")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Assessment of Pain and Anxiety During Arteriovenous Fistula Cannulation Among Hemodialysis Patients: A Cross-Sectional Study in Saudi Arabia
Authors Ibrahim MB, Abdelaal Badawi SE, Alameri RA
Received 13 October 2021
Accepted for publication 21 January 2022
Published 5 April 2022 Volume 2022:15 Pages 705—718
DOI https://doi.org/10.2147/JMDH.S344256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Maryam Bakr Ibrahim,1 Sahar Elmetwally Abdelaal Badawi,2 Rana Ali Alameri2
1Home Healthcare Administration, Ministry of Health, Madinah, Kingdom of Saudi Arabia; 2Department of Fundamental Nursing, College of Nursing, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia
Correspondence: Rana Ali Alameri, Tel +9661333 32934, Email [email protected]
Background: The number of hemodialysis patients has dramatically increased over the years. The cost of healthcare provision to those patients has been rising as well. In addition, pain management during arteriovenous fistula (AVF) cannulation is an important aspect of nursing care. Patients’ outcomes and appropriate pain control are one of the most critical issues in healthcare.
Purpose: To measure the level of pain and anxiety associated with arteriovenous fistula cannulation among hemodialysis patients.
Methods: A correlational cross-sectional research design was used in this study at the Hemodialysis Unit at King Fahad Hospital of the university, Al-Khobar, in the Eastern region of the Kingdom of Saudi Arabia using a self-administered questionnaire. Ethical approval was obtained. A convenience sample of 117 HD patients from the previous mentioned setting were included in the study. The data were collected using three tools: sociodemographic characteristics, Numerical Analogue Scale (NAS), and Hospital Anxiety and Depression Scale (HADS). Using IBM SPSS software package version 25.0, statistical significance of the obtained results was judged at the 5% level.
Results: According to the results, most of the participants experienced a mild to moderate level of pain and anxiety during arteriovenous fistula cannulation. Furthermore, there was a positive association between the level of pain and anxiety, with statistical significance (p< 0.001).
Conclusion: Based on the results of the study, most of the study participants’ level of pain and anxiety during AVF cannulation ranged between mild and moderate.
Keywords: chronic renal failure, hemodialysis, anxiety, depression, cannulation, AVF
Introduction
One of the most common emotional disorders presented by chronic kidney disease (CKD) patients is anxiety due to the hemodialysis (HD) procedure (a procedure in which the blood is cleared of any impurities and waste; and it is the foremost approach to manage renal failure).1,2 Anxiety disorders are common in end stage renal disease (ESRD), with rates ranging between 12% and 52%. HD necessitates that patients comply with diet and fluid restrictions, as the process is associated with chronic pain and discomfort. Anxiety in ESRD patients is also attributed to the invasive procedures related to HD, such as arteriovenous fistula (AVF) cannulation and alarm sounds going off the dialysis machine. Patients also reported anxiety episodes on the lack of permanent nurses that take care of the patients during the HD treatment sessions.3
HD treatment can cause a series of complications during the procedure. A common complication during hemodialysis treatment is a drop in blood pressure associated with a rapid decrease in blood circulation due to ultrafiltration. Also, the patients may suffer and report abdominal pain, cramping, low back pain, chest pain, nausea and vomiting, shortness of breath, or indigestion. Cardiac changes may occur if potassium levels are elevated, leading to arrhythmias or bradycardia. A sharp drop in hematocrit may be seen as the red blood cells rupture.4,5
Air embolism is one of the fatal complications of HD which may cause severe pain around the chest and leads to shortness of breath. It is caused by blockage of the blood supply due to air bubbles in the vascular system. Air embolism can also occur if arterial or venous lines detached, and blood or saline infusion emptied. The nurse is responsible for avoiding that happening. Symptoms will vary depending on the volume of air presented, the site of introduction, the patient’s position, and the speed at which air is introduced, and it must be treated immediately as a medical emergency.6 The “first-use syndrome” is referred to dialyzer reactions, some patients show allergic reaction signs after first exposure to certain types of dialyzer within the first 5 minutes of HD, which may lead to pain and anxiety. Dialyzer reactions produced anaphylactic type symptoms such as dyspnea, chest itching, urticaria, coughing, and back pain, and in a worst case situation cardiac arrest.4,7
Anxiety is described as disruptive feelings of uncertainty and fearfulness. Patients often complain of palpitations, tremors, nervousness, and shortness of breath during HD. It was identified in a recent study that about 45.7% of an HD center population have the criteria for anxiety disorders.8 Even though anxiety during HD is common, it is often overlooked, rarely assessed or treated.9 It is associated with many consequences and impacts the patient’s health. Cukor et al8 found that ESRD patients undergoing HD have a lower quality-of-life than patients without psychiatric diagnoses. Therefore, assessing the level of pain and anxiety among ESRD patients undergoing HD is an essential part of patient care to help recognize the patients’ experience and outcomes.
The pain during HD and AVF cannulation (a connection made between an artery and a vein) can be dependent of the skills and expertise of HD nurses or surgeons. HD nurses are professionals, specialized in AVF cannulation, which is an essential skill required during the HD process. Nurses develop and improve those skills throughout their professional careers. The AVF cannulation requires highly experienced, well-skilled nurses to ensure safe and complication free vascular access considering the significant negative consequences, which may result in severe pain and anxiety levels if the AVF cannulation procedure is not done properly.10 Nurses play an essential role in their patients’ emotional, social, and spiritual support during HD treatment sessions. When a nurse does not successfully perform the cannulation of the AVF site the risk of complications increases. Some of the complications include severe pain HD failure and infection. Additionally, AVF puncture causes pain every time HD patients have a treatment session. Furthermore, when the AVF cannulation is incorrect this would result in inadequate pumping and backflow from the machine resulting from the low blood flow. It would also cause AVF bulging and clotting.10
HD is the common modality used for patients with ESRD. Vascular access is required for all the hemodialysis patients. The most common type of vascular access is AVF for HD patients. HD patients experience anxiety and pain due to the insertion of HD needles, an estimated 320 times per year. Patients still suffer from this pain through their life or until they have a successful renal transplantation. Repeated AVF puncturing may cause anxiety, pain, depression, and negative effects on quality-of-life. AVF puncture-related pain is the most frequent problem for maintenance HD patients. Therefore, pain control during AVF needling should be prioritized in dialysis care.11
Although many studies have examined this issue globally, no studies have been identified in Saudi Arabia. Saudi Arabia is one of the countries in the Middle East where there is a high prevalence of renal diseases. The number of HD patients has significantly increased from 10,000 in 2008 to 19,522 in 2019. The number of new HD patients has almost doubled in ten years from 2,643 in 2009 to 5,036 in 2019. Furthermore, the number of patients taking peritoneal dialysis in 2019 was 1,546, and the number of patients taking post-renal replacement therapy was 7,188.12 The significant increase in the number of HD patients in Saudi Arabia emphasizes the need for increasing research studies on HD related issues and factors. To address this gap, this study aims to evaluate the severity of pain associated with AVF cannulation by using the Numerical Analogue Scale (NAS) in ESRD adult patients undergoing hemodialysis. Also, this study aims to examine anxiety before and after AVF cannulation. Accordingly, the following research questions were identified to be addressed in this study.
