Back to Journals » Infection and Drug Resistance » Volume 17
Antimicrobial Resistance of Clostridioides difficile in Children from a Tertiary Pediatric Hospital in Shanghai, China
Authors Li X, Wang Y ![]() , Cao R, Xiao F, Wang X, Ye L, Xiao Y, Li D, Zhang T
, Cao R, Xiao F, Wang X, Ye L, Xiao Y, Li D, Zhang T
Received 21 September 2023
Accepted for publication 13 December 2023
Published 26 January 2024 Volume 2024:17 Pages 329—339
DOI https://doi.org/10.2147/IDR.S441312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaolu Li,1,* Yizhong Wang,1,2,* Rong Cao,1 Fangfei Xiao,1 Xufei Wang,1 Lin Ye,1 Yongmei Xiao,1 Dan Li,1 Ting Zhang1,2
1Department of Gastroenterology, Hepatology and Nutrition, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Gut Microbiota and Metabolic Research Center, Institute of Pediatric Infection, Immunity and Critical Care Medicine, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yizhong Wang; Ting Zhang, Department of Gastroenterology, Hepatology and Nutrition, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, 355 Luding Road, Shanghai, 200062, People’s Republic of China, Tel/Fax +86 2152976335, Email [email protected]; [email protected]
Background: Our previous study reported a high rate of recurrence in children with Clostridioides difficile (C. difficile) infection (CDI) after conventional antibiotic therapy. Here, we aimed to explore whether metronidazole and vancomycin resistant C. difficile isolates are circulating in pediatric CDI.
Methods: Antimicrobial susceptibility testing (AST) using the agar dilution method according to the Clinical and Laboratory Standard Institute (CLSI) were performed on C. difficile isolates collected from children with CDI between 2019 and 2022 at the Shanghai Children’s Hospital. Whole-genome sequencing (WGS) was performed on all C. difficile isolates, and the presence of antibiotic resistance genes (ARGs) were identified using Resfinder and the Comprehensive Antibiotic Resistance Database (CARD). The presence of plasmid pCD-METRO was detected using SRST2 (v0.2.0) against 8 pCD-METRO coding sequences.
Results: A total of 50 C. difficile isolates were collected from stools of CDI children. The overall resistance rate on all isolates was 30.00% for metronidazole, 6.00% for vancomycin, 0% for rifaximin, 2.00% for rifampin, 24.00% for meropenem, 100.00% for ceftriaxone and clindamycin, 86.00% for erythromycin, 30.0% for levofloxacin, and 50.0% for tetracycline. Multidrug-resistant (MDR) was presented in 44 isolates (88.00%). Sixteen reported potential ARGs relating with resistance to antibiotic classes of aminoglycoside (AAC(6’)-Ie-APH(2”)-Ia, aad(6), ANT(6)-Ib, APH(2”)-If, APH(3’)-IIIa), lincosamide-clindamycin-erythromycin (ErmB, ErmQ), fluoroquinolones (CdeA), glycopeptides (vanRG), nucleoside (SAT-4), tetracycline (tetM, tetA(P), tetB(P), tetO), and trimethoprim (dfrF) were identified. However, the pCD-METRO plasmid and vanA/B were not detected in any isolates.
Conclusion: C. difficile isolates from children with reduced susceptibility to metronidazole and vancomycin are emerging in pediatric CDI in China. The lack of pCD-METRO plasmid and vanA/B associated with reduced antibiotic susceptibility suggests there are additional mechanisms of resistance.
Keywords: Clostridioides difficile, antibiotic resistance, metronidazole, vancomycin, children
Introduction
Clostridioides difficile (C. difficile), an anaerobic, gram-positive, spore-forming bacillus, is a leading cause of healthcare-associated diarrhea in humans.1 Clinical manifestations of C. difficile infection (CDI) range from asymptomatic colonization, or self-resolving diarrhea to colitis, severe pseudomembranous enterocolitis, toxic megacolon, and death.2 The pathogenicity of C. difficile is mainly attributed to the two major virulence factors produced by toxigenic C. difficile strains, enterotoxin A (TcdA) and cytotoxin B (TcdB).3 The development of CDI in children is major associated with an increased susceptibility of C. difficile colonization caused by an alteration of gut microbiota.4 Events implicated in the gut microbiota disruption, including antibiotic exposure, proton pump inhibitors (PPI) use, and inflammatory bowel diseases (IBD), are recognized as the risk factors for pediatric CDI.4 Discontinuation of antibiotics and appropriate rehydration are generally effective for symptoms resolution in children with CDI, and specific antibiotics are advised for the treatment of severe pediatric CDI, such as metronidazole, vancomycin, and fidaxomicin.5 In addition, fecal microbiota transplantation (FMT) is recommended for the treatment of recurrent CDI (rCDI).
Multiple antibiotics resistance has been identified in C. difficile.6,7 Several recent studies indicated that the susceptibility of clinical C. difficile isolates to metronidazole and vancomycin is also declining.8,9 Our previous single center analysis showed that RCDI occurred in 48.53% (33/68) and 46.33% (19/41) of pediatric CDI cases initially treated with metronidazole and vancomycin, respectively.10 Failure of antibiotics therapy implicates C. difficile strains with a reduced susceptibility to metronidazole and vancomycin may exist in our patients. Researches have shown that metronidazole resistance is associated with pCD-METRO,11 heme responsive genes,12 nitroimidazole reductase genes8,13 and chromosomal loci.14 For vancomycin resistance, recent evidence indicated drug-binding site alterations, efflux pumps, RNA polymerase mutations, plasmid acquisition and biofilm formation may play important roles.15–17
Given the high occurrence of RCDI post-antibiotic treatment in our center,10 we aimed to explore whether metronidazole and vancomycin resistant C. difficile isolates are circulating in pediatric CDI by performing AST and WGS. Here, we show that the emergence of C. difficile isolates with reduced susceptibility to metronidazole and vancomycin may be associated with the failure of antibiotic therapy in CDI children.
