Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Application Study of Health Management Model Based on Traditional Chinese Medicine Constitution Identification in COPD Patients: A Retrospective Analysis
Authors Liang T, An NN, Huang YQ, Wang PF, Yan YJ, Wang YJ, Zhang SH, Yang QY
Received 20 May 2025
Accepted for publication 13 November 2025
Published 9 December 2025 Volume 2025:20 Pages 3965—3978
DOI https://doi.org/10.2147/COPD.S541677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Tao Liang,1,* Nan-Nan An,1,* Yan-Qiu Huang,2 Peng-Fei Wang,1 Ying-Jie Yan,1 Yan-Jun Wang,1 Su-Hua Zhang,3 Qing-Yan Yang4
1Department of Traditional Chinese Medicine, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, 056002, People’s Republic of China; 2Department of Data Center, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, 056002, People’s Republic of China; 3Department of Respiratory, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, 056002, People’s Republic of China; 4Department of General Surgery, Affiliated Hospital of Hebei University of Engineering, Handan, Hebei, 056002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qing-Yan Yang, Department of General Surgery, Affiliated Hospital of Hebei University of Engineering, No. 81, Congtai District, Congtai Road, Handan, Hebei, 056002, People’s Republic of China, Tel +86 0310-3961028, Email [email protected]
Objective: This retrospective study aimed to evaluate a health management model based on traditional Chinese medicine (TCM) constitution identification in Chronic Obstructive Pulmonary Disease (COPD) patients.
Methods: This retrospective case-control study selected 108 COPD patients from the Respiratory Department of our hospital, divided into an observation group (n=54, receiving TCM constitution-based health management) and a control group (n=54, receiving routine health guidance). Primary outcome measures included COPD Assessment Test (CAT) scores and Forced Expiratory Volume in one second (FEV1).
Results: After 6 months, the observation group showed improvements in CAT scores (baseline: 24.93± 2.61 to 6 months: 22.31± 2.12, p< 0.001) and FEV1 values (baseline: 1.34± 0.71 L to 6 months: 1.79± 0.73 L, p< 0.001). After propensity score matching, clinical response rates remained higher in the observation group (CAT: 48.8% vs 18.6%; FEV1: 72.1% vs 7.0%, both p< 0.001). However, significant baseline differences existed between groups, with the observation group being younger, having shorter disease duration, and better baseline lung function (all GOLD II vs 55.6% GOLD III in controls).
Conclusion: This retrospective study provides preliminary evidence suggesting potential value of TCM constitution-based health management in COPD patients. However, significant baseline differences and methodological limitations necessitate cautious interpretation. Well-designed prospective randomized controlled trials with matched cohorts are essential to establish efficacy definitively.
Keywords: chronic obstructive pulmonary disease, COPD, traditional Chinese medicine, TCM, constitution identification, health management, individualized treatment
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a chronic respiratory disease characterized by persistent airflow limitation, primarily caused by long-term exposure to harmful particles or gases such as smoking, air pollution, and occupational dust.1 According to the World Health Organization (WHO), COPD has become the third leading cause of death globally, second only to cardiovascular diseases and cancer, and it is expected to maintain this trend through 2030.2 In China, the prevalence of COPD has significantly increased with the acceleration of industrialization and urbanization, especially among middle-aged and elderly populations, imposing a heavy burden on the national public health system and economic development.3
Clinically, COPD manifests as persistent cough, sputum production, dyspnea, and acute exacerbations, which severely impact patients’ quality of life and work capacity.4 Additionally, COPD is often accompanied by various comorbidities such as cardiovascular diseases, osteoporosis, and depression, further increasing patients’ health risks and medical expenses.5 Currently, the management of COPD primarily relies on pharmacological treatments (eg, bronchodilators and inhaled corticosteroids), oxygen therapy, pulmonary rehabilitation, and comprehensive health education, aiming to alleviate symptoms, reduce acute exacerbations, and improve quality of life.6 However, traditional management models still face certain limitations in individualized treatment and long-term health management, particularly in enhancing patient adherence, personalized interventions, and comprehensive health management effectiveness.7
Traditional Chinese Medicine (TCM), as an essential component of Chinese traditional medicine, boasts a long history and a rich theoretical system, emphasizing a holistic view and individualized treatment. TCM constitution theory categorizes individuals into various types, such as Qi deficiency, Yin deficiency, Yang deficiency, and Phlegm-dampness, each corresponding to specific physiological and pathological characteristics.8 Through “pattern differentiation and treatment,” TCM can formulate personalized treatment and health maintenance plans based on different constitutions, thereby achieving comprehensive disease management.9 In recent years, health management models based on TCM constitution identification have gradually attracted attention, particularly demonstrating unique advantages in the management of chronic diseases.10
Emerging evidence suggests potential relationships between TCM constitution types and Western clinical phenotypes in COPD. For instance, the “Blue-Bloater” phenotype in Western medicine, characterized by chronic bronchitis with significant sputum production and cyanosis, may correlate with the Phlegm-dampness constitution in TCM.11 Similarly, the “Pink-Puffer” phenotype, presenting with emphysema and dry cough, might correspond to Yin deficiency or Qi deficiency constitutions. These preliminary associations warrant further investigation to establish more definitive connections between TCM and Western medical frameworks.
Various TCM interventions have shown promise in COPD management. Herbal medicine formulations such as Bufei Yishen granules and Yuebijia Banxia Tang have demonstrated improvements in lung function and quality of life in multiple clinical trials.12,13 Acupuncture therapy has also shown benefits in reducing dyspnea and improving exercise tolerance in COPD patients.14 Furthermore, traditional exercises like Tai Chi and Qigong have been incorporated into pulmonary rehabilitation programs with positive outcomes.15,16 These studies provide a foundation for the comprehensive TCM constitution-based intervention model evaluated in our study.
In the management of COPD, individualized health management strategies are particularly important due to significant differences in patients’ conditions and constitutions. Studies have shown that COPD patients with different constitution types exhibit significant differences in symptom presentation, disease progression, and treatment responses.17 Integrating TCM constitution identification into health management allows for targeted interventions, potentially enhancing treatment efficacy and improving patients’ quality of life. For instance, Qi deficiency patients may require Qi-tonifying medications and appropriate exercise to boost physical strength, while Phlegm-dampness patients might benefit from dietary and lifestyle adjustments to resolve phlegm and dampness.18 These personalized interventions may help improve patients’ self-management capabilities, reduce the frequency of acute exacerbations, and thereby potentially slow disease progression.19
Although TCM constitution identification shows potential in chronic disease management, systematic application research in COPD patients remains limited. Existing studies primarily focus on specific herbal treatments or acupuncture therapies, lacking comprehensive evaluations of integrated health management models.20 Furthermore, current research is mostly short-term with limited long-term evaluations of the health management model based on TCM constitution identification. Therefore, this retrospective study aims to explore the application effects of a health management model based on TCM constitution identification in COPD patients through case-control analysis, assessing its potential value and prospects in symptom improvement, lung function recovery, and overall health management, while acknowledging the inherent limitations of the retrospective design.
