Back to Journals » Clinical Interventions in Aging » Volume 20
Sarcopenia as a Stronger Predictor for All-Cause Mortality Than Osteoporosis in a Medical Center in Central Taiwan
Authors Hsieh PI, Lin SY, Hsu CY ![]() , Huang SM
, Huang SM ![]() , Huang HT, Weng SC
, Huang HT, Weng SC ![]()
Received 19 June 2025
Accepted for publication 3 October 2025
Published 7 October 2025 Volume 2025:20 Pages 1681—1692
DOI https://doi.org/10.2147/CIA.S548332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Pei-Iun Hsieh,1 Shih-Yi Lin,1– 5 Chiann-Yi Hsu,6 Shih-Ming Huang,7 Hsin-Ti Huang,8,9 Shuo-Chun Weng1– 3,5,8
1Department of Post‑Baccalaureate Medicine, College of Medicine, National Chung Hsing University, Taichung, 402202, Taiwan; 2Geriatrics and Gerontology Research Center, College of Medicine, National Chung Hsing University, Taichung, 402202, Taiwan; 3Center for Geriatrics and Gerontology, Taichung Veterans General Hospital, Taichung, 407219, Taiwan; 4Division of Endocrinology and Metabolism, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, 407219, Taiwan; 5Institute of Clinical Medicine, School of Medicine, National Yang Ming Chiao Tung University, Taipei, 112304, Taiwan; 6Biostatistics Task Force of Taichung Veterans General Hospital, Taichung, 407219, Taiwan; 7Department of Pharmacy, Taichung Veterans General Hospital, Puli Branch, Nantou, 545402, Taiwan; 8Division of Nephrology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, 407219, Taiwan; 9Institute of Medicine, Chung Shan Medical University, Taichung, 40201, Taiwan
Correspondence: Shuo-Chun Weng, Email [email protected]
Purpose: Sarcopenia (SP) and osteoporosis (OP) both pose higher risks for adverse health outcomes. This study explored the relationship among sarcopenia, osteoporosis and all-cause mortality.
Patients and Methods: This retrospective cohort utilized a tertiary-hospital-based cohort during the years from 2018 to 2024. Patients received dual-energy X-ray absorptiometry scans. Osteoporosis was diagnosed when T-scores of <-2.5 were determined at the L-spine or femoral neck. Sarcopenia was defined using the Asian Working Group for Sarcopenia 2019 criteria: low muscle strength, low physical performance, and a low appendicular skeletal mass index. We utilized the Cox proportional hazard model and Kaplan-Meier curves to depict observed time to mortality. Post-hoc analysis was applied for subgroup comparison and statistical power calculation. Interaction terms sensitivity analysis was used for analyzing mutually exclusive groups.
Results: A total of 545 patients (median age [interquartile range] 68.7 [52.8– 80.7] years; 72.3% women) were analyzed. At baseline, 15.6% had SP alone, 23.1% had OP alone, and 14.3% had both conditions. Over median 0.7 (interquartile range = 0.2– 1.4) years of follow-up, 24 deaths occurred. Older age, multimorbidity, sarcopenia, and osteoporosis were significantly associated with higher mortality. In multivariable analysis adjusting for age and multimorbidity, sarcopenia alone was a stronger predictor of mortality compared to osteoporosis alone (hazard ratio [HR] 7.34 vs 3.99), and the mortality HR was 7.34 for sarcopenia with or without osteoporosis higher than 3.99 for osteoporosis with/without sarcopenia. Interaction analysis was not feasible in the four-group comparison, as the interaction term overlapped with the ‘both sarcopenia and osteoporosis’ group; in the other three groups, the SP×OP interaction was not significant. SP patients were more likely to be older, male, and have lower body mass index, total tissue, and lean mass.
Conclusion: These findings suggest that sarcopenia may be a more important predictor of mortality than osteoporosis in patients, highlighting the need for muscle health assessment.
Keywords: sarcopenia, osteoporosis, dual-energy X-ray absorptiometry scans, all-cause mortality, interaction analysis
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Li has been published for this article.
Introduction
Sarcopenia (SP) is an aging-related loss of muscle mass and physical performance with a prevalence of 1.5% in men and 1.2% in women as determined by a T-score < −2.5 in community-dwelling adults,1 while its prevalence is 14–33% for those in a long-term care facility and 10–23.2% in an acute hospital or rehabilitation inpatient center, possibly caused by a low examination rate.2,3 Osteoporosis (OP) and it’s complications is a progressively devastating bone disease which offers a competing risk of mortality as well.4 SP and OP are centered upon a primarily age-related and/or cumulative chronic disease-deteriorating pathophysiological process that involves a deprivation of nutrition and vitamin D, as well as the dysregulation of biochemical factors (estrogen, testosterone, growth hormone, insulin-like growth factor 1, osteocalcin and muscle-derived myokines), iatrogenesis and a sedentary lifestyle.5 There is a direct mutual communication between muscle and bone, and both diseases, no matter whether due to primary or secondary reasons, share a common pathway leading to muscle catabolism and accumulation of intramuscular and bone marrow fat. Similarly, both conditions are strongly associated with frailty, disability, fragility fractures, hospitalization and mortality.5
Although bioimpedance analysis (BIA) of muscle and quantitative ultrasound (QUS) for bone have each been widely and separately used to evaluate SP and OP in community screenings, it should be noted that when using BIA, skeletal muscle mass is obtained through a specific equation, which in turn may limit its reliability thus requiring validation and cut-off points in both clinical practice and research.6 QUS measurements across the calcaneus bone cannot substitute for dual-energy X-ray absorptiometry due to its use in a single location.7 Individually, SP and OP often remain undetected and undertreated in acute hospital and hospital-based institutes.2,5 Geriatric patients with SP diagnosed through BIA in a rehabilitation inpatient unit experienced unfavorable outcomes, including 3-month readmission, institutionalization, and 3-month and 1-year mortality.3 In addition to prevention and management of hip fractures, vertebral fractures, osteoporosis and falls in multiple Fracture Liaison Service programs,8 physical performance and sarcopenia emerged as important issues.9 Furthermore, SP and OP coexist concurrently in patients diagnosed with multi-morbidity who experience more functional impairment and poor synergistic outcomes. To address this knowledge gap, we identified SP and OP through a gold standard measurement, dual-energy X-ray absorptiometry (DXA), in tertiary hospital-based stable outpatient and inpatient individuals to determine if there is single or combined effect between SP and OP on all-cause mortality.
