Back to Journals » Clinical Epidemiology » Volume 15
Association Between Autoimmune Diseases and Sarcopenia: A Two-Sample Mendelian Randomization Study
Authors Su Q ![]() , Jin C
, Jin C ![]() , Yang Y
, Yang Y ![]() , Wang J, Wang J, Zeng H, Chen Y, Zhou J, Wang Y
, Wang J, Wang J, Zeng H, Chen Y, Zhou J, Wang Y
Received 1 May 2023
Accepted for publication 27 July 2023
Published 25 August 2023 Volume 2023:15 Pages 901—910
DOI https://doi.org/10.2147/CLEP.S416778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lars Pedersen
Qing Su,1 Chen Jin,2 Yi Yang,1 Jingxian Wang,1 Juejin Wang,1 Hao Zeng,1 Yaqing Chen,1 Junxi Zhou,1 Yi Wang1
1Department of Epidemiology and Biostatistics, School of Public Health and Management, Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Department of Epidemiology, Center for Global Health, School of Public Health, Nanjing Medical University, Nanjing, People’s Republic of China
Correspondence: Yi Wang, Department of Epidemiology and Biostatistics, School of Public Health and Management, Wenzhou Medical University, Chashan High Education Zone, Wenzhou, Zhejiang, 325035, People’s Republic of China, Tel +86-577-8669-9358, Email [email protected]
Purpose: Observational studies have reported that autoimmune diseases are closely related to sarcopenia, but the causalities of autoimmune diseases with sarcopenia have not been established. We conducted this Mendelian randomization (MR) study to reveal the causal associations of overall autoimmune disease and five common autoimmune diseases with sarcopenia-related traits.
Methods: The publicly available summary-level data of autoimmune diseases and three sarcopenia-related traits were used for analysis. The causal effects of autoimmune diseases on sarcopenia-related traits were first identified in discovery samples using the inverse-variance-weighted method as the primary method, and the robustness of results was examined by additional sensitivity analyses. Replication MR analyses were then conducted using replication samples of five autoimmune diseases. Finally, the possibility of reverse causation was assessed by reverse MR analyses.
Results: In both the discovery and replication samples, we identified potential causal effects of rheumatoid arthritis (RA) on appendicular lean mass (ALM) and low grip strength (OR = 0.979, 95% CI: 0.964– 0.995 for ALM; OR = 1.042, 95% CI: 1.013– 1.072 for low grip strength), but not on walking pace. We also found that inflammatory bowel disease (IBD) and type 1 diabetes (T1D) were only causally negatively associated with ALM in the discovery stage (OR = 0.986, 95% CI: 0.974– 0.999 for IBD; OR = 0.987, 95% CI: 0.975– 0.999 for T1D), whereas systemic lupus erythematosus, multiple sclerosis, and overall autoimmune disease were not associated with any of the three sarcopenia-related traits. Additionally, reverse MR analysis only found an association between walking pace and overall autoimmune disease, but this association did not remain in the weighted-median method.
Conclusion: This study demonstrates that RA is causally associated with low grip strength and reduced ALM, and that IBD and T1D may be causally negatively related to ALM.
Keywords: Mendelian randomization, autoimmune disease, sarcopenia, rheumatoid arthritis, grip strength, appendicular lean mass
Introduction
Sarcopenia, a condition characterized by decreased muscle mass and function, is related to adverse health consequences, including frailty, falls, and increased mortality.1 Currently, a single diagnostic criterion for sarcopenia has not been established, and according to different diagnostic standards, the prevalence of sarcopenia in individuals older than 60 years varies between 10% and 27%.2 Sarcopenia is generally considered an age-related condition, but patients with some disorders were found to have a higher prevalence of sarcopenia, including autoimmune diseases.3–5
Autoimmune diseases refer to conditions in which the immune system incorrectly generates immunologic responses that damage self-tissues, and the persistent chronic inflammation that it causes may be a risk factor for sarcopenia.5 Several epidemiological studies have found a higher prevalence of sarcopenia in patients with type 1 diabetes (T1D), inflammatory bowel disease (IBD), rheumatoid arthritis (RA), multiple sclerosis (MS), and systemic lupus erythematosus (SLE) compared with healthy controls.6–10 Notably, the association between RA and sarcopenia has been relatively well studied, with many observational studies demonstrating a strong relationship between RA and sarcopenia.11 In addition, there appear to be some shared biological processes between autoimmune diseases and sarcopenia. For example, pro-inflammatory cytokines including interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) cause loss of skeletal muscle, and they are also closely related to the development of autoimmune diseases.12–15 However, the causality of autoimmune diseases with sarcopenia has not been established, as observational studies are inevitably affected by residual confounding and reverse causation.
Mendelian randomization (MR) is a method for inferring causality between exposure and outcome. Here, we used two-sample MR analysis to evaluate causal associations of overall autoimmune disease and five common autoimmune diseases (RA, SLE, IBD, MS, and T1D) with sarcopenia-related traits [appendicular lean mass (ALM), walking pace, and grip strength].
