Back to Journals » Journal of Inflammation Research » Volume 19
Association Between Complete Blood Cell Count (CBC)-Derived Inflammatory Markers and Natural Killer Cell Activity: A Cross-Sectional Study
Authors Cho AR, Oh H, Suh E, Jeon JH, Moon J, Cho BH, Lee YK ![]()
Received 17 September 2025
Accepted for publication 24 January 2026
Published 4 February 2026 Volume 2026:19 557260
DOI https://doi.org/10.2147/JIR.S557260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anh Ngo
A-Ra Cho,1,* Hyoju Oh,2,* Eunkyung Suh,2 Joo-Hwan Jeon,2 Junhyung Moon,3 Baek Hwan Cho,3 Yun-Kyong Lee2
1Department of Family Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, 06273, Republic of Korea; 2Chaum Life Center, CHA University, Seoul, 06062, Republic of Korea; 3Department of Biomedical Informatics, CHA University School of Medicine, CHA University, Seongnam, 13488, Republic of Korea
*These authors contributed equally to this work
Correspondence: Baek Hwan Cho, Department of Biomedical Informatics, CHA University School of Medicine, CHA University, Seongnam, 13488, Republic of Korea, Tel +82-10-8704-5768, Email [email protected] Yun-Kyong Lee, Department of Family Medicine, Chaum Life Center, CHA University, Seoul, 06062, Republic of Korea, Tel +82-2-3015-5575 ; +82-10-3220-5202, Email [email protected]
Introduction: This study investigated the association between natural killer cell activity (NKA) and five complete blood cell count (CBC)-derived inflammatory markers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI).
Methods: This cross-sectional study included a total of 10,329 individuals who underwent CBC and NKA tests at Chaum Life Center in Korea between January 2016 and May 2022. NKA was estimated by measuring the amount of interferon-gamma (IFN-γ) released by activated natural killer cells; low NKA was defined as IFN-γ level < 500 pg/mL.
Results: The results showed a significant increase in the percentage of subjects with low NKA with increasing CBC-derived inflammatory markers. The odds ratios (ORs) for low NKA were 3.90 (3.45– 4.41), 2.69 (2.38– 3.05), 1.45 (1.29– 1.63), 2.96 (2.62– 3.35), and 4.80 (4.23– 5.45) in the highest quartile of NLR, PLR, MLR, SIRI, and SII, respectively, compared to the lowest quartile. Moreover, NLR, SIRI, and SII showed higher discriminatory performance for low NKA compared with traditional inflammatory markers, such as C-reactive protein (CRP) and white blood cell (WBC) count.
Conclusion: These findings indicate that CBC-derived inflammatory markers are associated with low NKA in a large health-screening population, suggesting their potential relevance as indicators of immune–inflammatory status.
Keywords: natural killer cell activity, inflammatory marker, complete blood cell count, inflammation, innate immunity
Introduction
Natural killer (NK) cells are a key component of the innate immune system, responsible for identifying and destroying virus-infected and malignant cells without prior sensitization.1 Natural killer cell activity (NKA) has emerged as a critical indicator of immune competence, influencing both immunity and disease progression. In clinical practice, NK cell dysfunction has been linked to a variety of conditions, including many types of cancers, autoimmune diseases, and chronic infections.2–4 Given the role of NK cells in immune surveillance, understanding factors associated with variations in NKA may contribute to improved immune monitoring.
Conventional NKA measurement methods, such as flow cytometric assays or chromium-51 release assays, require isolation of peripheral blood mononuclear cells and involve substantial technical complexity, limiting their applicability in large-scale clinical studies.5 A whole-blood–based assay that measures the amount of interferon-gamma (IFN-γ) released from activated NK cells has been available for over a decade and has been widely used in clinical practice for NKA assessment.6 Previous studies have shown that decreased NKA measured using this assay is associated with the presence and prognosis of various cancers,7,8 as well as systemic inflammatory markers including white blood cell (WBC) count and C-reactive protein (CRP).9
Complete blood cell count (CBC)-derived inflammatory markers, which are routinely measured in clinical settings, have recently gained attention as composite indices that integrate information from multiple immune cell populations and may reflect systemic inflammatory and immune status. Markers such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), and systemic inflammation response index (SIRI) have been shown to correlate with inflammation in various pathological conditions, including many types of cancers,10,11 cardiovascular diseases,12–15 neurological diseases,16 autoimmune disorders,17,18 and overall mortality.19,20 Since neutrophils, monocytes, lymphocytes, and platelets play distinct yet complementary roles in inflammatory and immune responses,21,22 composite indices derived from their ratios or combinations are considered to provide a more integrated assessment of systemic inflammatory-immune status than single-cell parameters alone.23,24
To date, there has been limited research examining how these CBC-derived inflammatory markers are associated with innate immune function, particularly NK cell activity, in large population-based settings. Understanding the relationship between NKA and CBC-based inflammatory indices may provide insight into immune–inflammatory interactions at the population level. Accordingly, the present study investigated the association between NKA and multiple CBC-derived inflammatory markers and compared their performance in relation to NKA with that of traditional inflammatory markers, such as WBC count and CRP.
