Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Application and Delphi Validation of an Omaha System–Based Evaluation Index for Post-PCI Rehabilitation Nursing
Authors Wu L, Gong Y, Liu X, Ning Y, Song J, Zhang Z, Zhou H, Xiong H
Received 8 August 2025
Accepted for publication 20 January 2026
Published 13 February 2026 Volume 2026:19 559427
DOI https://doi.org/10.2147/JMDH.S559427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Charles V Pollack
Lili Wu,1 Yahui Gong,1 Xueli Liu,1 Yaqian Ning,1 Jianlan Song,1 Zhifu Zhang,1 Hairong Zhou,1 Haiyan Xiong2
1General Medicine Department, People’s Hospital of Longhua, Shenzhen, 518109, People’s Republic of China; 2Nursing Department, People’s Hospital of Longhua, Shenzhen, 518109, People’s Republic of China
Correspondence: Haiyan Xiong, Nursing Department, People’s Hospital of Longhua, No. 38 Jinglong Construction Road, Shenzhen, 518109, People’s Republic of China, Tel +86-13713832572, Email [email protected] Hairong Zhou, General Medicine Department, People’s Hospital of Longhua, No. 38 Jinglong Construction Road, Shenzhen, 518109, People’s Republic of China, Tel +86-15012613566, Email [email protected]
Background: This study aimed to develop an evaluation index system based on the Omaha System to identify postoperative rehabilitation nursing problems in patients after percutaneous coronary intervention (PCI). This evaluation system aims to facilitate the timely identification of nursing problems and enhance the reliability of nursing interventions during postoperative rehabilitation.
Methods: Rehabilitation nursing problems were identified through a comprehensive literature review and case analysis, considering both the physical and psychological characteristics of post-PCI patients. These problems were classified and organized according to the Omaha System. From September 2020 to February 2021, Delphi consultations were conducted with experts in China to finalize the evaluation indicators.
Results: After two rounds of expert consultation, the authority coefficients of the experts were 0.858 and 0.875, and Kendall’s W coefficients were 0.194 and 0.150, respectively (both P < 0.01), indicating consensus. The final evaluation index system comprised 4 first-level indicators (domains), 21 second-level indicators (nursing problems), and 130 third-level indicators (specific symptoms/signs).
Conclusion: The Omaha System-based evaluation index developed in this study offers a clinically applicable framework for identifying and managing rehabilitation nursing problems in PCI patients. Supporting comprehensive and systematic assessment provides nurses with clear guidance for problem recognition, individualized care planning, and outcome monitoring. Its application has the potential to enhance care consistency, improve patient recovery, and promote evidence-based nursing decision-making, thereby contributing to improved quality of post-PCI rehabilitation care in clinical practice.
Keywords: coronary heart disease, percutaneous coronary intervention, Omaha System, index system, Delphi method, cardiovascular nursing, nursing care
Introduction
Coronary heart disease (CHD) remains the leading cause of morbidity and mortality in China and globally.1,2 The steadily rising incidence of CHD poses a significant threat to public health, making it a critical global concern.3 Percutaneous coronary intervention (PCI) is currently a primary treatment for CHD. Although it effectively alleviates vascular stenosis and occlusion,4 it does not halt or reverse the pathological process of coronary atherosclerosis.5 Consequently, patients who undergo PCI remain at risk for recurrent arterial stenosis or occlusion, which may necessitate secondary surgical interventions or result in adverse outcomes, including death,6 thereby severely impairing quality of life. Given these challenges, comprehensive nursing interventions addressing a range of factors are needed, including adverse environmental conditions,7 physiological imbalances,8 psychosocial stressors,9 and unhealthy behaviors,1 all of which can affect rehabilitation outcomes. Therefore, developing a scientific, comprehensive, and feasible evaluation index system for identifying postoperative rehabilitation nursing problems in patients undergoing PCI is of great clinical significance. This system may play a pivotal role in delaying CHD progression, preventing complications, and improving long-term health outcomes.
