Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Assessing the Cost and Resource Use Impact of Implantable Cardiac Defibrillator Shocks in the UK CareLink Population
Authors Llewellyn J, Barker E, Bowe C, Hallas N, Oghagbon R, Rao A
Received 9 February 2023
Accepted for publication 12 May 2023
Published 6 June 2023 Volume 2023:15 Pages 425—432
DOI https://doi.org/10.2147/CEOR.S403712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Jennifer Llewellyn,1 Erin Barker,2 Catherine Bowe,2 Natalie Hallas,3,* Ralphael Oghagbon,3,* Archana Rao1
1Liverpool Heart and Chest Hospital, Liverpool, UK; 2York Health Economics Consortium, University of York, Heslington, York, UK; 3Medtronic, Watford, Herts, UK
*These authors contributed equally to this work
Correspondence: Jennifer Llewellyn, Liverpool Heart and Chest Hospital, Thomas Drive, Liverpool, L14 3PE, UK, Tel +44 0151 600 1616, Fax +44 0151 600 1862, Email [email protected]
Objective: High voltage devices (implantable cardiac defibrillators (ICDs) and cardiac resynchronization therapy defibrillators referred to jointly as ICDs) reduce rates of sudden cardiac death in patients with cardiovascular disease. However, shocks from ICDs may be associated with healthcare resource use (HCRU) and costs. The aim of this study was to estimate the costs associated with both appropriate and inappropriate shocks from ICDs.
Methods: Patients with appropriate and inappropriate shocks from ICDs were identified via CareLink data from Liverpool Heart and Chest Hospital between March 2017 and March 2019. The devices were SmartShock activated, with anti-tachycardia pacing. Costs were estimated according to the dominant episode of healthcare, from an NHS payer perspective.
Results: There were 2445 patients on the CareLink system with ICDs. Over the two-year period, HCRU data from 143 shock episodes among 112 patients were reported. The total cost for all shocks was £ 252,552 with mean costs of £ 1608 and £ 2795 for appropriate and inappropriate shocks respectively. There was substantial variation in HCRU between shock episodes.
Conclusion: While there was a low rate of inappropriate shocks from ICDs, there were still substantial HCRU and costs incurred. In this study, the specific HCRU was not costed independently, meaning the costs reported are likely to be a conservative estimate. Whilst every attempt to reduce shocks should be made, appropriate shocks cannot be avoided. Strategies to reduce the incidence of inappropriate and unnecessary shocks should be implemented to reduce overall health care costs associated with ICDs.
Keywords: cardiology, implantable devices, hospital costs
Introduction
Sudden cardiac death (SCD) is a leading cause of mortality and approximately half of all coronary heart disease deaths are due to SCD.1 Left ventricular systolic dysfunction carries a high risk for SCD but high voltage devices (implantable cardiac defibrillators (ICDs) and cardiac resynchronization therapy defibrillators referred to jointly as ICDs) can potentially mitigate this risk by delivering rapid life-saving therapy.2
ICDs can detect and treat fast heart rhythms (tachyarrhythmias) with either anti-tachycardia pacing (ATP) or shocks to reset the rhythm.2,3 The National Institute for Health and Care Excellence (NICE) recommends the use of ICDs in patients at increased risk of SCD as a clinically and cost-effective treatment.4 Despite these recommendations, the National Institute for Cardiovascular Outcomes Research report confirms that ICDs are currently under used across the United Kingdom (UK).5
Although ICD shocks can be lifesaving, shocks are sometimes delivered inappropriately for a rhythm other than ventricular tachycardia/ventricular fibrillation, such as for supraventricular arrhythmias, noise or artefact.6 ICDs may also deliver unnecessary shocks, which are shocks that could have been terminated by ATP, had it been delivered, or, a slightly longer delay would have spontaneously terminated the arrhythmia.7 Historically, 16 to 17% of patients received an inappropriate shock from their ICD within the five years following implantation, and 43% of these shocks were associated with a hospital attendance.8,9 As well as the costs associated with these episodes, shocks have a detrimental impact on daily activity, self-perceived quality of life and anxiety, both for the ICD recipient and their relatives.10
Strategies to reduce shocks have been shown to be effective in recent studies. In the PainFree SmartShock technology (SST) trial, ICDs were activated with a novel suite of detection algorithms (known as SmartShock) in conjunction with routine implementation of a proven programming strategy at the time of device implantation. Based on a 2017 systematic review and meta-analysis, strategies such as this have reduced annual inappropriate shock rates from around 10% to just 1.9%.11 Real-world evidence has also recently confirmed the effectiveness of ATP treatment to limit overall ICD shock burden.12 However, despite the declining rates of shocks, the costs and healthcare resource use (HCRU) associated with shocks have not been assessed in the UK.