- What is the level of pain during AVF cannulation among HD patients?
- What is the level of anxiety during AVF cannulation among HD patients?
- Is there a relationship between the pain and anxiety during AVF cannulation among HD patients?
Materials and Methods
Study Design and Settings
A cross-sectional design was adopted in this study. This study complies with the Declaration of Helsinki. This study was conducted in the Hemodialysis Unit at King Fahad Hospital of the University (KFHU), Al Khobar City, in the Eastern Region of the kingdom of Saudi Arabia with a 440 bed capacity. The hemodialysis unit provides hemodialysis for patients diagnosed with ESRD and its capacity is 31, with it operating during the day over three shifts (7:00 AM–12:00 N, 12:00 N–5:00 PM, 5:00 PM–10:00 PM). It also provides Continuous Renal Replacement Therapy to patients in the intensive care units. The total number of hemodialysis nurses is 45 in the unit, and it is served by seven nephrologists and a transplant coordinator.12
Questionnaire Design
The questionnaire is divided into three parts. The first part focuses on the sociodemographic characteristics of the HD patients (age, gender, marital status, nationality, educational level, working status, address (commute distance between home and hospital), and frequency of pain during previous cannulation), and also includes the main HD prescription data as the year on HD, number of HD sessions/week, duration of HD session (hours), site of AVF, first use of AVF, assessment of AVF, smoking, and current medications. The second part uses Hospital Anxiety and Depression Scale (HADS) for measuring anxiety levels of the patients. HADS is a self-reported scale comprising of 14 items (seven items for anxiety and seven items for depression subscales), with responses being scored on a scale of 0–3, where 3 indicates higher symptom frequencies. Scores for each subscale (anxiety and depression) range from 0–21 with scores categorized as follows: normal 0–7, mild 8–10, moderate 11–14, and severe 15–21. The total score for each of anxiety and depression is between 0 and 21, with higher scores indicating severe anxiety.13 The third part uses the Numerical Analogue Scale (NAS) for measuring pain among the HD patients and is designed to measure pain intensity in individual patients. It has a scale of 0–10. Zero indicates no pain and ten indicates severe pain, none (0), mild (1–3), moderate (4–6), and severe (7–10) pain intensity. Patients are asked to rate their pain from zero to ten, choosing the number that best represents the intensity of the pain they are experiencing. It has been used with many populations.14 A copy of the questionnaire is presented in Appendix A.
Inclusion and Exclusion Criteria
Patients with end-stage kidney failure undergoing regular hemodialysis who have been treated for more than 3 months, at least twice per week (18 years old and above), with arteriovenous fistula in use for more than 1 month are included in the study. Patients on hemodialysis with arteriovenous graft (AVG) or central venous catheter (CVC) and patients with neurological diseases that have a history of chronic pain are excluded.
Sampling and Data Collection
In Saudi Arabia, the total population of ESRD patients on hemodialysis was 19,522, while 2,416 of them were in the Eastern Region.12 The sample size was computed based on the Slovin's formula.15 Level of confidence: 95%, Margin of error: 5%. The total population from the above-mentioned setting was about 120 HD patients. The estimated sample size was 92 hemodialysis patients. A total of 117 studied hemodialysis patients (HD) who are following in the previous mentioned setting and agreed to participate in the study. Data collection took place during February 2021 to April 2021. The researcher personally distributed the questionnaire to the participants before performing the AVF cannulation procedure and obtained written informed consent to record the data.
Ethical Procedure
All the participants were ensured of anonymity and their rights to privacy are protected by not disclosing any personal information. Furthermore, participants are made fully aware about the purpose of the study and an informed consent was signed by them before taking part in the study. The ethical approval has been obtained from Fundamentals of Nursing Department at the college of Nursing the Institutional Review Board (IRB) at Imam Abdulrahman Bin Faisal University in Dammam.
Statistical Analysis
The findings on each scale are initially analyzed statistically using relative frequencies for each item. Further, in order to identify the relation between the pain, anxiety, and depression, Chi-square tests, Monte Carlo, and Pearson coefficient correlation techniques are used to identify the relationship and significance.
Results
Table 1 shows the distribution of participants according to sociodemographic characteristics. Among the 117 HD patients enrolled in the study, 30 (25.6%) were in the age groups of 51–61 years old, followed by 27 (23.1%) in the age group of 62 years old and more. The majority were male (53.8%). The majority were married and holding Saudi nationality. However, 28.2% of participants had a secondary level of education and 22.2% of them were illiterate, while only 2.6% of patients had a post-graduate level of education. Moreover, the majority of the participants (82.1%) were unemployed and 68.4% of them need less than 30 minutes to arrive at hospital. In addition, it was observed that more than half of the studied HD patients (51.3%) respond with never had pain during previous cannulation.