The Omaha Problem Classification System is a nursing taxonomy developed in the 1970s in Omaha, USA.10 After decades of refinement and practical application, it has evolved into a standardized terminology system encompassing four domains, 42 nursing problem categories, and 256 symptoms and signs, supporting structured problem assessment and care planning. Internationally, several established nursing classification frameworks exist, such as NANDA-International for diagnostic terminology,11 the Nursing Interventions Classification for intervention coding,12 and the Nursing Outcomes Classification for outcome evaluation.13 While these systems have contributed significantly to the professionalization of nursing, they typically emphasize one dimension of care, such as diagnosis, intervention, or outcomes. In contrast, the Omaha System embeds a “problem-intervention-outcome” cycle that enables comprehensive assessment, targeted planning, and dynamic evaluation, making it well-suited for rehabilitation settings that require systematic follow-up, such as post-PCI care.14,15 Although the Omaha System has been widely applied in community health and chronic disease management in China,8,16,17 its use in constructing evaluation index systems for postoperative rehabilitation nursing problems in patients after PCI remains limited.
The nursing process is fundamental to nursing practice, and nursing assessment is an indispensable step.18 Accurate assessment enables healthcare professionals to identify patient-specific nursing problems and develop individualized nursing plans.19 Numerous studies have validated the problem classification table in the Omaha System as comprehensive and practical,20–22 supporting its application in diverse clinical settings. While the Omaha System is used in chronic disease management, a standardized, comprehensive assessment tool specifically for post-PCI rehabilitation nursing problems is lacking.
The present study employed the Delphi expert consultation method, using the Omaha Problem Classification System as its theoretical framework. By integrating existing research with clinical experience, the study aimed to develop an evaluation index system to identify postoperative rehabilitation nursing issues among patients undergoing PCI in China. This system is expected to enhance early detection and timely management of nursing problems, thereby improving patient outcomes and the quality of nursing care.
Methods
Research Team Composition
A multidisciplinary research team was established comprising six members: two cardiovascular surgeons (one chief physician and one associate chief physician), two cardiovascular nursing specialists (each a deputy chief nurse), one university internal medicine nursing educator (associate professor), and one graduate student specializing in nursing. All members had professional experience in cardiovascular medicine and nursing. Their responsibilities included identifying postoperative rehabilitation nursing problems in PCI patients based on a literature review and case analysis, classifying and organizing these problems using the Omaha System, designing an expert consultation questionnaire, and summarizing, analyzing, and interpreting the consultation results.
Development of Initial Evaluation Indicators for Postoperative Rehabilitation Nursing Problems
Literature Review
Articles were systematically screened from both Chinese databases (CNKI, Wanfang, VIP, CBM) and English databases (PubMed, Medline, Web of Science) from January 2011 to August 2020. The search strategy included the following terms: (“Coronary Heart Disease” OR “CHD”) AND (“Percutaneous Coronary Intervention” OR “PCI”) AND (“nursing” OR “nursing problems” OR “symptoms” OR “signs” OR “rehabilitation”). Equivalent Chinese search terms were applied for the Chinese databases.
Inclusion criteria were: (1) studies involving patients undergoing PCI; (2) studies addressing nursing problems, symptoms, signs, or health needs during the post-PCI rehabilitation period; (3) original research, reviews, or systematic reviews; and (4) publications in either Chinese or English. Exclusion criteria included: (1) studies with unavailable or unextractable data; (2) duplicate publications; (3) studies unrelated to the research topic; and (4) conference abstracts, commentaries, or animal studies.
The initial search yielded 386 articles. After screening titles and abstracts to remove duplicates and studies that did not meet the inclusion criteria, we were left with 89 articles. Full-text review further excluded irrelevant studies, resulting in a final set of 42 articles. From these, relevant findings related to post-PCI rehabilitation nursing problems, including symptoms, signs, and health needs, were extracted, analyzed, and summarized.
Case Analysis
To supplement the literature review, a retrospective analysis of medical records was conducted for 138 patients who underwent PCI and were hospitalized at Longhua District People’s Hospital, Shenzhen, China, between September and December 2020. Data were obtained from the hospital information system and nursing documentation system.
Two trained researchers independently reviewed the electronic medical records, focusing on the following sources: admission assessments (including chief complaints, history of present illness, and past medical history); nursing records documenting physiological, psychological, behavioral, and social symptoms or problems; progress notes and handover reports detailing changes in condition, complications, and interventions; and discharge assessments and education records noting health issues at discharge and patient/family guidance.
Content analysis was applied to identify and code explicit or implicit health problems within the records. For example, statements such as “the patient reports chest pain”, “nurse observed hematoma at the puncture site”, “the patient feels anxious about post-discharge medication”, or “family reports high-salt dietary habits” were coded respectively as “pain”, “circulatory dysfunction”, “anxiety”, and “nutritional imbalance”. Each extracted “problem-symptom/sign” pair was then compared and categorized according to the Omaha System problem classification framework. Items without a direct match were assigned to the closest relevant category or discussed within the research team to determine the most appropriate classification.
