Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Assessing Prevalence of Hypoglycemia in a Medical Transcription Database
Authors Uzoigwe C ![]() , Hamersky CM
, Hamersky CM ![]() , Arbit DI
, Arbit DI ![]() , Weng W, Radin MS
, Weng W, Radin MS
Received 19 October 2019
Accepted for publication 29 May 2020
Published 24 June 2020 Volume 2020:13 Pages 2209—2216
DOI https://doi.org/10.2147/DMSO.S235298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Chioma Uzoigwe, Carol Mahler Hamersky, Deborah I Arbit, Wayne Weng, Michael S Radin
Novo Nordisk Inc., Plainsboro, NJ, USA
Correspondence: Chioma Uzoigwe
Novo Nordisk Inc., 800 Scudders Mill Road, Plainsboro, NJ 08536, USA
Tel +1 609 786 4317
Email [email protected]
Purpose: The prevalence of hypoglycemia in patients with diabetes mellitus is likely underreported, particularly with regard to non-severe episodes, and representative estimates require more detailed data than claims or typical electronic health record (EHR) databases provide. This study examines the prevalence of hypoglycemia as identified in a medical transcription database.
Patients and Methods: The Amplity Insights database contains medical content dictated by providers detailing patient encounters with health care professionals (HCPs) from across the United States. Natural language processing (NLP) was used to identify episodes of hypoglycemia using both symptom-based and non-symptom-based definitions of hypoglycemic events. This study examined records of 41,688 patients with type 1 diabetes mellitus and 317,399 patients with type 2 diabetes mellitus between January 1, 2016, and April 30, 2018.
Results: Using a non-symptom-based definition, the prevalence of hypoglycemia was 18% among patients with T1DM and 8% among patients with T2DM. These estimates show the prevalence of hypoglycemia to be 2- to 9-fold higher than the 1% to 4% prevalence estimates suggested by claims database analyses.
Conclusion: In this exploration of a medical transcription database, the prevalence of hypoglycemia was considerably higher than what has been reported via retrospective analyses from claims and EHR databases. This analysis suggests that data sources other than claims and EHR may provide a more in-depth look into discrepancies between the mention of hypoglycemia events during a health care visit and documentation of hypoglycemia in patient records.
Keywords: natural language processing, type 1 diabetes mellitus, type 2 diabetes mellitus
Introduction
The prevalence of hypoglycemia as reported by administrative claims databases is very low, with estimates of 4% for patients with type 1 diabetes mellitus (T1DM) and 1% to 3% for patients with type 2 diabetes mellitus (T2DM).1,2 These estimates only highlight the prevalence of severe hypoglycemia, as patients typically do not seek medical treatment for hypoglycemia unless the event is severe.3 During a single medical encounter, the number of health care concerns raised and/or addressed may often exceed the maximum of four ICD-9/ICD-10 (International Classification of Diseases, 9th revision/10th revision) codes reported on the reimbursement claim. Therefore, while they may be captured in physician notes, all concerns may not be recorded in the claims database. Furthermore, the structured format of electronic health records (EHR) platforms may complicate the ability of health care professionals (HCPs) to document conditions such as hypoglycemia due to restrictive pull-down menus and limited options for entering free-text, and to retrieve and process information regarding these conditions for subsequent research. The aforementioned challenges in patient reporting and HCPs recording of events make it likely that non-severe hypoglycemia is substantially underreported and underdocumented.
The attempt to determine more representative estimates of the prevalence of hypoglycemia requires more detailed data than that provided by claims or EHR databases. For example, detailed provider treatment notes may capture a greater number of health care concerns raised during the patient encounter. Previous studies examining EHR or patient diaries have reported higher prevalence of hypoglycemia among patients with T2DM than prevalence estimates identified from administrative claims.4,5 Additionally, studies have found higher estimates for the prevalence of hypoglycemia based on combined use of clinical notes and structured data from EHR compared with structured data from EHR alone.4
As with clinical notes, medical transcripts often capture underlying complaints discussed by the patient, such as hypoglycemic events, even if they were not the primary reason for the visit and were not recorded in an EHR or by a billing code for reimbursement. In this retrospective cohort study, we sourced Amplity Insights (formerly RealHealthData), a US medical transcription database. The Amplity Insights database contains medical content dictated by providers and transcribed from verbal to written form detailing patient encounters with HCPs. Dictation as a means of documenting patient care has existed long before the advent of EHR systems. There is an entire medical transcription industry built around the choice by providers to dictate the details of the care they are providing for their patients. Historically, this involved medical transcriptionists typing the contents of the dictation but also now includes the use of voice recognition and human editing of the output. These physician treatment notes capture health care concerns raised during the patient encounter that the physician thought were relevant to the patient’s condition and care.