Methods
Study Design and Participants
This retrospective study was conducted in a Fracture Liaison Service (FLS) program at a medical center in central Taiwan during the period from March 31, 2018 to February 05, 2024. A total of 553 patients were included, with eight patients being excluded due to having no appendicular skeletal muscle index (ASMI) data. Through information system referrals (Figure S1), both inpatients and outpatients aged 18 years and older, including new fragility hip fracture from low-energy trauma, vertebral compression fracture, other common osteoporotic fractures, or high-risk osteoporosis associated with conditions such as kidney transplantation, chronic obstructive pulmonary disease, or autoimmune disease, are identified simultaneously. In those patients without fracture, but receiving osteoporosis medication are referred to a case manager for osteoporosis education. The case manager will also monitor the patient’s follow-up clinic appointments. In those patients’ fracture, they will receive simultaneous care from a geriatrician, rehabilitation specialist and dietitian, as well as a comprehensive geriatric assessment (Figure S2), and later concrete FLS optimization strategies are proposed (eg, incorporating grip strength and gait speed into routine screening), along with practical guidance on sarcopenia interventions—such as tailored nutritional support and structured exercise programs—to enhance patient outcomes.
The exclusion criteria consisted of those diagnosed with severe cognitive impairment or dementia; those with multiple fractures or fractures from more than 3 days past, atypical femoral shaft fractures; those fractures related to trauma; those with pathological fractures; and those participating in other fracture or osteoporosis intervention trials.
Ultimately, 545 subjects who concurrently had an ASMI and complete baseline data of their muscle strength and physical performance (Figure 1) were included. These physical function data, collected by trained research nurses, must have been obtained within three months of the baseline ASMI assessment. Handgrip strength was measured using a dynamometer (Smedley’s Dynamometer, TTM, Tokyo, Japan) three times in their dominant hand, with the strongest grip being recorded.10 The 6-meter walking test measures the time it takes an individual to walk a distance of 6 meters and is commonly used to assess mobility and functional capacity.10 In the Timed up-and-go (TUG) test, patients were instructed to rise from a chair, walk a distance of three meters, turn around, return to the chair, and sit down, with the resultant time taken measured to assess mobility and functional ability. Dual-energy X-ray absorptiometry (Lunar iDXA GE Healthcare) scans were performed for body composition and bone mineral density (BMD) in the Department of Radiology, Bone Health Center, with the date of those patients receiving the DXA examination registered as their index date. The ASMI was calculated as the ratio of appendicular skeletal muscle mass and square of body height (kg/m2). Demographic information and anthropometric data, such as age, gender and body mass index (BMI), were all collected. Multimorbidity, represented by an age-adjusted Charlson comorbidity index (ACCI) was determined by twelve common diseases (osteoarthritis, rheumatoid arthritis, diabetes mellitus, hypertension, stroke, cataract, chronic kidney disease, coronary artery disease, peripheral artery disease, congestive heart failure, liver cirrhosis and cancer) based upon self-reporting or patient medical records. Osteoporosis-related medications were also recorded, including Denosumab, Evenity, Fosamax, Raloxifene, Teriparatide, Zoledronic and Ibandronate. The study was approved by the Institutional Review Board of the medical center (IRB NOs.: CE20293A and CE22474A). All methods were carried out in accordance with the approved study protocol under standard regulations as well as the Declaration of Helsinki.
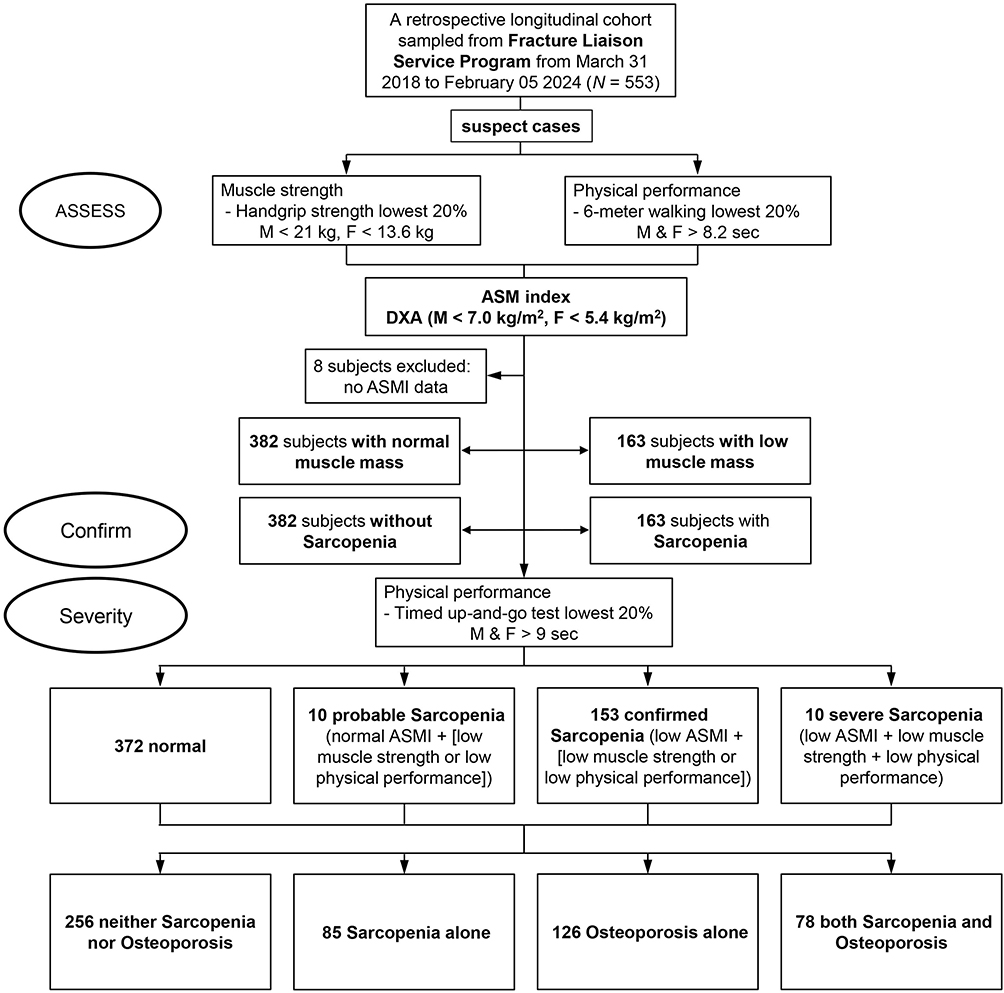 |
Figure 1 Flowchart of patient selection for the study cohort. Abbreviations: DXA, dual-energy X-ray absorptiometry; ASMI, appendicular skeletal muscle index. |
Definitions of Sarcopenia and Osteoporosis
