Back to Journals » Risk Management and Healthcare Policy » Volume 16
Evaluating the Environmental Impact of Single-Use and Multi-Use Surgical Staplers with Staple Line Buttressing in Laparoscopic Bariatric Surgery
Authors Meissner M ![]() , Hafermann J
, Hafermann J ![]() , Silas U
, Silas U ![]() , Saunders R
, Saunders R ![]()
Received 20 April 2023
Accepted for publication 24 July 2023
Published 4 August 2023 Volume 2023:16 Pages 1423—1433
DOI https://doi.org/10.2147/RMHP.S415989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Markus Meissner,1 Juliane Hafermann,2 Ubong Silas,2 Rhodri Saunders2
1Austrian Institute of Ecology, Vienna, Austria; 2Coreva Scientific GmbH & Co. KG, Koenigswinter, Germany
Correspondence: Rhodri Saunders, Coreva Scientific GmbH & Co KG, Im Muehlenbruch 1, Koenigswinter, 53639, Germany, Tel +49 2223 781 8010, Fax +49 761 76 999 421, Email [email protected]
Purpose: Operation rooms have a large environmental impact. Single-use staplers (SUS) are widely used surgical instruments that contribute to resource consumption and waste generation, whereas multi-use staplers (MUS) can greatly reduce the environmental impact of surgery. The staple lines are often reinforced with buttressing material to prevent leaks and bleeding. We explore current clinical practice and environmental concerns regarding stapling and buttressing, as well as the environmental impact of staple line buttressing in sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB). Furthermore, we extend this analysis by taking packaging material and the lithium in power supplies into consideration.
Materials and Methods: A survey of bariatric surgeons was conducted to assess stapler and buttressing use in clinical practice. We deconstructed and analyzed the product and packaging composition of a commonly used SUS with separate staple line reinforcement (Echelon Flex™ with Echelon Endopath™, Ethicon) and MUS (Signia™ with Tri-Staple™ reinforced reloads, Medtronic), where the buttressing material was delivered separately or already incorporated in the reload cartridge, respectively. Both systems were compared regarding total waste generation, resource use (determined as total material requirement), and greenhouse gas emission caused by their lithium content.
Results: 60 mm cartridges were most frequently used in bariatric surgery, and 67% of surveyed surgeons applied staple line reinforcement. MUS with pre-attached buttressing resulted in a reduction of waste, material consumption, and greenhouse gas emissions compared to SUS with separate buttressing: they reduced product waste by 40% (SG and RYBG), packaging waste by 60% (SG) and 57% (RYGB), resource consumption by more than 90%, and greenhouse gas emissions related to the lithium in the batteries by 99.7%. Preloaded buttressing produced less waste than separate buttressing per stapler firing.
Conclusion: The environmental impact of surgery can be greatly reduced by using MUS with pre-attached buttressing rather than SUS with separate buttressing.
Keywords: circular economy, staple line reinforcement, reuse, resource efficiency, bariatric surgery, healthcare economics
Introduction
The environmental impact of health care is an increasing cause for concern.1 Global health care contributes between 1% and 5% of the total global environmental impact, depending on the indicator considered.2 Hospitals and medical retail of devices and pharmaceuticals together account for 52% of the CO2eq emissions caused by health care.3 In 2021, seven European countries committed to strengthening the climate resilience and sustainability of their health systems.4 Their health carbon footprint amounted to 145.4 Mt CO2eq,5 or approximately 58% of all healthcare emissions across the EU.6 Since then, programs to promote environmentally friendly purchasing decisions have been put in place, and the environmental impact of healthcare decisions is an increasing focus.
The generation of waste and greenhouse gases as well as resource consumption are central to the environmental impact of health care. In developed countries, hospitals generate an average 1% of a nation’s solid waste and 2.1% of its greenhouse gas emissions annually.1 In the USA, hospitals generate an average 5500 tons of waste daily.7 Operation rooms (ORs) in particular are responsible for a large share of waste, producing approximately 20% of a hospital’s total waste.7 The ORs of a single hospital can produce over 100 tons of waste per year, with a 30% proportion of plastics.8 The need for sterility in the OR encourages the use of disposable devices and materials sealed in plastic packaging.1,9–11 Waste disposal costs for an OR were estimated to be USD 45,000 per year.8
Single-use devices contribute to resource consumption and waste generation.12 Reusing medical devices is a favorable circular economic strategy13 that can greatly reduce the environmental impact of surgery14 and can even reduce costs.15 In bariatric surgery, the use of reusable instead of single-use staplers has been shown to decrease both waste and resource use.14
Staple lines are reinforced in more than 50% of bariatric surgeries to reduce bleeding and leaks.16 One method of staple line reinforcement with improved clinical outcomes is the use of buttressing:16,17 a thin strip of material that is incorporated into the staple line. The buttress can either be a separate component or it can be pre-attached and therefore already a component of the reload.18,19
As surgical stapling and staple line reinforcement are frequently used in laparoscopic bariatric surgery and based on the previous study on the environmental impact of multi-use staplers in bariatric surgery,14 we reassessed the environmental impact of reusable versus single-use staplers in sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) including staple line buttressing. We not only assessed the material composition of the devices but also the impact of packaging on waste generation and the lithium in power supplies contributing to greenhouse gas emissions. The evaluation involved three stages: (1) a survey of bariatric surgeons to understand and quantify stapler and buttressing use in clinical practice; (2) a product deconstruction to assess the material composition of the staplers to determine their environmental impact; and (3) use and product composition data were combined into an environmental impact model.
Materials and Methods
Devices and Setting
This study compares two frequently used stapling systems and their respective buttressing material: the single-use Echelon Flex™ stapler (SUS) with the Echelon Endopath™ Staple Line Reinforcement (Ethicon, Cincinnati, OH, USA) and the multi-use Signia™ stapler (MUS) with Tri-Staple™ reinforced reloads that already have buttressing incorporated (Medtronic, Minneapolis, MN, USA). The use of these stapling systems is evaluated in laparoscopic SG and laparoscopic RYGB.
Survey
A survey of bariatric surgeons was done to estimate surgical stapler use and staple line reinforcement in clinical practice including surgeons’ awareness of environmental issues. The survey was reviewed and approved by the Health Media Lab Institutional Review Board (Health Media Lab is registered with the US Department of Health & Human Services, Office of Human Research Protections; HML IRB Review #1071GSGC22). An independent IRB was approached to review this study as the authors are not affiliated with a research institute and therefore do not have access to an internal IRB. All participants provided informed consent electronically prior to survey participation. A full list of all survey questions and answer options is provided in Supplementary Table 1.
The survey took place online on an open-source survey tool provided by LimeSurvey GmbH, Hamburg, Germany (http://www.limesurvey.org) between April 2022 and June 2022. A total of 46 surgeons who perform bariatric surgery were contacted; 37 surgeons consented to being surveyed and 18 participants from Australia, Canada, France, Italy, New Zealand, the USA, and the UK completed the survey.
