Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Association Between Insulin Regimen and Cardiovascular Risk in Indonesian Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Authors Natsir RM ![]() , Halimah E
, Halimah E ![]() , Diantini A
, Diantini A ![]() , Levita J
, Levita J ![]()
Received 28 March 2026
Accepted for publication 23 May 2026
Published 3 June 2026 Volume 2026:22 611165
DOI https://doi.org/10.2147/TCRM.S611165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Ramdhani M Natsir,1,2,* Eli Halimah,3,4,* Ajeng Diantini,3,4,* Jutti Levita3,4,*
1Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia; 2Department of Medical Laboratory Technology, Maluku Health Polytechnic of the Ministry of Health, Ambon, Indonesia; 3Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia; 4Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, Indonesia
*These authors contributed equally to this work
Correspondence: Jutti Levita, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, 45363, Indonesia, Email [email protected]
Background: Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality among patients with type 2 diabetes mellitus (T2DM). Despite the widespread use of insulin therapy, evidence on how different insulin regimens influence cardiovascular risk stratification remains limited and inconsistent, particularly in Asian populations, including Indonesia.
Purpose: To evaluate the association between insulin regimens and cardiovascular risk, as assessed by the Framingham Risk Score (FRS), among patients with T2DM.
Methods: A cross-sectional study was conducted involving 118 patients with T2DM receiving insulin therapy, including basal insulin therapy and combined basal–prandial insulin therapy. Cardiovascular risk was assessed using the FRS and categorized as low, moderate, or high. Differences between groups were analyzed using the Chi-square test. The association between insulin regimen and cardiovascular risk was evaluated using ordinal logistic regression.
Results: Most patients in both treatment groups were classified as having high cardiovascular risk according to the FRS. After adjustment for potential confounders, the insulin regimen was not significantly associated with cardiovascular risk (OR = 2.14; 95% CI: 0.81– 5.65; p = 0.124). In contrast, the duration of T2DM was significantly associated with cardiovascular risk (OR = 3.63; 95% CI: 1.30– 10.15; p = 0.014).
Conclusion: Cardiovascular risk among patients with T2DM receiving insulin therapy was predominantly moderate to high. The insulin regimen was not significantly associated with cardiovascular risk, whereas the duration of T2DM played a more prominent role in cardiovascular risk stratification.
Keywords: cardiovascular disease, cholesterol, insulin therapy, type 2 diabetes mellitus
Introduction
Type 2 diabetes mellitus (T2DM) has emerged as one of the most significant, fastest-growing global health challenges in the twenty-first century.1 Aging populations, sedentary lifestyles, and rising obesity rates are some factors that significantly enhance the worldwide prevalence of diabetes.2 In 2024, more than 588 million individuals live with DM, and this number is projected to rise substantially over the coming decades.3 Beyond the burden of hyperglycemia itself, the long-term complications associated with T2DM represent a major public health concern. Among these complications, cardiovascular disease (CVD) remains the leading cause of morbidity and mortality in individuals with T2DM, accounting for a substantial proportion of diabetes-related deaths.4 The coexistence of metabolic abnormalities such as dyslipidemia, hypertension, endothelial dysfunction, and chronic low-grade inflammation contributes to accelerated atherosclerosis in this population.5
The pathophysiological relationship between T2DM and CVD is multifactorial and complex. Chronic hyperglycemia promotes oxidative stress, activation of inflammatory pathways, and the formation of advanced glycation end products, all of which contribute to vascular damage.6 In addition, insulin resistance (IR) as a central feature of T2DM leads to disturbances in lipid metabolism, including elevated triglycerides, reduced high-density lipoprotein cholesterol (HDL-C), and increased concentrations of atherogenic lipoproteins.7 These metabolic abnormalities collectively form the characteristic pattern of diabetic dyslipidemia, which plays a critical role in the development of atherosclerotic CVD. Over time, the persistent exposure of vascular tissues to these metabolic disturbances accelerates endothelial dysfunction and plaque formation, thereby increasing the likelihood of adverse cardiovascular events.
Cardiovascular complications are known to develop gradually over many years. Risk prediction models have therefore become important tools in clinical practice for estimating the probability of future cardiovascular events in high-risk patients. Among the available models, the Framingham Risk Score (FRS) is one of the most widely used and validated methods for estimating the 10-year risk of CVD.8 The FRS comprehensively incorporates several established risk factors, including age, sex, total cholesterol (TC), HDL-C, systolic blood pressure, smoking status, and antihypertensive treatment, to generate a comprehensive estimate of cardiovascular risk.9 Owing to its simplicity and clinical applicability, the FRS has been widely adopted for risk stratification in both research and routine clinical care.
Despite its widespread use, evidence evaluating the impact of various antidiabetic treatment strategies particularly insulin regimens, on overall FRS-based cardiovascular risk remains limited. Existing studies have predominantly focused on glycemic outcomes or individual lipid parameters rather than integrated cardiovascular risk prediction models. This highlights the need for studies that specifically evaluate cardiovascular risk using comprehensive and validated prediction tools such as the FRS.
In patients with T2DM, the assessment of cardiovascular risk is particularly important because the disease itself significantly increases the likelihood of cardiovascular events. Many individuals with T2DM already present with multiple risk factors at the time of diagnosis, including hypertension, obesity, and lipid abnormalities. Consequently, evaluating the overall cardiovascular risk profile may provide a more comprehensive understanding of disease prognosis than examining isolated metabolic parameters. Identifying factors associated with higher cardiovascular risk may also guide therapeutic decision-making and help clinicians implement more targeted interventions to reduce long-term complications.
Insulin therapy remains an essential component of the management of T2DM, particularly in patients who fail to achieve adequate glycemic control with oral antidiabetic agents.10 As pancreatic β-cell function progressively declines, many patients eventually require insulin to maintain acceptable glucose levels.11 Different insulin regimens are used in clinical practice depending on patient characteristics and treatment goals. Basal insulin therapy primarily targets fasting plasma glucose by providing a continuous background level of insulin, thereby suppressing hepatic glucose production during fasting.12 In contrast, basal–prandial insulin therapy combines long-acting basal insulin with rapid-acting prandial insulin to control both fasting and postprandial glucose levels, more closely mimicking physiological insulin secretion.13
Beyond glycemic control, insulin therapy may also influence broader metabolic processes that are related to cardiovascular risk. Improved glucose regulation may reduce glucotoxicity and metabolic stress, which in turn may contribute to improvements in lipid metabolism and vascular function.14 However, the extent to which different insulin regimens influence overall cardiovascular risk remains uncertain. While numerous studies have suggested that intensive insulin therapy can improve metabolic parameters associated with CVD,15,16 the relationship between insulin regimen type and global cardiovascular risk assessment has not been fully explored. In particular, most previous investigations have focused primarily on glycemic outcomes or specific lipid biomarkers17–19 rather than on integrated cardiovascular risk prediction models.