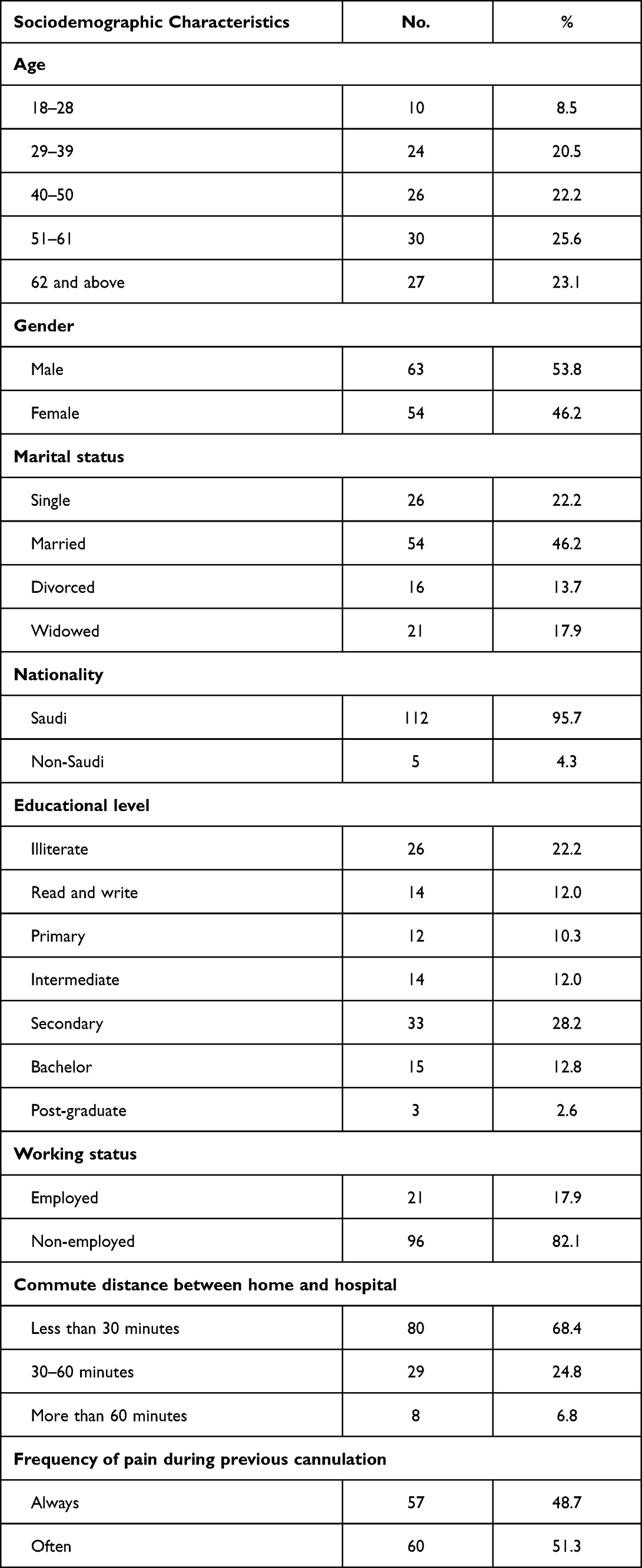 |
Table 1 Distribution of Study Participants According to Their Sociodemographic Characteristics (n=117) |
Analysis of prescription data revealed that the majority of participants were in HD for 1 year or more, having had three sessions of HD or more. The sessions lasted for 3 hours, and the majority were non-smokers. It also noticed that the “lower left arm” and “upper left arm” showed the highest use site of AVF (39.3%, 30.8%, respectively) among study participants, with 36 (30.8%) of them having used the AVF for more than 5 years. However, in the category of “Assessment of AVF”, the majority of studied HD patients (99; 84.6%) had normal thrill vascular access and 33 (28.2%) of them had an Aneurysm. Approximately half of the participants were on pain medication and 86 (73.5%) were using other medication.
Table 2 illustrates the distribution of the study participants according to their responded anxiety. The number of patients who most of the time felt tense or “wound up” was 17 (14.5%). Where 52 (44.4%) of the participants respondes “sometime” regarding the item of frightened feeling “butterflies in my chest”, regarding the item of “frightened feeling some things awful may happen”, the number of patients responding “sure and badly” and “a little but does not fear them” were 17 (14.5%%) and 35 (29.9%), respectively.
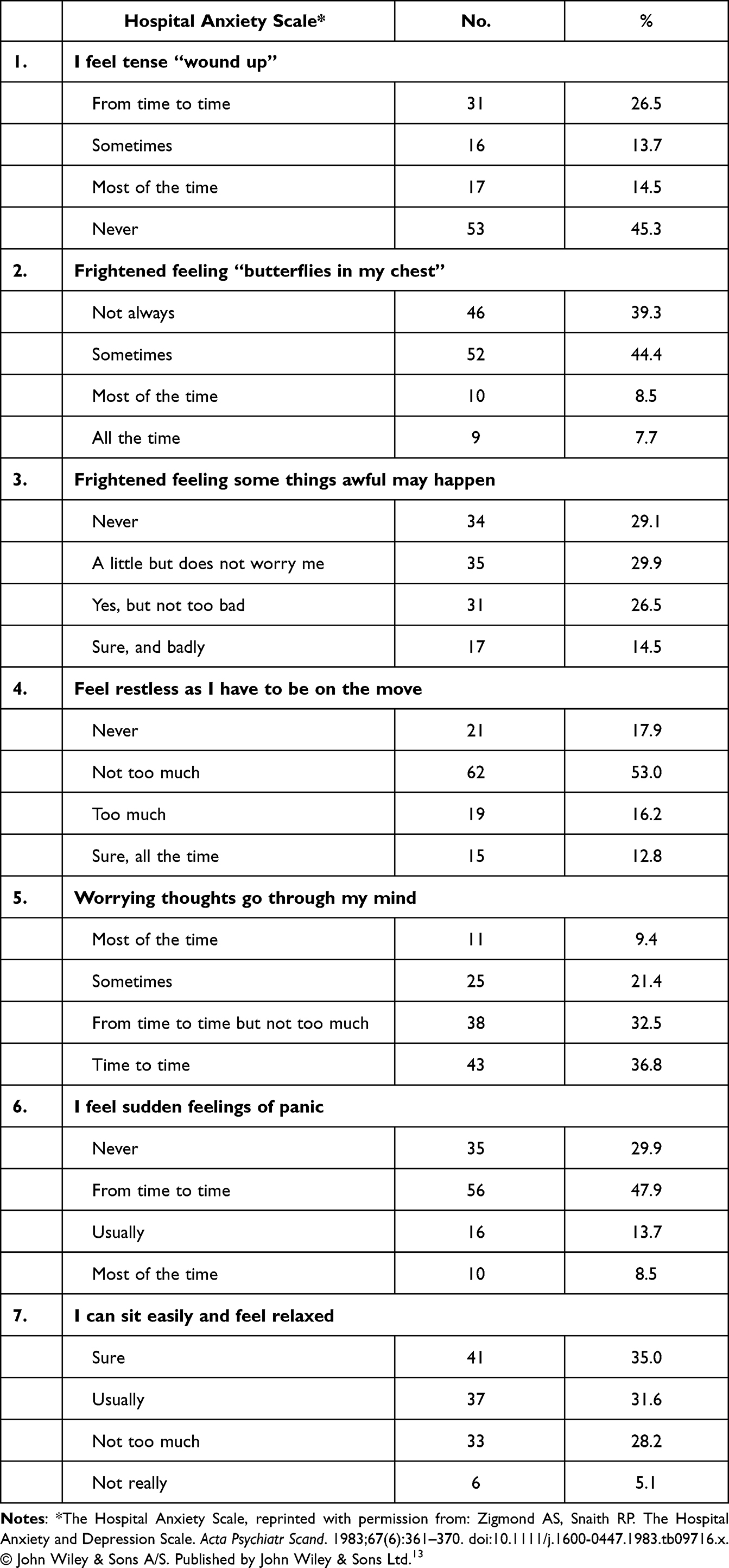 |
Table 2 Distribution of the Study Participants According to Their Responded Anxiety (n=117) |
Concerning the items of “restless feeling on moves” it was observed that 19 (16.2%) of the study participants felt too much restlessness and 15 (12.8%) felt restless sure all the time, 11 (4.9%) of study participants responded “most of the time” as regards the items of “worrying thoughts in their mind”. In relation to “sudden feeling of panic”, it was noticed that less than half of the study participants (47.9%) felt it from time to time and six (5.1%) study participants said “not really”, they can sit at ease and feel relaxed.
