Back to Journals » Nature and Science of Sleep » Volume 17

Association Between Dietary Magnesium Intake and Sleep Quality in Saudi University Students: A Cross-Sectional Study
Authors Alshammari AA ![]() , Alsawad KA, Ahmed NK, Alsaadi R, Alholieli RS, Alsaif S, Al Mulhim NS
, Alsawad KA, Ahmed NK, Alsaadi R, Alholieli RS, Alsaif S, Al Mulhim NS ![]() , Rafique N
, Rafique N ![]() , Al Ghamdi K
, Al Ghamdi K ![]() , ALQarni AS, Al-Hariri M
, ALQarni AS, Al-Hariri M ![]()
Received 24 September 2025
Accepted for publication 2 December 2025
Published 16 December 2025 Volume 2025:17 Pages 3127—3136
DOI https://doi.org/10.2147/NSS.S569883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Asma Ahmed Alshammari,1 Kawthar Abdullah Alsawad,1 Noorah Khalid Ahmed,1 Rahaf Alsaadi,1 Rawan Saeed Alholieli,1 Seham Alsaif,1 Noura Saad Al Mulhim,1 Nazish Rafique,1 Kholoud Al Ghamdi,1 Abdullah S ALQarni,2 Mohammed Al-Hariri1
1Department of Physiology, Collage of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Respiratory Care Department, Collage of Applied Medical Sciences, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
Correspondence: Mohammed Al-Hariri, Department of Physiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Eastern Province, Saudi Arabia, Email [email protected]
Purpose: Background: Sleep is essential for both physical and cognitive functioning. Magnesium, a vital mineral, plays a key role in sleep regulation. Adequate sleep and sufficient magnesium intake are critical for university students’ overall well-being, academic performance, and long-term health. This study aimed to investigate the association between dietary magnesium intake and sleep quality in university students in Saudi Arabia.
Methods: An analytic cross-sectional study was conducted using an electronic questionnaire distributed to 1206 university students in the Eastern Province of Saudi Arabia via social media. Data were collected from December 2023 to March 2024 over a 3-month period. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), and magnesium intake was evaluated using a magnesium food frequency questionnaire (MgFFQ).
Results: Of 1206 participants, 305 met the inclusion criteria, of which 69% were female. A significant association was observed between shorter sleep duration (< 5 h) and lower monthly magnesium intake (p = 0.008). Daytime dysfunction was also significantly associated with a low monthly magnesium intake (p = 0.009). The median PSQI score was significantly higher in females than males (p = 0.038).
Conclusion: Higher dietary magnesium intake was associated with better sleep quality, longer sleep duration, and reduced daytime dysfunction, highlighting the potential benefits of magnesium-rich diets for sleep health. Importantly, a significant sex disparity was observed in this university cohort, where females demonstrated poorer sleep quality than males. Therefore, dietary awareness programs that promote magnesium-rich food sources should be incorporated into student health initiatives to support improved sleep quality.
Keywords: sleep quality, magnesium, students, Pittsburgh sleep quality index, gender disparity
Introduction
Sleep is a fundamental physiological process that is essential for physical restoration and mental health. High-quality sleep is characterized by adequate duration, continuity, and restorative properties, whereas poor sleep can impair immune function and increase the risk of chronic diseases. A recent global systematic review reported a poor sleep quality rate of ~40% among community-dwelling adults.1 The prevalence in Spain was found to be 38.2%,2 while in Thailand a study among older adults reported a rate of approximately 44.0%3 These values emphasize the high and relatively stable burden of poor sleep quality across diverse international settings.
Adequate sleep is increasingly being recognized as the cornerstone of physical recovery and psychological well-being. Restorative sleep, characterized by sufficient duration, stability, and depth, supports immune competence, metabolic balance, and healthy cognitive performance. In contrast, inadequate or fragmented sleep has been linked to dysregulated immune activity, greater vulnerability to infections, and a higher risk of long-term conditions such as cardiovascular disease, diabetes, and mood disorders.4 Recent investigations further show that disturbed sleep modifies immune cell profiles and cytokine secretion, promoting persistent low-grade inflammation that may accelerate chronic illness.5,6
In Saudi Arabia, 72.5% of 433 primary healthcare visitors in Al-Ahsa reported poor sleep, with the highest prevalence (81.7%) among those aged 18–28 years.7 Similarly, and 75.93% of students exhibited poor sleep quality. Lower grade point averages (GPAs) were associated with higher PSQI scores, suggesting a link between sleep quality and academic performance.8
Magnesium (Mg) is an essential micronutrient involved in over 300 enzymatic reactions, including those related to energy metabolism, protein synthesis, glucose regulation, and neuromuscular function. A recent systematic review found that magnesium supplementation is associated with lowered levels of inflammatory biomarkers (eg, hs-CRP and IL-1), improved lipid profiles, enhanced glycemic control, and reduced blood pressure, especially in populations with metabolic or cardiovascular risk.9
Mg intake has been linked to better endothelium-dependent vasodilation, favorable alterations in lipid metabolism, and lower odds of hypertension and dyslipidemia.10 Diets rich in magnesium (leafy greens, legumes, seeds, whole grains, nuts) also correlate inversely with the risk of osteoporosis, especially in older adults, when magnesium depletion is taken into account.11 Thus, maintaining sufficient magnesium status through diet or supplementation where needed may help in the prevention of metabolic disorders, bone demineralization, and inflammation.