Materials and Methods
Study Design
Figure 1 shows the overall study design. To reliably infer the causal relationships between autoimmune diseases and sarcopenia-related traits, we tried to satisfy three key assumptions of MR approach. First, the instrumental variables (IVs) are correlated with autoimmune diseases. Second, IVs are unrelated to confounders affecting this relationship. Third, IVs influence sarcopenia-related traits only through autoimmune diseases.16
 |
Figure 1 The study design and workflow of the present MR study. Abbreviations: GWAS, genome-wide association study; SLE, systemic lupus erythematosus; RA, rheumatoid arthritis; MS, multiple sclerosis; IBD, inflammatory bowel disease; T1D, type 1 diabetes; IVs, instrumental variables; MR, Mendelian randomization; SNP, single-nucleotide polymorphism. |
Data Sources of Autoimmune Diseases
In the discovery stage, genome-wide association study (GWAS) summary statistics for SLE (5201 cases and 9066 controls) were drawn from the study by Bentham et al;17 the summary-level data of RA (14,361 cases and 43,923 controls) were extracted from the study by Okada et al;18 the genetic data of IBD (12,882 cases and 21,770 controls) were obtained from the study by Liu et al;19 the summary statistics of MS (14,498 cases and 24,091 controls) came from the International MS Genetics Consortium (IMSGC);20 and the summary data of T1D (6683 cases and 12,173 controls) were derived from the study by Onengut-Gumuscu et al.21 More details are available in the original publications.17–21
In addition, the GWAS summary data of overall autoimmune disease in FinnGen consortium R5 considering forty-five autoimmune diseases (42,202 cases and 176,590 controls) were used to explore the causality between overall autoimmune disease and sarcopenia-related traits. The forty-five autoimmune diseases included in overall autoimmune disease are shown in Supplementary Table S1.
The replication samples for SLE (538 cases and 213,145 controls), RA (6236 cases and 147,221 controls), IBD (3753 cases and 210,300 controls), MS (1048 cases and 217,141 controls), and T1D (2542 cases and 182,573 controls) were derived from the FinnGen consortium R5, but no other available GWAS data for overall autoimmune disease were found. The sources and corresponding information on the discovery and replication samples are listed in Supplementary Table S2.
Data Sources of Sarcopenia-Related Traits
The European Working Group on Sarcopenia in Older People (EWGSOP) defines sarcopenia by three parameters: low muscle strength (such as grip strength), low muscle quantity, and low physical performance (such as gait speed).22 Therefore, we included the three sarcopenia-related traits of ALM, low hand grip strength, and walking pace as our study outcomes.
GWAS summary statistics for ALM were drawn from UK Biobank, including 450,243 participants.23 ALM was measured by determining the sum of fat-free mass of the arms and legs by bioelectrical impedance analysis. The genetic data of walking pace were also obtained from UK Biobank (n = 459,915), which captured data on walking pace through touch-screen questionnaires. The summary data for low hand grip strength were derived from the GWAS meta-analysis comprising 22 cohorts with 48,596 cases and 207,927 controls.24 Low grip strength was defined depending on EWGSOP criteria (Male: < 30 kg, Female: < 20 kg). The sources and corresponding information on outcomes are listed in Supplementary Table S2.
Instrumental Variable Selection
A series of single-nucleotide polymorphisms (SNPs) screening steps were performed to ensure the reliability of the conclusions on the causal associations between autoimmune diseases and sarcopenia. First, IVs that attained genome-wide significance threshold were selected (P < 5.0×10−8). Second, independent SNPs were retained by the PLINK clumping method (r2 < 0.001, kb = 10,000). Third, we searched the PhenoScanner website and removed SNPs associated with confounders (type 2 diabetes, body mass index, weight, hip circumference, waist circumference, height, smoking, blood pressure, blood lipids, coronary artery disease, hypothyroidism, heel bone mineral density, knee pain, irritable bowel syndrome, Hodgkin’s lymphoma, and number of self-reported non-cancer illnesses) and other autoimmune diseases (P < 5.0×10−8). Fourth, palindromic SNPs were excluded. Finally, SNPs not available in the outcome datasets or SNPs with inconsistent alleles between exposures and outcomes (eg, T/C vs T/G) were removed.
Statistical Analysis
The causalities of autoimmune diseases and sarcopenia-related traits were primarily calculated by inverse-variance-weighted (IVW) method. To test the heterogeneity, we conducted Cochran’s Q test. If heterogeneity was significant (P < 0.05), we used random-effects IVW and, conversely, fixed-effects IVW. The robustness of results was examined by two methods of sensitivity analysis: MR-robust adjusted profile score (MR-RAPS) method and weighted-median (WM) method. The former can make robust inferences when weak IVs are included, and the latter yields valid estimates of causal effects when less than half of SNPs are invalid instruments.25,26 MR-Egger regression was used for assessment of pleiotropy.27 MR-Pleiotropy RESidual Sum and Outlier (MR-PRESSO) detected outliers, and the results before and after eliminating outliers were tested for differences.28 In addition, we calculated the F-statistics (formula: R2 / K × (N − K − 1) / (1 − R2)) for the SNPs.29
The replication MR analyses were performed using replication samples of five autoimmune diseases. Finally, reverse MR analyses were conducted with sarcopenia-related traits as exposures and autoimmune diseases from FinnGen samples as outcomes. “TwoSampleMR” and “MR-PRESSO” packages were used for analyses in R program (version 4.2.2).
Results
Selection of Instrumental Variables
In discovery samples, a total of 45, 60, 65, 49, 36, and 53 independent SNPs were related to SLE, RA, IBD, MS, T1D, and overall autoimmune disease (P < 5.0 × 10−8, r2 < 0.001), respectively. After removing SNPs associated with possible confounders, palindromic SNPs, SNPs not present in any of the three sarcopenia-related trait datasets, and SNPs with inconsistent alleles between exposures and outcomes, 24 SLE-associated SNPs, 26 RA-associated SNPs, 31 IBD-associated SNPs, 22 MS-associated SNPs, 12 T1D-associated SNPs, and 22 overall autoimmune disease-associated SNPs were included in the analysis. The excluded SNPs and the detailed reasons for removing these SNPs are listed in Supplementary Table S3, and the characteristics of the SNPs finally retained in the analysis are shown in Supplementary Table S4-S9. No SNPs with F-statistic <10, indicating that the estimates were unlikely to suffer from weak IV bias. Replication samples were screened following the same SNP screening procedure, ultimately retaining 2 SLE-associated SNPs, 3 RA-associated SNPs, 5 IBD-associated SNPs, 3 MS-associated SNPs, and 3 T1D-associated SNPs in replication samples.