Survey responses were analyzed in Microsoft® Excel®. Analyses focused on the number of procedures performed, types of stapling systems, size and number of cartridges used, and number of buttressed staple lines per surgery category. The survey also assessed how environmental concerns, if at all, impact decision-making.
Product Material Analysis
All system components of both stapling systems and their packaging were manually deconstructed, and their total weight was calculated.
For the SUS, the components PSEE60A, ECR60W, and ECH60R were disassembled and analyzed. For the MUS, the single-use components SIGPSHELL and SIGTRSB60AMT (with buttressing) or EGIA60AMT (without buttressing) and the reusable components SIGPHANDLE, SIGADAPTSTND, SIGRIG, and SIGSBCHGR were assessed.
This study focused on the 60 mm cartridges, which were commonly used in bariatric surgery. For both stapler systems, cartridge options are available for different tissue thicknesses. As their core components remained unchanged, it was considered sufficient to undertake the full analysis only on the 60 mm stapler cartridges. An overview of the surgical stapling system components is provided in Table 1.
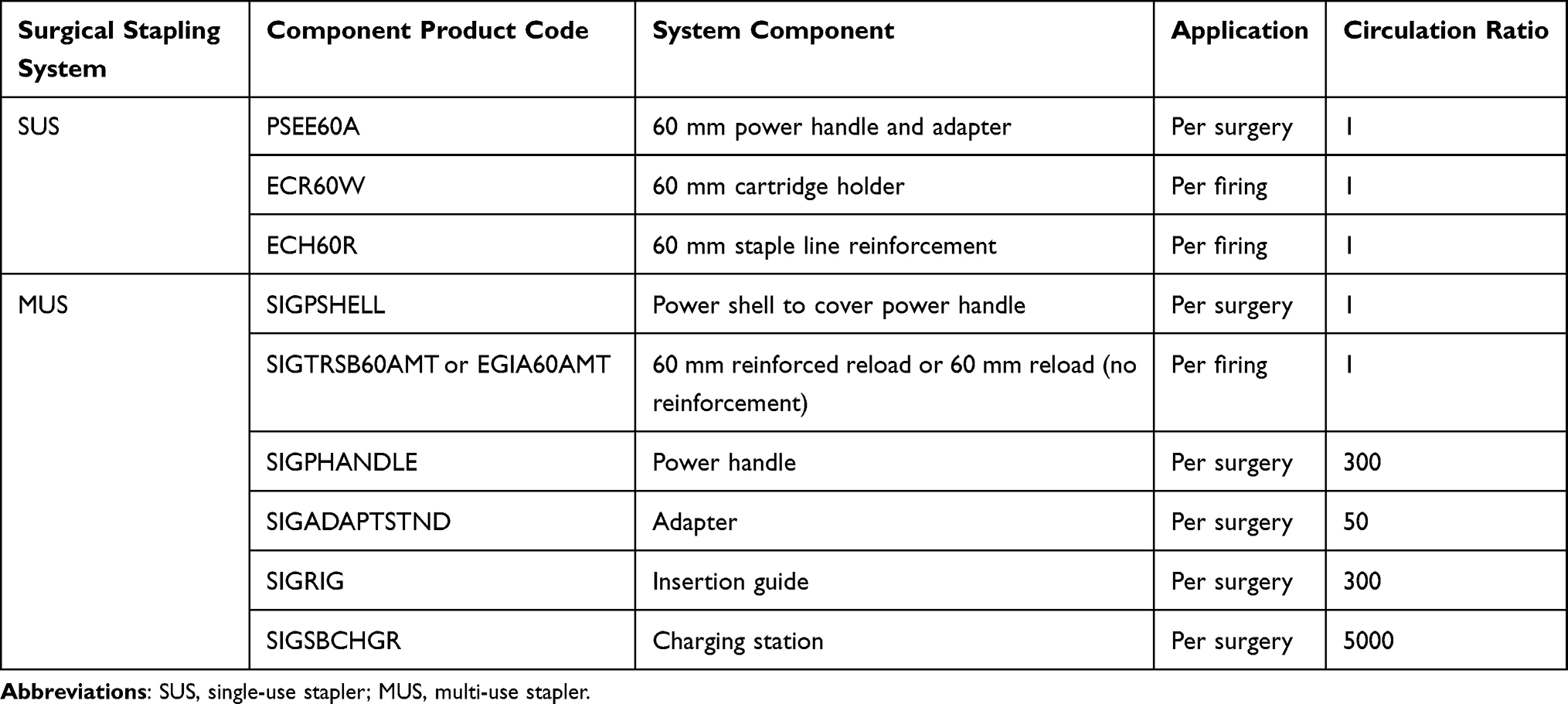 |
Table 1 Surgical Stapling System Components |
Waste Generation
Based on the product material analysis, the amount of waste that is generated per surgery in clinical practice was determined. The stapling systems were compared as described previously.14 The circulation rates (how many times each component can be used before it has to be replaced) of both stapling systems were determined (Table 1). The circulation rates of reusable MUS components were pre-defined by the manufacturer based on useful life estimates,20 and the MUS ensures that it is not possible to exceed the maximum number of uses for the power handle and the adapter.21 We also analyzed the supplies used for each reinforced staple line firing. The SUS requires one 60 mm staple line reinforcement per firing. The MUS buttressing is preloaded in the stapler cartridge, so no additional components beyond the buttressing material required analysis. For a complete view on waste generation, the analysis of packaging was included.
The average number and type of cartridges and reinforcements used per procedure were estimated from survey results. Based on these numbers and the circulation rates per component, the waste associated with each stapler firing and surgical procedure was calculated.
Total Material Requirement
As an indicator for the material intensity of the product,22 the total material requirement (TMR) was calculated for each component and stapling system. It reflects all biotic and abiotic materials and moved soil that is needed to manufacture a product.23,24 The TMR is calculated based on the material composition and weight of each component: the masses of all used elements are multiplied with TMR coefficients reflecting the primary material use. Here, the TMR of each system component is used to extrapolate the total amount of natural resources used to perform each surgery.
Lithium Content
The environmental impact of the stapler’s power supply was estimated by regarding lithium use. The SUS battery is non-rechargeable, whereas the MUS battery is rechargeable. The cells were mechanically separated and deconstructed, and their components dried at 20°C in an extraction hood until their weight remained constant. The dried material underwent an aqua regia digestion and was then analyzed in an Inductively Coupled Plasma Mass Spectrometry screening following EN ISO 17294–2:2017-01 to determine the lithium content. The greenhouse gas emission per surgery was calculated by multiplying the lithium mass per stapler with the emission factor for lithium25 and dividing it by the circulation rate of the power supply.
Sensitivity Analysis
Sensitivity analyses were performed in order to understand how different input variables and assumptions affect the end results.26 The impact of circulation ratios of SUS and MUS was already explored previously.14 Therefore, we varied the rate of buttressing per procedure to explore the impact on the waste prevention potential and TMR results.
