Back to Journals » Journal of Inflammation Research » Volume 15
Anti-Inflammatory Effect of Ulinastatin on the Association Between Inflammatory Phenotypes in Acute Type A Aortic Dissection
Authors Liu H, Qian SC, Shao YF, Li HY
Received 28 April 2022
Accepted for publication 21 June 2022
Published 27 June 2022 Volume 2022:15 Pages 3709—3718
DOI https://doi.org/10.2147/JIR.S369703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Hong Liu,1,* Si-chong Qian,2,* Yong-feng Shao,1 Hai-yang Li2 On behalf of the Additive Anti-inflammatory Action for Aortopathy & Arteriopathy (5A) Investigators Group
1Department of Cardiovascular Surgery, the First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, People’s Republic of China; 2Department of Cardiovascular Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, 100029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong-feng Shao, Department of Cardiovascular Surgery, the First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, People’s Republic of China, Email [email protected] Hai-yang Li, Department of Cardiovascular Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, 100029, People’s Republic of China, Email [email protected]
Background: Acute type A aortic dissection (ATAAD) is a heterogeneous systemic inflammatory response syndrome. Identification of distinct inflammatory phenotypes may allow more precise therapy and improved care. We aim to investigate whether distinct inflammatory subphenotypes exist in ATAAD patients and respond differently to pharmacotherapies.
Methods: Retrospective analysis of data sets was conducted from the Additive Anti-inflammatory Actions for Aortopathy & Arteriopathy (5A) III study. Inflammatory subphenotypes were derived among 2008 ATAAD patients who received surgical repair at 11 Chinese hospitals (2016– 2020) using latent class analysis applied to 14 laboratory signatures within 6 hours of hospital admission. Outcomes included operative mortality (Society of Thoracic Surgeons definition), derived subphenotype frequency, and the potential consequences of phenotype frequency distributions on the treatment effects.
Results: The median (interquartile range) age of patients was 54 (45– 62) years, and 1423 (70.9%) were male. A two-class (two subphenotype) model was an improvement over a one-class model (P<· 001), with 1451 (72.3%) patients in the hypoinflammatory subphenotype group and 557 (27.7%) in the hyperinflammatory subphenotype group. Patients with the hyperinflammatory subphenotype had higher operative mortality (71 [12.7%] vs 127 [8.8%]; P=0· 007) than did those with the hypoinflammatory subphenotype. Furthermore, the interaction between ulinastatin treatment and subphenotype is not significant for operative mortality (P=0.15) but for ventilator time (P=0· 04).
Conclusion: Two subphenotypes of ATAAD were identified in the 5A cohort that correlated with clinical outcomes, with significant interaction effect between anti-inflammatory treatment and subphenotypes for ventilator time, suggesting these phenotypes may help in understanding heterogeneity of treatment effects.
Trial Registration: Clinical Trials. Gov: number NCT04918108.
Keywords: aortic dissection, inflammatory response, latent class analysis
Background
Previous studies have demonstrated that patients with acute Type A aortic dissection (ATAAD) have a marked inflammatory response.1 Given the heterogeneity of these critically ill patients and their underlying illnesses, it is plausible that several subphenotypes of ATAAD exist, analogous to those in asthma,2 acute respiratory distress syndrome3 and sepsis.4 It is not known, most importantly, whether they might respond differently to pharmacotherapies.
Since the time of the original classification of aortic dissection, there has been recognition of anatomopathological heterogeneity within aortic dissection; this heterogeneity might reflect our incomplete understanding of the disease characteristics and probably contributes to the poor treatments for patients with aortic dissection.5 As a result, some investigators have proposed subdividing aortic dissection on the basis of dissection’s extension, primary entry location and end-organ malperfusion as well as clinical presentation, without deep insight into concomitant systemic inflammatory response.6 It is well recognized that ATAAD is usually complicated by extensive systemic inflammatory response to its aetiopathologies; however, little knowledge exists on identifying inflammatory subphenotypes among aortic dissection patients.7 We hypothesize that TAAD is a heterogeneous inflammatory syndrome that might have inflammatory subphenotypes.
Ulinastatin, a type of urinary trypsin inhibitor, is a glycoprotein and a nonspecific protease inhibitor, which could suppress proinflammatory cytokine elevation and upregulate the release of anti-inflammatory mediators.8 Recent evidence has demonstrated that ulinastatin can reduce pulmonary injury, improve pulmonary function,9 and improve intensive care unit length of stay in cardiopulmonary bypass patients.10 However, little is known regarding whether distinct inflammatory subphenotypes exist in ATAAD patients and respond differently to pharmacotherapies.
Accordingly, we use a combination of clinically available laboratory data of ATAAD patients from Chinese multicenter cohort aimed at identifying inflammatory subphenotypes of ATAAD and investigating whether distinct subphenotypes respond differently to pharmacotherapies.
Patients and Methods
Patients
Form an investigator-initiated Additive Anti-inflammatory Action for Aortopathy & Arteriopathy (5A) III Project, we retrospectively identified 2008 adult patients with ATAAD who underwent open surgical repair for ATAAD from 11 Chinese cardiovascular centers (the First Affiliated Hospital of Nanjing Medical University; the First Affiliated Hospital of Guangzhou Medical University; the First Affiliated Hospital of Shantou University Medical College; Nanjing First Hospital; the Affiliated Hospital of Qingdao University; Xiamen Cardiovascular Hospital; Teda International Cardiovascular Hospital; Shanghai East Hospital; Xiangya Hospital; Beijing Anzhen Hospital; Tianjin Chest Hospital) between Jan 2016 and Dec 2020. Patients with chronic aortic dissection/aneurysms and traumatic aortic rupture and those with only endovascular or medical management were excluded (Figure 1). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Review Board of Aortic Collaborative Institutions involved (2021-SR-381). This study was registered with ClinicalTrials.gov number NCT04918108. Considering this retrospective study, the committee gave up the written informed consent, and the data has been analyzed anonymously and all personal information of the participants was confidential.