Materials and Methods
Study Design and Population
This cross-sectional study analyzed health check-up data from Chaum Life Center, a single health-screening center in Seoul, Republic of Korea. The data were obtained from the electronic medical records, and were de-identified and extracted by the institution for analysis. The investigators did not have direct access to the full database, and no additional data cleaning or imputation procedures were performed. We screened subjects who underwent NKA assay from January 2016 to May 2022 (n = 11,251). Among the 11,251 eligible subjects, we excluded 29 subjects under 18 years of age. Then, we further excluded individuals with 1) a history of malignant disease or autoimmune disease, such as rheumatoid arthritis or inflammatory bowel disease (n = 563); 2) recent use of steroid, non-steroidal anti-inflammatory drugs (NSAIDs), or immuno-suppressants (n = 237); 3) missing data of CBC (n = 93). After these exclusions, a total of 10,329 subjects were included in the analysis. Missing data were handled using a complete-case analysis approach, and the study flow diagram is presented in Figure 1.
 |
Figure 1 Flow chart of the selection of the study population. |
This study was approved by the Institutional Review Board of CHA Bundang Medical Center (CHAMC 2022–09-045). The study protocol conformed to the ethical guidelines of the 1964 Declaration of Helsinki and its subsequent amendments. Also, the study conductance and manuscript were drafted according to the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines for cross-sectional studies.
Data Collection
Body weight (to the nearest 0.1 kg) and height (to the nearest 0.1 cm) were measured while the subjects wore lightweight clothing and no shoes. Body mass index (BMI) was calculated as the ratio of weight (kg) to height squared (m2). Blood samples were collected from the antecubital vein in the morning after at least 8 hours of fasting. The complete blood cell count (CBC) was measured using XN-10 Hematology Analyzer (Sysmex, IL, USA), which count the number of blood cells (red blood cell, WBC, and platelet) and WBC differential counts (neutrophil, lymphocyte, and monocyte) in a given volume of blood. CRP was measured using the Hitachi 7600 Analyzer (Hitachi Co., Tokyo, Japan). Smoking status, drinking status, and exercise habits of the participants were obtained from a self-reported questionnaire. Smoking and drinking status were categorized into three groups, respectively: current smoker/drinker, former smoker/drinker, or never smoker/drinker. We defined regular exercise as regularly exercising more than two days a month. Hypertension was defined as a systolic blood pressure of ≥140 mmHg, a diastolic blood pressure of ≥90 mmHg, or treatment with anti-hypertensive medication.25 Diabetes mellitus was defined as follows: a fasting plasma glucose level of ≥126 mg/dL; glycosylated hemoglobin of ≥6.5%; or treatment with oral anti-diabetic medication or insulin therapy.26
Assessment of CBC-Derived Inflammatory Markers
We calculated five CBC-derived inflammatory markers as follows: NLR = neutrophil counts/lymphocyte counts, PLR = platelet counts/lymphocyte counts, MLR = monocyte counts/lymphocyte counts, SIRI = (neutrophil counts × monocyte counts)/lymphocyte counts, SII = (platelet counts × neutrophil counts)/lymphocyte counts.23,24
IFN-γ Measurement for NKA
Natural killer (NK) cell activity was assessed by quantifying interferon-gamma (IFN-γ) secretion using a commercially available blood test (NK Vue® Kit, NKMAX, Seongnam, Korea). For this assay, 1 mL of peripheral whole blood was collected directly into a specialized tube (Promoca®, NKMAX, Seongnam, Korea) containing a proprietary cytokine stimulant that selectively activates NK cells. The tube was gently mixed within 30 minutes of collection and then incubated at 37.0 °C for 20 to 24 hours. During incubation, the stimulant induces IFN-γ release primarily from NK cells, with minimal contribution from other immune cells.6,27,28 After incubation, the supernatant was separated by centrifugation at 3000 × g for 3 minutes, and IFN-γ levels were measured in pg/mL using an enzyme-linked immunosorbent assay (ELISA). According to the manufacturer’s validation data, the assay demonstrated acceptable precision, with inter-assay coefficients of variation below 10% across different sessions, operators, laboratories, days, and reagent lots.29 Low NK cell activity was defined as an IFN-γ level below 500 pg/mL, based on previously published clinical studies using the same whole-blood assay and manufacturer-recommended thresholds, in which this cut-off has been associated with impaired immune function and adverse clinical outcomes.7,9
Statistical Analysis
All data were presented as means ± standard deviations for continuous variables and as numbers (percentages) for categorical variables. Differences in clinical characteristics between participants with normal and low NKA were analyzed using the independent t-test for continuous variables and the chi-square test for categorical variables. We categorized the participants into four groups according to quartiles of each CBC-derived inflammatory marker. The odds ratios (OR) and 95% confidence intervals (CI) for low NKA of Q2, Q3, and Q4 compared to Q1, as the reference, were calculated by using multiple logistic regression analysis after adjusting for potential confounding variables. Non-linear relationship between CBC-derived markers and NKA was assessed by comparing a linear model with a generalized additive model using penalized splines. P-values for non-linearity were obtained from a F-test comparing the two models. Furthermore, to compare the discriminatory performance of CBC-derived inflammatory markers with that of traditional inflammatory markers (WBC count and CRP) for low NKA, we calculated receiver operating characteristic (ROC) curves and compared the areas under the ROC curves (AUROC). Sensitivity analyses were also performed using alternative cut-off values for low NKA (IFN-γ level below 250 pg/mL and 100 pg/mL). All statistical analyses were conducted using SPSS statistical software (version 25.0, SPSS Inc., Chicago, IL, USA) and R (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria). A p-value of <0.05 was considered statistically significant.