Low muscle strength was considered to be the lowest 20% of handgrip strength (<13.6 kg in women and <21 kg in men). Low physical performance was identified as the lowest 20% of the 6-meter walking speed test (>8.2 seconds in both women and men) and lowest 20% of TUG (>9 seconds both in women and men). These criteria were used because the cases were from a tertiary hospital, where patients typically have more severe conditions, making it inappropriate to apply the Asian Working Group for Sarcopenia (AWGS) 2019 definitions developed for community-dwelling individuals. Low muscle mass was defined as an appendicular skeletal mass index (ASMI) <7.0 kg/m2 for men and <5.4 kg/m2 for women. According to the AWGS 2019 criteria,11 low muscle strength or low physical performance was termed as probable SP (n = 10), low muscle mass with low muscle strength or low physical performance was characterized as confirmed SP (n = 153), and low muscle mass with low muscle strength and low physical performance was described as severe SP (n =10) (Figure 1). Osteoporosis (OP) was delineated as a T-score < −2.5 standard deviation (SD) at the L-spine, femoral neck, and trabecular bone as measured by DXA scans according to the World Health Organization (WHO) classification. Then all 545 patients were classified into neither SP nor OP (n = 256), SP alone (n = 85), OP alone (n = 126), and both SP and OP (n = 78) groups (Figure 1).
Sensitivity Analyses
Combining SP with/without OP versus OP alone, or OP with/without SP versus SP alone, may introduce bias. Therefore, four-group comparisons (neither sarcopenia nor osteoporosis, sarcopenia alone, osteoporosis alone, and both sarcopenia and osteoporosis) and interaction terms were applied in sensitivity analyses to account for the unclear SP–OP interaction.
Outcomes
The primary outcome was all-cause mortality. The patients were followed up from the index date until death or February 29, 2024. Information on incident deaths were retrieved from the Clinical Information Research and Development Center, Taichung Veterans General Hospital, with the accuracy of death being validated by Taiwan’s National Death Registry, according to either ICD-9 (ICD9 001.x–999.x) or ICD10 (A00.x–Z99.x) during a follow-up period lasting a median of 0.7 (interquartile range = 0.2–1.4) years.
Statistical Analysis
For the continuous variables (baseline characteristics), we used the Kolmogorov–Smirnov test to determine the normality of sample distributions. We utilized Mann–Whitney U-tests to compare the distributions of continuous variables across groups of independent variables, and Chi-square tests or Fisher’s exact tests for categorical variables. Due to the relatively small sample size in our analysis, individuals with sarcopenia alone and those with both sarcopenia and osteoporosis were combined into a single category, referred to as “sarcopenia with or without osteoporosis”. If the sarcopenia-only group exhibits a higher mortality rate compared to the group with osteoporosis (with or without sarcopenia), the results would support the conclusion suggested by the title of this paper. To explore the opposite possibility, namely, that the mortality rate is higher in those with osteoporosis (with or without sarcopenia) than in those with sarcopenia alone, we applied various permutations and combinations to further examine the role and importance of sarcopenia.
To assess the association between SP, OP, and the risk of all-cause mortality, Cox proportional hazards models were employed, adjusting for potential confounding variables. Kaplan-Meier survival curves were generated to illustrate time to mortality, and the Log-Rank (Mantel-Cox) test was used to compare cumulative survival rates across subgroups. Pairwise comparisons were conducted to evaluate the effects of SP, OP, and their combined status on long-term mortality. For subgroup comparisons, the Dunn–Bonferroni post-hoc test was performed. Statistical power was evaluated using Fisher’s exact test. Sensitivity analysis with interaction terms was conducted to assess mutually exclusive groups. When contingency tables exceed the 2×2 format (eg, 2×3, 3×3) and the sample size is relatively small, the Fisher–Freeman–Halton exact test serves as a generalized extension of Fisher’s exact test, enabling exact inference for larger tables and more complex hypotheses. All statistical tests were two-sided, with a significance level set at p < 0.05. Analyses were performed using SPSS for Windows, version 22.0 (SPSS Institute Inc., Chicago, USA).
Results
At baseline, 545 patients having a median age (interquartile range) of 68.7 (52.8–80.7) years were 72.3% female. The prevalence of SP alone was 15.6%, OP alone 23.1%, and both SP and OP 14.3%. Baseline characteristics of the participants by SP and OP status are shown in Table 1. The mean age, gender, body mass index (BMI), body composition with android to gynoid fat ratio, total tissue, total fat, total lean tissue, bone density, albumin, medications, ASMI, and T-score significantly differed across all characteristics by SP and OP status.
