shown in Figure 1.
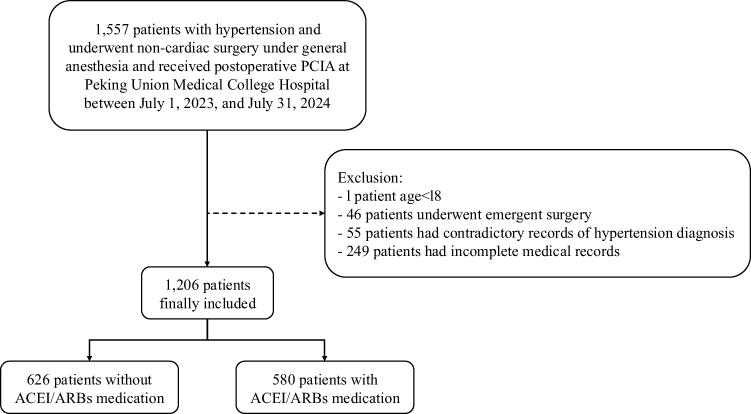 |
Figure 1 The flow chart of inclusion and exclusion criteria of retrospective cohort study. |
Data Collection and Exposure Definition
Demographic and clinical data, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, comorbidities, surgical details, and medication use, were extracted from the PeriOperative Patient Safety (POPS)-PUMCH database. Antihypertensive medication use was defined based on preoperative prescription. ACEI/ARB exposure was defined as the use of either ACEIs or ARBs continuously within one month before surgery. Medications discontinued for more than one month preoperatively were not considered. Acute postoperative pain was measured by Numerical Rating Scale (NRS) on postoperative day (POD) 1 and 3, recorded by Acute Pain Service (APS). Postoperative opioid consumption was calculated from electronic records of PCIA.
Anesthetic and Pain Management Procedure
All participants who had long-term use of ACE//ARBs discontinued their medication on the morning of surgery and resumed on postoperative day 1 if there is no contraindication. General anesthesia was induced by propofol (1.5–2mg/kg) and fentanyl (1–2µg/kg), followed by maintenance of propofol (target-controlled infusion) or sevoflurane in oxygen/air mixture at the discretion of anesthesiologist in charge. Remifentanil was administered during anesthetic maintenance and titrated based on hemodynamic parameters. Multimodal analgesia was performed by combining opioids and NSAIDs during general anesthesia.
All participants involved in our study received postoperative pain management with PCIA with sufentanil (150 μg in 250 mL normal saline, 0.6 μg/mL). The pump was set to deliver a continuous background infusion plus patient-controlled boluses with a 15-min lockout interval. Analgesic efficacy was monitored using NRS scores by APS, and rescue medication was available for breakthrough pain.
Outcomes
The primary outcome was the moderate-to-severe acute postoperative pain, defined as a score ≥4 on the NRS recorded on POD 1 and 3. The secondary outcome was opioid consumption on POD 1 and 3, quantified as morphine milligram equivalents (MME).
Confounding Adjustment
Confounding factors in this study included gender, age, BMI, ASA physical status, surgery duration, surgery type, smoking history, alcohol abuse, medication history, coronary heart disease, diabetes mellitus, asthma, chronic obstructive pulmonary disease (COPD), hyperthyroidism, renal dysfunction, neurologic disease, digestive disease, baseline blood pressure. Preoperative comorbidities were extracted from medical record homepage diagnoses coded according to International Classification of Diagnosis (ICD) standards. We used inverse probability of treatment weighting (IPTW) to adjust the confounding factors.16 We used the exposure of ACEI/ARBs as outcome and all confounding factors as exposure to perform a multiple logistic regression to calculate the propensity score for each confounding factor. The propensity score was included in our subsequent analysis. We assessed propensity score overlap (Supplementary Figure 1) and weight distributions (Supplementary Figure 2) to verify model assumptions. Extreme weights were managed using percentile-based Winsorization, where values below the 1st and above the 99th percentiles were replaced with the corresponding percentile values (P1 and P99).
Statistical Analysis
Baseline characteristics were compared between groups using standardized mean differences (SMD). We considered SMD <0.10 to indicate adequate balance. Chi-square test was used to analyze the differences of the incidence of moderate-to-severe pain, and Mann–Whitney U-test was used to analyze the differences of opioids consumption. A binary logistic regression was applied to compute odd ratios (ORs) and 95% confidence intervals (95% CIs) to assess the association between moderate-to-severe acute postoperative pain and ACEI/ARBs medication. Absolute risk reduction (ARR) and number need to treat (NNT) were calculated for clinical significance. Opioid consumption at POD1 and POD3 was analyzed using zero-inflated Gamma regression with IPTW weighting, modeling the probability of any use and amount consumed among users separately. Missing data was handled using multiple imputation with chained equations (MICE). We used the Fully Conditional Specification (FCS) automatic method (Number of imputations: 25, iterations: 10) by SPSS R27.0.1.0. The imputation model included all the outcomes and confounding factors mentioned above. Analyses of the single-center retrospective cohort study were performed by SPSS R27.0.1.0 and RStudio (2025.05.1+513).