This study was approved by the Ethics Committee of Longhua District People’s Hospital. It adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study. Patient data were anonymized and kept confidential in accordance with ethical guidelines.
Standardization of Nursing Problems
Findings from the literature review and case analysis were integrated and analyzed. Using the Omaha Problem Classification Scheme, nursing problems were standardized in terminology and categorized into four domains: physiological, environmental, psychosocial, and health-related behaviors. This process produced a preliminary draft of the evaluation index system comprising 4 first-level indicators (domains), 23 second-level indicators (nursing problems), and 141 third-level indicators (specific symptoms/signs).
Expert Consultation
Development of the Expert Consultation Questionnaire
The expert consultation questionnaire was designed based on the preliminary set of evaluation indicators. It consisted of three components: (1) Letter to experts: outlines the research background, objectives, and instructions for completing the questionnaire; (2) Main questionnaire body: presents the evaluation indicators for postoperative rehabilitation nursing problems in PCI patients according to the Omaha System. The importance of each indicator was rated on a 5-point scale: 5, very important; 4, important; 3, neutral; 2, unimportant; 1, very unimportant. An open comment section was provided for qualitative suggestions. (3) Expert basic information: This section includes personal and professional information, such as education level, institution, professional title, and current work status. In addition, experts reported their familiarity with the Omaha System and clinical nursing knowledge regarding CHD. A survey section assessed the basis of their judgment in four dimensions: theoretical analysis, practical experience, relevant materials, and subjective feelings, and the authority coefficient was calculated. Each dimension was rated as having high, medium, or low influence, with coefficients ranging from 0.05 to 0.50.
Selection of Experts
Expert candidates were invited based on their attendance at relevant academic conferences and authorship of publications. Experts were then selected according to the following inclusion criteria: (1) Employment in tertiary grade A hospitals or higher institutions; (2) professional title of intermediate level or above; (3) at least 10 years of relevant professional experience and familiarity with the Omaha System; (4) Willingness to participate voluntarily, confirmed by prior communication via WeChat, phone, or email.
Experts rated their familiarity with two knowledge areas, clinical nursing of myocardial infarction and the Omaha classification system, on a five-point scale: very familiar (1.0), quite familiar (0.8), average (0.6), not very familiar (0.4), and unfamiliar (0.2).
The Delphi method recommends an optimal panel size of 15–50 experts.23 Ultimately, 16 qualified experts were selected for this study. No member of the research team was included in the expert panel.
Implementation of Delphi Expert Consultation
Experts were contacted in advance to obtain informed consent via email or WeChat. The Delphi process was conducted in two rounds between September 2020 and February 2021. In each round, experts rated the importance of each indicator and could provide suggestions for modifications. After the first round, the research team analyzed the responses and adjusted the indicator set based on the screening criteria and expert feedback. The inclusion criteria24 for retaining an indicator were: mean importance score > 3.5 and coefficient of variation < 0.25. Proposed additions, deletions, or modifications to indicators were reviewed and decided through group discussion within the research team. Results from the first round were provided to the experts in the second round to facilitate consensus building. A flowchart illustrating the two rounds of Delphi expert consultation is shown in Figure 1.
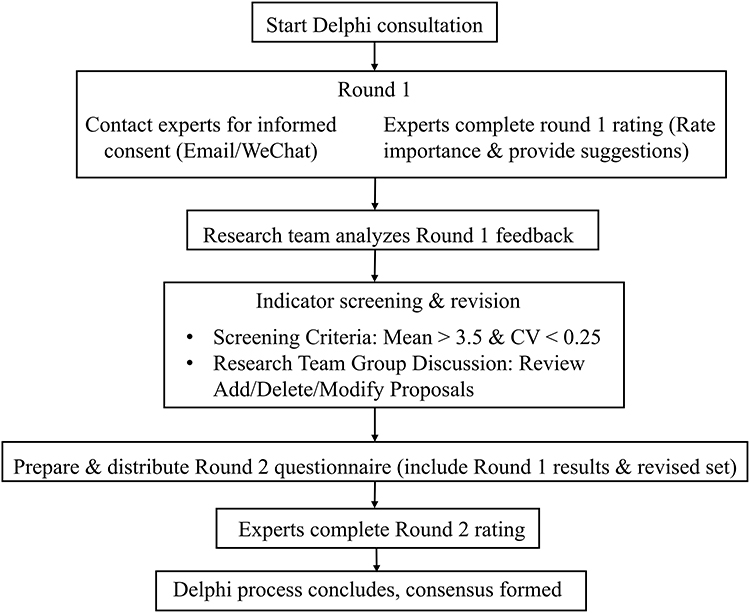 |
Figure 1 Flow diagram illustrating the two rounds of Delphi consultation. |
Statistical Methods
Data were processed and analyzed using Microsoft Excel 2020 and SPSS 25.0. Descriptive statistics, including means and standard deviations, were used to summarize continuous variables. To assess expert engagement and the reliability of the Delphi process, the following indicators were analyzed: (1) Response rate to evaluate expert enthusiasm; (2) Expert authority coefficient to measure the credibility of expert judgments; (3) Kendall’s coefficient of concordance (W) to determine the level of agreement; (4) weights of second-level indicators (nursing problems); and (5) mean importance scores and coefficient of variation.