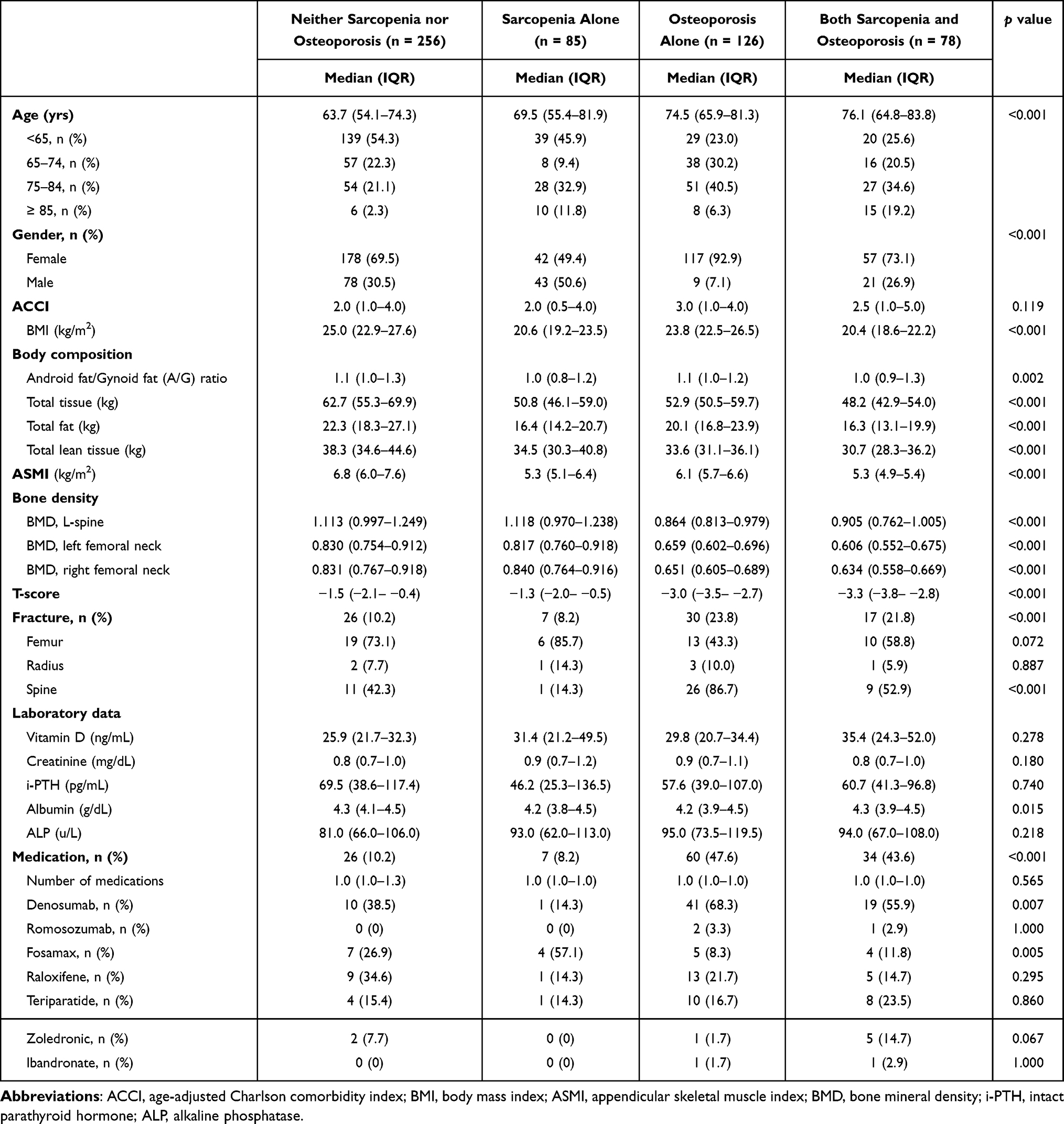 |
Table 1 Characteristics of the Study Population by the Status of Sarcopenia and Osteoporosis at Baseline |
When combining patients with sarcopenia, with or without osteoporosis, they were found to be older, predominantly male (39.3%), and exhibited significantly lower BMI (20.5 kg/m²), total tissue, total fat, and total lean tissue compared to the other groups. The appendicular skeletal muscle mass index (ASMI) was significantly lower in this group than in those with osteoporosis alone or with neither condition (p <0.001).
In contrast, the osteoporosis-alone group had a significantly higher proportion of females (92.9%) compared to the other groups (p <0.001). Medication use was also more prevalent in the osteoporosis-alone group (47.6%) (p <0.001). Moreover, bone mineral density (BMD) of the lumbar spine and femoral neck (both left and right) was significantly lower in the osteoporosis-alone group than in the sarcopenia with/without osteoporosis group (p <0.001). T-scores were significantly reduced in both the osteoporosis-alone and sarcopenia with/without osteoporosis groups (p <0.001; Table 2).