Results
Clinical Characteristics of the Study Population
Table 1 represents the clinical characteristics of the study population. Participants with low NKA showed significantly higher age, CRP levels, WBC, neutrophil, monocyte, platelet counts, and five CBC-derived inflammatory markers, and higher proportions of current smokers and current drinkers. The mean lymphocyte count and proportion of regular exercise were significantly lower in subjects with low NKA. The mean BMI and proportions of male sex, hypertension, and diabetes mellitus showed no significant differences between subjects with normal and low NKA.
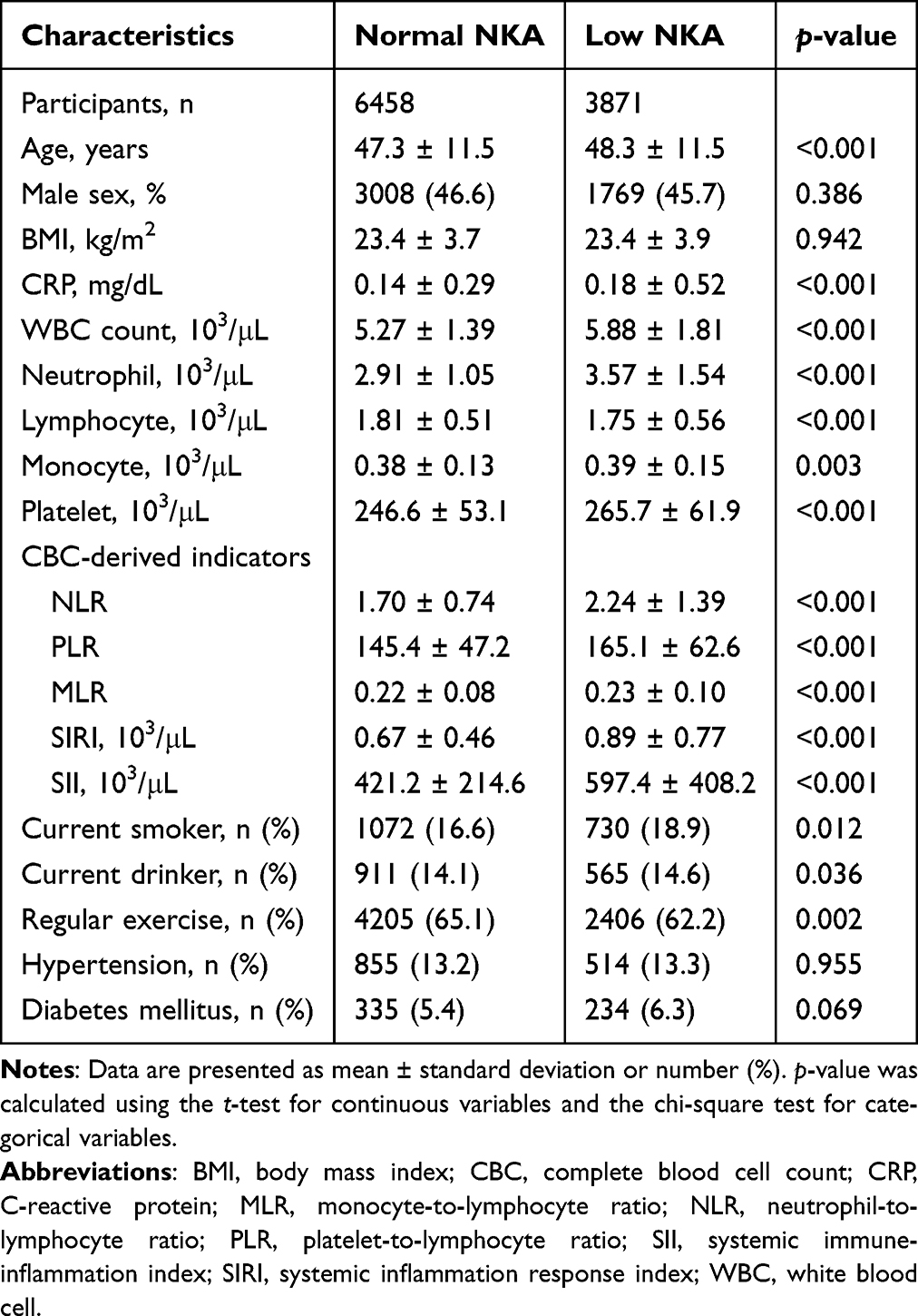 |
Table 1 Clinical Characteristics of the Study Population |
Relationship Between CBC-Derived Inflammatory Markers and Low NKA
Figure 2 shows the proportion of subjects with low NKA according to quartiles of NLR, PLR, MLR, SIRI, and SII. The proportion of low NKA increased with higher CBC-derived inflammatory indices for all indices (p for trend <0.05 by the Cochran–Armitage test).