Methods
Clinical C. difficile Isolates
Clinical CDI is defined as patients with three or more liquid stools (Bristol 6–7) per day, and either a positive stool test for CD toxins or a PCR detection of toxigenic CD, or colonoscopic findings revealing pseudomembranous colitis according to the 2017 update clinical practice guidelines for CDI in children.2 Stool samples were collected from pediatric patients with confirmed CDI at the Shanghai Children’s Hospital from 2019 to 2022. About 1 mL (1 g) of stool was mixed with same volume of 95% ethanol for 30 min at room temperature for spore selection. The supernatant was discarded after centrifugation at 2500 g for 5 min. The lower sediment was serially diluted and plated on selective taurocholate cycloserine-cefoxitin fructose agar (CCFA, Oxoid, UK) plates supplemented with sheep blood (7%). Plates were placed in an anaerobic workstation (ELECTROTEK AW500 SG, UK) incubated for 48 h, at 37°C. Colony was picked based on typical morphology of C. difficile (yellowish/white with a ground-glass appearance, and has a horse-like odor). C. difficile isolates were further confirmed by PCR and Sanger sequencing of the housekeeping gene tpi and the 16S rRNA gene. Confirmed C. difficile colony was re-cultured on 5% Columbia blood agar twice to obtain pure C. difficile isolates. Each pure isolate was stored at −80°C in brain heart infusion (BHI) broth supplemented with 0.5% yeast extract (YBHI, Oxoid, UK) containing 50% glycerol.
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013), and was approved by the Ethical Review Board of the Shanghai Children’s Hospital (2022R043-E01), and informed consent was taken from parent or legal guardian of all the participates.
Antimicrobial Susceptibility Testing
All C. difficile isolates were tested for susceptibility using the agar dilution method according to the Clinical and Laboratory Standard Institute (CLSI) for the following 10 antibiotics: metronidazole, vancomycin, rifaximin, rifampin, ceftriaxone, clindamycin, meropenem, erythromycin, levofloxacin, and tetracycline.18 All AST were performed on Brucella agar plates supplement with 1 mg/L of vitamin K, 5 mg/L of hemin, and 5.0% sheep blood at 37°C for 48 h under anaerobic condition in duplicate from independent cultures for 3 times. C. difficile ATCC 43255 strain was used as quality control and was included in each AST test. Antimicrobial susceptibility was mostly interpreted according to the minimal inhibitory concentrations (MIC) breakpoints of CLSI18 and European Committee on Antimicrobial Susceptibility Testing (EUCAST).19 Multidrug-resistant (MDR) was defined as an isolate with resistance to three or more classes of antibiotics.18 All AST data were verified by three different people independently.
Whole-Genome Sequencing
All clinical C. difficile isolates were recovered on CCFA agar plates. Single colony was picked and grown in YBHI broth for 16 h at 37°C anaerobically. Genomic DNA was extracted from the bacteria pellet using the Wizard® Genomic DNA Purification Kit (Promega, USA). High quality genomic DNA (at least 1 μg) was used for generating libraries with ∼400 bp insert sizes for paired-end sequencing using TruePrep DNA Library PrepTM Kit V2 (Illumina, USA). Whole-genome sequencing (WGS) was performed using the Illumina NovaSeq 6000 platform (Illumina, USA) with 150-base paired-end reads according to the standard protocol (Shanghai Winnerbio Technology Co., Ltd., China). Raw reads were processed and quality controlled by fastp (V0.22.0) and remove sequencing adapters and low-quality reads (reads containing more than 3 unknown bases, more than 50% of the bases scored below Q20, and read length less than 30 bp). Genome assembly was performed using SPAdes (V3.15.3). CDS was predicted using Glimmer (V3.02). Isolates with evidence of contamination were excluded. Sequence type (ST) and clade were determined by alignment of assembled scaffold to C. difficile PubMLST.20 Prediction of non-redundant coding sequence (CDS) was performed using Glimmer (V3.02). Roary (v.3.12.0) was used for the identification of core genome.21 The phylogenetic tree was first generated by a built-in Species Tree inference from all genes (STAG) algorithm in OrthoFinder based on FastTree. FastTree infers approximately maximum-likelihood (ML) phylogenetic trees from alignments with up to hundreds of thousands of sequences.22 Beautification and visualized of the tree were performed using iTOL.23 The toxin genes including tcdA, tcdB, cdtA and cdtB were detected using Virulence Factors of Pathogenic Bacteria database (VFDB).24
Antibiotic Resistance Genes Analysis
Antibiotic resistance genes (ARGs) in the obtained C. difficile genome were identified using Resfinder (v4.1)25 and Comprehensive Antibiotic Resistance Database (CARD 2.0.0) databases with cutoff values of 70% nucleotide identity and 90% coverage of the gene query length.26 Reads were compared using SRST2 (v0.2.0) against 8 pCD-METRO (GenBank accession: CAADHH010000057) coding sequences to find the presence of plasmid pCD-METRO.27
Results
Clinical C. difficile Isolates and Patient Characteristics
A total of 50 clinical C. difficile isolates were obtained from stools collected from 50 unique pediatric CDI patients enrolled in our center during 2019 to 2022. The characteristics of patients with positive C. difficile cultures are shown in Table 1. The median age of the 50 CDI children was 5 years (interquartile range (IQR), 2.50–9.30 y). Thirty-six cases (72.00%) were community-acquired CDI and 13 (28.00%) patients were hospital-acquired CDI. Exposure history included previous antibiotics exposure (29/50, 58.00%) and PPI use (8/50, 16.00%). The main clinical symptoms were diarrhea (29/50, 58.00%), and hematochezia (16/50, 32.00%). For the initial specific antibiotic treatment, 18 (36.00%) patients received metronidazole and 15 (32.00%) patients received vancomycin. After following up for 8 weeks, the total sustained clinical remission rate of the first round of metronidazole and vancomycin therapy was 77.78% and 81.25%, respectively.