Aim
The aim of this study was to describe the HCRU and associated costs resulting from appropriate and inappropriate shocks from SmartShock-activated, ICDs. This assessment was based on a retrospective review of data from an NHS tertiary single center (Liverpool Heart and Chest Hospital).
Methods
A retrospective, observational review of all patients with Medtronic SmartShock-activated, ICDs, receiving shock therapy between March 2017 and March 2019, was undertaken independently by staff at Liverpool Heart and Chest Hospital. In addition to SmartShock, the devices were ATP activated.
All Medtronic ICDs are remotely monitored via CareLink. Data were collected from a patient’s device and stored on the CareLink Clinician website, as previously described by Rao et al.13
A shock episode was defined as one or more spontaneous shocks delivered by the device within the same arrhythmia episode. An appropriate shock was one delivered for ventricular tachycardia or ventricular fibrillation; an inappropriate shock was one delivered for anything other than the above, such as atrial arrhythmia. Shock episode data were retrieved via Discovery Link, the web-based platform that enables the analysis of device data. Each shock episode was interrogated independently to validate the patient cohort. All patients identified as receiving shock therapy, both appropriate and inappropriate, from their device during the pre-determined period, were included in the data collection. Patient demographics, device indication, aetiology, medication, device details and programming were obtained from the electronic patient records. Medical and device information was recorded on the day of the shock episode and, therefore, reflect the settings and medications that were received on the day of the shock episode.
The minimum follow-up period was 13 months (range 13 to 39 months). Descriptive HCRU data were reported for all shock episodes. Summary statistics were performed in R v4.1.1 or later.14
Costing
All shock episodes were examined by clinicians and resulting HCRU was collected for all patients. The Coding and Finance department at Liverpool Heart and Chest Hospital allocated costs pertaining to HCRU data for each patient.
Each shock episode identified was followed through to ascertain health care utilization that included various interventions, phone calls, clinic appointments and hospitalizations. Further details of medical and procedural intervention, as well as duration of hospital stay for each shock episode, were collected in a retrospective manner.
Shock episode costs were estimated using healthcare resource group (HRG) tariffs. HRG tariffs are reflective of average costs and do not account for differences in patient activity. For example, a single HRG tariff was applied to all patients that attended a clinical appointment regardless of the specific HCRU related to that appointment. For hospital admissions, HRG tariffs were applied based on the dominant episode of health care and any complexities. Procedures were assessed without reference to the costs, meaning activities such as lead revisions, medication changes, blood tests and programming changes were reported for each episode but were not individually captured in the costs. Hence, the costs used in this analysis were a reflection of the price that was received by the hospital rather than the actual cost of care.15 Shock episodes that occurred during an ongoing hospital admission did not incur additional tariffs. Unplanned admissions via Accidents and Emergency (A&E) incurred a tariff for non-elective admission. HRG codes and tariffs are available in Table S1.
Results
There were 2445 patients in total on the CareLink system with ICDs. In this CareLink population, 163 shock episodes (143 appropriate and 20 inappropriate) in 116 patients were observed from March 2017 to March 2019 (~5% of all patients). Of these, four patients (six episodes, five appropriate and one inappropriate) were excluded because there was no local HCRU information available due to patient relocation. A further 14 episodes (all appropriate) occurred while patients were already in hospital for a previous episode and, therefore, did not generate unique HCRU. In these cases, all HCRU was associated with the original shock episode. Hence, a total of 143 shock episodes requiring unique HCRU in 112 patients were used in the analysis.
The patient demographics are shown in Table 1.