Given the high burden of CVD in individuals with T2DM and the widespread use of insulin therapy in clinical practice, understanding the relationship between insulin regimen and cardiovascular risk is of considerable importance. From a clinical perspective, clarifying this relationship is important to support more personalized treatment strategies and help optimize both glycemic control and long-term cardiovascular outcomes. A previous study conducted by our research group has ascertained that basal–prandial insulin regimens were more beneficial in maintaining normal remnant cholesterol (RC) levels when compared to basal insulin alone, although this association was partially mediated by HDL-C, duration of DM, and body mass index.20 However, the study focused on metabolic outcomes and did not comprehensively assess cardiovascular risk using validated prediction models.
To address this gap, the present study extends these findings by evaluating cardiovascular risk using the FRS and incorporating additional clinical variables. This study provides a novelty through a more comprehensive cardiovascular risk assessment, rather than focusing solely on metabolic parameters such as RC. It also incorporates additional clinical variables and updated population characteristics. By applying an integrated cardiovascular risk model, this study aims to provide a more clinically relevant assessment of the impact of insulin regimens. Therefore, this study aimed to compare cardiovascular risk levels based on the FRS between patients with T2DM receiving basal insulin therapy and those receiving combined basal–prandial insulin therapy. In addition, it sought to evaluate the association between insulin regimen type and cardiovascular risk while appraising relevant clinical factors that may influence this relationship.
Methods
Study Design and Setting
This study builds upon our previous research, which compared the associations between basal and basal-prandial insulin regimens on RC and lipid profiles in patients with T2DM.20 The protocol was reviewed and approved by the Research Ethics Committee of Padjadjaran University (ethical approval document number 652/UN6.KEP/EC/2025 dated July 30, 2025, signed by Dr. med. Muhammad Hasan Bashari).
In the present study, an analytical observational design with a cross-sectional approach was used to evaluate the association between insulin regimen and cardiovascular risk among patients with T2DM. The study was conducted at the endocrine outpatient clinic of Dr. Wahidin Sudirohusodo General Hospital, Makassar, Indonesia. Data collection was carried out between August 8 and November 8, 2025. Due to the cross-sectional design, causal relationships cannot be established. This design also limits the ability to assess long-term outcomes.
Study Population and Sample Size
The study population consisted of patients diagnosed with T2DM who were receiving insulin therapy and attending the endocrine clinic during the study period. The minimum required sample size was calculated using the Lemeshow formula for comparison of two proportions. Based on this calculation, 59 patients receiving basal insulin therapy and 59 patients receiving combined basal–prandial insulin therapy were required. Patients were selected using purposive sampling based on predefined inclusion and exclusion criteria. The inclusion criteria were as follows: (1) T2DM patients aged 30–79 years with HbA1c ≥ 9%; (2) receiving either basal insulin therapy or a combination of basal and prandial insulin therapy; (3) availability of laboratory lipid profile data, including TC, LDL cholesterol (LDL-C), and HDL-C, and (4) agreed to participate in the study by signing written informed consent. The exclusion criteria were: (1) use of sodium–glucose cotransporter-2 (SGLT2) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, fibrates, or statins within the previous three months; (2) advanced chronic kidney disease defined as estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2 or patients undergoing dialysis; (3) severe liver dysfunction indicated by alanine aminotransferase (ALT) or aspartate aminotransferase (AST) levels greater than five times the upper limit of normal; (4) use of systemic corticosteroids within the previous month, and (5) pregnant or breastfeeding women. These exclusion criteria were applied to minimize potential confounding from medications and conditions that may influence lipid metabolism and cardiovascular risk; however, residual confounding from unmeasured variables cannot be fully excluded.
Data Collection
Clinical and demographic information was obtained from patients’ medical records. The collected variables included age, sex, body mass index (BMI), duration of T2DM, smoking status, blood pressure, and type of insulin therapy. Information on insulin dosage was also recorded, including the total daily dose (TDD), expressed as international units per kilogram of body weight per day (IU/kg/day). Laboratory data were obtained from routine clinical examinations and included measurements of TC, LDL-C, HDL-C, and calculated RC. These lipid parameters were used as part of the cardiovascular risk assessment. Only patients with complete clinical and laboratory data were included in the final analysis (complete-case analysis).
Study Variables
The primary independent variable in this study was the type of insulin regimen, categorized into two groups: basal insulin therapy and combined basal-prandial insulin therapy. The primary outcome variable was cardiovascular risk, assessed using the FRS, which estimates the 10-year probability of cardiovascular events. Several clinical variables were considered as potential covariates in the analysis, including BMI, TDD, and duration of T2DM. These covariates were selected based on clinical relevance and prior evidence of their association with cardiovascular risk.
Cardiovascular Risk Assessment
Cardiovascular risk was estimated using the FRS, which calculates the 10-year risk of developing CVD based on multiple clinical parameters. The variables included in the FRS calculation were age, sex, TC, HDL-C, systolic blood pressure, smoking status, and antihypertensive treatment. Based on the calculated FRS values, participants were classified into three cardiovascular risk categories: low risk (male: ≤10 points, female: ≤13 points), moderate risk (male: 11–14 points, female: 14–17 points), and high risk (male: ≥15 points, female: ≥18 points). Separate scoring systems were applied for male and female participants according to standard FRS guidelines.20 Although widely used, the FRS was originally developed in Western populations, which may influence its applicability to other populations.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 33.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize baseline characteristics of the study population. Continuous variables were described using mean, standard deviation, median, and interquartile range, while categorical variables were presented as frequencies and percentages. Bivariate analysis was conducted using the Chi-square test to evaluate differences in cardiovascular risk distribution between insulin regimen groups. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to estimate the strength of associations. The relatively small sample size may contribute to wider confidence intervals, reflecting limited statistical power. To further examine factors associated with cardiovascular risk, multivariate analysis was performed using ordinal logistic regression. Variables with p < 0.25 in bivariate analysis and/or strong clinical relevance were included in the multivariate model. Variables considered clinically relevant or showing potential association in bivariate analysis were included in the regression model. Statistical significance was defined as a p-value < 0.05. Given the single-center design and moderate sample size, the findings should be interpreted with caution regarding generalizability and statistical power.
Results
Baseline Characteristics
The baseline demographic and clinical characteristics of the participants are presented in Figure 1. The distribution of patient characteristics between the two treatment groups was generally comparable. In both groups, the majority of participants were male, accounting for 52.5% in the basal insulin group and 57.6% in the basal-prandial group. Most patients were classified as elderly (50–79 years), representing 52.5% of participants in each group. Regarding nutritional status, the majority of patients were categorized as non-obese, with proportions of 57.6% in the basal insulin group and 54.2% in the basal-prandial group.
 |
Figure 1 Baseline demographics and clinical characteristics of T2DM patients receiving (A) combined basal-prandial insulin therapy and (B) only basal insulin therapy. * indicates a statistically significant difference between groups (p = 0.001). |
Most patients had a duration of T2DM of less than 10 years, accounting for 64.4% of individuals in the basal insulin group and 52.5% in the combination therapy group. A similar pattern was observed for smoking status, where the majority of participants in both groups reported no smoking history. Additionally, a high proportion of patients in both groups had elevated blood pressure, with abnormal blood pressure observed in 74.6% of patients receiving basal insulin and 67.8% of those receiving basal-prandial therapy.