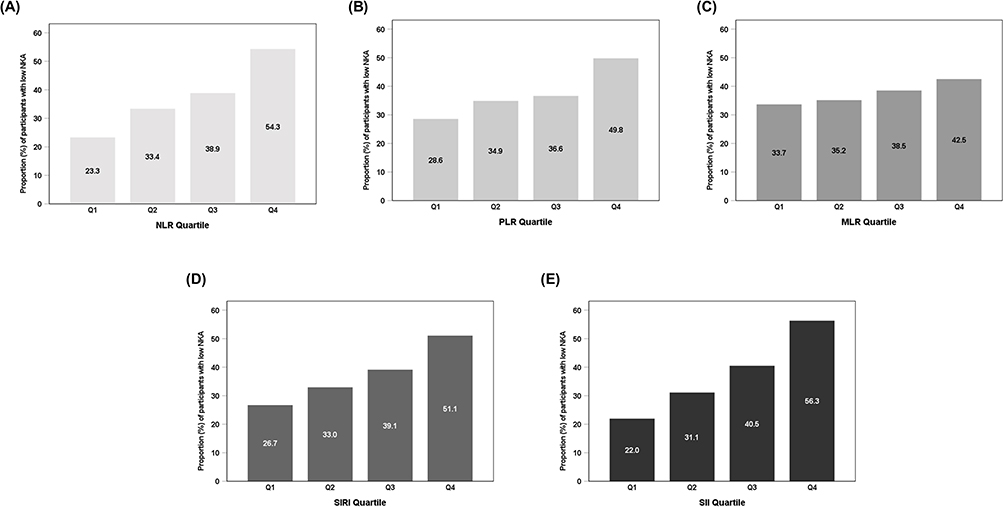 |
Figure 2 The proportion of subjects with low NKA according to each quartile of CBC-derived inflammatory markers. (A) NLR; (B) PLR; (C) MLR; (D) SIRI; (E) SII. |
Table 2 presents the ORs (95% CIs) for low NKA according to the quartiles of each CBC-derived inflammatory marker. Compared to the lowest quartile, the multivariable-adjusted ORs (95% CIs) for low NKA were 3.90 (3.45–4.41) in the highest quartile of NLR, 2.69 (2.38–3.05) in the highest quartile of PLR, 1.45 (1.29–1.63) in the highest quartile of MLR, 2.96 (2.62–3.35) in the highest quartile of SIRI, and 4.80 (4.23–5.45) in the highest quartile of SII, respectively, after adjusting for age, sex, BMI, smoking status, drinking status, regular exercise, hypertension, and diabetes mellitus. Although these estimates should be interpreted cautiously given the cross-sectional design, the observed effect sizes indicate a meaningful gradient in the likelihood of low NKA across increasing levels of CBC-derived inflammatory markers. Sensitivity analyses using alternative cut-off values for low NKA yielded results consistent with the primary analysis (Supplementary Table S1).
 |
Table 2 Odds Ratios for Low NKA According to Quartiles of Complete Blood Cell Count (CBC)-Derived Inflammatory Markers |
When NKA was analyzed as a continuous variable using generalized additive models, significant non-linear associations were observed for NLR, PLR, SIRI, and SII (all p for non-linearity <0.0001), whereas no evidence of non-linearity was found for MLR (p for non-linearity >0.1) (Figure 3).
