Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Artificial Intelligence Integration in Multidisciplinary Wound Management: A Scoping Review of Barriers and Facilitators in Clinical Workflows
Authors Sa’ban FZ ![]() , Purba CIH
, Purba CIH ![]() , Rahayu U, Aziz MA
, Rahayu U, Aziz MA ![]() , Afriana R, Yudha F
, Afriana R, Yudha F ![]()
Received 23 April 2026
Accepted for publication 28 May 2026
Published 8 June 2026 Volume 2026:19 619318
DOI https://doi.org/10.2147/JMDH.S619318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Faiza Zulfikar Sa’ban,1 Chandra Isabella Hostanida Purba,2 Urip Rahayu,2 Muhammad Afiif Aziz,1 Reni Afriana,1 Fendria Yudha1
1Faculty of Nursing, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, Indonesia; 2Department of Medical-Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, Indonesia
Correspondence: Faiza Zulfikar Sa’ban, Faculty of Nursing, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, Indonesia, Tel +62 851-6151-2597, Email [email protected]
Background: Chronic wound management is a complex global health challenge that requires coordinated multidisciplinary care. Artificial intelligence (AI) has the potential to improve wound assessment, documentation, and clinical decision support. However, its successful implementation depends not only on algorithmic accuracy but also on its alignment with existing sociotechnical systems and clinical workflows.
Objective: This scoping review aimed to map the operational barriers and facilitators encountered by interprofessional healthcare teams when integrating AI-based wound management technologies into clinical practice.
Methods: Guided by the Arksey and O’Malley framework and the PRISMA-ScR guidelines, a systematic literature search was conducted in PubMed, Scopus, and ScienceDirect. Empirical studies published between 2021 and 2026 were included if they examined AI-based wound management technologies in relation to clinical workflows, workload, documentation, or implementation outcomes.
Results: Nine primary studies met the eligibility criteria. The thematic synthesis identified several workflow-related facilitators, including improved documentation efficiency, greater adherence to evidence-based guidelines, enhanced diagnostic objectivity, and support for preventive care. Key barriers included increased cognitive and administrative workload during early adoption, limited interoperability with primary electronic health records, risk of automation bias, and concerns that AI may weaken relational and sensory-based aspects of clinical care.
Conclusion: AI integration in multidisciplinary wound care may support workflow efficiency and clinical decision-making, but its implementation remains a sociotechnical challenge. Sustainable adoption requires native EHR interoperability, careful mitigation of digital fatigue, and human-in-the-loop design to ensure that AI enhances clinical practice without compromising professional judgment and humanistic patient care.
Keywords: artificial intelligence, clinical workflows, wound care, barriers and facilitators, scoping review
Introduction
Chronic wound management represents a formidable global health challenge, significantly impairing patients’ quality of life while imposing an escalating financial burden on healthcare systems.1 Epidemiologically, the prevalence of chronic wounds continues to surge in tandem with an aging population and the rising incidence of diabetes, reportedly affecting up to 2.5% of the population in developed countries.2 Effective wound management is inherently complex, demanding a highly collaborative, multidisciplinary approach. Within this interprofessional dynamic, frontline nurses serve an indispensable role in continuous wound assessment and care coordination. However, conventional wound evaluation relying heavily on visual observation and manual measurement is fraught with subjectivity, inherent cognitive bias, and profound inter-rater variability across healthcare providers.3
To circumvent these clinical limitations, the integration of artificial intelligence (AI) and mobile health (mHealth) applications is rapidly being adopted to power clinical decision support systems.4 AI leverages sophisticated computational algorithms to emulate human cognitive intelligence, particularly in the rapid processing and analysis of complex medical imagery.5 Recent advances have rigorously validated these models, demonstrating their capability to detect, segment, and classify wound pathologies with a diagnostic accuracy that consistently matches or surpasses standard human clinical evaluation.6
Despite this promising clinical trajectory, the integration of AI into routine wound care disrupts established interprofessional workflow dynamics, presenting a complex paradox for clinical management. On one hand, AI acts as a potent facilitator; empirical evidence suggests that algorithmic applications significantly augment clinical decision-making and standardize adherence to evidence-based wound care guidelines.7 Conversely, AI can precipitate substantial operational barriers. This paradox is most evident in the amplified administrative burden particularly the duplicative demands of electronic health record (EHR) documentation which consumes critical care time.8 Furthermore, during the initial implementation phase, navigating fragmented AI interfaces has been shown to prolong documentation duration, thereby exacerbating the cognitive load and risking digital fatigue among healthcare professionals.9
Previous AI wound-care reviews have largely focused on algorithmic performance, diagnostic accuracy, wound image analysis, segmentation, and predictive modeling.6 However, limited attention has been given to how AI technologies are integrated into real-world multidisciplinary clinical workflows, particularly in relation to end-user readiness, documentation burden, interoperability challenges, workflow disruption, automation bias, and relational patient care.10 Given the heterogeneity of the available evidence, including variations in study design, AI applications, clinical settings, end-user populations, and implementation outcomes, a scoping review methodology was considered more appropriate than a systematic review. This approach enables the mapping of a broad and emerging body of evidence rather than the quantitative assessment of intervention effectiveness. Therefore, this study aims to systematically synthesize empirical evidence regarding the operational barriers and facilitators of implementing AI in multidisciplinary wound management, with particular emphasis on sociotechnical integration, clinical workflow alignment, and the preservation of humanistic nursing care.
