Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Association Analysis of Polymorphisms in BIN1, MC1R, STARD6 and PVRL2 with Mild Cognitive Impairment in Elderly Carrying APOE ϵ4 Allele
Authors Wu Y ![]() , Yin J
, Yin J ![]() , Yang B, Tang L, Feng W, Liu X, Zhao X, Cheng Z
, Yang B, Tang L, Feng W, Liu X, Zhao X, Cheng Z
Received 7 December 2020
Accepted for publication 22 March 2021
Published 21 April 2021 Volume 2021:17 Pages 1125—1133
DOI https://doi.org/10.2147/NDT.S296144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yue Wu,1,* Jiajun Yin,2,* Bixiu Yang,3 Li Tang,4 Wei Feng,5 Xiaowei Liu,1 Xingfu Zhao,1 Zaohuo Cheng1
1Department of Geriatric Psychiatry, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, Wuxi, Jiangsu Province, People’s Republic of China; 2Brain Science Basic Laboratory, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, Wuxi, Jiangsu Province, People’s Republic of China; 3Department of Clinical Psychology, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, Wuxi, Jiangsu Province, People’s Republic of China; 4Department of General Psychiatry, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, Wuxi, Jiangsu Province, People’s Republic of China; 5Department of Social Prevention and Control, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, Wuxi, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zaohuo Cheng
Department of Geriatric Psychiatry, The Affiliated Wuxi Mental Health Center with Nanjing Medical University, 156 Qianrong Road, Wuxi, 214151, Jiangsu Province, People’s Republic of China
Tel +86 510 830 30359
Fax +86 510 830 12201
Email [email protected]
Background: Apolipoprotein (APOE) ϵ4 is recognized as an independent risk factor for mild cognitive impairment (MCI). However, not everyone with the ϵ4 allele develops MCI, suggesting that other susceptibility genes exist. This study aimed to identify MCI susceptibility genes, including BIN1, MC1R, STARD6, and PVRL2, in elderly Han Chinese and to verify their association with APOE ϵ4 allele in MCI onset.
Methods: To determine whether polymorphisms in BIN1 (rs6733839, rs7561528), MC1R (rs2228479), STARD6 (rs10164112), and PVRL2 (rs6859) occurred in elderly MCI patients carrying APOE ϵ4 allele, we carried out a case–control study including 285 MCI patients and 326 healthy controls.
Results: Statistically significant differences in the proportion of APOE ϵ4 carriers, and BESCI, ADAS-cog, and CNT scores existed between the NC and MCI groups (all P < 0.01). Frequencies of the rs10164112 T and rs6859 A alleles were significantly higher in the latter than in the former (P = 0.01; 0.029). However, no significant differences in allele and genotype distribution of BIN1 (rs6733839, rs7561528) and MC1R (rs2228479) existed between samples in our two groups (all P > 0.05). When stratified by APOE ϵ4 status (carriers/non-carriers), genotype frequencies of BIN1 rs7561528, STARD6 rs10164112, and PVRL2 rs6859 among the four groups (NCϵ4+, NCϵ4-, MCIϵ4+, MCIϵ4-) were significantly different. Additionally, our results suggest a significant association between MCI and BIN1 rs7561528, STARD6 rs10164112, and PVRL2 rs6859 (all P< 0.05) in elderly carriers.
Conclusion: This suggests that among the Han Chinese, MCI in elderly APOE ϵ4 carriers may be related to the BIN1 (rs7561528), STARD6 (rs10164112) and PVRL2 (rs6859). Genotype AA of rs7561528 and TT of rs10164112 might be protective factors against MCI in elderly APOE ϵ4 carriers.
Keywords: mild cognitive impairment, BIN1, MC1R, STARD6, PVRL2, APOE, polymorphism, association analysis
Introduction
Dementia, in the elderly, is a continuous pathophysiological process, with preclinical, early clinical, and dementia stages. The early clinical stage is also known as mild cognitive impairment (MCI) and can be considered a transitional stage between normal aging and dementia, with an annual conversion rate of 10%–15% to Alzheimer’s disease (AD), which is more than 10 times greater than that of the normal elderly population.1,2 Although MCI has a greater risk of developing dementia, dementia is not the only result of MCI progression. A 5-year follow-up study showed that 29% of MCI patients did not progress to dementia and 10% reverted to normal status. Since there is no exact cure for dementia, it is urgent to establish potential diagnostic markers for MCI in the elderly population to carry out accurate interventions to reduce, delay, or even reverse the progression of MCI. The combined pathogenesis of MCI and AD is complex and is mainly caused by the joint action of genetic and environmental factors.3,4 Twin studies suggest that 37% to 78% of variance in age-at-onset of cognitive impairment can be attributed to additive genetic effects. Consequently, genes involved in MCI or late-onset Alzheimer’s disease (LOAD) could be highly valuable diagnostic tools.5 Mutations in amyloid precursor protein (APP), presenilin 1 (PSEN1) and presenilin 2 (PSEN2) genes have been confirmed to cause early-onset Alzheimer’s disease (EOAD), which accounts for less than 1% of all AD cases. To date, only the apolipoprotein E (APOE) ε4 allele has been described as being strongly associated with cases of sporadic AD (SAD) in diverse populations worldwide; specifically, in those without a family history of the condition.