To analyze these records, natural language processing (NLP) was employed. NLP is a type of artificial intelligence enabling computational recognition and processing of human language. In this study, NLP was used to search unstructured text data from medical record transcriptions to identify encounters that specifically mentioned keywords of interest revolving around hypoglycemia. Previous studies have demonstrated the effectiveness of NLP in identifying hypoglycemic events in medical records,4,6 although to our knowledge, no studies to date have used NLP to investigate the prevalence of hypoglycemia in a medical transcription database.
The goal of this study was to determine the prevalence of hypoglycemia among patients with T1DM and T2DM. The study investigators hypothesized that in a qualitative and rich unstructured database where providers are not restricted to entering information directly tied to a billing claim nor forced to use designated drop-down boxes for diagnoses or codes, that instances of hypoglycemia events (based upon spoken word and/or symptom intersection) captured would be higher than what is reported in more structured databases. That is, within this unique dataset where providers are free of the restrictive nature of structured data entry, more details around information shared by the patient may be included, which would highlight at some basic level, a gap in the reporting of hypoglycemic events via EHR and claims. Therefore, using Amplity Insights’ database, we examined the prevalence of hypoglycemia by searching for mentions of hypoglycemia and related terms in the transcriptions. We then compared these estimates with the prevalence reported in claims and EHR databases.
Patients and Methods
Amplity Insights
The Amplity Insights database provides unstructured health records generated from provider notes as transcribed from verbal to written form. Health care encounters included initial office consultations, follow-up visits, urgent care visits, emergency department and hospital admissions and discharges, postoperative consultations, office notes, and referral letters. The most frequent provider types represented in the database were “multispecialty” (defined as a combination of emergency department or urgent care and specialists in hospital networks) and general practitioner, internal medicine, or family medicine. Endocrinologists represented a small number of the providers. After the patient visit, the provider dictated the details of the encounter, including the patient’s medical history, family history, exam, prescription information, and plan for treatment. A transcription company then processed the dictated notes and sent the transcription to the provider’s office for final approval. Amplity Insights collects these transcripts in their database, deidentifies patient data, then analyzes these texts using NLP to identify patient encounters that mentioned keywords or concepts of interest (see Appendix 1). Data were then aggregated to the patient level to provide quantitative data about the study cohort.
The Amplity Insights database contains records on more than 15 million patient-lives from all 50 states representing more than 150,000 unique providers. Males are slightly underrepresented each year compared with national estimates (~45% Amplity Insights vs ~49% national estimates). The proportion of African-Americans in the Amplity Insights database is similar to the proportion reported by nationally representative data sources (~13% Amplity Insights vs ~16% national estimates). However, Caucasians are overrepresented compared with national estimates (~80% Amplity Insights vs 62% national estimates); Hispanics and those in the “Other” race/ethnicity category are underrepresented. Age is skewed older in the Amplity Insights database vs federal data sources (~70% ≥45 years of age in Amplity Insights vs ~60% ≥45 years of age in the various nationally representative data sets). When compared with federal sources of demographics such as the National Health Interview Survey, the proportion of patients from the South in the US in the Amplity Insights database is close to nationally representative estimates (~34% vs ~36%); however, the Northeast and Midwest are slightly overrepresented (~22% vs ~18% and ~30% vs ~22%, respectively), and the West is underrepresented (~14% vs ~23%).7
Study Design
The study analyzed transcripts generated over a 2-year period (January 1, 2016, to April 30, 2018) to reflect the most recent clinical practice patterns available at the time of this analysis. No minimum follow-up time or length of data was required. The study cohort included patients aged 18 years or older with one or more records during the study period and mention of diabetes. Mention of diabetes served as a proxy for ICD-9 or ICD-10 codes for diabetes, as the use of these codes in the database was quite low (<1%). Patients were excluded if there was a mention of both T1DM and T2DM for the same patient or if there was evidence of being younger than 18 years of age. Patients were then stratified into T1DM or T2DM cohorts based on the type of diabetes mentioned in their record, and subsequent analyses were performed separately on these cohorts. As this was an observational study using de-identified data and patients were not contacted, approval from an institutional review board was not required.