In terms of lipid profile parameters, more than half of the patients in the basal insulin group indicated elevated TC levels (57.6%), whereas a slightly larger proportion of patients in the basal-prandial group indicated normal TC levels (54.2%). Most participants in both groups had normal LDL-C levels. However, reduced HDL-C levels were commonly observed in both groups, affecting 83.1% of patients in the basal insulin group and 72.9% of patients in the basal-prandial group. Among all baseline variables examined, only the TDD of insulin showed a statistically significant difference between groups (p = 0.001). Patients receiving basal-prandial therapy were more likely to receive higher insulin doses (≥ 0.5 IU/kg/day) compared with those receiving basal insulin therapy.
The distribution of insulin regimens used in this study is illustrated in Figure 2. Among patients receiving the basal-prandial therapy group, the majority of patients received a combination of insulin degludec and insulin aspart (67.8%), representing the most frequently used regimen among combination therapies. In contrast, within the basal insulin therapy group, insulin detemir was the most commonly used basal insulin (61%), followed by insulin glargine (39%).
 |
Figure 2 Distribution of insulin regimens in T2DM patients receiving (A) combined basal-prandial insulin therapy and (B) only basal insulin therapy. |
Distribution of Continuous Clinical Variables
The distribution of continuous clinical and laboratory variables among the study participants is summarized in Table 1. These variables describe the overall clinical profile of patients with T2DM included in the study population. The mean age of the participants was 59.1 ± 9.0 years, with a range of 30–79 years. The duration of T2DM showed considerable variability across individuals, with a median of 5.0 years (IQR 9.0) and a range of 1–31 years. This indicates considerable variability in disease duration, with a substantial proportion of patients having relatively shorter durations of diabetes.
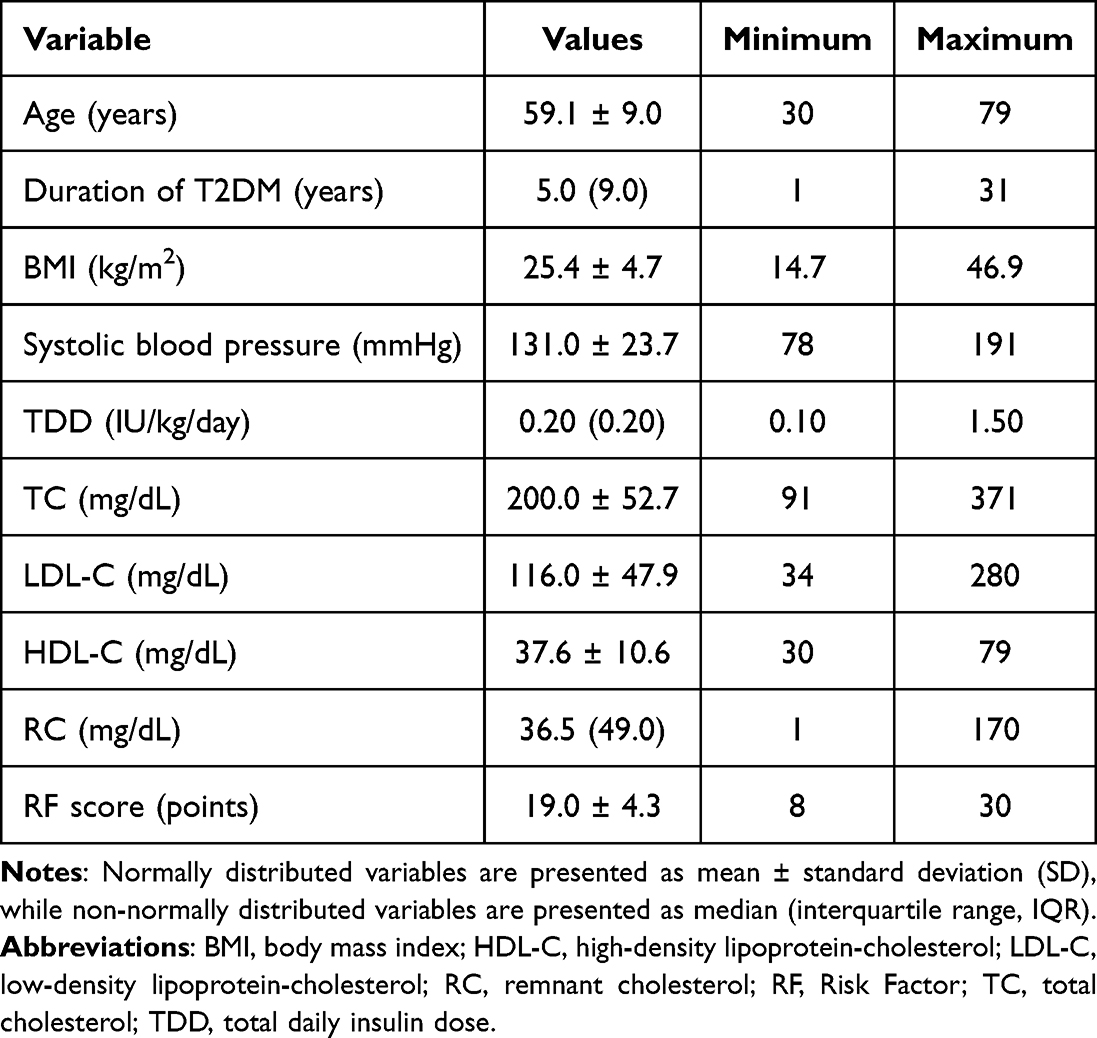 |
Table 1 Distribution of Continuous Clinical and Laboratory Variables Among Patients with T2DM Included in the Study |
Regarding anthropometric measurements, the mean BMI was 25.4 ± 4.7 kg/m2, with values ranging from 14.7 to 46.9 kg/m2, reflecting variability in nutritional status among participants. The mean systolic blood pressure was 131.0 ± 23.7 mmHg, with a range of 78–191 mmHg, suggesting that some patients experienced elevated blood pressure levels. This result is consistent with the known coexistence of hypertension and T2DM.
The TDD of insulin also varied substantially among patients, with a median of 0.20 IU/kg/day (IQR 0.20) and a range of 0.10–1.50 IU/kg/day, indicating variability in insulin requirements. The lipid profile of the study population showed a mean total cholesterol level of 200.0 ± 52.7 mg/dL, LDL cholesterol of 116.0 ± 47.9 mg/dL, and HDL cholesterol of 37.6 ± 10.6 mg/dL. HDL-C values were generally lower than other lipid parameters, which is commonly observed in patients with T2DM.
RC had a median of 36.5 mg/dL (IQR 49.0), with a range of 1–170 mg/dL, indicating substantial variability in atherogenic remnant lipoproteins within the population. Finally, cardiovascular risk assessed using the FRS resulted in a mean value of 19.0 ± 4.3 points, with a range of 8–30 points, suggesting that many participants were classified within moderate to high cardiovascular risk categories, reflecting an integrated assessment of cardiovascular risk rather than isolated metabolic parameters.
Distribution of Cardiovascular Risk
The distribution of cardiovascular risk among patients with T2DM receiving insulin therapy is illustrated in Figure 3. Risk was estimated using the FRS and categorized into low, moderate, and high-risk groups. In the group receiving combined basal-prandial insulin therapy, most patients were classified as having a high cardiovascular risk, accounting for 72.9% of the group. Moderate cardiovascular risk was observed in 20.3% of patients, while only a small proportion (6.8%) were categorized as having low cardiovascular risk.