Results
Survey
The majority of survey respondents, 12 (67%) surgeons, stated that they are concerned about the environmental impact of surgery, although only 4 (22%) participants reported that their hospital promoted environmentally friendly purchasing. Half (50%) of the survey participants reported that they never made changes to their work practice based on environmental concerns, with 11 (61%) survey participants prioritizing ease of use and price over environmental impact in purchasing decisions.
On average, respondents performed 24.9 (range: 4–100) SGs and 9.6 (range: 2–23) RYGBs per month. The majority (88%) of surgeons preferred powered staplers over manual staplers. Staple line reinforcement was frequently applied, with 12 (67%) surgeons using staple line reinforcement, and 7 (39%) of the 12 surgeons applying reinforcement in every procedure.
For each SG, an average 0.6 45 mm cartridges and 5.0 60 mm cartridges were used. No use of 30 mm cartridges was reported. Per RYGB, an average 0.2 30 mm cartridges, 1.0 45 mm cartridges, and 5.0 60 mm cartridges were used. Staple-line buttressing was most frequently used with 60 mm cartridges (Table 2).
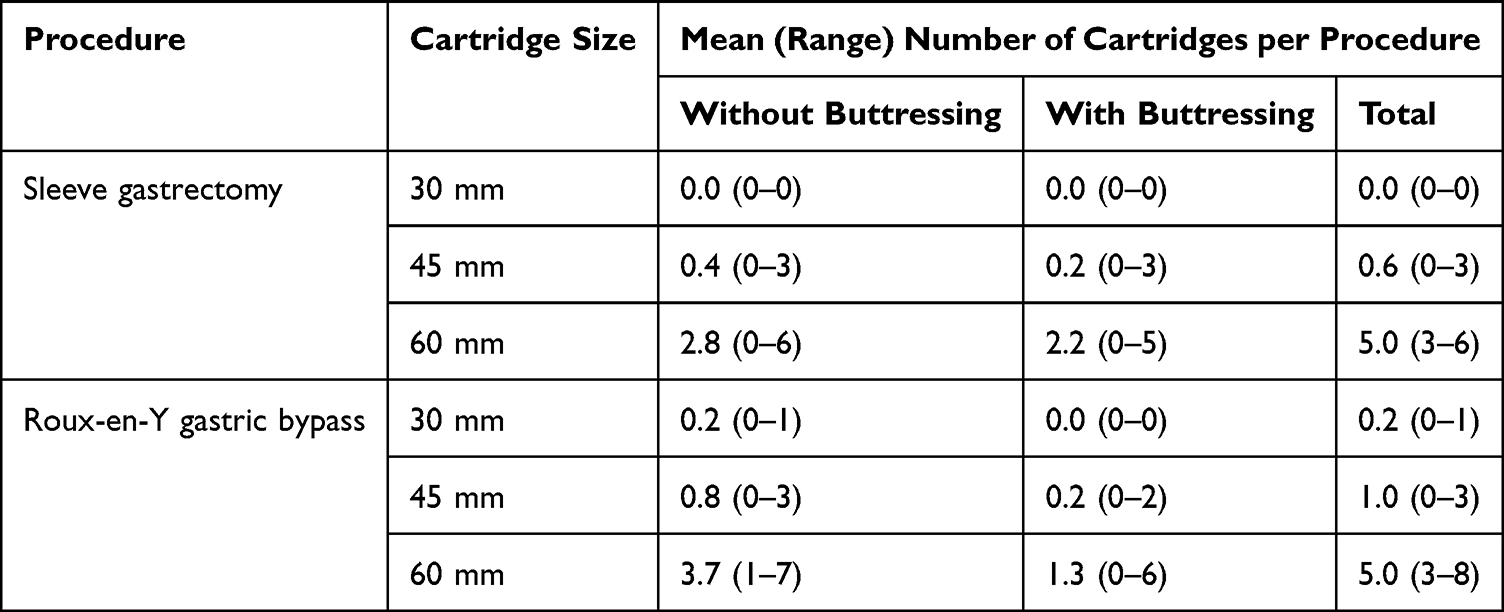 |
Table 2 Use of Staplers and Staple Line Buttressing in Bariatric Surgery |
Product Material Analysis
The total weight of each stapling system component is provided in Table 3. Overall, the MUS is heavier than the SUS by 1,356.08 g, of which 388.34 g are packaging material. The addition of buttressing material slightly increases the total weight of the MUS by 14.22 g; the total weight of the SUS is increased more substantially by 88.67 g (Table 4).