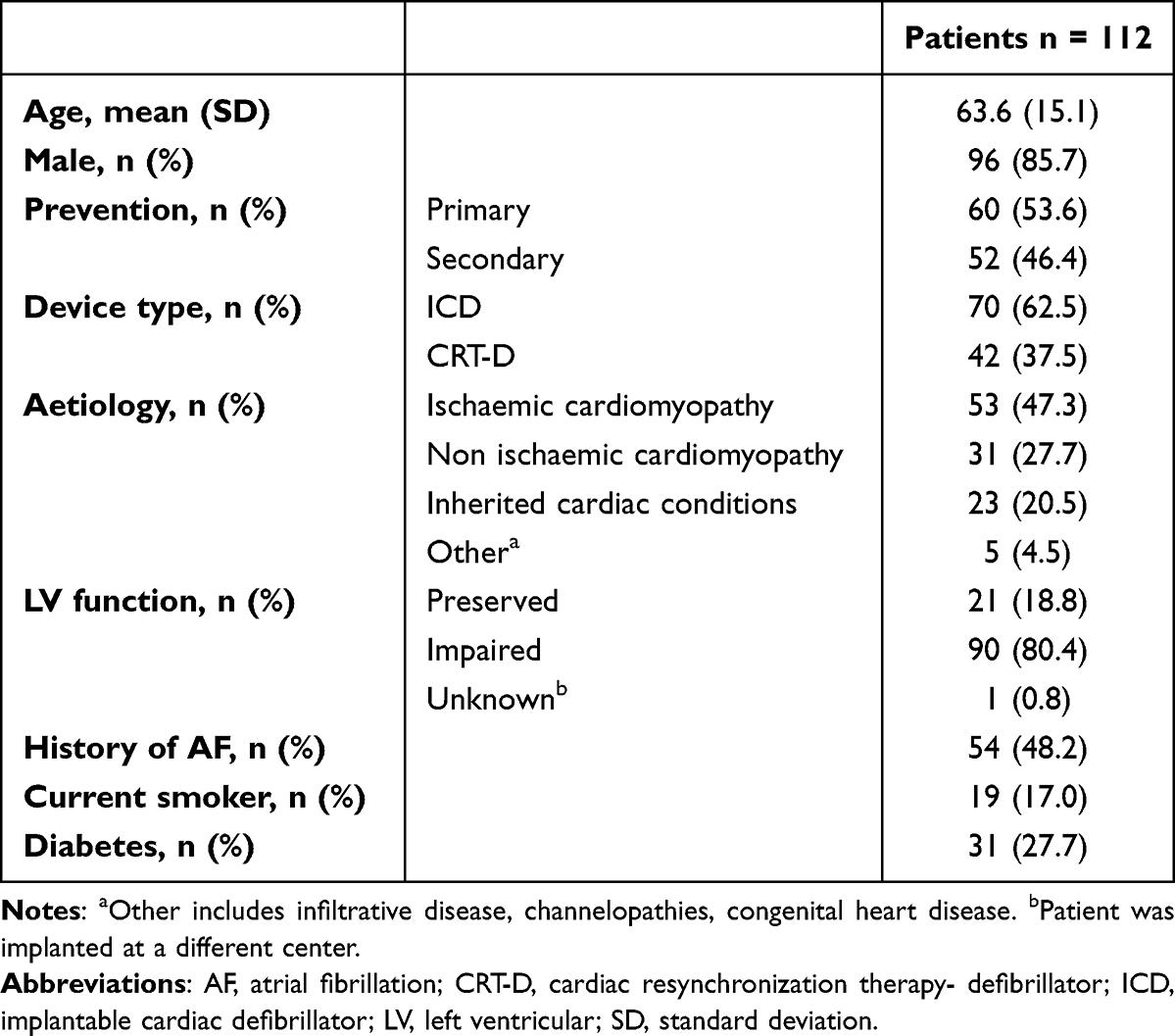 |
Table 1 Patient Demographics |
Medication data retrieved at the time of the shock episode indicated that the cohort was appropriately medicated. In 92.3% of episodes, patients were receiving beta blockers; in 79.7% of episodes, patients were receiving renin-angiotensin-aldosterone system inhibitors, and in 62.9% of episodes, the patients were receiving statins. The full list of medications at the time of each shock episode is available in Table S2.