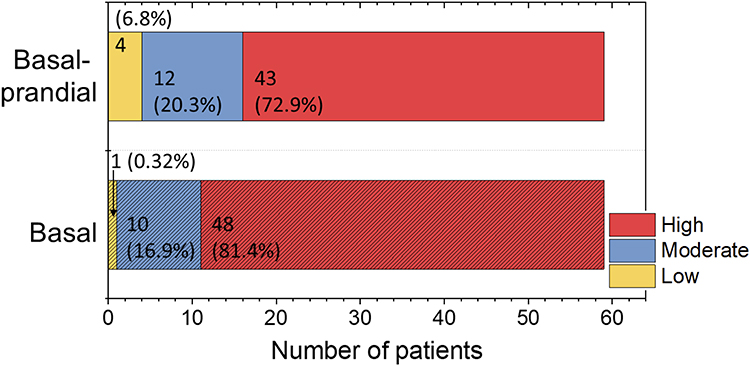 |
Figure 3 Distribution of cardiovascular risk categories based on the FRS in T2DM patients receiving combined basal-prandial and only basal insulin therapy. |
A similar pattern was observed among patients treated with basal insulin alone. The majority of patients in this group also fell into the high risk category (81.4%). Moderate risk was present in 16.9% of patients, whereas only 1.7% were classified as having low cardiovascular risk. Although the basal insulin group showed a slightly higher proportion of patients in the high-risk category compared with the basal-prandial group, statistical analysis indicated that the difference in cardiovascular risk distribution between the two treatment groups was not significant (p = 0.324). These findings indicate that a high cardiovascular risk burden was observed in both groups, regardless of insulin regimen, although the difference between groups was not statistically significant.
Association Between Insulin Regimen and Cardiovascular Risk
The association between insulin regimen and risk category was further evaluated using bivariate analysis. Patients receiving basal insulin therapy showed a higher likelihood of being classified in a higher risk category compared with those receiving combined basal-prandial insulin therapy. This suggests that the observed association should be interpreted with caution, given the lack of statistical significance. The crude odds ratio (OR) was 1.69 (95% CI: 0.71–4.03), indicating that patients treated with basal insulin had approximately 1.7-fold higher odds of having increased risk than those treated with combination therapy. However, the confidence interval (CI) crossed the null value of 1, and the association did not reach statistical significance (p = 0.236), indicating a non-significant trend toward higher cardiovascular risk among patients receiving basal insulin therapy. The forest plot shown in Figure 4 visually represents the estimated OR and its 95% CI for the relationship between insulin regimen and cardiovascular risk. The wide CI indicates considerable variability in the estimate, reflecting heterogeneity within the study population.
 |
Figure 4 Forest plot showing the association between insulin therapy and CVD risk. |
Multivariate Model of Factors Associated with Cardiovascular Risk
To further evaluate factors associated with cardiovascular risk, a multivariate analysis was performed using ordinal logistic regression. The variables included in the model were BMI, TDD, duration of T2DM, and insulin regimen. The results of this analysis are presented in Table 2. Among the variables included in the model, duration of T2DM emerged as the only factor significantly associated with cardiovascular risk. Patients with a longer duration of diabetes had higher odds of being classified into a higher risk category (OR = 3.63; 95% CI: 1.30–10.15; p = 0.014), indicating that the length of time a patient has lived with diabetes may play an important role in determining cardiovascular risk, suggesting a greater influence of cumulative disease exposure compared with treatment modality.
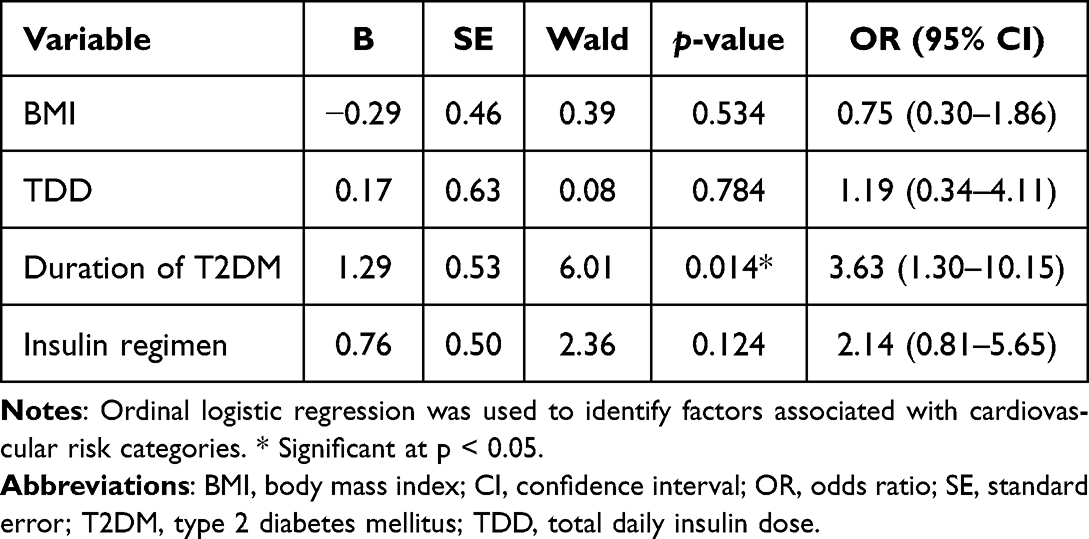 |
Table 2 Factors Associated with Cardiovascular Risk Based on Ordinal Logistic Regression Analysis in Patients with T2DM |
In contrast, other variables included in the model did not demonstrate statistically significant associations. BMI showed an OR of 0.75 (95% CI: 0.30–1.86; p = 0.534), indicating no meaningful relationship between BMI and cardiovascular risk in this analysis. Similarly, TDD showed no significant association (OR = 1.19; 95% CI: 0.34–4.11; p = 0.784). In addition, the insulin regimen variable was not statistically significant in the multivariate model. Patients receiving basal insulin therapy showed higher odds of increased cardiovascular risk compared with those receiving combined basal-prandial therapy (OR = 2.14; 95% CI: 0.81–5.65), but the association was not statistically significant (p = 0.124). This indicates that the insulin regimen was not independently associated with cardiovascular risk after adjustment for other variables.
To explore the crude relationship between insulin regimen and cardiovascular risk before adjustment for other variables, a crude analysis was performed. The results are summarized in Table 3. The crude analysis showed that patients receiving basal insulin therapy had an OR of 1.69 for higher cardiovascular risk compared with those receiving basal-prandial therapy. However, this association was not statistically significant (p = 0.236). These findings are consistent with the multivariate analysis results. These findings suggest that while an insulin regimen alone was not independently associated with cardiovascular risk in this study population, the duration of T2DM appears to be an important factor influencing cardiovascular risk among patients with T2DM, supporting the use of an integrated risk assessment approach and providing incremental evidence that cumulative disease exposure may be more influential than insulin regimen type.
 |
Table 3 Confounding Assessment of Factors Associated with Cardiovascular Risk Based on Ordinal Logistic Regression in Patients with T2DM |
Discussion
Patient Characteristics and Clinical Profile
This study evaluated cardiovascular risk among patients with T2DM receiving different insulin regimens in a clinical setting. The baseline characteristics of the study population indicate that most patients were older adults with long-standing diabetes and multiple metabolic risk factors. Such characteristics are commonly observed in patients who require insulin therapy, as insulin is typically initiated when glycemic control cannot be achieved with oral antidiabetic agents alone.
