Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Assessment of Knowledge, Attitudes, and Practices on Antibiotic Use and Resistance Among Healthcare Workers in Monrovia, Liberia: A Facility-Based Cross-Sectional Study
Authors Shobayo BI ![]() , Taylor VS, Freeman BM, Kokro JS, Chea SKP
, Taylor VS, Freeman BM, Kokro JS, Chea SKP
Received 2 September 2025
Accepted for publication 8 November 2025
Published 19 November 2025 Volume 2025:17 Pages 253—264
DOI https://doi.org/10.2147/DHPS.S564658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Bode Ireti Shobayo,1,2,* Victor Saah Taylor,1,* Bluefin Masell Freeman,1,2 James Saysay Kokro,2 Sampson K P Chea1
1Department of Biological Sciences, University of Liberia, Louisiana, Liberia; 2Division of Public Health and Medical Research, National Public Health Institute of Liberia, Monrovia, Liberia
*These authors contributed equally to this work
Correspondence: Bode Ireti Shobayo, Division of Public Health and Medical Research, National Public Health Institute of Liberia, Monrovia, Liberia, Tel +231775912252, Email [email protected]; [email protected]
Background: Globally, healthcare systems are currently facing a significant challenge in terms of antibiotic resistance. Healthcare professionals actively participate in the process of prescribing, dispensing and administering antibiotics.
Objective: We examined the knowledge, attitudes and practices regarding antibiotic use and antibiotic resistance among healthcare professionals working in a tertiary hospital located in Monrovia, Liberia.
Methods: A hospital-based cross-sectional survey was carried out from January to June, 2023 involving 61 healthcare workers at the ELWA Hospital, Liberia. A purposive sample of healthcare workers across diverse professional roles was surveyed using a structured questionnaire on antibiotic use and resistance. Data were analyzed in SPSS v25 using descriptive statistics to summarize participant characteristics and inferential tests to explore variable associations.
Results: Participants ages ranged from 20 to 60 years (mean = 40.7 ± 5) and nurses constituted the majority professional group (59%). Most respondents (68.9%) disagreed that antibiotics are effective against viral infections (OR = 0.45; p = 0.020). However, 36.1% believed antibiotics could be stopped when symptoms resolve and 24.6% believed leftover antibiotics could be reused (OR = 0.33; p = 0.002). Majority, 72.1% and 70.5%, reported never using antibiotics for body pain or headaches, respectively (OR = 3.67; p = 0.001 and OR = 4.78; p < 0.001). Despite this, 39.3% admitted to sometimes or always storing leftover antibiotics and 39.3% agreed or strongly agreed that stopping antibiotics early is safe (OR = 0.36; p = 0.016).
Conclusion: The study identified persistent gaps in healthcare workers’ knowledge, attitudes, and practices regarding antibiotic use and resistance, despite encouraging awareness in some areas. Misconceptions such as premature discontinuation and reuse of leftover antibiotics were common. Findings underscore the need for targeted education and strengthened stewardship programs in Liberia’s healthcare settings.
Plain Language Summary: This study looked at how healthcare workers in Monrovia, Liberia understand and use antibiotics. It focused on their knowledge, beliefs, and everyday practices related to antibiotic use and resistance, a growing global health problem. Researchers surveyed 61 healthcare workers at ELWA Hospital, a major health facility in Monrovia. Participants included nurses, doctors, pharmacists, lab technicians, and midwives. They answered a structured questionnaire designed to measure what they know, how they feel, and what they do when it comes to antibiotics.
The study found that most healthcare workers knew that antibiotics do not work against viruses and should not be used for things like headaches or body pain. However, many still held incorrect beliefs like thinking it is okay to stop antibiotics early or reuse leftover medicine. Nearly 40% admitted to storing leftover antibiotics, and some disposed of them improperly. On the positive side, most participants followed infection prevention guidelines and recognized antibiotic resistance as a serious public health threat.
Antibiotic resistance makes infections harder to treat and is especially dangerous in places with limited healthcare resources. Healthcare workers play a key role in preventing resistance, so it is important they have accurate information and follow best practices. The study shows that while awareness is improving, there are still gaps that need to be addressed. Targeted training and stronger hospital policies can help healthcare workers use antibiotics more responsibly and protect public health in Liberia.
Keywords: knowledge, attitudes, practices, antibiotic resistance, antibiotic use, healthcare workers, Liberia
Introduction
Since their introduction, antibiotics have become routine in treating infectious diseases, significantly reducing disease-related morbidity and mortality.1 Recent data, however, point to a significant issue for public health because of the rise in antibiotic resistance.2,3 The World Health Organization (WHO) has identified antimicrobial resistance (AMR) as among the top 10 global public health challenges to mankind4 with approximately 700,000 people die each year as a result of infections with antibiotic-resistant (ABR) organisms.5,6 The impact of ABR is especially severe in low- and middle-income settings, where limited diagnostics and stewardship measures amplify irrational antibiotic use.7–10 These systemic weaknesses highlight the need to examine the human factors, particularly healthcare workers’ behaviors and practices that influence antibiotic use and resistance dynamics.
Several studies have shown that knowledge, attitudes, and practices (KAP) regarding antibiotic use are often inadequate, even among healthcare professionals, leading to inappropriate prescribing and misuse of antibiotics. In many contexts, healthcare workers lack sufficient understanding of antimicrobial resistance mechanisms, appropriate antibiotic selection, and guideline-based prescribing, while attitudes such as patient-pressure compliance and misconceptions about antibiotic efficacy further compound the problem.11–13 These deficiencies in KAP contribute directly to irrational antibiotic use, including self-medication, over-prescription, and incomplete treatment courses, all of which accelerate the development and spread of resistant pathogens.14 The consequences of rising antibiotic resistance are profound, resulting in prolonged illnesses, higher healthcare costs, limited treatment options, and increased morbidity and mortality, particularly in resource-limited settings.5,10
Irrational medication use in Liberia is related to systemic issues such as the high frequency of use of expired medications and insufficient numbers of trained healthcare providers. In many cases, health facility dispensaries may also be inadequately maintained and personnel may not be aware, therefore do not consult the standard treatment guidelines and essential medicines list when prescribing.15 The escalating threat of ABR in the country presents a critical challenge to an already fragile health system, which continues to recover from the compounded effects of civil conflict and past epidemics.16 These systemic gaps hinder effective antibiotic stewardship and increase the risk of resistant infections across healthcare settings.17,18
Despite these realities, there remains a critical lack of empirical evidence on the knowledge, attitudes, and practices (KAP) of healthcare professionals regarding antibiotic use and resistance. Most existing studies on ABR in sub-Saharan Africa have focused on microbiological surveillance and antibiotic consumption trends, with less attention to the behavioral and systemic factors driving irrational antibiotic use among healthcare workers. This knowledge gap constrains the development of context-specific interventions that could strengthen antimicrobial stewardship and guide national policy implementation. Therefore, this study was conducted to assess the knowledge, attitudes, and practices of healthcare workers regarding antibiotic use and resistance at the Eternal Love Winning Africa (ELWA) Hospital in Montserrado County, northwestern Liberia. Findings from this study are intended to inform tailored educational strategies, enhance institutional stewardship programs, and contribute evidence to support the formulation of Liberia’s renewed National Action Plan on AMR.