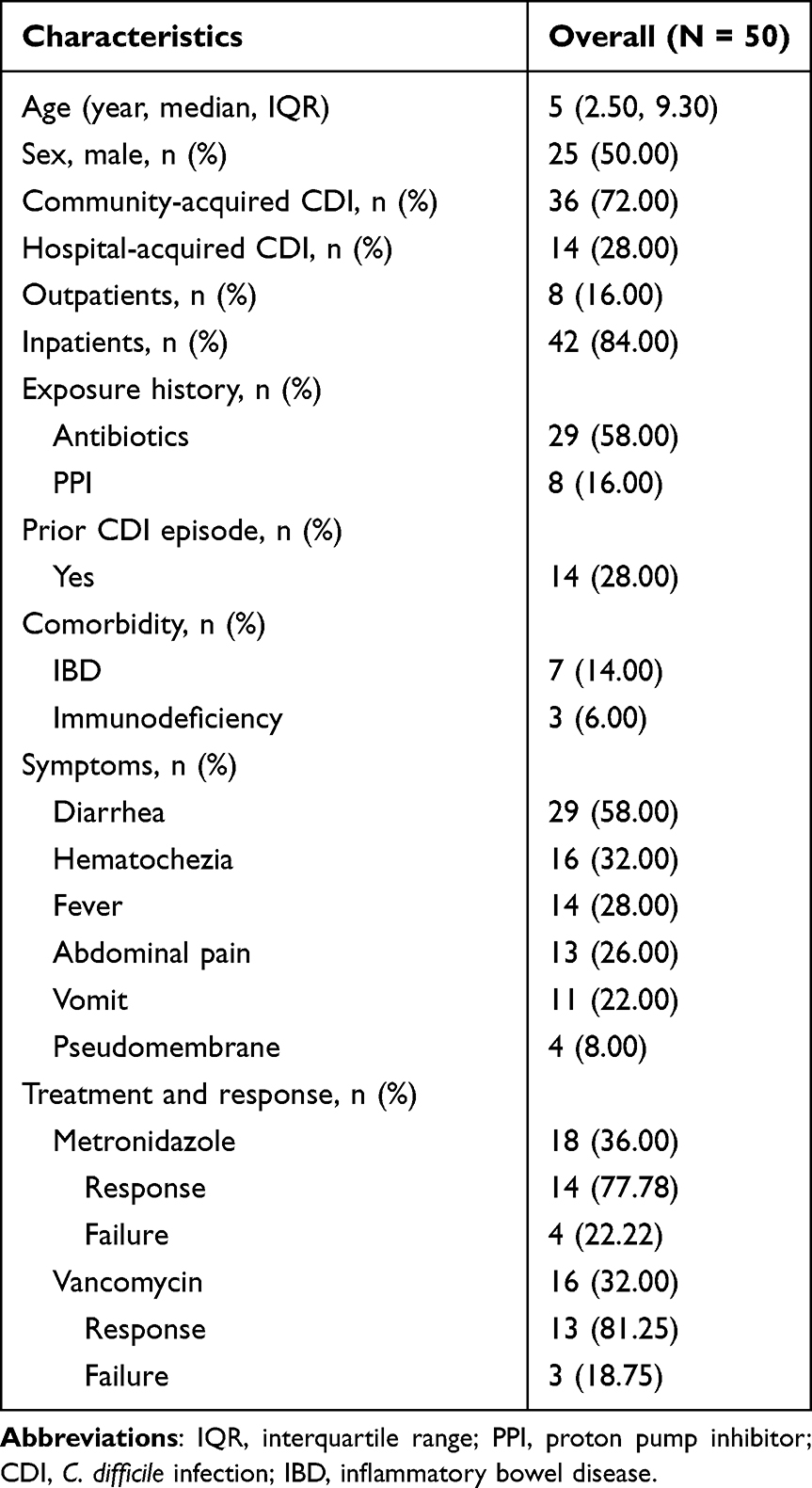 |
Table 1 Characteristics of the Pediatric Patients with C. Difficile Infection |
Antimicrobial Susceptibility Testing
Susceptibility tests of 10 antibiotics using the agar dilution method were performed for all 50 clinical C. difficile isolates according to the CLSI standard performed in the microbiology laboratory of Department of Clinical Laboratory, Shanghai Children’s Hospital. As shown in Table 2, the metronidazole MIC50 was 0.25 μg/mL, and MIC90 was 128 μg/mL; the vancomycin MIC50 was 1 μg/mL, and MIC90 was 8 μg/mL; the rifaximin MIC50 was <0.064 μg/mL, and MIC90 was 2 μg/mL; the rifampin MIC50 was <0.064 μg/mL, and MIC90 was 8 μg/mL; the ceftriaxone, clindamycin, and erythromycin MIC50 was >128 μg/mL, and MIC90 was >128 μg/mL; the levofloxacin MIC50 was 4 μg/mL, and MIC90 was 32 μg/mL; the meropenem MIC50 was 8 μg/mL, and MIC90 was 32 μg/mL; the tetracycline MIC50 was 8 μg/mL, and MIC90 was 64 μg/mL for all isolates. The overall resistance rate was 30.00% for metronidazole, 6.00% for vancomycin, 0% for rifaximin, 2.00% for rifampin, 24.00% for meropenem, 100.00% for ceftriaxone and clindamycin, 86.00% for erythromycin, 30.00% for levofloxacin, and 50.00% for tetracycline (Table 2). MDR was presented in 44 isolates (88.00%) according to CLSI. AST data for all C. difficile isolates were summarized in Table S1.