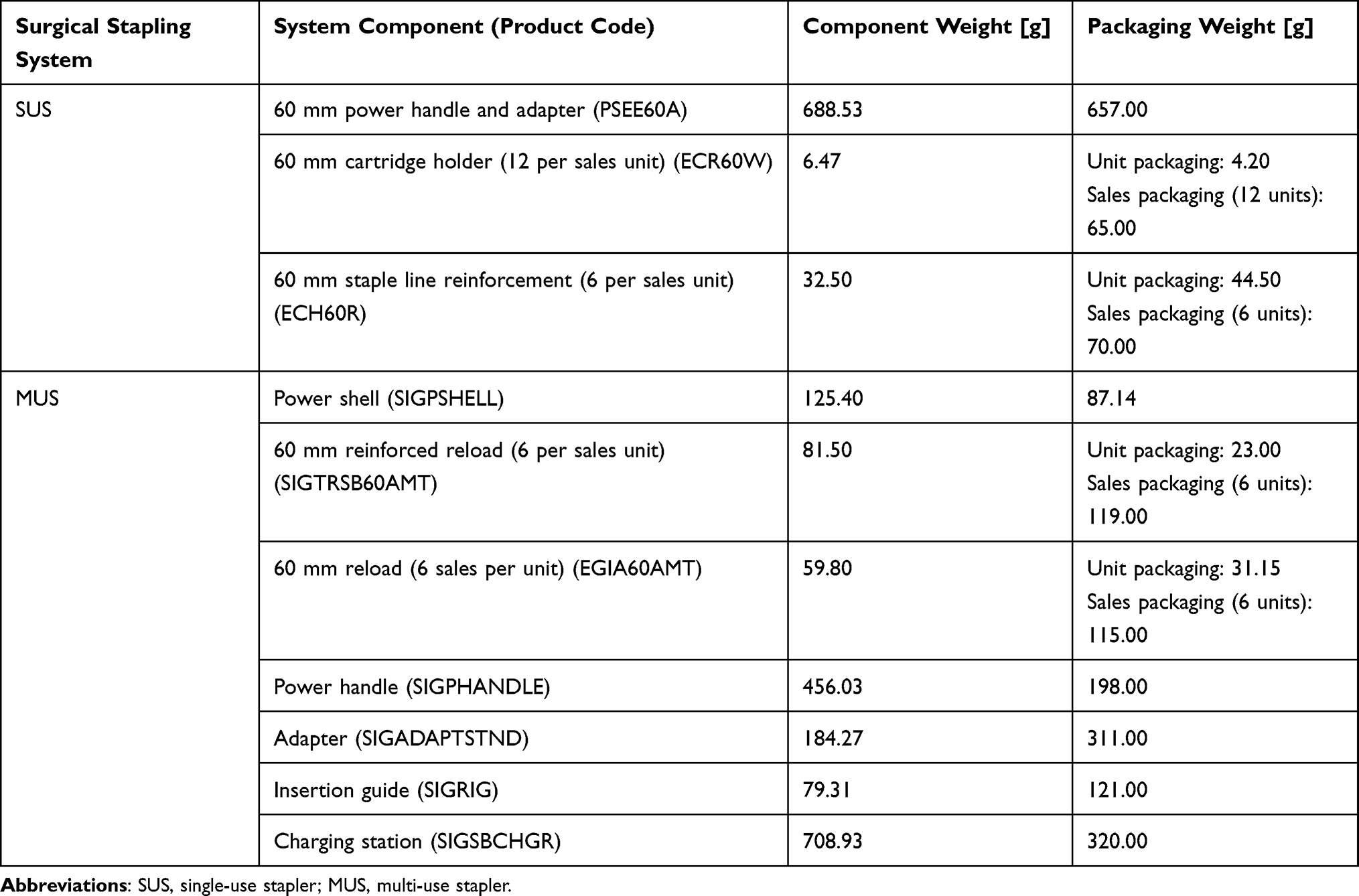 |
Table 3 Material Composition of the Surgical Stapling Systems |
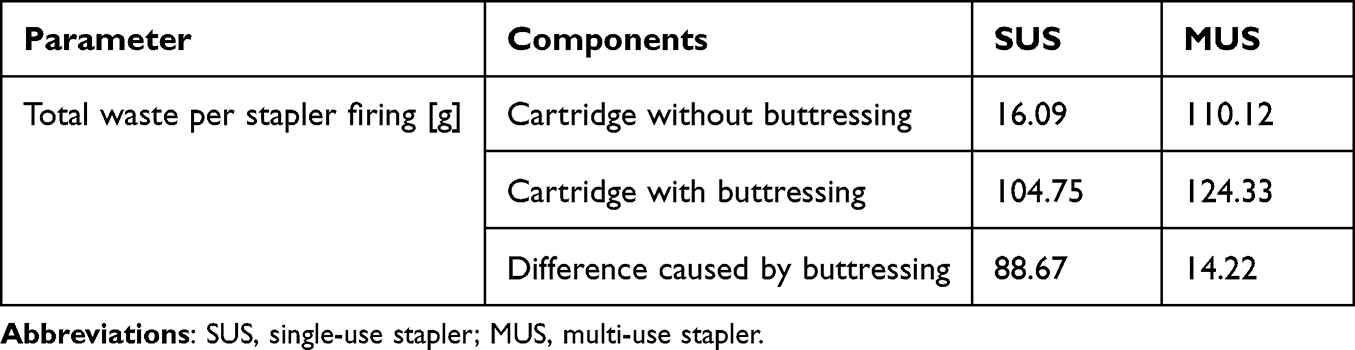 |
Table 4 Total Waste of Stapler Cartridges with and without Buttressing per Stapler Firing |
Waste Generation
MUS considerably reduce the amount of product and packaging waste per surgery compared to SUS (Table 5). They reduce the total waste by 813.67 g and 746.47 g for SG and RYGB, respectively. This translates to a total waste prevention potential of 50% for SG and 48% for RYGB. The product waste is reduced by 40% in both types of surgery, and the packaging waste is reduced by 60% per SG and by 57% per RYGB.
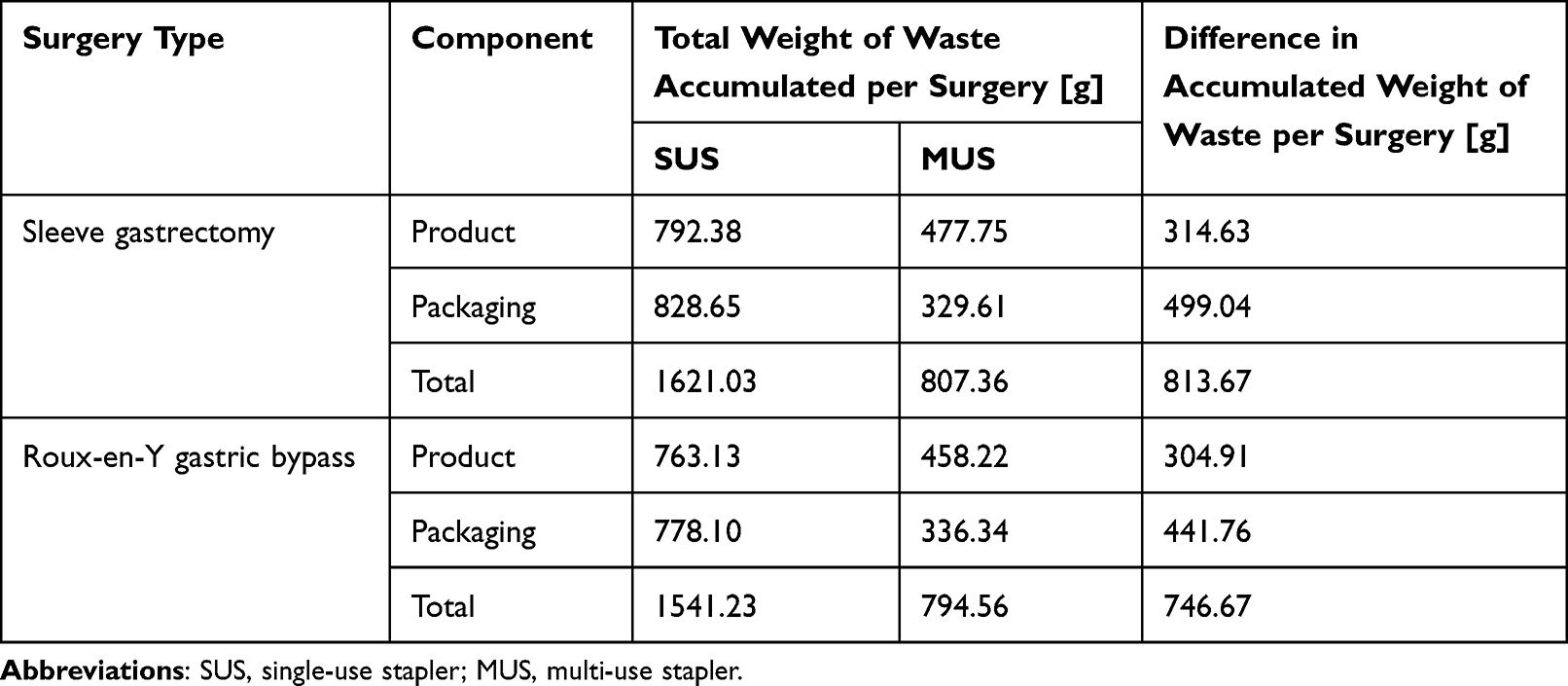 |
Table 5 Total Waste Generated per Surgery |
Total Material Requirement (TMR)
The TMR per surgery of MUS stapler cartridges (with and without preloaded buttressing) was substantially greater than that of the SUS stapler cartridges (Table 6). Despite the higher TMR, the MUS shows an overall reduction compared to the SUS due to the reusability of the most resource-intensive components. The TMR associated with one SG is reduced from 330 kg (SUS) to 30.9 kg (MUS). For RYGB, the TMR drops from 329 kg to 29.2 kg, respectively. In both procedures, the TMR is reduced by more than 90%, indicating that over 90% of raw material consumption can be saved by switching from SUS to MUS. The resource efficiency is increased by factor 11.