Methods
Study Design and Participants
This hospital-based retrospective case-control study analyzed data from COPD patients treated at the Respiratory Department of our hospital from January 2023 to September 2024, a comprehensive tertiary hospital in Handan City. Clinical data were systematically extracted from the hospital’s electronic medical record system and standardized case report forms. The study protocol underwent rigorous review and received approval from the Ethics Committee of our Hospital (Protocol No.: 2024[K]078). Given the retrospective observational nature of the study and the use of de-identified data, the requirement for informed consent was waived by the ethics committee in accordance with institutional guidelines for retrospective chart reviews.
Through detailed review of medical records spanning the study period, 108 COPD patients’ records were identified and analyzed. These records were divided into two groups based on their documented healthcare management approach: the observation group (n=54) who received comprehensive TCM constitution-based health management, and the control group (n=54) who received routine health guidance. To minimize selection bias and ensure comparability between groups, cases were carefully matched using a 1:1 ratio based on age (±5 years), baseline disease severity, and initial hospital visit date (±30 days). This matching process was performed by two independent researchers using a standardized protocol, with any discrepancies resolved through discussion with a senior respiratory specialist. The specific protocol diagram is shown in Supplemental Figure 1.
The inclusion of patient records followed stringent criteria: (1) confirmed diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2021 guidelines, requiring documented characteristic symptoms (dyspnea, chronic cough, and/or sputum production) and a post-bronchodilator FEV1/FVC ratio <0.70 confirmed by standard spirometry; (2) lung function classified as either stage II (moderate, defined as 50% ≤ FEV1 < 80% predicted) or stage III (severe, defined as 30% ≤ FEV1 < 50% predicted) according to GOLD criteria; (3) documented disease duration exceeding 3 months with clinically stable condition, defined as no acute exacerbations requiring hospitalization or systemic corticosteroids in the preceding 4 weeks; (4) complete medical records containing all required assessment data points, including pulmonary function tests, symptom assessments, and TCM constitution evaluations; and (5) documented regular follow-up attendance over a minimum 6-month period, with no more than one missed appointment.
Records were excluded based on the following criteria: (1) concurrent diagnosis of lung cancer, active tuberculosis, bronchiectasis, or other severe pulmonary diseases that might confound COPD assessment; (2) presence of severe cardiovascular or cerebrovascular diseases, including but not limited to unstable angina, myocardial infarction within 6 months, or stroke with significant functional impairment; (3) documented mental disorders or cognitive impairment that could affect symptom reporting or treatment compliance; (4) incomplete follow-up data, defined as missing more than one scheduled assessment or lacking key outcome measurements; or (5) documented participation in other clinical trials or interventional studies during the study period.
Clinical Management
The management approaches for both groups were thoroughly documented in the medical records and standardized case report forms. For the control group, routine health guidance from the respiratory department followed a structured protocol based on current COPD management guidelines. This included several key components. First, patients received standardized education through one-on-one sessions conducted by respiratory nurses with at least 3 years of COPD management experience. These sessions covered comprehensive educational materials on COPD pathophysiology, risk factors, and progression, along with detailed instruction on proper inhaler technique using device-specific demonstration kits. Second, smoking cessation counseling was provided following the 5A’s approach (Ask, Advise, Assess, Assist, and Arrange), supplemented by written action plans for managing COPD exacerbations. Third, monthly group education sessions focused on lifestyle modification and self-management strategies were conducted.
Regular clinical monitoring for the control group involved scheduled follow-up visits at 1, 3, and 6 months. During these visits, standardized assessment of symptoms using validated questionnaires was performed, along with regular review of medication adherence and inhaler technique. Physical activity levels and exercise tolerance were monitored, and any COPD exacerbations or complications were thoroughly documented.
The observation group received a comprehensive TCM constitution-based health management program consisting of several integrated components. Initially, comprehensive health records were established incorporating both Western and TCM perspectives. These records included detailed documentation of medical history, including family history, environmental exposures, and lifestyle factors, along with physical examination findings according to both Western and TCM diagnostic criteria. Laboratory test results, including routine blood work, inflammatory markers (C-reactive protein, interleukin-6, tumor necrosis factor-alpha when available), and arterial blood gases, were systematically recorded, complemented by baseline pulmonary function tests and exercise capacity assessments.
TCM constitution assessment was conducted by two TCM practitioners with minimum 5 years of clinical experience and specific training in constitution assessment through repeatedly interpreting 30 random medical records based on the “Classification and Evaluation Scale of Traditional Chinese Medicine Constitution” (CCMQ, 2009)21,22 with weighted κ=0.81, ICC=0.88 and Cronbach’s α=0.72–0.82. The CCMQ evaluates nine basic constitution types: Balanced, Qi deficiency, Yang deficiency, Yin deficiency, Phlegm-dampness, Damp-heat, Blood stasis, Qi stagnation, and Special diathesis. For this study, particular focus was placed on four COPD-relevant types: Yang deficiency (characterized by cold intolerance and fatigue), Yin deficiency (manifesting as dry mouth and night sweats), Qi deficiency (presenting with shortness of breath and spontaneous sweating), and Phlegm-dampness (showing excessive sputum production and heaviness sensation). Constitution-specific symptoms and physical signs were meticulously documented, with regular reassessment conducted at 3-month intervals to track constitutional changes.
Based on identified constitution type(s), personalized health management strategies were developed and implemented through self-proposed standardized case report forms. These encompassed:
Dietary recommendations: Constitution-specific dietary modifications were prescribed according to published TCM dietary guidelines.23,24 For example, Yin deficiency patients received recommendations to increase intake of Yin-nourishing foods such as pears, white fungus, lily bulbs, and tremella, while avoiding spicy and warming foods. Phlegm-dampness patients were advised to reduce intake of greasy, sweet, and cold foods while increasing consumption of spleen-strengthening and dampness-resolving foods such as pearl barley, winter melon, and Chinese yam.
Exercise prescriptions: Personalized exercise programs were designed based on both constitution type and physical condition,25 incorporating traditional Chinese exercises such as Tai Chi, Qigong (specifically Liuzijue breathing exercises), and Baduanjin. Exercise intensity and duration were individualized according to baseline exercise tolerance and GOLD stage.
