Back to Journals » ImmunoTargets and Therapy » Volume 10
Anti-CD52 Therapy for Multiple Sclerosis: An Update in the COVID Era
Authors Kasarello K, Mirowska-Guzel D
Received 18 March 2021
Accepted for publication 22 May 2021
Published 7 July 2021 Volume 2021:10 Pages 237—246
DOI https://doi.org/10.2147/ITT.S240890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Kaja Kasarello,1 Dagmara Mirowska-Guzel2,3
1Department of Experimental and Clinical Physiology, Centre for Preclinical Research, Medical University of Warsaw, Warsaw, Poland; 2Department of Experimental and Clinical Pharmacology, Centre for Preclinical Research, Medical University of Warsaw, Warsaw, Poland; 3Second Department of Neurology, Institute of Psychiatry and Neurology, Warsaw, Poland
Correspondence: Dagmara Mirowska-Guzel
Department of Experimental and Clinical Pharmacology, Centre for Preclinical Research, Medical University of Warsaw, Banacha 1b, Warsaw, 02-097, Poland
Tel +48 22 116-6160
Fax +48 22 1166202
Email [email protected]
Abstract: CD52 is a small surface glycoprotein composed of 12 amino acids. CD52 is found mostly on the surface of mature immune cells, such as lymphocytes, monocytes, eosinophils, and dendritic cells, as well as the male genital tract: within the epididymis and on the surface of mature sperm. Low CD52 expression is also found in neutrophils. CD52 function is not fully understood, although experiments with anti-CD52 antibodies have shown that CD52 is essential for lymphocyte transendothelial migration and may contribute to costimulation of CD4+ T cells and T-cell activation and proliferation. Although knowledge about exact CD52 function is still poor, CD52 presence on the surface of a broad spectrum of immune cells makes it a therapeutic target, especially in immunomediated diseases, such as multiple sclerosis. In multiple sclerosis, alemtuzumab is registered for adult patients with the relapsing–remitting form of the disease defined by clinical and imaging features. Despite the high efficacy of the drug, the main issue is its safety. The main adverse effects of alemtuzumab are associated with drug infusion due to cytokine release and cytotoxic effects of antibodies associated with lymphocyte depletion, which leads to immunosuppression, and secondary autoimmunity that may be the effect of excessive B-cell repopulation and cancer. This review presents current knowledge on the drug’s mechanism of action, efficacy and safety data from clinical trials, and real-world observations, including available though scarce data on using alemtuzumab in the COVID era.
Keywords: CD52, therapy, multiple sclerosis, alemtuzumab
Biology of Anti-CD52 Therapy
CD52
CD52, also known as the Campath-1 antigen, is a small surface glycoprotein composed of 12 amino acids. CD52 is anchored to the cell membrane by glycosylphosphatidylinositol at the C terminus.1,1–4 CD52 is found mostly on the surface of mature immune cells (lymphocytes, monocytes, eosinophils, and dendritic cells [DCs] and the male genital tract: within the epididymis and on the surface of mature sperm. Low CD52 expression is found in neutrophils.5 What is important is that CD52 is found neither on stem/progenitor immune cells, erythrocytes, nor platelets.3 CD52 function is not fully understood, although experiments with anti-CD52 antibodies have shown that it is essential for lymphocyte transendothelial migration6 and may also contribute to costimulation of CD4+ T cells7 and T-cell activation and proliferation.8
The role of soluble CD52 has been reported on. Release of CD52 from activated T cells is mediated by phospholipase C. Soluble CD52 binds to the HMGB1 protein, subsequently to Siglec 10 receptors present on the adjacent T cells.9 This binding lead to suppression of T-cell activation by inhibition of phosphorylation of tyrosine residues, which is required for signaling via T-cell receptors. Suppression of other immune cells by soluble CD52 is also possible while those cells also express Siglec 10.10–12 Soluble CD52 likewise inhibits Toll-like receptors or TNF signaling, thus inhibiting the NFκB pathway and proinflammatory cytokine production. High levels of CD52 induce apoptotic cell death via BAK and BAX signaling.13
Anti-CD52
Although knowledge about CD52 function is poor, CD52 presence on the surface of a broad spectrum of immune cells makes it a good therapeutic target. Eliminating CD52-expressing cells may be beneficial in lymphocyte-mediated diseases, as CD52 is highly expressed in those cells.3,14
The anti-CD52 antibody Campath-1 was first designed for preventing graft-versus-host disease and possible antileukemic activity. Campath-1 is a rat monoclonal antibody directed against human CD52, leading to lysis of the lymphocytes expressing the CD52 antigen. While progenitor cells do not express CD52, they are not depleted by anti-CD52. This is beneficial for preservation of capability for restoring the leukocyte population.15 As Campath-1 is the rat antibody, to increase its safety and to exclude possible reactions against rat-derived proteins and antibody clearance, humanized Campath-1 (Campath-1H), also known as alemtuzumab, was created.16 Campath-1H is an IgG1-class antibody, and like rat Campath-1, it binds to the C terminus of the CD52 antigen and partly to the glycosylphosphatidylinositol anchor. The mechanism of action of the anti-CD52 antibody is depletion of lymphocytes via two mechanisms: complement-dependent cytolysis (CDC) and antibody-dependent cellular cytotoxicity.14,17,18
Results of detailed analysis of specific cell subtypes susceptible to alemtuzumab have shown the highest CD52-antigen density on memory B cells and naïve CD4+ T cells from the lymphoid-cell subset and also on DCs from the myeloid-cell population. Subsequently, alemtuzumab mediated CDC was tested, and the results indicated the strongest cytolytic activity of alemtuzumab on the T- and B-cell subsets, but not myeloid DCs, probably due to higher expression of complement-inhibitory proteins in myeloid cells. This points to alemtuzumab efficacy being not only dependent on antigen density.4 However, research has shown that myeloid monocyte–derived DCs both highly express the CD52 antigen and are sensitive to CDC mediated by humanized anti-CD52, but in a maturity-dependent manner with less sensitivity in mature myeloid monocyte–derived DCs. This may be important, as DCs are antigen-presenting cells and clearance of such from the center of inflammatory reaction would inhibit antigen presentation and antigen-specific lymphocyte activation.19