The main pathological indicators of AD are extracellular amyloid (Aβ) plaques, intracellular neurofibrillary tangles (NFTs), and a loss of neurons and synapses, resulting in brain atrophy. Genetic, biochemical, and neuropathological data suggest that aggregation of Aβ, the key component of plaques formed by proteolysis of β- amyloid precursor protein (β-APP), is central to initiating AD pathogenesis. PSEN1 and PSEN2 have also been shown to act as susceptibility genes, leading to the initiation of the “amyloid cascade”, a basic biochemical process for the production of Aβ. APOE, located on chromosome 19q13.2, is an important serum lipoprotein and plays a role in the mobilization and redistribution of cholesterol. It may act by affecting the metabolism of Aβ, promoting its deposition. APOE has also been implicated in neuronal growth and repair, nerve regeneration, immune response, and activation of lipolytic enzymes. In humans, it is expressed as three common isoforms coded for by three alleles: APOEε2, ε3 and ε4. APOE ε4 is the strongest known genetic risk factor for AD. The ε4 allele has been widely verified as a pathogenic gene of MCI and AD, and it serves as a predictor of conversion from MCI to AD. Large epidemiological studies have demonstrated that APOE ε4 is associated with lower cognitive performance (particularly with regard to memory), occurrence of MCI, and progression from MCI to dementia.6,7 However, not all APOE ε4 carriers develop MCI or AD. Only 50% of individuals with AD carry the APOEε4 allele, and some elderly dementia patients exhibit no association with APOE subtypes being linked to AD, indicating that additional undiscovered genetic factors may contribute to MCI or AD susceptibility.
As the field of molecular genetics has developed, meta-analysis and genome-wide association studies (GWAS) have given us the ability to described additional genes that may be associated with MCI, including BIN1, MC1R, STARD6, and PVRL2. The pathogenesis of these genes may be related to a number of factors in the body, including lipid metabolism, immune system function, inflammatory factors, synaptic-cell-functioning pathways, cell membrane processing. The bridging integrator 1 (BIN1) gene located in the 2q14.3 region is the most important genetic susceptibility gene of LOAD after APOE ε4. BIN1 may be involved in clathrin-mediated endocytosis by modifying the vesicles transport of β-APP. This increases both the abnormal phosphorylation of tau proteins and Aβ deposition, affecting the onset of AD.8,9 Steroidogenic acute regulatory-related lipid transfer domain 6 (STARD6) is located on 8p11.23 region and might play an important role in regulating neurosteroid synthesis by participating in the intramembranous transfer of cholesterol in mitochondria. It was reported that the neurosteroid levels in the brain of patients with AD were decreased, which negatively correlated with the density of beta-amyloid deposits. As a result, the function of STARD6 has become the focus of most AD studies.10
The pathogenesis of neurodegenerative diseases primarily involves neuroinflammation and oxidative stress. As such, tumor necrosis factor-alpha (TNFα), which serves as the main effector of the inflammatory response, is involved in the occurrence and development of AD. Melanocortin might regulate neuroinflammation and oxidative stress by inhibiting the activation of NF-κB and reducing TNFα levels. The melanocortin 1 receptor (MC1R) gene located on chromosome 16 is a highly polymorphic G protein-coupled seven-transmembrane receptor primarily concerned with regulating skin pigmentation.11,12 Epidemiological studies have provided evidence of co-occurrence of Parkinson’s disease (PD) and cutaneous melanoma (CM), indicating that MC1R may be involved in the bidirectional link between both diseases.13
One gene near APOE is PVRL2 (poliovirus receptor-related 2), which belongs to the immunoglobulin group. Its encoded nectin-2 protein may bind to membrane protein receptors, initiating the signaling pathway leading to downstream lipid metabolism.14,15 In diseases involving polygenic inheritance, a single nucleotide polymorphisms (SNP) contributes little to disease risk predictions, but the presence of multiple abnormal alleles also multiplies the risk of disease. It is known that racial differences in gene polymorphism exist. Nevertheless, no study has evaluated SNPs of BIN1, MC1R, STARD6 and PVRL2 among MCI patients in the Han Chinese population. Therefore, this study analyzed these four SNPs, which were recently reported as putative genetic risk factors associated with the onset of MCI, in the Han Chinese population alongside the APOE ε4 allele.
Materials and Methods
Subjects
1850 elderly volunteers aged 50 and over were recruited by hospital staff from the Wuxi community using a questionnaire survey that allowed researchers to preliminarily exclude individuals with severe physical and mental illnesses. A total of 1500 participants were initially screened and brought to hospital for clinical interviews, psychological tests, and laboratory tests, of which 1302 persons completed clinical interviews and neurocognitive tests. Next, 394 cognitively normal elderly individuals and 346 patients with mild cognitive impairment were selected from this group, based on the interview and test results. Petersen MCI diagnostic criteria and DSM–5 mild neurocognitive impairment diagnostic criteria were also used to reinforce this selection. Of the 562 excluded participants, 248 were diagnosed with subjective cognitive impairment, 125 were diagnosed with mild Alzheimer’s disease, and 189 failed to complete the test. Blood samples were collected from all subjects for biochemical and genetic polymorphism tests.16 As a result, we obtained 611 valid research participants.