Materials and Methods
Study Setting and Design
This cross-sectional study was conducted from January to June, 2023, at the ELWA Hospital, a prominent tertiary healthcare facility located in Paynesville, Montserrado County, within the capital city of Monrovia, Liberia. The ELWA Hospital, with at least 250 beds, serves as a critical hub for both general and specialized medical services in Liberia, operating under the auspices of the ELWA Ministries and playing a significant role during past public health emergencies,19 including the Ebola outbreak. The hospital houses multiple clinical departments—including internal medicine, surgery, pediatrics, obstetrics and gynecology, and emergency care—and is supported by functional laboratory and pharmacy units. Its workforce comprises a diverse group of healthcare professionals, including doctors, nurses, laboratory technicians, pharmacists, and midwives, who provide care to a high-volume patient population drawn from both urban and peri-urban communities. This setting offers a representative context to evaluate HCWs knowledge and practices related to ABR, particularly given Liberia’s growing emphasis on infection prevention and control (IPC), antibiotic stewardship, and ongoing post-Ebola health system strengthening efforts.
Study Population and Sample Size
While the ELWA Hospital hosts a larger pool of healthcare professionals across various departments, a sample size of 61 participants (Nurses – 36, Pharmacists – 8, Doctors – 7, Laboratory technicians - 6, Midwives – 4) was deemed adequate based on logistical feasibility, time constraints, and resource availability. This sample was selected purposively to include diverse cadres—such as nurses, physicians, laboratory staff, midwives and pharmacists—ensuring representation of key professional roles relevant to antibiotic use and stewardship. The size was also informed by precedent in similar facility-based KAP studies, where samples of 50–100 HCWs have yielded sufficient variability for meaningful analysis.20,21 Additionally, the study aimed for depth of insight rather than breadth, using structured questionnaires and stratified analysis to explore patterns of knowledge and behavior among actively practicing professionals. As such, the sample of 61 was both methodologically sound and practical given the institutional context and study objectives.
Data Collection
A structured questionnaire was adapted from previously validated instruments assessing KAP related to antibiotic use and ABR.22,23 The tool was modified to fit the study context and content was reviewed independently by two subject matter experts in pharmacy and public health to assess its relevance, clarity, and comprehensiveness. Iterative revisions were made until a content validity index (CVI) of ≥0.70 was achieved, with the final instrument attaining a CVI of 0.79, indicating satisfactory content validity.24 To further refine the questionnaire, a pilot test was conducted among 10 HCWs who were excluded from the main analysis. Internal consistency reliability was evaluated using Cronbach’s alpha, which yielded a coefficient of 0.79, reflecting acceptable reliability.
The final questionnaire comprised 35 items divided into four sections. Section I collected demographic information, including age, sex, academic qualification, and professional cadre. Section II consisted of 12 dichotomous (“true”/“false”) items assessing knowledge of antibiotic use and resistance, with correct answers scored as 1 and incorrect responses as 0. Certain statements in the knowledge assessment were designed to identify common misconceptions about antibiotic use, even if they could be interpreted as technically true in narrow clinical contexts. For the purpose of this survey, participants were instructed to interpret the statements in the context of general, non-prescribed, or patient-initiated use. Specifically, the statement “Antibiotics are effective in preventing infectious diseases” was intended to be marked “False”. The correct interpretation is that antibiotics are not effective for the general prevention of community-acquired infectious diseases by individuals and should only be used for prophylaxis under specific, direct medical supervision (eg, prior to surgery). Section III included 9 statements evaluating attitudes toward antibiotic use and ABR. Responses to positively worded items were scored on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree), while negatively worded items were reverse-coded. Section IV assessed self-reported practices using 10 items, with appropriate behaviors scored on a scale from 0 (“never”) to 2 (“always”) and reverse scoring applied to inappropriate practices.