Anti-CD52 Mechanism of Action in EAE and Multiple Sclerosis
Multiple sclerosis (MS) is an autoimmune disease mediated by autoreactive T cells recognizing myelin antigens in the central nervous system (CNS). Besides T cells, while immunoreaction is developed, B cells, which produce antibodies directed against myelin, and innate immunity mechanisms are involved. Immunoreaction causes demyelination, axon loss, and damage to whole neurons. Therefore, depleting cells responsible for antigen-specific reactions would be beneficial.20,21
Experimental autoimmune encephalomyelitis (EAE), the animal model of MS, provides more precise data on alemtuzumab’s mechanism of action, some of which are unobtainable from human studies. Depletion of T and B cells from the periphery is the main outcome of alemtuzumab, also observed in experimental animals. Despite peripheral depletion of T and B cells, in mice injected intraperitoneally with alemtuzumab, there is still a detectable amount of lymphocytes present in the spleen, thymus, and lymph nodes. On the periphery, the pool of neutrophiles and NK cells remains unaffected. Considering lymphocyte-repopulation differences are seen for B and T cells, less time is needed for B-cell repopulation (7–10 weeks), than T-cell repopulation (25 weeks). Partial depletion of thymocytes may contribute to prolonged T-cell reconstitution. Mechanisms engaged in cytokine release after alemtuzumab administration have also been analyzed. The effect of complement or NK-cell depletion was tested, and the results indicated that complement removal did not alter cytokine release, while NK depletion did. This indicates engagement of direct cellular mechanisms (eg, activation of innate immune cells by damaged lymphocytes) and not the complement-mediated mechanism for cytokine release.22
Animal studies have also supplied data on the effects of anti-CD52 therapy in the CNS. In mice with induced EAE, intravenous treatment with anti-CD52 at the peak of symptoms but not in the chronic phase diminished disease severity. T- and B-cell infiltration into the CNS was decreased after anti-CD52 treatment during both acute and chronic phases of EAE. B-cell aggregates in the CNS were depleted, probably due to the lack of supplementation of aggregates by B cells infiltrating from the periphery. In mice treated with anti-CD52, reduction in axon damage,23 reduction in demyelination in the CNS, and unaltered axonal conductance has been observed.24 Such observations have been further confirmed, and increased anti-inflammatory cytokines (IL10 and TGFβ) and BDNF expression and decreased proinflammatory cytokine expression (TNF, IFNγ, and IL17) was observed.25 As there is poor anti-CD52 penetration through the blood–brain barrier,26 intrathecal administration of antimurine CD52 to EAE mice was tested. No influence of intrathecal anti-CD52 on circulating immune cells was observed in healthy animals. In EAE mice, administration on the 10th but not 20th day after immunization reduced clinical symptoms of the disease and decreased the number of CD3+ T cells in mice spinal cord sections and the number of peripheral CD4+ and CD8+ T cells. Reduction in the number of peripheral CD4+ and CD8+ cells was however smaller than in mice where anti-CD52 was administered subcutaneusly.27 Despite high expression of CD52 mRNA in cultured microglia, neurons, and astrocytes, protein expression was strongest in neurons, weaker in microglia, and scant in astrocytes. Nevertheless, no microglia depletion under the influence of anti-CD52 was observed in tisssue sections. Anti-CD52–treated microglia presented morphology of an activated state, but probably not affecting functioning or interactions with cocultured lymphocytes. In neurons, anti-CD52 did not exert protective activity against excitotoxicity induced by NMDA and Th17 cells.28
After infusion of alemtuzumab in MS patients, depletion in circulating lymphocytes is observed. Also, within a few hours transient increases in TNFα, IFNγ, and IL6 levels due to antibody-mediated cytotoxicity and cell lysis, which induces inflammatory reactions, is noted.29–31 Repopulation of the lymphocyte pool occurs from the lymphocytes escaping depletion and from bone marrow and thymic progenitors.30 Patterns for T- and B-cell population recovery in patients is similar to experimental animals, with 3–6 months needed for B cells repopulation and up to 61 months for T cells reconstitution.32,33 Increased secretion of neurotrophic factors, such as BDNF and ciliary neurotrophic factor, by regenerating immune cells may exert a neuroprotective effect and provide some explanation for disability improvement in patients treated with alemtuzumab.34 Alemtuzumab decreases the level of NfL concentrations in plasma obtained from relapsing–remitting MS (RRMS) patients. As NfL is a markers of neuroaxonal damage, reflecting disease progress, this may also indicate the neuroprotective outcome of alemtuzumab.35 What is interesting is that CD4+CD25+ Treg cells repopulate within 3 months of alemtuzumab administration.36 In vitro studies on peripheral blood mononuclear cells isolated from patients have indicated that costimulation of CD4+ T cells with anti-CD3 and anti-CD52 induce CD4+CD25+ regulatory cells eventually suppressing CD4+ cells by direct cell-to-cell contact via T-cell receptors.7,37 Differential repopulation of T cells may contribute to prolonged suppression of MS. A combination of fast Treg repopulation and long-lasting depletion of Th17 and Th1 subsets creates an immunotolerant environment.38 Additionally, Breg cells also repopulate within short time after alemtuzumab administration.39 On the other hand, faster repopulation of T-memory cells from the pool escaping depletion, rather than naïve T cells, may contribute to secondary autoimmunity.40,41
Alemtuzumab binds also soluble CD52. This may interfere with the suppressor activity of soluble CD52 molecules, thus leading to possible limited efficacy of alemtuzumab as the immunosuppressive agent. On the other hand, this may be beneficial, as inhibiting immunosuppression prevents infections in patients.10 Figure 1 summarizes the effect of anti-CD52 on the immune system.