Materials and Methods
Study Design
This study employed a scoping review design to systematically map the existing empirical literature regarding the operational barriers and facilitators of implementing artificial intelligence (AI) within clinical wound care workflows. The methodology was guided by the foundational framework developed by Arksey and O’Malley,11 and was further informed by the updated methodological guidance for scoping reviews, ensuring a rigorous approach to evidence synthesis. To guarantee maximum transparency and methodological accountability, the protocol and findings are reported in strict accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.
The execution of this review followed five iterative stages: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, summarizing, and reporting the results. The entire study selection process was systematically documented using a PRISMA flow diagram to visually illustrate the literature yield from initial identification through to the final synthesis.
Search Strategy
A comprehensive and systematic literature search was executed across three major electronic databases: PubMed, Scopus, and ScienceDirect. The search parameters were purposefully restricted to articles published between January 2021 and April 2026. This precise five-year limitation was applied to capture the most contemporary evolution of AI technologies, specifically reflecting the exponential advancement and active clinical deployment of deep learning algorithms within healthcare settings during this period.
The search strategy was systematically constructed utilizing Boolean operators (AND, OR) to combine Medical Subject Headings (MeSH) and relevant free-text terms encompassing artificial intelligence, wound management, clinical workflows, and implementation outcomes. The core search string employed in the identification process included: (“Artificial Intelligence” OR “Machine Learning” OR “Deep Learning”) AND (“Wound Care” OR “Chronic Wound” OR “Pressure Ulcer”) AND (“Nursing Workflow” OR “Clinical Workflow” OR “Nursing Practice”) AND (“Barriers” OR “Facilitators” OR “Challenges”). This primary syntax was iteratively adapted to fulfill the specific indexing and search requirements of each respective database. The complete, reproducible search strings utilized for all databases are detailed in Supplementary File 1.
Eligibility Criteria
The eligibility criteria were strictly formulated utilizing the Population, Concept, and Context (PCC) framework, in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews, to objectively establish transparent inclusion and exclusion parameters.
Inclusion Criteria
- Population: Primary empirical studies involving interprofessional healthcare teams, with a specific and definitive focus on registered nurses or wound care specialists as the primary clinical end-users of the technology.
- Concept: Studies that implemented and evaluated artificial intelligence (AI), machine learning (ML), or computer vision-based clinical decision support systems specifically designated for chronic or acute wound management, assessment, or diagnosis.
- Context: Studies conducted in clinical care settings (eg., inpatient wards, outpatient clinics, or home healthcare) that explicitly evaluated the sociotechnical impact of these technologies on clinical workflows, administrative workload, or documentation efficiency, reporting either operational barriers or facilitators.
- Study Types & Characteristics: Primary research (quantitative, qualitative, or mixed-methods designs) published as full-text, peer-reviewed manuscripts in the English language between January 2021 and April 2026.
Exclusion Criteria
- Algorithmic/Technical Isolation: Studies exclusively focused on the computational architecture, mathematical validation, or image pixel accuracy (eg., algorithm training datasets) of AI models without incorporating direct sociotechnical evaluation, usability testing, or feedback from human clinical end-users.
- Non-Clinical Models: Studies utilizing animal subjects (in vivo) or purely laboratory-based simulated testing (in vitro) lacking translation to human clinical environments.
- Non-Empirical Literature: Secondary literature (eg., literature, systematic, or scoping reviews), expert opinions, editorials, letters to the editor, and conference abstracts lacking complete primary empirical data.
Study Selection
Following the comprehensive database search, all identified records were imported into a reference management software Mendeley to systematically identify and eliminate duplicates. To rigorously mitigate selection bias, the screening process was executed in two distinct, blinded phases.
Initially, three reviewers (F.Z.S., M.A.A., and F.Y.) independently screened the titles and abstracts of all retrieved articles against the predefined eligibility criteria. In the subsequent phase, the full texts of all potentially relevant articles were retrieved and subjected to a comprehensive, independent evaluation by the same three reviewers to confirm final inclusion.
Any discrepancies or disagreements regarding study eligibility at either screening phase were resolved through structured discussion to reach a mutual consensus. If a consensus could not be achieved, an independent senior reviewer (C.I.H.P. or U.R.) was consulted for final adjudication.