Statistical Analysis
Data were entered into a database created with Microsoft Excel 2016, cleaned and verified for completeness. The Statistical Package for Social Sciences (SPSS) version 25 (IBM USA) was used to analyze the data. Descriptive data analyses was conducted, which involved summarizing frequencies and percentages into categorical variables, which included the general characteristics of the participants. KAP items were individually scored, and composite mean scores were calculated and treated as continuous variables for initial analysis. To further explore associations between selected independent variables and higher KAP scores, multivariable logistic regression models were employed to derive Odds Ratios (ORs). For this purpose, responses were dichotomized to generate a binary outcome reflecting “Positive Attitude” versus “Negative/Neutral Attitude”. Coding decisions were guided by the evidence-based desirability of each statement. For desirable statements (eg, “Antibiotics should be taken only when prescribed”), responses of “Strongly Agree” or “Agree” were classified as indicating a positive attitude. Conversely, for undesirable statements (eg, “It is okay to share leftover antibiotics”), responses of “Strongly Disagree” or “Disagree” were coded as positive. The resulting ORs thus represented the likelihood of respondents expressing a positive attitude toward appropriate antibiotic use. The threshold for determining statistically significant differences was established at a significance level of p < 0.05.
Results
Demographic Characteristics of Study Participants
A total of 61 healthcare workers participated in the study. The mean age of the study participants was 40.7 years; interquartile range (IQR): 32–45. Males accounted for 19 (31.1%) of the participants while 42 (68.9%) were females. The majority of participants were nurses 36 (59%), followed by pharmacists 8 (13.1%), doctors 7 (11.4%) laboratory technicians 6 (9.8%) and midwives 4 (6.5%). Regarding academic qualification, most participants 28 (45.9%) were high school diploma holders followed by Bachelor’s degree holders 22 (36%), and Masters’ degree holders 11 (18%) (Table 1).
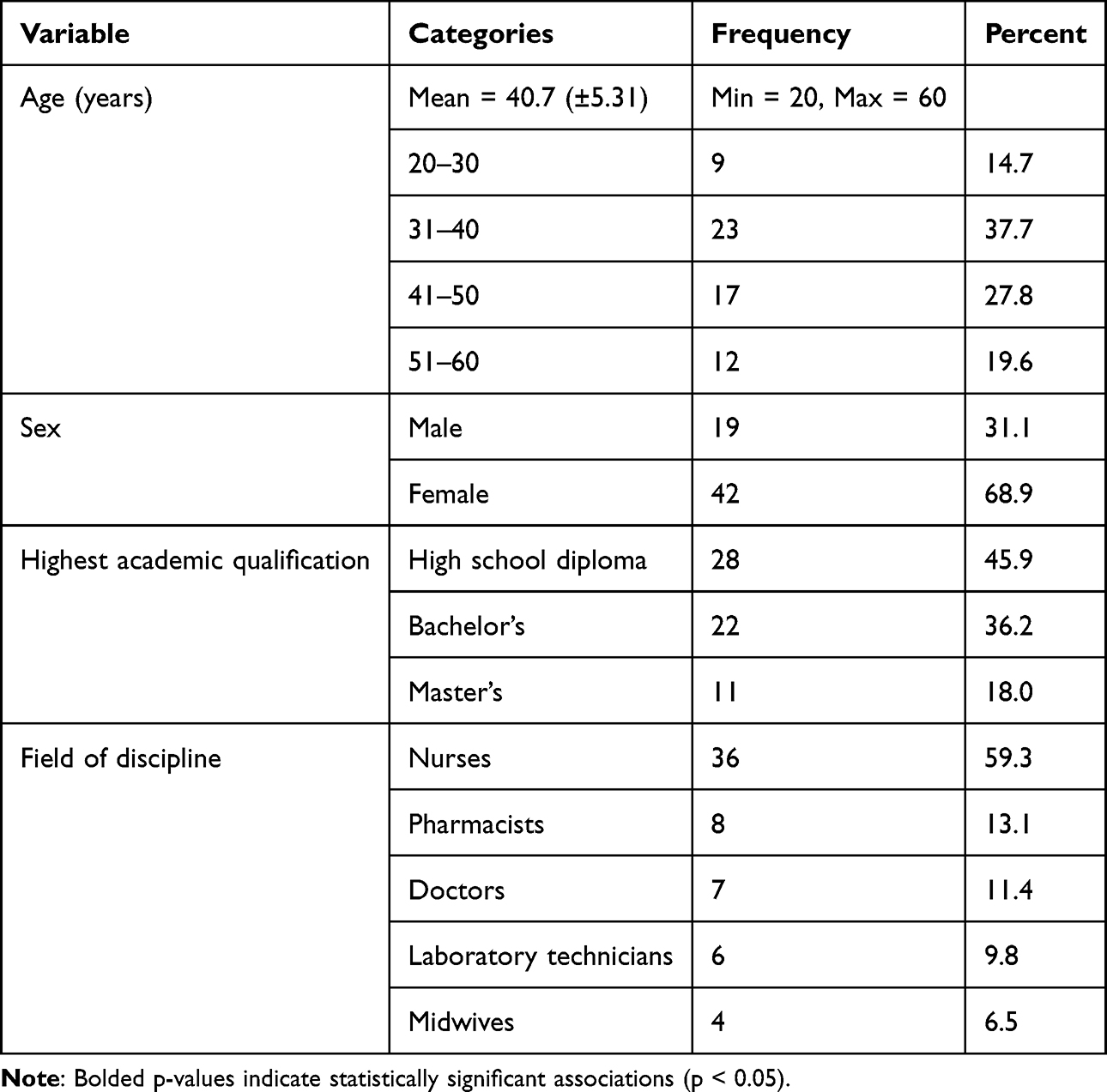 |
Table 1 Demographic Characteristics of the Participants (n=61) |
Knowledge of ABR Among Study Participants
Regarding understanding of the appropriate use of antibiotics, 70.5% of respondents correctly disagreed with the statement that antibiotics are effective in preventing infectious diseases. This response was significantly associated with higher knowledge scores (Odds Ratio [OR] = 0.42; 95% Confidence Interval [CI]: 0.21–0.83; p = 0.012). Similarly, 68.9% of participants disagreed that antibiotics are effective against viral infections (p = 0.020). However, 36.1% incorrectly believed that antibiotics could be discontinued once symptoms resolve, and the same proportion also believed antibiotics reduce fever and allergies. Close to a quarter of respondents (24.6%) believed leftover antibiotics can be reused and this misconception was significantly associated with lower knowledge levels (OR = 0.33; p = 0.002) (Table 2).
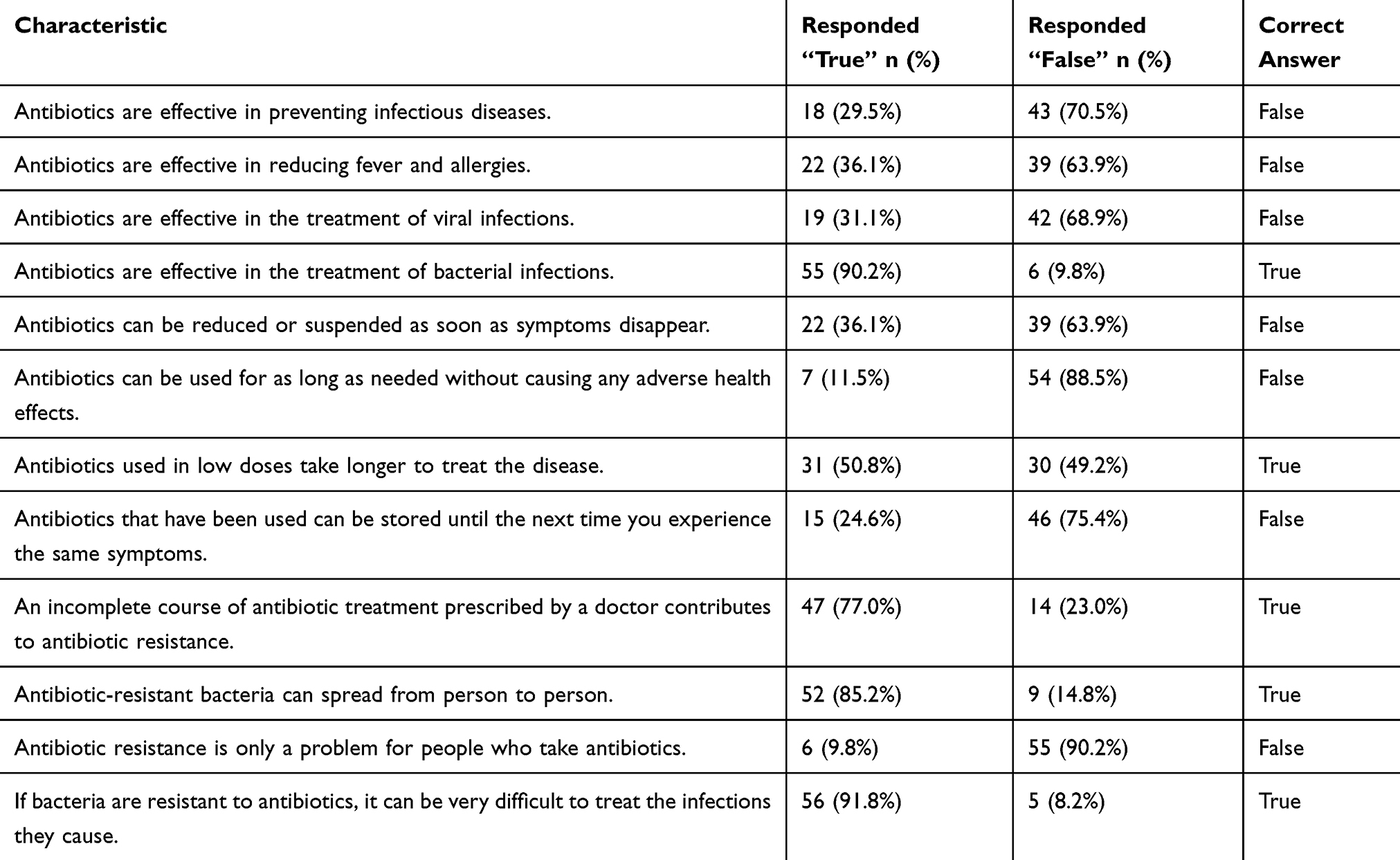 |
Table 2 Overall Knowledge of Antibiotic Use and ABR Among Study Participants (n = 61) |
Attitude Towards Antibiotic Use and ABR
Up to 18% of respondents (11.5% agreeing, 6.6% strongly agreeing) believed it is acceptable to share leftover antibiotics with others while 39.3% of participants agreed or strongly agreed that it is safe to stop taking antibiotics once symptoms improve. This belief was statistically associated with negative attitudes toward antibiotic use (OR = 0.36; p = 0.016). A minority of participants (8.2%) expressed distrust in healthcare workers’ prescribing practices and the majority rejected the idea that pharmacists should sell antibiotics without prescriptions, with 68.8% disagreeing or strongly disagreeing (OR = 0.20; 95% CI: 0.07–0.54; p = 0.002). Less than a quarter (14.7%) either agreed or strongly agreed with the false notion that antibiotic resistance only affects individuals who misuse antibiotics (Table 3).