Results
Characteristics of Participating Experts
Two rounds of Delphi consultation were conducted with 16 experts. They represented diverse professional backgrounds, including nursing management, clinical nursing practice, nursing education, and clinical medicine. Experts were affiliated with six tertiary hospitals and two universities in Guangdong Province, China. They had a median age of 39 (interquartile range: 34–53) years and 17 ± 6.351 years of work experience (range: 8–32 years). Ten experts held a master’s degree or above (62.5%), and 6 held a bachelor’s degree (37.5%). Half (50.0%) had senior or associate senior titles, and the other half (50.0%) had intermediate titles.
Expert Enthusiasm
Expert enthusiasm was assessed using the consultation response rate. In the first round, 16 questionnaires were distributed, and 15 valid responses were received, yielding an effective response rate of 93.75%. In the second round, all 15 distributed questionnaires were returned, for an effective response rate of 100%. An effective response rate of 70% or more indicates high expert engagement.25 The demographic and professional characteristics of the 15 experts are shown in Supplementary Table 1.
Expert Authority
In the first round of expert consultation, the average familiarity coefficient among the experts was 0.850, indicating a high level of self-reported familiarity with the relevant knowledge areas. In the second round, the average familiarity coefficient (Cs) increased to 0.867. The average judgment coefficient, reflecting the experts’ evaluation of the basis for their judgments (ie, theoretical analysis, practical experience, relevant materials, and subjective feelings), was 0.867 and 0.883 for the first and second rounds, respectively. The authority coefficient reflects the reliability of expert judgment. The authority coefficient values for the two Delphi rounds were 0.858 and 0.875, respectively, indicating a high level of authority. An authority coefficient above 0.7 suggests strong expert credibility.21
Expert Consensus
Expert consensus was evaluated using Kendall’s W coefficients, which indicate the consistency of expert ratings on indicators.26 In the first consultation round, Kendall’s W was 0.194 (χ² = 407.139, P < 0.01) for primary indicators and 0.150 (χ² = 289.295, P < 0.01) for secondary indicators. In the second round, consensus markedly increased, with Kendall’s W increasing to 0.867 (χ² = 260.000, P < 0.01) for primary indicators and 0.809 (χ² = 1566.306, P < 0.01) for secondary indicators. These results indicate a statistically significant level of agreement among experts on postoperative rehabilitation nursing problems in PCI patients.
Expert Feedback on the Postoperative Rehabilitation Nursing Problem Assessment Tool Based on the Omaha System
After each round of expert consultation, the research team carefully reviewed expert feedback. Experts were invited to provide additional information or clarification when their opinions were unclear. In the first round, 45 opinions were received from 15 experts. After two consultation rounds, the indicator system was refined as follows: (1) All first-level indicators (domains) were retained without modification; (2) Two second-level indicators (nursing problems) were removed: “neighborhood/workplace safety” and “cognition”, along with their associated third-level indicators; (3) Nine third-level indicators (symptoms/signs) were deleted; (4) Eight third-level indicators were added; (5) Nine third-level indicators were revised for clarity.