These subjects were then divided into two groups: the normal control group (NC) and the MCI group. The subjects were aged 51– 85 years (mean ± SD = 65.31 ± 6.36 years), with the lengths of their educations varying from 3 to 19 years (mean ± SD = 9.63 ± 2.73 years). 555 were married (549 original spouses and 6 remarried) and 56 were single (41 widowed, 13 divorced, and 2 unmarried). Their family structures also varied: 238 lived with children and/or grandchildren, 346 lived with spouses, 27 lived alone. Their main occupations were as follows: 72 technicians, 54 administrators, 370 workers, 78 farmers and 37 assorted others. All subjects, or their guardians, signed an informed consent form at the time of recruitment, with the ethics committee of the Wuxi Mental Health Center of Nanjing Medical University approving the study. The study protocols were conducted in accordance with the Declaration of Helsinki.
Procedure
Subjective Memory Complaint Screening
The brief elderly cognitive screening questionnaire screening (BECSI) was used to screen the elderly in the community.17 It contained 13 items aimed at assessing the following four functional domains: memory function, temporal orientation, work efficiency, and mental pathology. Each item was scored on a scale of 0–3, with total scores determining the degree of cognitive impairment. Those with fewer than 5 points had non–subjective cognitive impairment, those with 5–9 points had mild cognitive impairment, and those with less than 10 points had severe cognitive impairment.
Clinical Interview and Examinations
Our interview and examination process had 4 primary sections: (1) social demographic data, (2) medical history collection and simple psychiatric examination, (3) physical examination, and (4) necessary auxiliary examinations and psychological tests. The first section included demographics questions, such as subject name, gender, age, nationality, marriage, culture, occupation, educational level, family status, as well as economic status, alcohol and tobacco habits, and outdoor activities. The second collected information related to memory and cognitive decline, psychiatric examinations, and family and individual medical history. The third collected information focused around examination of the central nervous system, as well as assorted other physical data, such as heart rate, blood pressure, height, weight, vision and hearing. Finally, the last section included more detailed exams: electrocardiograms, electroencephalograms, routine blood tests such as blood glucose and blood lipids, T3/T4 tests, folic acid/vitamin B12 tests, and brain CTs, Alzheimer’s Disease Assessment Scale-Cognitive (ADAS-Cog), Activity of Daily Living Scale (ADL) and Hamilton Depression Scale (HAMD) were also used to evaluate subject conditions in this section.18,19
Objective Cognitive Impairment Assessment
The core neurocognitive test (NCT) was used to assess individual evaluation.20,21 It consisted of eight subtests: digit span, word completion, quick coding, picture-symbol matching, verbal analogy, numeral operation, picture recall, and trail marking test. We calculated the scores of each subtest to find neurocognitive total score following objective cognitive impairment assessment criteria. These scores were also organized by degree of impairment as follows: no cognitive impairment (each subtest score >7 points, neurocognitive total score ≥85 points), mild cognitive impairment (two or more subtests scores ≤7 points, neurocognitive total score ≥70 points), severe cognitive impairment (two or more subtests scores ≤4 points, neurocognitive total score <70).
Gene Polymorphism Detection
Gene polymorphism was detected in three steps. First, we selected SNPs: MCI risk-related SNP retrieval was conducted according to CHB data from the HapMap database. Five SNPs of the BIN1, MC1R, STARD6, and PVRL2 genes (rs6733839, rs7561528, rs10164112, rs2228479 and rs6859) were selected according to the principle of minimum allele frequency (MAF), where MAF > 10% and linkage disequilibrium coefficient (r2) >0.8. Then, we completed genomic DNA extraction. 5 mL of fasting venous blood was collected from all participants using 2% ethylenediaminetetraacetic acid anticoagulant (EDTA) tubes. The Tiangen DNA extraction technique (Tiangen Biotech Co., Ltd, Beijing, China) was used to isolate leukocytes from those samples and extract DNA, which was then stored at -80°C for later use. We then engaged in SNP genotyping. The ligase detection reaction-PCR (LDR-PCR) method (Shanghai Biowing Applied Biotechnology Co., Ltd, Shanghai, China) was used to detect gene polymorphism, and DNA sequencing was used to detect the LDR reaction products. rs6733839, rs7561528, rs10164112, rs2228479, and rs6859 genotypes were then analyzed and verified by sequencing.
Statistical Analysis
All analyses were performed using SPSS24.0 software (IBM Corporation, Armonk, NY, USA). Goodness-of-fit tests for Hardy–Weinberg equilibrium (HWE) were used to ascertain how representative of the population the study sample was. Two-sample t-tests were performed, comparing group comparisons such as age, years of education, BMI, and family medical history. Psychological tests of the two groups were compared using analysis of covariance (ANCOVA). Chi-squared tests were used to compare categorical variables, including gender, marital status, APOE genotype, genotype and allele distributions of BIN1, MC1R, STARD6, and PVRL2. Bonferroni correction was used, and significance was set at P<0.05.
Results
Participant Characteristics
The general clinical characteristics of the two groups are summarized in Table 1. The NC group consisted of 326 older adults without any cognitive deficits, and the MCI group consisted of 285 individuals with MCI. Statistically significant differences were observed in terms of age, years of education, type of pre-retirement employment, APOE genotype, and psychological tests scores between the two groups (P<0.000 for all). ANCOVA was conducted to control the impact of age on the scores of psychological tests. However, statistically significant differences still existed between their adjusted BECSI, ADAS-COG, NCT, and ADL scores (all P<0.01). No statistically significant differences between the two groups were found in terms of sex (P=0.058), marital status (P=0.276), BMI (P=0.346), or in terms of family history of neurodegenerative disease in first-degree relatives.