The number of shock episodes and reasons for shocks are presented in Table 2. Of the reported episodes, 124 episodes were considered “appropriate” and 19 episodes were considered “inappropriate”. In 74.8% of episodes, the patient received only one shock, with a range of 1 to 48 shocks per episode observed. Regarding device programming, in 96.5% of episodes, the number of intervals to detect (NID) arrhythmia was ≥30/40. Two patients were programmed with 18/24 NID, and in one patient the NID was unknown. The NID for each patient did not vary across the study.
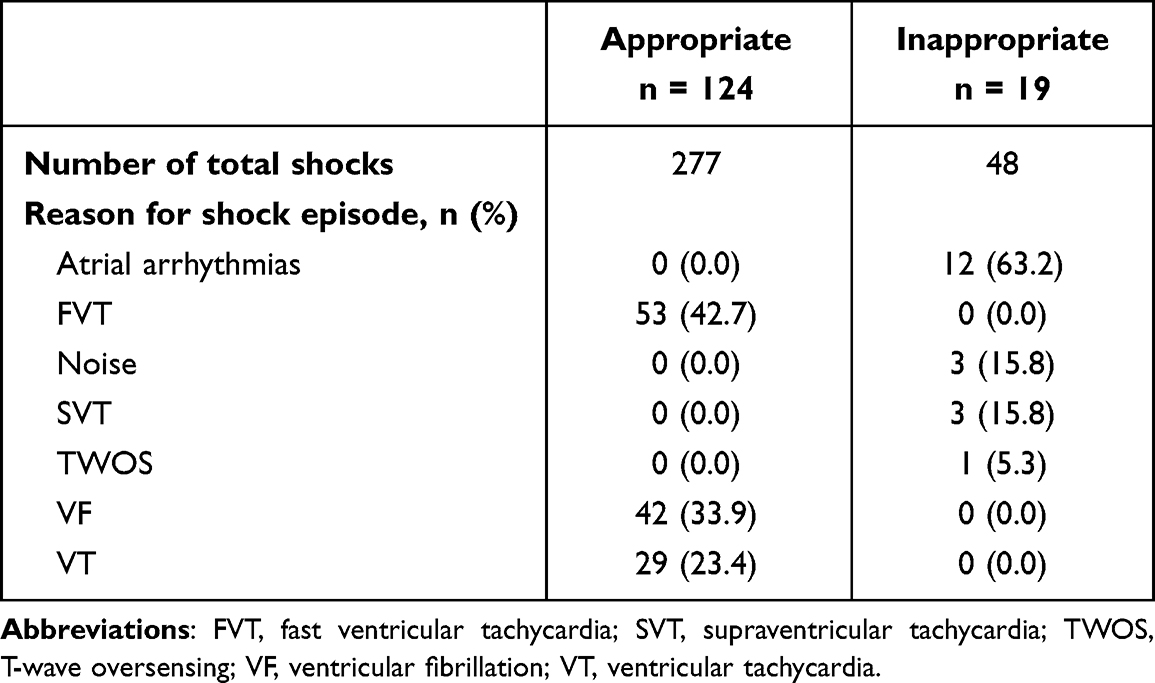 |
Table 2 Shock Episode Details |
While not costed independently, the procedures and interventions associated with both appropriate and inappropriate shocks were captured from the patient records. These are summarized in Figure 1.
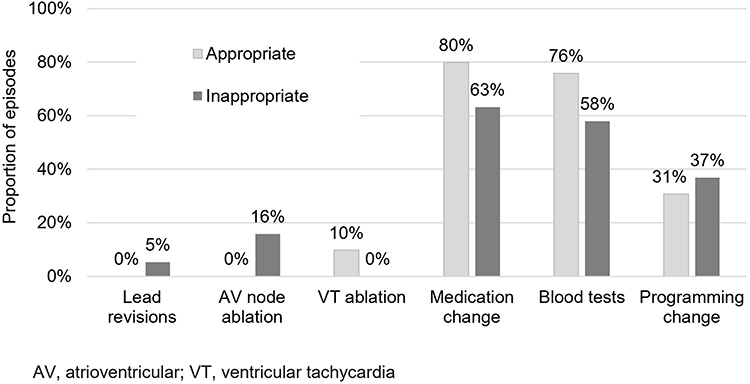 |
Figure 1 Procedures and interventions for appropriate and inappropriate shock episodes. |
Table 3 shows the HCRU for appropriate and inappropriate shock episodes and the associated cost. There were seven appropriate and two inappropriate shock episodes that did not result in additional HCRU and, therefore were not assigned a tariff. Overall, the cost for an inappropriate shock episode was higher than that for an appropriate shock. There was a trend towards higher inpatient admissions and longer length of stay in the appropriate shock group, that may not have been fully covered by the tariff. Hence, the tariff cost may have underestimated the actual healthcare costs.