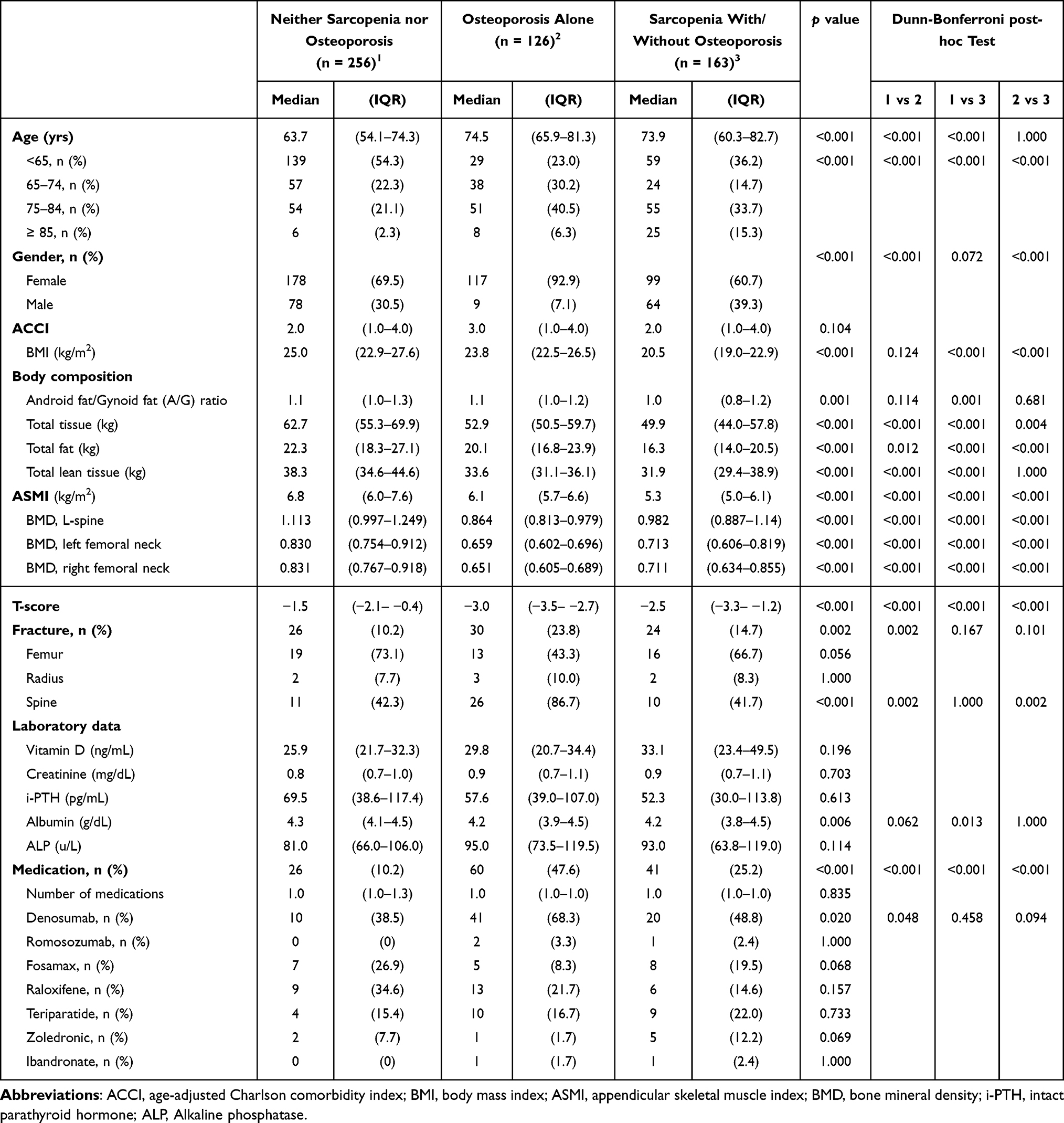 |
Table 2 Comparative Analysis of Clinical Parameters and Data From Dual-Energy X-Ray Absorptiometry Across Different Sarcopenia and Osteoporosis Groups |
When combining patients with osteoporosis, with or without sarcopenia, they were also older, predominantly female (85.3%), and had significantly lower BMD of the lumbar spine and both femoral necks compared to the other groups. ASMI was significantly lower in the sarcopenia-alone group than in the osteoporosis with/without sarcopenia and control groups (p <0.001). A higher proportion of individuals in the osteoporosis with/without sarcopenia group were on medication (46.1%) compared to other groups (p <0.001). T-scores were significantly lower in this group as well (p <0.001; Table S1).
After median 0.7 (interquartile range = 0.2–1.4) years of follow-up, 24 patients had died. The mortality of the group “neither SP nor OP” was 8.3%, compared with 29.2% for the group with SP alone, 37.5% for the group with OP alone, and 25.0% for both SP and OP (p <0.001). Comparisons between survivors and deceased participants with different SP and OP statuses are shown in Table S2. Given the lower mortality number in a short follow up time, we further used Fisher’s exact test to conduct a post-hoc power calculation for survival status in relation to the sarcopenia. The estimated power (1-β error probability) was 0.6787769 (68%). Second, for osteoporosis, the post-hoc power for survival status was 0.7076415 (71%) (Table S3). Overall, our findings suggest that the number of deaths (events) was insufficient to achieve adequate statistical power, although true associations may exist. In addition, from the results of Table S2, it can be seen that the 24 deceased patients were older and had poorer bone and muscle status. According to the medication data, all of the deceased had received denosumab treatment for osteoporosis, indicating that they belonged to a high-risk group. The relatively short observation period (median follow-up of only 0.7 years) was mainly due to the fact that 382 of the 545 patients (about 70%) were enrolled later and therefore had less than one year of follow-up. Although patient enrollment began in 2018 and ended on February 29, 2024, the majority of cases (71%) were recruited after 2023, resulting in an overall short observation period that limited the ability to capture long-term outcomes. Besides, denosumab was analyzed separately (regardless of concomitant use of other medications). Whether adjusting for denosumab alone or additionally for age and ACCI, the mortality risk remained higher in patients with sarcopenia. This pattern was more evident in the group without denosumab use, as reflected in the data distribution (Table S4).
In the unadjusted Cox proportional hazards regression model, older age, higher age-adjusted Charlson Comorbidity Index (ACCI), sarcopenia, and osteoporosis were all significantly associated with increased risk of all-cause mortality. Specifically, the crude hazard ratio (HR) for mortality was 10.72 for sarcopenia alone (95% CI: 2.23–51.64, p = 0.003), 7.52 for osteoporosis alone (95% CI: 1.62–34.91, p = 0.010), and 8.74 for the combination of sarcopenia and osteoporosis (95% CI: 1.76–43.36, p = 0.008), when compared to individuals without either condition (Table 3).