 |
Figure 1 Effects of anti-CD52 on immune system. Administration of anti-CD52 causes depletion of circulating CD52+ cells, which are T cells, B cells, and immature myeloid dendritic cells (DCs). Depletion is due to complement-dependent cytolysis (CDC) and antibody-dependent cellular cytotoxicity (ADCC). In the periphery, after CD52+-cell depletion, a transient increase in TNFα and IFNγ is observed. Repopulation of depleted cells occurs from the thymus and bone-marrow population of cells, taking in human 3–6 months for B cells and up to 61 months for T cells. Fast repopulation of regulatory T and B cells is observed, which creates an immunotolerant environment. After depletion in the periphery, CD52+-cell infiltration into the CNS is decreased. This further decreases cell aggregates in the CNS and increases levels of anti-inflammatory cytokines, and decreased levels of proinflammatory cytokines are observed. Increased levels of neurotrophic factors are also noted. Abbreviations: BDNF, brain-derived neurotrophic factor; CNTF, ciliary neurotrophic factor. |
Alemtuzumab in Clinical Trials on MS
The efficacy and safety of alemtuzumab were established in three double-blinded comparative trials in treatment-naïve patients (phase II CAMMS223, NCT00050778) and phase III (CARE MS I, NCT00530348) and patients who had inadequate response to prior treatment with IFNβ or glatiramer acetate (phase III CARE MS II/CAMMS324, NCT00548405).32,42,43 The phase II and III clinical trials showed that alemtuzumab was more efficient in reducing annualized relapse ratedisability scores, and magnetic resonance imaging (MRI) lesion burden in treatment-naïve, the same as prior-treated, RRMS patients comparing to subcutaneous IFNβ1a.Results from the phase III CARE MS II study showed that alemtuzumab can be used in patients with refractory RRMS to reduce the risk of sustained accumulation of disability when treatment with first-line drugs has failed.43 A 3-year extension study with a total of 5 years’ follow-up from CARE MS I enrollment showed durable alemtuzumab efficacy in the absence of continuous treatment, with 68.5% patients not receiving additional courses.44 Similar conclusions were drawn from CARE MS II 5-year follow-up, where 59.8% of patients did not receive alemtuzumab retreatment.45 The next study evaluated 6-year outcomes in patients who had relapsed between the first and second alemtuzumab courses. These patients were dubbed “early relapsers”. Outcomes in these patients improved if they completed the second alemtuzumab course. This observation supports the hypothesis that administering two-course treatment is more efficient.46
Subsequent extension studies confirmed alemtuzumab efficacy and safety (CAMMS03409 NCT00930553 and subsequent TOPAZ extension NCT02255656) over 12 years. Of the 108 patients who received alemtuzumab 12 mg/day in CAMMS223, 60 (56%) enrolled in the CAMMS03409 extension and were further followed-up in the TOPAZ study. At year 12, 54 (50%) patients remained on the study. During 12 years, 33% of patients received a total of two courses of alemtuzumab and 65% received additional as-needed courses: three (38%), four (15%), five (3%), six (7%), and seven (2%). In total, 73% of patients received no more than three treatment courses. Over 12 years, the annualized relapse rate was 0.09, 71% of alemtuzumab-treated patients had improved or stable Expanded Disability Status Scale scores, and the average score change from baseline to year 12 was +0.33. In year 12, 73% of patients were free of MRI disease activity. The main limitation of the study was the small sample in the 12-year cohort. In sum, 42 patients were lost due to noncompliance with the study drug, withdrawal, loss to follow-up, physician decision, or unknown reasons. That might cause a selection bias in favor of patients with positively experiences of alemtuzumab, as patient participation in the extension study was voluntary.47 Nevertheless, the study confirmed the efficacy and safety of alemtuzumab on long-term follow-up.
Use of Alemtuzumab in MS
The drug was registered by the European Medicines Agency (EMA) in 2013 for adult MS patients with RRMS defined by clinical and imaging features. In 2014, it was also approved by the US Food and Drug Administration (FDA). It is indicated as a single disease-modifying therapy (DMT) in adult patients with highly active RRMS despite a full and adequate course of treatment with at least one DMT or patients with rapidly evolving severe RRMS, multiple sclerosis defined as two or more disabling relapses in one year and one or more gadolinium-enhancing lesions on brain MRI or a significant increase in T2 lesion load compared to a recent MRI.48
The recommended dose of alemtuzumab is 12 mg/day administered by intravenous infusion for two initial treatment courses, with up to two additional treatment courses if needed. The first regular treatment consists of 12 mg alemtuzumab per day for 5 consecutive days (in total 60 mg), and the second treatment consists of 12 mg per day on 3 consecutive days (in total 36 mg) administered 12 months after the first treatment course. If needed, up to two additional treatment courses may be considered, each of 12 mg per day on 3 consecutive days (in total an additional 36 mg) administered at least 12 months after the prior treatment course.48
Safety of Alemtuzumab
The main adverse effects (AEs) of alemtuzumab are associated with drug infusion, due to cytokine release and cytotoxic effect of antibodies leading to a brief exacerbation of disease symptoms, fever, nausea, and headache etc, associated with lymphocyte depletion leading to immunosuppression, which contributes to increased vulnerability of patients to infections (but preserved innate immunity decreases the severity of such event, secondary autoimmunity, which may be the effect of excessive B cells repopulation, and cancer.30,32
The most common AEs of alemtuzumab are infusion-associated reactions and infections, which occur at the highest rate after the first treatment course and decline thereafter.49 Alemtuzumab is also known to increase the risk of autoimmune events, such as thyroid disease and immunthrombocytopenia, nephropathies that may manifest months to years after treatment.50 The findings of the clinical trials led to requirements for extensive safety monitoring, allowing for early recognition and management of AEs during alemtuzumab therapy.51 However, in April 2019 the EMA initiated a review of alemtuzumab, as AEs had been reported, including immunomediated (autoimmune hepatitis, hemophagocytic lymphohistiocytosis) and new cardiovascular (lung bleeding, myocardial infarctions, ischemic and hemorrhagic strokes, and cardiocephalic arterial dissections) ones. During the review alemtuzumab was restricted to patients with active RRMS despite a full and adequate course of treatment with at least two other DMTs or to patients with contraindications to all other DMTs.52
The EMA Safety Committee recommended that alemtuzumab should no longer be used in in patients with certain heart, circulation, or bleeding disorders or those who have autoimmune disorders other than MS. Later, in October 2019 the restriction was loosened and alemtuzumab was allowed to be used when at least one other DMT was ineffective or contraindicated.53 Decisions on these restriction changes were made by European Commission on January 16, 2020.54 Due to the deep and long-lasting immunosuppression, patients on alemtuzumab may experience opportunistic infections. High risk of infections is expected within the first 6 months after dosing, with the peak during the first month of treatment and later diminishing. In clinical trials, the most commonly reported infections were those of the upper and lower respiratory tract, urinary tract, masticatory muscles, and gastrointestinal tract.55 History of infectious diseases and vaccination status should always be taken into account before alemtuzumab treatment.