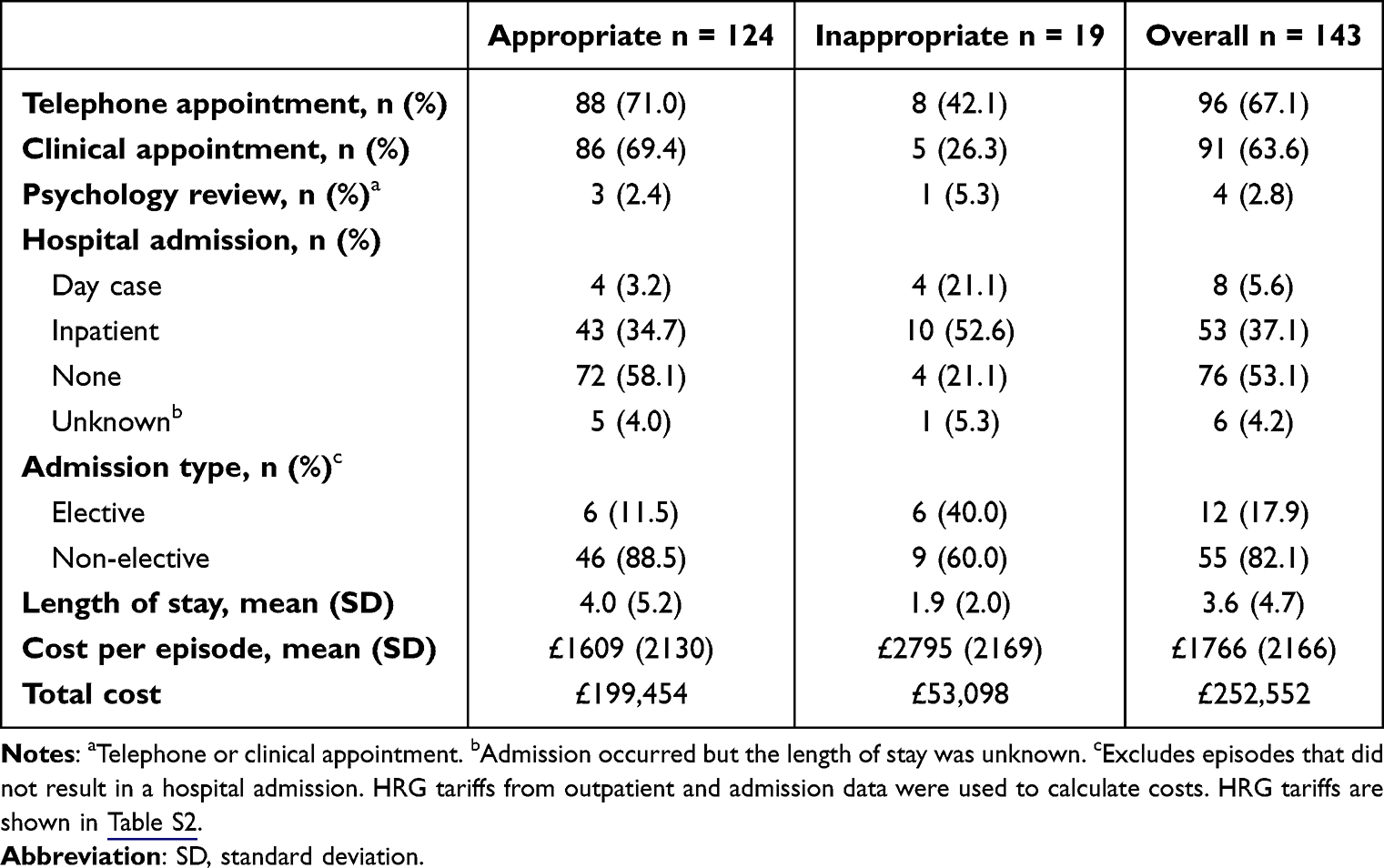 |
Table 3 Shock Episode Resource Use and Associated Costs |
Discussion
In this CareLink population, 116 out of 2445 patients (5%) experienced a shock from their device and 20 of these patients experienced an inappropriate shock, representing 0.8% of all patients. Overall, the proportion of inappropriate shocks was lower than that reported in the Pain Free SST trial, where the rate of inappropriate therapy was 2.8% for dual/triple chamber ICDs and 3.7% for single-chamber ICDs at two years post implant.11 This low inappropriate shock rate is likely due to the activation of SmartShock technology, long-detection interval programming (NID ≥30/40 in 96.5% of patients) and evidence-based optimal medical management. New medications and improvements in intervention methods may also influence the decline in the number of inappropriate shocks observed. Furthermore, the Liverpool Heart and Chest Hospital has longstanding expertise in ICD management, and aims to ensure that patients are appropriately selected for ICD and CRT-D implantation. The devices are programmed as per the European Heart Rhythm Association (EHRA) recommendations and patients are optimized on adjunct medication.16 The Medtronic ICD nominal settings are also the closest to the EHRA ICD Programming Guidelines, which facilitates implementation of best practice.
Programming optimization to reduce shocks includes the use of ATP. ATP has been shown to help treat patients painlessly without delaying the necessary shock therapy. Data from the ADVANCE III trial showed that using ATP during charging in combination with long-detection interval programming was effective in reducing appropriate but unnecessary shocks by 52% compared with using long-detection interval alone.17
Impact of Shocks on Costs
Shock episodes generally incurred substantial HCRU and associated cost, which corresponded to a total cost of £252,552 at the Liverpool Heart and Chest Hospital over the two-year period. While comparative cost data from other centers are not available, it is reasonable to assume that costs will be higher at centers where optimal management