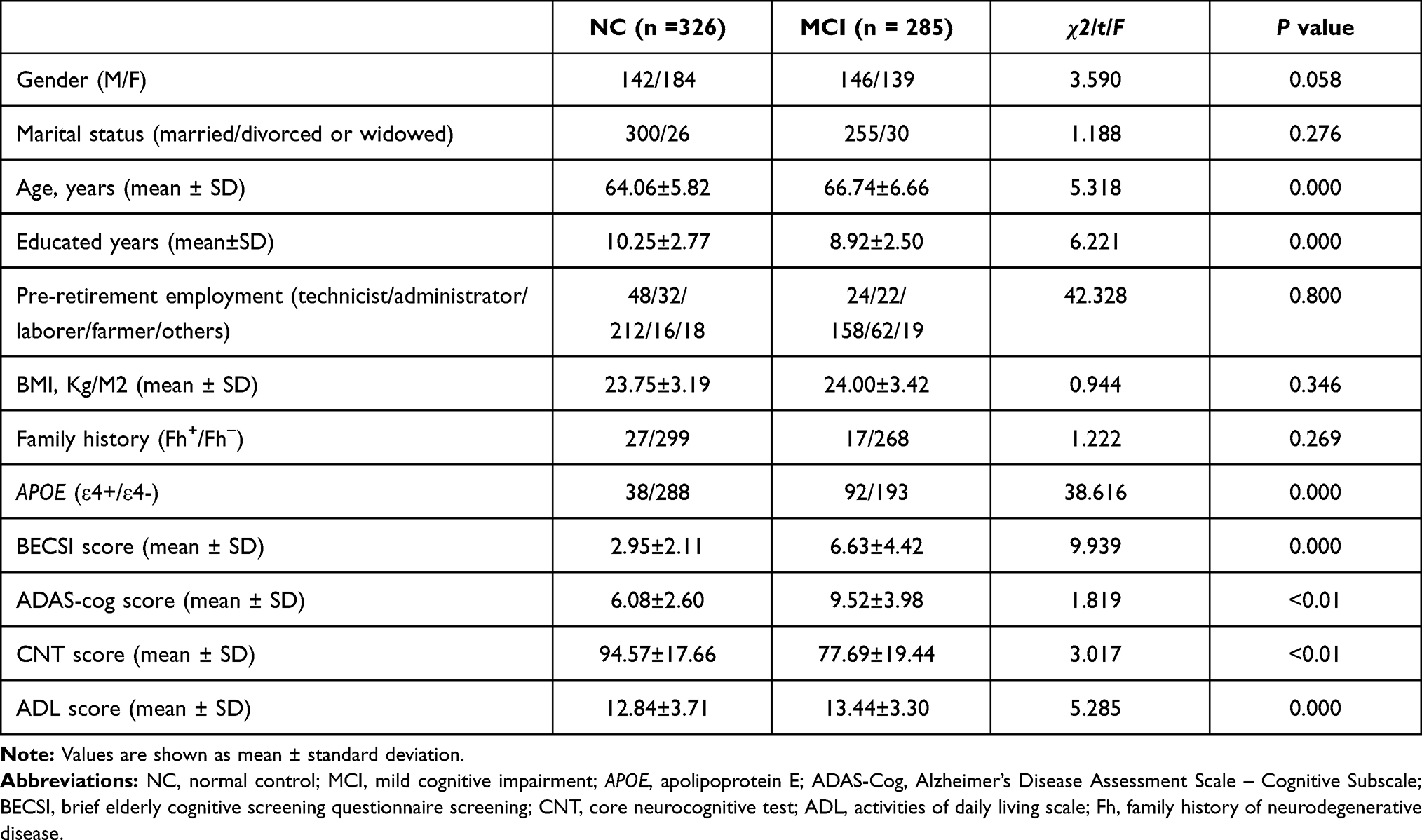 |
Table 1 Demographic Characteristics of the Study Participants |
Alleles and Genotypes
As shown in Table 2, the T allele frequency and genotype frequencies of rs10164112 were significantly different between the NC and MCI groups (P = 0.01, P = 0.003). Meanwhile, the A allele frequency of rs6859, but not the genotype frequency, was significantly different between the two groups (P=0.029). There were no significant differences between the allele or genotype frequencies of rs6733839, rs7561528, or rs2228479 between the two groups.