By the second round of consultation, expert opinions had converged, and consensus was achieved. Therefore, the Delphi process was concluded. The finalized PCI Postoperative Rehabilitation Nursing Problem Assessment Tool based on the Omaha System included 4 first-level indicators (domains), 21 second-level indicators (nursing problems), and 130 third-level indicators (specific symptoms/signs). Supplementary Table 2 summarizes the types of suggestions provided by experts in the two Delphi rounds and the corresponding decisions made by the research team. The results of the two consultation rounds are summarized in Table 1.
 |
Table 1 Expert Consensus on the Postoperative Rehabilitation Nursing Problem Indicators in Two Delphi Consultation Rounds |
Discussion
Validity and Reliability of the Postoperative Rehabilitation Nursing Problem Assessment Index System for PCI Patients Based on the Omaha System
This study developed a postoperative rehabilitation nursing problem assessment index system for patients undergoing PCI, based on the Omaha System, by integrating a literature review, case analyses, and clinical observations. The system was finalized through two rounds of expert consultation using the Delphi method.
The Delphi method typically involves 15–30 experts to ensure the validity and stability of the results.27 The quality and reliability of Delphi consultation outcomes depend on the selection of experts, their enthusiasm, authority, and consensus.28 In this study, 15 experts were recruited from six tertiary hospitals and two universities in Shenzhen and Guangzhou, two major cities in Guangdong Province, China. Their professional backgrounds covered nursing management, nursing education, nursing practice, and clinical medicine, all highly relevant to the study content. Of these experts, 8 (53.3%) held senior or associate senior titles and had more than 10 years of experience in cardiovascular care, indicating both extensive expertise and practical experience; therefore, their opinions were highly representative and authoritative.
The questionnaire response rates were 93.75% in the first round and 100% in the second, indicating high expert engagement. Self-assessment data showed that 6 (40.0%) experts were “very familiar” and 9 (60.0%) were “relatively familiar” with the subject, indicating sufficient experience with the research topic and supporting the reliability of the consultation results. The authority coefficients for the two rounds were 0.858 and 0.875, respectively, confirming that participants had strong practical authority and relevant experience.
The relatively low Kendall’s W value observed in our study may be influenced by the diverse backgrounds of the participating experts. Experts from different specialties may have varying perspectives, experiences, and priorities, leading to differences in their ratings. Nevertheless, the statistically significant χ² result indicates that the agreement observed is unlikely to be due to chance, suggesting a meaningfulconsensus.
The indicator system developed in this study builds on the Omaha System but is specifically adapted for post-PCI rehabilitation. It is more relevant to the target patient population, focusing on 21 core problems closely related to PCI recovery. The system is structured along four dimensions (ie, physiological, psychological, health-related behaviors, and environmental factors), allowing comprehensive, staged assessment aligned with the rehabilitation process. Finally, all indicators were validated through two rounds of Delphi consultation with 15 senior experts, ensuring contextual relevance and content validity within the Chinese clinical setting.
Feasibility of the Postoperative Rehabilitation Nursing Problem Assessment Index System for PCI Patients Based on the Omaha System
The Omaha System is frequently used as a comprehensive and effective tool for assessing and collecting health information.29,30 It not only addresses patients’ physiological and psychological concerns but also considers environmental and health-related issues, allowing for a comprehensive patient assessment.10,31 International experiences further support its applicability and adaptability across diverse healthcare systems. For instance, in the United States and several European countries, the Omaha System has been integrated into home-care, community health, and chronic disease management programs, demonstrating its value in clinical decision-making, nursing documentation standardization, and outcome monitoring.32 Similarly, studies in Asian countries have shown that the Omaha System can effectively guide care planning, enhance interdisciplinary communication, and support the development of electronic health records.33,34 These findings suggest that although healthcare delivery models differ across regions, the Omaha System provides a flexible structure that can bridge variations in practice patterns, patient needs, and resource settings. In this study, a postoperative rehabilitation nursing problem assessment index system for patients undergoing PCI was developed using the Omaha System framework. The system was constructed by integrating a literature review, case analyses, and clinical observations, and was finalized through two rounds of expert consultation. The resulting assessment tool consists of 4 first-level domains, 21 second-level indicators, and 130 third-level indicators, enabling the comprehensive identification of postoperative nursing problems across four key domains: physiological, health-related behavior, psychosocial, and environmental. This index system also allows timely detection of high-risk cardiovascular factors such as smoking, poor medication adherence, hypertension, and abnormal lipid profiles. Furthermore, it provides practical guidance for clinical healthcare professionals and demonstrates strong feasibility for application in postoperative rehabilitation care for patients undergoing PCI.