is not implemented and devices are not SmartShock activated. In these scenarios, implementing a strategy to reduce shocks has the potential to reduce HCRU and the associated costs by a substantial amount. Given the ability to re-program ICDs in an outpatient setting, this could be done through improved algorithms and adapting programming settings, such as those developed in the PainFree SST.
More broadly, the societal cost impact of shocks can be significant to patients, particularly with regard to work and family commitments. For example, driving bans ranging from one to up to six months or more, are mandated by the DVLA following an inappropriate or appropriate shock, respectively, which can result in work productivity losses.
Further, the impact of shocks on patient health-related quality of life (HRQoL) is a significant concern that should be minimized to improve patient and physician confidence in ICDs and address the low rates of implantation in the UK. A US study found that ICD shocks reduced overall HRQoL by 4% (p = 0.04);18 and other studies have shown that there was no statistically significant difference in health status between appropriate and inappropriate shocks, highlighting that receiving any type of shock has a negative impact on patient HRQoL.19
Costing studies for patients with ICDs have traditionally focused on the initial costs of the implant and follow on care.4 This current study has shown that both appropriate and inappropriate shocks are associated with a cascade of HCRU. At least 89% of all shock episodes were associated with additional HCRU and 37% required an inpatient stay. This level of HCRU is higher than that reported previously by Turakhia et al, who found that in the US, 46% of shock episodes (both appropriate and inappropriate) were associated with HCRU and 14% required an inpatient stay.9 In another US study, the annual treatment cost for post-implant patients who received an inappropriate shock was $7000 more than for patients who did not receive a shock.20 Hence, the costs of shock-related HCRU from ICDs should be accounted for when considering the overall costs of device implantation.