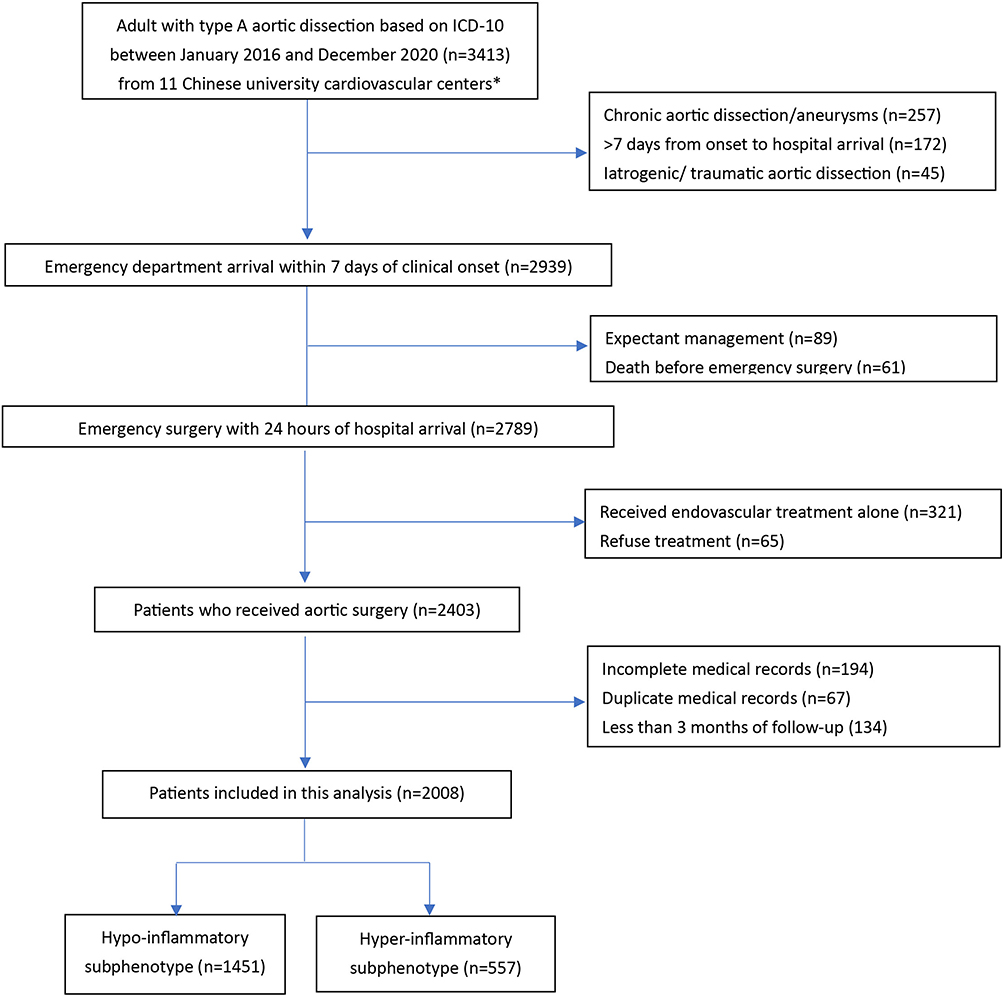 |
Figure 1 Patient selection flow chart. |
Candidate Variables for Phenotyping
We selected 14 candidate laboratory variables based on their association with aortic dissection onset or outcome and their availability in the electronic health record at hospital presentation. These included neutrophils, lymphocytes, monocyte, platelet, neutrophils-lymphocyte ratio (NLR), platelet–lymphocyte ratio (PLR), lymphocyte–monocyte ratio (LMR), systemic inflammation-immune index (SII), creatinine, blood urea nitrogen, alanine aminotransferase, fibrinogen, and D-dimer. For each variable, we extracted the most abnormal value recorded within the first 6 hours of hospital presentation. In addition, we recorded whether patients received ulinastatin (a human urinary trypsin inhibitor) therapy immediately after surgery within intensive care unit (ICU) admission. The main surgical techniques used in this study have been described before.11
Outcome
The primary outcome was operative mortality, defined as any death, regardless of cause, occurring within 30 days after surgery in or out of the hospital, and after 30 days during the same hospitalization subsequent to the operation, according to the Society of Thoracic Surgeons criteria.12 Secondary outcomes included the 30-day, 90-day, hospital, and ICU mortality, as well as mechanical ventilation duration, ICU length of stay, and hospital length of stay. All outcomes were adjudicated independently by an event collaborative team.