Sensitivity Analysis and Power Calculation
To evaluate robustness to missing data assumptions, we conducted complete case analysis and worst-case scenario analysis where all missing values were imputed in the absence of moderate-to-severe pain, examining the consistency between them. For significant outcome, we calculated the minimum detectable effect size (MDE) based on ESS, assuming α=0.05 (two-sided) and 80% power. For non-significant outcomes, we conducted a post-hoc power analysis based on ESS, assuming α=0.05 (two-sided) and 80% power. Power calculation was performed by G*Power 3.1.
Mendelian Randomization
Exposure
Antihypertensive Drugs Target Genes
Commonly used antihypertensives including ACEIs, ARBs, BBs, CCBs, diuretics, alpha-adrenoceptor blockers, adrenergic neuron blocking drugs and centrally acting antihypertensive drugs were included in this MR analysis. A total of 327 target genes for antihypertensive agents documented in previously published studies were systematically extracted from DrugBank (https://go.drugbank.com/) databases and Drug–Gene Interaction database (DGIdb, https://www.dgidb.org/). We employed expression quantitative trait loci (eQTLs) mapped to antihypertensive drug target genes as genetic proxies for exposure. eQTL summary statistics of whole blood sample (n = 31,684) were retrieved from the eQTLGen Consortium (https://www.eqtlgen.org/). Single-nucleotide polymorphisms (SNPs) were retained as instrumental variables if they (i) displayed a significant cis-association (located within 1 Mb of the transcription start site) with the corresponding drug target gene at genome-wide significance (p < 5 × 10−8) and (ii) had a minor allele frequency ≥1%.
Systolic Blood Pressure
To obtain reliable tools for studying the antihypertensive agents of interest, we conducted a two-sample MR analysis, utilizing the systolic blood pressure (SBP) as predictor and the multisite chronic pain (MCP) as outcome variable. SBP was selected due to its greater significance in hypertension management compared with diastolic blood pressure (DBP).17 The GWAS summary statistics for SBP were derived from a study involving 757,601 individuals of European descent (both males and females), sourced from the UK Biobank and the International Consortium of Blood Pressure Genome-Wide Association Studies (ICBP).18
Outcome
We obtained the publicly available GWAS statistics for chronic pain from a sex-stratified genome-wide association study of MCP.19 The analysis of MCP included 178,556 men and 209,093 women in UK Biobank.19
Statistical Analysis
We assessed whether the genetic instruments satisfied the three core assumptions of Mendelian randomization: relevance, independence, and exclusion restriction.20 To conduct the drug-target Mendelian randomization (MR), we employed the summary-based MR (SMR) method (version 1.02).21 SNPs that surpassed the statistical significance threshold of p < 0.05 in the SMR test were considered. Furthermore, we applied the Heterogeneity in Dependent Instruments (HEIDI) test, with a p-value threshold of 0.05, to differentiate pleiotropy from linkage.21 Multiple testing correction was performed using the Benjamini–Hochberg false discovery rate (FDR) method, with a significance threshold set at FDR < 0.05. For two-sample MR, effect estimates were generated using three methods by MendelR package in R: inverse-variance weighted (IVW) regression as the primary estimator, supplemented by MR-Egger regression and weighted median estimator (WME). Heterogeneity was assessed by Cochran’s Q test. Potential directional pleiotropy was evaluated via the MR-Egger intercept test. Additional sensitivity analysis known as leave-one-out was used to evaluate the robustness of the findings. All analyses were performed by RStudio 2023.03.1, R 4.22.
Result
Study Population
The final analysis comprised a total of 1206 hypertensive patients who fulfilled the inclusion criteria (Figure 1). Among them, 580 patients (48.1%) had a history of continuous ACEI/ARB use within one month prior to surgery. The remaining 626 patients did not receive ACEI/ARBs during the same period. After applying inverse probability of treatment weighting (IPTW), baseline characteristics were approximately balanced between two groups. The demographic and clinical features before and after IPTW were summarized in Table 1 and Supplementary Figure 3. The mean (SD) of inverse probability weights was 2.00 (0.44) before Winsorization (Supplementary Table 1). After the 1st and 99th percentile Winsorization, the maximum weight decreased from 5.50 to 3.44, and the effective sample size (ESS) was 1157.7 (96.0% of the original sample).