Herbal medicine: Classical herbal formulations were prescribed according to constitution type and symptom patterns.26 For Qi deficiency constitution, formulations based on Bufei Yishen granules were commonly used. For Yin deficiency, modifications of Sha Shen Mai Dong Tang were prescribed. For Phlegm-dampness, variations of Erchen Tang were utilized. All herbal prescriptions followed the Chinese Pharmacopoeia standards and were prepared by certified hospital pharmacies.
Lifestyle modifications: TCM-based lifestyle advice included sleep hygiene recommendations, emotional regulation techniques (such as meditation and breathing exercises), environmental modifications (maintaining appropriate room temperature and humidity), and seasonal health maintenance practices aligned with TCM principles.
Physical therapy: Specific breathing exercises (pursed-lip breathing, diaphragmatic breathing), acupressure techniques for self-application at specific acupoints (Feishu BL13, Zusanli ST36, Dingchuan EX-B1), and chest percussion techniques were taught to patients for daily practice.
The management approach was continuously monitored and adjusted based on documented patient responses and observed constitutional changes throughout the 6-month study period. Medication adherence, adverse events, and constitutional changes were systematically recorded at each follow-up visit.
Assessment and Outcomes
The primary outcomes were changes in CAT scores and FEV1 values, assessed at baseline, 3 months, and 6 months. The CAT questionnaire, a validated 8-item instrument measuring the impact of COPD on health status, was administered in a standardized manner by trained research assistants who were blinded to group allocation when possible. Each item was scored from 0 to 5, with total scores ranging from 0 to 40; lower scores indicated better health status.
Spirometry was performed using a calibrated spirometer (model documented in medical records) according to American Thoracic Society/European Respiratory Society guidelines. Tests were conducted by certified pulmonary function technicians. Three acceptable maneuvers were required, and the highest FEV1 value was recorded. Post-bronchodilator measurements were obtained 15 minutes after administration of 400 μg salbutamol via a metered-dose inhaler with a spacer.
TCM constitution assessment followed the standardized procedures outlined in the TCM Constitution Classification and Determination Scale. The scale includes both subjective symptom evaluation and objective physical examination findings. Constitution types were determined based on established scoring criteria. For each of the nine constitution types, a score ≥40 was considered as having that constitution type, and individuals could have multiple constitution types simultaneously. The assessment was conducted in a dedicated clinic room under consistent environmental conditions.
Treatment response was defined based on clinically meaningful changes: a ≥10% improvement in CAT score or a ≥12% improvement in FEV1 from baseline to 6 months. These thresholds were selected based on previously established minimal clinically important differences in COPD research. Dyspnea was evaluated using a standardized 0–4 scale (Modified Medical Research Council dyspnea scale), where 0 represented no dyspnea and 4 indicated severe dyspnea at rest.
Statistical Analysis
Statistical analyses were performed using R software (version 4.2.0). Continuous variables were presented as mean ± standard deviation, and categorical variables as frequencies and percentages. Between-group comparisons were conducted using independent t-tests for continuous variables and chi-square tests or Fisher’s exact test (when cell counts <5) for categorical variables.
To address potential selection bias due to baseline differences between groups, propensity score matching was performed based on age, disease duration, and baseline lung function using nearest-neighbor matching with a caliper width of 0.2 standard deviations. This resulted in 43 matched pairs for the adjusted analyses. Additionally, analysis of covariance (ANCOVA) was conducted with baseline values, age, disease duration, and lung function stage as covariates to control for pre-existing differences when examining outcome measures.
Repeated measures analysis of variance (ANOVA) was performed to assess changes in CAT scores and FEV1 over time, with Mauchly’s test for sphericity and Greenhouse-Geisser corrections applied when the assumption of sphericity was violated. For all comparative analyses, effect sizes were calculated using Cohen’s d, and 95% confidence intervals were reported to better assess the magnitude and precision of treatment effects.
The relationships between constitutional types and clinical indicators were analyzed using Spearman correlation coefficients for non-parametric data. To account for multiple comparisons in the correlation analyses, Bonferroni corrections were applied by adjusting the significance threshold to p<0.01 (0.05/5 comparisons). These correlation analyses were exploratory and cross-sectional in nature, and no causal inferences were drawn from these associations.
Treatment response rates were calculated for each group and compared using chi-square tests. Subgroup analyses were conducted based on Yin deficiency constitution status and GOLD stage to assess potential effect modifiers. Statistical significance was set at p<0.05 for primary outcomes, and all tests were two-sided.
Results
Baseline Characteristics
Table 1 presents the baseline characteristics of all participants. A total of 108 COPD patients were enrolled and assigned to either the observation group (n=54) or control group (n=54) based on the treatment received. Significant baseline differences were observed between groups. The observation group was significantly younger than the control group (64.13±15.04 vs 70.24±9.44 years, p=0.013) and had a shorter disease duration (97.61±66.59 vs 144.22±129.95 months, p=0.021). Notably, all patients in the observation group were classified as GOLD stage II (Moderate) in lung function, while in the control group, 44.4% were GOLD II and 55.6% were GOLD III (Severe) (p<0.001). These baseline differences represent a significant limitation of this retrospective study.
 |
Table 1 Baseline Characteristics of Study Participants |
For TCM constitution types, there were significant differences in Yin deficiency distribution between groups (75.9% vs 92.6%, p=0.035), while other constitution types including Yang deficiency (24.1% vs 11.1%, p=0.129), Qi deficiency (79.6% vs 83.3%, p=0.804), and Phlegm-dampness (35.2% vs 46.3%, p=0.327) showed no significant differences. Baseline CAT scores were significantly lower in the observation group (24.93±2.61 vs 26.56±3.86, p=0.012), and baseline FEV1 values were significantly higher (1.34±0.71 vs 0.85±0.38 L, p<0.001), indicating better baseline health status in the observation group.
Following propensity score matching, 43 matched pairs were included in the adjusted analysis. After matching, the baseline characteristics showed improved balance with no statistically significant differences in age (matched control: 67.8±8.7 vs matched observation: 66.2±9.5 years, p=0.37), although some differences in lung function classification remained (p=0.04), indicating residual confounding that could not be fully eliminated through matching alone.
Treatment Outcomes
Changes in CAT Scores
The observation group showed consistent improvement in CAT scores over the 6-month period, decreasing from 24.93±2.61 at baseline to 23.52±2.43 at 3 months and 22.31±2.12 at 6 months (mean improvement: 2.62 points, 95% CI: 1.87–3.37, Cohen’s d=0.78). In contrast, the control group showed slight deterioration, with scores increasing from 26.56±3.86 to 27.85±3.92 at 3 months before slightly decreasing to 26.52±3.78 at 6 months (mean change: 0.04 points, 95% CI: −0.51–0.59, Cohen’s d=0.01).