COVID-19 and MS Patients Treated with Alemtuzumab
In the era of COVID-19, there is still little known about the effects of immunosuppression in various autoimmune diseases on the SARS-CoV2–infection course. From the beginning of the pandemic, different hypothesis were made, starting from these that patients under immunosuppression might be more susceptible to COVID-19 complications to those that such therapy may be protective against overly active immunoresponse.56,57 It is still not known whether patients with MS are at increased risk of developing severe forms of COVID-19. Generally, lymphopenia and immunosuppression are associated with worse outcomes.58 It might be suspected that immunosuppressive drugs used in MS lead to more severe courses of infection, but this is still not clear or clinically supported.
Alemtuzumab-treated patients are at higher risk of such infections as nasopharyngitis, urinary tract infections, herpetic infections, influenza, and bronchitis, including serious infections.48 It might be suspected that alemtuzumab can also reduce both humoral and cellular response against SARS-CoV2; however, it is speculated to vary according to the phase of immunoreconstitution. Patients who return to normal or near-normal lymphocyte counts are possibly not at increased risk of SARS-CoV2 infection.59 In patients who have received one cycle of alemtuzumab, delaying the second cycle or switching to safer DMT should be considered. It is suggested that redosing alemtuzumab during a pandemic in high-risk areas may be unsafe, as the risk of infection is highest when dose initiation occurs during maximum lymphopenia. There is also a link between alemtuzumab and cardiocephalic arteria dissection and stroke.60 As during COVID-19, there is a risk of thrombosis and intracerebral hemorrhage, and redosing alemtuzumab during infection or within a short period may increase that risk.61
The Association of British Neurologists suggests delaying starting or redosing of alemtuzumab in patients with MS during the COVID-19 pandemic; however, patient condition and individual factors, such as highly active disease, should be taken into account before the final decision to postpone therapy or choose another DMT.62 At the time of writing, there were five published case reports on seven MS patients treated with alemtuzumab who had developed COVID-19.63–67 Three of seven needed hospitalization, but all of them fully recovered without any serious complications (Table 1). It might be speculated that immunosuppression is favorable in such patients; however, the question about the time frame between dosing and infection and the efficacy of vaccination against COVID-19 is open.
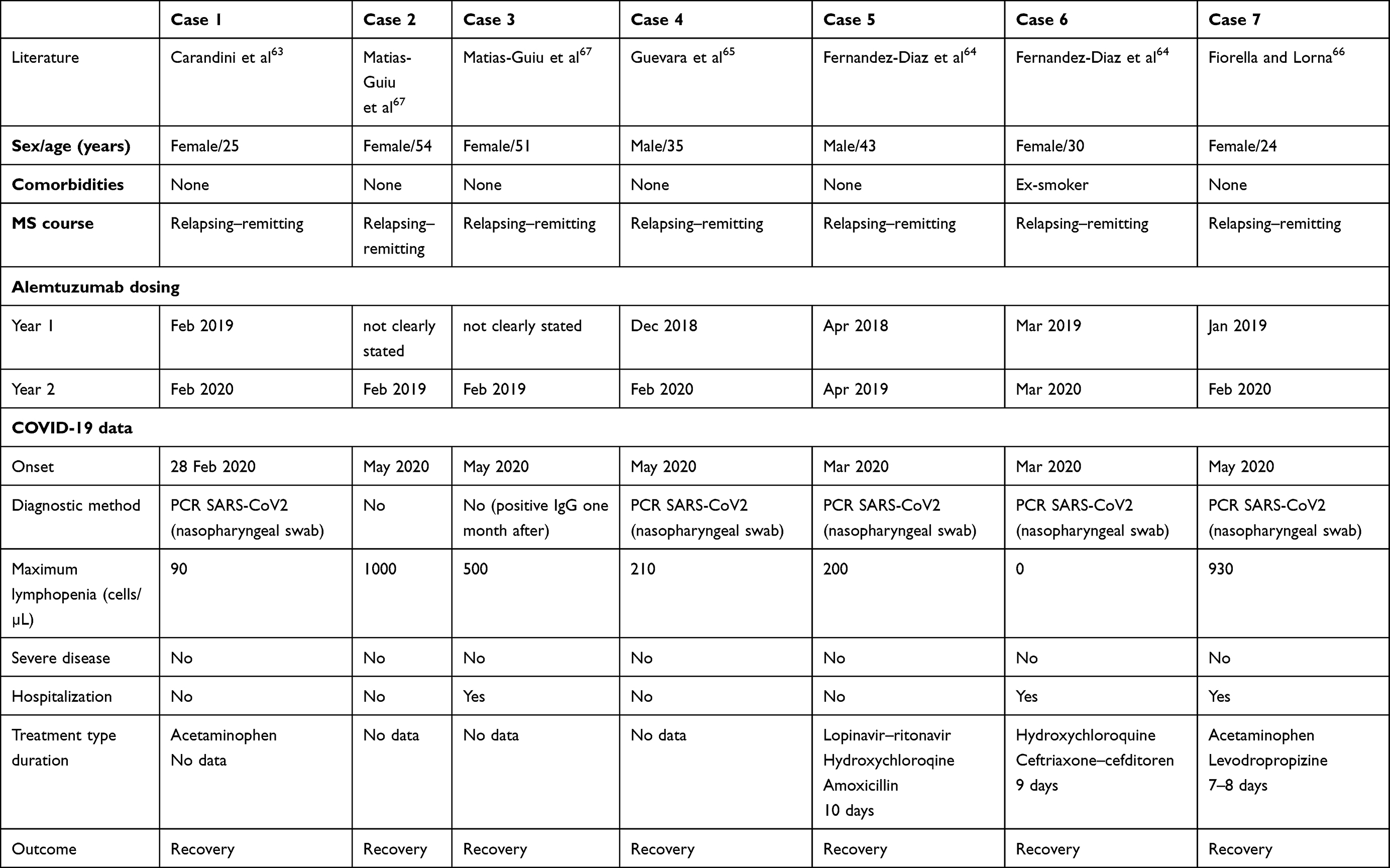 |
Table 1 Alemtuzumab treated MS patients with COVID-19 described in the literature |
One explanation for mild MS course in alemtuzumab-treated patients might be that following initial depletion, the drug produces lymphocyte reconstitution from a new lineage. This includes changes in composition, phenotype, and lymphocyte function, and leads to possible resistance of this new lineage to the virus or blunts the cytokine storm responsible for life-threating complications of SARS-COV2.67 Parotta et al found that in MS patients, risk factors of severe COVID-19 course or related death were older age, comorbidities, progressive form of MS, and nonambulatory status. Until now, no DMT, including alemtuzumab, has been noted as a factor in worsening COIVID-19.68
Alemtuzumab and Vaccination