Latent Class Analysis
To estimate the optimal number of classes in the data, we fitted latent class models in Mplus v8 using 14 available baseline laboratory data of interest as class-defining variables, without consideration of clinical outcomes.13 We estimated models ranging from one to four classes to identify the optimal number of classes, using Bayesian Information Criteria, the Vuong-Lo-Mendell-Rubin likelihood ratio test, class size, and entropy.3,14 To estimate model parameters, we placed continuous variables on a Z scale with a mean of 0 and SD of 1.15
Statistical Analysis
Once we established the optimal number of classes, we assigned study participants to their most likely class, and compared their baseline characteristics using t-tests, Pearson’s χ2, or Wilcoxon rank-sum test depending on the nature of the variable. We used Kaplan–Meier curves with Log rank test to test for inflammatory categorization of survival (time to death). We assessed the association of inflammatory categorization class with the odds ratio (OR) of operative mortality with 95% confidence interval (CI) using crude and adjusted logistic regression model for potential risk factors. We explored traditional analyses of heterogeneity to understand the potential consequences of different phenotype frequency distributions on the estimation of the treatment effects in a similar adjusted multivariable model. We did analyses other than latent class analysis using Stata version 14 (Stata Corp, College Station, TX, USA) and R software (version 3.2.0). The p values of less than 0.05 were considered statistically significant.
Results
A total of 2008 patients with ATAAD were included in this study with a median (IQR) age of 54 (45–62) years and 1423 (70.9%) male, of which 1556 (77.5%) underwent total arch replacement plus frozen elephant trunk and 1715 (85.4%) underwent circulatory arrest of lower body. Baseline, clinical and procedural characteristics are listed in Table 1.
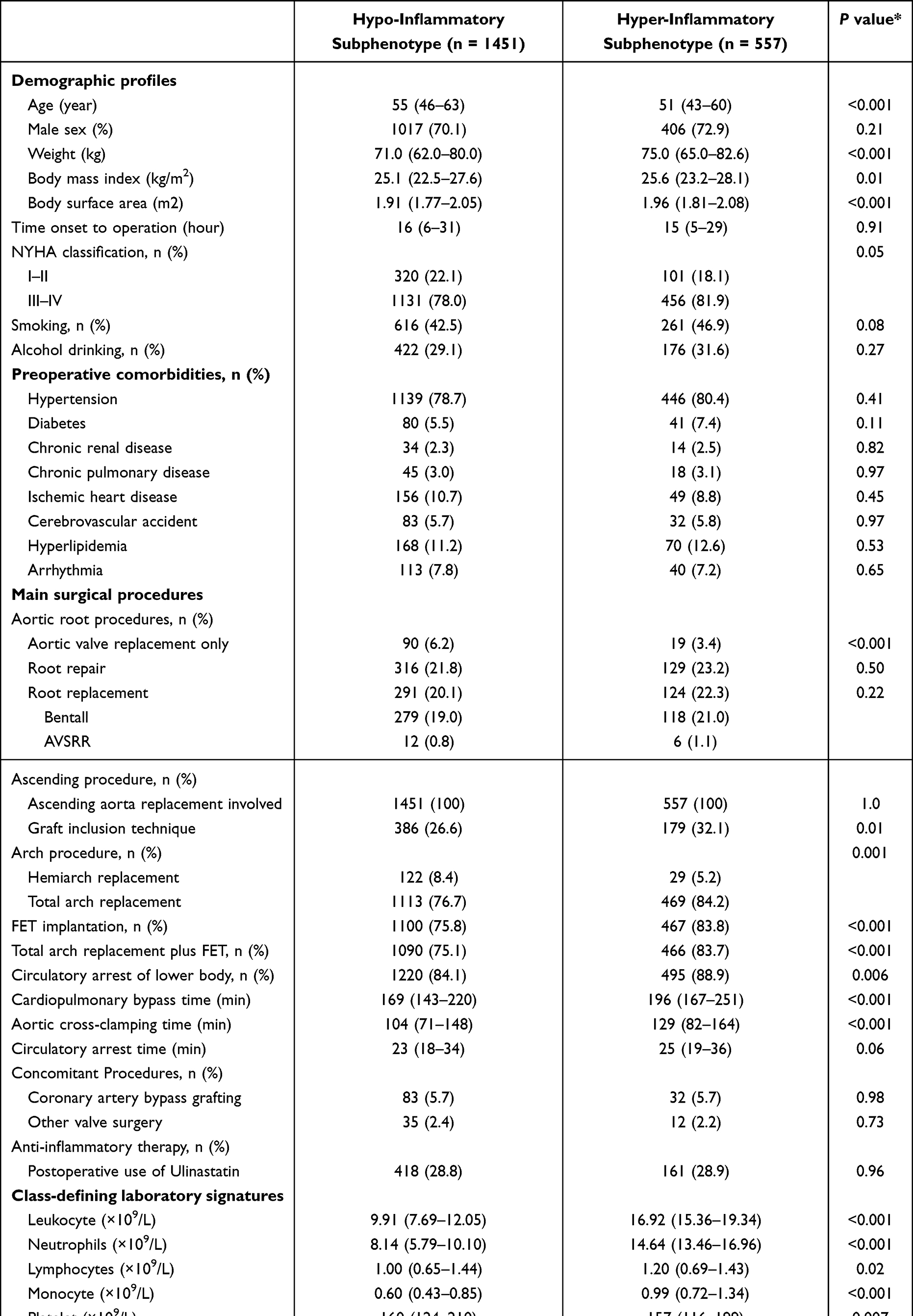 |
Table 1 Baseline and Clinical Characteristics and Class-Defining Variables Between Subphenotypes |
Analysis of latent-class models showed that a two-class model provided the best fit (Table 2), with 1451 (72.3%) patients assigned to class one (hypoinflammatory subphenotype) and 557 (27.7%) patients to class two (hyperinflammatory subphenotype). The average latent class probabilities were 0.957 for class one and 0.915 for class 2. Specifically, patients in hyperinflammatory subphenotype had higher values of neutrophils, lymphocytes, monocyte counts, NLR, SII, creatinine, blood urea nitrogen, alanine aminotransferase, and D-dimer, and lower platelet counts, PLR, LMR, and fibrinogen than did those in hypoinflammatory subphenotype (Figure 2; Table 1).