Data Extraction
Data from the final included studies were systematically extracted by two independent reviewers (F.Z.S. and M.A.A.) utilizing a bespoke, standardized data charting matrix developed explicitly for this scoping review. To ensure strict inter-rater reliability and mitigate extraction bias, the charting instrument was iteratively piloted and calibrated on a representative subset of the included studies prior to full-scale implementation.
The extracted variables were structurally aligned with the review’s objectives and encompassed: foundational study characteristics (author(s), year of publication, country of origin, and methodological design), intervention specifics (the precise architecture of the AI or machine learning technology deployed), and clinical end-user details. Crucially, the primary findings were systematically bifurcated into two sociotechnical domains: operational barriers (eg., administrative burden, integration challenges) and operational facilitators (eg., documentation efficiency, diagnostic support) experienced by healthcare professionals within the clinical workflow.
Any interpretive discrepancies encountered during the data extraction phase were rigorously resolved through structured dialogue to reach a mutual consensus, ensuring the high fidelity of the extracted data.
Data Synthesis
The extracted data were synthesized using a convergent descriptive and thematic approach. First, quantitative and descriptive study characteristics, including study design, country, clinical setting, type of AI technology, target end-users, and implementation outcomes, were charted and summarized narratively. Second, textual findings related to AI integration in clinical practice were reviewed and coded iteratively. The initial coding focused on recurring concepts such as documentation burden, usability, interoperability, clinician trust, automation bias, diagnostic support, workflow efficiency, and preservation of relational care. Third, similar codes were compared, refined, and grouped into two overarching sociotechnical domains: operational barriers and operational facilitators. Operational barriers included themes such as increased administrative workload, cognitive burden, limited EHR interoperability, automation bias, and concerns regarding the erosion of humanistic care. Operational facilitators included documentation efficiency, diagnostic objectivity, standardized clinical decision support, preventive care orientation, and improved workflow coordination. Any differences in interpretation during the coding and synthesis process were resolved through discussion among the review team until consensus was reached.
Result
Literature Search and Selection
The comprehensive literature search across the three designated electronic databases retrieved a total of 1699 records. Following the removal of 706 duplicate citations, 993 unique records advanced to the primary screening phase. An independent evaluation of the titles and abstracts resulted in the exclusion of 919 records that did not align with the overarching thematic focus of the review.
Subsequently, a rigorous full-text evaluation was conducted on the remaining 74 articles to definitively ascertain eligibility. During this secondary phase, 65 articles were excluded based on the strict application of the predefined criteria. The specific reasons for exclusion were: the study outcomes did not evaluate clinical workflow or workload (n=30), the subject population did not involve relevant healthcare professionals (n=20), the study design lacked primary empirical data (n=10), and the intervention did not implement AI-based technologies (n=5).
Ultimately, nine primary studies met all inclusion parameters and were retained for data extraction and thematic synthesis. This systematic selection and attrition process is comprehensively depicted in the PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA-ScR flow diagram of the study selection process. *Considered from automation tools or other sources. **Excluded by a human reviewer or due to specific criteria. |
Characteristics of Included Studies
The nine primary studies, published predominantly within the last five years (2021–2026), underscore the exponential trajectory and rapid clinical deployment of AI technologies within wound care environments. Geographically, the literature reflects broad global traction, encompassing heterogeneous healthcare infrastructures across Europe (Germany, the Netherlands, Sweden, the UK), Asia (China, Malaysia), and the Americas (the USA, Brazil). The synthesized evidence demonstrated substantial methodological heterogeneity, ranging from rigorous quantitative intervention studies (eg., controlled clinical trials) to exploratory qualitative and mixed-methods designs. This diversity indicates a maturing research field that increasingly prioritizes sociotechnical and user-experience evaluations alongside sheer algorithmic accuracy.
Technologically, the predominant interventions leveraged advanced machine learning algorithms and computer vision frequently embedded within mobile health (mHealth) applications or integrated into electronic documentation systems to facilitate chronic wound assessment. Crucially, the target populations across these studies consistently centered on frontline registered nurses and dedicated wound care specialists. This demographic focus unequivocally establishes nursing professionals as the primary technological end-users and critical gatekeepers within the interprofessional care continuum. A comprehensive matrix detailing specific study characteristics, geographical origins, methodological designs, and AI architectures is provided in Table 1.