Vaccination guidelines provide indications for timing of inactivated vaccines prior to disease DMT, but not after it.69 The same concerns live attenuated vaccines in a majority of drugs used for DMT. It is recommended that patients treated with immunosuppressive drugs do not receive these kind of vaccines immediately before (ie, 4–6 weeks), during,or for a certain time after treatment; however, in the case of alemtuzumab, this has not been clearly defined.69 A recent Delphi consensus statement shares that opinion, and recommends that in cases of inactivated vaccines (either first or recall dose), alemtuzumab should be administered at least 1 month before and 6 months after treatment.70 This is in line with data from Ciotti et al.71 In the alemtuzumab summary of product characteristics (SPCs), it is recommended that patients have completed local immunization requirements at least 6 weeks prior to treatment.54 The ability to generate an immunoresponse to any vaccine following alemtuzumab has not been studied. The safety of immunization with live viral vaccines following a course of alemtuzumab treatment has not been formally studied in controlled clinical trials on MS, and the drug should not be administered to MS patients who have received it.48
When different types of vaccination are taken into account, still little is known. Considering the anti–SARS-CoV2 vaccination SmPCs do not contain any information about mRNA vaccines in patients treated with alemtuzumab. A literature search does not reveal any publications on the use of alemtuzumab in combination with any mRNA vaccine in patients. Alemtuzumab has not been studied with any registered vaccine, eg, mRNA vaccine (nucleoside-modified, Pfizer/BionTech, Moderna),-ChAdOx1-S (recombinant, Astra Zeneca), or Ad26.COV2-S recombinant, Janssen-Cilag International). In all SmPCs, there is information that though no formal studies have been performed in immunocompromised patients, including those receiving immunosuppressants, diminished immunoresponse might be expected.72–75
In the literature, there is scarce information about vaccination in patients treated with alemtuzumab. Rolla et al41 found that despite induced B lymphopenia, alemtuzumab appeared to have no effect on immunoresponses to vaccines. RRMS patients treated with that drug maintained humoral immunomemory and an ability to develop an immunoresponse against such vaccines antidiphteria, antitetanus, antipoliomyelitis, type B anti–Haemophilus influenzae, anti meningococcus C and antipneumococcal polysaccharide.41 On the other hand, Zheng et al59 found that alemtuzumab had an effect on both T and B cells and an innate immunoresponse. These may affect early and long-term immunity against SARS-CoV2 increasing infection susceptibility and reinfection rates. Alemtuzumab may reduce humoral and cellular response against SARS-CoV2 viral infection and inactivated vaccine, especially when given in the time frame of cell depletion.59 As of May 2021, there were no published case reports describing the use of live vaccines in alemtuzumab-treated patients in terms of safety and efficacy. Decisions should be always made by treating physician after risk–benefit analysis.
Conclusion
Data from preclinical and clinical studies provide enough rationale for using alemtuzumab as a highly efficient drug in MS. Due to deep immunosuppression, some doubts on acceptable drug safety have appeared. Markers for not only treatment response but also risk stratifications are urgently needed. COVID brings another challenge, which is determination of COVID-19 course in patients on highly efficient immunosuppression, as well as the efficacy and safety of anti–SARS-CoV2 vaccination in such patients. Further studies are expected to determine the risk of COVID in individuals with autoimmune diseases and those on immunosuppression, including alemtuzumab-treated MS patients.
Disclosure
Dagmara Mirowska-Guzel reports personal fees from Sanofi Genzyme during the conduct of the study, personal fees from Roche Polska outside the submitted work, and grants and personal fees for serving on advisory boards organized by Roche, Sanofi Genzyme, and Teva. The authors report no other potential conflicts of interest for this work.