 |
Figure 3 Spline curves between CBC-derived inflammatory markers and continuous NKA. Generalized additive models with penalized splines were used to examine potential non-linear associations between CBC-derived inflammatory markers and continuous NKA. Solid lines represent fitted spline curves, and shaded areas indicate 95% confidence intervals. (A) NLR; (B) PLR; (C) MLR; (D) SIRI; (E) SII. |
Comparison of the Discriminatory Performance of CBC-Derived Inflammatory Markers for Low NKA
Figure 4 and Table 3 present the comparative discriminatory performance of traditional inflammatory markers (CRP and WBC) and CBC-derived inflammatory markers for low NKA. The AUROCs of CRP, WBC, NLR, PLR, MLR, SIRI, and SII were 0.534, 0.601, 0.645, 0.595, 0.544, 0.616, and 0.667, respectively. Among the evaluated markers, SII exhibited the largest AUROC, followed by NLR and SIRI. Pairwise comparisons of AUROCs demonstrated statistically significant differences between SII and other CBC-derived inflammatory markers (Supplementary Table S2). Compared with CRP, the AUROCs of NLR, PLR, SIRI, and SII were significantly higher, whereas no significant difference was observed between MLR and CRP. In addition, the AUROCs of NLR, MLR, SIRI, and SII were significantly higher than that of WBC, while no significant difference was observed between PLR and WBC.
 |
Table 3 Comparison of AUROCs of CBC-Derived Inflammatory Markers and Traditional Inflammatory Markers (CRP and WBC) for Low NKA |
 |
Figure 4 Comparison of the discriminatory performance of CBC-derived inflammatory markers and traditional inflammatory markers (CRP and WBC) for low NKA. Key CBC-derived inflammatory markers (SII, NLR, and SIRI) are highlighted in the legend; other indices are shown for reference. |
Discussion
This study explored the relationship between CBC-derived inflammatory markers and NKA in a large cohort of healthy individuals. The findings suggest that higher levels of certain inflammatory markers, such as SII, NLR, and SIRI, were significantly associated with reduced NKA. These findings are consistent with an association between systemic inflammatory status and immune dysfunction, particularly in relation to lower NK cell activity, an important component of immune surveillance and host defense.
Many studies have already shown that elevated levels of CBC-derived inflammatory markers (SII, NLR, and SIRI) are associated with a higher risk of cancer development and poor prognosis. Several studies have shown that higher SII scores are correlated with poor prognosis in cancers such as gastric cancer,30 cervical cancer,31 and Hodgkin lymphoma,32 where they are linked to increased tumor progression and metastasis. Similarly, NLR, a simple and cost-effective marker, has been associated with poor cancer outcomes by reflecting the balance between neutrophils and lymphocytes. Higher NLR ratios have been linked to adverse outcomes in non-small cell lung cancer,33 cholangiocarcinoma,34 and colorectal cancer.35 Elevated SIRI has been found to reflect immune dysfunction and has been identified as a valuable marker for evaluating immune suppression, particularly in cancers like pancreatic cancer,24 colorectal cancer,36 and breast cancer.37 From all these previous studies, inflammation is believed to be linked to immunosuppression, which in turn is related to cancer occurrence. The results of this study indicate that higher inflammatory marker levels are associated with lower NKA, a functional measure of innate immune activity.
Beyond cancer, elevated NLR, SIRI, and SII have also been widely recognized as markers associated with cardiovascular and metabolic diseases. Elevated SII, NLR and SIRI have been linked to increased cardiovascular mortality and adverse outcomes, particularly in conditions like acute coronary syndrome, as they reflect systemic inflammation and immune dysregulation.38,39 Similarly, SIRI has shown prognostic value in predicting cardiovascular mortality.40 In metabolic diseases, a higher NLR has been associated with diabetic mortality,41 SII and SIRI related to complications such as diabetic retinopathy42 highlighting their role in chronic inflammation-driven pathologies. Obesity and metabolic syndrome is also positively associated with SII and SIRI in adults43 and NLR, SII, SIRI with children.44
Although studies directly linking CBC-derived inflammatory markers to NKA are limited, it was previously demonstrated that reduced NKA levels correlate with elevated inflammatory markers, including neutrophil counts and NLR,9 as well as with a higher resting heart rate, a physiological indicator of increased sympathetic activity and stress.45 These observations suggest that reduced NKA may be associated with heightened systemic inflammation. From a biological perspective, chronic inflammatory environments have been shown to impair NK cell function through cytokine-mediated mechanisms, including suppression of activating receptors and reduced IFN-γ production.1,46 Sustained inflammatory signaling may also promote functional exhaustion of NK cells, characterized by diminished effector capacity and altered immune regulation.47 These mechanisms provide biological plausibility for the observed association between elevated inflammatory markers and lower NKA, without implying a causal relationship. In the present study, a larger sample size was incorporated and a broader range of inflammatory markers, including MLR, PLR, SIRI, and SII, was simultaneously evaluated. In addition, the comparative assessment of these CBC-derived inflammatory markers in relation to NKA demonstrated that SII showed relatively stronger discriminatory performance than other indices, although the overall predictive ability remained modest.