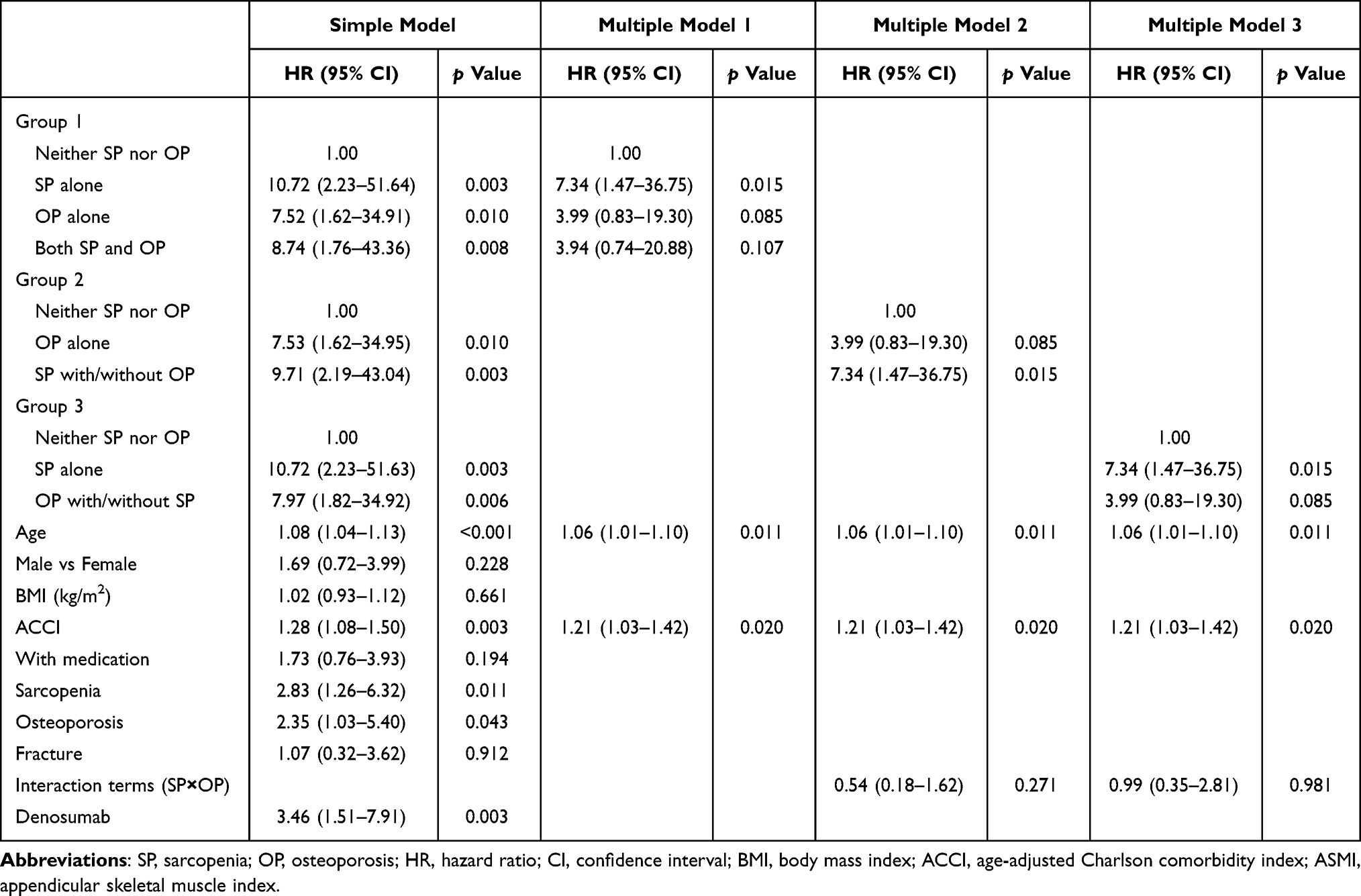 |
Table 3 Cox Regression Analysis for All-Cause Mortality in Patients With or Without Sarcopenia and Osteoporosis |
After adjusting for age and ACCI, sarcopenia with or without osteoporosis (SP±OP) remained significantly associated with the highest risk of mortality (HR: 7.34; 95% CI: 1.47–36.75; p = 0.015), followed by osteoporosis alone (HR: 3.99; 95% CI: 0.83–19.30), relative to the reference group without sarcopenia and osteoporosis (Table 3).
In an alternative grouping approach, after similar adjustments, sarcopenia alone was associated with the highest HR for mortality (HR: 7.34; 95% CI: 1.47–36.75), followed by osteoporosis with or without sarcopenia (HR: 3.99; 95% CI: 0.83–19.30), compared to those without either condition (Table 3). Moreover, since the patients in Table 3 were already divided into four categories—neither sarcopenia nor osteoporosis, sarcopenia alone, osteoporosis alone, and both sarcopenia and osteoporosis—the interaction term analysis did not yield meaningful results. In addition, the interaction terms for groups 2 and 3 in Table 3 were not statistically significant.
Kaplan-Meier survival curves demonstrate that, within the first 36 months, individuals without sarcopenia or osteoporosis exhibit the highest survival rates, followed by those with osteoporosis alone. The lowest survival is observed among individuals with sarcopenia, irrespective of concurrent osteoporosis (p <0.001; Figure 2a). In an alternative grouping approach, individuals with sarcopenia alone show the poorest survival outcomes when compared to those without either condition and those with osteoporosis, with or without sarcopenia (Figure 2b). Although the “SP±OP” group had the lowest survival rate (92.4%), post-hoc pairwise comparisons showed no significant difference between “SP±OP” (92.4%) and the next lowest group, “OP alone” (96.8%). A similar pattern was observed in Figure 2b: while overall survival differed among the three groups, the difference was mainly driven by the highest-survival group compared with the other two, as no significant difference was found between the second and lowest groups (Table S5).