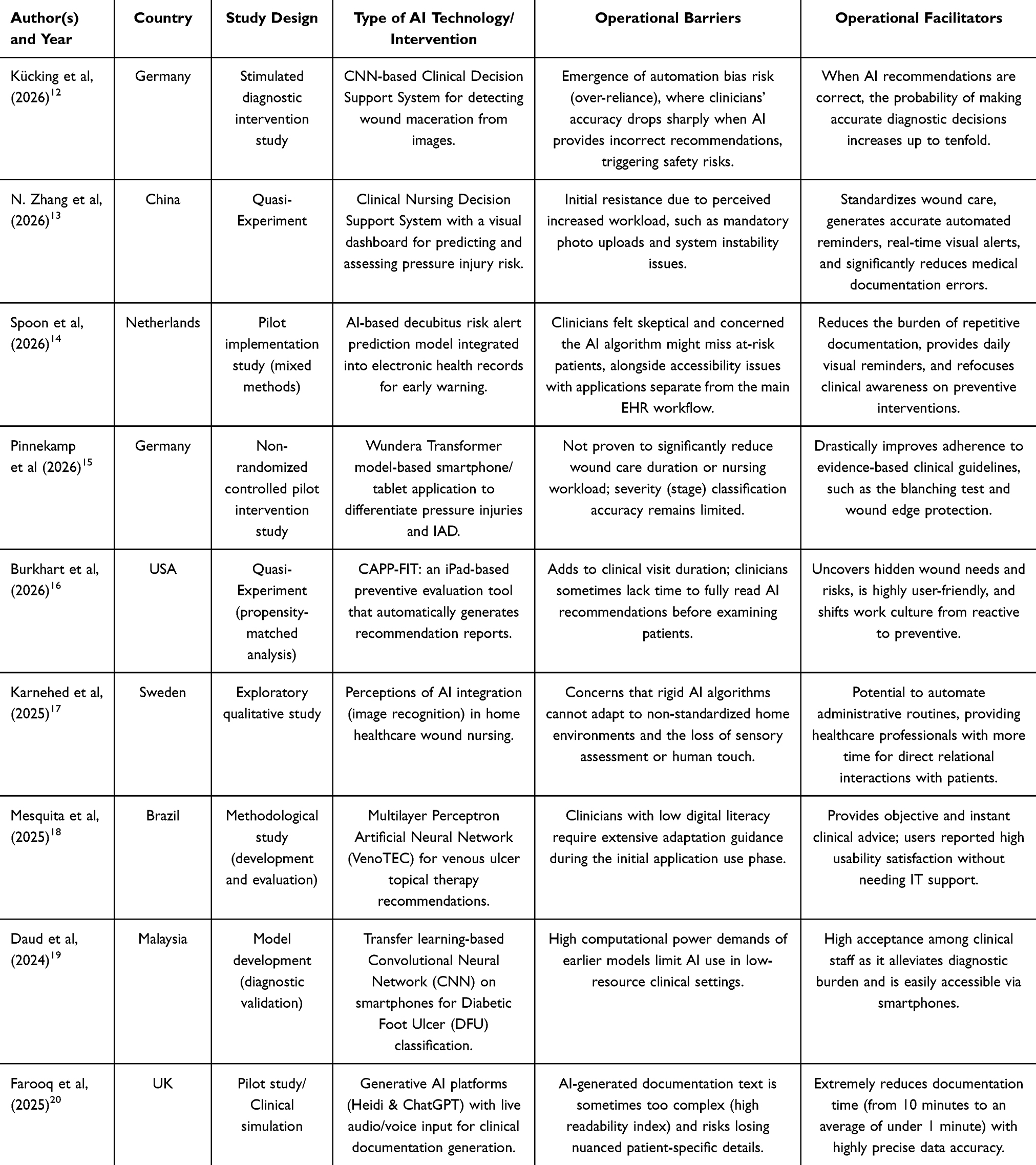 |
Table 1 Characteristics of Included Studies and Data Extraction |
Barriers to AI Integration in Clinical Workflows
The thematic synthesis identified several formidable barriers impeding the seamless adoption of AI by interprofessional healthcare teams. The most prominent operational barrier during the initial implementation phase is the acute exacerbation of cognitive and administrative workloads. The deployment of standalone, siloed AI applications that lack native interoperability with primary Electronic Health Records (EHR) consistently triggers clinical resistance. This lack of integration forces nursing staff into redundant tasks such as double data entry and the manual uploading of wound images which severely disrupts established clinical workflows.13,14 Furthermore, the additional temporal demands required to navigate these interfaces and interpret algorithmic recommendations during patient consultations have been perceived to prolong overall care duration.16 This digital burden is disproportionately borne by clinicians with lower digital literacy, who require extensive orientation and cognitive effort to adapt.18 Beyond individual readiness, the high computational and bandwidth demands of certain AI models pose substantial infrastructural barriers, particularly in resource-constrained clinical settings.19
A second, deeply profound barrier relates to clinical risk and the potential erosion of the humanistic essence of interprofessional patient care. Kücking et al12 highlighted the severe clinical threat of automation bias; when an algorithm generates an erroneous recommendation, clinicians may exhibit an over-reliance on the system, overriding their independent critical thinking. This automation complacency leads to a drastic decline in diagnostic accuracy, ultimately jeopardizing patient safety. Furthermore, there are profound ethical and philosophical concerns that the rigid diagnostic standardization imposed by AI could systematically marginalize crucial human sensory assessments such as tactile intuition, olfactory cues, and the nuanced, psychosocial details of the patient. These elements are fundamentally anchored in direct, relational nursing care, and their elimination risks reducing holistic wound management to a purely transactional, pixel-driven interaction.17,20
Facilitators of AI Integration in Clinical Workflows
Conversely, when sociotechnical barriers are effectively navigated, AI integration serves as a potent catalyst for workflow optimization across the interprofessional team. The most immediate operational advantage manifests in unprecedented documentation efficiency. Once clinical staff overcome the initial adaptation curve, the temporal savings are substantial. For instance, the deployment of generative AI platforms utilizing ambient voice recognition has been shown to drastically compress clinical documentation time from an average of 10 minutes to under a single minute per encounter.20 Furthermore, AI-driven early warning and predictive systems demonstrate significant potential in eradicating repetitive manual data entry, thereby streamlining the administrative burden across the care continuum.14
Beyond administrative relief, a paramount facilitator is the substantial augmentation of diagnostic objectivity and clinical standardization. AI systems function as a highly calibrated, objective “second opinion” for complex wound differentiation and risk stratification. When algorithmic recommendations are accurate, this capability has been shown to amplify diagnostic precision up to tenfold.12,18, Mobile AI applications are particularly impactful; they not only alleviate the acute cognitive burden associated with complex bedside decision-making19 but also systematically enforce adherence to evidence-based clinical pathways. This strategic standardization effectively shifts the overarching interprofessional work culture from a paradigm of reactive treatment to one of proactive, preventive care.15 Ultimately, the automation of both routine administrative and complex diagnostic tasks liberates invaluable clinical time. This empowers nursing professionals to reclaim their core mandate: delivering direct, high-quality, humanistic, and relational care to their patients.17
Discussion
This scoping review comprehensively synthesizes the barriers and facilitators influencing the integration of artificial intelligence (AI) into clinical wound care workflows. Given the inherent complexity of multidisciplinary wound management, technological solutions are urgently required to optimize operational efficiency and alleviate routine clinical burdens.21 The synthesized evidence elucidates that AI integration in clinical settings operates as a double-edged sword. While AI offers transformative documentation efficiency and substantially augments diagnostic accuracy,20 its successful adoption is heavily contingent upon intuitive interface design, the mitigation of cognitive load during early adaptation, and the preservation of core humanistic care values. Consequently, robust sociotechnical evaluations are imperative prior to the systemic deployment of AI in healthcare institutions.22