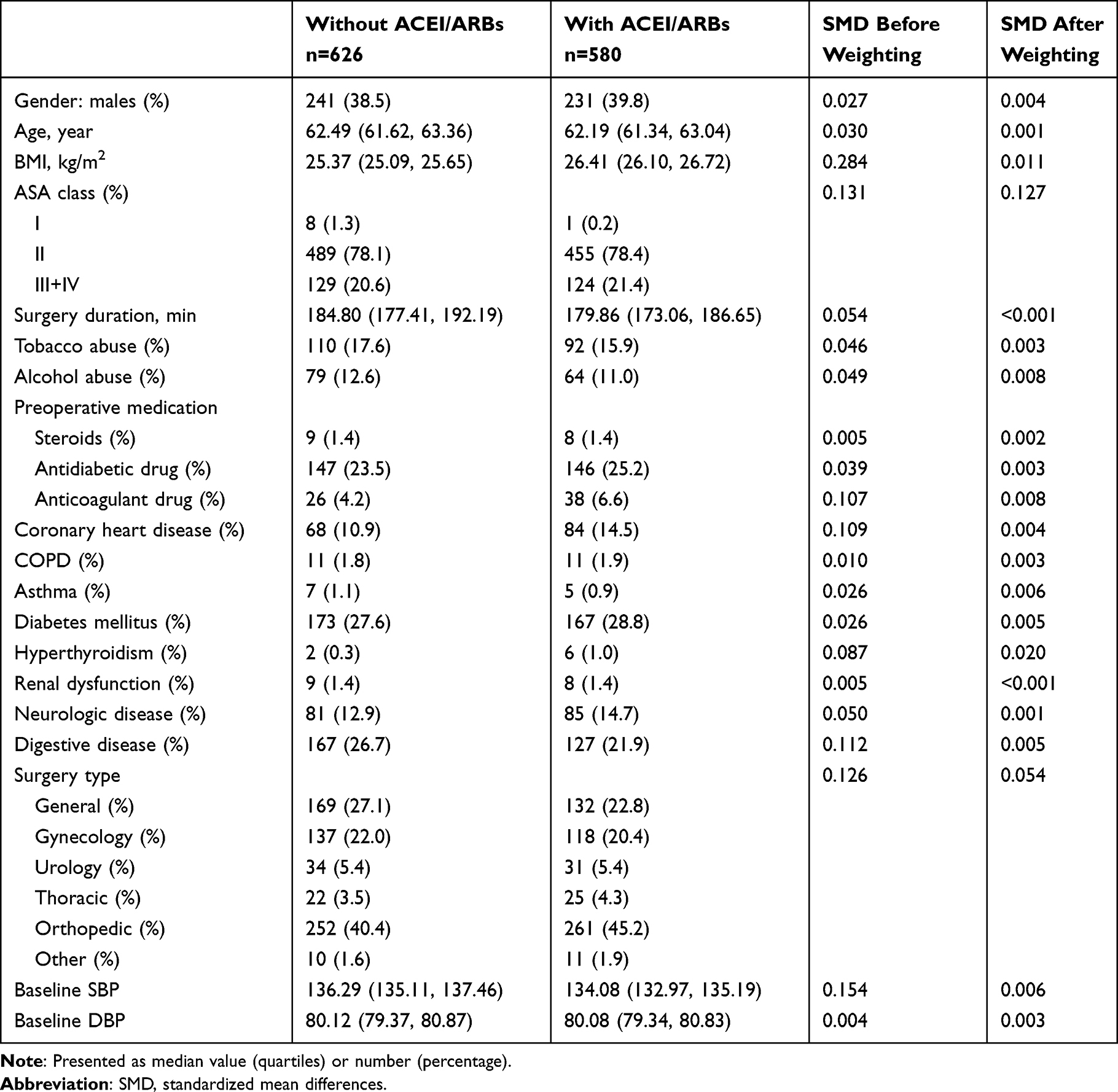 |
Table 1 Population Characteristics Before and After IPTW |
Postoperative Pain and Opioid Consumption
Postoperative pain outcomes are presented in Table 2. The number of participants with available pain scores at POD1 and POD3 was 1206 (100.0%) and 756 (62.7%), respectively. On postoperative day (POD) 1, 61.2% of patients in the ACEI/ARB group reported moderate-to-severe pain (NRS ≥4) compared to 67.7% in the non-ACEI/ARB group (p = 0.019). On POD3, the incidence of moderate-to-severe pain was 33.7% in the ACEI/ARB group versus 42.0% in the non-ACEI/ARB group (p = 0.020).