The patients in the CareLink system were a heterogenous cohort and presented in diverse settings. Hence, shocks were managed in a number of different ways, resulting in varied utilization of healthcare resources. This is turn, impacted significantly on the tariffs generated. For instance, sometimes a shock was only detected via the CareLink platform, thus, the only HCRU accrued was a phone call from the notified clinician. In other cases, patients with symptomatic shocks presented at an A&E department, resulting in an unplanned admission lasting several days with inpatient intervention, therefore accruing different HCRU accordingly. In addition, patient response to shocks is known to vary, with post-traumatic stress disorder reported in 20% of ICD recipients and anxiety reported in 24 to 87% of patients.21 This variable response creates a demand for tailored interventions.22 As such, strategies where patients can be managed efficiently via remote platforms and virtual consultations could be explored further.
Limitations
A limitation of this study is that the NHS England national tariffs payment system has been replaced with a blended payment system. While the current analysis was based on tariffs, this still provides a benchmark for the cost of an ICD shock in the UK. We recommend that future cost analysis could be done from a provider perspective to capture a true reflection of hospital costs; for example, the recent costing analyses conducted by Ahmed et al on true cardiac device infection costs to providers.23
The costs reported are a conservative estimate of the true cost of shocks as many patients had additional shocks while in hospital, but only the HCRU from their first shock episode was costed for. As such, future costing analyses should attempt to capture full procedure and intervention costs. Further, the cost analysis is subject to individual management regimes employed within the NHS. It is possible that alternative regimes would incur higher costs (ie if there was a mandated admission for appropriate shocks).
Within a single-center setting, variations were observed in patient presentation and management. This is a real-world study and care pathways will be subject to numerous differences depending on patient cohort and clinical presentation. Hence, there may not be a “typical” care pathway followed by patients who receive a shock from their ICD, and thus, costs will inherently vary given the heterogenous cohort of patients and their presentations.
Another limitation lies in the data collection methods. Data were retrospectively collected from patient records, rather than at the time of the shock.
Finally, the number of people who experienced an inappropriate shock was small, likely attributable to the activation of SmartShock technology and the high standards of cardiac care employed at Liverpool Heart and Chest Hospital. As such, the robustness of these results cannot be ascertained, nor can we be certain on the applicability of these results to other regions. Ideally, larger cohorts over multiple centers would be required to gain a more accurate cost for inappropriate ICD shocks in the UK. The aim of this current study was to describe the HCRU and associated costs resulting from appropriate and inappropriate shocks and not intended as a comparative analysis.
Conclusion
Although the total number of shocks was low, this study found that HCRU resulting from both appropriate and inappropriate shocks was substantial, with high associated costs to the NHS.
The low rate of shocks observed can be attributed to the use of SmartShock enabled devices, as well as optimal device programming strategies to reduce shocks, which overall, can minimize unnecessary healthcare spending and distress to the patient. Further investigation on the impact of optimal ICD programming strategies on HCRU and costs is warranted to explore the potential cost savings such interventions could bring on a national level.
Ethical Approval
This service evaluation project was approved by the local ethics committee at Liverpool Heart and Chest Hospital. All patients signed the CareLink consent form and data agreements at the time of enrolment in accordance with local policy.
Acknowledgments
We would like to thank Mike Harding, Matthew Shaw, Susan Hughes and Professor Jay Wright at Liverpool Heart and Chest Hospital for their database support. We would also like to thank Angela Stainthorpe for providing additional review of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Erin Barker and Catherine Bowe are employees of YHEC, who received funding from Medtronic to write this manuscript. Natalie Hallas and Ralphael Oghagbon are employees of Medtronic. Archana Rao reports grants, personal fees from Medtronic, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Myerburg RJ. Sudden cardiac death: exploring the limits of our knowledge. J Cardiovasc Electrophysiol. 2001;12(3):369–381. doi:10.1046/j.1540-8167.2001.00369.x
2. NHS. Implantation of a cardiac resynchronisation therapy defibrillator (CRT-D); 2019. Available from: https://www.ouh.nhs.uk/patienImt-guide/leaflets/files/12323Pcrt-d.pdf.
3. Sears SF, Shea JB, Conti JB. How to respond to an implantable cardioverter-defibrillator shock. Circulation. 2005;111(23):e380–e382. doi:10.1161/CIRCULATIONAHA.104.508663
4. NICE [TA314]. Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure. Available from: https://www.nice.org.uk/guidance/ta314/chapter/1-Guidance.