Future Evaluation of the Omaha System
Future evaluation of the usefulness and clinical benefits of the Omaha System-based assessment system can be conducted through clinical empirical studies, such as randomized controlled trials or pre-post intervention studies. The system could be applied to a group of post-PCI patients, while a control group receives standard care. Its effectiveness can then be assessed by comparing differences in nursing quality process indicators, such as the accuracy of identifying postoperative rehabilitation nursing problems, and patient outcome indicators, including cognitive outcomes (eg, disease knowledge), behavioral outcomes (eg, medication adherence), and clinical status (eg, frequency of angina episodes). Moreover, future research could employ multidimensional assessments to systematically identify often-overlooked factors that significantly impact quality of life and recovery, such as mental health (eg, anxiety, depression), social support, income, and sleep patterns, enabling multidisciplinary and personalized interventions. Evaluation could also incorporate internationally recognized generic scales, such as the SF-36, to assess broader dimensions, including physical function, pain, social functioning, and mental health, alongside the Omaha System outcomes, by quantifying patient scores in cognition, behavior, and condition before and after interventions.
Future Application of the Omaha System
The Omaha-based evaluation index developed in this study is intended to serve as a practical tool to guide nurses in identifying and managing post-PCI rehabilitation nursing problems. In clinical practice, nurses can use the index at key time points, such as the first postoperative day, one day before discharge, and one month after discharge, to systematically screen for problems based on observed signs, symptoms, and patient reports. Identified problems then inform development of individualized care plans, with goals agreed upon by nurses, patients, and families, aligned with Omaha intervention categories. Interventions are delivered and documented using structured records or digital tools, and outcomes are evaluated dynamically using Omaha cognitive, behavioral, and status ratings. Comparing pre- and post-intervention scores enables quantification of care effectiveness, guiding feedback, goal adjustment, and refinement of care strategies, thus supporting an iterative, patient-centered nursing process.
In future clinical implementation, developing a supporting mobile or PC application would be essential to facilitate effective use of the Omaha System-based evaluation system. Such digital tools could standardize data entry, enhance real-time assessment, and support decision-making by automatically linking identified problems with corresponding intervention and outcome indicators.
Limitations and Future Directions
Although the questionnaire covers 21 nursing problems, only 9 can be reliably assessed through medical record review, nursing observation, and routine patient communication. Consequently, completing the full questionnaire takes 40 min, which may pose a time constraint in busy clinical settings. To address this limitation in future implementation, several strategies could be considered. One approach is to integrate the tool into electronic health record systems with smart forms that automate scoring, pre-fill data, and provide decision-support prompts, thereby reducing manual workload. Another option is to develop a shortened screening version for routine use, followed by the complete assessment only for patients flagged as high risk or presenting complex needs. These optimization strategies could improve feasibility, enhance efficiency, and support wider clinical adoption. In addition, the expert panel was relatively small and geographically concentrated, which may limit the representativeness of opinions collected and reduce generalizability. Future research should expand the panel size and diversify expert selection across regions and practice settings to enhance robustness and applicability. Finally, this study represents the initial stage of system construction and pilot implementation. Comprehensive validation of the system’s clinical effectiveness, long-term applicability, and generalizability remains needed.
Conclusion
This study developed a postoperative rehabilitation nursing problem assessment index system for patients undergoing PCI, based on the Omaha System. The system shows strong potential to identify key postoperative risks and guide individualized interventions. Such structured linkage between assessment and tailored intervention supports more proactive and patient-centered care. Further studies are warranted to evaluate its clinical effectiveness, monitor its implementation in broader clinical settings, and maximize its benefits for PCI patient outcomes.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from Haiyan Xiong on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Longhua District People’s Hospital and adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study. Patient data were anonymized and kept confidential in accordance with ethical guidelines.
Acknowledgments
We thank Medjaden Inc. for the scientific editing of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Medical Research Project of Shenzhen Longhua Medical Association (2024LHMA07).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hu SS.; The Writing Committee of The Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2021: an updated summary. J Geriatr Cardiol. 2023;20:399–21. doi:10.26599/1671-5411.2023.06.001
2. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. doi:10.1161/CIR.0000000000000950
3. Bansal A, Hiwale K. Updates in the management of coronary artery disease: a review article. Cureus. 2023;15:e50644. doi:10.7759/cureus.50644
4. Abubakar M, Javed I, Rasool HF, et al. Advancements in percutaneous coronary intervention techniques: a comprehensive literature review of mixed studies and practice guidelines. Cureus. 2023;15:e41311.