Subclinical hypomagnesemia, characterized by suboptimal Mg levels, often goes undiagnosed because of nonspecific symptoms and can disrupt circadian rhythms, neuromuscular function, cardiovascular health, and metabolism. It is associated with chronic conditions such as type 2 diabetes and hypertension, underscoring the importance of dietary or supplemental Mg to mitigate long-term health risks.12
Mg facilitates sleep through multiple mechanisms, including the activation of glutamatergic and gamma-aminobutyric acid (GABA) systems, inhibition of N-methyl-D-aspartate (NMDA) receptors for muscle relaxation, and reduction of stress biomarkers, thereby decreasing nervous system excitability.13 Additionally, Mg enhances melatonin secretion, supporting circadian regulation, and alleviating insomnia symptoms.13
Emerging evidence indicates that sleep quality is not uniform between sexes in university students, with females consistently reporting poorer sleep and more frequent insomnia symptoms than males, including within Saudi Arabia,8 however, few studies have examined the role of specific micronutrients. Recent findings point to an emerging issue of insufficient magnesium intake among younger populations in Saudi Arabia.14 This deficiency appears to be associated with the growing reliance on modern dietary patterns, particularly those dominated by refined carbohydrates, sugars, and processed foods.14 In this context, limited research has been conducted in Saudi Arabia, particularly among university students. This study addresses this gap by examining the association between dietary magnesium intake and sleep quality in a university setting.
Material and Methods
This analytic cross-sectional study targeted students at Imam Abdulrahman Bin Faisal University (IAU), Saudi Arabia. An electronic, self-administered questionnaire was distributed via social media platforms between December 2023 and March 2024.
The Pittsburgh Sleep Quality Index (PSQI) is a validated tool for assessing sleep quality over the preceding month.15 The questionnaire comprised three sections: (1) demographic information, medical or psychiatric history, supplement/drug use, and pregnancy status; (2) sleep quality assessment using the PSQI, which includes seven components—subjective sleep quality, sleep latency, duration, efficiency, disturbances, medication use, and daytime dysfunction—scored from 0 to 3, yielding a global score of 0–21 (scores >5 indicate poor sleep quality);15 and (3) magnesium intake evaluation via the MgFFQ, a self-reported tool estimating daily, weekly, and monthly Mg consumption across 33 items.16
Sleep latency was categorized according to the PSQI scoring criteria: No delay: sleep latency ≤ 15 minutes; Mild delay: 16–30 minutes; Moderate delay: 31–60 minutes; and Severe delay: > 60 minutes.
The inclusion criterion was healthy students aged 18–25 years with a body mass index (BMI) of 20–25 kg/m2. This study intentionally restricted the BMI range (20–25 kg/m2) to minimize adiposity-related confounding, as overweight and obesity are known to be independently associated with altered sleep architecture and poorer nocturnal restoration.17
Exclusion criteria included BMI ≥26 kg/m2, chronic diseases, sleep disorders, pregnancy, neurological or psychiatric conditions, and use of medications or supplements affecting Mg levels or sleep (eg, central nervous system drugs, Zinc, L-tryptophan, or melatonin) within the previous two weeks.
Sample size estimation was conducted using a single-population proportion formula based on an assumed prevalence of poor sleep quality among university students of approximately 30%–40% reported in previous literature,18 a 95% confidence level, and a 5% margin of error. This calculation indicated that a minimum sample of approximately 289 participants was required to achieve adequate statistical power for cross-sectional comparison.
A convenience sampling technique was employed to recruit participants. Of the 1,206 initial responses, 709 were completed. Out of the initial 709 participants surveyed, 305 met the inclusion criteria, while the remaining 404 participants were excluded for various reasons. Specifically, 167 participants reported chronic diseases such as diabetes mellitus or hypertension; additional exclusions were made for individuals with diagnosed sleep disorders or those taking sleeping pills during the preceding two weeks. Furthermore, 237 participants were excluded due to being overweight or obese (Body Mass Index [BMI] >25 kg/m2) as showed in Figure 1.
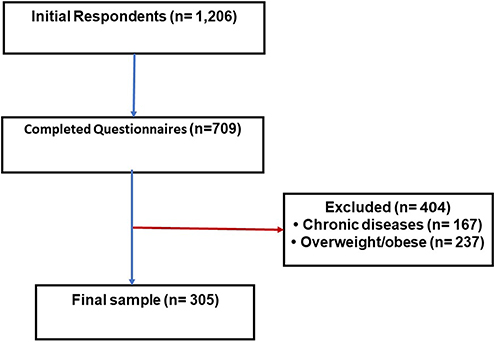 |
Figure 1 Participants flow diagram. |
The accuracy of self-reported variables such as BMI was ensured by using standard measurement units and posing clear, direct questions within the questionnaire. Participants were explicitly instructed to report their height in centimeters and weight in kilograms, which minimized confusion and enhanced consistency across responses. Moreover, as the participants were university students, they were generally educated and health-aware, and most routinely measured their height and weight during regular health checkup campaigns organized by the university. These measures collectively improved the reliability of the self-reported anthropometric data used to calculate BMI.