While CRP and WBC count are commonly used to assess systemic inflammation, their utility as sole indicators of NKA remains controversial. One study indicated that while the NLR was significant, CRP levels did not significantly correlate with NKA, suggesting that CRP may not be a reliable marker for assessing NKA.48 In this context, CBC-derived inflammatory markers (NLR, SII, and SIRI) showed greater discriminatory ability for low NKA than traditional inflammatory markers such as CRP and WBC count, with SII demonstrating the highest AUROC among the evaluated indices. This finding aligns with previous studies demonstrating that SII, which integrates neutrophil, lymphocyte, and platelet counts, provides a comprehensive assessment of the inflammatory-immune balance and has shown superior predictive value in various inflammatory-related conditions.23,49,50 While CRP and WBC are widely used to assess inflammation, CBC-derived inflammatory markers are derived from standard hematologic parameters and therefore may be conveniently assessed in routine laboratory data, particularly in observational or population-based studies.
Despite the significance of our findings, several limitations should be acknowledged. First, this study was conducted at a single health-screening center, which may limit the representativeness and generalisability of the results. Second, NKA was assessed using an IFN-γ–based assay without direct measurement of NK cell counts; however, this assay offers practical advantages for large-scale studies. Third, residual confounding cannot be fully excluded, as information on acute illness or transient medical conditions at the time of examination was unavailable. In addition, although this study was supported by institutional funding and employed a commercially available assay, neither the funder nor the manufacturer had any role in the study design, analysis, interpretation, or manuscript preparation; nonetheless, the possibility of residual bias cannot be entirely ruled out. Finally, the cross-sectional design precludes causal inference, and future longitudinal and mechanistic studies are needed to clarify temporal and biological relationships between inflammatory markers and NK cell activity.
Conclusions
In conclusion, this study demonstrates that CBC-derived inflammatory markers, particularly NLR, SIRI, and SII, are associated with lower NKA in a health check-up population. These indices may serve as simple and accessible indicators reflecting immune–inflammatory status in observational and research settings. The present findings highlight an association rather than establishing clinical applicability or predictive utility. While CBC-derived inflammatory markers, especially SII, show potential usefulness for identifying individuals with low NKA, further longitudinal and mechanistic studies are required before these markers can inform screening strategies or personalized clinical decision-making.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Approval and Informed Consent
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board of CHA Bundang Medical Center (CHAMC 2022-09-045). Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We thank all researchers and subjects who participated in this study.
Author Contributions
A-RC: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Conceptualization. HO: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. ES: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. J-HJ: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. JM: Writing – review & editing, Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. BC: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Funding acquisition, Conceptualization. Y-KL: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Funding acquisition, Conceptualization.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
A-Ra Cho and Hyoju Oh contributed equally to this work and share first authorship. Baek Hwan Cho and Yun-Kyong Lee are co-corresponding authors.
Funding
This research was supported in part by the Institute of Information & Communications Technology Planning & Evaluation (IITP) grant funded by the Korea government (MSIT) (No. RS-2024-00357879, AI-based Biosignal Fusion and Generation Technology for Intelligent Personalized Chronic Disease Management), the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. NRF2023R1A2C2003577), and NKMAX Co., Ltd. (grant number 2021-09-047).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Vivier E, Raulet DH, Moretta A, et al. Innate or adaptive immunity? The example of natural killer cells. Science. 2011;331(6013):44–11. doi:10.1126/science.1198687
2. Liu M, Liang S, Zhang C. NK cells in autoimmune diseases: protective or pathogenic? Front Immunol. 2021;12:624687. doi:10.3389/fimmu.2021.624687
3. Shin E, Bak SH, Park T, et al. Understanding NK cell biology for harnessing NK cell therapies: targeting cancer and beyond. Front Immunol. 2023;14:1192907. doi:10.3389/fimmu.2023.1192907
4. Cao WJ, Zhang XC, Wan LY, et al. Immune dysfunctions of CD56(neg) NK cells are associated with hiv-1 disease progression. Front Immunol. 2021;12:811091. doi:10.3389/fimmu.2021.811091
5. Valiathan R, Lewis JE, Melillo AB, Leonard S, Ali KH, Asthana D. Evaluation of a flow cytometry-based assay for natural killer cell activity in clinical settings. Scand J Immunol. 2012;75(4):455–462. doi:10.1111/j.1365-3083.2011.02667.x
6. Lee SB, Cha J, Kim IK, et al. A high-throughput assay of NK cell activity in whole blood and its clinical application. Biochem Biophys Res Commun. 2014;445(3):584–590. doi:10.1016/j.bbrc.2014.02.040
7. Lee J, Park KH, Ryu JH, et al. Natural killer cell activity for IFN-gamma production as a supportive diagnostic marker for gastric cancer. Oncotarget. 2017;8(41):70431–70440. doi:10.18632/oncotarget.19712
8. Lee HS, Leem G, Kang H. Peripheral natural killer cell activity is associated with poor clinical outcomes in pancreatic ductal adenocarcinoma. J Gastroenterol Hepatol. 2021;36(2):516–522. doi:10.1111/jgh.15265
9. Lee YK, Haam JH, Cho SH, Kim YS. Cross-sectional and time-dependent analyses on inflammatory markers following natural killer cell activity. Diagnostics. 2022;12(2). doi:10.3390/diagnostics12020448
10. Shoji F, Kozuma Y, Toyokawa G, Yamazaki K, Takeo S. Complete blood cell count-derived inflammatory biomarkers in early-stage non-small-cell lung cancer. Ann Thorac Cardiovasc Surg. 2020;26(5):248–255. doi:10.5761/atcs.oa.19-00315
11. Nanava N, Betaneli M, Giorgobiani G, Chikovani T, Janikashvili N. Complete blood count derived inflammatory biomarkers in patients with hematologic malignancies. Georgian Med News. 2020(302):39–44.