5. Doenst T, Thiele H, Haasenritter J, Wahlers T, Massberg S, Haverich A. The treatment of coronary artery disease. Dtsch Arztebl Int. 2022;119:716–723. doi:10.3238/arztebl.m2022.0277
6. Masoomi R, Azzalini L. Survival following recanalization of chronic total occlusion: the devil is in the details. J Am Heart Assoc. 2023;12:e032178. doi:10.1161/JAHA.123.032178
7. Chinese Society of Cardiology of Chinese Medical Association, Cardiovascular Disease Prevention and Rehabilitation Committee of Chinese Association of Rehabilitation Medicine, Cardiovascular Disease Committee of Chinese Association of Gerontology and Geriatrics, Thrombosis Prevention and Treatment Committee of Chinese Medical Doctor Association. [Chinese guideline on the primary prevention of cardiovascular diseases]. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48:1000–1038. Polish. doi:10.3760/cma.j.cn112148-20201009-00796
8. Fang X, Jia S, Wang Q, et al. The application of the omaha system in community rehabilitation nursing for patients with stroke and previous falls. Front Neurol. 2022;13:711209. doi:10.3389/fneur.2022.711209
9. Terry D, Hills D, Bradley C, Govan L. Nurse-led clinics in primary health care: a scoping review of contemporary definitions, implementation enablers and barriers and their health impact. J Clin Nurs. 2024;33:1724–1738. doi:10.1111/jocn.17003
10. Topaz M, Golfenshtein N, Bowles KH. The Omaha System: a systematic review of the recent literature. J Am Med Inform Assoc. 2014;21:163–170. doi:10.1136/amiajnl-2012-001491
11. Rodríguez-Suárez CA, González-de la Torre H, Hernández-De Luis MN, Fernández-Gutiérrez D, Martínez-Alberto CE, Brito-Brito PR. Effectiveness of a standardized nursing process using NANDA international, nursing interventions classification and nursing outcome classification terminologies: a systematic review. Healthcare. 2023;11:2449. doi:10.3390/healthcare11172449
12. Rodríguez-Suárez CA, Rodríguez-álvaro M, García-Hernández AM, Fernández-Gutiérrez D, Martínez-Alberto CE, Brito-Brito PR. Use of the nursing interventions classification and nurses’ workloads: a scoping review. Healthcare. 2022;10:1141. doi:10.3390/healthcare10061141
13. de Freitas Luzia M, Vidor ID, da Silva A, de Fátima Lucena A. Fall prevention in hospitalized patients: evaluation through the nursing outcomes classification/NOC. Appl Nurs Res. 2020;54:151273. doi:10.1016/j.apnr.2020.151273
14. Yin S, Ou Y, Ting E. Impacts of Omaha System-based continuing care on the medication compliance, quality of life, and prognosis of coronary heart disease patients after PCI. Braz J Cardiovasc Surg. 2022;37:472–480. doi:10.21470/1678-9741-2021-0222
15. Wu L, Liu X, Tang X, et al. Effect of case management based on Omaha system on clinical symptoms and quality of life of coronary heart disease patients after percutaneous coronary intervention. Medicine. 2024;103:e38553. doi:10.1097/MD.0000000000038553
16. Zhang Q, Zhang A, Wang Y, et al. Feasibility of the Omaha system for the care of children with dilated cardiomyopathy. Front Pediatr. 2023;11:1136663. doi:10.3389/fped.2023.1136663
17. Xiao S, Fan L, Dai H. Omaha System-based discharge guidance improves knowledge and behavior in Mainland Chinese patients with angina who are not receiving interventional treatment: a randomized controlled trial. Jpn J Nurs Sci. 2019;16:355–363. doi:10.1111/jjns.12244
18. Lotfi M, Zamanzadeh V, Khodayari-Zarnaq R, Mobasseri K. Nursing process from theory to practice: evidence from the implementation of “Coming back to existence caring model” in burn wards. Nurs Open. 2021;8:2794–2800. doi:10.1002/nop2.856
19. Suhonen R, Stolt M, Edvardsson D. Personalized nursing and health care: advancing positive patient outcomes in complex and multilevel care environments. J Pers Med. 2022;12:1801. doi:10.3390/jpm12111801
20. Austin RR, McLane TM, Pieczkiewicz DS, Adam T, Monsen KA. Advantages and disadvantages of using theory-based versus data-driven models with social and behavioral determinants of health data. J Am Med Inform Assoc. 2023;30:1818–1825. doi:10.1093/jamia/ocad148
21. Li YD, Qu N, Yang J, Lv CY, Tang Y, Li P. Effects of an Omaha System-based follow-up regimen on self-care and quality of life in gastrointestinal surgery patients. World J Gastrointest Surg. 2023;15:2179–2190. doi:10.4240/wjgs.v15.i10.2179
22. Chen J, He F, Wu Q, et al. Identifying self-reported health-related problems in home-based rehabilitation of older patients after Hip replacement in China: a machine learning study based on Omaha system theory. BMC Med Inform Decis Mak. 2023;23:268. doi:10.1186/s12911-023-02353-7
23. Manyara AM, Purvis A, Ciani O, Collins GS, Taylor RS. Sample size in multistakeholder Delphi surveys: at what minimum sample size do replicability of results stabilize? J Clin Epidemiol. 2024;174:111485. doi:10.1016/j.jclinepi.2024.111485
24. Shi C, Zhang Y, Li C, Li P, Zhu H. Using the Delphi method to identify risk factors contributing to adverse events in residential aged care facilities. Risk Manag Healthc Policy. 2020;13:523–537. doi:10.2147/RMHP.S243929
25. Robin RA, Craig S, Karen AM. An informatics approach to inter-professional management of low back pain: a feasibility study using the Omaha System. BMJ Health Care Inform. 2017;24.