The average age of participants was approximately 59 years, with many patients categorized as elderly. Aging is known to contribute to the progression of metabolic disturbances and vascular dysfunction, both of which increase the likelihood of cardiovascular complications in patients with diabetes.21 Additionally, the majority of participants exhibited abnormal blood pressure and reduced HDL-C levels, conditions that are frequently associated with insulin resistance and diabetic dyslipidemia.22 These facts reflect the complex cardiometabolic profile commonly observed in individuals with T2DM.
These clinical characteristics suggest that patients receiving insulin therapy already represent a population with elevated baseline cardiovascular risk. Consequently, the management of such patients should not focus solely on glycemic control but also on comprehensive risk reduction strategies targeting multiple cardiovascular risk factors.
Distribution of Cardiovascular Risk in Patients with T2DM
The calculated FRS indicates that a substantial proportion of patients with T2DM were classified within the moderate to high cardiovascular risk categories. This pattern was observed consistently across both insulin regimen groups, suggesting that elevated cardiovascular risk is common among patients with T2DM receiving insulin therapy. The high prevalence of moderate and high cardiovascular risk observed in this study is consistent with the well-established relationship between diabetes and CVD.23 Individuals with T2DM frequently exhibit multiple metabolic abnormalities, including hypertension, dyslipidemia, and chronic hyperglycemia, all of which contribute to the development of atherosclerosis.24 Prolonged exposure to these factors promotes endothelial dysfunction, vascular inflammation, and plaque formation, ultimately increasing the likelihood of cardiovascular events.25
Age and duration of T2DM may further contribute to these risk profiles. Many participants in the present study were older adults with several years of DM history, conditions that are known to accelerate vascular damage.26 Aging itself is associated with structural and functional changes in the vascular system, including increased arterial stiffness and reduced endothelial function. When combined with the metabolic abnormalities associated with DM, these changes may substantially elevate the risk of CVD.
In addition, the coexistence of hypertension and low HDL levels was common in the study population. Both factors are included in cardiovascular risk prediction models, such as the FRS, and are recognized contributors to cardiometabolic risk.27 Their presence may therefore partly explain the predominance of moderate to high cardiovascular risk categories among the participants.
Association Between Insulin Regimen and Cardiovascular Risk
The FRS classification indicates that the type of insulin regimen was not significantly associated with cardiovascular risk categories. Although patients receiving basal insulin therapy showed a slightly higher proportion of individuals in the high cardiovascular risk category (81.4%) compared with those receiving combined basal-prandial therapy (72.9%), the difference between the two groups was not statistically significant. Similarly, the crude OR analysis suggested a tendency toward higher cardiovascular risk among patients treated with basal insulin alone; however, this association did not reach statistical significance. This finding may partly reflect the nature of the FRS model, which primarily incorporates long-term cardiovascular risk determinants such as age, blood pressure, lipid levels, and smoking status. Because these variables represent cumulative cardiometabolic exposure, differences in insulin regimen may have a limited influence on the calculated cardiovascular risk unless they substantially modify these underlying factors over time.
Additionally, the absence of a significant association may be attributed to the relatively short-term metabolic effects of insulin regimens compared with the long-term nature of cardiovascular risk development. While insulin therapy primarily improves glycemic control, its indirect effects on lipid metabolism, blood pressure, and vascular function may require prolonged exposure to produce measurable changes in overall cardiovascular risk. Furthermore, confounding by indication may occur, whereby patients with more severe metabolic disturbances are more likely to receive intensive insulin regimens potentially attenuating observable differences between groups.
From a physiological perspective, insulin therapy mainly acts to regulate glucose metabolism by facilitating cellular glucose uptake and suppressing hepatic glucose production.28 Basal insulin therapy predominantly targets fasting plasma glucose by providing a steady level of circulating insulin throughout the day,29 while basal-prandial regimens include rapid-acting insulin to control postprandial glucose excursions.30 Although these treatment approaches differ in their mechanisms of glycemic regulation, their impact on global cardiovascular risk may be less pronounced when evaluated through risk prediction models that rely heavily on demographic and metabolic parameters.
Previous studies have similarly reported that different insulin formulations generally demonstrate comparable cardiovascular safety profiles. Reviews of insulin therapy indicate that modern insulin analogues do not substantially differ in their effects on major cardiovascular outcomes.31 Observational and comparative studies have also reported similar cardiovascular risk across commonly used basal insulin preparations, suggesting that patient characteristics and underlying cardiometabolic risk factors may play a greater role than the specific insulin regimen itself.32,33 Additionally, patients requiring insulin therapy often share similar clinical profiles, including longer disease duration and greater metabolic disturbance. These factors, together with other cardiovascular risk determinants such as hypertension, dyslipidemia, and obesity, may have a stronger influence on cardiovascular outcomes than differences in insulin regimen.34,35
Conversely, some studies have reported contrasting findings. In these, more intensive insulin regimens were associated with improvements in cardiometabolic parameters, including better lipid profiles and reduced postprandial glucose variability. These discrepancies may be related to differences in study design, population characteristics, follow-up duration and the specific outcomes measured. Studies focusing on short-term metabolic markers may demonstrate benefits, whereas risk prediction models such as the FRS may be less sensitive to these changes.
These findings indicate that while insulin therapy remains essential for glycemic management, the specific insulin regimen alone may not independently determine cardiovascular risk in patients with T2DM. Instead, cardiovascular risk appears to be driven by a combination of demographic characteristics, metabolic abnormalities, and the cumulative burden of disease. In comparison with our previous published study, which demonstrated that basal–prandial insulin regimens were more beneficial in maintaining normal RC levels,20 the current study expands the analysis by evaluating cardiovascular risk using the FRS and incorporating additional covariates with more detailed risk stratification. This approach provides a more integrated assessment of cardiovascular risk compared with studies that focus solely on individual metabolic markers, thereby offering a broader clinical perspective. These differences in study focus and analytical approach may explain the variation in findings and provide a deeper understanding of the role of insulin therapy in cardiovascular risk among patients with T2DM. Taken together, these findings further support the notion that cardiovascular risk in type 2 diabetes is more strongly influenced by cumulative cardiometabolic burden than by the specific insulin regimen alone. This finding contributes to the existing body of evidence by suggesting that diabetes duration may play a more influential role than insulin regimen in determining overall cardiovascular risk.
Role of Diabetes Duration in Cardiovascular Risk
In the multivariate analysis of this study, the duration of T2DM emerged as the only variable significantly associated with cardiovascular risk. Patients with a longer history of DM had markedly higher odds of being categorized into higher cardiovascular risk groups compared with those with shorter disease duration. This observation supports the notion that long-term metabolic exposure may play a more important role in shaping cardiovascular risk than the specific insulin regimen used. The consistency of these findings across analyses supports the internal validity of the results.