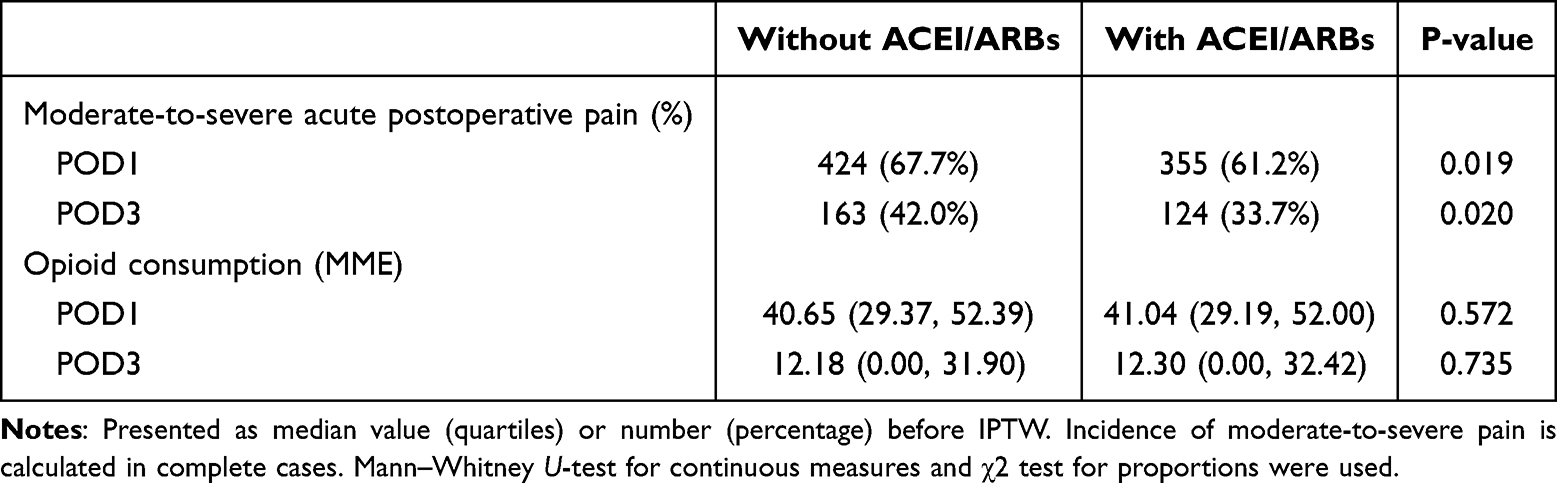 |
Table 2 Postoperative Pain Outcomes Grouped by ACEI/ARBs Medication |
No significant differences of opioid consumption were observed between the two groups. Median morphine milligram equivalent (MME) on POD1 was 41.04 (IQR 29.19–52.00) in the ACEI/ARB group and 40.65 (IQR 29.37–52.39) in the non-ACEI/ARB group (p = 0.572). On POD3, median MME was 12.30 (IQR 0.00–32.42) in the ACEI/ARB group and 12.18 (IQR 0.00–31.90) in the non-ACEI/ARB group (p = 0.735).
Multivariable Regression Analysis
After IPTW adjustment and MICE, the incidence of moderate-severe pain was 60.40% in ACEI/ARB group versus 67.30% in non-ACEI/ARB group (adjusted OR 0.74, 95% CI 0.57–0.94, p=0.015) on POD1 (Table 3). This corresponds to an absolute risk reduction of 6.87% (95% CI 6.88%–6.86%) and a number needed to treat of 14.6 (95% CI 14.6–14.5). The minimum detectable effect (MDE) size with 80% power was 8%. On POD3, the incidence of moderate-to-severe pain was 31.10% in ACEI/ARB group versus 36.70% in non-ACEI-ARB group (adjusted OR 0.77, 95% CI 0.57–1.04, p=0.091) (Table 3). Post-hoc power analysis indicated 51.1% power to detect a significant difference at α=0.05 for incidence of moderate-to-severe pain on POD3. Zero-inflated Gamma regression models showed no significant association between ACEI/ARB use and opioid consumption on POD1 or POD3 (Table 4).
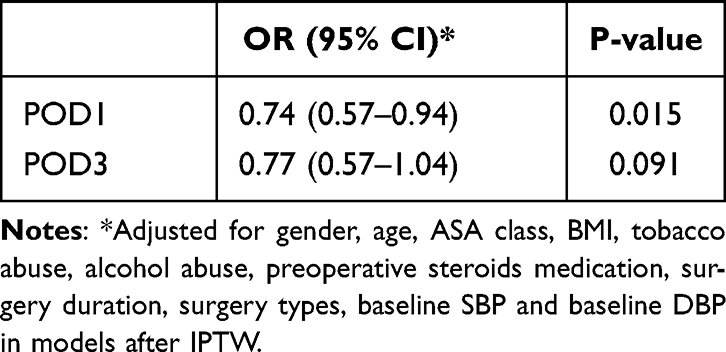 |
Table 3 Association Between ACEI/ARBs Medication and Postoperative Moderate-to-Severe Pain |
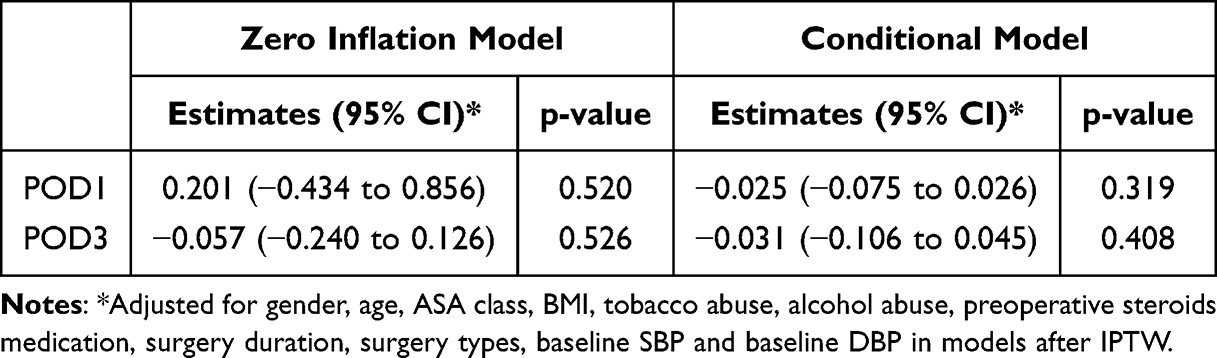 |
Table 4 Association Between ACEI/ARBs Medication and Postoperative Opioids Consumption |
Sensitivity analyses using complete-case analysis and worst-case scenario analysis yielded consistent effect directions with the primary multiple imputation analysis, though statistical significance varied (Supplementary Table 2).