Our analysis underscores that the most formidable operational barrier during the initial implementation phase is the exacerbated administrative burden stemming from poor system interoperability. Medical data fragmentation remains a pervasive challenge that paralyzes seamless information exchange across interprofessional healthcare platforms.23 Currently, most AI tools for wound assessment function as standalone applications siloed from primary Electronic Health Records (EHR).13,14 His lack of native EHR integration precipitates undesirable data redundancy for the clinical staff.24 Viewed through the theoretical lens of the Technology Acceptance Model (TAM), the necessity of duplicative documentation such as manually uploading images to a separate application while retyping narratives into the EHR drastically diminishes the perceived ease of use. Because perceived ease of use directly predicts the long-term intention to adopt advanced technology among healthcare professionals,25 such redundancies often provoke significant clinical resistance. Particularly in dynamic, high-workload inpatient settings, every additional second spent on documentation is perceived as a direct impediment to patient interaction.16 Alarmingly, this amplified digital burden is a recognized catalyst for EHR-related burnout among healthcare professionals, necessitating strong managerial support during the technological transition phase.26
Beyond infrastructural constraints, such as wireless network instability impeding cloud-based applications,27 this review exposes profound ethical and patient safety dilemmas, most notably the risk of automation bias. As Kücking et al12 demonstrated, an over-reliance on algorithmic outputs can erode clinicians’ critical thinking; when AI generates erroneous predictions, healthcare professionals may override their independent judgment and defer to the algorithm. In complex multidisciplinary care environments, such automation complacency poses a severe threat to patient safety.28 This dilemma is deeply intertwined with clinicians’ apprehension regarding the erosion of clinical autonomy and the “art” of care. Comprehensive wound assessment transcends visual pixel analysis; it intrinsically demands sensory observation, olfactory assessment, and tactile empathy nuances fundamentally anchored in relational, interprofessional care, which AI algorithms cannot fully replicate.17,29 Therefore, preserving a “human-in-the-loop” architecture is non-negotiable, ensuring AI functions strictly as a clinical decision support system rather than an autonomous diagnostic entity. This framework inherently reinforces the legal and professional accountability of the multidisciplinary team when incorporating AI recommendations into care plans,30 alongside the uncompromising ethical mandate to secure patient medical imagery.31
Conversely, when these sociotechnical barriers are systematically dismantled, AI manifests as a potent workflow facilitator. The application of deep learning and computer vision introduces unprecedented diagnostic objectivity, effectively neutralizing the inter-rater variability that has historically plagued manual wound assessments.19,32 Ultimately, the strategic automation of diagnostic and administrative tasks serves to reclaim valuable clinical time, allowing the multidisciplinary team to reinvest their focus into direct, high-quality patient care. Given that increased direct care time is robustly correlated with improved patient safety and satisfaction metrics,33 involving frontline clinical end-users in the initial AI design phase is critical to ensure these technologies reflect operational realities. Moving forward, integrating health informatics into formal clinical curricula will be essential to equip the next generation of healthcare professionals with the technological fluency required to navigate this rapidly evolving landscape.34,35
Limitations
While this scoping review provides a comprehensive synthesis of the current sociotechnical landscape, several methodological limitations warrant acknowledgment. First, the systematic literature search was restricted to three primary electronic databases (PubMed, Scopus, and ScienceDirect) and limited exclusively to English-language publications. This parameter introduces a potential language and regional publication bias, as relevant empirical studies indexed in local healthcare databases or published in other languages may have been inadvertently omitted.