The relationship between diabetes duration and CVD has been widely documented. Long-standing diabetes is associated with progressive vascular damage resulting from persistent hyperglycemia, oxidative stress, and chronic inflammation.36 Over time, these mechanisms contribute to endothelial dysfunction and accelerate the formation of atherosclerotic plaques within the arterial wall.37,38 Epidemiological evidence has also shown that longer DM duration significantly increases the risk of cardiovascular complications, including coronary heart disease and myocardial infarction.39,40
Large cohort analyses have reported that each additional five years of diabetes duration is associated with a measurable increase in the incidence of CVD outcomes such as myocardial infarction and stroke.41 Another cohort analysis has reported that longer duration of T2DM is associated with a higher incidence of myocardial infarction even among individuals with relatively controlled lipid levels.42 This observation suggests that the cumulative metabolic exposure associated with long-term DM plays a critical role in the development of cardiovascular complications.
Another explanation for this association lies in the progressive deterioration of metabolic control that often occurs as diabetes advances. With longer disease duration, patients commonly experience worsening insulin resistance, declining β-cell function, and increased difficulty maintaining stable glycemic levels.43 In addition, prolonged diabetes may lead to structural and functional changes in the vascular system, including increased arterial stiffness, impaired endothelial nitric oxide production, and enhanced inflammatory activity within the vascular wall.44 These alterations promote a pro-atherogenic environment that increases susceptibility to cardiovascular events. Consequently, diabetes duration can be considered an indicator of cumulative cardiometabolic exposure rather than merely a measure of time since diagnosis.
This finding further emphasizes that cumulative exposure to metabolic abnormalities over time is a dominant factor in determining cardiovascular risk, surpassing the impact of individual treatment modalities.
In summary, these findings reinforce the importance of early and effective management of T2DM. Identifying patients at earlier stages of the disease and implementing aggressive strategies to control glycemia and other cardiometabolic risk factors may help slow the progression of vascular complications. In this context, the duration of diabetes should be recognized as an important clinical factor when evaluating cardiovascular risk and determining appropriate preventive interventions.
Clinical Implications
The result of this study provides several practical implications for the clinical management of patients with T2DM. Although insulin therapy remains an essential component in achieving glycemic control, the results suggest that the type of insulin regimen alone may not substantially alter the overall cardiovascular risk profile when assessed using the FRS. This observation highlights the importance of adopting a comprehensive approach to cardiovascular risk management in patients with T2DM.
These findings suggest that optimizing cardiovascular risk in patients with T2DM should prioritize long-term risk factor control rather than focusing solely on insulin regimen selection. In clinical practice, treatment decisions for insulin therapy are often guided primarily by glycemic targets. However, the present findings indicate that broader cardiometabolic factors should also be considered when managing patients with diabetes. Risk factors such as hypertension, dyslipidemia, obesity, and smoking status contribute significantly to cardiovascular risk and may have a greater influence on long-term outcomes than the specific insulin regimen used. Therefore, effective cardiovascular risk reduction requires simultaneous management of multiple metabolic abnormalities rather than focusing solely on blood glucose control. Importantly, this study suggests that clinicians should avoid overemphasizing insulin regimen selection as a primary strategy for cardiovascular risk reduction. Instead, greater benefit may be achieved through aggressive management of modifiable risk factors including blood pressure, lipid levels, and lifestyle interventions.
The results also emphasize the importance of early identification and monitoring of cardiovascular risk among patients with diabetes who require insulin therapy. Since many patients in this study were already categorized within moderate to high cardiovascular risk groups, routine cardiovascular risk assessment may help clinicians identify individuals who require more intensive preventive interventions. Such interventions may include stricter blood pressure control, lipid-lowering therapy, lifestyle modification, and patient education aimed at reducing modifiable risk factors.
These results support the concept that comprehensive cardiometabolic management remains the cornerstone of preventing cardiovascular complications in patients with T2DM. While insulin therapy is essential for maintaining glycemic control, optimal outcomes are more likely to be achieved when treatment strategies simultaneously address the multiple risk factors that contribute to CVD.
Furthermore, these results also emphasize the importance of integrating routine cardiovascular risk assessment into diabetes management, which enables the earlier identification of high-risk individuals and the implementation of targeted preventive strategies.
Limitations and Future Perspectives
These factors may also limit the broader impact and generalizability of the findings, and should be considered when interpreting the results. Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design limits the ability to establish causal relationships between insulin regimen and cardiovascular risk. Because exposure and outcome variables were measured at the same point in time, it is not possible to determine whether differences in insulin therapy preceded changes in cardiovascular risk.
Second, the study population was drawn from a single clinical center, which may limit the generalizability of the findings to broader populations. Patients treated in specialized endocrine clinics may have different clinical characteristics compared with those managed in primary care settings or other healthcare environments.
Third, the sample size was relatively modest, which may have limited the statistical power to detect small differences between treatment groups. Although trends were observed in the distribution of cardiovascular risk between insulin regimens, larger studies may be required to confirm whether these differences are clinically meaningful.
Another limitation relates to the variables included in the cardiovascular risk assessment. The FRS relies primarily on traditional risk factors such as age, blood pressure, lipid levels, and smoking status. While this model is widely used in clinical practice, it does not incorporate several other factors that may influence cardiovascular risk in patients with diabetes, including markers of inflammation, insulin resistance, or emerging lipid biomarkers.
Finally, this study did not evaluate additional lipid-related indicators such as apolipoprotein B, apolipoprotein A1, or very-low-density lipoprotein (VLDL) levels. Inclusion of these biomarkers might provide further insight into the complex relationship between insulin therapy, lipid metabolism, and cardiovascular risk in patients with T2DM.
Future research with larger, multicenter populations and prospective study designs is therefore needed to better understand the long-term impact of insulin therapy on cardiovascular outcomes in patients with T2DM.
Conclusion
This study evaluated the association between insulin regimen and cardiovascular risk among patients with T2DM using the FRS. The majority of patients receiving insulin therapy were classified within the moderate to high cardiovascular risk categories, with a high proportion of patients in both basal insulin and basal–prandial groups categorized as high risk. Although patients treated with basal insulin showed a slightly higher proportion of high cardiovascular risk, the difference between the two treatment groups was not statistically significant. Similarly, crude association analysis indicated that patients receiving basal insulin had higher odds of increased cardiovascular risk compared with those receiving basal–prandial therapy, but this association was not statistically significant. Multivariate analysis demonstrated that the type of insulin regimen was not independently associated with cardiovascular risk. In contrast, duration of diabetes emerged as a significant predictor of cardiovascular risk.