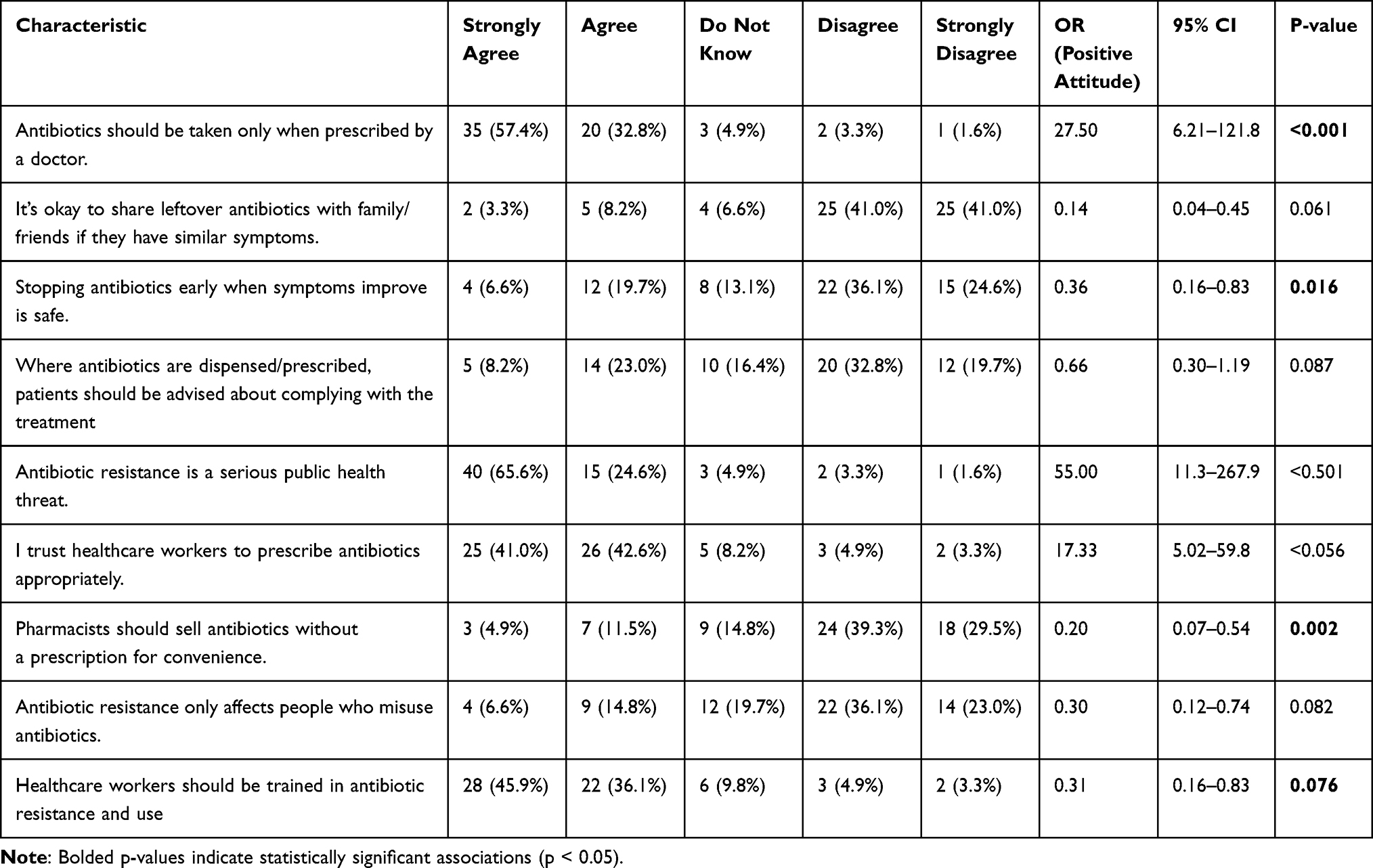 |
Table 3 Attitude Towards Antibiotic Use and ABR Among Study Participants (n = 61) |
Practices Towards Antibiotic Use and ABR
A majority of respondents reported never using antibiotics for body pain (72.1%) or headaches (70.5%), behaviors that were significantly associated with safe practices (ORs: 3.67 and 4.78; p=0.001 and p<0.001, respectively). Despite these encouraging findings, approximately 39.3% admitted to sometimes or always keeping leftover antibiotics. Notably, 77.0% consistently adhered to infection prevention and control protocols (p<0.001). However, 16.4% indicated they always discard antibiotics in regular trash, highlighting a persistent gap in proper medication disposal practices (Table 4).
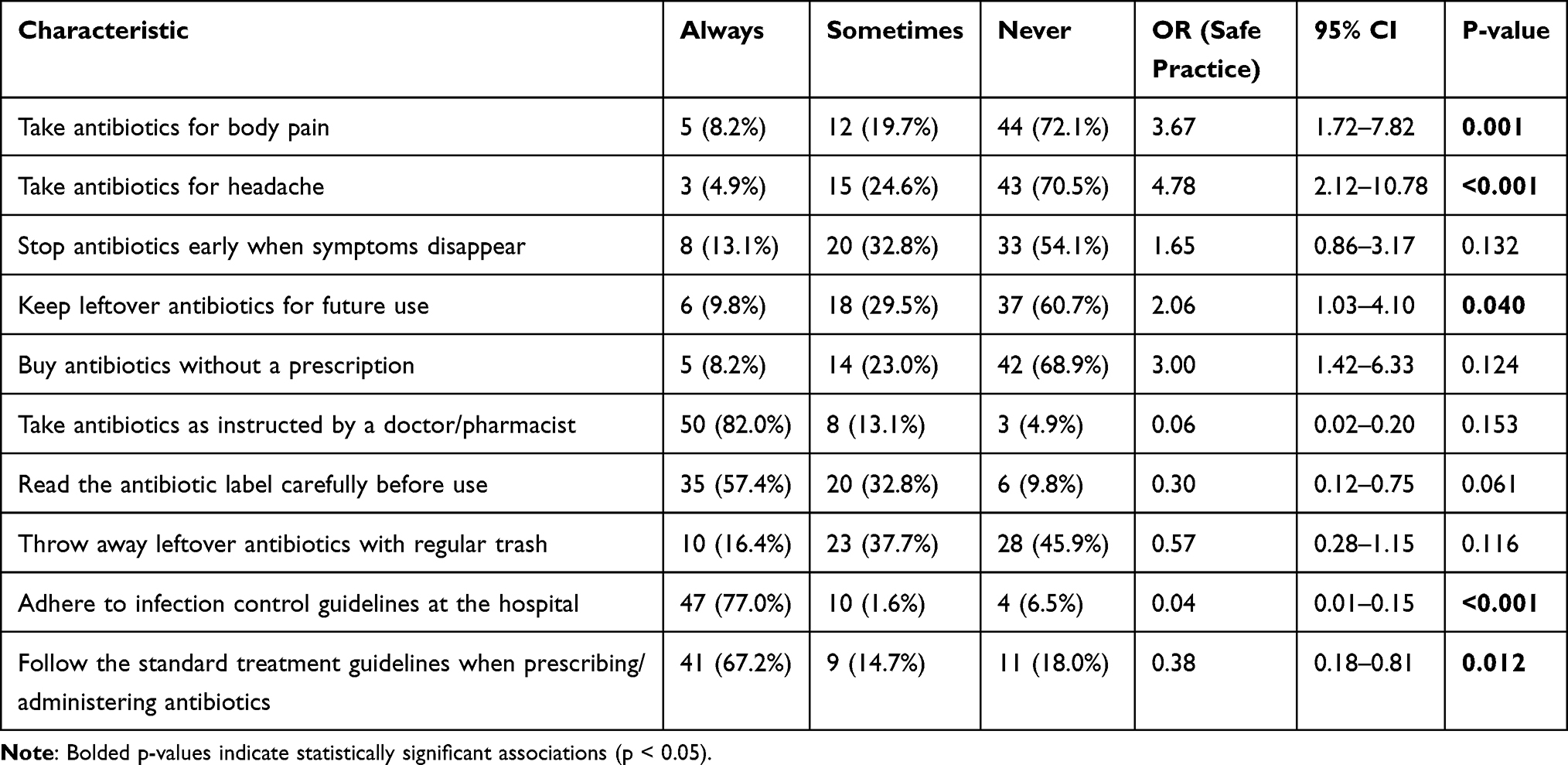 |
Table 4 Practices Towards Antibiotic Use and ABR Among Study Participants (n = 61) |
Association Between Demographic Characteristics Knowledge on Antibiotic Use and ABR
The analysis of factors associated with comprehensive knowledge on antibiotic use and resistance revealed several significant associations. Participants holding a Bachelor’s degree demonstrated significantly higher odds of correct knowledge compared to those with a high school diploma. Similarly, when compared to nurses, doctors were significantly more likely to possess accurate knowledge. An association was also observed with age, as individuals in the 31–40 year age group had greater odds of correct knowledge than their younger counterparts (20–30 years). Conversely, female participants showed significantly lower odds of high knowledge scores compared to males. No other categories for academic qualification, age, or field of discipline showed statistically significant associations (Table 5).