Informed consent was obtained electronically before beginning the study. Participants were presented with clear instructions outlining the study’s purpose and procedures. They were required to read this information thoroughly and then indicate their agreement by selecting agree to participate in this study. Institutional review board (IRB) approval was obtained for this study from Imam Abdulrahman Bin Faisal University (IRB #: IRB-UGS-2024-01-880). The questionnaire was distributed by data collectors and the data were stored on a secure platform. All procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Pilot Study
A pilot study involving 116 male and female participants was conducted online to assess the questionnaire’s validity and reliability. Validity was evaluated using item-total correlations and reliability was evaluated using Cronbach’s alpha. The MgFFQ demonstrated high validity (correlation coefficients were significant at p < 0.01) and reliability (Cronbach’s alpha = 0.906 for monthly magnesium consumption).
Data Analysis
Data were analyzed using IBM SPSS Statistics version 25, with statistical significance defined at p < 0.05. The independent variables included the frequency of dietary magnesium intake (daily, weekly, monthly) obtained from the MgFFQ, while the dependent variables were the PSQI global score and its seven domains (subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, medication use, and daytime dysfunction). Potential demographic confounding was examined by testing associations between participant characteristics (academic year, age, BMI, marital status) and sleep outcomes. Normality of continuous variables was assessed using the Shapiro–Wilk test, which demonstrated that most sleep quality sub-scores were non-normally distributed. Therefore, non-parametric methods were used. Descriptive statistics are reported as median (minimum–maximum) for skewed variables, while categorical variables are presented as frequencies and percentages. Pearson’s correlation was used to examine bivariate associations. For inferential analysis, Mann–Whitney U-tests were used for two-group comparisons and Kruskal–Wallis tests for comparisons across three or more groups, followed by Bonferroni-adjusted post-hoc tests when appropriate. This analysis strategy was selected a priori due to the non-normality of outcomes and to avoid unstable multivariable models given the number of categorical covariates relative to sample size. Stratified non-parametric comparisons allowed us to examine group differences while minimizing model overfitting.
Results
Basic Participant Features
The study included 305 participants (69.2% female; mean age 21.4 ± 1.8 years; mean BMI 20.7 ± 2.5 kg/m2). Analysis of sleep duration and daytime dysfunction scores across demographic categories including academic year, age group, BMI classification, and marital status revealed no statistically significant differences in any of the comparisons as presented in Table 1. Although minor variations in median and mean values were observed between subgroups, none of the Kruskal–Wallis tests reached statistical significance for either sleep duration or daytime dysfunction (all p > 0.05). The borderline trend noted for sleep duration across academic years (H=11.04, p=0.051) did not meet the threshold for significance. Overall, these findings indicate that sleep duration and daytime dysfunction did not differ meaningfully across the demographic variables examined, suggesting that these sleep components were relatively stable and not influenced by students’ academic level, age, BMI, or marital status. This validates our univariate analytical approach and strengthens confidence in findings (Table 1). Based on PSQI scores, 63% of the participants exhibited poor sleep quality. Descriptive statistics for PSQI and MgFFQ are presented in Table 2.