Mendelian Randomization Results
We identified 327 antihypertensive drug target genes; however, only 188 of these possessed available genetic proxies suitable for subsequent analyses. All genetic proxies included in analysis had F-statistics above 10 (Supplementary Table 3). Part of the genetically proxied antihypertensive drugs effects were associated with reduced or increased risk of MCP after excluding 3 proxies with linkage disequilibrium (Figure 2). Seventeen antihypertensive drug target genes were associated with a reduced risk of MCP, while six genes were associated with increased risk. After multiple testing correction by FDR, GRK4, HLA-DRB1 and CSK remained significant (Figure 2).
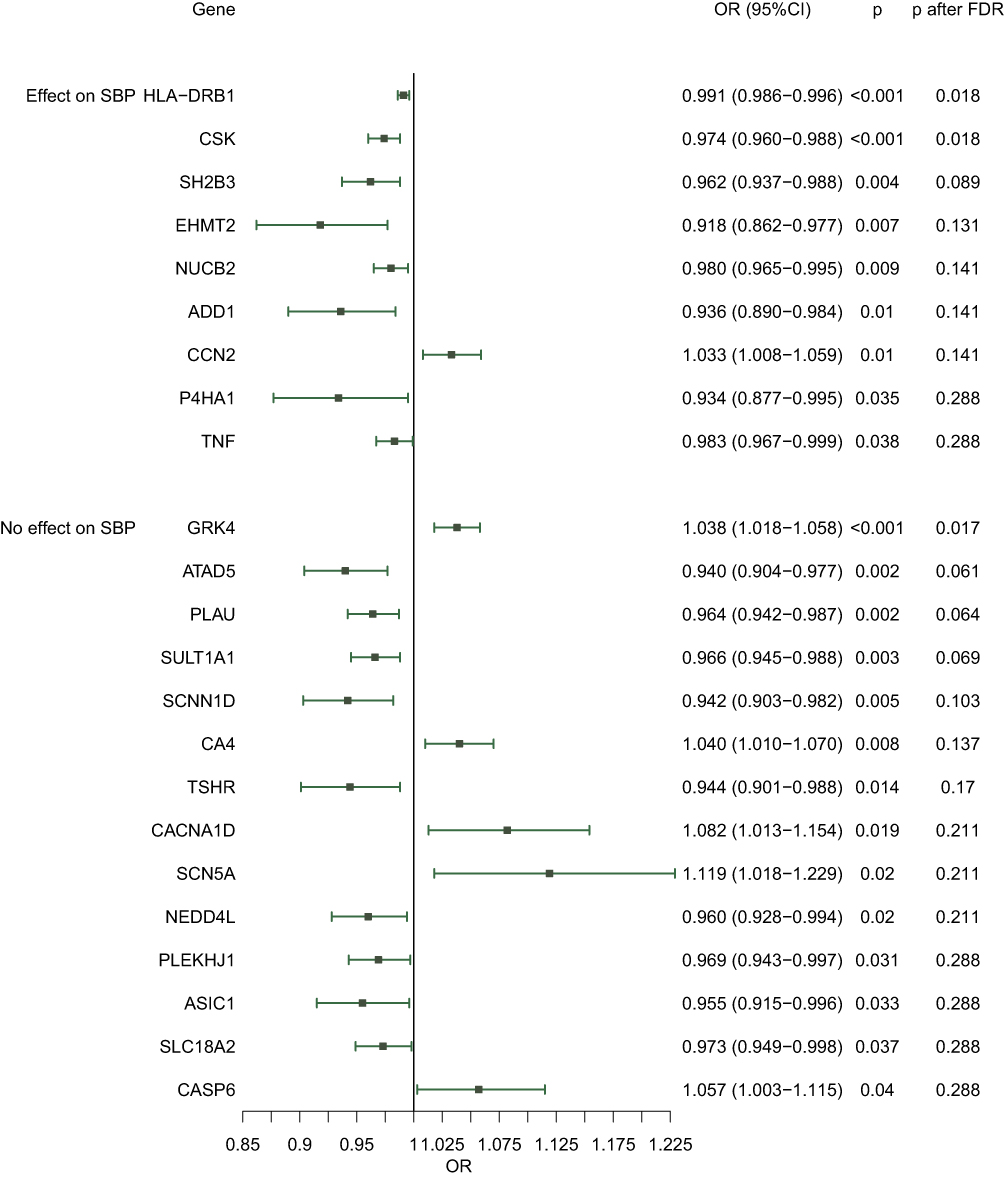 |
Figure 2 Mendelian randomization estimates multisite chronic pain for antihypertensive drugs effects, grouped by their effects on SBP. Mendelian randomization is conducted by summary-based Mendelian randomization. Genes are stratified by their effect on systolic blood pressure (SBP). Effect estimates represent odds ratios (OR) with 95% confidence intervals (CI). P values before and after false discovery rate (FDR) correction are shown. |
The correspondence between genes and antihypertensive medication categories are shown in Figure 3 and Supplementary Table 4. Notably, among ACEI/ARB-related genes, SH2B3 and PLEKHJ1 were associated with decreased MCP risk, whereas CCN2 was associated with increased risk. These genetic findings were consistent with the clinical observations from the retrospective cohort.