Repeated measures ANOVA revealed significant effects for group (F=34.820, p<0.001), time (F=26.668, p<0.001), and group×time interaction (F=22.012, p<0.001). After adjusting for baseline differences using ANCOVA with baseline CAT score, age, disease duration, and lung function stage as covariates, the between-group difference remained statistically significant (adjusted mean difference: 3.26 points, 95% CI: 2.38–4.14, p<0.001).
In the propensity score-matched sample, the difference in CAT score improvement remained significant (between-group difference: 2.84 points, 95% CI: 1.93–3.75, p<0.001). The clinical response rate (≥10% improvement) was substantially higher in the observation group (48.8% in matched analysis) compared to the control group (18.6% in matched analysis, p<0.001) (Figure 1A).
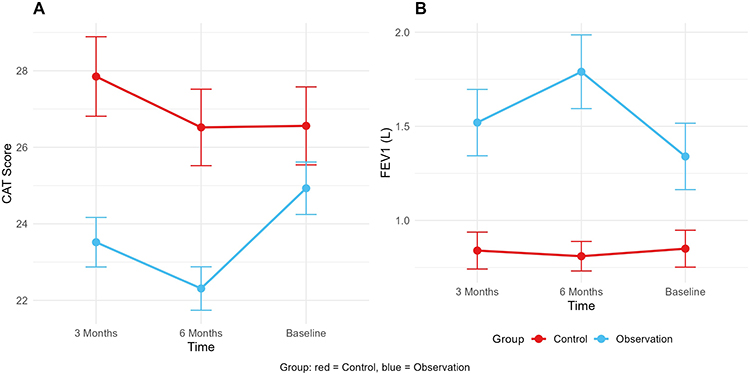 |
Figure 1 Changes in outcome measures over the 6-month treatment period. (A) CAT scores showed greater improvement in the observation group compared to the control group. (B) FEV1 values demonstrated more substantial increases in the observation group. Data are presented as mean ± SE with 95% confidence intervals. |
Changes in FEV1
FEV1 values in the observation group showed progressive improvement from baseline (1.34±0.71 L) to 3 months (1.52±0.68 L) and 6 months (1.79±0.73 L) (mean improvement: 0.45 L, 95% CI: 0.31–0.59, Cohen’s d=0.62). The control group showed minimal change, from 0.85±0.38 L at baseline to 0.84±0.36 L at 3 months and 0.81±0.35 L at 6 months (mean change: −0.04 L, 95% CI: −0.09–0.01, Cohen’s d=−0.11).
Analysis revealed significant effects for group (F=38.139, p<0.001), time (F=7.097, p=0.001), and group×time interaction (F=10.844, p<0.001). After adjusting for baseline differences using ANCOVA, the between-group difference in FEV1 change remained significant (adjusted mean difference: 0.31 L, 95% CI: 0.21–0.41, p<0.001).
In the propensity score-matched analysis, the difference in FEV1 improvement remained significant (between-group difference: 0.38 L, 95% CI: 0.27–0.49, p<0.001). The FEV1 response rate (≥12% improvement) was markedly higher in the observation group (72.1% in matched analysis) versus the control group (7.0% in matched analysis, p<0.001) (Figure 1B).
Constitution-Based Analysis
Effect of Yin Deficiency Constitution
The impact of treatment was analyzed according to Yin deficiency status. For non-Yin-deficient patients, the observation group showed mean CAT score improvements of 11.2% (95% CI: 8.6–13.8%) compared to a deterioration of −2.01% (95% CI: −4.7–0.7%) in the control group (between-group difference: 13.2%, 95% CI: 9.7–16.7%, p<0.001). Similarly, among Yin-deficient patients, the observation group demonstrated improvements of 10.2% (95% CI: 8.1–12.3%) versus minimal change (0.023%, 95% CI: −1.8–1.9%) in the control group (between-group difference: 10.2%, 95% CI: 7.7–12.7%, p<0.001).
Subgroup analysis by GOLD stage revealed that among patients with moderate COPD (GOLD II), the observation group showed a mean CAT score improvement of 10.7% (95% CI: 8.9–12.5%) compared to 0.3% (95% CI: −2.1–2.7%) in the control group (p<0.001). For patients with severe COPD (GOLD III, present only in the control group), the mean change was −0.6% (95% CI: −2.9–1.7%).
The box plot visualization shows consistently better outcomes in the observation group regardless of Yin deficiency status (Figure 2).
 |
Figure 2 Box plot showing CAT score improvement rates stratified by Yin deficiency constitution status and treatment group. The observation group (blue boxes) showed superior improvement regardless of constitution type compared to the control group (red boxes). Horizontal lines represent medians, boxes represent interquartile ranges, and whiskers extend to the most extreme data points not considered outliers. |
Correlation Analysis
The correlation matrix revealed several associations between constitutional types and clinical indicators after Bonferroni correction for multiple comparisons (adjusted significance threshold p<0.01). It is important to emphasize that these are cross-sectional correlations and do not establish causality:
Dyspnea grade showed moderate positive correlations with CAT score (r=0.37, p<0.001) and Phlegm-dampness (r=0.31, p<0.01);
CAT score demonstrated positive correlations with Phlegm-dampness (r=0.29, p<0.01);
FEV1 showed negative correlations with Yin deficiency (r=−0.37, p<0.001) and Yang deficiency (r=−0.29, p<0.01);
A negative correlation was observed between Yang deficiency and baseline FEV1 values (r=−0.34, p<0.001) (Figure 3).
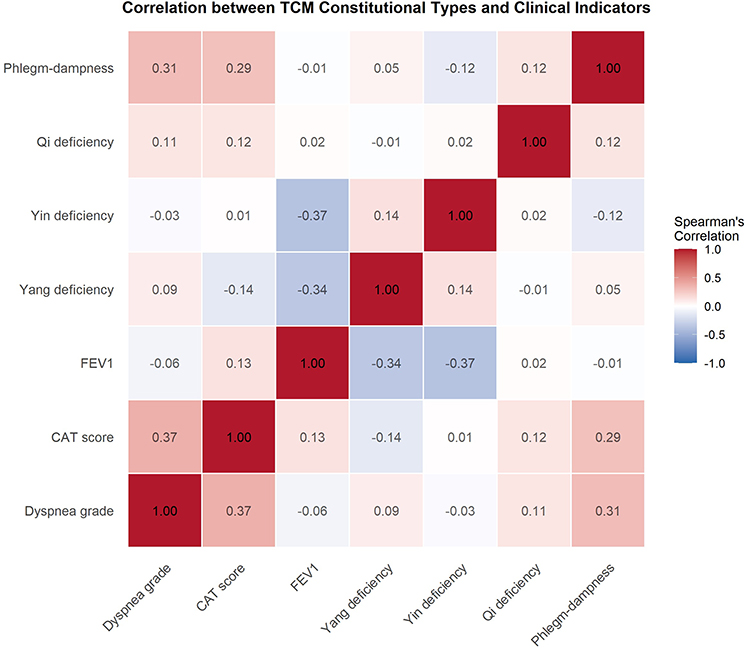 |
Figure 3 Heat map showing Spearman correlation coefficients between TCM constitutional types and clinical indicators. Color intensity indicates correlation strength, with red representing positive correlations and blue representing negative correlations. Statistically significant correlations (p<0.01 after Bonferroni correction) are shown with stronger color intensity. |
These cross-sectional correlations suggest potential associations between constitutional types and clinical presentations. However, causality cannot be inferred from these observational data, and these relationships may be confounded by unmeasured variables including disease severity, duration, and treatment history.