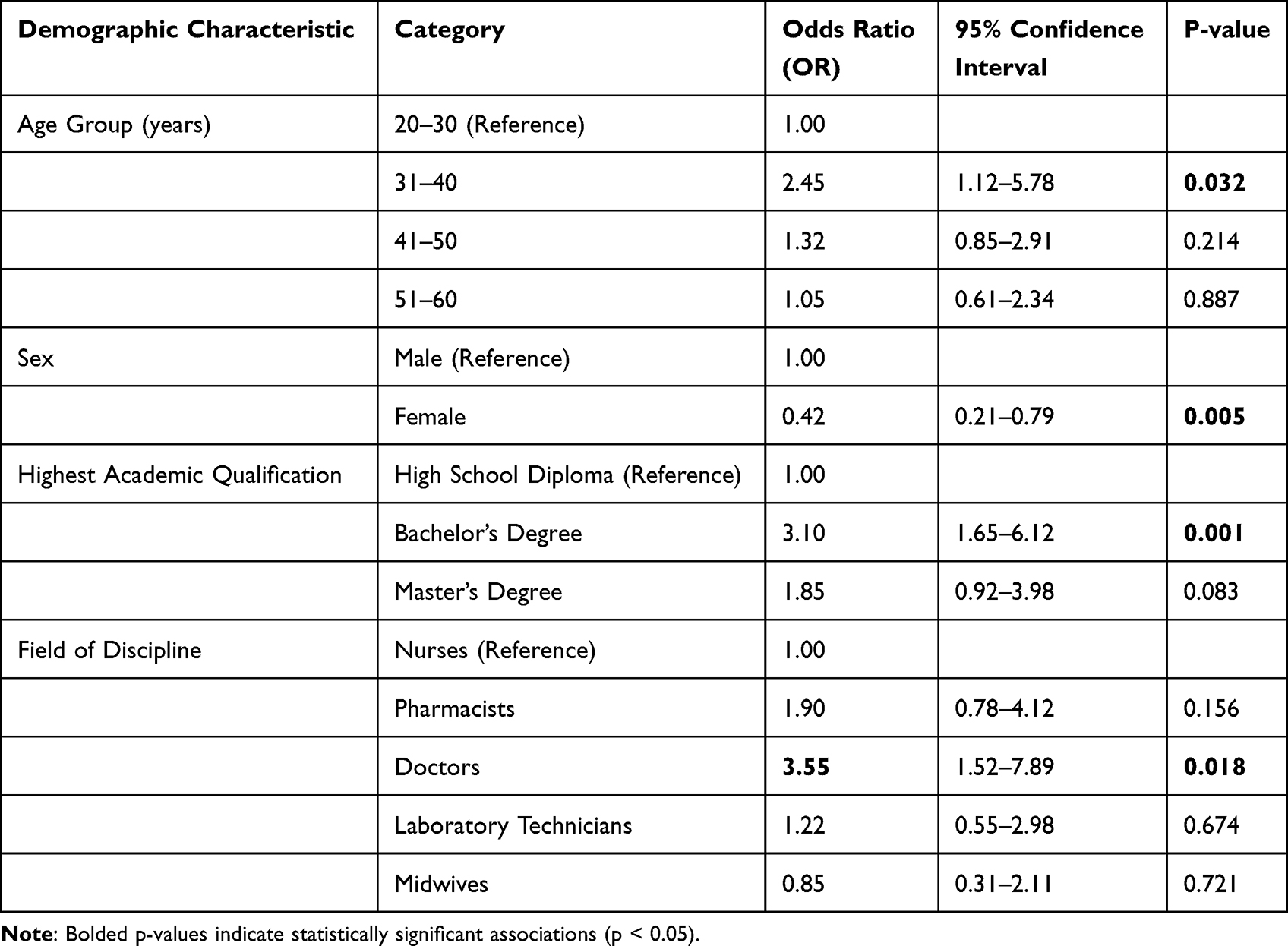 |
Table 5 Association Between Demographic Characteristics and Overall Correct Knowledge on Antibiotic Use and Resistance |
Discussion
Healthcare professionals have a crucial role in preventing the development and spread of ABR by educating patients and minimizing the spread of infections in healthcare settings, especially when treating infections by prescribing, dispensing, and administering antibiotics.24,25 The objective of this study was to assess the level of knowledge regarding antibiotic resistance and its related aspects among healthcare professionals. Our study has several significant findings.
The mean age of the participants was 40.7 years, suggesting a relatively mature and experienced workforce, and the majority were female (68.9%), with nurses comprising the largest professional group (59%). These demographics align with similar studies in sub-Saharan Africa, where the healthcare workforce is predominantly female and nursing-led.11,26 The educational background of the participants was varied, with nearly half holding only a high school diploma. This finding is significant as prior studies have shown that the level of formal education is a strong determinant of knowledge and appropriate use of antibiotics.27,28
Most participants (70.5%) correctly disagreed with the statement that antibiotics prevent infectious diseases, and 68.9% recognized their ineffectiveness against viral infections, reflects a relatively strong foundational understanding of antibiotic use. These results are more favorable than those reported in a global WHO multi-country survey, where 64% of respondents incorrectly believed antibiotics could treat viral infections such as colds and flu.29 Similarly, a study among university students in Saudi Arabia found that 46% mistakenly believed antibiotics were effective against viral infections, and 53% thought viruses could develop antibiotic resistance.30 However, the persistence of misconceptions in the present study—such as the belief by 36.1% of participants that antibiotics can be stopped once symptoms resolve or that they reduce fever and allergies—mirrors findings from other regions. For instance, a European Delphi study identified widespread confusion about the role of antibiotics in managing non-bacterial symptoms like fever and allergies, even among healthcare professionals.31 These misconceptions are critical, as they can lead to premature discontinuation of treatment and inappropriate prescribing, both of which are known contributors to ABR.29,32 The contrast between accurate knowledge on some core principles and lingering myths underscores the need for targeted, behavior-focused education that goes beyond factual awareness to address ingrained beliefs and practices.
In this study, 24.6% of participants believed leftover antibiotics could be reused, and 18% considered it acceptable to share them with others. Additionally, 39.3% agreed or strongly agreed that stopping antibiotics once symptoms improve is safe—a belief that was significantly associated with negative attitudes toward appropriate antibiotic use. These findings are consistent with evidence from other regions. For instance, a US survey found that 26% of adults had used leftover antibiotics, and over half intended to do so again, often citing convenience as justification.33 In Canada, another study reported that 73% of parents who stored leftover antibiotics had shared them with others.34 The misconception around stopping treatment early is echoed in studies from the UK, where patients frequently discontinued antibiotics upon symptom relief, despite clinical guidance.35 While emerging research suggests shorter antibiotic courses may be effective for select conditions, treatment duration should remain under clinical oversight, as emphasized by the WHO.36 These persistent misconceptions underscore the importance of reinforcing stewardship principles through targeted, behavior-focused interventions—even among healthcare professionals.