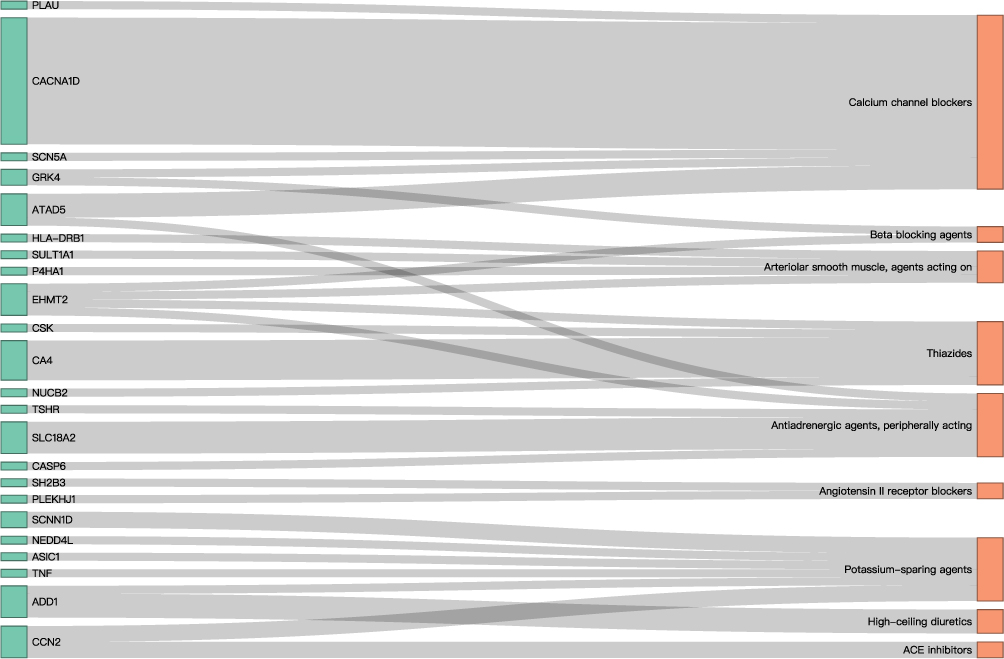 |
Figure 3 Sankey diagram of the correspondence between target genes and antihypertensive medication categories. Left nodes (green): target genes for antihypertensive agents. Right nodes (red): classification of antihypertensive agents. Flow width represented the number of antihypertensive agents. |
Further MR analyses (proxies shown in Supplementary Table 5) indicated that nine of the 23 identified genes influenced MCP through their effects on systolic blood pressure (SBP), while others appeared to exert SBP-independent effects (Figure 2 and Supplementary Table 6). Sensitivity analyses supported the robustness of these associations (Supplementary Table 7).
Discussion
In this hybrid study combining a single-center retrospective cohort and a drug-target Mendelian randomization analysis, we found that long-term use of ACEIs or ARBs was associated with a reduced incidence of moderate-to-severe acute postoperative pain on POD1 among hypertensive patients undergoing non-cardiac surgery. Notably, this association persisted after rigorous confounder adjustment using inverse probability of treatment weighting. Furthermore, Mendelian randomization analysis identified several ACEI/ARB target genes that were associated with decreased risk of multisite chronic pain (MCP), providing genetic validation for a potential analgesic effect of these agents. However, as no previous observational studies have confirmed such a link and analgesic data were unavailable, this finding should be considered exploratory.
ACEI/ARBs act on the renin-angiotensin-aldosterone system (RAAS) and are currently among the most commonly used antihypertensive drugs in clinical practice.22 As we mentioned, prior basic research has demonstrated that ACEIs and ARBs play a dual role in pain modulation upon distinct inflammatory states.14 Notably, prior systematic reviews found no perioperative benefit of continuing ACEIs/ARBs on major clinical outcomes, though pain was not evaluated.23 Our findings align with preclinical studies suggesting that RAAS blockade may reduce hyperalgesia, and extend these observations to a real-world surgical setting. In our cohort, the ARR for moderate-to-severe pain was 6.87%, corresponding to a NNT of 14.6. This suggests that for every 15 hypertensive patients on long-term ACEI/ARB therapy, one case of moderate-to-severe acute postoperative pain may be prevented, assuming the observed association reflects a true therapeutic effect. While clinical medication adjustments require further high-quality evidence, our study generates a hypothesis that long-term ACEI/ARB use may confer potential analgesic benefits. We anticipate prospective cohorts or RCTs to validate this effect, thereby informing preoperative antihypertensive switching (eg, from reserpine) from a pain management perspective with carefully consideration of hypotension risk.