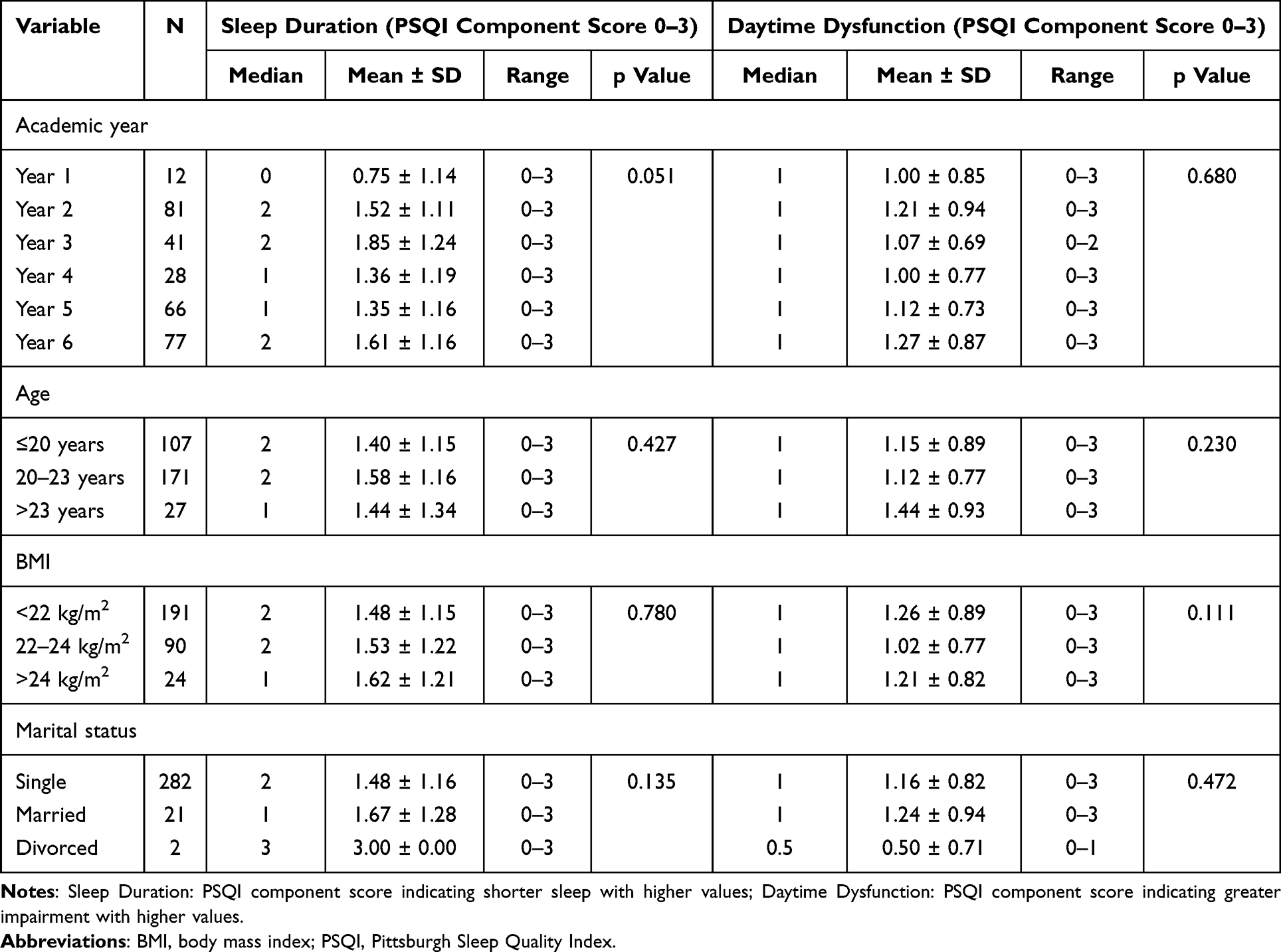 |
Table 1 Sleep Duration and Daytime Dysfunction by Demographic Characteristics |
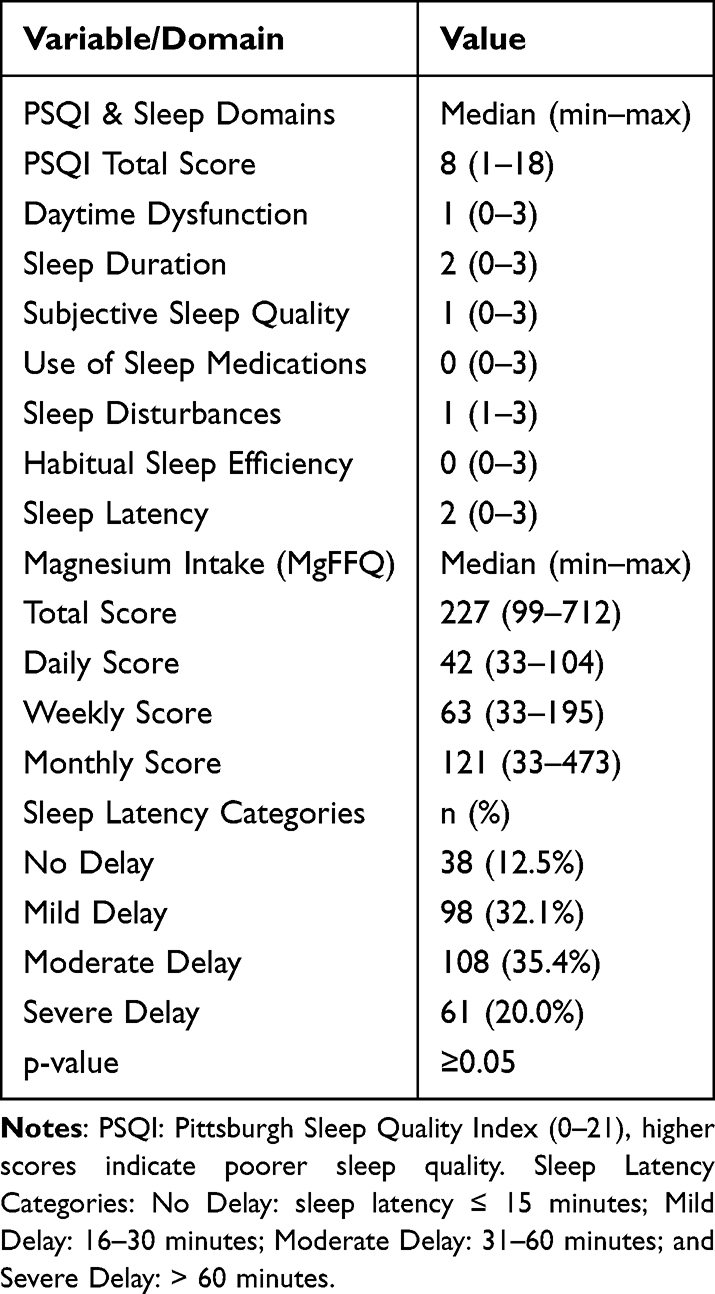 |
Table 2 Sleep Measures, Magnesium Intake Scores, and Sleep Latency Categories |
Association Between PSQI Domains and Monthly Mg Intake
Daytime dysfunction (categorized as 0–3, with 3 indicating the worst) was significantly associated with lower monthly Mg intake (Kruskal–Wallis H(3) = 11.57, p = 0.009), with the highest dysfunction linked to the lowest Mg scores (Figure 2). Post-hoc analysis (Mann–Whitney with Bonferroni correction, p = 0.0167) revealed significant differences between categories 0 and 2 (p = 0.001).