Discussion
This retrospective case-control study systematically evaluated the application effects of a health management model based on TCM constitution identification in COPD patients. The results indicated that the observation group, which received TCM constitution-based health management, showed significantly greater improvements in COPD Assessment Test (CAT) scores and Forced Expiratory Volume in one second (FEV1) values compared to the control group, which received routine health guidance (p<0.001). These differences remained statistically significant after propensity score matching and covariate adjustment, with moderate to large effect sizes (Cohen’s d ranging from 0.62–0.78). The clinical response rates were 48.8% versus 18.6% for CAT scores and 72.1% versus 7.0% for FEV1 values in the matched analysis, respectively.
However, it is crucial to acknowledge that significant baseline differences between groups represent a major limitation of this study and warrant cautious interpretation of these findings. The observation group was significantly younger (64.13 vs 70.24 years), had shorter disease duration (97.61 vs 144.22 months), better baseline lung function (all GOLD II vs 55.6% GOLD III), higher baseline FEV1 values (1.34 vs 0.85 L), and lower baseline CAT scores (24.93 vs 26.56). These differences likely contributed to the observed outcomes independently of the intervention itself, as patients with less severe disease, younger age, and better baseline status generally have greater capacity for improvement and slower disease progression. While we attempted to control for these differences through propensity score matching and covariate adjustment, residual confounding cannot be excluded. Therefore, the observed improvements may be partially or substantially attributed to the more favorable baseline characteristics of the observation group rather than solely to the TCM intervention.
Despite these significant limitations, the personalized intervention measures of TCM constitution-based health management may have contributed to the observed outcomes through several potential mechanisms. Systemic inflammation in patients with COPD (such as elevated IL-6 and TNF-α) may accelerate muscle atrophy and metabolic disorders, promote the occurrence of frailty, and thereby aggravate the symptoms of COPD patients.27 Among patients with stable COPD, those with Qi deficiency constitution and Yang deficiency constitution account for high proportions.28 Previous research has suggested that TCM intervention based on Qi deficiency/Yang deficiency constitution may improve FEV1 and muscle mass.29 Due to the increased load on the respiratory muscles, patients with COPD are in a long-term state of hypoxia, which further inhibits muscle anabolic metabolism, manifested as breathing difficulties and muscle weakness, forming a cycle of “hypoxia - muscle atrophy - limited movement”.30
Our intervention aimed to address these issues through tailored dietary recommendations, personalized exercise prescriptions, and specific respiratory therapy techniques. Similarly, the combination of bronchodilators and low-intensity physical activity guidance has been shown to be beneficial for COPD patients.31 By identifying the specific constitution types of patients, TCM can formulate targeted dietary, exercise, and lifestyle adjustment plans that more closely align with patients’ individual characteristics.32 For example, patients with Yin deficiency may be advised to increase the intake of Yin-nourishing foods such as pears and white fungus and to ensure adequate rest to help alleviate symptoms like dry cough and night sweats. The potential mechanism may involve restoring fluid balance and reducing airway dryness, though this hypothesis requires validation through mechanistic studies. Conversely, patients with Phlegm-dampness may be encouraged to reduce the intake of greasy foods and incorporate spleen-strengthening, dampness-resolving foods, along with moderate exercise such as Tai Chi or Qigong, to decrease phlegm accumulation and breathing difficulties. The association between Phlegm-dampness constitution and higher CAT scores and dyspnea grades observed in our correlation analysis (r=0.29–0.31, p<0.01) may reflect increased mucus hypersecretion and airway obstruction, though this remains speculative and warrants further investigation.
The negative correlations observed between Yin deficiency and FEV1 (r=−0.37, p<0.001) and between Yang deficiency and FEV1 (r=−0.29–0.34, p<0.01) are intriguing but require careful interpretation. These associations do not establish causality and may be explained by several mechanisms. Yin deficiency may be associated with fluid depletion leading to airway dryness, reduced mucociliary clearance, and increased susceptibility to infection. Yang deficiency, characterized by decreased metabolic activity and cold intolerance, may correlate with reduced physical activity, muscle weakness, and impaired respiratory muscle function. However, these cross-sectional correlations could also reflect that patients with more severe COPD (lower FEV1) are more likely to be classified as having these constitution types, rather than the constitution types causing lower FEV1. Longitudinal studies specifically designed to test these causal relationships are needed.
Moreover, the TCM constitution-based health management model emphasizes prevention, focusing on early identification of constitution types and potential health risks to implement appropriate preventive measures, which may contribute to disease management.33 This preventive health management philosophy aligns with modern medical concepts of disease prevention and health promotion.
The slight decline in FEV1 observed in the control group (from 0.85±0.38 L at baseline to 0.81±0.35 L at 6 months, decline of 40 mL over 6 months) is consistent with the natural history of COPD, which typically involves progressive airflow limitation over time. Various studies have reported annual FEV1 decline rates ranging from 33–79 mL/year in COPD patients receiving conventional treatment.34,35 Our finding falls within this expected range and may represent the natural disease progression in this more severe patient subgroup. However, it is important to note that measurement variability, the retrospective nature of data collection, and potential differences in spirometry technique or equipment calibration between time points may have also contributed to this observation. The control group’s higher proportion of GOLD stage III patients (55.6% vs 0%) would be expected to show faster decline, which emphasizes the importance of baseline matching in future prospective studies.