Figure 1 shows the distribution of the study participants according to their level of anxiety.
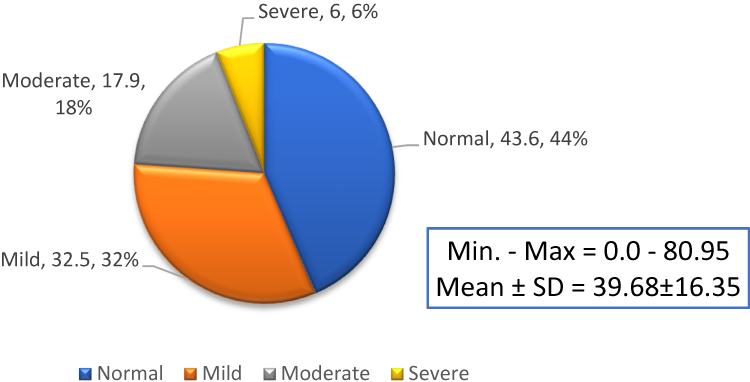 |
Figure 1 Distribution of the study participants according to their level of anxiety (n=117). |
The findings revealed that the mean score±standard deviation was 39.68±16.35 (as shown in Figure 1), the maximum score was 80.95 and the minimum score was zero. This also indicates that less than half of the tudied hemodialysis patients (32.5%) had a mild level of anxiety, while only 6% had a severe level of anxiety.
Table 3 shows the distribution of the study participants according to hospital depression. It was found that 11 (9.4%) of the study participants responded “all the time” and 50 (42.7%) of the study participants responded “sometimes” regarding “felt slowed down”. Fifty-three (45.3) of the study participants responded “not too much” to the item of “I still enjoy the things I used to enjoy”, while 23 (19.7) of the study participants responded “sure” to the item of “I have lost interest in my appearance”.
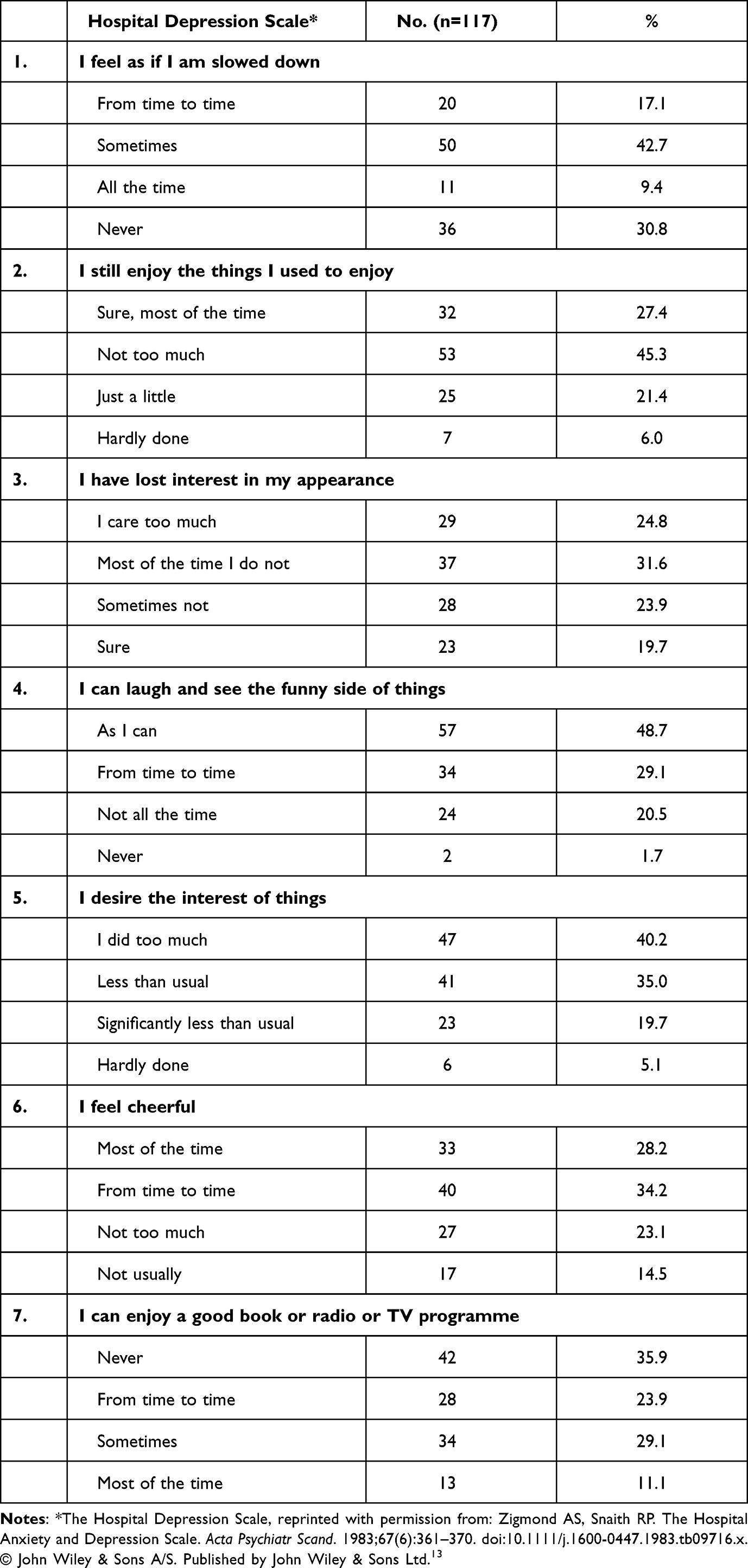 |
Table 3 Distribution of the Study Participants According to Hospital Depression |
Regarding the item of “I can laugh and see the funny side of things”, it was observed that 24 (20.5%) of the study participants respond not all the time, moreover 23 (19.7%) of them responded less than usual regarding the item of “I desire the interest of things”. In relation to the items “I feel cheerful”, it was noticed that 27 (23.1%) of the study participants responded “not too much”. It also shows that 42 (35.9%) of the patients never enjoy a good book or radio or TV programme.