Identifying Hypoglycemic Events
Non-Symptom-Based Definition
NLP was used to identify symptom-based and non-symptom-based definitions of hypoglycemic events. Parameters for the non-symptom-based definition of hypoglycemia included the mention of “hypoglycemia,” relevant medical ontology such as “low glucose,” or a blood glucose laboratory value ≤70 mg/dL documented in patient encounter data.
Symptom-Based Definition
Symptom-based selection for hypoglycemia was informed in part from the results of an online survey of 283 endocrinologists practicing in the United States who identified the words they recall patients using most frequently to describe severe hypoglycemia (hypoglycemia with severe cognitive impairment requiring external assistance for recovery).8 The resulting list was curated to include neuroglycopenic and adrenergic symptomology associated with hypoglycemia9 (Appendix 1). To refine the symptom-based list further, the study investigators recognized that symptoms of hypoglycemia may not be mutually exclusive to hypoglycemia if those symptoms were potentially related to comorbid conditions common among adults with T1DM and T2DM. A list of common comorbid conditions among patients with T1DM and T2DM was determined a priori (Appendix 2). The comorbid conditions served as an exclusion criterion added to the symptom-based definition of hypoglycemia. By searching for symptom-based terms while also excluding symptom-based comorbidities, the investigators hoped to reduce confounding in the capture of events resulting from hypoglycemia rather than from a condition with similar symptoms.
The search for symptom-based hypoglycemia was combined with the search for non-symptom-based hypoglycemia to arrive at a prevalence of hypoglycemia thought to be the result of recorded plus potentially “missed” hypoglycemia; in other words, the difference between the combined prevalence and the prevalence of non-symptom-based hypoglycemia alone would be hypothesized undocumented hypoglycemia (discussed during the health visit but not recorded in a medical claim).
Additional data explorations included evaluating the most frequent terms in the symptom-based definition that appeared in the non-symptom-based records and evaluating the prevalence of hypoglycemia in the non-symptom-based transcripts, excluding confounding comorbid conditions. A sensitivity analysis was performed to examine the prevalence of hypoglycemia by combining the non-symptom-based criteria with exclusion of confounding comorbidities and any 1, 2, 3, or 4 symptom-based terms. The goal of the sensitivity analysis was to understand how prevalence of hypoglycemia would change if we narrowed criteria down to as specific a definition as possible for hypoglycemia in the database.
Results
The study identified 1,070,697 unique patients with at least one medical transcript mentioning diabetes during the study. The T1DM study cohort included 41,688 patients, and the T2DM cohort included 317,399 patients (Appendix 3). Patient demographics and clinical characteristics for each cohort are detailed in Table 1. Patient records that were excluded did not distinguish between T1DM and T2DM in their transcript. Health care providers were most frequently listed as “multispecialty” (37.7% of patients with T1DM; 38.2% of patients with T2DM) and primary care providers (37.5% of patients with T1DM; 37.0% of patients with T2DM). Approximately 10% of patients in each cohort had at least one acute care or emergency department visit (9.9% of patients with T1DM; 9.5% of patients with T2DM). Approximately 1% of patients had data detailed from an endocrinologist encounter (1.2% of patients with T1DM; 1.0% of patients with T2DM). About 14% of both T1DM and T2DM cohorts listed a provider as “other,” which included cardiology, general surgery, and urgent care providers.
 |
Table 1 Patient Demographics and Clinical Characteristics of Study Cohorts by Type of Diabetes |
Hypertension was the most common comorbidity (61% of patients with T1DM; 81% of patients with T2DM), followed by hyperlipidemia (43.8% of patients with T1DM; 61% of patients with T2DM), and cardiovascular disease (39.3% of patients with T1DM; 50% of patients with T2DM).