 |
Figure 2 (a) Kaplan-Meier Plot based on categorization as neither sarcopenia nor osteoporosis, osteoporosis alone, and sarcopenia with/without osteoporosis at baseline. Pairwise Comparisons: osteoporosis alone versus neither sarcopenia nor osteoporosis p <0.001, sarcopenia with/without osteoporosis versus osteoporosis alone p = 0.199, and sarcopenia with/without osteoporosis versus neither sarcopenia nor osteoporosis p = 0.013. (b) Kaplan-Meier Plot based on categorization as neither sarcopenia nor osteoporosis, sarcopenia alone, and osteoporosis with/without sarcopenia at baseline. Pairwise Comparisons: sarcopenia alone versus neither sarcopenia nor osteoporosis p <0.001, osteoporosis with/without sarcopenia versus sarcopenia alone p = 0.199, and osteoporosis with/without sarcopenia versus neither sarcopenia nor osteoporosis p = 0.013. |
Discussion
Advanced age, a high Charlson comorbidity index (ACCI), sarcopenia, and osteoporosis are all associated with increased mortality risks in older adults. Research shows that sarcopenia poses the highest risk for all-cause mortality, even more so than osteoporosis. Our analysis has confirmed that individuals with sarcopenia, regardless of whether they have osteoporosis, experience the highest risk. Factors such as older age, male gender, and low body mass index (BMI) further increase this vulnerability. Post-hoc analysis of our cohort revealed that these individuals often had low total tissue, fat and lean mass, highlighting the complex nature of their mortality risk.
A meta-analysis performed by Shu et al revealed that individuals with sarcopenia had a significantly higher mortality risk (HR: 1.82) when compared to those without.12 This finding underscores the importance of addressing sarcopenia as a primary target in the health management of aging populations. Our study further reinforces this, demonstrating that even when adjusted for the presence of osteoporosis, sarcopenia continues to exhibit the highest HR for mortality risk. This indicates that muscle strength and mass may play a more critical role in predicting outcomes than bone density alone.
In our multivariable regression analysis, individuals with sarcopenia, regardless of the presence of osteoporosis, displayed the highest HR for all-cause mortality. This aligns with findings from the available literature which emphasizes that sarcopenic individuals often exhibit additional vulnerabilities, such as reduced functional capacity and increased comorbidity, leading to higher mortality rates.13
Furthermore, our post-hoc analysis of this specific cohort identified additional risk factors: older age, male gender, low body mass index (BMI), and low levels of total tissue, total fat and total lean tissue which were prevalent among those with the highest mortality risk. These factors not only exacerbate the effects of sarcopenia and osteoporosis but also signal a multifactorial risk profile. The interaction of low BMI and low muscle mass, particularly in older males, is noteworthy; a cross-sectional study via the Korea National Health and Nutrition Examination survey highlighted that men are more susceptible to sarcopenic obesity, which further complicates the clinical picture and increases mortality risk.14
Additionally, the low total tissue and lean tissue measurements in our cohort may reflect not only the impact of sarcopenia but also an underlying state of malnutrition or inadequate physical activity, both of which are prevalent in the elderly. According to the Framingham Study Offspring Cohort, higher abdominal adiposity is associated with higher lean muscle mass but lower muscle quality in middle to old age men and women.15 In turn, muscle-secreted inflammatory cytokines may exacerbate adipose tissue atrophy, support chronic low-grade inflammation, and lead to irreversible sarcopenia and even cachexia, known as the so called Metabaging Cycle.16 Additional evidence has suggested that adequate nutrition and regular exercise were vital for both maintaining muscle mass and reducing mortality risk in older populations. These findings suggest that healthcare providers must consider comprehensive assessments that include muscle mass, nutritional status, and physical activity levels when evaluating older adults for potential interventions.
This study has some limitations. First, our study participants were recruited from a tertiary-hospital and thus tended to have a multimorbid physical status with a high comorbidity burden (eg, ACCI ≥ 2) at baseline, which may not be generalized to healthier community-dwelling older adults. Second, this study had a relatively short follow-up period, so future studies are still warranted in order to capture the trajectory of long-term outcomes. Nevertheless, despite the limited statistical power, our findings suggest that sarcopenia is associated with a higher risk of mortality compared with osteoporosis alone, osteoporosis with or without sarcopenia, and neither condition. With a longer follow-up and a greater number of accumulated events, sarcopenia is likely to be confirmed as a significant independent risk factor for mortality. Third, osteoporosis alone patients received significantly more treatment (47.6%) than sarcopenia with/without osteoporosis (25.2%) or controls (10.2%) (Table 2). This may bias mortality outcomes if medications reduce osteoporosis-related deaths. However, stratified analyses by medication use showed that, in the non-medication group, patients with sarcopenia with/without osteoporosis had a higher risk of mortality compared with controls (Table S6A), whereas osteoporosis-alone patients did not show an increased risk compared with controls. In the medication group, osteoporosis (OP)-alone patients did not have a higher risk of mortality compared with sarcopenia with/without osteoporosis patients (HR: 2.05; 95% CI, 0.54–7.76) (Table S6C). Fourth, nutrition (albumin), mobility, and rehabilitation were important covariates among patients with sarcopenia; however, these factors were not adjusted for in the multivariable models due to missing data, which may have led to the omission of critical confounders. Fifth, only all-cause mortality was reported. Differentiating specific causes of death (eg, infections, cardiovascular events, or re-fractures) would provide greater clarity on the mechanisms linking sarcopenia to adverse outcomes.
In conclusion, our findings emphasize the critical role which sarcopenia may play in being a primary risk factor for all-cause mortality in older individuals with a high ACCI. The multifactorial nature of mortality risk in this population necessitates a holistic approach to care, encompassing physical, nutritional and medical management strategies. As the global population ages, understanding these dynamics will be essential in developing effective interventions which can enhance longevity and the quality of life in older adults.
Data Sharing Statement
The data that support the findings of this study are available upon request to the correspondent author.
Ethics Approval and Consent to Participants
This observational study was conducted in accordance with the Declaration of Helsinki. All methods were conducted in accordance with relevant guidelines and regulations. Study approval was obtained from the Taichung Veterans General Hospital’s Institutional Review Board (TCVGH-IRB No. CE20293A and CE22474A). Due to the retrospective nature of this study, the Taichung Veterans General Hospital’s Institutional Review Board waived the requirement for informed consent. Those data were accessed anonymously.