References
1. Domagała A, Kurpisz M. Cd52 antigen - A review. Med Sci Monit. 2001;7(2):325–331.
2. Treumann A, Lifely MR, Schneider P, Ferguson MA. Primary structure of CD52. J Biol Chem. 1995;270(11):6088–99. doi:10.1074/jbc.270.11.6088.
3. Zhao Y, Su H, Shen X, Du J, Zhang X, Zhao Y. The immunological function of CD52 and its targeting in organ transplantation. Inflamm Res. 2017;66(7):571–578. doi:10.1007/s00011-017-1032-8
4. Rao SP, Sancho J, Campos-Rivera J, et al. Human peripheral blood mononuclear cells exhibit heterogeneous CD52 expression levels and show differential sensitivity to alemtuzumab mediated cytolysis. PLoS One. 2012;7(6):1–12. doi:10.1371/journal.pone.0039416
5. Ambrose LR, Morel AS, Warrens AN. Neutrophils express CD52 and exhibit complement-mediated lysis in the presence of alemtuzumab. Blood. 2009;114(14):3052–3055. doi:10.1182/blood-2009-02-203075
6. Masuyama J, Yoshio T, Suzuki K, et al. Characterization of the 4C8 antigen involved in transendothelial migration of CD26hi T cells after tight adhesion to human umbilical vein endothelial cell monolayers. J Exp Med. 1999;189(6):979–990. doi:10.1084/jem.189.6.979
7. Watanabe T, Masuyama J, Sohma Y, et al. CD52 is a novel costimulatory molecule for induction of CD4+ regulatory T cells. Clin Immunol. 2006. doi:10.1016/j.clim.2006.05.006
8. Rowan WC, Hale G, Tite JP, Brett SJ. Cross-linking of the CAMPATH-1 antigen (CD52) triggers activation of normal human T lymphocytes. Int Immunol. 1995. doi:10.1093/intimm/7.1.69
9. Shathili AM, Bandala-Sanchez E, John A, et al. Specific sialoforms required for the immune suppressive activity of human soluble CD52. Front Immunol. 2019;10(AUG):1–13. doi:10.3389/fimmu.2019.01967
10. Bandala-Sanchez E, Zhang Y, Reinwald S, et al. T cell regulation mediated by interaction of soluble CD52 with the inhibitory receptor Siglec-10. Nat Immunol. 2013;14(7):741–748. doi:10.1038/ni.2610
11. Bandala-Sanchez E, Bediaga NG, Goddard-Borger ED, et al. CD52 glycan binds the proinflammatory B box of HMGB1 to engage the Siglec-10 receptor and suppress human T cell function. Proc Natl Acad Sci U S A. 2018;115(30):7783–7788. doi:10.1073/pnas.1722056115
12. Toh BH, Kyaw T, Tipping P, Bobik A. Immune regulation by CD52-expressing CD4 T cells. Cell Mol Immunol. 2013;10(5):379–382. doi:10.1038/cmi.2013.35
13. Rashidi M, Bandala-Sanchez E, Lawlor KE, et al. CD52 inhibits toll-like receptor activation of NF-κB and triggers apoptosis to suppress inflammation. Cell Death Differ. 2018;25(2):392–405. doi:10.1038/cdd.2017.173
14. Tati K, Yazdanpanah-Samani M, Ramezani A, Mahmoudi Maymand E, Ghaderi A. Establishment a CHO cell line expressing human CD52 molecule. Rep Biochem Mol Biol. 2016;5(1):56–61.
15. Hale G, Bright S, Chumbley G, et al. Removal of T cells from bone marrow for transplantation: a monoclonal antilymphocyte antibody that fixes human complement. Blood. 1983;62(4):873–882. doi:10.1182/blood.v62.4.873.873
16. Riechmann L, Clark M, Waldmann H, Winter G. Reshaping human antibodies for therapy. Nature. 1988;332(6162):323–327. doi:10.1038/332323a0
17. Hale G. The CD52 antigen and development of the CAMPATH antibodies. Cytotherapy. 2001. doi:10.1080/146532401753174098
18. Lowenstein H, Shah A, Chant A, Khan A. Different mechanisms of campath-1H-mediated depletion for CD4+ and CD8+ T cells in peripheral blood. Transpl Int. 2006. doi:10.1111/j.1432-2277.2006.00382.x
19. Ratzinger G, Reagan JL, Heller G, Busam KJ, Young JW. Differential CD52 expression by distinct myeloid dendritic cell subsets: implications for alemtuzumab activity at the level of antigen presentation in allogeneic graft-host interactions in transplantation. Blood. 2003;101(4):1422–1429. doi:10.1182/blood-2002-04-1093
20. Sospedra M, Martin R. Immunology of multiple sclerosis. Annu Rev Immunol. 2005;23:683–747. doi:10.1146/annurev.immunol.23.021704.115707
21. Sospedra M, Martin R. Immunology of multiple sclerosis. Semin Neurol. 2016;36(2):115–127. doi:10.1055/s-0036-1579739
22. Hu Y, Turner MJ, Shields J, et al. Investigation of the mechanism of action of alemtuzumab in a human CD52 transgenic mouse model. Immunology. 2009. doi:10.1111/j.1365-2567.2009.03115.x
23. Simon M, Ipek R, Homola GA, et al. Anti-CD52 antibody treatment depletes B cell aggregates in the central nervous system in a mouse model of multiple sclerosis. J Neuroinflammation. 2018;15(1):1–15. doi:10.1186/s12974-018-1263-9
24. Turner MJ, Pang PT, Chretien N, et al. Reduction of inflammation and preservation of neurological function by anti-CD52 therapy in murine experimental autoimmune encephalomyelitis. J Neuroimmunol. 2015;285:4–12. doi:10.1016/j.jneuroim.2015.05.018
25. Pant AB, Wang Y, Mielcarz DW, et al. Alteration of CD39+Foxp3+ CD4 T cell and cytokine levels in EAE/MS following anti-CD52 treatment. J Neuroimmunol. 2017;303:22–30. doi:10.1016/j.jneuroim.2016.12.010