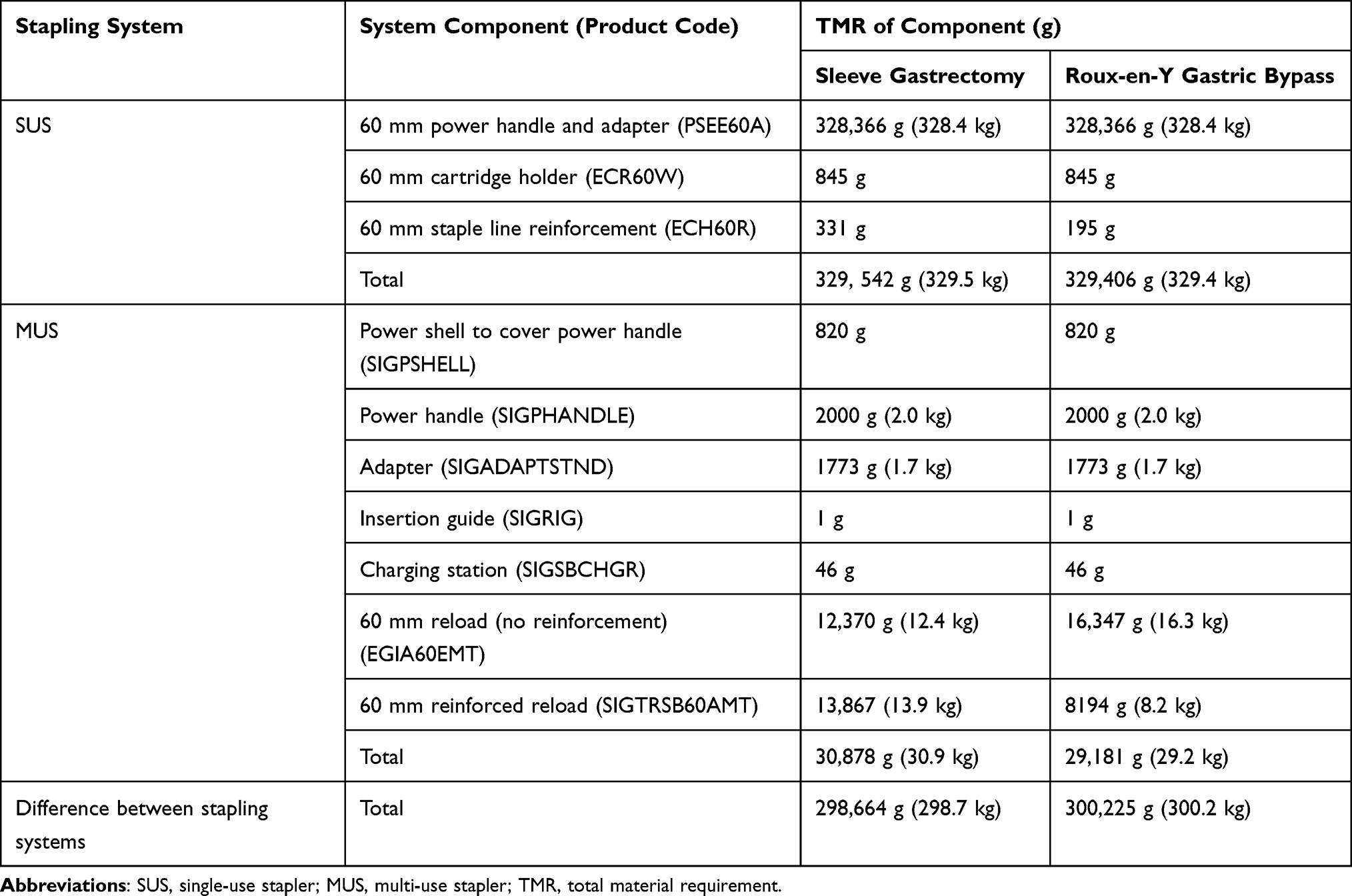 |
Table 6 Total Material Requirement per Stapling System and per Surgery |
Impact of Lithium in Power Supply
The impact on greenhouse gas emissions per surgical procedure was based on the lithium content of the stapler’s power supplies (Table 7). The MUS contains less lithium than the SUS, both in terms of relative content of the battery cells (MUS: 4.96%, SUS: 6.72%) and absolute mass (MUS: 0.348 g, SUS: 0.376 g). Due to this lower lithium content and the higher circulation rate of the MUS, its impact on greenhouse gas emissions per surgery at 0.018 g CO2eq is 324 times smaller than that of the SUS at 5.904 g CO2eq.
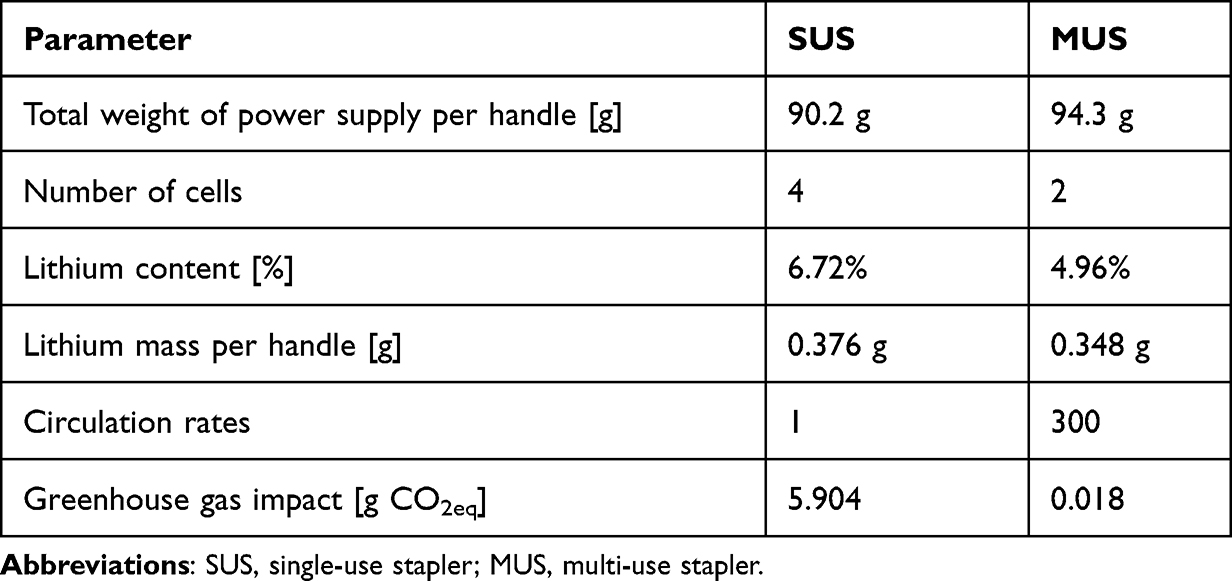 |
Table 7 Lithium Content of Stapler System Power Supplies and Its Impact on Greenhouse Gas Emission |
Sensitivity Analysis
Both surgery types use five 60 mm staple cartridges per surgery on average, the only difference is the number of cartridges that apply buttressing. In the sensitivity analysis, buttressing is either applied to none or all staple firings.