Causal Effects of Autoimmune Diseases on Appendicular Lean Mass
In the discovery stage, the IVW analysis indicated that RA (OR = 0.979, 95% CI: 0.964–0.995, P = 0.0084), IBD (OR = 0.986, 95% CI: 0.974–0.999, P = 0.0346), and T1D (OR = 0.987, 95% CI: 0.975–0.999, P = 0.0331) were negatively related to ALM (Figure 2). Similar estimates were yielded with both two sensitivity methods in associations of RA and T1D with ALM, whereas the MR-RAPS method found no statistical significance in the association between IBD and ALM (Figure 2). In addition, IVW, WM, and MR-RAPS methods detected that SLE, MS, and overall autoimmune disease were unrelated to ALM (Figure 2). The scatter plot across MR analyses of autoimmune diseases and ALM is presented in Supplementary Figure S1. There was one SNP each associated with ALM in RA, T1D, MS and overall autoimmune disease (P < 5.0×10−8). The sensitivity analysis of removing SNPs associated with ALM found that the results remained stable, and the negative associations of RA (OR = 0.983, 95% CI: 0.970–0.997, P = 0.0187) and T1D (OR = 0.990, 95% CI: 0.985–0.995, P = 0.0001) with ALM still existed. Cochran’s Q test found heterogeneity in SLE, RA, IBD, MS, T1D, and overall autoimmune disease (P < 0.05, Supplementary Table S10), so we used random-effects IVW model. MR-Egger regression found pleiotropy only in IBD (intercept P = 0.004 for IBD), but MR-PRESSO found outliers in SLE, RA, IBD, MS, T1D, and overall autoimmune disease (Supplementary Table S10). MR-PRESSO distortion tests indicated non-significant difference between the estimates before and after eliminating outliers for SLE, IBD, MS, and T1D (P > 0.05), while the difference was significant in RA and overall autoimmune disease (P = 0.015 for RA and P = 0.039 for overall autoimmune disease).
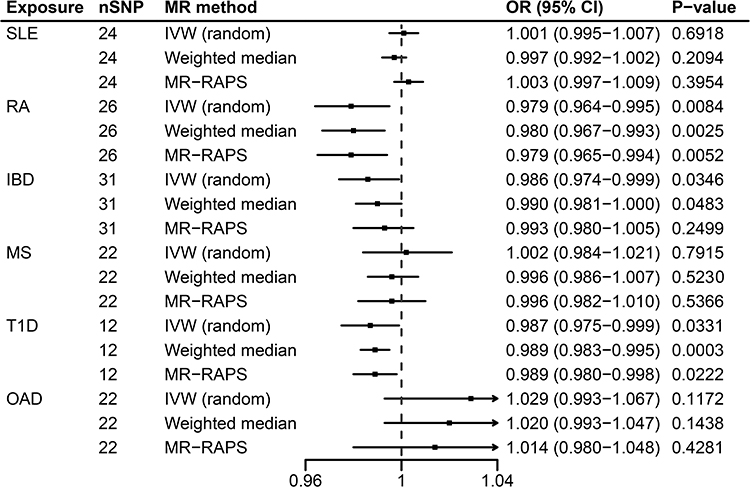 |
Figure 2 MR analysis of associations between autoimmune diseases and appendicular lean mass in discovery samples. Abbreviations: SLE, systemic lupus erythematosus; RA, rheumatoid arthritis; MS, multiple sclerosis; IBD, inflammatory bowel disease; T1D, type 1 diabetes; OAD, overall autoimmune disease; nSNP, number of single-nucleotide polymorphisms; MR, Mendelian randomization; IVW, inverse-variance-weighted; MR-RAPS, MR-robust adjusted profile score; OR, odds ratio; CI, confidence interval. |
In replication samples, the causal effect of RA on ALM was successfully replicated, and the direction of the effect was consistent with that of the discovery stage (Table 1 and Supplementary Table S11). Based on the above results, although the association between RA and ALM was found to be potentially affected by outliers in MR-PRESSO analysis of discovery samples, it is reasonable to believe that RA has a negative causal effect on ALM. However, the associations of IBD and T1D with ALM failed to replicate in replication samples.