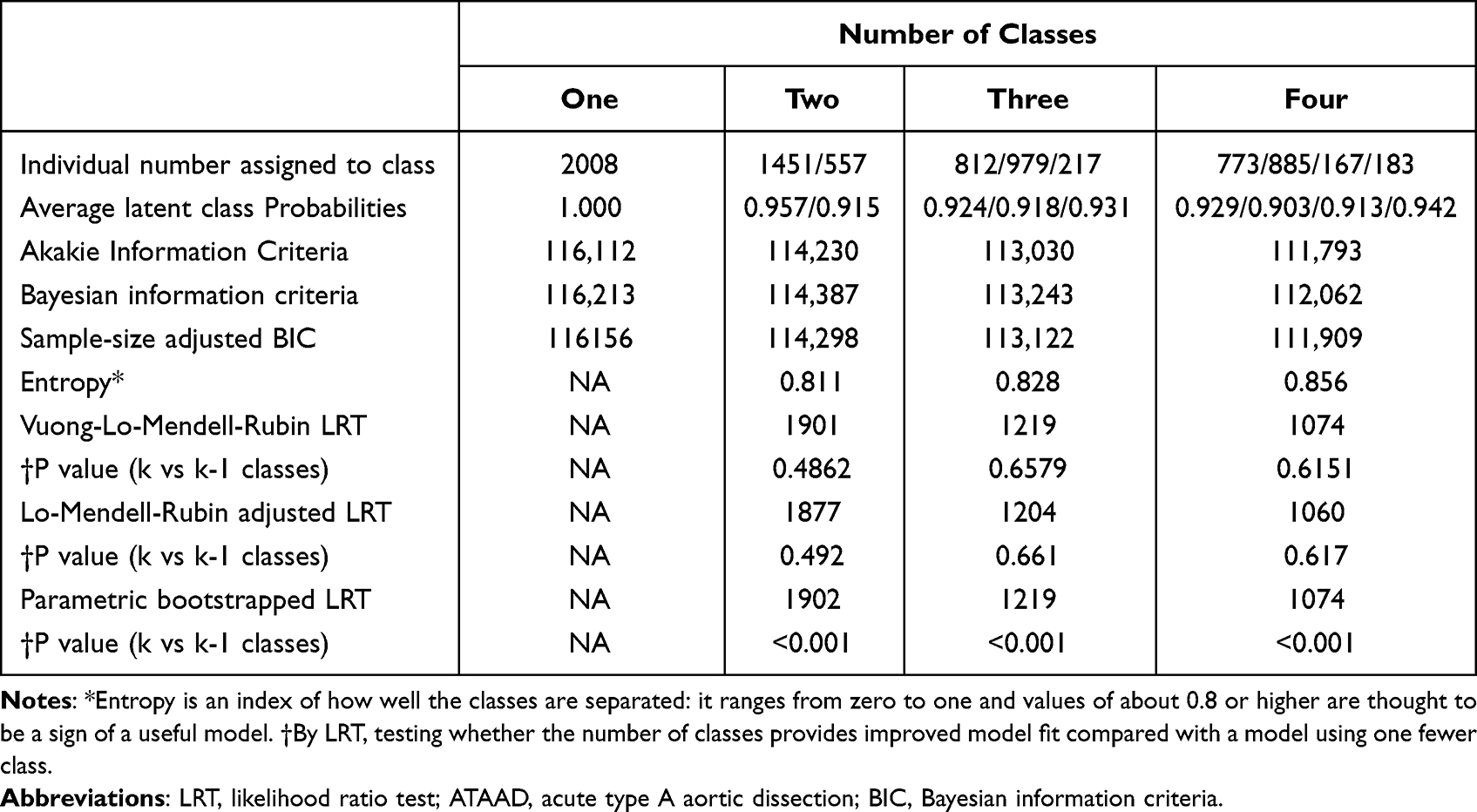 |
Table 2 Model Fit Statistics for One to Four Latent Classes of Subjects with ATAAD |
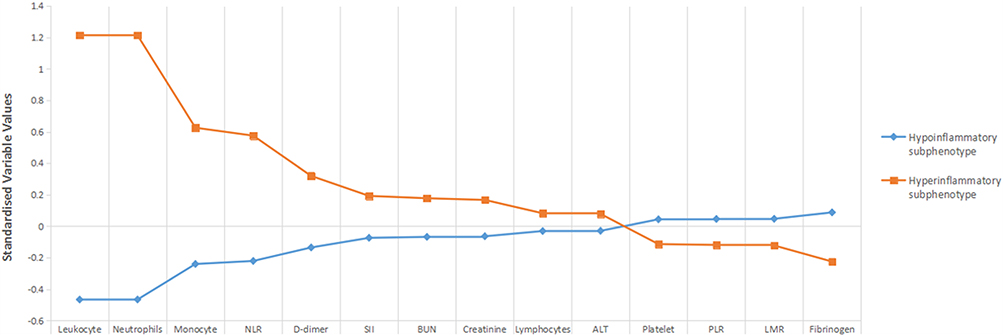 |
Figure 2 Differences in standardised values of each continuous variable by subphenotype. Variables are sorted on the basis of the degree of separation between the subphenotypes, from maximum positive separation on the left (ie, hyperinflammatory subphenotype higher than hypoinflammatory subphenotype) to maximum negative separation on the right (ie, hyperinflammatory subphenotype lower than hypoinflammatory subphenotype). The y-axis represents standardised variable values, in which all means are scaled to 0 and SDs to 1. A value of +1 for the standardised variable signifies that the mean value for a given subphenotype was 1 SD higher than the mean value in the cohort as a whole. Mean values are joined by lines to facilitate display of subphenotype profiles. Abbreviations: NLR, neutrophils-lymphocyte ratio; PLR, platelet–lymphocyte ratio; LMR, lymphocyte–monocyte ratio; SII, systemic inflammation-immune index; BUN, blood urea nitrogen; ALT, alanine aminotransferase. |
Besides, patients in hyperinflammatory subphenotype were more likely to have younger age (P < 0.001), heavier weight (P < 0.001), and worse cardiac function as evidenced by the NYHA classification (P = 0.05). With respect to the procedures, patients in hyperinflammatory subphenotype were more likely to receive less aortic valve replacement only (P < 0.001), more graft inclusion technique (P = 0.01), more total arch replacement (P = 0.001), more FET implantation (P < 0.001), and more circulatory arrest of lower body (P = 0.006). In contrast, there were similar distributions between hypoinflammatory and hyperinflammatory subphenotype in terms of demographic profiles, preoperative comorbidities and surgical procedures in Table 1.