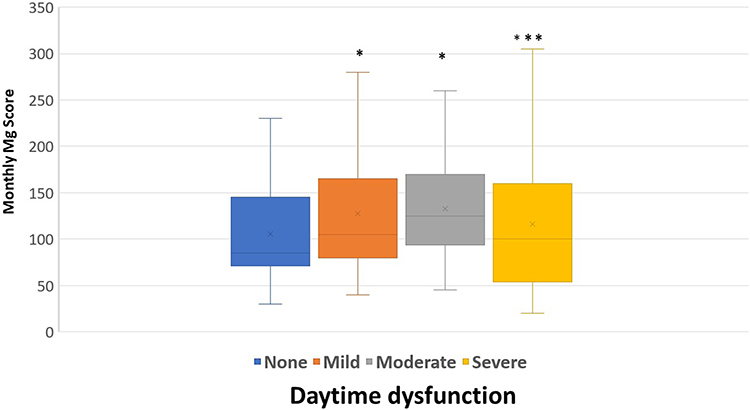 |
Figure 2 Association between monthly magnesium intake score and daytime dysfunction. *: p<0.05; ***: significantly worse daytime dysfunction in participants with the lowest magnesium scores; X: mean value. |
Association Between Sleep Duration and Monthly Mg Intake
Sleep duration (categorized as 0–3, with 3 indicating <5 h) was significantly associated with lower monthly Mg intake (H(3) = 11.75, p = 0.008), with the shortest duration linked to the lowest Mg scores (Figure 3). Post-hoc analysis showed differences between 0 and 3 (p = 0.002), 1 and 3 (p = 0.002), and 2 and 3 (p = 0.006). Other PSQI domains (efficiency, and disturbances) were not significantly associated with monthly Mg intake (P >0.05).
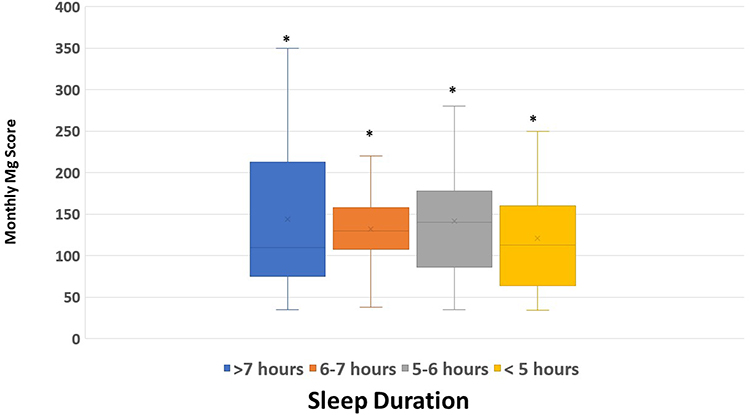 |
Figure 3 Association between monthly magnesium intake score and sleep duration. *: p<0.05; X: mean value. |
Sex Differences
No significant difference in Mg intake was found between males and females (Mann–Whitney test, p > 0.05). However, females had a higher median PSQI rank (159.9) than males (137.4; p = 0.038). Among poor sleepers (PSQI >5), females had lower Mg scores than males, the difference was not statistically significant (Figure 4).