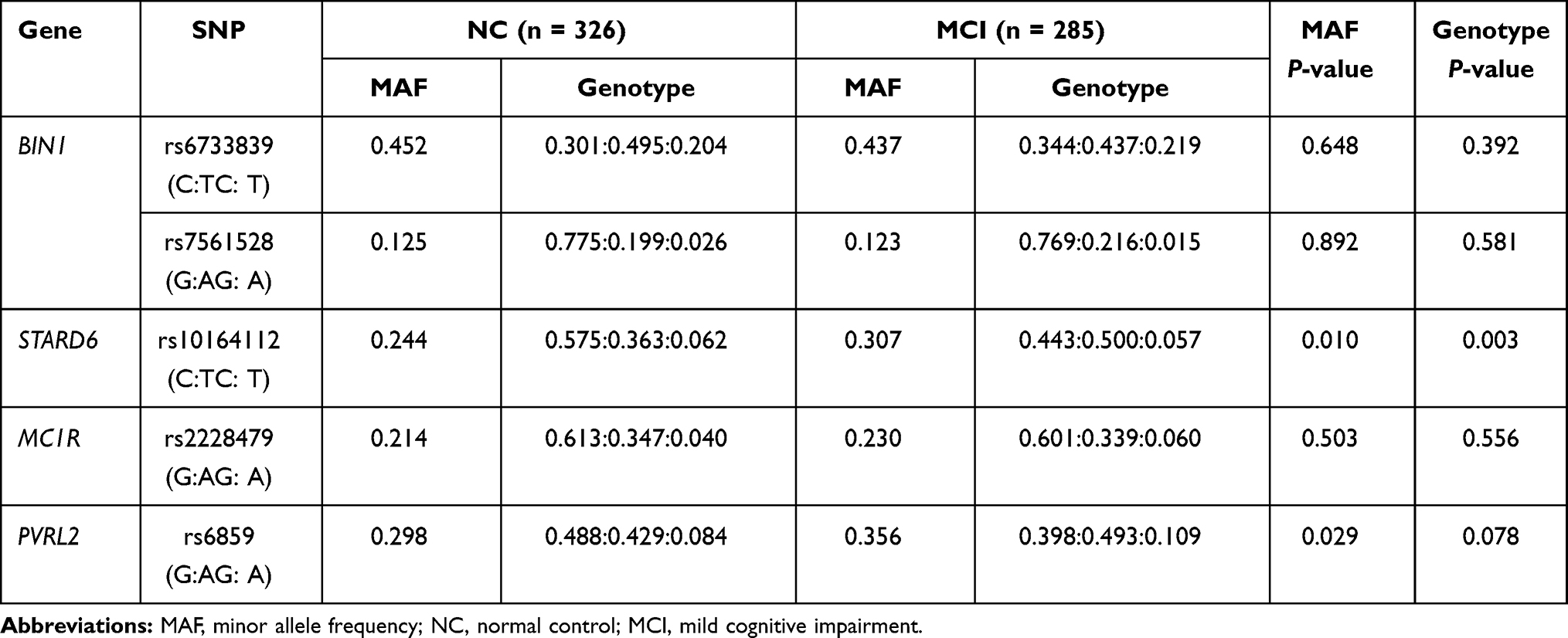 |
Table 2 Comparison of Genotype and Allele Frequencies of SNPs Between MCI Group and NC Group |
Association Analysis
After Bonferroni correction among the four groups (NCε4+, NCε4-, MCIε4+, and MCIε4-; Table 3), as well as stratification by APOE ε4 status (carriers/non-carriers), the genotype frequencies of BIN1 rs7561528, STARD6 rs10164112, and PVRL2 rs6859 were significantly different. In addition, our results suggest, that in elderly APOE ε4 carriers, there may be a significant association between BIN1 rs7561528, STARD6 rs10164112, and PVRL2 rs6859 with MCI (all P<0.05). We did not detect any significant correlation between BIN1 rs6733839 or MC1R rs2228479 and MCI in elderly APOE ε4 carriers.
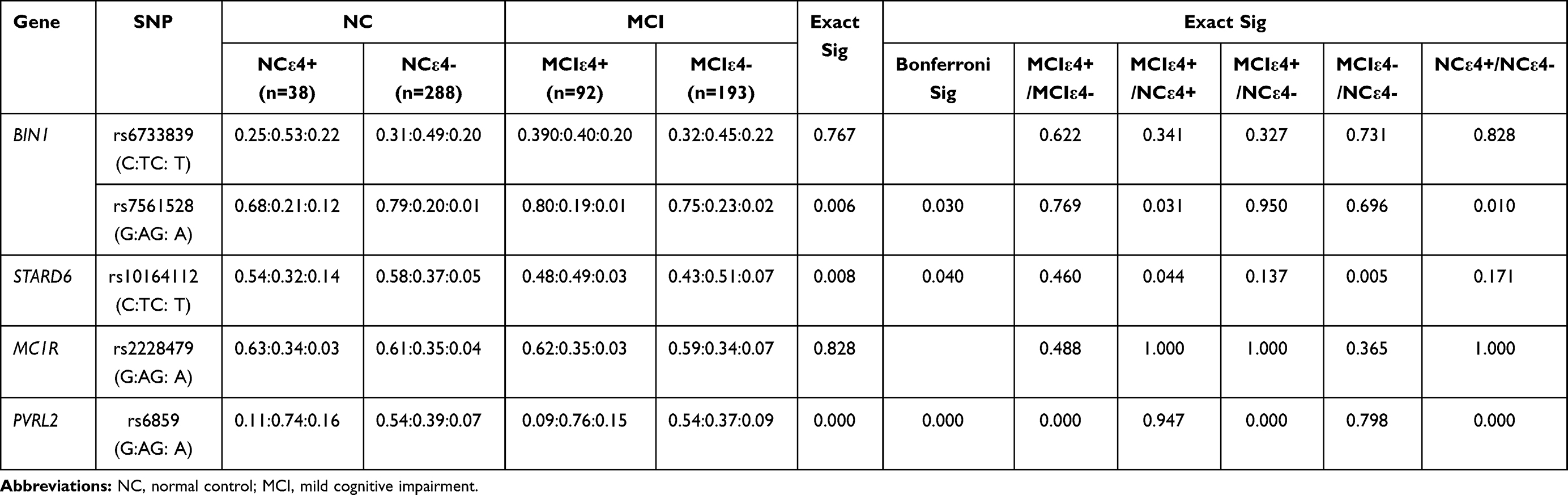 |
Table 3 Results of Association Analysis of SNPs and APOE ε4 in MCI Patients and Controls |
Discussion
Recent GWAS have identified multiple candidate genes associated with MCI, but results varied due to ethnic and regional differences in gene polymorphism. In this study, we aimed to further confirm and explore the susceptibility genes of MCI. We examined the distribution of SNPS of BIN1, MC1R, STARD6, and PVRL2, which were associated with MCI in the GWAS analysis, and analyzed whether that distribution was associated with MCI patients carrying the APOE ε4 allele in the Han Chinese population.