Patients with the hyperinflammatory subphenotype had higher operative mortality (71 [12.7%] vs 127 [8.8%]; crude OR 1.523 [95% CI 1.119–2.073]; P = 0.008) than did those with the hypoinflammatory subphenotype. After adjustment for potential risk factors, hyperinflammatory subphenotype remained significantly associated with higher risk of operative mortality than hypoinflammatory subphenotype: adjusted for demographic profiles OR 1.513 [1.091–2.100], P = 0.013; additional adjusted for preoperative comorbidities OR 1.745 [1.222–2.491], P = 0.002; and additional adjusted for surgical procedures OR 1.912 [1.323–2.761], P < 0.001.
Furthermore, hyperinflammatory subphenotype was significantly associated with higher risk of 30-day mortality, 90-day mortality, ICU mortality, and hospital mortality, as well as longer ventilation support time and ICU stay compared with hypoinflammatory subphenotype, respectively (Table 3). When stratified by inflammatory subphenotype, the survival curve was significantly lower for the hyperinflammatory subphenotype than for the hypoinflammatory subphenotype in ATAAD patients (hypoinflammatory vs hyperinflammatory, 0.913 [95% CI 0.899–0.928] vs 0.873 [95% CI 0.845–0.900], respectively; P for Log rank test = 0.005, Figure 3).
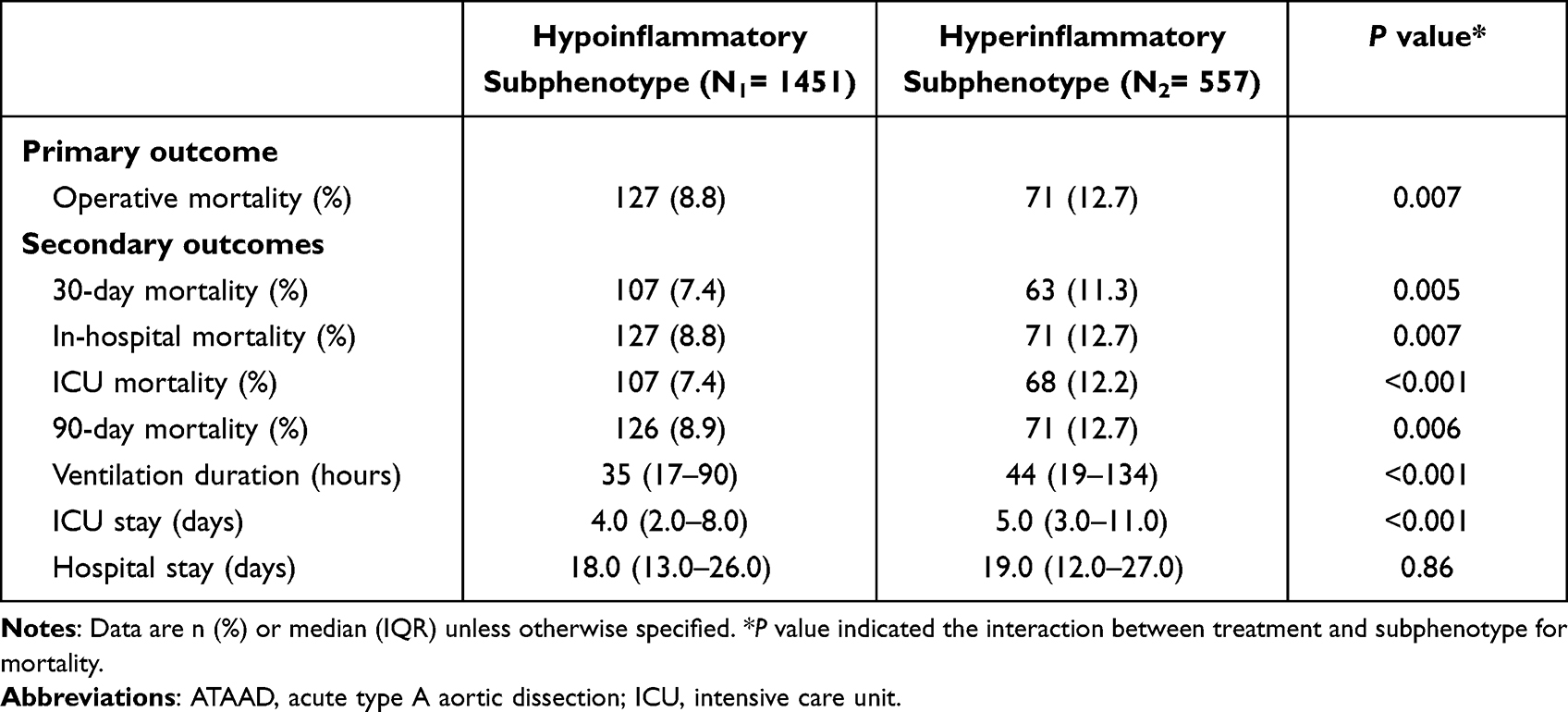 |
Table 3 Clinical Outcomes by ATAAD Inflammatory Subphenotype |
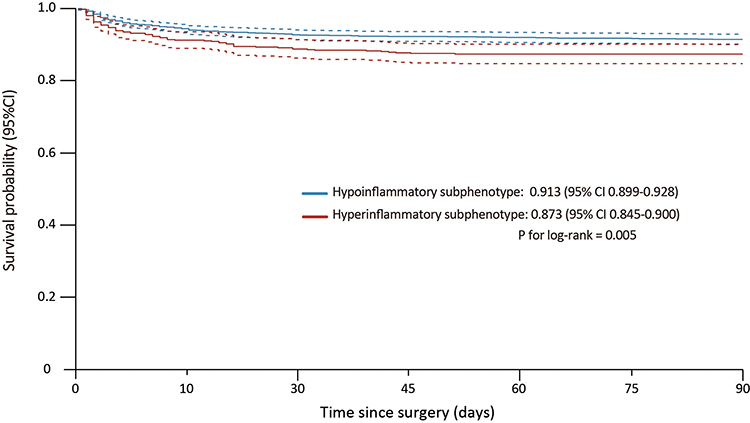 |
Figure 3 Kaplan-Meier survival curves. 90-day patient survival in stratified by acute type A aortic dissection inflammatory subphenotype. |