12. Balta S, Celik T, Mikhailidis DP, et al. The relation between atherosclerosis and the neutrophil-lymphocyte ratio. Clin Appl Thromb Hemost. 2016;22(5):405–411. doi:10.1177/1076029615569568
13. Balta S, Ozturk C. The platelet-lymphocyte ratio: a simple, inexpensive and rapid prognostic marker for cardiovascular events. Platelets. 2015;26(7):680–681. doi:10.3109/09537104.2014.979340
14. Bhat T, Teli S, Rijal J, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013;11(1):55–59. doi:10.1586/erc.12.159
15. Haybar H, Pezeshki SMS, Saki N. Evaluation of complete blood count parameters in cardiovascular diseases: an early indicator of prognosis? Exp Mol Pathol. 2019;110:104267. doi:10.1016/j.yexmp.2019.104267
16. Novellino F, Donato A, Malara N, Madrigal JL, Donato G. Complete blood cell count-derived ratios can be useful biomarkers for neurological diseases. Int J Immunopathol Pharmacol. 2021;35:20587384211048264. doi:10.1177/20587384211048264
17. Tiucă OM, Morariu SH, Mariean CR, Tiucă RA, Nicolescu AC, Cotoi OS. Impact of blood-count-derived inflammatory markers in psoriatic disease progression. Life. 2024;14(1):114. doi:10.3390/life14010114
18. Tutan D, Doğan AG. Pan-immune-inflammation index as a biomarker for rheumatoid arthritis progression and diagnosis. Cureus. 2023;15(10):e46609. doi:10.7759/cureus.46609
19. Tang Y, Zhai Y, Song W, et al. Association between complete blood count-derived inflammatory markers and the risk of frailty and mortality in middle-aged and older adults. Front Public Health. 2024;12:1427546. doi:10.3389/fpubh.2024.1427546
20. Ke J, Qiu F, Fan W, Wei S. Associations of complete blood cell count-derived inflammatory biomarkers with asthma and mortality in adults: a population-based study. Front Immunol. 2023;14:1205687. doi:10.3389/fimmu.2023.1205687
21. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
22. Koupenova M, Clancy L, Corkrey HA, Freedman JE. Circulating platelets as mediators of immunity, inflammation, and thrombosis. Circ Res. 2018;122(2):337–351. doi:10.1161/circresaha.117.310795
23. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.Ccr-14-0442
24. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
25. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. The task force for the management of arterial hypertension of the european society of cardiology (ESC) and the european society of hypertension (ESH)]. G Ital Cardiol. 2018;19(11 Suppl 1):3s–73s. doi:10.1714/3026.30245
26. Care D. 2. classification and diagnosis of diabetes: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S14–s31. doi:10.2337/dc20-S002
27. Koo KC, Shim DH, Yang CM, et al. Reduction of the CD16(-)CD56bright NK cell subset precedes NK cell dysfunction in prostate cancer. PLoS One. 2013;8(11):e78049. doi:10.1371/journal.pone.0078049
28. Nederby L, Jakobsen A, Hokland M, Hansen TF. Quantification of NK cell activity using whole blood: methodological aspects of a new test. J Immunol Methods. 2018;458:21–25. doi:10.1016/j.jim.2018.04.002