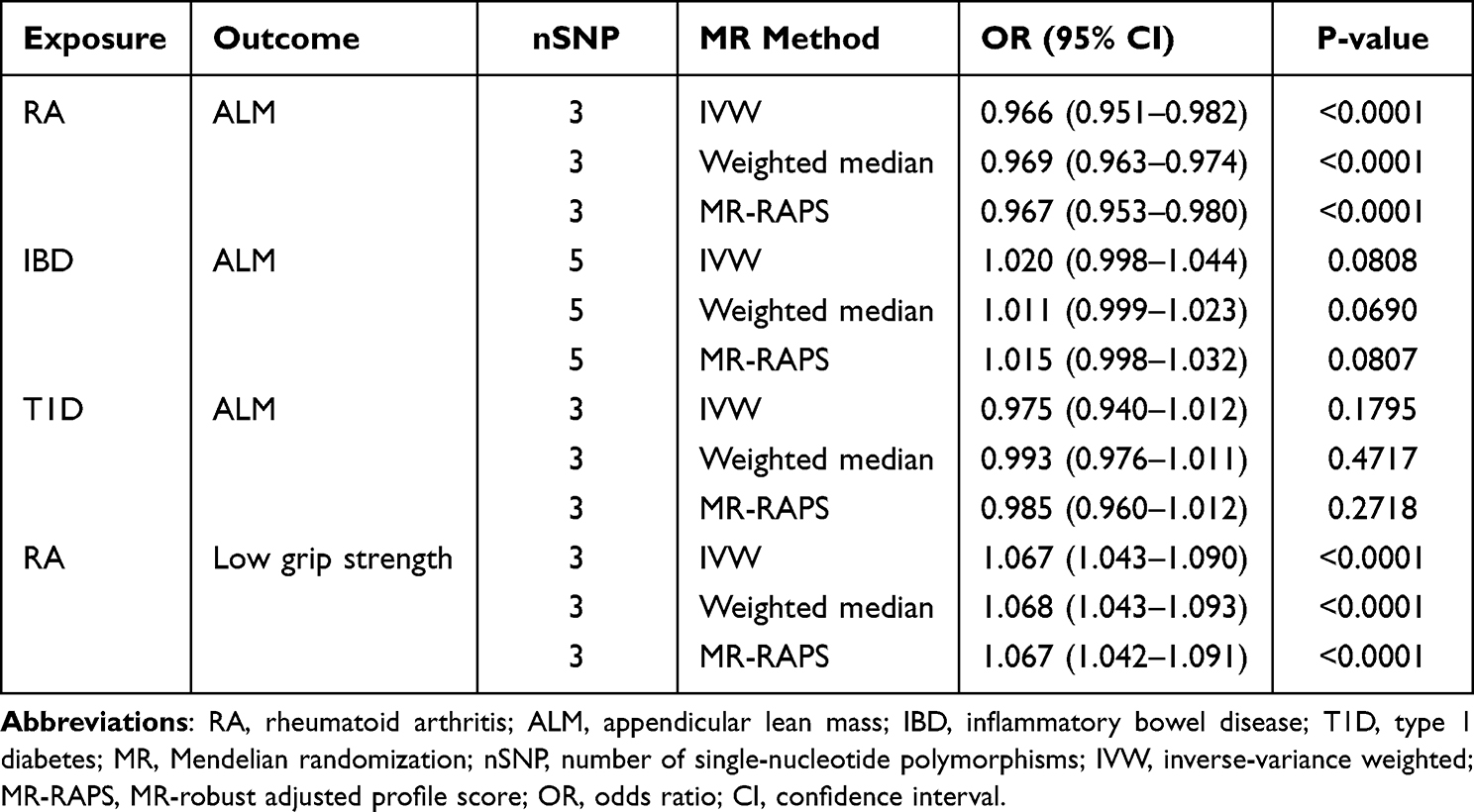 |
Table 1 Results of MR Analysis in Replication Samples |
Causal Effects of Autoimmune Diseases on Low Grip Strength
Through IVW analyses of discovery samples, we detected that RA was correlated with a higher risk of low grip strength (OR = 1.042, 95% CI: 1.013–1.072, P = 0.0049), but did not observe associations between SLE, IBD, MS, T1D, and overall autoimmune disease with low grip strength (Figure 3). These results were supported by other sensitivity analyses (Figure 3). The scatter plot of various MR tests is shown in Supplementary Figure S2. As no heterogeneity was revealed (all Q_P values > 0.05, Supplementary Table S10), we used fixed-effects IVW model. Furthermore, MR-Egger regression and MR-PRESSO detected no evidence of pleiotropy and outliers (all P > 0.05, Supplementary Table S10).
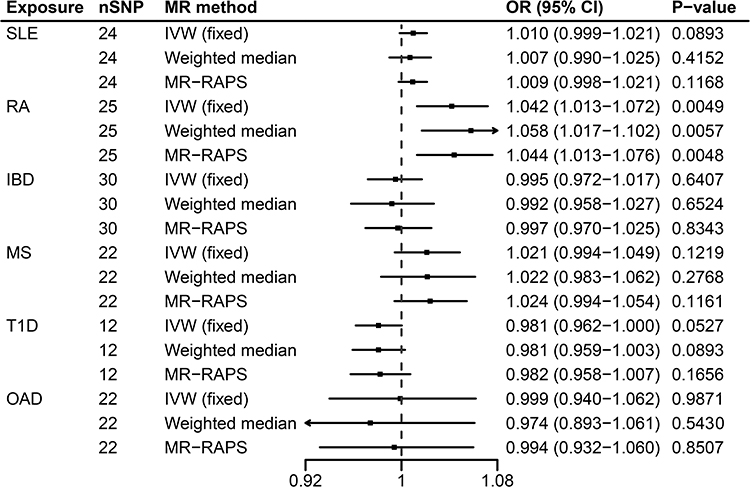 |
Figure 3 MR analysis of associations between autoimmune diseases and low grip strength in discovery samples. Abbreviations: SLE, systemic lupus erythematosus; RA, rheumatoid arthritis; MS, multiple sclerosis; IBD, inflammatory bowel disease; T1D, type 1 diabetes; OAD, overall autoimmune disease; nSNP, number of single-nucleotide polymorphisms; MR, Mendelian randomization; IVW, inverse-variance-weighted; MR-RAPS, MR-robust adjusted profile score; OR, odds ratio; CI, confidence interval. |
As shown in Table 1, the causality of RA and low grip strength was validated in MR analyses of replication samples. Complete results of the replication analyses for associations between five autoimmune diseases and low grip strength are presented in Supplementary Table S12.