The subgroup analysis revealed that among patients with Yin deficiency constitution, those receiving TCM constitution-based health management showed significantly greater improvements in CAT scores compared to the control group (10.2% improvement vs 0.023% change, p<0.001). This finding suggests that the TCM constitution-based health management model may be adaptable for specific constitution types. However, this interpretation must be tempered by the recognition that the observation group’s better baseline characteristics may have facilitated greater response potential regardless of constitution type. Yin deficiency typically manifests as dry cough and night sweats, and targeted Yin-nourishing interventions through diet (pears, white fungus, lily bulbs), herbal medicine (Sha Shen Mai Dong Tang modifications), and lifestyle adjustments (adequate rest, avoiding overexertion) may help alleviate these symptoms.36 This preliminary finding, while requiring validation in prospective studies, supports the potential application of TCM constitution identification in COPD management and suggests differential responses to health management interventions among different constitution types, providing considerations for future personalized treatment strategies.37
TCM theory posits that emotional imbalance is a significant factor in disease onset or exacerbation. By addressing emotional regulation, TCM interventions may improve patients’ overall health. For instance, TCM often employs acupuncture, massage, herbal medicine, and psychological counseling to help patients regulate emotions and alleviate stress, thereby potentially promoting physiological function recovery.38 In COPD management, emotional regulation may not only improve patients’ mental health but also enhance self-management abilities.39
Specifically, for COPD patients with Yin deficiency, the TCM constitution-based health management model optimizes dietary structures by increasing the intake of Yin-nourishing foods, combines appropriate herbal treatments (such as Sha Shen and Mai Dong), and incorporates moderate exercise training, which may help alleviate symptoms like dry cough and night sweats, thereby potentially improving sleep quality and overall health.40 Additionally, emotional regulation and psychological support may play roles in the health management of Yin deficiency patients, potentially helping them reduce psychological stress and support immune function.41
Previous studies have examined various aspects of TCM interventions in COPD. Research has demonstrated that personalized interventions based on TCM constitution identification may improve lung function and quality of life in COPD patients, especially in those with Qi deficiency and Yin deficiency constitution types.42,43 Other studies have suggested that TCM constitution-based health management models may reduce the incidence of acute exacerbations in COPD patients through multifaceted interventions.44 Specific TCM therapies have also shown promise: herbal formulations such as Bufei Yishen granules have demonstrated improvements in lung function and quality of life,45 acupuncture therapy has shown benefits in reducing dyspnea,46 and traditional exercises like Tai Chi and Qigong have been incorporated into pulmonary rehabilitation programs with positive outcomes.47,48 These findings from the literature provide context for our comprehensive intervention model, though direct comparisons are limited by differences in study design, patient populations, and outcome measures.
However, our study has several important limitations that must be acknowledged. First and most importantly, the substantial baseline differences between groups represent a fundamental limitation of this retrospective design. Despite our statistical attempts to control for these differences through propensity score matching and covariate adjustment, the observation group’s younger age, shorter disease duration, better baseline lung function (all GOLD II vs 55.6% GOLD III), higher baseline FEV1 values, and lower baseline CAT scores may have influenced treatment responses independently of the intervention itself. Patients with less severe disease and better baseline status generally have greater capacity for improvement, making it difficult to isolate the true effect of the TCM intervention from the effect of more favorable baseline characteristics. This limitation is inherent to retrospective case-control designs and cannot be fully overcome through statistical adjustment alone.
Second, the retrospective case-control design is inherently susceptible to selection bias and information bias. The allocation to observation versus control groups was based on treatment received rather than random assignment, introducing the possibility of systematic differences beyond those we could measure and control for. Patients who received TCM constitution-based management may have differed in unmeasured ways (such as motivation, health beliefs, socioeconomic status, or social support) that could independently influence outcomes.
Third, the assessment of TCM constitution relies on the experience and judgment of physicians, introducing potential subjectivity. While we used a standardized assessment tool (CCMQ) and demonstrated good inter-rater reliability (weighted κ=0.81, ICC=0.88), the subjective nature of constitutional assessment remains a limitation. Future research should explore more objective biomarkers or quantitative assessment methods to complement subjective evaluations. Additionally, while we reported on four main constitution types relevant to COPD (Yin deficiency, Yang deficiency, Qi deficiency, and Phlegm-dampness), the complete CCMQ assesses nine constitution types, and patients may have multiple constitution types simultaneously. A more comprehensive analysis of all constitution types and their combinations may provide additional insights.
Fourth, our outcome assessments were not conducted in a blinded manner for all measures. While pulmonary function technicians performed spirometry according to standardized protocols, the assessment of CAT scores and the provision of care were not blinded to group allocation. This may introduce measurement bias, particularly for subjective measures like the CAT score, where patients’ knowledge of receiving a “special” intervention might influence their reporting (potential Hawthorne effect or placebo response).
Fifth, the single-center nature of our study conducted at one tertiary hospital in Handan City limits generalizability. The specific patient population, healthcare delivery system, expertise of TCM practitioners, and local practice patterns may differ from other settings. The relatively small sample size (108 total, 43 matched pairs) further restricts statistical power and the ability to detect smaller effects or conduct more detailed subgroup analyses.
Sixth, while we observed improvements over a 6-month period, this timeframe is relatively short for a chronic progressive disease like COPD. Longer follow-up is essential to determine the sustainability of these benefits and the impact on important clinical outcomes such as exacerbation rates, hospitalizations, mortality, and long-term disease progression. The natural variability in COPD symptoms and lung function over 6 months may not fully capture the true treatment effect.
Seventh, we did not systematically collect data on acute exacerbations, inflammatory biomarkers (such as serial CRP, IL-6, TNF-α measurements), or other important clinical outcomes beyond CAT scores and FEV1. Exacerbation prevention is a key goal of COPD management, and future studies should include comprehensive assessment of exacerbation frequency, severity, and time to first exacerbation. Similarly, inflammatory marker data could provide mechanistic insights into how TCM interventions may work, if indeed they do.
Eighth, although our intervention included multiple components (dietary recommendations, exercise prescriptions, herbal medicine, lifestyle modifications, and physical therapy techniques), we did not systematically evaluate which specific components contributed most to the observed outcomes or their relative contributions. This makes it difficult to identify the “active ingredients” of the intervention and to optimize the treatment protocol. Component analysis in future studies would be valuable.
Ninth, considering the long-term use of TCM, some herbal components (such as those containing aristolochic acid or Polygonum multiflorum) have been associated with potential liver toxicity or other adverse effects.49 Our study did not systematically track and report adverse events or safety outcomes related to the TCM interventions, which is an important limitation. Future studies should include comprehensive safety monitoring, including liver function tests, renal function tests, and systematic adverse event reporting.
Finally, we did not assess treatment adherence, intervention fidelity, or implementation quality in detail. Variations in how the TCM constitution-based intervention was delivered, patient adherence to prescribed treatments, or the quality of conventional care in the control group could all influence outcomes and introduce additional variability.
Despite these substantial limitations, our study provides preliminary observational evidence that suggests potential value of TCM constitution-based health management approaches in COPD care. However, these findings must be interpreted with considerable caution given the methodological constraints. The results should be viewed as hypothesis-generating rather than conclusive. Well-designed prospective randomized controlled trials with matched cohorts at baseline, larger sample sizes, blinded outcome assessment, longer follow-up periods, comprehensive outcome measures including exacerbations and biomarkers, safety monitoring, and multi-center designs are essential to establish efficacy and safety definitively. Such studies should also include detailed component analysis, mechanistic investigations, cost-effectiveness evaluations, and pragmatic assessments of implementation in real-world clinical settings.