GWAS meta-analysis showed that multiple SNP sites of BIN1 gene were significantly correlated with AD, with rs744373, rs7561528, and rs67338393 being the most representative of that association.22,23 However, these findings were inconsistent between different ethnic groups and regions. The rs7561528 A allele was found to increase the risk of AD in Caucasian and African American populations.24 However, Yang et al believed that rs7561528 A allele might be a protective factor for AD in southern Chinese population.25 It was recently reported by Chen et al that allele C of BIN1 rs744373 was positively correlated with the incidence of MCI in the Tujia Chinese population, but no correlation was found between rs7561528 and MCI.26 It has been reported that expression of BIN1 varies according to gender and race in the brains of normal and sporadic AD patients, and its associated with later age-at-onset and shorter disease duration in AD patients.27,28 MCI is the prodromal stage of AD, and its speed of progression and age-at-onset are generally lower than that of AD. Therefore, in our total samples, we found no significant differences between the polymorphism distributions of BIN1 rs7561528 and rs67338393 in normal and MCI groups. Depending on whether or not group members carried the APOE ε4 allele, the genotype frequency of rs7561528 could vary significantly between the MCIε4+ group and NCε4+ groups. The frequency of GG genotype in the MCI ε4+ group was higher than that in the NCε4+ group (0.80 vs 0.68), and the frequency of the AA genotype in the MCI ε4+ group was lower than that in the NCε4+ group (0.01 vs 0.12), suggesting that rs7561528 polymorphism might be associated with the onset of MCI in elderly patients carrying the APOE ε4 allele.
Recent studies have found that the STARD6 distribution serves a neuroprotective role in the peripheral and central nervous systems. Initial studies by Kim et al suggest that rs10164112 is associated with AD risk in Korean population, and the frequency of the T allele in the AD patients was significantly lower than it was in the healthy controls. Kim et al also speculated that rs10164112 may regulate gene expression by controlling the binding of transcription factors, and that Sp1 transcription factor binds to C-containing promoter, but not to the T-containing promoter.29,30
Our previous results showed that, alone, the rs10164112-T allele was not an independent risk factor for AD in the Han Chinese population. However, it was an independent risk factor when combined with APOE ε4 allele. These results were inconsistent with the results reported by Kim.31 In this study, there were significant differences in the allele and genotype distributions of STARD6 rs10164112 polymorphism between the MCI and control groups. The frequency of the T allele in MCI patients was significantly higher than that in normal controls (0.307 vs 0.244). Moreover, the frequency of the TT genotype in the MCI ε4+ group was lower than that in the NCε4+ group (0.03 vs 0.14), and genotype frequencies of STARD6 rs10164112 were significantly different between the MCIε4- and NCε4- groups. Our results suggest that STARD6 rs10164112 polymorphism may be associated with the occurrence of MCI in the Han Chinese population, and independently effects MCI without interacting with APOE ε4.
To date, studies have confirmed that MC1R is widely distributed in a variety of tissue cells, including skin cells, vascular endothelial cells, melanoma cells and central nervous system, and is a target for drug research in a variety of neurodegenerative diseases. MC1R rs2228479 is a highly polymorphic locus that occurs frequently in Western and Asian populations.32,33 Tell-Marti et al found that rs2228479 polymorphism increased the risk of developing LOAD, especially in patients whose genetic risk could not be explained by the presence of the APOE genotype. However, it had no effect on the age of onset.34 Rs2228479 polymorphism may act on the body through inflammation, or through immunomodulatory pathways unrelated to pigmentation. In this study, there was no significant difference in rs2228479 polymorphism distribution between the MCI and NC groups. At the same time, no significant association was observed between rs2228479 polymorphism and MCI risk in the elderly with APOEε4+ carriers. To date, there are limited numbers of functional evaluations of MC1R gene polymorphisms in the neurocognitive system, and larger genetic studies are necessary to confirm the association between MC1R gene polymorphism and MCI.