Causal Effects of Autoimmune Diseases on Walking Pace
No significant causal effects of SLE, RA, IBD, MS, T1D, and overall autoimmune disease on walking pace were found in the primary analysis of the discovery stage, and the estimates remained stable in WM and MR-RAPS methods (Figure 4). The scatter plot of MR analyses is displayed in Supplementary Figure S3. According to the heterogeneity tests (Supplementary Table S10), random-effects IVW analyses were performed for SLE, RA, and IBD (Q_P values < 0.05), while fixed-effects IVW analyses were performed for MS, T1D, and overall autoimmune disease (Q_P values > 0.05). The MR-Egger did not detect notable pleiotropy (all intercept P > 0.05). MR-PRESSO detected outliers in RA and IBD, but MR-PRESSO distortion tests showed that the results did not change after eliminating outliers (P = 0.791 for RA, P = 0.337 for IBD). Additionally, similar estimates were obtained in replication samples (Supplementary Table S13).
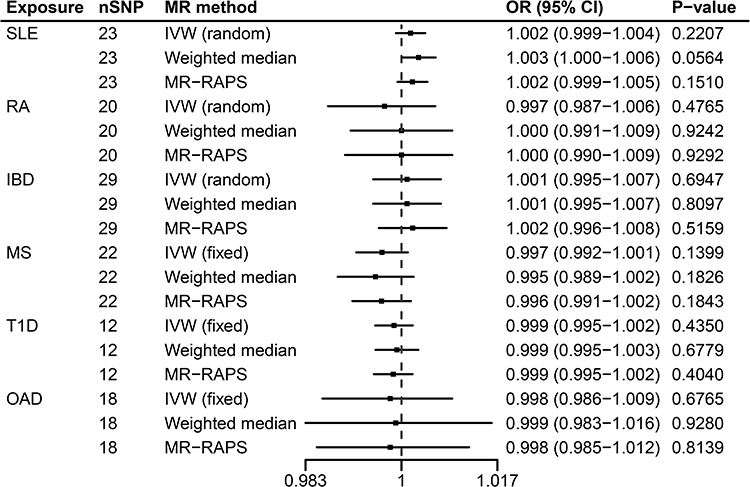 |
Figure 4 MR analysis of associations between autoimmune diseases and walking pace in discovery samples. Abbreviations: SLE, systemic lupus erythematosus; RA, rheumatoid arthritis; MS, multiple sclerosis; IBD, inflammatory bowel disease; T1D, type 1 diabetes; OAD, overall autoimmune disease; nSNP, number of single-nucleotide polymorphisms; MR, Mendelian randomization; IVW, inverse-variance-weighted; MR-RAPS, MR-robust adjusted profile score; OR, odds ratio; CI, confidence interval. |
Reverse MR Analyses
After a series of SNP screening steps, 224 ALM-associated SNPs, 2 low grip strength-associated SNPs, and 16 walking pace-associated SNPs were eligible IVs for reverse MR analyses. Details of these IVs are listed in Supplementary Table S14-S16. In reverse MR analyses, the IVW method detected that walking pace was negatively related to overall autoimmune disease, whereas ALM and low grip strength were unrelated to overall autoimmune disease (Supplementary Table S17). And the association between walking pace and overall autoimmune disease did not obtain a consistent result in the WM method. Besides, we did not observe reverse causalities between five common autoimmune diseases and three sarcopenia-related traits.
Discussion
In this study, we examined the causal impact of five common autoimmune diseases and overall autoimmune disease on sarcopenia-related traits using two-sample MR analyses. Results from discovery samples showed that RA, IBD, and T1D were causally negatively correlated with ALM, RA was causally positively related to low grip strength, and no association was found between autoimmune diseases and walking pace. Of note, the associations of RA with ALM and low grip strength were successfully replicated in replication samples. Additionally, reverse MR analysis only found an association between walking pace and overall autoimmune disease, but this association did not remain in the WM method. To our knowledge, this work reveals the causalities between autoimmune diseases and sarcopenia-related traits using MR analysis for the first time.
Observational studies have found that RA is associated with sarcopenia. A cross-sectional study including 289 RA patients and 280 controls found an 11-fold higher prevalence of sarcopenia in RA patients than in controls, and the study also found significantly lower ALM and grip strength values in RA patients than in controls.6 Another study including three cohorts of patients with RA and two general population cohorts (444 cases and 17,668 controls) found a higher rate of low lean mass in RA patients.30 Besides, other studies also found lower ALM in RA patients.31,32 These studies are consistent with our findings that RA has causal impacts on ALM and low grip strength. Sarcopenia is diagnosed when both low grip strength and low muscle mass are met, according to EWGSOP and EWGSOP2 definitions for sarcopenia, and severe sarcopenia is diagnosed when combined with slow gait speed.22,33 Therefore, although our study did not find a correlation between RA and walking pace, it is reasonable to infer that RA has a potentially causal role in sarcopenia. Inflammatory cytokines, such as TNF and IL-6, may play an important role in RA-induced sarcopenia. Increased serum levels of these cytokines can activate the ubiquitin-proteasome system, leading to the breakdown of muscle proteins.34,35 One study also found that IL-6 and TNF-α activated signal transducer and activator of transcription 3, which then collaborated with the nuclear factor kappa B (NF-kappa B) pathway to induce muscle wasting by activating the inducible nitric oxide synthase pathway.36 In addition, TNF can also inhibit MyoD, a myogenic regulatory factor, through the activation of NF-kappa B to impair myogenesis.37 But contradictory results were also obtained. For example, Castillero et al observed elevated MyoD and myogenin in arthritic rats.38 The underlying mechanism of sarcopenia induced by RA requires further investigation.