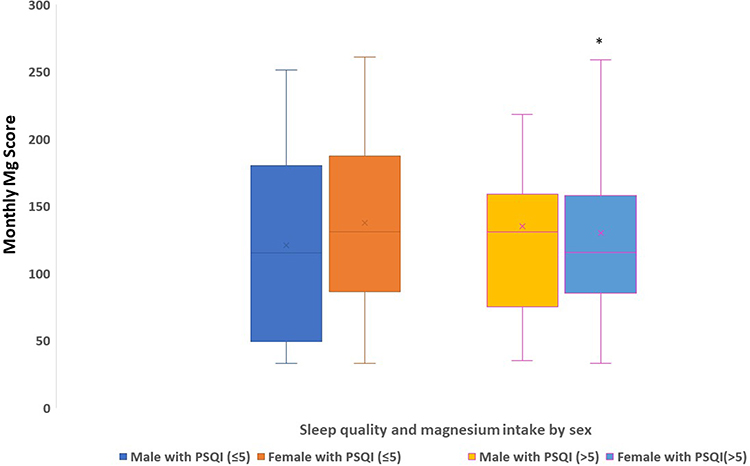 |
Figure 4 Association between monthly magnesium intake score and Pittsburgh Sleep Quality Index scores, stratified by sex. *: p<0.05; X: mean value. Abbreviation: PSQI, Pittsburgh Sleep Quality Index. |
Sleep Latency
For sleep latency (Table 2), most participants fell within the moderate (35.4%) and mild (32.1%) categories, while 12.5% reported no delay and 20.0% reported severe delay. Dietary magnesium intake was not significantly associated with sleep latency (p > 0.05).
Discussion
The findings of this study highlight a significant relationship between low dietary magnesium intake and poor sleep quality parameters, particularly daytime dysfunction and shorter sleep duration among Saudi university students. Furthermore, the higher PSQI scores observed among females suggest a potential sex disparity in sleep quality, with women being more vulnerable to the adverse effects of inadequate magnesium intake.
The absence of significant differences in sleep duration and daytime dysfunction across demographic groups in this study may be largely attributable to the relative homogeneity of the sample. All participants were drawn from the same university environment, sharing similar academic pressures, lifestyle patterns, and socio-cultural backgrounds. Such uniformity reduces between group variability and limits the ability to detect demographic influences on sleep outcomes.
Participants reported low Mg intake, consistent with other studies showing intake below the recommended daily allowances (RDAs).14,19 Lower monthly Mg intake was associated with poorer sleep quality (PSQI >5), suggesting that dietary Mg insufficiency may contribute to sleep issues.
Our finding that female participants exhibited both poorer sleep quality and lower magnesium intake than males align with several prior investigations and warrants closer consideration of hormonal and behavioral mechanisms. For example, Cao et al found that among Chinese adults, higher dietary magnesium intake was significantly associated with a decreased likelihood of daytime falling asleep only in women, suggesting that magnesium status may interact with female-specific physiology to affect sleep symptoms.20 Recently, Mazza et al (2025) reported that hormonal fluctuations, especially changes in estrogen, can influence magnesium absorption, distribution, and retention, potentially altering sleep-relevant metabolic processes.10 Taken together, these findings suggest that in our cohort, the observed sex differences may stem not only from disparities in dietary intake but also from fluctuations in sex hormones that influence sleep regulation, possibly via effects on circadian rhythms, thermoregulation, and neurotransmitter or mineral metabolism.
Shorter sleep duration was correlated with lower Mg intake, supported by cohort studies showing higher Mg linked to ≥7 h of sleep,13 supplementation improving sleep time and efficiency,21 and higher serum Mg in longer sleepers.22 Mechanisms include GABA/glutamatergic regulation, melatonin production,23 and cortisol reduction.24
Daytime dysfunction is associated with low Mg levels, consistent with links to sleepiness, anxiety, and fatigue.25 It modulates NMDA, GABA, melatonin, renin, and cortisol levels, with deficiencies causing electrolyte imbalances.26,27 Thus, Mg supplementation may enhance daytime function, mood, and productivity.28
In the current study, sleep latency showed no significant association with Mg intake, in contrast with some systematic reviews and clinical trials reporting modest improvements in sleep onset following magnesium supplementation.29 Conversely, other investigations, including those exploring Mg status in patients with RLS, have failed to demonstrate a clear link between magnesium and sleep quality.30 Such inconsistencies across the literature may be attributable to differences in study design, sample size, duration of intervention, and the bioavailability of Mg formulations used. A notable strength of this study is the inclusion of a large and diverse sample, which enhances the external validity and generalizability of the findings. Furthermore, the use of validated instruments, such as the PSQI and MgFFQ, provided a comprehensive assessment of both sleep and dietary Mg intake, while sex-stratified analyses offered additional depth to the interpretation.
Conclusion
These results underscore the importance of nutritional factors, particularly magnesium consumption, in maintaining optimal sleep among university students. Our findings demonstrated that lower dietary Mg intake is associated with reduced sleep duration, poor sleep quality, and increased daytime dysfunction. Importantly, a significant sex disparity was observed in this university cohort, where females demonstrated poorer sleep quality than males. These findings emphasize the role of Mg-rich diets in promoting optimal sleep and overall health. Our study extends the literature by highlighting Mg as a potential dietary factor underlying sleep problems in this population, suggesting that nutritional interventions aimed at improving Mg intake may help ameliorate sleep disturbances and improve health outcomes.