It was revealed in this study that 91.8% of participants recognized antibiotic-resistant infections as harder to treat and understood that ABR can affect everyone—not just those who misuse antibiotics. This is highly encouraging and suggests a strong foundational awareness. This contrasts with some global trends where misconceptions remain widespread. For instance, a WHO multi-country survey found that 64% of respondents incorrectly believed antibiotics could treat viral infections, and many assumed ABR only affects individuals who misuse antibiotics.31 Similarly, a study in Saudi Arabia reported that 53% of university students believed viruses could develop antibiotic resistance, reflecting confusion about ABR mechanisms.30 In contrast, only 14.7% of participants in the present study endorsed the false notion that ABR affects only misusers, indicating a more nuanced understanding. These findings align with the WHO’s assertion that ABR is a universal threat, affecting even those who have never taken antibiotics, due to the spread of resistant pathogens through healthcare settings, food systems, and the environment.7 The relatively high awareness observed in this study may reflect the impact of targeted professional training or national stewardship efforts, and underscores the value of continued investment in ABR education across all sectors.
The majority of participants, 72.1% and 70.5%, reported never using antibiotics for body pain and headaches, respectively, reflecting a commendable level of awareness and aligns with responsible antibiotic use practices. This contrasts with findings from a study among healthcare students at the University of Rwanda, where 50% believed antibiotics were appropriate for treating pain and inflammation, indicating persistent misconceptions among future prescribers.37 Similarly, in a multicenter study across Kenya, antibiotics were prescribed in 73% of outpatient visits, with nearly half lacking a confirmed bacterial diagnosis—suggesting frequent empirical use, potentially including for non-bacterial symptoms like pain and headache.38 A systematic review across African hospitals also reported high antibiotic use for non-specific symptoms, with prevalence ranging from 27.6% to 83.5%, particularly in West and North Africa.39 Compared to these studies, the present findings suggest a more cautious and informed approach among participants, possibly reflecting the impact of targeted stewardship interventions or professional experience. Nonetheless, the contrast with student and outpatient populations underscores the need for continued education and system-wide reinforcement of appropriate antibiotic use.
The finding that 39.3% of participants admitted to storing leftover antibiotics and 16.4% regularly discarded them in household trash aligns with trends observed in other low- and middle-income settings, where improper disposal remains a persistent challenge. For instance, a study in Kisumu, Kenya reported that over half of respondents kept leftover antibiotics for future use, and 32% disposed of them in pit latrines or compost pits, with only 4% using safer methods like burning.40 Similarly, in Mwanza, Tanzania, 75.5% of households disposed of unused medications in domestic trash, and 15.5% in pit latrines.41 These practices not only pose environmental hazards but also contribute to the proliferation of antibiotic-resistant genes in soil and water systems, as highlighted in global reviews.42,43 In contrast, countries with structured pharmaceutical return programs, such as the UK, have demonstrated improved disposal behaviors following community pharmacy-led campaigns.44 The persistence of unsafe disposal in many African contexts underscores the urgent need for public education, regulatory enforcement, and accessible take-back systems to mitigate environmental contamination and the indirect spread of antibiotic resistance.
Our study reveals that 77% of participants consistently adhered to infection prevention and control (IPC) protocols. This is encouraging and aligns with global evidence linking high IPC compliance to reduced transmission of ABR pathogens and hospital-acquired infections (HAIs). This rate is notably higher than that reported in a study from The Gambia, where only 49.5% of healthcare workers complied with IPC standards despite adequate knowledge and positive attitudes.45 Similarly, a multicounty assessment across 17 African nations during the COVID-19 pandemic found that primary and secondary healthcare facilities had median IPC compliance scores of 56.8% and 62.3%, respectively, with higher scores observed only in tertiary or COVID-19-dedicated centers.46 In contrast, a regional IPC learning network in East Africa demonstrated that structured training and quality improvement initiatives could raise compliance from 65% to over 90% in participating hospitals.47 These comparisons suggest that while the 77% adherence observed in this study reflects commendable progress, further gains may be achievable through sustained training, leadership engagement, and institutional support. Encouragingly, 77% of participants consistently adhered to infection prevention and control (IPC) protocols, which is critical in curbing the spread of resistant pathogens in healthcare settings. High IPC compliance has been linked to lower rates of hospital-acquired infections and ABR transmission.48
The study addresses a critical gap in empirical data on antibiotic use and resistance among healthcare workers in Liberia, a context marked by systemic challenges in antimicrobial stewardship. By triangulating knowledge, attitudes, and self-reported practices, the study reveals both promising trends such as high adherence to infection prevention and control (IPC) protocols and widespread recognition of antimicrobial resistance (AMR) as a public health threat, but also persistent misconceptions, including the reuse of leftover antibiotics. These findings offer a nuanced foundation for designing targeted interventions.
In our study, the significantly higher knowledge among doctors compared to nurses (OR: 3.55) reinforces results from studies in Nigeria and India which attribute this to the physicians’ central role in prescribing and their more extensive pharmacology training.49–51 Similarly, the strong association of a Bachelor’s degree with correct knowledge (OR: 3.10) echoes research from Saudi Arabia, highlighting tertiary education as a critical foundation.52,53 However, our finding of significantly lower knowledge among female healthcare workers (OR: 0.42) contrasts with a study from Egypt which found no significant gender difference, and another from Nepal where females had better knowledge.54,55 This discrepancy suggests that gender roles and access to professional development may be highly context-specific, meriting local investigation. The peak knowledge in the 31–40 year age group supports the notion that early-career experience solidifies theoretical learning, a pattern also observed in a systematic review of early-career general practitioners’ antibiotic prescribing for acute infections.56 Collectively, these results confirm that knowledge is multifaceted and that one-size-fits-all educational interventions are inadequate; they must be tailored to specific professional, educational, and demographic subgroups.
While the study’s scope is limited by its relatively small sample drawn from a single healthcare facility, participants were purposively selected to represent a diverse range of professional roles relevant to antibiotic stewardship. This sampling approach carries a risk of selection bias, as the participants may not be fully representative of all healthcare professionals in Liberia. To address this, the study intentionally included respondents from diverse departments and professional cadres to enhance representativeness and balance perspectives. Recognizing the potential for social desirability bias in self-reported responses, the study placed strong emphasis on ensuring complete confidentiality to mitigate this risk and enhance the reliability of findings.
Conclusion
This study revealed that while healthcare professionals generally demonstrated good knowledge and positive attitudes toward antibiotic use, significant gaps remain in their practices, particularly concerning the use of leftover antibiotics, premature discontinuation of treatment, and improper disposal. These findings fill an essential evidence gap in evaluating the level of knowledge of ABR among healthcare professionals in Liberia, and highlight the need for continuous professional education and the incorporation of ABR stewardship modules in in-service training for all healthcare workers. Strengthening hospital policies on antibiotic use and disposal, alongside national surveillance and regulation efforts, will be crucial to preserving the effectiveness of antibiotics and protecting public health in Liberia. In the context of the research setting, the study supplies baseline data that may be used to build a program that can improve the knowledge of healthcare workers.