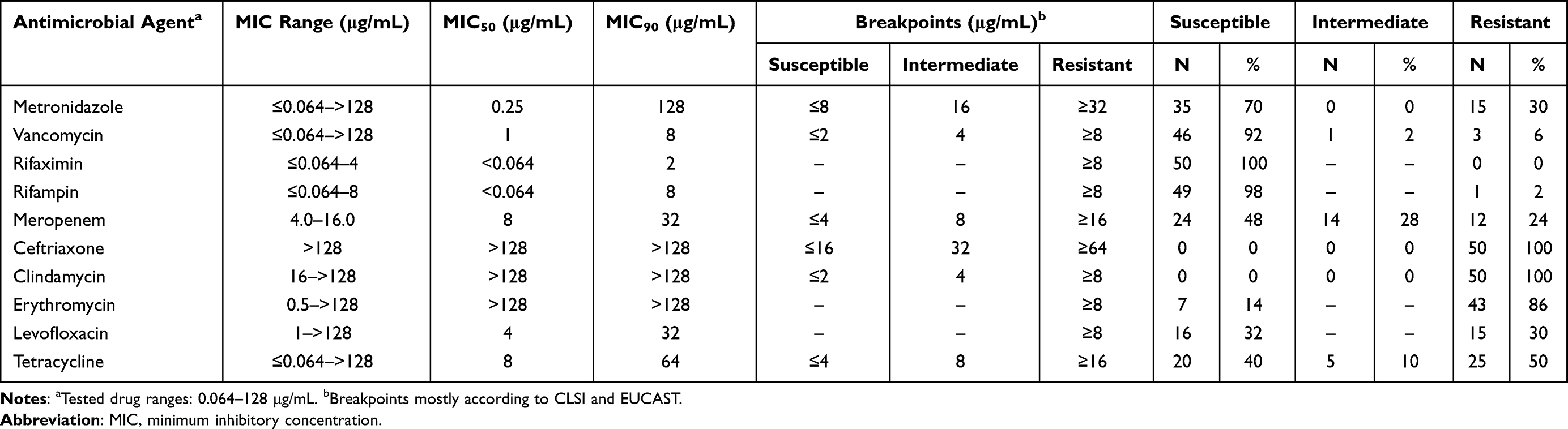 |
Table 2 Summary of Antimicrobial Susceptibility Testing Data for C. Difficile Isolates (N = 50) |
Whole-Genome Sequencing
All 50 clinical C. difficile isolates underwent WGS. As shown in Table S2, clean data of86950Mbp with an average of 1739 Mbp (range, 743–7043 Mbp) were obtained after the quality control process. The average read coverage was 414× (range, 177–1607×) across the assembly genome (about 4.2 Mbp). De novo assembly of the reads generated an average scaffold of 87 (range, 28–994), and the average N50 was207182bp (range, 8937–448 661). The average G + C content was 28.60% (range, 28.10–29.30%). A total of191036CDSs (average, 3820; range, 3573–4138) were identified, out of which 2950 CDSs were identified as core genes (genes present in 100.00% of the 50 genomes) by pan-genome analysis, accounting 77.20% of the average number of CDS per genome (3820 CDS). Multi-locus sequence typing (MLST) analysis identified 19 STs, including ST2, ST3, ST8, ST15, ST26, ST33, ST35, ST37, ST39, ST42, ST43, ST44, ST51, ST54, ST69, ST81, ST102, ST103, and ST129. The phylogenetic tree generated by a STAG algorithm in OrthoFinder separated our clinical pediatric C. difficile isolates into 2 of the 5 C. difficile clades, and the majority of the isolates belongs to clade 1 (45/50, 90.00%, Figure 1). For toxin gene identification, 31 (62.00%) isolates carried tcdA, tcdB, cdtA and cdtB, 9 (18.00%) isolates carried tcdA and tcdB, and 10 (20.00%) isolates did not harbor neither tcdA, tcdB nor cdtA, cdtB (Figure 1). Antibiotic resistance rates of each antibiotic based on in vitro MIC data across STs and corresponding clades were shown in Figure 2A. Most of the isolates with metronidazole and vancomycin resistances belong to clade 1.