A Japanese study involving 177 patients with T1D and 506 participants without diabetes found that sarcopenia was more frequent in T1D patients than in participants without diabetes.9 A hyperglycemic and hypoinsulinemic milieu is characteristic of T1D. Insulin has been reported to have the effect of reducing muscle protein breakdown.39 Conversely, hyperglycemia inhibits the degradation of Krüppel-like factor 15 in skeletal muscle, which can upregulate E3 ubiquitin ligases, thereby promoting proteolysis.40,41 These lines of evidence support the association between T1D and muscle loss. Our MR analysis of discovery samples also identified that T1D was causally inversely associated with ALM. Paradoxically, the negative association between T1D and ALM failed to be replicated in replication samples. Well-designed prospective studies and more MR studies are needed in the future to validate this association. As for the impact of T1D on grip strength, conflicting results have been obtained in observational studies.9,42 In our study, no causal relationship between T1D and low grip strength was found at both the discovery and replication phases.
Similar to T1D, we found that IBD was only causally negatively related to ALM in the discovery stage. Many studies have used muscle mass alone to assess sarcopenia in patients with IBD, and computed tomography (CT) is commonly used for the assessment of muscle mass.43 Zhang et al evaluated the skeletal muscle index (SMI) at the third lumbar vertebrae of 204 IBD patients and 60 controls by CT and found that the SMI was lower in IBD patients than in controls.44 This is similar to our results. Sarcopenia in IBD patients may be related to malnutrition due to IBD, such as protein and micronutrient deficiencies.45,46 The concomitant increase in pro-inflammatory cytokines (eg, IL-6 and TNF-α) in IBD may also play an important role in sarcopenia.47 However, as MR-Egger regression detected pleiotropy in the association between IBD and ALM, and this association failed to be validated in the replication sample, more MR studies with better data are needed in the future to validate this association. Moreover, several studies have found lower grip strength values in IBD patients, but these studies only compared differences in grip strength values between IBD patients and controls, rather than the prevalence of low grip strength.48,49 In our study, IBD was not found to be associated with low grip strength as defined by EWGSOP. This may be because IBD is associated with reduced grip strength but not low grip strength.
There are currently fewer studies on the association of SLE and MS with sarcopenia, and studies on the relationship between SLE and sarcopenia have yielded conflicting results. One study that judged sarcopenia solely on the fat-free mass index showed that sarcopenia was more common in SLE patients.7 Whereas another study found no significant difference in lean mass between SLE patients and controls.50 Consistently, we did not find a causal relationship between SLE and sarcopenia-related traits in our study. As for MS, limited studies have found a higher prevalence of sarcopenia among MS patients.8 However, this is inconsistent with our findings. The reason for the inconsistency may be that observational studies are susceptible to confounding factors. Furthermore, we found that overall autoimmune disease was not associated with any of the three sarcopenia-related traits, suggesting that only some specific autoimmune diseases are associated with sarcopenia, such as rheumatoid arthritis, which was found in our study.
The main advantage of this study is that we comprehensively analyzed the causal relationships of five common autoimmune diseases and overall autoimmune disease with sarcopenia-related traits in discovery samples, and validated the causalities of five common autoimmune diseases and sarcopenia-related traits in replication samples, thereby increasing the credibility of the results. Besides, we performed reverse MR analyses to examine possible reverse causal associations. However, several limitations of this study should be mentioned. First, muscle mass was estimated using ALM rather than appendicular skeletal muscle mass in our study. ALM contains some other components such as tendons and connective tissue, which may cause some bias. But ALM is predictive of total-body skeletal muscle, as a large proportion of total-body skeletal muscle appears in the extremities and a large proportion of ALM is skeletal muscle.51,52 Second, because our study was based on summary-level data, subgroup analysis by age or sex was not available. Third, MR studies using genetic variants as instrumental variables only profile the contribution of genetic components to the trait, not environmental variation. This may explain why the causal effect of RA on sarcopenia observed in our study was small. Fourth, the present study was confined to European populations, which may limit the applicability of the results to other populations.
Conclusion
In summary, this MR study demonstrates that RA is causally associated with low grip strength and reduced ALM, and that IBD and T1D may be causally negatively related to ALM. However, SLE, MS, and overall autoimmune disease are not associated with any of the three sarcopenia-related traits. Based on our current findings, we believe that it may be meaningful to screen sarcopenia in patients with RA, IBD, and T1D.
Data Sharing Statement
The original contributions presented in the study are included in the article/ Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics Statement
Our study was based on publicly available GWAS summary-level data and all original studies have been approved by their Institutional Review Boards or local ethics committees. Besides, our study did not involve individual-level data and was deemed not to require ethical approval after consultation with the Ethics Committee of Wenzhou Medical University.
Acknowledgments
The authors gratefully acknowledge all researchers and participants who provided publicly available GWAS summary data.
Author Contributions
All authors made a significant contribution to the work reported, whether is in conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81703310).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
2. Petermann-Rocha F, Balntzi V, Gray SR, et al. Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2022;13(1):86–99.
3. Shu X, Lin T, Wang H, et al. Diagnosis, prevalence, and mortality of sarcopenia in dialysis patients: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2022;13(1):145–158.
4. Tantai X, Liu Y, Yeo YH, et al. Effect of sarcopenia on survival in patients with cirrhosis: a meta-analysis. J Hepatol. 2022;76(3):588–599.