Acknowledgments
We are grateful to the Biostatistics Task Force and Clinical Information Research & Development Center of Taichung Veterans General Hospital, Taichung, Taiwan, R.O.C., for assistance in statistics analysis. The authors also sincerely appreciate the assistance provided by the Center for Translational Medicine of Taichung Veterans General Hospital, Taichung, Taiwan.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We are deeply indebted to Taichung Veterans General Hospital, Taichung for providing the grants for this study (TCVGH-1138202C, TCVGH-1144902C, TCVGH-1144901D, TCVGH-NCHU1110114, TCVGH-NCHU1127616, TCVGH-NCHU1137624 and TCVGH-NCHU1137625). This study was also supported by Taiwan’s Ministry of Science and Technology (MOST 106-2314-B-075A-003).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kirk B, Bani Hassan E, Brennan-Olsen S, et al. Body composition reference ranges in community-dwelling adults using dual-energy X-ray absorptiometry: the Australian Body Composition (ABC) Study. J Cachexia Sarcopenia Muscle. 2021;12(4):880–890. doi:10.1002/jcsm.12712
2. Cruz-Jentoft AJ, Landi F, Schneider SM, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. report of the international sarcopenia initiative (EWGSOP and IWGS). Age Ageing. 2014;43(6):748–759. doi:10.1093/ageing/afu115
3. Verstraeten LMG, de Haan NJ, Verbeet E, van Wijngaarden JP, Meskers CGM, Maier AB. Handgrip strength rather than chair stand test should be used to diagnose sarcopenia in geriatric rehabilitation inpatients: rEStORing health of acutely unwell adulTs (RESORT). Age Ageing. 2022;51(11):afac242. doi:10.1093/ageing/afac242
4. Ensrud KE, Kats AM, Boyd CM, et al. Association of disease definition, comorbidity burden, and prognosis with hip fracture probability among late-life women. JAMA Intern Med. 2019;179(8):1095–1103. doi:10.1001/jamainternmed.2019.0682
5. Kirk B, Zanker J, Duque G. Osteosarcopenia: epidemiology, diagnosis, and treatment-facts and numbers. J Cachexia Sarcopenia Muscle. 2020;11(3):609–618. doi:10.1002/jcsm.12567
6. Donini LM, Busetto L, Bischoff SC, et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Clin Nutr. 2022;41(4):990–1000. doi:10.1016/j.clnu.2021.11.014
7. Shimada H, Suzuki T, Doi T, et al. Impact of osteosarcopenia on disability and mortality among Japanese older adults. J Cachexia Sarcopenia Muscle. 2023;14(2):1107–1116. doi:10.1002/jcsm.13209
8. Chao CT, Yang RS, Huang WJ, Tsai KS, Chan DD. Risk factors for poor functional recovery, mortality, recurrent fractures, and falls among patients participating in a fracture liaison service program. J Am Med Dir Assoc. 2019;20(9):1129–1136.e1. doi:10.1016/j.jamda.2018.12.011
9. Schene MR, Willems HC, Driessen JHM, et al. Physical performance and sarcopenia assessment in patients with a recent fracture visiting the fracture liaison service. Osteoporos Int. 2024;35(5):851–862. doi:10.1007/s00198-023-07009-w
10. Weng SC, Hsu CY, Wu MF, Lee WH, Lin SY. The impact of frailty status on pulmonary function and mortality in older patients with chronic obstructive pulmonary disease. J Nutr Health Aging. 2023;27(11):987–995. doi:10.1007/s12603-023-2017-7
11. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
12. Shu X, Lin T, Wang H, et al. Diagnosis, prevalence, and mortality of sarcopenia in dialysis patients: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2022;13(1):145–158. doi:10.1002/jcsm.12890
13. Damluji AA, Alfaraidhy M, AlHajri N, et al. Sarcopenia and cardiovascular diseases. Circulation. 2023;147(20):1534–1553. doi:10.1161/CIRCULATIONAHA.123.064071
14. Hwang J, Park S. Gender-specific prevalence and risk factors of sarcopenic obesity in the Korean elderly population: a nationwide cross-sectional study. Int J Environ Res Public Health. 2023;20(2):1140. doi:10.3390/ijerph20021140
15. Raghupathy R, McLean RR, Kiel DP, Hannan MT, Sahni S. Higher abdominal adiposity is associated with higher lean muscle mass but lower muscle quality in middle-aged and older men and women: the Framingham Heart Study. Aging Clin Exp Res. 2023;35(7):1477–1485. doi:10.1007/s40520-023-02427-6
16. Li CW, Yu K, Shyh-Chang N, et al. Pathogenesis of sarcopenia and the relationship with fat mass: descriptive review. J Cachexia Sarcopenia Muscle. 2022;13(2):781–794. doi:10.1002/jcsm.12901
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bibliometrics Analysis and Visualization of Sarcopenia Associated with Osteoporosis from 2000 to 2022
Yang J, Jiang T, Xu G, Liu W
Journal of Pain Research 2023, 16:821-837
Published Date: 13 March 2023
Advances in the Study of Denosumab Treatment for Osteoporosis and Sarcopenia in the Chinese Middle-Aged and Elderly Population
Li S, Zou J, Ran J, Wang L, Nie G, Liu Y, Tian C, Yang X, Liu Y, Wan J, Peng W
International Journal of General Medicine 2024, 17:6089-6099
Published Date: 11 December 2024
Association Between Dietary Patterns and All-Cause Mortality in Individuals with Hypertension and Osteoporosis: A Retrospective Cohort Study
Guan J, Ding L, Wang Y, Zhu Z, Pan M, Du L, Yin N
Journal of Multidisciplinary Healthcare 2025, 18:3781-3791
Published Date: 30 June 2025
The Relation of Osteoporotic Vertebral Fractures and Sarcopenic Characteristics on the Occurrence of Complications: A Systematic Review
Roschke E, Wiersbicki DW, Pieroh P, Heyde CE, Osterhoff G
Clinical Interventions in Aging 2025, 20:1471-1480
Published Date: 2 September 2025