29. NK Vue® Kit: instructions for use. Seoul, Republic of Korea: NKMAX Co. Ltd.; 2023.
30. Wang Q, Zhu D. The prognostic value of systemic immune-inflammation index (SII) in patients after radical operation for carcinoma of stomach in gastric cancer. J Gastrointest Oncol. 2019;10(5):965–978. doi:10.21037/jgo.2019.05.03
31. Huang H, Liu Q, Zhu L, et al. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci Rep. 2019;9(1):3284. doi:10.1038/s41598-019-39150-0
32. Mirili C, Paydas S, Kapukaya TK, Yılmaz A. Systemic immune-inflammation index predicting survival outcome in patients with classical Hodgkin lymphoma. Biomarker Med. 2019;13(18):1565–1575. doi:10.2217/bmm-2019-0303
33. Diem S, Schmid S, Krapf M, et al. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. 2017;111:176–181. doi:10.1016/j.lungcan.2017.07.024
34. Beal EW, Wei L, Ethun CG, et al. Elevated NLR in gallbladder cancer and cholangiocarcinoma - making bad cancers even worse: results from the US extrahepatic biliary malignancy consortium. HPB. 2016;18(11):950–957. doi:10.1016/j.hpb.2016.08.006
35. Nakamoto S, Ohtani Y, Sakamoto I, Hosoda A, Ihara A, Naitoh T. Systemic immune-inflammation index predicts tumor recurrence after radical resection for colorectal cancer. Tohoku J Exp Med. 2023;261(3):229–238. doi:10.1620/tjem.2023.J074
36. Cai H, Chen Y, Zhang Q, Liu Y, Jia H. High preoperative CEA and systemic inflammation response index (C-SIRI) predict unfavorable survival of resectable colorectal cancer. World J Surg Oncol. 2023;21(1):178. doi:10.1186/s12957-023-03056-z
37. Zhang S, Cheng T. Prognostic and clinicopathological value of systemic inflammation response index (SIRI) in patients with breast cancer: a meta-analysis. Ann Med. 2024;56(1):2337729. doi:10.1080/07853890.2024.2337729
38. Gürdal A, Serin E, Sarilar M, et al. Prognostic value of systemic immune-inflammation index in older patients with acute coronary syndrome. Coron Artery Dis. 2025;36(6):e45–e52. doi:10.1097/mca.0000000000001496
39. Karadeniz FÖ, Karadeniz Y, Altuntaş E. Systemic immune-inflammation index, and neutrophilto-lymphocyte and platelet-to-lymphocyte ratios can predict clinical outcomes in patients with acute coronary syndrome. Cardiovasc J Afr. 2023;34:1–7. doi:10.5830/cvja-2023-011
40. Fan W, Wei C, Liu Y, et al. The prognostic value of hematologic inflammatory markers in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Clin Appl Thromb Hemost. 2022;28:10760296221146183. doi:10.1177/10760296221146183
41. Dong G, Gan M, Xu S, Xie Y, Zhou M, Wu L. The neutrophil-lymphocyte ratio as a risk factor for all-cause and cardiovascular mortality among individuals with diabetes: evidence from the NHANES 2003-2016. Cardiovasc Diabetol. 2023;22(1):267. doi:10.1186/s12933-023-01998-y
42. Wang S, Pan X, Jia B, Chen S. Exploring the correlation between the systemic immune inflammation index (SII), systemic inflammatory response index (SIRI), and type 2 diabetic retinopathy. Diabetes Metab Syndr Obes. 2023;16:3827–3836. doi:10.2147/dmso.S437580
43. Zhou Y, Wang Y, Wu T, Zhang A, Li Y. Association between obesity and systemic immune inflammation index, systemic inflammation response index among US adults: a population-based analysis. Lipids Health Dis. 2024;23(1):245. doi:10.1186/s12944-024-02240-8
44. Nicoară DM, Munteanu AI, Scutca AC, et al. Assessing the relationship between systemic immune-inflammation index and metabolic syndrome in children with obesity. Int J Mol Sci. 2023;24(9):8414. doi:10.3390/ijms24098414
45. Oh H, Cho AR, Jeon JH, et al. Association between resting heart rate and low natural killer cell activity: a cross-sectional study. Front Immunol. 2024;15:1465953. doi:10.3389/fimmu.2024.1465953
46. Raveney BJ, Copland DA, Dick AD, Nicholson LB. TNFR1-dependent regulation of myeloid cell function in experimental autoimmune uveoretinitis. J Immunol. 2009;183(4):2321–2329. doi:10.4049/jimmunol.0901340
47. Bi J, Tian Z. NK cell exhaustion. Front Immunol. 2017;8:760. doi:10.3389/fimmu.2017.00760
48. Kim BR, Chun S, Cho D, Kim KH. Association of neutrophil-to-lymphocyte ratio and natural killer cell activity revealed by measurement of interferon-gamma levels in a healthy population. J Clin Lab Anal. 2019;33(1):e22640. doi:10.1002/jcla.22640
49. Morikawa S, Okumura K, Inoue N, Ogane T, Takayama Y, Murohara T. Systemic immune-inflammation index as a predictor of prognosis after carotid artery stenting compared with C-reactive protein. PLoS One. 2023;18(7):e0288564. doi:10.1371/journal.pone.0288564
50. Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8–19. doi:10.4103/tjem.tjem_198_23
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
New Inflammatory Marker Associated with Disease Activity in Gouty Arthritis: The Systemic Inflammatory Response Index
Jiang Y, Tu X, Liao X, He Y, Wang S, Zhang Q, Qing Y
Journal of Inflammation Research 2023, 16:5565-5573
Published Date: 24 November 2023