 |
Figure 1 The phylogenetic tree of clinical C. difficile isolates collected from children with CDI. The phylogenetic tree was generated by a STAG algorithm in OrthoFinder including 50 genomes sequenced in this study and 7 reference genomes. STs and clades are labeled on the outer circle. The background shading represents the MLST clades. Different toxin profiles are indicated as colored stars at the start of the branches. Abbreviations: CDI, C. difficile infection; STAG, Species Tree inference from all genes; ST, sequence type; MLST, multi-locus sequence typing; CARD, Comprehensive Antibiotic Resistance Database. |
 |
Figure 2 Resistance rates based on in vitro MIC data and distribution of in silico predicted ARGs. (A) Antibiotic resistance rate across ST and MLST clades. The heatmaps present proportions of antibiotic resistant samples for each antibiotic from top to bottom against MLST and color-coded according to clade. The number is the proportion of antibiotic resistance rate. (B) The presence of ARGs identified using the CARD indicated with a red line. The ARGs are implied by gene name (top) and Antibiotic Resistance Ontology accession number (bottom), and the relevant antibiotic class and clade are separately showed by the color-coded X and Y axes. The heatmaps represent the proportions of antibiotic resistant isolates. Abbreviations: MIC, minimum inhibitory concentration; ARGs, antibiotic resistance genes; ST, sequence type; MLST, multi-locus sequence typing; CARD, Comprehensive Antibiotic Resistance Database. |
Antibiotic Resistance Genes
A total of 16 ARGs were identified according to the CARD database, which relating resistance to antibiotic classes of aminoglycoside, erythromycin, fluoroquinolone, glycopeptide, lincosamide, nucleoside, tetracycline, and trimethoprim (Table S3). Multiple ARGs conferred resistance to antibiotic aminoglycoside class were detected, including AAC(6’)-Ie-APH(2”)-Ia, aad(6), ANT(6)-Ib, APH(2”)-If, and APH(3’)-IIIa. ErmB conferred resistance to macrolide-lincosamide-streptogramin B (MLSB) class of antibiotics was detected in 35 isolates (70.00%) with both erythromycin and clindamycin resistance. In addition, all 5 isolates of ST129 belong to clade 1 with both erythromycin and clindamycin resistance carried ErmQ. CdeA relating resistance to fluoroquinolone class was detected in all 50 isolates. VanRG associated with acquired vancomycin resistance was detected in 43 isolates (86.00%), including 3 isolates with resistance to vancomycin. Several ARGs of tetracycline resistance were identified in isolates with resistance to tetracycline, including tetM, tetA(P), tetB(P), and tetO in 23 (46.00%), 7 (14.00%), 7 (14.00%), and 1(2.00%) isolates, respectively. Seven isolates with resistance to tetracycline carried both tetA(P) and tetB(P). The pCD-METRO plasmid associated with metronidazole resistance, and ARGs related to cephalosporin resistance were not identified in any isolates. The distribution of ARGs in different clades of clinical C. difficile isolates was presented in Figure 2B.
Discussion
A few antibiotics are conventionally recommended as the treatment for CDI, such as metronidazole, vancomycin, and fidaxomicin.2 Treatment failure of oral metronidazole is associated with its low stool concentration and interaction with gut microbiota. C. difficile strain can easily overcome this insufficient concentration by higher MIC. Studies showed that an increasing MIC of metronidazole in several epidemic C. difficile ribotypes lead to a high rate of treatment failure.28 In addition, the emergence of plasmid-mediated resistance to metronidazole further increases the risks of treatment failure.28 Although oral vancomycin can quickly reduce C. difficile shedding through reaching high concentration in the stool, several mechanisms of vancomycin resistance in C. difficile were identified, include drug-binding site alterations, efflux pumps, RNA polymerase mutations, and biofilm formation.16 Fidaxomicin has the lowest rate of recurrence of CDI, which might be associated with its narrow spectrum of antimicrobial activity and persistence on spores.28 A high recurrence rate of CDI has been reported (5–50%) previously, and it can be even higher (40–75%) after the first recurrence.1,29,30 RCDI can further aggravate the burden both to patients and healthcare system by causing increased morbidity and mortality of CDI.31,32 Multiple factors are involved in the occurrence of RCDI, such as gut microbiota dysbiosis, continued C. difficile exposure, an incomplete host immune response, and reduced susceptibility to antibiotics.33
In this study, we showed that C. difficile isolates with reduced susceptibility to both metronidazole and vancomycin were emerging in the pediatric patients at a tertiary pediatric hospital in Shanghai, China. AST performed in clinical C. difficile isolates from 50 pediatric CDI patients indicated that 15 (30.00%) harbored C. difficile isolates with resistance to metronidazole, and 3 (6.00%) of them also resistant to vancomycin. The resistance rates of metronidazole and vancomycin were significantly higher in comparison with recent reports conducted in China,34,35 as well as other reports from worldwide7,36 suggesting a low resistance rate to metronidazole and vancomycin. Another adult study in China found that the resistance rate to metronidazole was 23.1%, which was similar with our study.37 A recent systematic review and meta-analysis included a total of 111 studies published between 1992 and 2019 revealed that the weighted pooled resistance (WPR) for metronidazole and vancomycin was 1.0% and 1.0% for the breakpoint > 2 μg/mL and 0% for breakpoint ≥ 32 μg/mL.7 Gargis et al showed that among 593 clinical C. difficile isolates, 98.50% and 97.30% were sensitive to vancomycin (MIC ≤ 2 μg/mL) and metronidazole (MIC ≤ 2 μg/mL), respectively.36 In contrast, several studies reported high rates of clinical C. difficile isolates with decreased susceptibility to metronidazole and vancomycin.8,9 For example, Darkoh et al showed that 29% (128/438) and 26% (114/438) of Houston diarrheal stool samples (114/438), 85% (83/98) and 67% (66/98) of Nairobi diarrheal stool samples harbored metronidazole and vancomycin non-susceptible C. difficile isolates, respectively.9 However, Greentree et al did not yield vancomycin non-susceptible C. difficile isolates by screening of 176 CDI stool specimens in a Cleveland-area hospital, which highlighting the potential for false-positive results due to contamination with vancomycin-resistant enterococci.38 The overall reduced susceptibility/resistance rates of 1501 clinical C. difficile isolates from MODIFY I and II studies were 14.5% for metronidazole, and 32.8% for vancomycin.8 For other tested antibiotics conducted in this study, high resistant rates were observed in ceftriaxone and clindamycin (100%), erythromycin (85.7%), levofloxacin (30.6%), meropenem (24.5%), and tetracycline (50.0%). No rifaximin resistant C. difficile isolate was observed, which is different with a previously study showing a high reduced susceptibility/resistance rates to rifaximin (99.5%) in adult patients.8 It may be associated with less usage of rifaximin in children in China. Taken together, differences in antibiotics resistance of clinical C. difficile isolates were reported, which can likely be explained by studies conducted in different location, different populations (age, race, etc.), antibiotic exposure history, or specific C. difficile STs. AST data need independent verification and need to be split out per isolate in relation to appropriate reference strains, particularly the doubly reduced susceptible strains of metronidazole and vancomycin. Given the majority of the reports were focus on the adults CDI patients, studies in pediatric CDI are needed to be conducted in the future.