5. An HJ, Tizaoui K, Terrazzino S, et al. Sarcopenia in autoimmune and rheumatic diseases: a comprehensive review. Int J Mol Sci. 2020;21(16): 5678.
6. Dietzel R, Wiegmann S, Borucki D, et al. Prevalence of sarcopenia in patients with rheumatoid arthritis using the revised EWGSOP2 and the FNIH definition. RMD Open. 2022;8(2):67.
7. Santos MJ, Vinagre F, Canas da Silva J, Gil V, Fonseca JE. Body composition phenotypes in systemic lupus erythematosus and rheumatoid arthritis: a comparative study of Caucasian female patients. Clin Exp Rheumatol. 2011;29(3):470–476.
8. Yuksel H, Balaban M, Tan OO, Mungan S. Sarcopenia in patients with multiple sclerosis. Mult Scler Relat Disord. 2022;58:103471.
9. Mori H, Kuroda A, Yoshida S, et al. High prevalence and clinical impact of dynapenia and sarcopenia in Japanese patients with type 1 and type 2 diabetes: findings from the Impact of Diabetes Mellitus on Dynapenia study. J Diabetes Investig. 2021;12(6):1050–1059.
10. Pizzoferrato M, de Sire R, Ingravalle F, et al. Characterization of Sarcopenia in an IBD Population Attending an Italian Gastroenterology Tertiary Center. Nutrients. 2019;11(10):2281. doi:10.3390/nu11102281
11. Bennett JL, Pratt AG, Dodds R, Sayer AA, Isaacs JD. Rheumatoid sarcopenia: loss of skeletal muscle strength and mass in rheumatoid arthritis. Nat Rev Rheumatol. 2023;19: 239.
12. Jimenez-Gutierrez GE, Martinez-Gomez LE, Martinez-Armenta C, Pineda C, Martinez-Nava GA, Lopez-Reyes A. Molecular Mechanisms of Inflammation in Sarcopenia: diagnosis and Therapeutic Update. Cells. 2022;11(15): 239.
13. Corvaisier M, Delneste Y, Jeanvoine H, et al. IL-26 is overexpressed in rheumatoid arthritis and induces proinflammatory cytokine production and Th17 cell generation. PLoS Biol. 2012;10(9):e1001395.
14. Jang DI, Lee AH, Shin HY, et al. The Role of Tumor Necrosis Factor Alpha (TNF-alpha) in Autoimmune Disease and Current TNF-alpha Inhibitors in Therapeutics. Int J Mol Sci. 2021;22(5): 2719.
15. Murakami M, Kamimura D, Hirano T. Pleiotropy and Specificity: insights from the Interleukin 6 Family of Cytokines. Immunity. 2019;50(4):812–831.
16. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601.
17. Bentham J, Morris DL, Graham DSC, et al. Genetic association analyses implicate aberrant regulation of innate and adaptive immunity genes in the pathogenesis of systemic lupus erythematosus. Nat Genet. 2015;47(12):1457–1464.
18. Okada Y, Wu D, Trynka G, et al. Genetics of rheumatoid arthritis contributes to biology and drug discovery. Nature. 2014;506(7488):376–381.
19. Liu JZ, van Sommeren S, Huang H, et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat Genet. 2015;47(9):979–986.
20. Beecham AH, Patsopoulos NA, et al; International Multiple Sclerosis Genetics C. Analysis of immune-related loci identifies 48 new susceptibility variants for multiple sclerosis. Nat Genet. 2013;45(11):1353–1360.
21. Onengut-Gumuscu S, Chen WM, Burren O, et al. Fine mapping of type 1 diabetes susceptibility loci and evidence for colocalization of causal variants with lymphoid gene enhancers. Nat Genet. 2015;47(4):381–386.
22. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412–423.
23. Pei YF, Liu YZ, Yang XL, et al. The genetic architecture of appendicular lean mass characterized by association analysis in the UK Biobank study. Commun Biol. 2020;3(1):608.
24. Jones G, Trajanoska K, Santanasto AJ, et al. Genome-wide meta-analysis of muscle weakness identifies 15 susceptibility loci in older men and women. Nat Commun. 2021;12(1):654.
25. Zhao Q, Chen Y, Wang J, Small DS. Powerful three-sample genome-wide design and robust statistical inference in summary-data Mendelian randomization. Int J Epidemiol. 2019;48(5):1478–1492.
26. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol. 2016;40(4):304–314.
27. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525.
28. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698.
29. Palmer TM, Lawlor DA, Harbord RM, et al. Using multiple genetic variants as instrumental variables for modifiable risk factors. Stat Methods Med Res. 2012;21(3):223–242.
30. Baker JF, Giles JT, Weber D, et al. Sarcopenic obesity in rheumatoid arthritis: prevalence and impact on physical functioning. Rheumatology. 2022;61(6):2285–2294.
31. Dao HH, Do QT, Sakamoto J. Abnormal body composition phenotypes in Vietnamese women with early rheumatoid arthritis. Rheumatology. 2011;50(7):1250–1258.
32. Lin JZ, Liang JJ, Ma JD, et al. Myopenia is associated with joint damage in rheumatoid arthritis: a cross-sectional study. J Cachexia Sarcopenia Muscle. 2019;10(2):355–367.
33. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31.
34. Perez-Baos S, Prieto-Potin I, Roman-Blas JA, Sanchez-Pernaute O, Largo R, Herrero-Beaumont G. Mediators and Patterns of Muscle Loss in Chronic Systemic Inflammation. Front Physiol. 2018;9:409.
35. Li W, Moylan JS, Chambers MA, Smith J, Reid MB. Interleukin-1 stimulates catabolism in C2C12 myotubes. Am J Physiol Cell Physiol. 2009;297(3):C706–714.