These results suggest that cardiovascular risk among patients with T2DM is more strongly influenced by the duration of the disease rather than the specific insulin regimen used. Clinically, this highlights the importance of early and sustained risk factor control including glycemic management and comprehensive cardiovascular risk reduction strategies regardless of insulin regimen. Overall, these conclusions are consistent with the study findings, particularly the absence of a significant association between insulin regimen and cardiovascular risk and the significant role of diabetes duration. However, these findings should be interpreted with caution due to the cross-sectional design and limited sample size which may affect causal inference and generalizability.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Approval and Consent to Participate
This study has been reviewed and approved by the Research Ethics Committee of Padjadjaran University with ethical approval document number 652/UN6.KEP/EC/2025 dated July 30, 2025, signed by Dr. med. Muhammad Hasan Bashari. This study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki. Informed consent was obtained from all participants. In cases where participants had limitations in decision-making capacity or other clinical conditions that prevented them from providing consent directly, consent was obtained from their family members.
Acknowledgments
The author extends their sincere gratitude to the Indonesian Endowment Fund for Education (LPDP), Ministry of Finance of the Republic of Indonesia, for its financial support for this research through scholarship and research funding programs that enabled this study to be conducted. The article processing charge (APC) is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, and managed under the EQUITY Program (document contract number 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025). This study is the dissertation work of the first author in the Doctoral Program in Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran. The authors also thank all reviewers and editors for their valuable feedback that helped improve the quality and clarity of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. The study is funded by the Indonesian Endowment Fund for Education (LPDP), Ministry of Finance of the Republic of Indonesia. 2. The APC is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors declare that there are no conflicts of interest—financial, academic, or personal—related to the research, authorship, or publication of this article.
References
1. Hossain MJ, Al-Mamun M, Islam MR. Diabetes mellitus, the fastest growing global public health concern: early detection should be focused. Health Sci Rep. 2024;7(3):e2004. doi:10.1002/hsr2.2004
2. Xu ST, Sun M, Xiang Y. Global, regional, and national trends in type 2 diabetes mellitus burden among adolescents and young adults aged 10-24 years from 1990 to 2021: a trend analysis from the Global Burden of Disease Study 2021. World J Pediatr. 2025;21(1):73–15. doi:10.1007/s12519-024-00861-8
3. Genitsaridi I, Salpea P, Salim A, et al. 11th edition of the IDF Diabetes Atlas: global, regional, and national diabetes prevalence estimates for 2024 and projections for 2050. Lancet Diabetes Endocrinol. 2026;14(2):149–156. doi:10.1016/S2213-8587(25)00299-2
4. Song DK, Hong YS, Sung YA, et al. Risk factor control and cardiovascular events in patients with type 2 diabetes mellitus. PLoS One. 2024;19(2):e0299035. doi:10.1371/journal.pone.0299035
5. Alshaya OA, Korayem GB, Alghwainm M, et al. The prevalence of cardiovascular diseases, chronic kidney disease, and obesity in patients with type 2 diabetes mellitus and the description of concurrent treatments: a two-center retrospective cross-sectional study in Saudi Arabia. Saudi Pharm J. 2024;32(5):102054. doi:10.1016/j.jsps.2024.102054
6. González P, Lozano P, Ros G, et al. Hyperglycemia and oxidative stress: an integral, updated and critical overview of their metabolic interconnections. Int J Mol Sci. 2023;24(11):9352. doi:10.3390/ijms24119352
7. Flores-Guerrero JL, Been RA, Shalaurova I, et al. Triglyceride/HDL cholesterol ratio and lipoprotein insulin resistance score: associations with subclinical atherosclerosis and incident cardiovascular disease. Clin Chim Acta. 2024;553:117737. doi:10.1016/j.cca.2023.117737
8. Liu Y, Bian W, Li S, et al. Regional variations in cardiovascular risk predictions: a comparative analysis of Framingham, SCORE2, and WHO models across 53 countries. J Glob Health. 2025;15:04323. doi:10.7189/jogh.15.04323
9. Momayyezi M, Sefidkar R, Fallahzadeh H. Agreement between ten-years cardiovascular disease risk assessment tools: an application to Iranian population in Shahedieh Cohort Study. Heliyon. 2023;9(10):e20396. doi:10.1016/j.heliyon.2023.e20396
10. Silver B, Ramaiya K, Andrew SB, et al. EADSG Guidelines: insulin therapy in diabetes. Diabetes Ther. 2018;9(2):449–492. doi:10.1007/s13300-018-0384-6
11. Lu X, Xie Q, Pan X, et al. Type 2 diabetes mellitus in adults: pathogenesis, prevention and therapy. Signal Transduct Target Ther. 2024;9(1):262. doi:10.1038/s41392-024-01951-9
12. Bolli GB, Home PD, Porcellati F, et al. The modern role of basal insulin in advancing therapy in people with type 2 diabetes. Diabetes Care. 2025;48(5):671–681.
13. Natsir RM, Halimah E, Diantini A, et al. Clinical outcomes and complications of basal, bolus, and combination insulin regimens in type 2 diabetes mellitus: evidence from published case reports. Diabetes Metab Syndr Obes. 2025;18:3215–3236. doi:10.2147/DMSO.S545571
14. Wang L, Yan N, Zhang M, et al. The association between blood glucose levels and lipids or lipid ratios in type 2 diabetes patients: a cross-sectional study. Front Endocrinol. 2022;13:969080. doi:10.3389/fendo.2022.969080
15. Kunutsor SK, Balasubramanian VG, Zaccardi F, et al. Glycaemic control and macrovascular and microvascular outcomes: a systematic review and meta-analysis of trials investigating intensive glucose-lowering strategies in people with type 2 diabetes. Diabetes Obes Metab. 2024;26(6):2069–2081. doi:10.1111/dom.15511
16. Pei J, Wang X, Pei Z, et al. Glycemic control, HbA1c variability, and major cardiovascular adverse outcomes in type 2 diabetes patients with elevated cardiovascular risk: insights from the ACCORD study. Cardiovasc Diabetol. 2023;22(1):287. doi:10.1186/s12933-023-02026-9
17. Lu S, Kuang M, Qiu J, et al. Lipids as the link between central obesity and diabetes: perspectives from mediation analysis. BMC Endocr Disord. 2024;24(1):229. doi:10.1186/s12902-024-01764-5
18. Yamaguchi Y, Tanimura-Inagaki K, Fukuda I, et al. Early effects of insulin therapy on cholesterol synthesis and absorption markers in patients with type 2 diabetes. Clinical Nutr Open Sci. 2023;48:64–74. doi:10.1016/j.nutos.2023.03.001
19. Hatif ZS, Abbassi HA, Mohammed HR, et al. Impact of antidiabetic medications on inflammatory markers and adiponectin levels: a cross-sectional study in Iraqi patients with type2 diabetes. Egypt J Intern Med. 2025;37:139. doi:10.1186/s43162-025-00529-3