The sensitivity analysis (Table 8) shows that MUS generate less waste and have lower TMR than SUS regardless of the rate of buttressing applied. If buttressing is applied to all staple lines, the waste reduction offered by the MUS increases to 1,022.13 g (54.7%) from 649.88 g (45.6%) if no staple line reinforcement is used, as the waste created by the separate buttressing material and its packaging is avoided.
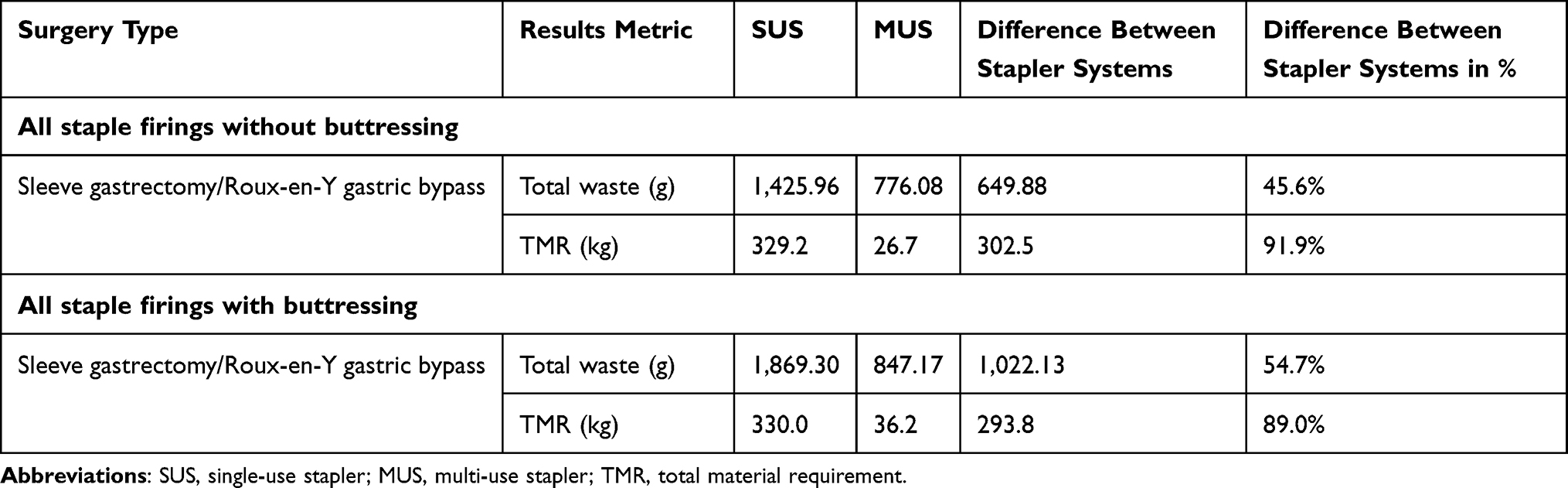 |
Table 8 Results of the Sensitivity Analysis |
The TMR results of the MUS showed a larger increase than those of the SUS if staple line reinforcement was applied at all stapler firings. This suggests that the resource consumption to create the preloaded buttressing may be higher than that needed to create the separate buttressing. As buttressing is only responsible for a very small part of the total TMR, however, this change does not noticeably affect the overall advantage provided by the MUS.
Discussion
Laparoscopic surgery can offer many benefits if it is applied in the interest of the patient as well as the operating surgeon.27 A laparoscopic approach to bariatric surgery has been shown to offer benefits compared to an open procedure,28,29 and often relies on stapling for tissue approximation. The use of buttressing to reinforce the staple line has been shown to reduce bleeding and leakage.16,17 However, the single-use staplers produce large amounts of waste, which can be addressed by using multi-use staplers.14,27
The results of our study show that preloaded buttressing reduces the amount of waste created by reinforcement per staple firing compared to separate buttressing. The preloaded buttressing is used with a MUS, whose reuse further reduces the environmental impact, whereas the separate buttressing is paired with the SUS. A previous study already showed that MUS compared to SUS substantially reduce the amount of waste and resource consumption per surgery.14 We confirmed these findings and showed an even larger reduction in OR waste by including packaging materials. Packaging waste has a large impact: more than half of the waste produced by SUS is from packaging. MUS reduced the contribution of packaging waste by approximately 60% and substantially reduced the impact of lithium in the power supply on greenhouse gas emission.
Similar to MUS, the reuse of other medical devices has repeatedly been reported to be more resource efficient, reduce waste, and have a lower environmental footprint than single-use options.14,15,30,31 However, most of these devices require reprocessing, and the efficiency of the reprocessing determines whether reusable devices are actually environmentally more sustainable.31 The handle of the MUS does not require reprocessing for reuse, as it is covered by the disposable power shell component during surgery.
In addition to the environmental benefits, MUS may also offer an economic benefit. A recent review estimated that the cost of waste contributed approximately 25% of healthcare spending in the US, and that interventions to reduce waste could lead to a 25% cost reduction with potential savings between USD 191–282 billion.32 Assuming disposal cost for hazardous medical waste of USD 3.93 per kg,33 the waste disposal for the SUS (55.2 kg per surgeon per month) would cost USD 217, whereas the waste created by the MUS (27.7 kg per surgeon per month) would cost USD 109 to dispose of.
A substantial part of the OR waste that is disposed of as regulated waste is actually general waste1,34 with lower disposal costs.33–35 At disposal costs of USD 1.14 per kg for general waste,33 separating OR waste may increase financial benefits.35 In our study, proper waste separation could reduce the costs of waste disposal per surgeon per month by 36.2% to USD 138 for SUS and by 29.3% to USD 77 for MUS.