36. Ma JF, Sanchez BJ, Hall DT, Tremblay AK, Di marco S, Gallouzi IE. STAT3 promotes IFNgamma/TNFalpha-induced muscle wasting in an NF-kappaB-dependent and IL-6-independent manner. EMBO Mol Med. 2017;9(5):622–637.
37. Guttridge DC, Mayo MW, Madrid LV, Wang CY, Baldwin AS. NF-kappaB-induced loss of MyoD messenger RNA: possible role in muscle decay and cachexia. Science. 2000;289(5488):2363–2366.
38. Castillero E, Martin AI, Lopez-Menduina M, Granado M, Villanua MA, Lopez-Calderon A. IGF-I system, atrogenes and myogenic regulatory factors in arthritis induced muscle wasting. Mol Cell Endocrinol. 2009;309(1–2):8–16.
39. Abdulla H, Smith K, Atherton PJ, Idris I. Role of insulin in the regulation of human skeletal muscle protein synthesis and breakdown: a systematic review and meta-analysis. Diabetologia. 2016;59(1):44–55.
40. Hirata Y, Nomura K, Senga Y, et al. Hyperglycemia induces skeletal muscle atrophy via a WWP1/KLF15 axis. JCI Insight. 2019;4(4):57.
41. Shimizu N, Yoshikawa N, Ito N, et al. Crosstalk between glucocorticoid receptor and nutritional sensor mTOR in skeletal muscle. Cell Metab. 2011;13(2):170–182.
42. Vilaca T, Paggiosi M, Walsh JS, Selvarajah D, Eastell R. The Effects of Type 1 Diabetes and Diabetic Peripheral Neuropathy on the Musculoskeletal System: a Case-Control Study. J Bone Miner Res. 2021;36(6):1048–1059.
43. Nishikawa H, Nakamura S, Miyazaki T, et al. Inflammatory Bowel Disease and Sarcopenia: its Mechanism and Clinical Importance. J Clin Med. 2021;10(18):567.
44. Zhang T, Ding C, Xie T, et al. Skeletal muscle depletion correlates with disease activity in ulcerative colitis and is reversed after colectomy. Clinical Nutrition. 2017;36(6):1586–1592.
45. Forbes A, Escher J, Hebuterne X, et al. ESPEN guideline: clinical nutrition in inflammatory bowel disease. Clinical Nutrition. 2017;36(2):321–347.
46. van Dronkelaar C, van Velzen A, Abdelrazek M, van der Steen A, Weijs PJM, Tieland M. Minerals and Sarcopenia; The Role of Calcium, Iron, Magnesium, Phosphorus, Potassium, Selenium, Sodium, and Zinc on Muscle Mass, Muscle Strength, and Physical Performance in Older Adults: a Systematic Review. J Am Med Dir Assoc. 2018;19(1):6–11 e13.
47. Dhaliwal A, Quinlan JI, Overthrow K, et al. Sarcopenia in Inflammatory Bowel Disease: a Narrative Overview. Nutrients. 2021;13(2): 2719.
48. Lu ZL, Wang TR, Qiao YQ, et al. Handgrip Strength Index Predicts Nutritional Status as a Complement to Body Mass Index in Crohn’s Disease. J Crohns Colitis. 2016;10(12):1395–1400.
49. Cioffi I, Marra M, Imperatore N, et al. Assessment of bioelectrical phase angle as a predictor of nutritional status in patients with Crohn’s disease: a cross sectional study. Clinical Nutrition. 2020;39(5):1564–1571.
50. Seguro LPC, Paupitz JA, Caparbo VF, Bonfa E, Pereira RMR. Increased visceral adipose tissue and altered adiposity distribution in premenopausal lupus patients: correlation with cardiovascular risk factors. Lupus. 2018;27(6):1001–1006.
51. Buckinx F, Landi F, Cesari M, et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J Cachexia Sarcopenia Muscle. 2018;9(2):269–278.
52. Kim J, Wang Z, Heymsfield SB, Baumgartner RN, Gallagher D. Total-body skeletal muscle mass: estimation by a new dual-energy X-ray absorptiometry method. Am J Clin Nutr. 2002;76(2):378–383.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bidirectional Mendelian Randomization Study of Sarcopenia-Related Traits and Knee Osteoarthritis
Zhang L, Zhang C, Zhang J, Liu A, Wang P, Xu J
Clinical Interventions in Aging 2023, 18:1577-1586
Published Date: 15 September 2023
Genetically Proxied Autoimmune Diseases and the Risk of Facial Aging
Zhang Z, Li M, Geng Y, Wang W, Wang W, Shao Y
Clinical, Cosmetic and Investigational Dermatology 2024, 17:981-991
Published Date: 3 May 2024
Causal Associations Between Sarcopenia and Gestational Diabetes Mellitus

Huang Y, Zhao S, Hong J, Shen L, Wang Z, Wang D
International Journal of Women's Health 2025, 17:259-269
Published Date: 1 February 2025
Development and Validation of a Cost-Effective Machine Learning Model for Screening Potential Rheumatoid Arthritis in Primary Healthcare Clinics
Wu W, Hu X, Yan L, Li Z, Li B, Chen X, Lin Z, Zeng H, Li C, Mo Y, Wu Y, Wang Q
Journal of Inflammation Research 2025, 18:1511-1522
Published Date: 3 February 2025
Role of Gut Microbiota in the Development of Some Autoimmune Diseases
Cui X, Cong Y
Journal of Inflammation Research 2025, 18:4409-4419
Published Date: 25 March 2025