5. Murgatroyd F, Linker N, Cunningham D, Cunningham M, Bradley A, Lange A. National audit of cardiac rhythm management devices. Nicor. 2016;2016:1.
6. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter–defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–237. doi:10.1056/NEJMoa043399
7. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol. 2018;72(14):e91–e220. doi:10.1016/j.jacc.2017.10.054
8. Saxon LA, Hayes DL, Gilliam FR, et al. Long-term outcome after ICD and CRT implantation and influence of remote device follow-up: the ALTITUDE survival study. Circulation. 2010;122(23):2359–2367. doi:10.1161/circulationaha.110.960633
9. Turakhia MP, Zweibel S, Swain AL, Mollenkopf SA, Reynolds MR. Healthcare utilization and expenditures associated with appropriate and inappropriate implantable defibrillator shocks. Circ Cardiovasc Qual Outcomes. 2017;10(2):e002210. doi:10.1161/CIRCOUTCOMES.115.002210
10. Schron EB, Exner DV, Yao Q, et al. Quality of life in the antiarrhythmics versus implantable defibrillators trial: impact of therapy and influence of adverse symptoms and defibrillator shocks. Circulation. 2002;105(5):589–594. doi:10.1161/hc0502.103330
11. Auricchio A, Schloss EJ, Kurita T, et al. Low inappropriate shock rates in patients with single- and dual/triple-chamber implantable cardioverter-defibrillators using a novel suite of detection algorithms: painFree SST trial primary results. Heart Rhythm. 2015;12(5):926–936. doi:10.1016/j.hrthm.2015.01.017
12. Regoli F, Graf D, Schaer B, et al. Arrhythmic episodes in patients implanted with a cardioverter-defibrillator - results from the prospective study on predictive quality with preferencing painFree ATP therapies (4P). BMC Cardiovasc Disord. 2019;19(1):146. doi:10.1186/s12872-019-1121-4
13. Rao A, Barker D, Kam Chuen MJ N, Hughes S, Cullen D. Shock rates in an unselected real world cohort of patients with Medtronic Protecta implantable cardioverter defibrillators. Cardiovasc Disord Med. 2017;2. doi:10.15761/CDM.1000140
14. R Foundation. The R project for statistical computing; 2021.
15. NHS. National Tariff Payment System. NHS; 2021.
16. NHS. Liverpool heart and chest hospital; 2022. Available from: https://www.lhch.nhs.uk/research/.
17. Arenal A, Proclemer A, Kloppe A, et al. Different impact of long-detection interval and anti-tachycardia pacing in reducing unnecessary shocks: data from the ADVANCE III trial. Europace. 2016;18(11):1719–1725. doi:10.1093/europace/euw032
18. Noyes K, Corona E, Veazie P, Dick AW, Zhao H, Moss AJ. Examination of the effect of implantable cardioverter-defibrillators on health-related quality of life: based on results from the multicenter automatic defibrillator trial-II. Am J Cardiovasc Drugs. 2009;9(6):393–400. doi:10.2165/11317980-000000000-00000
19. Suwanpasak A, Boonyapisit W. The quality of life in implantable cardioverter defibrillator patients. J Med Assoc Thai. 2014;97(3):S108–14.
20. Bhavnani SP, Giedrimiene D, Coleman CI, Guertin D, Azeem M, Kluger J. The healthcare utilization and cost of treating patients experiencing inappropriate implantable cardioverter defibrillator shocks: a propensity score study. Pacing Clin Electrophysiol. 2014;37(10):1315–1323. doi:10.1111/pace.12465
21. Shiga MDT, Suzuki MDT, Nishimura MDK. Psychological distress in patients with an implantable cardioverter defibrillator. J Arrhythm. 2013;29(6):310–313. doi:10.1016/j.joa.2013.05.006
22. Hirsh AT, Sears SF
23. Ahmed FZ, Fullwood C, Zaman M, et al. Cardiac implantable electronic device (CIED) infections are expensive and associated with prolonged hospitalisation: UK retrospective observational study. PLoS One. 2019;14(1):e0206611. doi:10.1371/journal.pone.0206611
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.