During the life-cycle of a lithium-ion battery, the production phase has the highest impact on global warming.36 The greenhouse gas emissions caused by the production of lithium in SUS are 324 times higher than those of MUS. This is in line with the finding that reusable medical devices reduce their carbon footprint between 50% and 97% compared to disposable ones.37 The reuse of rechargeable lithium-ion batteries should be prioritized over recycling of primary batteries, as the recycling process at the end of the battery life still requires harsh chemical- and energy-intensive processes.36
Reducing, reusing, and recycling medical waste is not only beneficial for the environment38 but is also accompanied by a substantial financial incentive. Despite these clear advantages of green policies, our survey showed that they are not widely implemented. The MUS in this study showed a substantially reduced environmental impact regarding waste generation, resource consumption, and greenhouse gas emissions. Waste reduction furthermore decreases waste disposal costs. Finally, the preloaded buttressing does not require additional steps and/or materials to apply it in the OR, which is expected to save time and reduce handling errors during the operation.18
The promising results of this analysis have to be interpreted with its limitations in mind. First, this study only considered buttressing as staple line reinforcement. Oversewing is another commonly used method.16 However, its clinical effectiveness is controversial, with different studies coming to different conclusions.16,39,40 In contrast, buttressing was generally found to be effective in reducing bleeding and leaks in gastrointestinal surgery.16,40 Second, this study only considers one type of separate buttressing material. Other buttressing materials may cause different outcomes in the waste and TMR analyses. Third, we only considered one brand of MUS and SUS each, and only focused on 60 mm cartridges as these were most commonly used in bariatric surgery. Although these systems are used very frequently, we cannot exclude that an analysis of alternative staplers could lead to different results and conclusions. Therefore, the results presented here should be considered within the context of this study, and further investigation is necessary for generalized conclusions.
The costs of the stapling systems were not included in the analysis, even though survey respondents rated the price of the device as more likely to influence their purchasing decision than its environmental impact. Although MUS are likely to reduce the costs of waste disposal, their upfront purchase cost is expected to be higher than those of SUS. To fully explore the financial impact, a more in-depth life-cycle cost analysis is needed.
Finally, an assessment of the ecological impact caused by production, use, and disposal of all components of SUS and MUS in the form of a life-cycle analysis was outside the scope of this study. The present analysis did not consider the environmental impact of the cleaning and sterilization process that is required to safely reuse surgical instruments,15,41 the recycling process of lithium-ion batteries,36 or the reprocessing process that would make single-use items reusable.13 A complete life-cycle analysis of the stapling systems used in clinical practice would be needed to fully understand all relevant processes, environmental impacts, consumed resources, and waste streams. So far, only a life-cycle analysis of SUS but not MUS is available.41
Conclusion
This study presents evidence that reusable staplers produce less waste, require less resource input, and have a reduced impact on greenhouse gas emissions caused by their lithium content than single-use staplers in laparoscopic sleeve gastrectomy and laparoscopic gastric bypass procedures. In addition to product waste, packaging waste is substantially reduced by reusable staplers. Furthermore, buttressing that is pre-attached to the stapler reload was found to reduce the amount of waste per stapler firing that is added by staple line reinforcement in comparison to separate buttressing material.
Abbreviations
MUS, Multi-use stapler; OR, Operation room; RYGB, Roux-en-Y gastric bypass; SG, Sleeve gastrectomy; SLR, Staple Line Reinforcement; SUS, Single-use stapler; TMR, Total material requirement.
Acknowledgments
Acknowledgments to Wuppertal Institut für Klima, Umwelt, Energie gGmbH, Montanuniversität Leoben, and the University of Natural Resources and Life Sciences Vienna – Institute of Waste Management and Circular Economy for performing the material analysis and TMR analysis.
We further thank QualWorld (www.qual-world.com) for their support in recruiting the survey participants and performing the survey.
Funding
This study was supported by funding from Medtronic. pulswerk GmbH and Coreva Scientific GmbH & Co KG received consultancy fees from Medtronic for work related to this manuscript. Outside of providing funding, Medtronic was not involved in the study and in the development of this manuscript.
Disclosure
Rhodri Saunders is the founding director and owner of Coreva Scientific GmbH & Co KG and Ubong Silas and Juliane Hafermann are employees of Coreva Scientific GmbH & Co KG, which received consultancy fees from Medtronic for performing, analyzing, and communicating the work presented here. Markus Meissner is an associate member of the Austrian Institute of Ecology and an employee of pulswerk GmbH, the latter of which received consultancy fees from Medtronic for performing, analyzing, and communicating the work presented here. The authors report no other conflicts of interest in this work.
References
1. Wyssusek KH, Keys MT, van Zundert AAJ. Operating room greening initiatives - The old, the new, and the way forward: a narrative review. Waste Manag Res. 2019;37(1):3–19. doi:10.1177/0734242X18793937
2. Lenzen M, Malik A, Li M, et al. The environmental footprint of health care: a global assessment. Lancet Planet Health. 2020;4(7):e271–e279. doi:10.1016/S2542-5196(20)30121-2
3. Weisz U, Pichler -P-P, Jaccard IS, et al. Carbon emission trends and sustainability options in Austrian health care. Resour Conserv Recycl. 2020;160:104862. doi:10.1016/j.resconrec.2020.104862
4. World Health Organization. Alliance for transformative action on climate and health (ATACH): country commitments; 2023. Available from: https://www.who.int/initiatives/alliance-for-transformative-action-on-climate-and-health/country-commitments.
5. Pichler -P-P, Jaccard IS, Weisz U, Weisz H. International comparison of health care carbon footprints. Environ Res Lett. 2019;14(6):64004. doi:10.1088/1748-9326/ab19e1
6. Karliner J, Slotterback S, Boyd R, Ashby B, Steele K. Health care’s climate footprint report: how the health sector contributes to the global climate crisis and opportunities for action; 2019. Available from: https://noharm-europe.org/ClimateFootprintReport.