Abbreviations
WHO, World Health Organization; AMR, Antimicrobial Resistance; ABR, Antibiotic Resistance; HCWs, Healthcare Workers; IPC, Infection Prevention and Control; HAIs, Hospital-Acquired Infections; UL-IRB, University of Liberia Institutional Review Board; CVI, Content Validity Index; SPSS, Statistical Package for the Social Sciences; CI, Confidence Interval; OR, Odds Ratio; KAP, Knowledge, Attitudes, and Practices; LMHRA, Liberia Medicines & Health Products Regulatory Authority.
Data Sharing Statement
All the datasets used for analysis are available from the corresponding author on request.
Ethical Approval and Consent to Participate
Ethical approval for this study was obtained from the University of Liberia Institutional Review Board (UL-IRB/JCT-CH/66/’23) and administrative clearance was granted by the management of ELWA Hospital. Written informed consent was obtained from each participant and participation was voluntary. Data were anonymized to ensure confidentiality.
Acknowledgments
The authors express their sincere gratitude to all the participants who contributed to this study. The authors also appreciate the support provided by the National Public Health Institute of Liberia, the University of Liberia, and the ELWA Hospital Management, whose collaboration was instrumental to the successful execution of this study.
Author Contributions
All authors made substantial contributions to the work reported, whether in the conception, study design, execution, data acquisition, analysis and interpretation, or across all these areas. Each author participated in drafting, revising, or critically reviewing the manuscript; approved the final version for publication; agreed on the journal of submission; and accepts responsibility for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sakeena MHF, Bennett AA, Jamshed S, et al. Investigating knowledge regarding antibiotics and antimicrobial resistance among pharmacy students in Sri Lankan universities. BMC Infect Dis. 2018;18:209. doi:10.1186/s12879-018-3107-8
2. Chukwu EE, Oladele DA, Awoderu OB, et al. A national survey of public awareness of antimicrobial resistance in Nigeria. Antimicrob Resist Infect Control. 2020;9(1):72. doi:10.1186/s13756-020-00739-0
3. Marston BJ, Dokubo EK, van Steelandt A, et al. Ebola response impact on public health programs, West Africa, 2014–2017. Emerg Infect Dis. 2017;23(Suppl 1):S25. doi:10.3201/eid2313.170727
4. World Health Organization. 10 global health issues to track in 2021. Available from: https://www.who.int/news-room/spotlight/10-global-health-issues-to-track-in-2021.
5. O’Neill J. Tackling drug-resistant infections globally: final report and recommendations. Government of the United Kingdom; 2016. Available from: https://apo.org.au/node/63983.
6. European Commission. EU action on antimicrobial resistance. 2023. Available from: https://health.ec.europa.eu/antimicrobial-resistance/eu-action-antimicrobial-resistance_en.
7. Ahmed SK, Hussein S, Qurbani K, et al. Antimicrobial resistance: impacts, challenges, and future prospects. J Med Surg Public Health. 2024;2:100081. doi:10.1016/j.glmedi.2024.100081
8. Drug-resistant infections: a threat to our economic future. World Bank. Available from: https://www.worldbank.org/en/topic/health/publication/drug-resistant-infections-a-threat-to-our-economic-future.
9. Serra-Burriel M, Keys M, Campillo-Artero C, et al. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: systematic review and meta-analysis. PLoS One. 2020;15(1):e0227139. doi:10.1371/journal.pone.0227139
10. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
11. Auta A, Hadi MA, Oga E, et al. Global access to antibiotics without prescription in community pharmacies: a systematic review and meta-analysis. J Infect. 2019;78(1):8–18. doi:10.1016/j.jinf.2018.07.001
12. Ayukekbong JA, Ntemgwa M, Atabe AN. The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrob Resist Infect Control. 2017;6(1):47. doi:10.1186/s13756-017-0208-x
13. Gebre M, Uddin MF, Duke T, et al. Perception and experience of clinicians and caregivers in treating childhood severe pneumonia and hypoxemia using bubble continuous positive airway pressure in Ethiopian tertiary and general hospitals. PLoS One. 2022;17(10):e0275952. doi:10.1371/journal.pone.0275952
14. Khan MS, Hutchison C, Coker RJ, et al. Preventing emergence of drug resistant tuberculosis in Myanmar’s transitioning health system. Health Policy Plan. 2017;32(suppl_2):i43–i50. doi:10.1093/heapol/czx093
15. Harris JT. Assessing the Rational Use of Essential Medicines in Public Health Facilities Montserrado County, Liberia [Thesis]. Muhimbili University of Health and Allied Sciences; 2012.
16. Guarding against antimicrobial resistance in Liberia | WHO | regional Office for Africa. 2025. Available from: https://www.afro.who.int/news/guarding-against-antimicrobial-resistance-liberia.
17. Liberia Medicines & Health Products, Regulatory Authority (LMHRA). Available from: https://www.lmhra.gov.lr/new/pg_img/25_05_28_PV%20Regulations_LMHRA_JG.pdf.
18. Ministry of Health. lbr-mn-78-02-guideline-2017-eng-national-standard-therapeutic-guidelines-eml.
19. Beaubien J. Startling Statistic: only 8 Patients In Largest Ebola Hospital. TPR; 2014. Available from: https://www.tpr.org/2014-12-03/startling-statistic-only-8-patients-in-largest-ebola-hospital.
20. Anargh V, Singh H, Kulkarni A, Kotwal A, Mahen A. Hand hygiene practices among health care workers (HCWs) in a tertiary care facility in Pune. Med J Armed Forces India. 2013;69(1):54–56. doi:10.1016/j.mjafi.2012.08.011
21. Sample size calculator for needs assessments and KAP surveys. ActivityInfo. Available from: https://www.activityinfo.org/support/docs/sampling/snapshot.html.
22. Lawshe CH. A quantitative approach to content validity. Personnel Psychol. 1975;28(4):563–575. doi:10.1111/j.1744-6570.1975.tb01393.x
23. Mudenda S, Bumbangi FN, Yamba K, et al. Drivers of antimicrobial resistance in layer poultry farming: evidence from high prevalence of multidrug-resistant Escherichia coli and enterococci in Zambia. Vet World. 2023;16(9):1803–1814. doi:10.14202/vetworld.2023.1803-1814
24. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. doi:10.1186/1748-5908-7-37
25. Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infect Control Hosp Epidemiol. 2011;32(2):101–114. doi:10.1086/657912
26. Precha N, Sukmai S, Hengbaru M, et al. Knowledge, attitudes, and practices regarding antibiotic use and resistance among health science and non-health science university students in Thailand. PLoS One. 2024;19(1):e0296822. doi:10.1371/journal.pone.0296822
27. Abbo LM, Cosgrove SE, Pottinger PS, et al. Medical students’ perceptions and knowledge about antimicrobial stewardship: how are we educating our future prescribers? Clinl Infect Dis. 2013;57(5):631–638. doi:10.1093/cid/cit370
28. Li P, Hayat K, Shi L, et al. Knowledge, attitude, and practices of antibiotics and antibiotic resistance among Chinese pharmacy customers: a multicenter survey study. Antibiotics. 2020;9(4):184. doi:10.3390/antibiotics9040184
29. Estany-Gestal A, Salgado-Barreira A, Vazquez-Lago JM. Antibiotic use and antimicrobial resistance: a global public health crisis. Antibiotics. 2024;13(9):900. doi:10.3390/antibiotics13090900
30. Albadrani RK, Alyenbawi AH, Albalawi M, et al. Assessment of knowledge, attitudes, and practices of antibiotic resistance among university students in Saudi Arabia. BMC Res Notes. 2025;18(1):161. doi:10.1186/s13104-025-07241-z
31. Jones ASK, Chan AHY, Beyene K, et al. Beliefs about antibiotics, perceptions of antimicrobial resistance, and antibiotic use: initial findings from a multi-country survey. Int J Pharm Pract. 2024;32(1):21–28. doi:10.1093/ijpp/riad089
32. Chalkidou A, Lambert M, Cordoba G, Taxis K, Hansen MP, Bjerrum L. Misconceptions and knowledge gaps on antibiotic use and resistance in four healthcare settings and five European countries—a modified Delphi study. Antibiotics. 2023;12(9):1435. doi:10.3390/antibiotics12091435
33. Shah J, Trautner BW, Olmeda K, et al. A survey of patient practices regarding leftover antibiotics reveals a potential source of antibiotic overuse. Antimicrob Agents Chemother. 2024;68(8):e0046924. doi:10.1128/aac.00469-24
34. Russell Publishing Ltd., Many families share leftover antibacterial drugs. PharmacoEcon Outcomes News. 2018;816(1):19. doi:10.1007/s40274-018-5439-4
35. Borek A, Ledda A, Pouwels K, et al. Stop antibiotics when you feel better? Opportunities, challenges and research directions. JAC Antimicrob Resist. 2024;6(5):dlae147.