PVRL2 rs6859, which increases the risk of AD, is located in the 19q13.2 region, which, in turn, is in strong linkage disequilibrium (LD) with APOE.25,35 This was verified in both Caucasian and southern Chinese population. However, these populations had different risk alleles (the G allele and A allele, respectively). It was recently reported by Cruz-Sanabria et al that, in the Spanish population, the decline in cognitive function was more pronounced in MCI patients with rs6859 GG genotype than in those without the GG genotype.36 In this study, we found that the A allele frequency of PVRL2 rs6859 in the patients with MCI was significantly higher than that in the normal controls, which was consistent with the results of Yang et al.25 We found that there were significant differences in the genotype distributions of rs6859 polymorphism among the four groups (NCε4+/NCε4-/MCIε4+/MCIε4-). In addition, our results support the existence of a synergistic effect between PVRL2 rs6859 and APOE ε4 that increases MCI risk in the Han Chinese population. It indicated that the ε4 allele may have a certain effect on rs6859 genotype expression, and that the association between PVRL2 SNPs and MCI is not simply based on the LD with APOE. However, the specific mechanism needs to be further studied.
The occurrence of MCI may be the result of the interaction between genetic and environmental factors. This study is an exploratory study based on the Wuxi community population. Although we have controlled for regional, population and ethnic bias, there are still some limitations. We did not further stratify our data by age and sex, which may have caused bias in our results. Secondly, this study mainly analyzes the co-phenotype model of gene polymorphism, excluding the dominant model and the recessive model, so there may be bias in the aspect of genetic heterogeneity.
Conclusions
Our findings suggest that BIN1 rs7561528, STARD6 rs10164112, and PVRL2 rs6859 may be related to incidences of MCI in elderly APOEε4 carriers belonging to the Han Chinese population. We did not detect any significant interactions between APOE ε4 and either MC1R rs2228497 or BIN1 rs6733839 in relation to MCI. The results we obtained were inconsistent results when compared with the results of previous research. Thus, it is necessary to perform additional replication studies, with larger sample sizes and across several populations, to confirm the associations between the APOE ε4 allele and BIN1, MC1R, STARD6, and PVRL2 polymorphisms in relation to MCI.
Acknowledgments
We thank the subjects for their willingness to participate in this study. This study was supported by the Social Development key Projects in Jiangsu Province (BE2015615) and the Science &Technology Development Foundation of Wuxi Municipal Science & Technology Bureau (WX18IIAN033).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no actual or potential conflicts of interest.
References
1. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183–194. doi:10.1111/j.1365-2796.2004.01388.x
2. Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1133–1142. doi:10.1212/WNL.56.9.1133
3. Larrieu S, Letenneur L, Orgogozo JM, et al. Incidence and outcome of mild cognitive impairment in a population-based prospective cohort. Neurology. 2002;59(10):1594–1599. doi:10.1212/01.WNL.0000034176.07159.F8
4. Palmer K, Wang HX, Backman L, Winblad B, Fratiglioni L. Differential evolution of cognitive impairment in nondemented older persons: results from the Kungsholmen Project. Am J Psychiatry. 2002;159(3):436–442. doi:10.1176/appi.ajp.159.3.436
5. Meyer JM, Breitner JC. Multiple threshold model for the onset of Alzheimer’s disease in the NAS-NRC twin panel. Am J Med Genet. 1998;81(1):92–97. doi:10.1002/(SICI)1096-8628(19980207)81:1<92::AID-AJMG16>3.0.CO;2-R
6. Blom ES, Giedraitis V, Zetterberg H, et al. Rapid progression from mild cognitive impairment to Alzheimer’s disease in subjects with elevated levels of tau in cerebrospinal fluid and the APOE epsilon4/epsilon4 genotype. Dement Geriatr Cogn Disord. 2009;27(5):458–464. doi:10.1159/000216841
7. Ramakers IH, Visser PJ, Aalten P, et al. The association between APOE genotype and memory dysfunction in subjects with mild cognitive impairment is related to age and Alzheimer pathology. Dement Geriatr Cogn Disord. 2008;26(2):101–108. doi:10.1159/000144072
8. Calafate S, Flavin W, Verstreken P, Moechars D. Loss of Bin1 promotes the propagation of tau pathology. Cell Rep. 2016;17(4):931–940. doi:10.1016/j.celrep.2016.09.063
9. Kingwell K. Alzheimer disease: BIN1 variant increases risk of Alzheimer disease through tau. Nat Rev Neurol. 2013;9(4):184. doi:10.1038/nrneurol.2013.34
10. Clark BJ. The mammalian START domain protein family in lipid transport in health and disease. J Endocrinol. 2012;212(3):257–275. doi:10.1530/JOE-11-0313
11. Ichiyama T, Zhao H, Catania A, Furukawa S, Lipton JM. alpha-melanocyte-stimulating hormone inhibits NF-kappaB activation and IkappaBalpha degradation in human glioma cells and in experimental brain inflammation. Exp Neurol. 1999;157(2):359–365. doi:10.1006/exnr.1999.7064
12. Gu HY, Zheng HX, Lu YY, et al. Association study of MC1R coding region polymorphisms and pigment phenotype in Chinese Han population. J East China Normal Univ. 2013;2:359–365.