7. McGain F, Naylor C. Environmental sustainability in hospitals - a systematic review and research agenda. J Health Serv Res Policy. 2014;19(4):245–252. doi:10.1177/1355819614534836
8. Lee B-K, Ellenbecker MJ, Moure-Eraso R. Analyses of the recycling potential of medical plastic wastes. Waste Manag. 2002;22(5):461–470. doi:10.1016/S0956-053X(02)00006-5
9. Harding C, van Loon J, Moons I, de Win G, Du Bois E. Design opportunities to reduce waste in operating rooms. Sustainability. 2021;13(4):2207. doi:10.3390/su13042207
10. Chia WY, Ying Tang DY, Khoo KS, Kay Lup AN, Chew KW. Nature’s fight against plastic pollution: algae for plastic biodegradation and bioplastics production. Environ Sci Ecotechnol. 2020;4:100065. doi:10.1016/j.ese.2020.100065
11. Dharmaraj S, Ashokkumar V, Chew KW, Chia SR, Show PL, Ngamcharussrivichai C. Novel strategy in biohydrogen energy production from COVID - 19 plastic waste: a critical review. Int J Hydrogen Energy. 2021;47:42051–42074. doi:10.1016/j.ijhydene.2021.08.236
12. Davidson MG, Furlong RA, McManus MC. Developments in the life cycle assessment of chemical recycling of plastic waste – a review. J Clean Prod. 2021;293:126163. doi:10.1016/j.jclepro.2021.126163
13. Benedettini O. Green servitization in the single-use medical device industry: how device OEMs create supply chain circularity through reprocessing. Sustainability. 2022;14(19):12670. doi:10.3390/su141912670
14. Meissner M, Lichtnegger S, Gibson S, Saunders R. Evaluating the waste prevention potential of a multi- versus single-use surgical stapler. Risk Manag Healthc Policy. 2021;14:3911–3921. doi:10.2147/RMHP.S325017
15. Sherman JD, Raibley LA, Eckelman MJ. Life cycle assessment and costing methods for device procurement: comparing reusable and single-use disposable laryngoscopes. Anesth Analg. 2018;127(2):434–443. doi:10.1213/ANE.0000000000002683
16. Shikora SA, Mahoney CB. Clinical benefit of gastric staple line reinforcement (SLR) in Gastrointestinal surgery: a meta-analysis. Obes Surg. 2015;25(7):1133–1141. doi:10.1007/S11695-015-1703-X
17. Gagner M, Kemmeter P. Comparison of laparoscopic sleeve gastrectomy leak rates in five staple-line reinforcement options: a systematic review. Surg Endosc. 2020;34(1):396–407. doi:10.1007/S00464-019-06782-2
18. Shigeeda W, Deguchi H, Tomoyasu M, et al. The utility of the Stapler with PGA sheet for pulmonary wedge resection: a propensity score-matched analysis. J Thorac Dis. 2019;11(4):1546–1553. doi:10.21037/JTD.2019.03.05
19. Yamamoto S, Kanai T, Osumi K, et al. Anastomotic leakage using linear stapling device with pre-attached bioabsorbable polyglycolic acid felt after laparoscopic anterior resection. Anticancer Res. 2017;37(12):7083–7086. doi:10.21873/ANTICANRES.12181
20. Medtronic. R2146-1018 Signia™ Stapling System Useful Life; 2021.
21. Medtronic. Signia™ stapling system in-service guide; 2020.
22. Wagner B, Enzler S. Material Flow Management: Improving Cost Efficiency and Environmental Performance.
23. Ritthoff M, Rohn H, Liedtke C, Merten T. MIPS berechnen: Ressourcenproduktivität von Produkten und Dienstleistungen. Wuppertal: Wuppertal Institut für Klima, Umwelt, Energie. Wuppertal spezial; 2002. Available from: http://nbn-resolving.de/urn:nbn:de:101:1-20091006989.
24. Saurat M, Ritthoff M. Calculating MIPS 2.0. Resources. 2013;2(4):581–607. doi:10.3390/resources2040581
25. Jiang S, Zhang L, Li F, et al. Environmental impacts of lithium production showing the importance of primary data of upstream process in life-cycle assessment. J Environ Manage. 2020:262. doi:10.1016/j.jenvman.2020.110253
26. Hauschild MZ, Rosenbaum RK, Olsen SI, eds. Life Cycle Assessment: Theory and Practice.
27. Molnar TF. Dark side of the moon: the price to pay in minimally invasive thoracic surgery (MITS). Shanghai Chest. 2023;7:3. doi:10.21037/shc-22-29
28. Aiolfi A, Tornese S, Bonitta G, Rausa E, Micheletto G, Bona D. Roux-en-Y gastric bypass: systematic review and Bayesian network meta-analysis comparing open, laparoscopic, and robotic approach. Surg Obes Relat Dis. 2019;15(6):985–994. doi:10.1016/j.soard.2019.03.006
29. Weller WE, Rosati C. Comparing outcomes of laparoscopic versus open bariatric surgery. Ann Surg. 2008;248(1):10–15. doi:10.1097/SLA.0b013e31816d953a
30. Eckelman M, Mosher M, Gonzalez A, Sherman J. Comparative life cycle assessment of disposable and reusable laryngeal mask airways. Anesth Analg. 2012;114(5):1067–1072. doi:10.1213/ANE.0b013e31824f6959
31. Perry H, Reeves N, Ansell J, et al. Innovations towards achieving environmentally sustainable operating theatres: a systematic review. Surgeon. 2023;21(3):141–151. doi:10.1016/j.surge.2022.04.012
32. Shrank WH, Rogstad TL, Parekh N. Waste in the US health care system: estimated costs and potential for savings. JAMA. 2019;322(15):1501–1509. doi:10.1001/jama.2019.13978
33. Vaccari M, Tudor T, Perteghella A. Costs associated with the management of waste from healthcare facilities: an analysis at national and site level. Waste Manag Res. 2018;36(1):39–47. doi:10.1177/0734242X17739968
34. Wormer BA, Augenstein VA, Carpenter CL, et al. The green operating room: simple changes to reduce cost and our carbon footprint. Am Surg. 2013;79(7):666–671. doi:10.1177/000313481307900708
35. Kwakye G, Brat GA, Makary MA. Green surgical practices for health care. Arch Surg. 2011;146(2):131–136. doi:10.1001/archsurg.2010.343
36. Alipanah M, Saha AK, Vahidi E, Jin H. Value recovery from spent lithium-ion batteries: a review on technologies, environmental impacts, economics, and supply chain. CTR. 2021;1(2):152–184. doi:10.3934/ctr.2021008
37. Rizan C, Steinbach I, Nicholson R, Lillywhite R, Reed M, Bhutta MF. The carbon footprint of surgical operations: a systematic review. Ann Surg. 2020;272(6):986–995. doi:10.1097/SLA.0000000000003951
38. Kagoma YK, Stall N, Rubinstein E, Naudie D. People, planet and profits: the case for greening operating rooms. CMAJ. 2012;184(17):1905–1911. doi:10.1503/cmaj.112139
39. Wu C, Wang FG, Yan WM, Yan M, Song MM. Is there necessity for oversewing the staple line during laparoscopic sleeve gastrectomy? An updated systematic review and meta-analysis of randomized controlled trials. J Invest Surg. 2020;33(9):839–850. doi:10.1080/08941939.2019.1665380
40. Wang Z, Dai X, Xie H, Feng J, Li Z, Lu Q. The efficacy of staple line reinforcement during laparoscopic sleeve gastrectomy: a meta-analysis of randomized controlled trials. Int J Surg. 2016;25:145–152. doi:10.1016/J.IJSU.2015.12.007
41. Freund J, Gast K, Zuegge K, Hicks A. Environmental considerations in the selection of medical staplers: a comparative life cycle assessment. J Clean Prod. 2022;371:133490. doi:10.1016/j.jclepro.2022.133490
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Life Cycle Assessment Between Single-Use and Reprocessed IPC Sleeves
Lichtnegger S, Meissner M, Paolini F, Veloz A, Saunders R
Risk Management and Healthcare Policy 2023, 16:2715-2726
Published Date: 13 December 2023