Figure 2 illustrates distribution of the studied hemodialysis patients according to their level of depression. The findings revealed that the mean score ± SD was 37.12±19.85, the maximum score was 100.0, and minimum score was zero. It also indicates that a quarter of the studied hemodialysis patients (29%) had a mild level of depression, while only 4% had a severe level of depression.
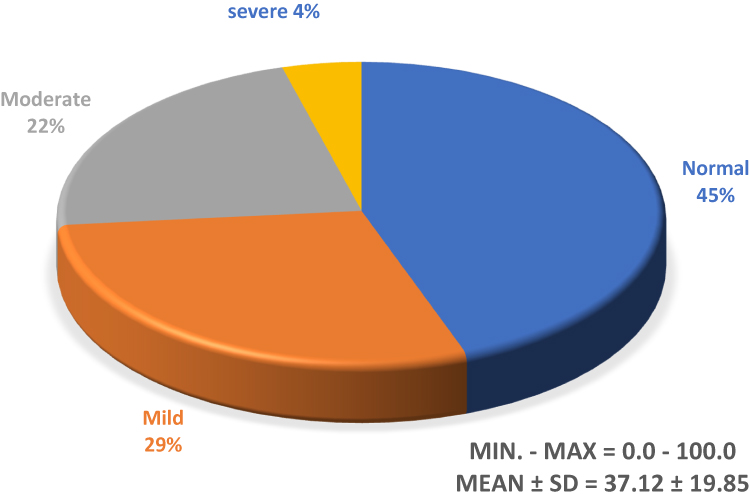 |
Figure 2 Distribution of the study participants according to their level of depression (n=117). |
Figure 3 shows distribution of the studied hemodialysis patients according to their level of pain intensity during AVF cannulation. The findings revealed that the mean score ± SD was 4.42±2.97, the maximum score was 10.0 and the minimum score was zero. It also indicates that 38 (32.5%) of the studied hemodialysis patients had moderate pain and 36 (30.8%) had mild pain, while 32 (27.4%) of them had severe pain.
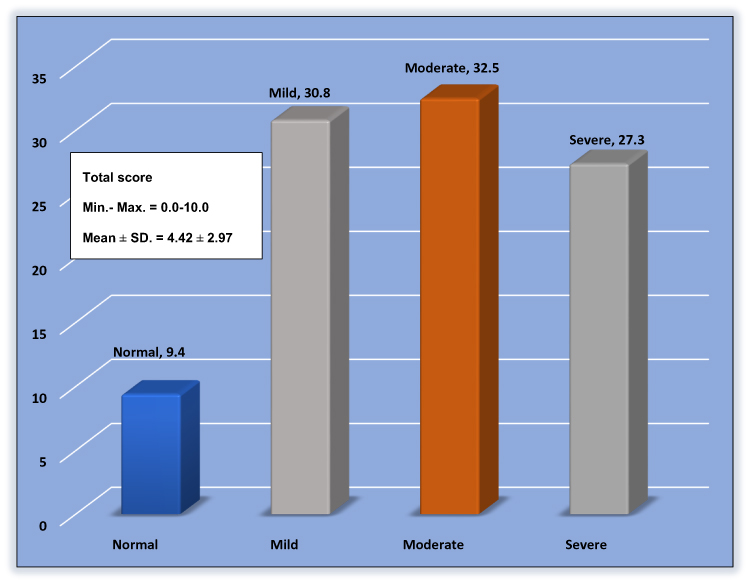 |
Figure 3 Distribution of the study participants according to their level of pain intensity during AVF cannulation (n=117). |
Table 4 and Figure 4 show the simple correlation between pain intensity with anxiety and depression among study participant regarding AVF cannulation. As a result, there is a statistically significant and positive relationship between pain intensity and level of anxiety among study participants regarding AVF cannulation (r=0.436, p<0.001).