Second, the synthesized evidence demonstrated profound methodological heterogeneity encompassing controlled intervention trials, simulated clinical environments, and exploratory qualitative designs. While this diversity is highly characteristic of a rapidly evolving and nascent technological field, it precludes direct comparative evaluations or the quantitative meta-synthesis of workflow efficiency metrics. Furthermore, in alignment with standard scoping review methodologies, this study did not conduct a formal critical appraisal or risk-of-bias assessment of the included literature. Consequently, while this review effectively maps the breadth of operational barriers and facilitators, the relative methodological quality and the strength of evidence from the primary studies were not formally evaluated.
Finally, the majority of the reviewed literature comprises pilot programs or early-phase implementations with relatively small sample sizes. Consequently, to definitively establish the long-term sustainability, scalability, and sociotechnical efficacy of AI integration within dynamic interprofessional clinical workflows, future research must transition toward large-scale, multi-center, and longitudinal empirical investigations.
Policy and Management Implications
Beyond altering immediate clinical workflows, the systemic integration of AI in multidisciplinary wound management necessitates profound strategic adaptations at both the institutional and macro-policy levels. Healthcare executives and nursing administrators must decisively pivot away from the procurement of fragmented, standalone AI applications. Instead, strategic capital investments must be directed toward robust IT infrastructures that guarantee native interoperability with primary electronic health records (EHR). This architectural alignment is non-negotiable for mitigating the administrative bottlenecks and duplicative documentation that precipitate EHR-related burnout among frontline clinical staff.
Furthermore, clinical governance boards and policymakers must proactively construct clear Standard Operating Procedures (SOPs) and rigorous legal frameworks. These regulations must unequivocally delineate professional and legal accountability in the event of AI-assisted diagnostic discrepancies or adverse patient outcomes. From a patient-centered perspective, institutional policies must actively safeguard trust by mandating transparent informed consent protocols, particularly concerning the algorithmic analysis of sensitive medical imagery. Ultimately, strategic technological procurement and rigorous clinical governance must operate in tandem to ensure that AI serves as a sustainable, secure adjunct to holistic interprofessional care, rather than an operational disruptor.
Conclusion
This scoping review shows that artificial intelligence (AI) can support multidisciplinary wound management by improving diagnostic objectivity, documentation efficiency, and adherence to evidence-based care. However, its clinical value depends on effective sociotechnical integration, particularly native EHR interoperability, reduced cognitive burden, mitigation of automation bias, and preservation of relational and sensory-guided nursing care. Future AI implementation should prioritize human-in-the-loop, user-centered design supported by strong clinical governance and managerial strategies to ensure that technological efficiency enhances, rather than compromises, humanistic interprofessional care.
The Patient’s Perspective and Trust
Equally critical to operational and legal frameworks is the preservation of the patient’s voice and trust within the AI-augmented care paradigm. From a patient-centered perspective, institutional policies must prioritize psychological comfort and transparency when algorithms are utilized to analyze sensitive wound imagery. Multidisciplinary teams must be equipped to clearly communicate how AI tools are being used as supportive adjuncts rather than replacements for human care, ensuring that informed consent protocols are thoroughly respected. Ultimately, technological procurement and clinical governance must work in tandem to guarantee that AI serves to enhance holistic patient care without eroding the fundamental human connection.
Declaration of Generative AI
The authors used Google Gemini during the preparation of this work to improve readability and language structure. After using this tool, the authors reviewed and edited the content and take full responsibility for the integrity of the manuscript.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its supplementary file.