36. Antimicrobial resistance. Available from: https://www.who.int/health-topics/antimicrobial-resistance.
37. Nisabwe L, Brice H, Umuhire MC, et al. Knowledge and attitudes towards antibiotic use and resistance among undergraduate healthcare students at University of Rwanda. J Pharm Policy Pract. 2020;13:7. doi:10.1186/s40545-020-00207-5
38. Kiener M, Ichura C, Ndenga BA, et al. Antibiotic prescribing patterns at outpatient clinics in Western and Coastal Kenya. PLOS Glob Public Health. 2025;5(1):e0004109. doi:10.1371/journal.pgph.0004109
39. Abubakar U, Salman M. Antibiotic use among hospitalized patients in Africa: a systematic review of point prevalence studies. J Racial Ethn Health Disparities. 2024;11(3):1308–1329. doi:10.1007/s40615-023-01610-9
40. Karimi KJ, Ngumba E, Ahmad A, et al. Contamination of groundwater with sulfamethoxazole and antibiotic resistant Escherichia coli in informal settlements in Kisumu, Kenya. PLoS Water. 2023;2(4):e0000076. doi:10.1371/journal.pwat.0000076
41. Marwa KJ, Mcharo G, Mwita S, Katabalo D, Ruganuza D, Kapesa A. Disposal practices of expired and unused medications among households in Mwanza, Tanzania. PLoS One. 2021;16(2):e0246418. doi:10.1371/journal.pone.0246418
42. Apreja M, Sharma A, Balda S, Kataria K, Capalash N, Sharma P. Antibiotic residues in environment: antimicrobial resistance development, ecological risks, and bioremediation. Environ Sci Pollut Res. 2022;29(3):3355–3371. doi:10.1007/s11356-021-17374-w
43. Antibiotics as environmental waste | EBSCO Research Starters. Available from: https://www.ebsco.com/research-starters/environmental-sciences/antibiotics-environmental-waste.
44. Hamilton RA, Ercolani MG, Aggarwal R, et al. Evaluation of antibiotics returned for safe disposal during and after a community pharmacy antibiotic amnesty campaign. JAC Antimicrob Resist. 2024;6(5):dlae172. doi:10.1093/jacamr/dlae172
45. Darboe SMK, Darfour-Oduro SA, Kpene GE, et al. Factors influencing healthcare workers’ perceived compliance with infection prevention and control standards, North Bank East region, The Gambia, a cross-sectional study. BMC Res Notes. 2025;18(1):43. doi:10.1186/s13104-025-07101-w
46. Kabego L, Balde T, Barasa D, et al. Analysing the implementation of infection prevention and control measures in health care facilities during the COVID-19 pandemic in the African Region. BMC Infect Dis. 2023;23(1):824. doi:10.1186/s12879-023-08830-8
47. Kassa G, Ogongo I, Rabkin M, et al. The East Africa Infection Prevention and Control (IPC) learning network: an approach to improving IPC competencies and practices during the COVID-19 pandemic, 2020–2023. Clinl Infect Dis. 2025;81(1):41–48. doi:10.1093/cid/ciaf245
48. Zingg W, Mutters NT, Harbarth S, Friedrich AW. Education in infection control: a need for European certification. Clin Microbiol Infect. 2015;21(12):1052–1056. doi:10.1016/j.cmi.2015.09.001
49. Abubakar B, Sárváry A. Knowledge, attitude, and practice on antibiotics use among healthcare workers: a cross-sectional study in Niger state, Nigeria. J Infect Prev. 2023;24(5):206–215. doi:10.1177/17571774231165407
50. Manga MM, Mohammed Y, Suleiman S, et al. Antibiotic prescribing habits among primary healthcare workers in Northern Nigeria: a concern for patient safety in the era of global antimicrobial resistance. PAMJ One Health. 2021;5:19. doi:10.11604/pamj-oh.2021.5.19.30847
51. Trikha S, Dalpath SK, Sharma M, Shafiq N. Antibiotic prescribing patterns and knowledge of antibiotic resistance amongst the doctors working at public health facilities of a state in northern India: a cross sectional study. J Family Med Prim Care. 2020;9(8):3937–3943. doi:10.4103/jfmpc.jfmpc_367_20
52. Nukaly HY, Aljuhani RA, Alhartani MM, et al. Knowledge of antibiotic use and resistance among medical students in Saudi Arabia. Adv Med Educ Pract. 2024;15:501–512. doi:10.2147/AMEP.S462490
53. Alshehri AA, Khawagi WY. Knowledge, awareness, and perceptions towards antibiotic use, resistance, and antimicrobial stewardship among final-year medical and pharmacy students in Saudi Arabia. Antibiotics. 2025;14(2):116. doi:10.3390/antibiotics14020116
54. Maarouf L, Amin M, Evans BA, Abouelfetouh A. Knowledge, attitudes and behaviour of Egyptians towards antibiotic use in the community: can we do better? Antimicrob Resist Infect Control. 2023;12:50. doi:10.1186/s13756-023-01249-5
55. Yunita SL, Yang HW, Chen YC, et al. Knowledge and practices related to antibiotic use among women in Malang, Indonesia. Front Pharmacol. 2022;13:1019303. doi:10.3389/fphar.2022.1019303
56. Baillie EJ, Merlo G, Van Driel ML, Magin PJ, Hall L. Early-career general practitioners’ antibiotic prescribing for acute infections: a systematic review. J Antimicrob Chemother. 2024;79(3):512–525. doi:10.1093/jac/dkae002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health Literacy Among University Students in Shaanxi Province of China: A Cross-Sectional Study
Wu S, Shao B, Wang G
Risk Management and Healthcare Policy 2023, 16:865-878
Published Date: 11 May 2023
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Liu X, Song Y, Wan L, Du R
Journal of Multidisciplinary Healthcare 2024, 17:937-947
Published Date: 2 March 2024
Knowledge, Attitudes, and Practices Among Elderly CHD Patients Towards Self-Perceived Health Abilities
Ren L, Li Z, Wu J, Duan L, Gao J
Journal of Multidisciplinary Healthcare 2024, 17:1999-2011
Published Date: 1 May 2024
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024
Knowledge, Attitude and Practice Regarding Thyroid Disorders in Pregnant Women: A Cross-Sectional Study in Guangdong, China
Han L, Jin J, Xu J, Wang H, Qin A, Chen J
International Journal of Women's Health 2025, 17:2001-2013
Published Date: 10 July 2025