Operative mortality was similar in patients with the hypoinflammatory subphenotype and in patients with the hyperinflammatory subphenotype regardless of ulinastatin, without interaction between ulinastatin and subphenotype (Pinteraction= 0.15). Importantly, ventilator time in the hyperinflammatory subphenotype was numerically lower in patients with ulinastatin than in those without, in contrast to patients with the hypoinflammatory subphenotype, for whom ventilator time was the same in patients with and without ulinastatin, with significant interaction between treatment and subphenotype (Pinteraction= 0.04) (Table 4).
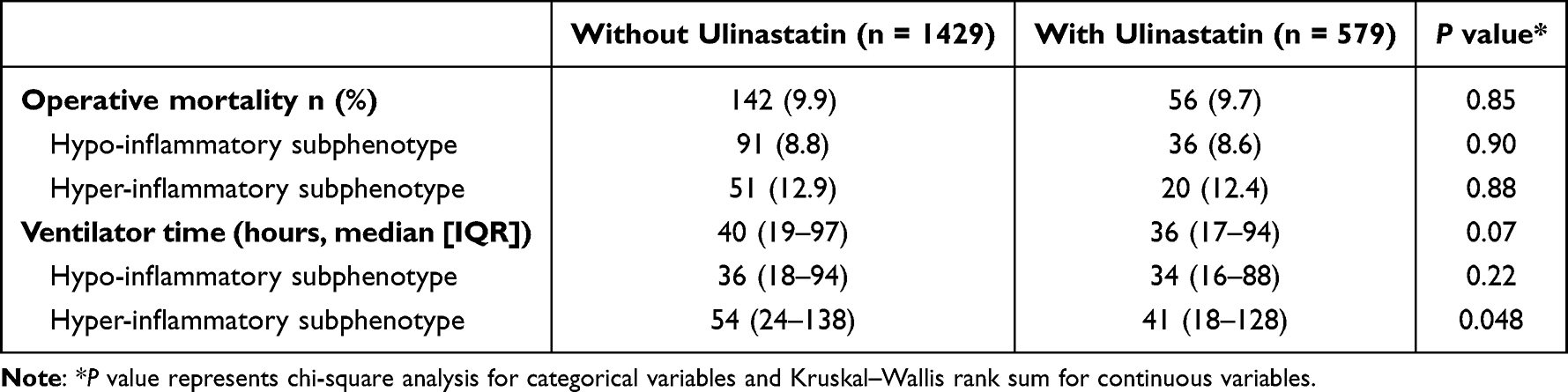 |
Table 4 Analysis of Clinical Outcome of Interest Across Patients Stratified by Ulinastatin Treatment and Subphenotype |
Discussion
In this study, two inflammatory subphenotypes were derived using routinely available clinical data of ATAAD patients at the time of hospital presentation. Hyperinflammatory subphenotype was more strongly correlated with abnormal values of inflammatory response biomarkers and 30-day, ICU, 90-day, and hospital mortality, as well as ventilation time in comparison to hypoinflammatory subphenotype.
Patients with these two subphenotypes of ATAAD responded differently to ulinastatin, with evidence of shorter ventilator time uniquely among those with hyperinflammatory subphenotype of ATAAD rather than hypoinflammatory subphenotype, with interaction between treatment and subphenotype.