Ethics Statement
Ethical approval and informed consent were not required for this study, as it constitutes a systematic review of previously published and publicly available literature. This research did not involve any direct interaction with human participants or animal subjects. All synthesized data were extracted from peer-reviewed publications, and the study was conducted in accordance with standard ethical guidelines for secondary research.
Acknowledgments
We would like to thank Universitas Padjadjaran, Bandung, West Java, Indonesia, for facilitating the database for this study. This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. El Arab RA, Al Moosa OA, Sagbakken M, et al. Integrative review of artificial intelligence applications in nursing: education, clinical practice, workload management, and professional perceptions. Front Public Heal. 2025;13(August). doi:10.3389/fpubh.2025.1619378
2. Sen CK. Human wound and its burden: updated 2022 compendium of estimates. Adv Wound Care. 2023;12(12):657–11. doi:10.1089/wound.2023.0150
3. Al-Mutairi HH, Al-Mansour HS, Al-Mutairi MS, et al. Complex Wound management: nursing intervention protocols-an updated review. J Ecohumanism. 2024;3(8):2921–2936. doi:10.62754/joe.v3i8.5788
4. Ramachandram D, Ramirez-GarciaLuna JL, Fraser RDJ, Martínez-Jiménez MA, Arriaga-Caballero JE, Allport J. Fully automated wound tissue segmentation using deep learning on mobile devices: cohort study. JMIR mHealth uHealth. 2022;10(4):e36977. doi:10.2196/36977
5. Yang CC. Explainable artificial intelligence for predictive modeling in healthcare. J Healthc Inform Res. 2022;6(2):228–239. doi:10.1007/s41666-022-00114-1
6. Reifs Jiménez D, Casanova-Lozano L, Grau-Carrión S, Reig-Bolaño R. Artificial intelligence methods for diagnostic and decision-making assistance in chronic wounds: a systematic review. J Med Syst. 2025;49(1):29. doi:10.1007/S10916-025-02153-8
7. Pinnekamp H, Rentschler V, Majjouti K, et al. Controlled pilot intervention study on the effects of an AI-based application to support incontinence-associated dermatitis and pressure injury assessment, nursing care and documentation: study protocol. Res Nurs Health. 2025;48(4):419–428. doi:10.1002/nur.22469
8. Corbett S, Maruthu R, Saab MM, Lehane E. Nurses’ perceptions of facilitators and barriers to their acceptance of electronic health records: a mixed-method systematic review. J Clin Nurs. 2025;34(8):3085–3100. doi:10.1111/jocn.17736
9. Stefanelli A, Zahia S, Chanel G, Niri R, Pichon S, Probst S. Developing an AI-powered wound assessment tool: a methodological approach to data collection and model optimization. BMC Med Inform Decis Mak. 2025;25(1):297. doi:10.1186/s12911-025-03144-y
10. Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23(1). doi:10.1186/s12909-023-04698-z
11. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
12. Kücking F, Busch DA, Przysucha M, et al. Impact of AI recommendation correctness on diagnostic accuracy in clinical decision-making. Int J Med Inform. 2026;207(August 2025):106223. doi:10.1016/j.ijmedinf.2025.106223
13. Zhang N, Meng Z, Xu L, Zhang Y, Wu Z, Fa T. Development and application of a clinical nursing decision support system for pressure injury in postoperative cardiac surgery patients. Digit Heal. 2026;12:1–15. doi:10.1177/20552076251411638
14. Spoon D, de Vroed A, Greup S, van Dijk M, Ista E. Integrating artificial intelligence in nursing practice with decubitus risk prediction alerts: a pilot process evaluation. J Clin Nurs. 2026;1–14. doi:10.1111/jocn.70212
15. Pinnekamp H, Priester V, Steidle J, et al. Effects of a transformer-based AI-based application to support incontinence-associated dermatitis and pressure injury assessment, nursing care and documentation: controlled pilot intervention study. Int J Nurs Stud Adv. 2026;10(September 2025):100479. doi:10.1016/j.ijnsa.2026.100479
16. Burkhart EL, Jacob RL, Bartle B, et al. Feasibility, usability, and satisfaction of a decision support tool to prevent community-acquired pressure injuries for use in the spinal cord injury clinic. Med Care. 2026;64(1):S73–S81. doi:10.1097/MLR.0000000000002214
17. Karnehed S, Larsson I, Petersson L, Erlandsson LK, Tyskbo D. Navigating artificial intelligence in home healthcare: challenges and opportunities in nursing wound care. BMC Nurs. 2025;24(1). doi:10.1186/s12912-025-03348-7
18. Da Mesquita SKC, Freitas LS, Da Silva IP, et al. Multilayer perceptron artificial neural network to support nurses’ decision-making on topical therapies for venous ulcers: construction, validation, and evaluation. BioMedInformatics. 2025;5(4):1–20. doi:10.3390/biomedinformatics5040072