In order to characterize the genetic determinants of the antibiotic resistance, we performed WGS in all 50 clinical C. difficile isolates. A total of 19 STs belong to clades 1 and 4 were identified based on the MLST analysis. Reduced susceptibility to metronidazole was more likely among the isolates belong to clade 1, as well as reduced susceptibility to vancomycin. The three STs with the highest metronidazole and vancomycin resistance rates were ST15, ST43, and ST18. Identifications of known genetic determinants conferred antibiotics resistance by CARD observed 16 ARGs among all 50 isolates. However, the pCD-METRO plasmid associated with metronidazole resistance11 was not identified in our genome collection, implicating other additional genetics determinants may be involved in the reduced susceptibility to metronidazole. The van operons, such as vanA, vanB, vanC, vanD, vanE, vanG, vanL, vanM and vanN, are recognized as the genetic basis of acquired vancomycin resistance in Enterococci.39 In our C. difficile genome collection, a high carry rate (42/50, 84.00%) of vanRG, a vanR variant in the vanG gene cluster were observed. The vanG operons correspond to a low-level of vancomycin resistance,39 which can explain the low reduced susceptibility to vancomycin in this study. Furthermore, the observations of ARGs mediating resistance to antibiotic classes of the lincosamide-clindamycin-erythromycin (ErmB, ErmQ),40 and tetracycline (tetM, tetA(P), tetB(P), and tetO)41 in our genome collection may be responsible for the high antibiotic resistance rates to erythromycin and clindamycin, and tetracycline, respectively. Several determinates were reported to be associated with fluoroquinolone resistance, such as CdeA, mutations in gyrA, and gyrB.42,43 Our results showed that CdeA was detected in both resistance and susceptible strains to levofloxacin, which implicating the mutations in gyrA, and gyrB are more likely the cause of the resistance. However, gyrA, and gyrB were not detected in the genome collection of C. difficile strains isolated from our pediatric patients. Taken together, further studies are warranted to investigate the additional determinates associated with drug resistance of C. difficile.
The current study has several limitations. First, this is a single-center study with a small cohort. Studies with large number of clinical C. difficile isolates form pediatric patients are further needed. Second, we collected only one colony from each sample for AST and WGS, other C. difficile strains might be missed in patients with mixed infections. Particularly, toxigenic (TCD) strain that cause the disease were most likely missed in case with a non-toxigenic (NTCD) isolate. Third, fidaxomicin was not included in the AST because the antibiotic was not available at the time of testing. It is important to evaluate the susceptibility to fidaxomicin in clinical C. difficile isolates from pediatric patients to guide the future treatment choice. Finally, the clinical implications of the C. difficile isolates with reduced susceptibility to metronidazole and vancomycin are not determined due to the inconsistence between the antibiotic resistance and treatment outcome.
In summary, our results indicate that clinical C. difficile isolates with reduced susceptibility to metronidazole and vancomycin are emerging in a group of pediatric patients, which may explain a decline effectiveness of antibiotic-based therapy. The lack of pCD-METRO plasmid and vanA/B consistently associated with reduced susceptibility to metronidazole and vancomycin suggests additional mechanisms of resistance. Studies of susceptibility for fidaxomicin are necessary to guide its use for future therapy in pediatric CDI.
Abbreviations
CDI, C. difficile infection; RCDI, recurrent CDI; CDT, binary toxin; TcdA, enterotoxin A; TcdB, cytotoxin B; IBD, inflammatory bowel diseases; ARGs, antibiotic resistance genes; CARD, Comprehensive Antibiotic Resistance Database; AST, antimicrobial susceptibility testing; WGS, whole-genome sequencing; CCFA, cycloserine-cefoxitin fructose agar; MIC, minimal inhibitory concentrations; CDS, coding sequence; BHI, brain heart infusion; CLSI, Clinical and Laboratory Standard Institute; EUCAST, European Committee on Antimicrobial Susceptibility Testing; MDR, multidrug-resistant; ST, sequence type; MLST, multi-locus sequence typing.