20. Natsir RM, Halimah E, Diantini A, Levita J, Umar H. Comparative association of basal and basal-prandial insulin regimens on remnant cholesterol and lipid profiles in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2026;19:588522. doi:10.2147/DMSO.S588522
21. García-Vega D, González-Juanatey JR, Eiras S. Diabesity in elderly cardiovascular disease patients: mechanisms and regulators. Int J Mol Sci. 2022;23(14):7886. doi:10.3390/ijms23147886
22. Patial R, Batta I, Thakur M, et al. Etiology, pathophysiology, and treatment strategies in the prevention and management of metabolic syndrome. Arch Intern Med Res. 2024;7(4):273–283. doi:10.26502/aimr.0184
23. Dziopa K, Asselbergs FW, Gratton J, et al. Cardiovascular risk prediction in type 2 diabetes: a comparison of 22 risk scores in primary care settings. Diabetologia. 2022;65(4):644–656. doi:10.1007/s00125-021-05640-y
24. Lu SX, Wu TW, Chou CL, et al. Combined effects of hypertension, hyperlipidemia, and diabetes mellitus on the presence and severity of carotid atherosclerosis in community-dwelling elders: a community-based study. J Chin Med Assoc. 2023;86(2):220–226. doi:10.1097/JCMA.0000000000000839
25. Xue C, Chen K, Gao Z, et al. Common mechanisms underlying diabetic vascular complications: focus on the interaction of metabolic disorders, immuno-inflammation, and endothelial dysfunction. Cell Commun Signal. 2023;21(1):298. doi:10.1186/s12964-022-01016-w
26. Yao X, Zhang J, Zhang X, et al. Age at diagnosis, diabetes duration and the risk of cardiovascular disease in patients with diabetes mellitus: a cross-sectional study. Front Endocrinol. 2023;14:1131395. doi:10.3389/fendo.2023.1131395
27. Okoh P, Olusanya DA, Erinne OC, et al. An integrated pathophysiological and clinical perspective of the synergistic effects of obesity, hypertension, and hyperlipidemia on cardiovascular health: a systematic review. Cureus. 2024;16(10):e72443. doi:10.7759/cureus.72443
28. Li M, Chi X, Wang Y, et al. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduct Target Ther. 2022;7(1):216. doi:10.1038/s41392-022-01073-0
29. Singh AK, Singh A, Singh R, et al. Once-weekly basal insulin icodec: looking ONWARDS from pharmacology to clinical trials. Diabetes Metab Syndr. 2022;16(9):102615. doi:10.1016/j.dsx.2022.102615
30. Dehghani M, Sadeghi M, Barzkar F, et al. Efficacy and safety of premixed versus basal-bolus regimens as intensification of insulin therapy in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized clinical trials. J Diabetes Investig. 2025;16(5):827–841. doi:10.1111/jdi.70002
31. Rajput R, Mukherjee JJ, Vageesh AS, et al. The impact of cardiovascular outcome trials on the choice of insulins in the management of type 2 diabetes mellitus: an expert review. Clinical Diabetol via Medica. 2018;7(5):234–246. doi:10.5603/DK.2018.0024
32. Yang CT, Li KY, Yang CY, et al. A nationwide cohort study for comparative vascular safety of long-acting insulin analogue versus intermediate-acting human insulin in type 2 diabetes. Sci Rep. 2021;11(1):4152. doi:10.1038/s41598-021-83253-6
33. Brunetti VC, Ohy Y, Platt RW, et al. The association of long-acting insulin analogue use versus neutral protamine Hagedorn insulin use and the risk of major adverse cardiovascular events among individuals with type 2 diabetes: a population-based cohort study. Diabetes Obes Metab. 2022;24(11):2169–2181. doi:10.1111/dom.14802
34. Młynarska E, Bojdo K, Frankenstein H, et al. Endothelial dysfunction as the common pathway linking obesity, hypertension and atherosclerosis. Int J Mol Sci. 2025;26(20):10096. doi:10.3390/ijms262010096
35. Mannucci E, Targher G, Nreu B, et al. Effects of insulin on cardiovascular events and all-cause mortality in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Nutr, Metab Cardiovasc Dis. 2022;32(6):1353–1360. doi:10.1016/j.numecd.2022.03.007
36. Morton JI, Lazzarini PA, Polkinghorne KR, et al. The association of attained age, age at diagnosis, and duration of type 2 diabetes with the long-term risk for major diabetes-related complications. Diabet Res Clin Pract. 2022;190:110022. doi:10.1016/j.diabres.2022.110022
37. Zhao N, Yu X, Zhu X, et al. Diabetes mellitus to accelerated atherosclerosis: shared cellular and molecular mechanisms in glucose and lipid metabolism. J Cardiovasc Transl Res. 2024;17(1):133–152. doi:10.1007/s12265-023-10470-x
38. Maruhashi T, Higashi Y. Pathophysiological association between diabetes mellitus and endothelial dysfunction. Antioxidants. 2021;10(8):1306. doi:10.3390/antiox10081306
39. Gao X, Yang HH, Xie F, et al. Diabetes duration, glycemic control, and risk of stroke and stroke subtypes: a nationwide prospective cohort study. Sci Rep. 2025;15(1):43633. doi:10.1038/s41598-025-27547-z
40. Yang HH, Li FR, Chen ZK, et al. Duration of diabetes, glycemic control, and risk of heart failure among adults with diabetes: a cohort study. J Clin Endocrinol Metab. 2023;108(5):1166–1172. doi:10.1210/clinem/dgac642
41. de Jong M, Woodward M, Peters SAE. Duration of diabetes and the risk of major cardiovascular events in women and men: a prospective cohort study of UK Biobank participants. Diabet Res Clin Pract. 2022;188:109899. doi:10.1016/j.diabres.2022.109899
42. Kim MK, Lee KN, Han K, et al. Diabetes duration, cholesterol levels, and risk of cardiovascular diseases in individuals with type 2 diabetes. J Clin Endocrinol Metab. 2024;109(12):e2317–e2323. doi:10.1210/clinem/dgae092
43. Rasouli N, Younes N, Ghosh A, et al. Longitudinal effects of glucose-lowering medications on β-cell responses and insulin sensitivity in type 2 diabetes: the GRADE randomized clinical trial. Diabetes Care. 2024;47(4):580–588. doi:10.2337/dc23-1070
44. Staef M, Ott C, Kannenkeril D, et al. Determinants of arterial stiffness in patients with type 2 diabetes mellitus: a cross-sectional analysis. Sci Rep. 2023;13(1):8944. doi:10.1038/s41598-023-35589-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Traditional Blood Lipid Indices for Metabolism Dysfunction-Associated Fatty Liver Disease Prediction in Non-Obese Type 2 Diabetes Mellitus
Gao Q, Feng L, Zhou W, Li X, Yin L, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2345-2354
Published Date: 7 August 2023
Influence of Low-Density Lipoprotein Cholesterol Levels on NSAID-Associated Cardiovascular Risks After Myocardial Infarction: A Population-Based Cohort Study

Basem M, Bonnesen K, Pedersen L, Sørensen HT, Schmidt M
Clinical Epidemiology 2024, 16:281-291
Published Date: 22 April 2024
Association Between Glycated Hemoglobin and the Lipid Profile at the Central Yunnan Plateau: A Retrospective Study
Luo B, Xu W, Ye D, Bai X, Wu M, Zhang C, Shi R
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2975-2981
Published Date: 9 August 2024
Systemic Predictors of Diabetic Retinopathy and Diabetic Macular Edema in an Adult Veteran Population
Tran EM, Gregori NZ, Rachitskaya A, Nandan A, Pershing S, Goldberg JL
Clinical Ophthalmology 2025, 19:101-110
Published Date: 8 January 2025