Conclusion
This retrospective study provides preliminary evidence suggesting that TCM constitution-based health management may be associated with improvements in clinical symptoms and lung function in COPD patients. However, significant baseline differences between groups, including younger age, shorter disease duration, and better baseline lung function in the observation group, represent major limitations that substantially affect the interpretation of these findings. The observed benefits may be partially or largely attributable to these more favorable baseline characteristics rather than to the intervention itself. Additionally, the retrospective design, lack of randomization, small sample size, single-center setting, short follow-up duration, and absence of comprehensive safety monitoring further limit the conclusions that can be drawn.
While these findings suggest that TCM constitution-based approaches warrant further investigation as a potential complementary strategy to conventional COPD management, they should be interpreted with considerable caution. Definitive conclusions about efficacy and safety cannot be made based on this retrospective analysis alone. Well-designed prospective randomized controlled trials with proper baseline matching, blinded outcome assessment, larger sample sizes, multi-center designs, longer follow-up periods, comprehensive outcome measures including exacerbations and biomarkers, and systematic safety monitoring are essential to establish whether this approach provides genuine clinical benefit beyond standard care.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Affiliated Hospital of Hebei University of Engineering (Protocol No.: 2024[K]078). Due to the retrospective nature of the study and the use of anonymized patient information, informed consent was waived with the approval of the Ethics Committee of Affiliated Hospital of Hebei University of Engineering. All methods were carried out in accordance with relevant guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Application of health management model based on TCM constitution identification in COPD patients (2025052).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Hu W, Fang L, Zhang H, et al. Global disease burden of COPD from 1990 to 2019 and prediction of future disease burden trend in China. Public Health. 2022;208:89–97. doi:10.1016/j.puhe.2022.04.015
3. Guo B, Wang Y, Pei L, et al. Determining the effects of socioeconomic and environmental determinants on chronic obstructive pulmonary disease (COPD) mortality using geographically and temporally weighted regression model across Xi’an during 2014-2016. Sci Total Environ. 2021;756:143869. doi:10.1016/j.scitotenv.2020.143869
4. Soler-Cataluña JJ, Novella L, Soler C, et al. Clinical characteristics and risk of exacerbations associated with different diagnostic criteria of asthma-COPD overlap. Arch Bronconeumol. 2020;56(5):282–290. doi:10.1016/j.arbres.2019.08.023
5. Aisanov Z, Khaltaev N. Management of cardiovascular comorbidities in chronic obstructive pulmonary disease patients. J Thorac Dis. 2020;12(5):2791–2802. doi:10.21037/jtd.2020.03.60
6. Agustí A, Vogelmeier C, Faner R. COPD 2020: changes and challenges. Am J Physiol Lung Cell Mol Physiol. 2020;319(5):L879–L883. doi:10.1152/ajplung.00429.2020
7. Watson A, Wilkinson TMA. Digital healthcare in COPD management: a narrative review on the advantages, pitfalls, and need for further research. Ther Adv Respir Dis. 2022;16:17534666221075493. doi:10.1177/17534666221075493
8. Zhao X, Tan X, Shi H, et al. Nutrition and traditional Chinese medicine (TCM): a system’s theoretical perspective. Eur J Clin Nutr. 2021;75(2):267–273. doi:10.1038/s41430-020-00737-w
9. Higgins V, Sohaei D, Diamandis EP, et al. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. 2021;58(5):297–310. doi:10.1080/10408363.2020.1860895
10. Bai F, Luo H, Wang L, et al. A meta-analysis of the association between diabetes mellitus and traditional Chinese medicine constitution. Evid Based Complement Alternat Med. 2021;2021:6390530. doi:10.1155/2021/6390530
11. Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122. doi:10.1186/1465-9921-11-122
12. Li SY, Li JS, Wang MH, et al. Effects of comprehensive therapy based on traditional Chinese medicine patterns in stable chronic obstructive pulmonary disease: a four-center, open-label, randomized controlled study. BMC Complement Altern Med. 2012;12:197. doi:10.1186/1472-6882-12-197
13. Yi Q, Li F, Lei S, et al. Clinical efficacy and safety of the self-developed zangsiwei qingfei mixture combined with conventional treatment in patients with acute exacerbation of chronic obstructive pulmonary disease. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024;49(6):921–931. doi:10.11817/j.issn.1672-7347.2024.230546
14. Gao Z, Jing J, Liu Y. Xiaoqinglong decoction (a traditional Chinese medicine) combined conventional treatment for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Medicine. 2020;99(14):e19571. doi:10.1097/MD.0000000000019571
15. Liu H, Cheng N. Effect of Tai Ji and/or Qigong on patients with stable chronic obstructive pulmonary disease: a meta-analysis and systematic review. Medicine. 2025;104(5):e41390. doi:10.1097/MD.0000000000041390
16. Sujie M, Kaiwen X, Hong X, Xiujin G. The impact of traditional mind-body exercises on pulmonary function, exercise capacity, and quality of life in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials. Front Med. 2024;11:1359347. doi:10.3389/fmed.2024.1359347
17. Chen X, Jiang X, Zhang X, et al. Assessing the impact of diverse mask types on COPD patients: a randomised controlled trial study protocol. BMJ Open. 2024;14(1):e080721. doi:10.1136/bmjopen-2023-080721
18. Luo Q, Peng B, Wei X, et al. Research progress of Chinese herbal medicines and classic prescriptions in the treatment of COPD based on the TCM theory and medicinal characteristics. Sci Tradit Chin Med. 2024;2(2):104–120. doi:10.1097/st9.0000000000000028
19. Huang Q, Lin P, Dang J, et al. Effect of internet-based self-management on pulmonary function rehabilitation and living quality in patients with chronic obstructive pulmonary disease. Am J Transl Res. 2021;13(5):5224–5231.
20. Ren M, Guo LP, Sun X, et al. Based on the process management of traditional Chinese medicine comprehensive intervention method on outcomes in patients with mild/moderate chronic obstructive pulmonary disease: study protocol for a practical randomized controlled trial. TMR Integr Med. 2018;2(4):197–201.
21. Zhu YB. Preliminary assessment on performance of constitution in Chinese medicine questionnaire. Chin J Clin Rehabil. 2006;10(3):15–17.
22. Wang Q. Classification and Determination of Constitution in Traditional Chinese Medicine [in Chinese]. Beijing: Sci. Press; 2009.