Data Sharing Statement
Raw sequencing data have been deposited in NCBI SRA database under BioProject number PRJNA1047048.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013), and was approved by the Ethical Review Board of Shanghai Children’s Hospital [2022R043-E01], and informed consent was taken from parent or legal guardian of all the participates.
Acknowledgments
We thank Prof. Hong Zhang (Department of Clinical Laboratory, Shanghai Children’s Hospital) for helping us with the antimicrobial susceptibility tests.
Funding
This work was supported by the grants from the National Natural Science Foundation of China [Grant number: 81900472], the Natural Science Foundation of Shanghai [Grant number: 22ZR1451800], Shanghai Municipal Health Commission [Grant number: 20214Y0349, 202040479], the Training program for young talents of Shanghai Children’s Hospital [Grant number: 2021YQ03] and Medical Engineering Cross Project of Shanghai Jiao Tong University ‘Jiao Tong University Star’ Fund [Grant number: YG2022ZD022].
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. Martin JS, Monaghan TM, Wilcox MH. Clostridium difficile infection: epidemiology, diagnosis and understanding transmission. Nat Rev Gastroenterol Hepatol. 2016;13(4):206–216. doi:10.1038/nrgastro.2016.25
2. McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for clostridium difficile infection in adults and children: 2017 update by the infectious diseases society of America (IDSA) and society for healthcare epidemiology of America (SHEA). Clin Infect Dis. 2018;66(7):e1–e48. doi:10.1093/cid/cix1085
3. Buddle JE, Fagan RP. Pathogenicity and virulence of Clostridioides difficile. Virulence. 2023;14(1):2150452. doi:10.1080/21505594.2022.2150452
4. Krutova M, de Meij TGJ, Fitzpatrick F, Drew RJ, Wilcox MH, Kuijper EJ. How to: clostridioides difficile infection in children. Clin Microbiol Infect. 2022;28(8):1085–1090. doi:10.1016/j.cmi.2022.03.001
5. Wolf J, Kalocsai K, Fortuny C, et al. Safety and efficacy of fidaxomicin and vancomycin in children and adolescents with clostridioides (Clostridium) difficile infection: a phase 3, multicenter, randomized, single-blind clinical trial (SUNSHINE). Clin Infect Dis. 2020;71(10):2581–2588. doi:10.1093/cid/ciz1149
6. Peng Z, Jin D, Kim HB, et al. Update on antimicrobial resistance in clostridium difficile: resistance mechanisms and antimicrobial susceptibility testing. J Clin Microbiol. 2017;55(7):1998–2008. doi:10.1128/JCM.02250-16
7. Sholeh M, Krutova M, Forouzesh M, et al. Antimicrobial resistance in Clostridioides (Clostridium) difficile derived from humans: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2020;9(1):158. doi:10.1186/s13756-020-00815-5
8. Zhao H, Nickle DC, Zeng Z, et al. Global landscape of clostridioides difficile phylogeography, antibiotic susceptibility, and toxin polymorphisms by post-hoc whole-genome sequencing from the MODIFY I/II studies. Infect Dis Ther. 2021;10(2):853–870. doi:10.1007/s40121-021-00426-6
9. Darkoh C, Keita K, Odo C, et al. Emergence of clinical clostridioides difficile isolates with decreased susceptibility to vancomycin. Clin Infect Dis. 2022;74(1):120–126. doi:10.1093/cid/ciaa912
10. Li X, Xiao F, Li Y, et al. Characteristics and management of children with Clostridioides difficile infection at a tertiary pediatric hospital in China. Braz J Infect Dis. 2022;26(4):102380. doi:10.1016/j.bjid.2022.102380
11. Boekhoud IM, Hornung BVH, Sevilla E, et al. Plasmid-mediated metronidazole resistance in Clostridioides difficile. Nat Commun. 2020;11(1):598. doi:10.1038/s41467-020-14382-1
12. Boekhoud IM, Sidorov I, Nooij S, et al. Haem is crucial for medium-dependent metronidazole resistance in clinical isolates of Clostridioides difficile. J Antimicrob Chemother. 2021;76(7):1731–1740. doi:10.1093/jac/dkab097
13. Olaitan AO, Dureja C, Youngblom MA, et al. Decoding a cryptic mechanism of metronidazole resistance among globally disseminated fluoroquinolone-resistant Clostridioides difficile. Nat Commun. 2023;14(1):4130. doi:10.1038/s41467-023-39429-x
14. Deshpande A, Wu X, Huo W, Palmer KL, Hurdle JG. Chromosomal resistance to metronidazole in clostridioides difficile can be mediated by epistasis between iron homeostasis and oxidoreductases. Antimicrob Agents Chemother. 2020;64(8). doi:10.1128/AAC.00415-20
15. Shen WJ, Deshpande A, Hevener KE, et al. Constitutive expression of the cryptic vanGCd operon promotes vancomycin resistance in Clostridioides difficile clinical isolates. J Antimicrob Chemother. 2020;75(4):859–867. doi:10.1093/jac/dkz513
16. Eubank TA, Gonzales-Luna AJ, Hurdle JG, Garey KW. Genetic mechanisms of vancomycin resistance in clostridioides difficile: a systematic review. Antibiotics. 2022;11(2). doi:10.3390/antibiotics11020258
17. Pu M, Cho JM, Cunningham SA, et al. Plasmid acquisition alters vancomycin susceptibility in clostridioides difficile. Gastroenterology. 2021;160(3):941–945 e948. doi:10.1053/j.gastro.2020.10.046
18. CLSI. CaLSI: Performance Standards for Antimicrobial Susceptibility Testing.
19. EUCAST. Clinical breakpoints and dosing of antibiotics; 2022. Available from: https://wwweucastorg/clinical_breakpoints/.