Recommendation
Based on the observed associations, it is recommended that greater awareness of Mg-rich dietary sources be promoted as part of student health initiatives to improve sleep quality. Future longitudinal and interventional studies are required to clarify the causal relationship between magnesium intake and sleep disturbances, including the potential benefits of magnesium supplementation. Integrating nutritional guidance with broader sleep hygiene education may provide a comprehensive approach to enhancing students’ overall well-being.
Data Sharing Statement
Data supporting the findings of this study are available upon request from the corresponding author.
Ethics
Institutional review board (IRB) approval was obtained for this study (IRB #: IRB-UGS-2024-01-880). Informed consent was obtained electronically before beginning the study. Participants were presented with clear instructions outlining the study’s purpose and procedures. They were required to read this information thoroughly and then indicate their agreement by selecting agree to participate in this study.
Author Contributions
Asma Ahmed Alshammari, Kawthar Abdullah Alsawad, Noorah Khalid Ahmed, Rahaf Marhoom Alsaadi, and Rawan Saeed Alholieli contributed to data curation, formal analysis, investigation, and writing – original draft preparation. Seham Sulaiman Alsaif and Noura Saad Khalifa Al Mulhim were responsible for methodology, validation, and writing – review and editing. Nazish Rafique and Kholoud Saad A. AlGhamdi contributed to visualization, resources, and writing – review and editing. Abdullah AlQarni contributed to supervision, project administration, formal analysis, and writing – review and editing. Mohammed Al-Hariri was responsible for overall supervision, formal analysis, validation, writing – review and editing. All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article has been submitted; reviewed and agreed on all versions of the article before submission, during revision, and the final version accepted for publication.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Canever JB, Zurman G, Vogel F, et al. Worldwide prevalence of sleep problems in community-dwelling older adults: a systematic review and meta-analysis. Sleep Med. 2024;119:118–134. doi:10.1016/j.sleep.2024.03.040
2. Madrid-Valero JJ, Martínez-Selva JM, Ribeiro Do Couto B, Sánchez-Romera JF, Ordoñana JR. Age and gender effects on the prevalence of poor sleep quality in the adult population. Gac Sanit. 2017;31(1):18–22. doi:10.1016/j.gaceta.2016.05.013
3. Thichumpa W, Howteerakul N, Suwannapong N, Tantrakul V. Sleep quality and associated factors among the elderly living in rural Chiang Rai, northern Thailand. Epidemiol Health. 2018;40:e2018018. doi:10.4178/epih.e2018018
4. Irwin MR, Opp MR. Sleep Health: reciprocal Regulation of Sleep and Innate Immunity. Neuropsychopharmacology. 2017;42(1):129–155. doi:10.1038/npp.2016.148
5. Liu X, Chen B, Huang Z, et al. Effects of poor sleep on the immune cell landscape as assessed by single-cell analysis. Commun Biol. 2021;4(1):1325. doi:10.1038/s42003-021-02859-8
6. Alves S, Silva F, Esteves F, et al. The Impact of Sleep on Haematological Parameters in Firefighters. Clocks Sleep. 2024;6(3):291–311. doi:10.3390/clockssleep6030021
7. Albinsaleh AA, Al Wael WM, Nouri MM, Alfayez AM, Alnasser MH, Alramadan MJ. Prevalence and Factors Associated With Poor Sleep Quality Among Visitors of Primary Healthcare Centers in Al-Ahsa, Kingdom of Saudi Arabia: an Analytical Cross-Sectional Study. Cureus. 2023;15(7):e42653. doi:10.7759/cureus.42653
8. Almojali AI, Almalki SA, Alothman AS, Masuadi EM, Alaqeel MK. The prevalence and association of stress with sleep quality among medical students. J Epidemiol Glob Health. 2017;7(3):169–174. doi:10.1016/j.jegh.2017.04.005
9. Cepeda V, Ródenas-Munar M, García S, Bouzas C, Tur JA. Unlocking the Power of Magnesium: a Systematic Review and Meta-Analysis Regarding Its Role in Oxidative Stress and Inflammation. Antioxidants. 2025;14(6):740. doi:10.3390/antiox14060740
10. Mazza E, Maurotti S, Ferro Y, et al. Magnesium: exploring Gender Differences in Its Health Impact and Dietary Intake. Nutrients. 2025;17(13):2226. doi:10.3390/nu17132226
11. Wang J, Xing F, Sheng N, Xiang Z. Associations of the Dietary Magnesium Intake and Magnesium Depletion Score With Osteoporosis Among American Adults: data From the National Health and Nutrition Examination Survey. Front Nutr. 2022;9:883264. doi:10.3389/fnut.2022.883264