The most frequently mentioned antidiabetic agents were insulin and metformin (Appendix 4). Insulin was documented in 89.4% of patients with T1DM and in 55% of patients with T2DM, while mention of metformin was captured in 12.1% of patients with T1DM and 36% of patients with T2DM.
Non-symptom-based hypoglycemia was captured in 18.1% of patients with T1DM and 7.6% of patients with T2DM (Table 2). Most records mentioning non-symptom-based hypoglycemia were from primary care encounters for those with T1DM (37%) and multispecialty encounters for those with T2DM (39%).
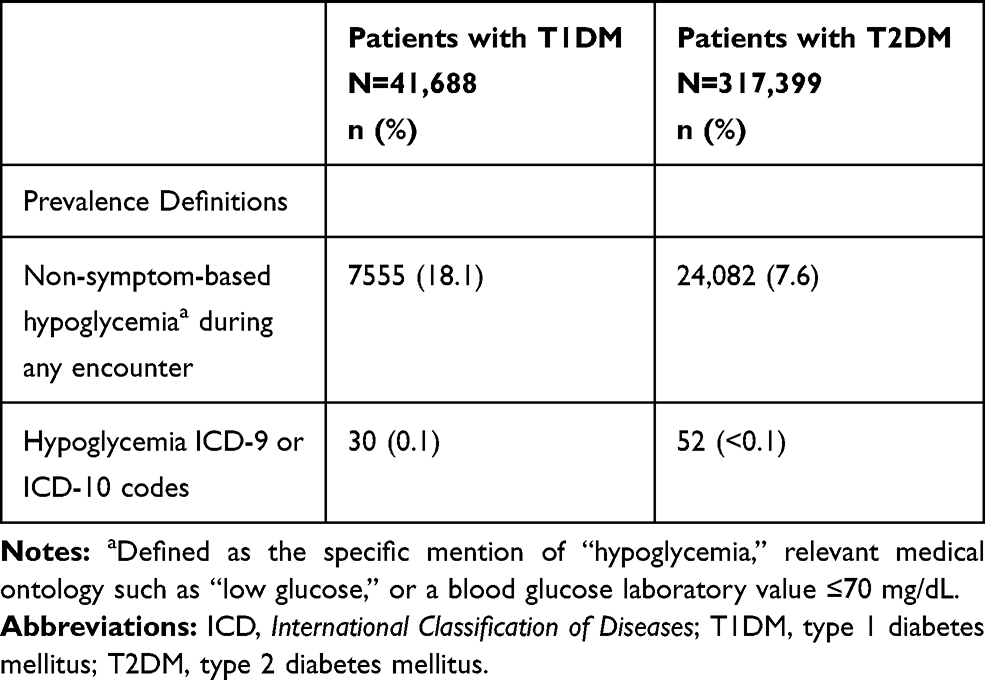 |
Table 2 Prevalence of Non-Symptom-Based Hypoglycemia by Type of Diabetes ICD Codes in Patients with T1DM and T2DM |
Among the most prevalent symptom-based definitions of hypoglycemia occurring in non-symptom-based records were irritability or anxiety (16% of patients with T1DM; 14.5% of patients with T2DM), cognitive issues (8.2% of patients with T1DM; 12.1% of patients with T2DM), and elevated/irregular heart rate (8.2% of patients with T1DM; 10.2% of patients with T2DM) (Table 3). The frequency of mentions of prespecified conditions (confounders) thought to be most associated with or potentially mistaken for symptoms of hypoglycemia were behavioral or mental illness (45.4% of patients with T1DM; 47.0% of patients with T2DM), gastrointestinal disorders (44.4% of patients with T1DM; 49.0% of patients with T2DM), and high blood sugar or diabetic ketoacidosis (33.7% of patients with T1DM; 15.0% of patients with T2DM). When confounding comorbid conditions were combined as exclusions among records of non-symptom-based hypoglycemia, prevalence of hypoglycemia was 24.8% for patients with T1DM and 23.9% for patients with T2DM. The sensitivity analyses yielded considerably lower prevalence of hypoglycemia, with the greatest record capture excluding any one confounding comorbid condition, compared to excluding any 2, any 3 or any 4 confounding comorbid conditions (Table 3).