Interestingly, we did not observe a significant difference in postoperative opioid consumption between groups, despite the reduction in moderate-to-severe pain incidence. We speculated that many patients tended to endure pain rather than actively demand additional boluses, with the concern of side-effects of opioids. It potentially resulted in homogeneous dosing across individuals. Furthermore, multimodal analgesics or rescue medications, most frequently with NSAIDs, administered in the ward were not captured in our retrospective data, which may also have contributed to the limited variability in opioid consumption.
We conducted sensitivity analyses to assess the impact of missing data on our findings. After multiple imputation for missing data of NRS on POD3, the direction of associations remained consistent, though statistical significance varied. It likely stemmed in the fact that missing data predominantly originated from patients who had their PCIA discontinued, a subgroup characterized by lower incidence of moderate-to-severe pain. Consequently, the effective sample size in this sensitivity analysis was insufficient to detect a significant effect (post-hoc power = 0.51). These results underscore the robustness of our primary findings while highlighting the importance of complete case ascertainment in future studies.
The Mendelian randomization analysis added a supplement to our findings by demonstrating that genetic proxies for ACEI/ARB targets, particularly SH2B3 and PLEKHJ1, were associated with lower MCP risk. Importantly, several of these associations appeared independent of SBP, suggesting potential pleiotropic analgesic effects beyond hemodynamic regulation. These results support the hypothesis that RAAS-targeting medications may exert beneficial effects on pain processing via off-target or downstream signaling mechanisms. In MR analysis, 23 target genes demonstrated associations with reduced MCP risk at the nominal significance level (P < 0.05). However, after stringent correction for multiple testing using the false discovery rate (FDR) method, only three genes (GRK4, HLA-DRB1 and CSK) remained statistically significant. This reduction in significant hits likely reflected the conservative nature of FDR correction applied to correlated genetic instruments and modest effect sizes typical of complex traits. Nevertheless, the coherent directional pattern across all 23 genes supports a biologically plausible aggregate effect of antihypertensive agents targets on pain modulation, with the top hits representing the most robust genetic evidence.
Our study has several strengths. First, the use of both observational and genetic epidemiological methods strengthens causal inference. Second, the integration of real-world clinical data with MR improves generalizability and biological plausibility. Third, the consistency of findings across two distinct methodological frameworks adds credibility to the observed associations.
Nonetheless, limitations should be acknowledged. First, the observed effect size did not reach our predetermined minimum detectable effect (MDE), suggesting warranted caution in interpreting the clinical significance of these findings pending replication in larger cohorts. Second, as a retrospective cohort study, residual confounding cannot be fully excluded, despite robust IPTW adjustment. Anesthetic regimens and postoperative ward analgesics could not be accurately ascertained from medical records. Moreover, preoperative antihypertensive use was extracted from prescription documentation, precluding assessment of patient compliance. Third, phenotypic discordance exists between the cohort and MR. Although acute pain plays an essential role in chronicity of pain,24 the absence of large-scale GWAS for acute pain necessitated this proxy approach. Consequently, the two analyses serve as complementary rather than causally linked evidence. Fourth, our outcomes were restricted to pain-related measures, omitting major clinical endpoints and pertinent functional outcomes. Prospective cohorts incorporating these broader outcomes are warranted. Fifth, the single-center retrospective design with population using PCIA carries inherent risk of selection bias, limiting generalizability to diverse surgical populations and practice settings. Sixthly, the dichotomy of pain may lead to loss of information.
Conclusions
This study identifies an association between long-term ACEI/ARB use and reduced incidence of moderate-to-severe acute postoperative pain in hypertensive patients. The concordance between our retrospective cohort findings and Mendelian randomization analyses supports a testable hypothesis that RAAS-targeting medications may exert analgesic effects beyond hemodynamic regulation. These observations provide preliminary insight into the potential pain-related implications of commonly prescribed antihypertensive agents. Further prospective studies and randomized trials are needed to validate this hypothesis and elucidate whether cardiovascular drugs could be leveraged to optimize perioperative pain management and postoperative recovery.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Peking Union Medical College Hospital (approval number: I-24PJ1981). The requirement for informed consent was waived due to the retrospective design and the use of de-identified clinical data. The Mendelian randomization analysis was based on publicly available, de-identified summary-level genetic data, and did not require ethical approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by CAMS Innovation Fund for Medical Sciences (CIFMS) Grant No. 2024-I2M-TS-001 and Medical High-Level Talent Program (National Outstanding Young Physician).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. (NCD-RisC) NRFC. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–11. doi:10.1016/S0140-6736(21)01330-1
2. Al-Ghamdi S, Shubair MM, El-Metwally A, et al. The relationship between chronic pain, prehypertension, and hypertension. A population-based cross-sectional survey in Al-Kharj, Saudi Arabia. Postgrad Med. 2021;133(3):345–350. doi:10.1080/00325481.2020.1863716
3. Bruehl S, Olsen RB, Tronstad C, et al. Chronic pain-related changes in cardiovascular regulation and impact on comorbid hypertension in a general population: the Tromsø study. Pain. 2018;159(1):119–127. doi:10.1097/j.pain.0000000000001070
4. Smith DK, Lennon RP, Carlsgaard PB. Managing hypertension using combination therapy. Am Fam Physician. 2020;101(6):341–349.