23. Chronic Obstructive Pulmonary Disease Integrated Traditional Chinese and Western Medicine Management Expert Consensus Writing Group. Expert consensus on integrated traditional Chinese and Western medicine management of chronic obstructive pulmonary disease (2023). Gen Pract Chin. 2023;26(35):4359–4371. doi:10.12114/j.issn.1007-9572.2023.0348
24. Chinese Nutrition Society. Dietary Guidelines for Chinese Residents: 2022. Beijing: PMPH; 2022.
25. Chinese Thoracic Society, Chinese Medical Association; Respiratory Rehabilitation Committee of Chinese Rehabilitation Medical Association; Editorial Board of Chinese Journal of Health Management. Guidelines for respiratory rehabilitation of chronic obstructive pulmonary disease in China (2021). Chin J Health Manag. 15;2021. doi:10.3760/cma.j.cn115624-20211011-00595
26. Chinese Pharmacopoeia Commission. Pharmacopoeia of the People’s Republic of China, Volume I. Beijing: CMSP; 2020.
27. Verduri A, Clini E, Carter B, et al. Impact of frailty on symptom burden in chronic obstructive pulmonary disease. J Clin Med. 2024;13(4):984. doi:10.3390/jcm13040984
28. Liang KY, Fu ZY, Zhou LM, et al. The relationship between TCM constitutional classification and life quality of patients with stable COPD. J Shaanxi Univ Chin Med. 2017;40(6):37–40.
29. Wang J, Zhang L, Chen X, et al. Personalized traditional Chinese medicine based on constitutional differentiation improves pulmonary function and nutritional status in stable COPD: a randomized controlled trial. J Ethnopharmacol. 2022;285:114853.
30. Li Y, Wang H, Zhang X, et al. Hypoxia-induced skeletal muscle atrophy in COPD: mechanisms and therapeutic targets. Respir Res. 2023;24(1):45.
31. Matsunaga K, Harada M, Suizu J, et al. Comorbid conditions in chronic obstructive pulmonary disease: potential therapeutic targets for unmet needs. J Clin Med. 2020;9(10):3078. doi:10.3390/jcm9103078
32. Li L, Yao H, Wang J, et al. The role of Chinese medicine in health maintenance and disease prevention: application of constitution theory. Am J Chin Med. 2019;47(3):495–506. doi:10.1142/S0192415X19500253
33. Huang P, Lin X, Liu Y, et al. The efficacy and safety of combined traditional Chinese and western medicine in the treatment of chronic obstructive pulmonary disease complicated with respiratory failure: a systematic review and meta-analysis study. Ann Palliat Med. 2022;11(3):1102–1111. doi:10.21037/apm-22-272
34. Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 Second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. doi:10.1056/NEJMoa1105482
35. Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:95–99. doi:10.2147/COPD.S27480
36. Lin D, Li S, Hou C, et al. Exploring the biological mechanism of qi deficiency syndrome with chronic obstructive pulmonary disease (COPD) based on integrated pharmacology. J Tradit Chin Med Sci. 2021;8(1):72–81. doi:10.1016/j.jtcms.2021.01.003
37. Cao X, Wang Y, Chen Y, et al. Advances in traditional Chinese medicine for the treatment of chronic obstructive pulmonary disease. J Ethnopharmacol. 2023;307:116229. doi:10.1016/j.jep.2023.116229
38. Gao F, Deng K, Hu C. Construction of TCM health management model for patients with convalescence of coronavirus disease based on artificial intelligence. In:
39. Volpato E, Poletti V. Navigating the behavioral and psychological dimensions of chronic obstructive pulmonary disease (COPD). In: Handbook of the Behavior and Psychology of Disease. Cham: Springer International Publishing; 2024:1–25.
40. Yu L, Yajing T, Lijun S. Study on the influence of lifestyle on constitution, health and disease of residents in Guanzhong area of Shaanxi Province. Acad J Med Health Sci. 2023;4(10):1–8.
41. Huang WL. The treatment of asthma based on traditional Chinese medicine and homeopathy. J Pediat Infants. 2018;1(1):24–30.
42. Li H, Guo P, Gao W, et al. Patient-reported outcome measures for advanced cancer in China: a systematic review of cross-cultural adaptation and psychometric properties. J Cancer Policy. 2023;35:100371. doi:10.1016/j.jcpo.2022.100371
43. Zhang P, Ren J, Xu B, et al. Further refinement is required for patient-reported outcome scales for respiratory diseases based on traditional Chinese medicine theory for applicability. Int J Gen Med. 2023;16:6099–6113. doi:10.2147/IJGM.S438297
44. Zhong LL, Wong YP, Leung CY, et al. Effects of Chinese medicine for COVID-19 rehabilitation: a multicenter observational study. Chin Med. 2022;17(1):99. doi:10.1186/s13020-022-00654-z
45. Li J, Zhang H, Ruan H, et al. Effects of Chinese herbal medicine on acute exacerbations of COPD: a randomized, placebo-controlled study. Int J Chron Obstruct Pulmon Dis. 2020;15:2901–2912. doi:10.2147/COPD.S276082
46. Han B, Pan Y, Li H. Recent research advancements in interventions and assessments related to chronic obstructive pulmonary disease rehabilitation. J Biomed Nanotechnol. 2023;19(2):228–233. doi:10.1166/jbn.2023.3532
47. Gendron LM, Nyberg A, Saey D, Maltais F, Lacasse Y. Active mind-body movement therapies as an adjunct to or in comparison with pulmonary rehabilitation for people with chronic obstructive pulmonary disease. Cochrane. Database Syst Rev. 2018;10(10):CD012290. doi:10.1002/14651858.CD012290.pub2
48. Zhang M, Xv G, Luo C, et al. Qigong Yi Jinjing promotes pulmonary function, physical activity, quality of life and emotion regulation self-efficacy in patients with chronic obstructive pulmonary disease: a pilot study. J Altern Complement Med. 2016;22(10):810–817. doi:10.1089/acm.2015.0224
49. Debelle FD, Vanherweghem JL, Nortier JL. Aristolochic acid nephropathy: a worldwide problem. Kidney Int. 2008;74(2):158–169. doi:10.1038/ki.2008.129
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis of the TCM “Yupingfeng Granules” in the Treatment of Acute Exacerbations of COPD Based on a Randomized Clinical Trial
Hu M, Ding P, Ma J, Yang N, Zheng J, Zhou N
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2369-2379
Published Date: 23 September 2022
Respiratory Symptoms, Disease Burden, and Quality of Life in Australian Adults According to GOLD Spirometry Grades: Data from the BOLD Australia Study
Zhou Y, Ampon MR, Abramson MJ, James AL, Maguire GP, Wood-Baker R, Johns DP, Marks GB, Reddel HK, Toelle BG
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2839-2847
Published Date: 30 November 2023