 |
Table 3 Frequency of Symptom-Based Hypoglycemia in Records of Non-Symptom-Based Hypoglycemia |
Discussion
The prevalence of hypoglycemia among patients with diabetes is likely to be underestimated due to underreporting and lack of documentation. The current study adds to the diabetes literature an alternative way to evaluate occurrence of hypoglycemia using an innovative data source. First, the provider transcription data in the Amplity Insights database used in this study combined patient history, current situation, underlying medical complaints, and treatment plans that are not typically detailed in EHR databases. Next, medical ontology and symptoms associated with hypoglycemia were identified, and NLP was employed to analyze the transcription data. The use of NLP and the data source used in this study improved the capture of hypoglycemic events that may have been missed or undocumented in data sources such as administrative claims databases or EHR. The estimated prevalence of hypoglycemia using combined symptom-based and non-symptom-based definitions was 20.4% (T1DM) and 11.4% (T2DM), demonstrating that hypoglycemia is more prevalent than previous analyses suggest.1,2
Findings from other studies using non-traditional methods have found an increased prevalence of hypoglycemia patients with diabetes. For example, the results of a study by Nunes et al, which assessed the prevalence of hypoglycemia in adults with T2DM using the Humedica EHR database by text mention using NLP, reported a period prevalence of 25%.4 Another study by Khunti et al employed patient questionnaires and diaries to capture self-reported hypoglycemic events over a 4-week period. Eighty-three percent of patients with T1DM and 46.5% of patients with T2DM reported non-severe, nocturnal, or severe hypoglycemia during the study period.5 Frier et al conducted a survey study in the United Kingdom that reported 2.4 non-severe hypoglycemic events per week in patients with T1DM and 0.8 events per week in patients with T2DM.10 Taken together, these studies suggest that hypoglycemia prevalence is significantly underreported by claims databases, EHR, and even medical transcription data from patient encounters. This also suggests that patients report hypoglycemia when asked, but do not often do so proactively, which is consistent with the notion that hypoglycemia frequently occurs but goes unreported to HCPs.
Although hypoglycemia is underreported, severe hypoglycemia has been shown to cause recurrent morbidity and predict mortality in patients with diabetes,11 and reduce quality of life by impairing sleep quality, reducing productivity at work, and causing anxiety and depression.12–15 Many patients fear hypoglycemia,16,17 which can influence disease management for better or worse; some coping strategies incorporate heightened vigilance and improved glycemic control, while other strategies include excessive eating and avoiding vigorous activity, actions which may result in impaired metabolic control.16,18,19
Hypoglycemia is an important consideration in the use and selection of antidiabetic medications, and this study suggests that improved documentation of hypoglycemia could provide insights into the value of optimal antidiabetic medications and dosages for payers, health systems, and employers. The T2DM patient cohort in this study was not restricted to those on insulin treatments, which may have diluted the prevalence of hypoglycemia, as hypoglycemia is more prevalent among patients with T2DM treated with insulin and/or sulfonylureas compared with other classes of medications.20,21
Despite attempts to capture as many true hypoglycemic events as possible, there were several challenges with the study methodology. First, many patients were excluded from the analyses because the type of diabetes could not be confirmed, potentially resulting in selection bias. However, given the aim of the study was to identify hypoglycemia events specifically in patients with T1DM or T2DM diabetes, confirmation of type of diabetes was necessary. Second, this qualitative method requires sensitivity to the context in which hypoglycemia and related symptomology appear in query searches. As a result, it is possible to overestimate hypoglycemia occurrences if restrictions placed on the context of the mention of hypoglycemia did not appropriately deduct what was not a hypoglycemia event, or to underestimate hypoglycemia occurrences if restrictions placed on the context of mentions of hypoglycemia were too limiting. There were also challenges in the symptom-based method for assessing prevalence of symptom-based or undocumented hypoglycemic events, including addressing confounding symptoms that resulted from other underlying conditions. Although 100% confidence cannot be guaranteed in the way hypoglycemia was counted using NLP, the study took several precautions to ensure that occurrences of true hypoglycemia were captured. Another limitation is the distribution of provider types in the Amplity Insights database. The most common encounter type was “multispecialty,” a group that encompasses a large variety of encounters/providers, including a combination of emergency department or urgent care and specialists in hospital networks. It should be noted that urgent care is a specialty category in the Amplity Insights database, and for this analysis, these encounters were recorded under the “other” category of provider type. A more detailed analysis is required to fully understand the types of providers and treatment settings comprising this classification. Additionally, endocrinologists were underrepresented in the database, which may have resulted in underestimates of hypoglycemia prevalence. Also, although the search was limited to January 1, 2016–April 30, 2018, because the information in the Amplity Insights database included patient history and their current situation, these methods were unable to determine if a hypoglycemia event occurred within a this chosen timeframe.