26. Eardley DL, Krumwiede KA, Secginli S, et al. The Omaha System as a structured instrument for bridging nursing informatics with public health nursing education: a feasibility study. Comput Inform Nurs. 2018;36:275–283. doi:10.1097/CIN.0000000000000425
27. Olsen JM, Thorson D, Baisch MJ, Monsen KA. Using Omaha System documentation to understand physical activity among rural women. Public Health Nurs. 2017;34:31–41. doi:10.1111/phn.12264
28. Wu L, Sun Y. Introduction to the Delphi method and its application status in nursing. Nurs Res. 2015;29:3599–3601.
29. Xu Y, Li S, Wang D. Preliminary construction of core competency evaluation indicators for continuity of care nurses. Nurs Res. 2016;30:2082–2086. doi:10.1007/s00464-015-4457-6
30. Shen L, He W, Du Y. Research on the performance evaluation index system of community public health Services. Chin Rural Health Serv Manage. 2011;31:127–130.
31. Yang J, Li M, Li C, Huang QH, Lin SQ, Zhou HZ. Construction and preliminary validation of a fall risk assessment scale for inpatients in ophthalmology department. Chin J Nurs. 2022;57:66–72.
32. Schleder goncalves L, Picanco GS, Dipp HM, da Silva CS. Omaha system: an integrative literature review from 2012 to 2022. Stud Health Technol Inform. 2024;315:600–601. doi:10.3233/SHTI240235
33. Bayuo J, Kwok WYY, Wong FKY, Wong AKC, Lam KKW, Chow KKS. A community-based health social partnership programme to enhance self-care management amongst older adults: a cluster randomised controlled hybrid implementation-effectiveness study. Age Ageing. 2025;54. doi:10.1093/ageing/afaf302
34. Li H, He Q, Liu S. Profiles of home-based medical care service demand among older patients with different characteristics: a cluster analysis. BMC Prim Care. 2025;26:294. doi:10.1186/s12875-025-03014-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perceived Determinants of Health-Related Behaviors Among Patients with Coronary Heart Disease After Percutaneous Coronary Intervention: A Longitudinal Qualitative Study
Su X, Zhang Y, Zhou H, Ma F, Jin X, Bai Y, Wei W, Zhang X, Zhou M
Patient Preference and Adherence 2024, 18:591-606
Published Date: 6 March 2024
The Effect of Cardiopulmonary Exercise Ability to Clinical Outcomes of Patients with Coronary Artery Disease Undergoing Percutaneous Coronary Intervention

Zhang W, Xu J
International Journal of General Medicine 2024, 17:6145-6152
Published Date: 14 December 2024
Moving Forward Despite Obstacles: A Qualitative Study on Healthy Lifestyle Adjustments Among Patients with Coronary Heart Disease After Their First Percutaneous Coronary Intervention
Cheng L, Wang WR, Wikström L, Mårtensson J
International Journal of General Medicine 2025, 18:1451-1461
Published Date: 15 March 2025
Analysis Impact of Positive Psychological Capital on Quality of Life Among Patients Post Percutaneous Coronary Intervention: A Cross-Sectional Study
Kudelati Z, Yin S, Chen S, Han S, Yuan S, Wang H
Journal of Multidisciplinary Healthcare 2025, 18:7413-7421
Published Date: 11 November 2025