26. Avasarala J. It’s time for combination therapies in multiple sclerosis. Innov Clin Neurosci. 2017.
27. Bogie JFJ, Grajchen E, Wouters E, et al. CNS delivery of anti-CD52 antibodies modestly reduces disease severity in an animal model for multiple sclerosis. Ther Adv Chronic Dis. 2020. doi:10.1177/2040622320947378
28. Ellwardt E, Vogelaar CF, Maldet C, Schmaul S, Bittner S, Luchtman D. Targeting CD52 does not affect murine neuron and microglia function. Eur J Pharmacol. 2020;871(October 2019):172923. doi:10.1016/j.ejphar.2020.172923
29. Moreau T, Coles A, Wing M, et al. CAMPATH-IH in multiple sclerosis. Mult Scler. 1996. doi:10.1177/135245859600100616
30. Evana JR, Bozkurta SB, Thomasa NC, Bagnatoa F. Alemtuzumab for the treatment of multiple sclerosis. Expert Opin Biol Ther. 2018. doi:10.1080/14712598.2018.1425388
31. Thomas K, Eisele J, Rodriguez-Leal FA, Hainke U, Ziemssen T. Acute effects of alemtuzumab infusion in patients with active relapsing-remitting MS. Neurol Neuroimmunol NeuroInflammation. 2016. doi:10.1212/NXI.0000000000000228
32. Coles AJ, Compston DA, Selmaj KW, et al.Alemtuzumab vs. interferon beta-1a in early multiple sclerosis. N Engl J Med. 2008. doi:10.1056/nejmoa0802670
33. Coles AJ, Cox A, Le Page E, et al. The window of therapeutic opportunity in multiple sclerosis: evidence from monoclonal antibody therapy. J Neurol. 2006. doi:10.1007/s00415-005-0934-5
34. Jones JL, Anderson JM, Phuah CL, et al. Improvement in disability after alemtuzumab treatment of multiple sclerosis is associated with neuroprotective autoimmunity. Brain. 2010. doi:10.1093/brain/awq176
35. Delcoigne B, Manouchehrinia A, Barro C, et al. Blood neurofilament light levels segregate treatment effects in multiple sclerosis. Neurology. 2020. doi:10.1212/WNL.0000000000009097
36. Cox AL, Thompson SAJ, Jones JL, et al. Lymphocyte homeostasis following therapeutic lymphocyte depletion in multiple sclerosis. Eur J Immunol. 2005. doi:10.1002/eji.200535075
37. Masuyama J, Kaga S, Kano S, Minota S. A novel costimulation pathway via the 4C8 antigen for the induction of CD4 + regulatory T cells. J Immunol. 2002. doi:10.4049/jimmunol.169.7.3710
38. Zhang X, Tao Y, Chopra M, et al. Differential reconstitution of T cell subsets following immunodepleting treatment with alemtuzumab (anti-CD52 monoclonal antibody) in patients with relapsing–remitting multiple sclerosis. J Immunol. 2013. doi:10.4049/jimmunol.1301926
39. Kim Y, Kim G, Shin HJ, et al. Restoration of regulatory B cell deficiency following alemtuzumab therapy in patients with relapsing multiple sclerosis. J Neuroinflammation. 2018. doi:10.1186/s12974-018-1334-y
40. Baker D, Herrod SS, Alvarez-Gonzalez C, Giovannoni G, Schmierer K. Interpreting lymphocyte reconstitution data from the pivotal Phase 3 trials of alemtuzumab. JAMA Neurol. 2017. doi:10.1001/jamaneurol.2017.0676
41. Rolla S, Maglione A, De Mercanti SF, Clerico M. The meaning of immune reconstitution after alemtuzumab therapy in multiple sclerosis. Cells. 2020. doi:10.3390/cells9061396
42. Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial. Lancet. 2012. doi:10.1016/S0140-6736(12)61769-3
43. Coles AJ, Twyman CL, Arnold DL, et al. Alemtuzumab for patients with relapsing multiple sclerosis after disease-modifying therapy: a randomised controlled phase 3 trial. Lancet. 2012. doi:10.1016/S0140-6736(12)61768-1
44. Havrdova E, Arnold DL, Cohen JA, et al. Alemtuzumab CARE-MS I 5-year follow-up. Neurology. 2017. doi:10.1212/wnl.0000000000004313
45. Coles AJ, Cohen JA, Fox EJ, et al. Alemtuzumab CARE-MS II 5-year follow-up: efficacy and safety findings. Neurology. 2017. doi:10.1212/WNL.0000000000004354
46. Van Wijmeersch B, Singer BA, Boster A, et al. Efficacy of alemtuzumab over 6 years in relapsing–remitting multiple sclerosis patients who relapsed between courses 1 and 2: post hoc analysis of the CARE-MS studies. Mult Scler J. 2020. doi:10.1177/1352458519881759
47. Steingo B, Al Malik Y, Bass AD, et al. Long-term efficacy and safety of alemtuzumab in patients with RRMS: 12-year follow-up of CAMMS223. J Neurol. 2020. doi:10.1007/s00415-020-09983-1
48. Michailidou A, Trenz H-J, de Wilde P. Annex I. Internet Eur Integr. 2019;167–172. doi:10.2307/j.ctvdf0dxq.12
49. Ziemssen T, Thomas K. Alemtuzumab in the long-term treatment of relapsing-remitting multiple sclerosis: an update on the clinical trial evidence and data from the real world. Ther Adv Neurol Disord. 2017. doi:10.1177/1756285617722706
50. Barclay K, Carruthers R, Traboulsee A, et al. Best practices for long-term monitoring and follow-up of alemtuzumab-treated MS patients in real-world clinical settings. Front Neurol. 2019. doi:10.3389/fneur.2019.00253
51. Bierhansl L, Ruck T, Pfeuffer S, Gross CC, Wiendl H, Meuth SG. Signatures of immune reprogramming in anti-CD52 therapy of MS: markers for risk stratification and treatment response. Neurol Res Pract. 2019. doi:10.1186/s42466-019-0045-x
52. Meeting highlights from the Pharmacovigilance Risk Assessment Committee (PRAC) 8–11 April 2019. European Medicines Agency. Availabvle from: https://www.ema.europa.eu/en/news/meeting-highlights-pharmacovigilance-risk-assessment-committee-prac-8-11-april-2019.