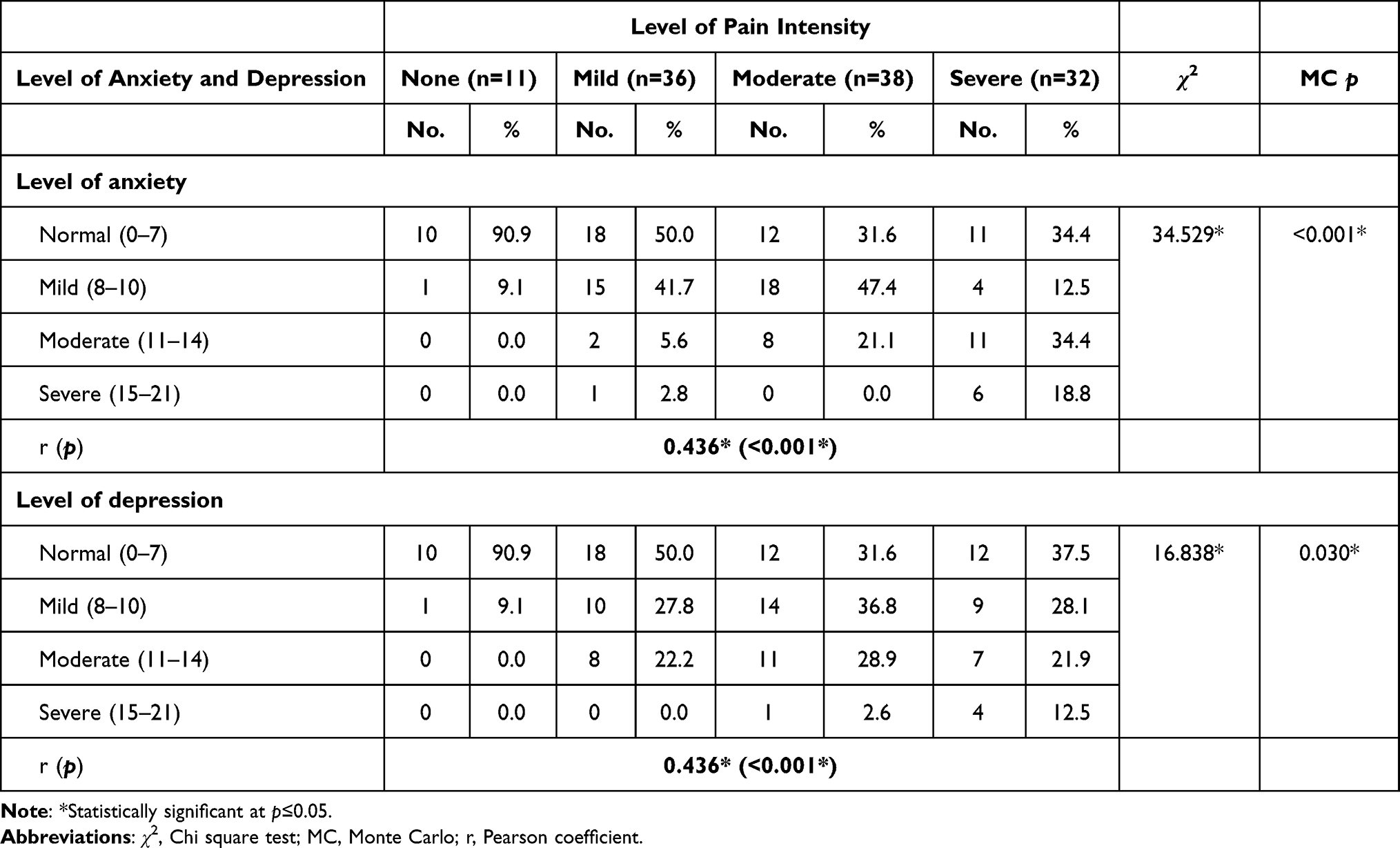 |
Table 4 Simple Correlation Analysis Between Pain Intensity with Anxiety and Depression Level Among Study Participants Regarding AVF Canulation (n=117) |
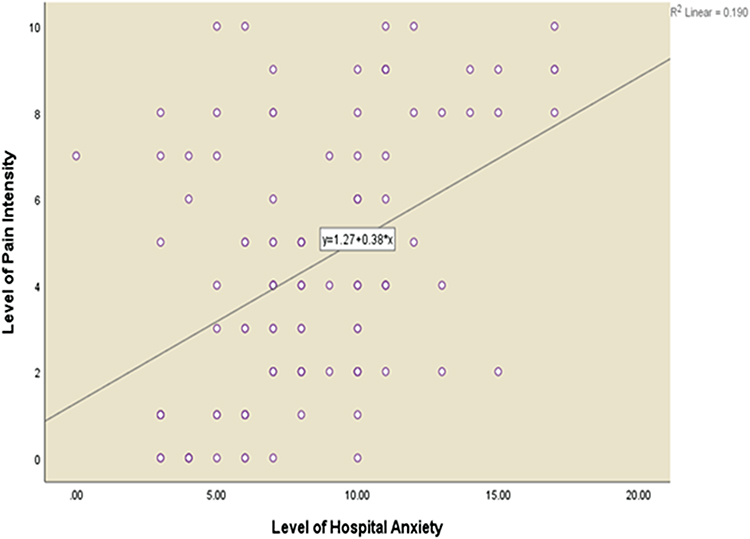 |
Figure 4 Simple correlation analysis between pain intensity with anxiety level among studied HD patients regarding AVF cannulation (n=117). |
Discussion
The Intensity of Pain During AVF Cannulation
The data of the present study showed that 38 of the HD patients (32.5%) had moderate pain during AVF cannulation. Meanwhile, 36 patients (30.8%) had mild pain. Only 32 patients (27.4%) reported severe pain during AVF cannulation. Da Silva et al16 found that around 58.5% of the sample of HD individuals reported a moderate level of pain. Of their sample, 30% reported severe pain. However, Da Silva et al16 used the VAS while this reported study used the NAS. Nevertheless, both study’s samples have a comparable level of pain. Pain is common with vascular access in HD patients. Unfortunately, pain associated with HD cannulation has not been studied extensively in research. Thus, there is a gap in the knowledge pertaining to pain and AVF cannulation among HD patients.
Arslan and Akca17 conducted a study to assess the level of pain during AVF needle insertion prior to HD. Pain was assessed using the Visual Analogue Scale (VAS). The study found that 4.8 (±2.6) out of 10 had moderate intensity. However, 25.5% of the study sample (n=26) reported severe pain (a score of 7–10) on the VAS. A study by Akca (2018) has shown that 75.7% of hemodialysis patients experience pain. Another study supported the idea that patients undergoing HD experience pain during AVF cannulation. Da Silva et al16 conducted a study in Brazil with a sample of 70 individuals undergoing HD, with 30% of participants indicating pain as intense. Davison (2003) reported that 35% of participants with CKD who undergo HD were not prescribed any analgesia for their symptoms. Only about 10 received strong opioids to manage their pain. In this regard, pain affects quality-of-life (QoL) and causes depression, anxiety, and sleep disturbances. Furthermore, pain may reduce the quality and efficiency of HD due to withdrawal or termination of sessions.11
Pain can be experienced due to various complications associated with HD such as hypertension, air embolism, etc. For instance, a significant association between the blood pressure and cardiovascular disease events in hemodialysis patients.18 Studies19,20 have suggested various approaches, such as achieving and maintaining dry weight, and using calcium channel blockers in order to minimize the impact of complications associated with HD procedures.