More efforts were made to optimize the classification systems of aortic dissections mainly based on the anatomopathological and clinical characteristics of ATAAD,16–18 however, it does not account for different systemic inflammatory responses to its aetiopathologies. Thus, we introduced a novel inflammatory aortic dissection classification to create a new system that categorizes the extent of inflammatory response. These phenotypes can be identified at the time of patient presentation to the emergency department, and thus it will provide physicians with inflammatory information in anti-inflammatory management of TAAD patients. Only routinely available data were used in the clustering models, and the phenotypes were derived from a large multicenter observational cohort to ensure generalizability. Furthermore, this proof-of-concept sub-phenotyping could be incorporated prospectively in future study designs that test new biologically active therapeutics.
Based on our analysis of all patients with ATAAD from 11 cardiovascular centers, more than 50% of them were categorized as hypo-inflammatory subphenotype. Emergency aortic repair was performed for patients included in this study, including ascending replacement in all patients and aortic arch replacement in three quarters of the patients in this study. Our finding showed that patients with hyper-inflammatory subphenotype were associated with higher 30-day mortality, 90-day mortality, ICU mortality and in-hospital mortality, as well as longer ventilation duration and ICU stay than those with hypo-inflammatory subphenotype. Recognition of the differences in inflammatory response will advance our best knowledge of acute aortic syndrome and improve our decision-making for better therapies19.
Knowledge is limited regarding the role of ulinastatin in the setting of aortic dissection. A prospective, randomized and double-blinded study from Xu et al investigated the effects of high-dose ulinastatin on the release of proinflammatory cytokines and lung injury in patients with aortic dissection after cardiopulmonary bypass under deep hypothermic circulatory arrest,20 suggesting that high-dose ulinastatin attenuates the elevation of cytokines, reduces the pulmonary injury and improves the pulmonary function after surgical repair. Despite no significant difference in ventilator time between patients without and with Ulinastatin, it may be anticipated that Ulinastatin is most effective in the hyperinflammatory patients, due to its anti-inflammatory effects, which is only 25% of the patients. Importantly, our subgroup analysis showed a significant interaction between ulinastatin treatment and subphenotype existed for ventilator time, suggesting that the patients with hyperinflammatory subphenotype were more likely to benefit from postoperative ulinastatin use than patients with hypoinflammatory subphenotype, especially in improving the lung function.9,21,22
ATAAD hyperinflammatory subphenotype patients preferentially responding to Ulinastatin have biological plausibility on the basis of the presumed mechanism of action of ulinastatin in ATAAD. Ulinastatin can systematically cause inflammation and injury in both animal models of lipopolysaccharide-induced acute inflammatory injury and preclinical human experimental studies and have lysosomal and protease stabilizing properties.23–25 Thus, patients with more systemic inflammations, such as those with the hyperinflammatory subphenotype, could be most likely to respond to this therapy.
Limitations
To our knowledge, our study is the first to report a differential response to pharmacotherapy by inflammatory subphenotype in ATAAD. Still, this study is not without limitations. First, the associations cannot be interpreted as causal and residual confounding cannot be excluded, owing to the observational nature of this study. Second, the analysis of anti-inflammatory treatment × subphenotype interactions may be limited by small sample sizes. Third, no genetic information was known about these patients included in this study, such as FBN1 mutations. Marfan patients have very little inflammation in their aortic aneurysm compared to the typical inflammatory thoracic aneurysms, thus hypoinflammatory patients are likely to have genetic variants in extracellular matrix-related genes. Also, our study lacked the information regarding the anatomical morphologies of aortic valve for included patients, such as bicuspid aortic valve (BAV). Patients with BAV may also have less inflammation, just like the Marfan patients. Therefore, the addition of the aforementioned genetic and anatomical information would advance our better understanding of these two phenotypes in the further studies. Finally, the ulinastatin treatment might be rarely used in the treatment of ATAAD in other countries; therefore, the specific expertise may differ from those of other countries, potentially limiting the generalizability of these results in other institutions.
Conclusion
Our analysis identified two distinct subphenotypes of ATAAD, one of which had significantly improved ventilation with ulinastatin therapy in comparison to those without. These findings support further pursuit of predictive enrichment strategies in critical care clinical trials.