Conclusion
The current and previous studies demonstrate that hypoglycemia is an underreported occurrence that requires further analysis to better understand its true frequency among patients with T1DM and T2DM. In this study, we estimated the prevalence of hypoglycemia using NLP of a medical transcription data. These results suggest that hypoglycemia events are most likely occurring more often and are being discussed more often than analyses of other databases indicate. Currently, there is no consistent way to report hypoglycemia in the EHR, which may preclude physicians from appropriately documenting the condition. Future studies may focus on designing a standardized method for accurately documenting this condition to better estimate the true prevalence of hypoglycemia.
Abbreviations
CVD, cardiovascular disease; DKA, diabetic ketoacidosis; DPP, dipeptidyl peptidase; EHR, electronic health record; GI, gastrointestinal; GLP, glucagon-like peptide; HbA1c, glycosylated hemoglobin; HCP, health care professional; ICD, International Classification of Diseases; MedDRA, Medical Dictionary for Regulatory Activities; MeSH, Medical Subject Headings; NCI, National Cancer Institute; NLP, natural language processing; SGLT, sodium glucose cotransporter; SNOMED, Systematized Nomenclature of Medicine; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the data license agreement but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This was a retrospective database study that did not involve patient contact.
Acknowledgments
The authors would like to thank the Amplity Insights research team, Karen Smoyer, PhD, of Curo, a division of the Envision Pharma Group, and Anna Wallace of Novo Nordisk for their assistance in analyzing the data. Karen Smoyer, PhD, also contributed to the study design. The authors acknowledge the medical writing assistance of Melissa Priest, PhD, of ETHOS Health Communications in Yardley, Pennsylvania, which was supported financially by Novo Nordisk Inc., Plainsboro, New Jersey, in compliance with international Good Publication Practice guidelines.
Author Contributions
All authors contributed to conception and design of the study, data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
CU, CMH, and MSR are employees of Novo Nordisk Inc. WW and DIA were employees of Novo Nordisk Inc. during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Liu J, Wang R, Ganz ML, Paprocki Y, Schneider D, Weatherall J. The burden of severe hypoglycemia in type 1 diabetes. Curr Med Res Opin. 2018;34(1):171–177. doi:10.1080/03007995.2017.1391079
2. Liu J, Wang R, Ganz ML, Paprocki Y, Schneider D, Weatherall J. The burden of severe hypoglycemia in type 2 diabetes. Curr Med Res Opin. 2018;34(1):179–186. doi:10.1080/03007995.2017.1391080
3. Frier BM. Hypoglycaemia in the diabetic adult. Baillieres Clin Endocrinol Metab. 1993;7(3):757–777. doi:10.1016/S0950-351X(05)80218-6
4. Nunes AP, Yang J, Radican L, et al. Assessing occurrence of hypoglycemia and its severity from electronic health records of patients with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2016;121:192–203. doi:10.1016/j.diabres.2016.09.012
5. Khunti K, Alsifri S, Aronson R, et al. Rates and predictors of hypoglycemia in 27585 people from 24 countries with insulin-treated type 1 and type 2 diabetes: the global HAT study. Diab Obes Metab. 2016;18(9):907–915. doi:10.1111/dom.12689
6. Li X, Yu S, Zhang Z, et al. Predictive modeling of hypoglycemia for clinical decision support in evaluating outpatients with diabetes mellitus. Curr Med Res Opin. 2019;35(11):1885–1891. doi:10.1080/03007995.2019.1636016
7. United States Census Bureau. Demographic and housing estimates; 2017. Available from: https://data.census.gov/cedsci/table?d=ACS%205-Year%20Estimates%20Data%20Profiles&table=DP05&tid=ACSDP5Y2017.DP05.