19. Daud MM, Bajuri MY, Sheng PLW, Ahmad MN. Revolutionizing diabetic foot ulcer treatment prediction: harnessing the power of artificial intelligence and transfer learning; 2024. doi:10.1016/B978-0-443-21475-2.00005-9
20. Farooq F, Cooper H, Shipman A, Mitchell CD. Artificial intelligence compared with traditional methods of generating dermatology consultation letters: a pilot study comparing accuracy, readability and efficiency. Clin Exp Dermatol. 2025;50(12):2425–2430. doi:10.1093/ced/llaf323
21. Pepito JA, Acaso NJ, Merioles R, Ismael J. Opportunities, challenges, and future directions for the integration of automation in nursing practice: discursive study. JMIR Nurs. 2025;8:e72674. doi:10.2196/72674
22. Alami H, Lehoux P, Papoutsi C, Shaw SE, Fleet R, Fortin JP. Understanding the integration of artificial intelligence in healthcare organisations and systems through the NASSS framework: a qualitative study in a leading Canadian academic centre. BMC Health Serv Res. 2024;24(1):701. doi:10.1186/s12913-024-11112-x
23. Matog D, Almuwallad ANA. Advancing healthcare delivery and patient safety through health information systems: an integrative review of digital transformation, interoperability challenges, and emerging technologies in clinical practice. J Int Cris Risk Commun Res. 2025;8(4):82–83. doi:10.63278/jicrcr.vi.3206
24. Akbar MA, Sukemi S, Wabula LR, Kurniawan D, Amir H. Healthcare providers’ interprofessional collaboration experience with integrated information system for non-communicable disease management at primary care in Indonesia: a qualitative study. Int J Community Based Nurs Midwifery. 2025;13(3):191–201. doi:10.30476/ijcbnm.2025.106621.2773
25. Hussain A, Zhiqiang M, Li M, et al. The mediating effects of perceived usefulness and perceived ease of use on nurses’ intentions to adopt advanced technology. BMC Nurs. 2025;24(1):33. doi:10.1186/s12912-024-02648-8
26. Moy AJ, Schwartz JM, Chen R, et al. Measurement of clinical documentation burden among physicians and nurses using electronic health records: a scoping review. J Am Med Inform Assoc. 2021;28(5):998–1008. doi:10.1093/jamia/ocaa325
27. Alsahfi T, Badshah A, Aboulola OI, Daud A. Optimizing healthcare big data performance through regional computing. Sci Rep. 2025;15(1):3129. doi:10.1038/s41598-025-87515-5
28. Wysocki O, Davies JK, Vigo M, et al. Assessing the communication gap between AI models and healthcare professionals: explainability, utility and trust in AI-driven clinical decision-making. Artif Intell. 2023;316:103839. doi:10.1016/j.artint.2022.103839
29. Buono RA, Nygren M, Bianchi-Berthouze N. Touch, communication and affect: a systematic review on the use of touch in healthcare professions. Syst Rev. 2025;14(1):42. doi:10.1186/s13643-025-02769-4
30. Mohammed SAAQ, Osman YMM, Ibrahim AM, Shaban M. Ethical and regulatory considerations in the use of AI and machine learning in nursing: a systematic review. Int Nurs Rev. 2025;72(1):e70010. doi:10.1111/inr.70010
31. Zhang D, Ren L, Shafiq M, Gu Z. A privacy protection framework for medical image security without key dependency based on visual cryptography and trusted computing. Comput Intell Neurosci. 2023;2023(1):6758406. doi:10.1155/2023/6758406
32. Derwin R, Patton D, Strapp H, Moore Z. Integrating point-of-care bacterial fluorescence imaging-guided care with continued wound measurement for enhanced wound area reduction monitoring. Diagnostics. 2024;14(1):2. doi:10.3390/diagnostics14010002
33. Li LZ, Yang P, Singer SJ, Pfeffer J, Mathur MB, Shanafelt TD. Nurse burnout and patient safety, satisfaction, and quality of care. JAMA Netw open. 2024;7(11):e2443059. doi:10.1001/jamanetworkopen.2024.43059
34. Van Houwelingen T, Meeuse ACM, Kort HSM. Enabling nurses’ engagement in the design of healthcare technology - core competencies and requirements: a qualitative study. Int J Nurs Stud Adv. 2024;6:100170. doi:10.1016/j.ijnsa.2023.100170
35. Kleib M, Arnaert A, Nagle LM, et al. Digital health education and training for undergraduate and graduate nursing students: scoping review. JMIR Nurs. 2024;7(1):e58170. doi:10.2196/58170
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Automated Filtering and Visualization of Patient-Centered Data from Electronic Health Records in Emergency Care: A Scoping Review
Lenz J, Richter I, Meister S
Journal of Multidisciplinary Healthcare 2025, 18:6503-6517
Published Date: 9 October 2025