20. PubMLST. Clostridioides difficile. Available from: https://pubmlst.org/cdifficile/.
21. Page AJ, Cummins CA, Hunt M, et al. Roary: rapid large-scale prokaryote pan genome analysis. Bioinformatics. 2015;31(22):3691–3693. doi:10.1093/bioinformatics/btv421
22. Emms DM, Kelly S. OrthoFinder: phylogenetic orthology inference for comparative genomics. Genome Biol. 2019;20(1):238. doi:10.1186/s13059-019-1832-y
23. iTOL. Interactive Tree of Life. Available from: https://itol.embl.de/itol.cgi.
24. VFDB. Available from: http://www.mgc.ac.cn/VFs/main.htm.
25. Resfinder. Available from: https://cge.cbs.dtu.dk/services/ResFinder.
26. Jia B, Raphenya AR, Alcock B, et al. CARD 2017: expansion and model-centric curation of the comprehensive antibiotic resistance database. Nucleic Acids Res. 2017;45(D1):D566–D573. doi:10.1093/nar/gkw1004
27. Inouye M, Dashnow H, Raven LA, et al. SRST2: rapid genomic surveillance for public health and hospital microbiology labs. Genome Med. 2014;6(11):90. doi:10.1186/s13073-014-0090-6
28. Krutova M, Wilcox M, Kuijper E. Clostridioides difficile infection: are the three currently used antibiotic treatment options equal from pharmacological and microbiological points of view? Int J Infect Dis. 2022;124:118–123. doi:10.1016/j.ijid.2022.09.013
29. Nicholson MR, Mitchell PD, Alexander E, et al. Efficacy of fecal microbiota transplantation for clostridium difficile infection in children. Clin Gastroenterol Hepatol. 2020;18(3):612–619 e611. doi:10.1016/j.cgh.2019.04.037
30. Alvarez AM, Rathore MH. Clostridium difficile Infection in Children. Adv Pediatr. 2019;66:263–280. doi:10.1016/j.yapd.2019.03.010
31. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825–834. doi:10.1056/NEJMoa1408913
32. Nicholson MR, Thomsen IP, Slaughter JC, Creech CB, Edwards KM. Novel risk factors for recurrent Clostridium difficile infection in children. J Pediatr Gastroenterol Nutr. 2015;60(1):18–22. doi:10.1097/MPG.0000000000000553
33. Farowski F, Solbach P, Tsakmaklis A, et al. Potential biomarkers to predict outcome of faecal microbiota transfer for recurrent Clostridioides difficile infection. Dig Liver Dis. 2019;51(7):944–951. doi:10.1016/j.dld.2019.01.012
34. Wen X, Shen C, Xia J, et al. Whole-genome sequencing reveals the high nosocomial transmission and antimicrobial resistance of clostridioides difficile in a single center in China, a four-year retrospective study. Microbiol Spectr. 2022;10(1):e0132221. doi:10.1128/spectrum.01322-21
35. Xu X, Luo Y, Chen H, et al. Genomic evolution and virulence association of Clostridioides difficile sequence type 37 (ribotype 017) in China. Emerg Microbes Infect. 2021;10(1):1331–1345. doi:10.1080/22221751.2021.1943538
36. Gargis AS, Karlsson M, Paulick AL, et al. Reference susceptibility testing and genomic surveillance of clostridioides difficile, United States, 2012–17. Clin Infect Dis. 2023;76(5):890–896. doi:10.1093/cid/ciac817
37. Huang H, Weintraub A, Fang H, Wu S, Zhang Y, Nord CE. Antimicrobial susceptibility and heteroresistance in Chinese Clostridium difficile strains. Anaerobe. 2010;16(6):633–635. doi:10.1016/j.anaerobe.2010.09.002
38. Greentree DH, Rice LB, Donskey CJ. Houston, we have a problem: reports of clostridioides difficile isolates with reduced vancomycin susceptibility. Clin Infect Dis. 2022;75(9):1661–1664. doi:10.1093/cid/ciac444
39. Peltier J, Courtin P, El Meouche I, et al. Genomic and expression analysis of the vanG-like gene cluster of Clostridium difficile. Microbiology. 2013;159(Pt 7):1510–1520. doi:10.1099/mic.0.065060-0
40. Farrow KA, Lyras D, Rood JI. Genomic analysis of the erythromycin resistance element Tn5398 from Clostridium difficile. Microbiology. 2001;147(Pt 10):2717–2728. doi:10.1099/00221287-147-10-2717
41. Roberts MC. Acquired tetracycline and/or macrolide-lincosamides-streptogramin resistance in anaerobes. Anaerobe. 2003;9(2):63–69. doi:10.1016/S1075-9964(03)00058-1
42. Dridi L, Tankovic J, Petit JC. CdeA of Clostridium difficile, a new multidrug efflux transporter of the MATE family. Microb Drug Resist. 2004;10(3):191–196. doi:10.1089/mdr.2004.10.191
43. Liu J, Peng L, Su H, et al. Chromosome and plasmid features of two ST37 clostridioides difficile strains isolated in China reveal distinct multidrug resistance and virulence determinants. Microb Drug Resist. 2020;26(12):1503–1508. doi:10.1089/mdr.2019.0461
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.