8. Novo Nordisk Inc. Data on File; 2017.
9. Hepburn DA, Deary IJ, Frier BM, Patrick AW, Quinn JD, Fisher BM. Symptoms of acute insulin-induced hypoglycemia in humans with and without IDDM. Factor-analysis approach. Diabetes Care. 1991;14(11):949–957. doi:10.2337/diacare.14.11.949
10. Frier B, Jensen M, Chubb B. Hypoglycemia in adults with insulin-treated diabetes in the UK: self-reported frequency and effects. Diabet Med. 2016;33(8):1125–1132.
11. McCoy RG, Van Houten HK, Ziegenfuss JY, Shah ND, Wermers RA, Smith SA. Increased mortality of patients with diabetes reporting severe hypoglycemia. Diabetes Care. 2012;35(9):1897–1901. doi:10.2337/dc11-2054
12. Polonsky WH, Fisher L, Hessler D. The impact of non-severe hypoglycemia on quality of life in patients with type 2 diabetes. J Diabetes Complicat. 2018;32(4):373–378. doi:10.1016/j.jdiacomp.2018.01.014
13. Brod M, Christensen T, Bushnell DM. Impact of nocturnal hypoglycemic events on diabetes management, sleep quality, and next-day function: results from a four-country survey. J Med Econ. 2012;15(1):77–86. doi:10.3111/13696998.2011.624144
14. Brod M, Pohlman B, Wolden M, Christensen T. Non-severe nocturnal hypoglycemic events: experience and impacts on patient functioning and well-being. Qual Life Res. 2013;22(5):997–1004. doi:10.1007/s11136-012-0234-3
15. Rossi MC, Nicolucci A, Ozzello A, et al. Impact of severe and symptomatic hypoglycemia on quality of life and fear of hypoglycemia in type 1 and type 2 diabetes. Results of the Hypos-1 observational study. Nutr Metab Cardiovasc Dis. 2019;29(7):736–743. doi:10.1016/j.numecd.2019.04.009
16. Martyn-Nemeth P, Schwarz Farabi S, Mihailescu D, Nemeth J, Quinn L. Fear of hypoglycemia in adults with type 1 diabetes: impact of therapeutic advances and strategies for prevention - a review. J Diabetes Complicat. 2016;30(1):167–177. doi:10.1016/j.jdiacomp.2015.09.003
17. Fidler C, Elmelund Christensen T, Gillard S. Hypoglycemia: an overview of fear of hypoglycemia, quality-of-life, and impact on costs. J Med Econ. 2011;14(5):646–655. doi:10.3111/13696998.2011.610852
18. Wild D, von Maltzahn R, Brohan E, Christensen T, Clauson P, Gonder-Frederick L. A critical review of the literature on fear of hypoglycemia in diabetes: implications for diabetes management and patient education. Patient Educ Couns. 2007;68(1):10–15. doi:10.1016/j.pec.2007.05.003
19. Martyn-Nemeth P, Quinn L, Penckofer S, Park C, Hofer V, Burke L. Fear of hypoglycemia: influence on glycemic variability and self-management behavior in young adults with type 1 diabetes. J Diabetes Complicat. 2017;31(4):735–741. doi:10.1016/j.jdiacomp.2016.12.015
20. Leese GP, Wang J, Broomhall J, et al. Frequency of severe hypoglycemia requiring emergency treatment in type 1 and type 2 diabetes: a population-based study of health service resource use. Diabetes Care. 2003;26(4):1176–1180. doi:10.2337/diacare.26.4.1176
21. Edridge CL, Dunkley AJ, Bodicoat DH, et al. Prevalence and incidence of hypoglycaemia in 532,542 people with type 2 diabetes on oral therapies and insulin: a systematic review and meta-analysis of population based studies. PLoS One. 2015;10(6):e0126427. doi:10.1371/journal.pone.0126427
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.