Anxiety Among HD Patients
The results of the current study showed that around half (56.4%) of the study participants suffer from varying degrees of anxiety during AVF cannulation. One third (38) of participants (32.5%) had mild anxiety, 21 (17.9%) had moderate anxiety, and only seven participants (6.0%) had severe anxiety during AVF cannulation. This result was expected considering the findings of similar studies. Among Saudis with CKD who are treated with HD, it was found that 19.7% of the sample had anxiety symptoms. This study included 122 individuals with CKD and 56% were females.18 The mentioned study only focused on the prevalence of depressive and anxiety symptoms among CKD patients. Meanwhile, the present study has focused on the relationship between anxiety and AVF cannulation during HD sessions.
In fact, patients undergoing hemodialysis suffer from anxiety and pain due to the insertion of hemodialysis needles, estimated to total 320 times per year. Patients still suffer from pain throughout their life or until they have a successful kidney transplantation. Such pain is caused by needle insertion into a fistula. Repeated AVF puncturing may cause adverse outcomes such as anxiety, fear, intense pain, discomfort, distress, and stress, as well as negative effects on the quality-of-life (QoL) of the patients undergoing hemodialysis.21,22
In the present finding, it was found that, during AVF cannulation, anxiety was associated with pain. The Chi-square tests indicated that as the severity of pain increases the level of anxiety increases as well (r=0.436, p=0.001). Additionally, the results show that anxiety during AVF cannulation was associated with the number of years the patients had been on HD, locations of the AVF, the condition of the AVF, weight before HD, dry weight, and their current medications (p<0.005). The other Saudi study used logistic regression to predict the anxiety scores and found that only gender was associated with anxiety. Other factors including age, duration of CKD, duration of HD, and the education level were not significant predictors of anxiety among HD Saudi patients. In comparison, the current study participants reported less severe anxiety symptoms as opposed to the other Saudi study (n=7 vs n=24).
The results were also consistent with a study conducted by Shafi and Shafi23 which concluded that the sample had moderate-to-severe anxiety. They reported that 38.5% of the sample had moderate anxiety and 34.6% of the patients had severe anxiety symptoms.
Moreover, using two measurement tools, a study reached similar conclusions. Collister et al24 conducted a study to examine the presence of depression and anxiety among ESRD and HD patients. A sample of 50 individuals (mean age of 64 years, females=52%) responded to the HADS and a single question from the Edmonton Symptom Assessment System (ESAS). They found that 56% had anxiety and 54% had depression.
In this context, assessing the level of pain and anxiety among ESRD patients undergoing HD is an important aspect of patient care to help understand the patients experience and outcomes. Depression is mostly recognized to be the most common psychological issue encountered in patients with ESRD.22 Issues such as depression and pain during HD procedures can be effectively addressed by improving the quality of service, which may result in increased patients’ satisfaction, thereby reducing the depression levels.25
Depression Among HD Patients
The results of the reported study showed that, during AVF cannulation, depressive symptoms were prevalent in 65 patients (55.6%). Thirty-four individuals (29.1%) reported mild depressive symptoms. Meanwhile, 26 patients (22.2%) had moderate depressive symptoms and five patients (5.3%) had severe depressive symptoms. The results with regards to depressive symptoms are also consistent with the findings from other research studies. A study was conducted in Brazil and had a sample of 173 older individuals. The study examined the prevalence of depression before and during their HD treatment sessions.23 The sample had a mean age of 68.7 years and were mostly males (58.4%). Depressive symptoms were present in about 43.3% (n=75) of the sample. Of the sample, 22.5% had a confirmed diagnosis of depression. Their data suggested a higher tendency to get depression among women compared to men. Depressive symptoms were measured using the Geriatric Depression scale which has five items. The International Neuropsychiatric Interview was used to confirm the diagnosis of depression. The study also examined the impact of depression on the quality-of-life (QoL). Researchers found that individuals who have depressive symptoms had lower QoL scores.26,27
An interventional study also examined the association between depression and HD. Investigators used the Hospital Anxiety and Depression Scale to collect data on depressive symptoms. The sample composed of 272 persons with an average age of 56.6 years and the majority were males. Patients who undergo HD were followed up for three visits. The prevalence of depression during the follow-up visits was 71.3%, 78.2%, and 84.9, respectively. The increased prevalence from visit 1 to visit 3 suggests that depressive symptoms worsened over time, indicating that HD patients suffer more emotionally from treatments as the time go on.25
Additionally, in the current study it was found that during AVF cannulation depression was associated with marital status, education level, travel time to dialysis location, and the presence of chronic pain.
In another study, it was found that depression as measured by the Beck’s Depression Inventory (BDI) has predicted mortality and morbidity among ESRD patients undergoing HD on both single and multiple variate analyses.28
Furthermore, the results indicated that depression was associated positively with the presence of pain so that as the pain level increases depression severity increases as well (r=0.436, p=0.030). This positive relationship suggests that, as HD patients undergo AVF cannulation, their level of pain increases and so does the level of depression. For instance, patients responded to HADS items of depression in a manner that confirms this finding. Around 42% of participants responded to the item “I feel as if I am slowed down” with “very often”, suggesting that they are impacted with some mood changes. Also, with regard to item 7 of the HADS-Depression, many patients (35.9%) stated that seldom did they enjoy a good book or TV show. This indicates that many of the patients has lost interest due to being on HD and having to go through AVF cannulation multiple times per week.
This study has certain limitations. Due to the unprecedented situation caused by coronavirus disease 2019 (COVID-19), the data collection setting has been limited to one sitting, changed from what was mentioned in the study proposal, which is a major limitation in this study. Furthermore, the pain, anxiety, and depression scales were analyzed only at a single time period, and a follow-up study was conducted. However, this study has both practical and theoretical implications. The findings suggested that courses should be developed so that nurses are prepared to manage and address the needs of patients during HD. For instance, during their residency program, future HD nurses should focus on the assessment of pain and anxiety among patients. Then about the importance of assessing and treating pain and depression and what if not treated. This study also has practical implications, as it can be used for assessing pain, anxiety, and depression; and highlights the HD patients’ trends which can be used for improving treatment procedures. Furthermore, the assessment in this study may help healthcare professionals plan and develop pain assessment and management protocols and strategies that aim to address the common signs and symptoms and improve the QoL of this group of patients.