5. Shoyombo I, Genetu A, Wong LY, et al. Measurements of surgical volume in low- and middle-income countries, a systematic review. Ann Glob Health. 2023;89(1):70. doi:10.5334/aogh.4251
6. Vervoort D, Lee G, Ghandour H, et al. Global cardiac surgical volume and gaps: trends, targets, and way forward. Ann Thorac Surg Short Rep. 2024;2(2):320–324. doi:10.1016/j.atssr.2023.11.019
7. Demilew BC, Zurbachew N, Getachew N, Mekete G, Lema DT. Prevalence and associated factors of postoperative acute pain for mothers who gave birth with cesarean section: a systematic review and meta-analysis. Pain Manag Nurs. 2024;25(6):e452–e64. doi:10.1016/j.pmn.2024.05.010
8. Wang L, Yang M, Meng W. Prevalence and characteristics of persistent postoperative pain after thoracic surgery: a systematic review and meta-analysis. Anesth Analg. 2023;137(1):48–57. doi:10.1213/ANE.0000000000006452
9. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
10. Turan A, Atim A, Dalton JE, et al. Preoperative angiotensin-converting enzyme inhibitor use is not associated with increased postoperative pain and opioid use. Clin J Pain. 2013;29(12):1050–1056. doi:10.1097/AJP.0b013e318287a258
11. Di Raimondo D, Tuttolomondo A, Buttà C, Miceli S, Licata G, Pinto A. Effects of ACE-inhibitors and angiotensin receptor blockers on inflammation. Curr Pharm Des. 2012;18(28):4385–4413. doi:10.2174/138161212802481282
12. Balogh M, Aguilar C, Nguyen NT, Shepherd AJ. Angiotensin receptors and neuropathic pain. Pain Rep. 2021;6(1):e869. doi:10.1097/PR9.0000000000000869
13. Bessaguet F, Magy L, Desmoulière A, Demiot C. The therapeutic potential of renin angiotensin aldosterone system (RAAS) in chronic pain: from preclinical studies to clinical trials. Expert Rev Neurother. 2016;16(3):331–339. doi:10.1586/14737175.2016.1150179
14. Bali A, Singh N, Jaggi AS. Renin-angiotensin system in pain: existing in a double life? J Renin Angiotensin Aldosterone Syst. 2014;15(4):329–340. doi:10.1177/1470320313503694
15. Gill D, Georgakis MK, Walker VM, et al. Mendelian randomization for studying the effects of perturbing drug targets. Wellcome Open Res. 2021;6:16. doi:10.12688/wellcomeopenres.16544.1
16. Chesnaye NC, Stel VS, Tripepi G, et al. An introduction to inverse probability of treatment weighting in observational research. Clin Kidney J. 2022;15(1):14–20. doi:10.1093/ckj/sfab158
17. Flint AC, Conell C, Ren X, et al. Effect of systolic and diastolic blood pressure on cardiovascular outcomes. N Engl J Med. 2019;381(3):243–251. doi:10.1056/NEJMoa1803180
18. Evangelou E, Warren HR, Mosen-Ansorena D, et al. Genetic analysis of over 1 million people identifies 535 new loci associated with blood pressure traits. Nat Genet. 2018;50(10):1412–1425. doi:10.1038/s41588-018-0205-x
19. Johnston KJA, Ward J, Ray PR, et al. Sex-stratified genome-wide association study of multisite chronic pain in UK Biobank. PLoS Genet. 2021;17(4):e1009428. doi:10.1371/journal.pgen.1009428
20. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
21. Zhu Z, Zhang F, Hu H, et al. Integration of summary data from GWAS and eQTL studies predicts complex trait gene targets. Nat Genet. 2016;48(5):481–487. doi:10.1038/ng.3538
22. Escobar J, Rawat A, Maradiaga F, et al. Comparison of outcomes between angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers in patients with myocardial infarction: a meta-analysis. Cureus. 2023;15(10):e47954. doi:10.7759/cureus.47954
23. Hollmann C, Fernandes NL, Biccard BM. A systematic review of outcomes associated with withholding or continuing angiotensin-converting enzyme inhibitors and angiotensin receptor blockers before noncardiac surgery. Anesth Analg. 2018;127(3):678–687. doi:10.1213/ANE.0000000000002837
24. Fregoso G, Wang A, Tseng K, Wang J. Transition from acute to chronic pain: evaluating risk for chronic postsurgical pain. Pain Physician. 2019;22(5):479–488.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Circulating Plasma Proteins Influence the Risk of Aortic Dissection via Blood Pressure: A Network Mendelian Randomization and Multi-Omics Study
Li Z, Liu J, Fan X, Shi L, Shi H, Li C, Duan C, Zhang C, Wu Q, Shao Y
Journal of Inflammation Research 2026, 19:600596
Published Date: 31 March 2026