53. Meeting highlights from the Pharmacovigilance Risk Assessment Committee (PRAC) 28–31 October 2019. European Medicines Agency. Availabvle from: https://www.ema.europa.eu/en/news/meeting-highlights-pharmacovigilance-risk-assessment-committee-prac-28-31-october-2019.
54. CHMP. Lemtrada; INN: alemtuzumab. Availabvle from: www.ema.europa.eu/contact.
55. Buonomo AR, Zappulo E, Viceconte G, Scotto R, Borgia G, Gentile I. Risk of opportunistic infections in patients treated with alemtuzumab for multiple sclerosis. Expert Opin Drug Saf. 2018. doi:10.1080/14740338.2018.1483330
56. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020. doi:10.1016/S0140-6736(20)30628-0
57. Ritchie AI, Singanayagam A. Immunosuppression for hyperinflammation in COVID-19: a double-edged sword? Lancet. 2020. doi:10.1016/S0140-6736(20)30691-7
58. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a Retrospective Cohort Study. Lancet. 2020. doi:10.1016/S0140-6736(20)30566-3
59. Zheng C, Kar I, Chen CK, et al. Multiple sclerosis disease-modifying therapy and the COVID-19 pandemic: implications on the risk of infection and future vaccination. CNS Drugs. 2020. doi:10.1007/s40263-020-00756-y
60. FDA warns about rare but serious risks of stroke and blood vessel wall tears with multiple sclerosis drug Lemtrada (alemtuzumab). FDA. Availabvle from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-warns-about-rare-serious-risks-stroke-and-blood-vessel-wall-tears-multiple-sclerosis-drug.
61. Oxley TJ, Mocco J, Majidi S, et al. Large-vessel stroke as a presenting feature of Covid-19 in the young. N Engl J Med. 2020. doi:10.1056/nejmc2009787
62. Brownlee W, Bourdette D, Broadley S, Killestein J, Ciccarelli O. Treating multiple sclerosis and neuromyelitis optica spectrum disorder during the COVID-19 pandemic. Neurology. 2020. doi:10.1212/WNL.0000000000009507
63. Carandini T, Pietroboni AM, Sacchi L, et al. Alemtuzumab in multiple sclerosis during the COVID-19 pandemic: a mild uncomplicated infection despite intense immunosuppression. Mult Scler J. 2020. doi:10.1177/1352458520926459
64. Fernández-Díaz E, Gracia-Gil J, García-García JG, Palao M, Romero-Sánchez CM, Segura T. COVID-19 and multiple sclerosis: a description of two cases on alemtuzumab. Mult Scler Relat Disord. 2020. doi:10.1016/j.msard.2020.102402
65. Guevara C, Villa E, Cifuentes M, Naves R, Grazia J. Mild COVID-19 infection in a patient with multiple sclerosis and severe depletion of T-lymphocyte subsets due to alemtuzumab. Mult Scler Relat Disord. 2020. doi:10.1016/j.msard.2020.102314
66. Matías-Guiu J, Montero-Escribano P, Pytel V, Porta-Etessam J, Matias-Guiu JA. Potential COVID-19 infection in patients with severe multiple sclerosis treated with alemtuzumab. Mult Scler Relat Disord. 2020. doi:10.1016/j.msard.2020.102297
67. Fiorella C, Lorna G. COVID-19 in a multiple sclerosis (MS) patient treated with alemtuzumab: insight to the immune response after COVID. Mult Scler Relat Disord. 2020;46:102447. doi:10.1016/j.msard.2020.102447
68. Parrotta E, Kister I, Charvet L, et al. COVID-19 outcomes in MS: observational study of early experience from NYU multiple sclerosis comprehensive care center. Neurol Neuroimmunol Neuroinflamm. 2020. doi:10.1212/NXI.0000000000000835
69. Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2014. doi:10.1093/cid/cit684
70. Riva A, Barcella V, Benatti SV, et al. Vaccinations in patients with multiple sclerosis: a Delphi consensus statement. Mult Scler J. 2020. doi:10.1177/1352458520952310
71. Ciotti JR, Valtcheva MV, Cross AH. Effects of MS disease-modifying therapies on responses to vaccinations: a review. Mult Scler Relat Disord. 2020. doi:10.1016/j.msard.2020.102439
72. European Medicines Agency. Annex I; Summary of Product Characteristics: Comirnaty concentrate for dispersion for injection; COVID-19 mRNA Vaccine (nucleoside modified); 2020. Available from: https://ec.europa.eu/health/documents/community-register/2020/20201221150522/anx_150522_en.pdf. Accessed June 29, 2021.
73. European Medicines Agency. Annex I; Summary of Product Characteristics: COVID-19 Vaccine Moderna dispersion for injection; COVID-19 mRNA Vaccine (nucleoside modified); 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-moderna-epar-product-information_en.pdf. Access June 29, 2021.
74. European Medicines Agency. Annex I; Summary of Product Characteristics: COVID-19 Vaccine AstraZeneca suspension for injection; COVID-19 Vaccine (ChAdOx1-S [recombinant]); 2021. Available from: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-astrazeneca-product-information-approved-chmp-29-january-2021-pending-endorsement_en.pdf. Accessed June 29, 2021.
75. European Medicines Agency. Annex I; Summary of Product Characteristics: COVID-19 Vaccine Janssen suspension for injection; COVID-19 vaccine (Ad26.COV2-S [recombinant]); 2021. Available from: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-janssen-epar-product-information_en.pdf. Accessed June 29, 2021.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.