12. Gröber U, Schmidt J, Kisters K. Magnesium in Prevention and Therapy. Nutrients. 2015;7(9):8199–8226. doi:10.3390/nu7095388
13. Zhang Y, Chen C, Lu L, et al. Association of magnesium intake with sleep duration and sleep quality: findings from the CARDIA study. Sleep. 2022;45(4):zsab276. doi:10.1093/sleep/zsab276
14. Abualrahi AM, Alhanabi FH, Alalloush RS, et al. Assessment of dietary magnesium intake in the Eastern Province of Saudi Arabia. J Med Life. 2023;16(12):1789–1795. doi:10.25122/jml-2023-0279
15. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
16. Sukumar D, DeLuccia R, Cheung M, Ramadoss R, Ng T, Lamoureux A. Validation of a Newly Developed Food Frequency Questionnaire to Assess Dietary Intakes of Magnesium. Nutrients. 2019;11(11):2789. doi:10.3390/nu11112789
17. T S, L L, A D, Y T, M E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004;1(3). doi:10.1371/journal.pmed.0010062
18. Al Shammari MA, Al Amer NA, Al Mulhim SN, Al Mohammedsaleh HN, AlOmar RS. The quality of sleep and daytime sleepiness and their association with academic achievement of medical students in the eastern province of Saudi Arabia. J Family Community Med. 2020;27(2):97–102. doi:10.4103/jfcm.JFCM_160_19
19. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala NB. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. 2012;35(8):1173–1181. doi:10.5665/sleep.2012
20. Cao Y, Zhen S, Taylor AW, Appleton S, Atlantis E, Shi Z. Magnesium Intake and Sleep Disorder Symptoms: findings from the Jiangsu Nutrition Study of Chinese Adults at Five-Year Follow-Up. Nutrients. 2018;10(10):1354. doi:10.3390/nu10101354
21. Rondanelli M, Opizzi A, Monteferrario F, Antoniello N, Manni R, Klersy C. The effect of melatonin, magnesium, and zinc on primary insomnia in long-term care facility residents in Italy: a double-blind, placebo-controlled clinical trial. J Am Geriatr Soc. 2011;59(1):82–90. doi:10.1111/j.1532-5415.2010.03232.x
22. Dhillon VS, Deo P, Thomas P, Fenech M. Low Magnesium in Conjunction with High Homocysteine and Less Sleep Accelerates Telomere Attrition in Healthy Elderly Australian. Int J Mol Sci. 2023;24(2):982. doi:10.3390/ijms24020982
23. Watanabe M, Maemura K, Kanbara K, Tamayama T, Hayasaki H. GABA and GABA receptors in the central nervous system and other organs. Int Rev Cytol. 2002;213:1–47. doi:10.1016/s0074-7696(02)13011-7
24. Petrović J, Stanić D, Mirković D, et al. P.1.e.018 - Effects of long-term magnesium administration on levels of stress hormones and interleukin-6 after acute stress in rats chronically treated with adrenocorticotropic hormone. Eur Neuropsychopharmacol. 2016;26:S207. doi:10.1016/S0924-977X(16)31053-7
25. Tunc M, Soysal P, Pasin O, et al. Hypomagnesemia Is Associated with Excessive Daytime Sleepiness, but Not Insomnia, in Older Adults. Nutrients. 2023;15(11):2467. doi:10.3390/nu15112467
26. Murck H. Magnesium and affective disorders. Nutr Neurosci. 2002;5(6):375–389. doi:10.1080/1028415021000039194
27. Nielsen F. Relation between Magnesium Deficiency and Sleep Disorders and Associated Pathological Changes. Modulation Sleep Obesity Diabet. 2015;291–296. doi:10.1016/B978-0-12-420168-2.00031-4
28. Hausenblas HA, Lynch T, Hooper S, Shrestha A, Rosendale D, Gu J. Magnesium-L-threonate improves sleep quality and daytime functioning in adults with self-reported sleep problems: a randomized controlled trial. Sleep Med X. 2024;8:100121. doi:10.1016/j.sleepx.2024.100121
29. Mah J, Pitre T. Oral magnesium supplementation for insomnia in older adults: a Systematic Review & Meta-Analysis. BMC Complement Med Ther. 2021;21(1):125. doi:10.1186/s12906-021-03297-z
30. Gade K, Blaschke S, Rodenbeck A, Becker A, Anderson-Schmidt H, Cohrs S. Uremic restless legs syndrome (RLS) and sleep quality in patients with end-stage renal disease on hemodialysis: potential role of homocysteine and parathyroid hormone. Kidney Blood Press Res. 2013;37(4–5):458–463. doi:10.1159/000355727
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Sleep Quality and Hypertension in Chinese Adults: A Cross-Sectional Analysis in the Tianning Cohort
Chen S, Song X, Shi H, Li J, Ma S, Chen L, Lu Y, Hong C, Zhu H, Sun H, Zhang M
Nature and Science of Sleep 2022, 14:2097-2105
Published Date: 28 November 2022
Sleep Quality, Academic Performance, and Associated Predictors Among Undergraduate Health Sciences Students at the University of Rwanda
Nzamwita F, Igihozo C, Turikumana PD, Nshimiyimana J, Nyangezi PM, Biracyaza E, Cloete LG
Advances in Medical Education and Practice 2026, 17:576834
Published Date: 6 February 2026