13. Liu R, Gao X, Lu Y, Chen H. Meta-analysis of the relationship between Parkinson disease and melanoma. Neurology. 2011;76(23):2002–2009. doi:10.1212/WNL.0b013e31821e554e
14. Takei N, Miyashita A, Tsukie T, et al. Genetic association study on in and around the APOE in late-onset Alzheimer disease in Japanese. Genomics. 2009;93(5):441–448. doi:10.1016/j.ygeno.2009.01.003
15. Yu CE, Seltman H, Peskind ER, et al. Comprehensive analysis of APOE and selected proximate markers for late-onset Alzheimer’s disease: patterns of linkage disequilibrium and disease/marker association. Genomics. 2007;89(6):655–665. doi:10.1016/j.ygeno.2007.02.002
16. American Psychiatric Organization. Diagnostic and Statistical Manual of Mental Disorders.
17. Wu Y, Xu WW, Cheng ZH, Wu B, Tang L, Zhou XQ. The establishment, reliability and validity of a simple cognitive screening questionnaire for the elderly. Chin J Geront. 2016;36(5):1211–1213.
18. Wang L, Shu L, Si TM, Tian CH, Zhang HY. Validity and reliability of Chinese version of Alzheimer’s Disease Assessment Scale. J Clin Psychol. 2000;56(02):89–93. doi:10.1002/(sici)1097-4679(200001)56:1<89::aid-jclp8>3.0.co;2-6
19. Zhang MY. Handbook of Psychiatric Rating Scale. Changsha: Hunan Science and Technology Press; 2016:143–316.
20. Cheng ZH, Li HH, Zheng H, Geng M, Wang L, Wang X. Reliability and validity of multiple memory assessments scale. Chin Mental Health J. 2002;16(4):237–241.
21. Cheng ZH, Sun JR. Theoretic framework of Chinese cognitive ability scale. J Clin Psychol. 2006;14(4):340–342.
22. Carrasquillo MM, Belbin O, Hunter TA, et al. Replication of BIN1 association with Alzheimer’s disease and evaluation of genetic interactions. J Alzheimers Dis. 2011;24(4):751–758. doi:10.3233/JAD-2011-101932
23. Shen L, Thompson PM, Potkin SG, et al. Genetic analysis of quantitative phenotypes in AD and MCI: imaging, cognition and biomarkers. Brain Imaging Behav. 2014;8(2):183–207. doi:10.1007/s11682-013-9262-z
24. Naj AC, Jun G, Beecham GW, et al. Common variants at MS4A4/MS4A6E, CD2AP, CD33 and EPHA1 are associated with late-onset Alzheimer’s disease. Nat Genet. 2011;43(5):436–441. doi:10.1038/ng.801
25. Yang P. Screening of Alzheimer’s disease associated genes in the southern Chinese population and possible mechanisms. Doctoral dissertation of Fudan University; 2014.
26. Chen J. Genes polymorphism of BIN1 and ApoE in patients with amnestic mild cognitive impairment from Enshi Tujia area. Natl Med J Chin. 2018;98(17):1322–1326.
27. Karch CM, Jeng AT, Nowotny P, Cady J, Cruchaga C, Goate AM. Expression of novel Alzheimer’s disease risk genes in control and Alzheimer’s disease brains. PLoS One. 2012;7(11):e50976. doi:10.1371/journal.pone.0050976
28. Glennon EB, Whitehouse IJ, Miners JS, et al. BIN1 is decreased in sporadic but not familial Alzheimer’s disease or in aging. PLoS One. 2013;8(10):e78806. doi:10.1371/journal.pone.0078806
29. Kim YJ, Paik JW, Kang WS, et al. Genetic association of STARD6 polymorphisms with Alzheimer’s disease in a Korean population. J Neurol Sci. 2016;366:100–101. doi:10.1016/j.jns.2016.05.013
30. Chang IY, Kim JH, Hwang G, et al. Immunohistochemical detection of StarD6 in the rat nervous system. Neuroreport. 2007;18(15):1615–1619. doi:10.1097/WNR.0b013e3282f0402f
31. Yin J, Feng W, Yuan H, et al. Association analysis of polymorphisms in STARD6 and near ECHDC3 in Alzheimer’s disease patients carrying the APOE ε4 Allele. Neuropsychiatr Dis Treat. 2019;15:213–218. doi:10.2147/NDT.S186705
32. Pérez Oliva AB, Fernéndez LP, Detorre C, et al. Identification and functional analysis of novel variants of the human melanocortin 1 receptor found in melanoma patients. Hum Mutat. 2009;30(5):811–822. doi:10.1002/humu.20971
33. Raimondi S, Sera F, Gandini S, et al. MC1R variants, melanoma and red hair color phenotype: a meta-analysis. Int J Cancer. 2008;122(12):2753–2760. doi:10.1002/ijc.23396
34. Tell-Marti G, Puig-Butille JA, Potrony M, et al. A common variant in the MC1R gene (p.V92M) is associated with Alzheimer’s disease risk. J Alzheimers Dis. 2017;56(3):1065–1074. doi:10.3233/JAD-161113
35. Ortega-Rojas J, Morales L, Guerrero E, et al. Association analysis of polymorphisms in TOMM40, CR1, PVRL2, SORL1, PICALM, and 14q32.13 regions in Colombian Alzheimer Disease patients. Alzheimer Dis Assoc Disord. 2016;30(4):305–309. doi:10.1097/WAD.0000000000000142
36. Cruz-Sanabria F, Bonilla-Vargas K, Estrada K, et al. Analysis of cognitive performance and polymorphisms of SORL1, PVRL2, CR1, TOMM40, APOE, PICALM, GWAS_14q, CLU, and BIN1 in patients with mild cognitive impairment and cognitively healthy controls. Neurologia. 2018. doi:10.1016/j.nrl.2018.07.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.