Ethics Statement
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the Institutional Review Board of Aortic Collaborative Institutions involved (2021-SR-381). This study was registered with ClinicalTrials.gov number NCT04918108. Considering this retrospective study, the committee gave up the written informed consent, and the data have been analyzed anonymously and all personal information of the participants was confidential.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgment
Group information: the 5A Investigators are listed in the Supplementary material.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82000305, 82070483), Scientific Research Common Program of Beijing Municipal Commission of Education (KM202110025014), and Beijing Municipal Science and Technology Commission (Z211100002921010).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Allaire E, Schneider F, Saucy F, et al. New insight in aetiopathogenesis of aortic diseases. Eur J Vasc Endovasc Surg. 2009;37(5):531–537. doi:10.1016/j.ejvs.2009.02.002
2. Depner M, Fuchs O, Genuneit J, et al.; PASTURE Study Group. Clinical and epidemiologic phenotypes of childhood asthma. Am J Respir Crit Care Med. 2014;189(2):129–138. doi:10.1164/rccm.201307-1198OC
3. Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA; NHLBI ARDS Network. Subphenotypes in acute respiratory distress syndrome: latent class analysis of data from two randomised controlled trials. Lancet Respir Med. 2014;2(8):611–620. doi:10.1016/S2213-2600(14)70097-9
4. Seymour CW, Kennedy JN, Wang S, et al. Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis. JAMA. 2019;321(20):2003–2017. doi:10.1001/jama.2019.5791
5. Takano H, Inoue K, Shimada A, Sato H, Yanagisawa R, Yoshikawa T. Urinary trypsin inhibitor protects against liver injury and coagulation pathway dysregulation induced by lipopolysaccharide/D-galactosamine in mice. Lab Invest. 2009;89(7):833–839. doi:10.1038/labinvest.2009.35
6. Czerny M, Schoenhoff F, Etz C, et al. The impact of pre-operative malperfusion on outcome in acute type A aortic dissection: results from the GERAADA registry. J Am Coll Cardiol. 2015;65:2628–2635. doi:10.1016/j.jacc.2015.04.030
7. Kanai T, Ishiwata T, Kobayashi T, et al. Ulinastatin, a urinary trypsin inhibitor, for the initial treatment of patients with Kawasaki disease: a retrospective study. Circulation. 2011;124(25):2822–2828. doi:10.1161/CIRCULATIONAHA.111.028423
8. Astrup T, Nissen U. urinary trypsin inhibitor (MINGIN): transformation into a new trypsin inhibitor by acid hydrolysis or by sialidase. Nature. 1964;203:255–257. doi:10.1038/203255a0
9. He G, Li Q, Li W, et al. Effect of ulinastatin on interleukins and pulmonary function in bypass patients: a meta-analysis of randomized controlled trials. Herz. 2020;45(4):335–346. doi:10.1007/s00059-018-4732-0
10. Zhenyu H, Qiaoli Y, Guangxiang C, Maohua W. The effect of ulinastatin on postoperative course in cardiopulmonary bypass patients in Asia: a meta-analysis of randomized controlled trials. J Cardiothorac Surg. 2022;17(1):66. doi:10.1186/s13019-022-01811-z
11. Sun L, Qi R, Zhu J, Liu Y, Zheng J. Total arch replacement combined with stented elephant trunk implantation: a new “standard” therapy for type a dissection involving repair of the aortic arch? Circulation. 2011;123(9):971–978. doi:10.1161/CIRCULATIONAHA.110.015081
12. Overman DM, Jacobs JP, Prager RL, et al. Report from the society of thoracic surgeons national database workforce: clarifying the definition of operative mortality. World J Pediatr Congenit Heart Surg. 2013;4(1):10–12. doi:10.1177/2150135112461924
13. Rindskopf D, Rindskopf W. The value of latent class analysis in medical diagnosis. Stat Med. 1986;5(1):21–27. doi:10.1002/sim.4780050105
14. Schwartz G. Estimating the dimension of a model. Ann Stat. 1978;6:461–464.
15. Lo YT, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88(3):767–778. doi:10.1093/biomet/88.3.767
16. Augoustides JG, Szeto WY, Desai ND, et al. Classification of acute type A dissection: focus on clinical presentation and extent. Eur J Cardiothorac Surg. 2011;39(4):519–522. doi:10.1016/j.ejcts.2010.05.038
17. Dake MD, Thompson M, van Sambeek M, Vermassen F, Morales JP. DEFINE Investigators. DISSECT: a new mnemonic-based approach to the categorization of aortic dissection. Eur J Vasc Endovasc Surg. 2013;46(2):175–190. doi:10.1016/j.ejvs.2013.04.029
18. Sievers HH, Rylski B, Czerny M, et al. Aortic dissection reconsidered: type, entry site, malperfusion classification adding clarity and enabling outcome prediction. Interact Cardiovasc Thorac Surg. 2020;30(3):451–457. doi:10.1093/icvts/ivz281
19. Rimmer LJ, Moughal S, Bashir M. Immunological therapeutics in acute aortic syndrome. Asian Cardiovasc Thorac Ann. 2020;28(8):512–519. doi:10.1177/0218492320943350
20. Xu CE, Zou CW, Zhang MY, Guo L. Effects of high-dose ulinastatin on inflammatory response and pulmonary function in patients with type-A aortic dissection after cardiopulmonary bypass under deep hypothermic circulatory arrest. J Cardiothorac Vasc Anesth. 2013;27(3):479–484. doi:10.1053/j.jvca.2012.11.001
21. Nakanishi K, Takeda S, Sakamoto A, Kitamura A. Effects of ulinastatin treatment on the cardiopulmonary bypass-induced hemodynamic instability and pulmonary dysfunction. Crit Care Med. 2006;34(5):1351–1357. doi:10.1097/01.CCM.0000215110.55899.AE
22. Cao C, Yin C, Shou S, et al. Ulinastatin protects against LPS-induced acute lung injury by attenuating TLR4/NF-κB pathway activation and reducing inflammatory mediators. Shock. 2018;50(5):595–605. doi:10.1097/SHK.0000000000001104
23. Wang J, Zhou J, Bai S. Combination of glutamine and ulinastatin treatments greatly improves sepsis outcomes. J Inflamm Res. 2020;13:109–115. doi:10.2147/JIR.S234122
24. Song D, Song G, Niu Y, et al. Ulinastatin activates haem oxygenase 1 antioxidant pathway and attenuates allergic inflammation. Br J Pharmacol. 2014;171(19):4399–4412. doi:10.1111/bph.12780
25. Karnad DR, Bhadade R, Verma PK, et al. Intravenous administration of ulinastatin (human urinary trypsin inhibitor) in severe sepsis: a multicenter randomized controlled study. Intensive Care Med. 2014;40(6):830–838. doi:10.1007/s00134-014-3278-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.