Conclusion
In the light of the importance, it can be concluded that most of the study participants have demonstrated mild-to-moderate levels regarding pain and anxiety during arteriovenous cannulation among HD patients. In addition, there was a statistically significant difference between study participants level of pain during AVF cannulation and years on hemodialysis, site of AVF, first use of AVF, non-prescribed medication, pain medication, and other medication. Furthermore, it also showed a statistically significant and positive relationship between pain intensity and level of anxiety among study participant regarding AVF cannulation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Daugirdas JT, Black PG, Ing TS. Handbook of Dialysis.
2. Murdeshwar HN, Anjum F. Hemodialysis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
3. Feroze U, Martin D, Kalantar-Zadeh K, Kim JC, Reina-Patton A, Kopple JD. Anxiety and depression in maintenance dialysis patients: preliminary data of a cross-sectional study and brief literature review. J Ren Nutr. 2012;22(1):207–210. doi:10.1053/j.jrn.2011.10.009
4. Kallenbach J. Review of Hemodialysis for Nurses and Dialysis Personnel.
5. Hinkle J, Hinkle JL, Cheever K. The 13th Edition of Brunner & Suddarth’s Textbook of Medical-Surgical Nursing. Philadelphia: Lippincott, Williams & Wilkins; 2013.
6. Flöge J. Comprehensive Clinical Nephrology.
7. Swift O, Vilar E, Farrington K. Unexplained inflammation in end-stage kidney disease: is the combination of enhanced gastrointestinal permeability and reticuloendothelial dysfunction its cause? Semin Dial. 2019;32(5):417–423. doi:10.1111/sdi.12810
8. Cukor D, Coplan J, Brown C, et al. Anxiety disorders in adults treated by hemodialysis: a single-center study. Am J Kidney Dis. 2008;52(1):128–136. doi:10.1053/j.ajkd.2008.02.300
9. Cohen M, Baron R, Gebhart G, et al. Do we need a third mechanistic descriptor for chronic pain states? PAIN. 2016;157:1382–1386. doi:10.1097/j.pain.0000000000000507
10. Harwood L, Wilson B, Goodman M. Cannulation outcomes of the arteriovenous fistula for hemodialysis: a scoping review. Nephrol Nurs J. 2017;44(5):411–425.
11. Alzaatreh MY, Abdalrahim MS. Management strategies for pain associated with arteriovenous fistula cannulation: an integrative literature review. Hemodial Int. 2020;24(1):3–11. doi:10.1111/hdi.12803
12. Saudi Center for Organ Transplantation. Annual report for organ transplantation in Kingdom of Saudi Arabia. Available from: https://www.scot.gov.sa/Files/96d41c8d-41c9-4bd5-9f01-07abb326e2fe.pdf.
13. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
14. Mudgalkar N, Bele S, Valsangkar S, Bodhare T, Gorre M. Utility of numerical and visual analog scales for evaluating the post-operative pain in rural patients. Indian J Anaesth. 2012;56(6):553–557. doi:10.4103/0019-5049.104573
15. Tejada JJ, Punzalan JRB. On the misuse of Slovin’ s formula. Philipp Stat. 2012;61(1):129–136.
16. Da Silva O, Rigon E, Corradi Dalazen J, Bissoloti A, Rabelo-Silva E. Pain during arteriovenous fistula cannulation in chronic renal patients on hemodialysis. Open J Nurs. 2016;6(12):1028–1037. doi:10.4236/ojn.2016.612098.
17. Arslan DE, Akca NK. Pain following needle insertion into a hemodialysis fistula and influencing factors. Int J Caring Sci. 2018;11(3):1662–1667.
18. Khan A, Khan A, Adnan A, Syed Sulaiman S, Gan S, Khan I. Management of patient care in hemodialysis while focusing on cardiovascular disease events and the atypical role of hyper- and/or hypotension: a systematic review. Biomed Res Int. 2016;2016:1–10.
19. Khan A, Khan A, Adnan A, Sulaiman S, Ahmad N, Gan S. Evaluation of factors affecting time to achieve dry weight among hemodialysis patients using bioimpedance spectroscopy. Irish J Med Sci. 2018;188(1):311–319. doi:10.1007/s11845-018-1813-2
20. Khan A, Khan A, Adnan A, et al. Hypertension control among euvolemic hypertensive hemodialysis patients in Malaysia: a prospective follow-up study. J Pharma Policy Pract. 2019;12(1). doi:10.1186/s40545-019-0169-y
21. Mosleh H, Alenezi M, Al Johani S, Alsani A, Fairaq G, Bedaiwi R. Prevalence and factors of anxiety and depression in chronic kidney disease patients undergoing hemodialysis: a cross-sectional single-center study in Saudi Arabia. Cureus. 2020;12(1):e6668. doi:10.7759/cureus.6668
22. Gong L, Liu J, Yan J, Wang L. Effect of puncture-related pain on the quality of life in patients undergoing maintenance hemodialysis through internal arteriovenous fistula. J Cent South Univ Med Sci. 2014;39(12):1292–1298.
23. Shafi ST, Shafi T. A comparison of anxiety and depression between pre-dialysis chronic kidney disease patients and hemodialysis patients using hospital anxiety and depression scale. Pak J Med Sci. 2017;33(4):876–880. doi:10.12669/pjms.334.12656
24. Collister D, Pyne L, Cunningham J, et al. Multidisciplinary chronic kidney disease clinic practices: a scoping review. Can J Kidney Health Dis. 2019;6:2054358119882667. doi:10.1177/2054358119882667
25. Khan A, Khan A, Adnan A, Sulaiman S, Mushtaq S. Prevalence and predictors of depression among hemodialysis patients: a prospective follow-up study. BMC Public Health. 2019;19(1). doi:10.1186/s12889-019-6796-z
26. Shirazian S, Grant CD, Aina O, Mattana J, Khorassani F, Ricardo AC. Depression in chronic kidney disease and end-stage renal disease: similarities and differences in diagnosis, epidemiology, and management. Kidney Int Rep. 2016;2(1):94–107. doi:10.1016/j.ekir.2016.09.005
27. de Alencar SB, de Lima FM, Dias LD, et al. Depression and quality of life in older adults on hemodialysis. Rev Bras Psiquiatr. 2020;42(2):195–200. doi:10.1590/1516-4446-2018-0345
28. Kimmel P, Peterson R. Depression in patients with end-stage renal disease treated with dialysis: has the time to treat arrived? Clin J Am Soc Nephrol. 2006;1(3):349–352. doi:10.2215/CJN.00890306
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.