")
Back to Journals » Journal of Pain Research » Volume 16
Analysis of the Risk Factors for Mechanical Allodynia in Herpetic Neuralgia: A Retrospective Cross-Sectional Study
Authors Xu G , Gong W, Dong S, Hu G, Tang W, Yu H
Received 24 April 2023
Accepted for publication 18 September 2023
Published 2 October 2023 Volume 2023:16 Pages 3309—3318
DOI https://doi.org/10.2147/JPR.S417454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Gang Xu,1,2 Weiwei Gong,2,3 Shihong Dong,2 Guojiong Hu,2,4 Weizhen Tang,1 Hecheng Yu1
1Department of Rehabilitation Medicine, Affiliated Tenth People’s Hospital of Tongji University, Shanghai Tenth People’s Hospital, Shanghai, 200072, People’s Republic of China; 2Department of Rehabilitation Medicine, Tongji University School of Medicine, Shanghai, 200092, People’s Republic of China; 3Department of Rehabilitation Medicine, Shanghai First Rehabilitation Hospital, Shanghai, 200090, People’s Republic of China; 4Department of Rehabilitation Medicine, Affiliated Yangzhi Rehabilitation Hospital of Tongji University, Shanghai, 201619, People’s Republic of China
Correspondence: Gang Xu, Department of Rehabilitation Medicine, Affiliated Tenth People’s Hospital of Tongji University, Shanghai Tenth People’s Hospital, Shanghai, 200072, People’s Republic of China, Tel +86 21-66306496, Fax +86 21-66301051, Email [email protected]
Purpose: Mechanical allodynia is reportedly common during herpetic neuralgia. The purpose of this study was to establish a risk prediction model to predict the individual risk of allodynia in herpetic neuralgia.
Methods: Three hundred and eighty-six patients with trunk herpetic neuralgia were divided into two regions, T2-5 and T6-11. The causality between allodynia and other factors was analyzed by a binary logistic regression model.
Results: 42.2% of subjects had allodynia, 137 suffered from dynamic allodynia, and 110 with dynamic allodynia experienced local sweating. The following 5 items as predictors determined this model: local sweating (Odd Ratio = 27.57, P< 0.001), lesion location (Odd Ratio=2.46, P =0.017), pain intensity (Odd Ratio=1.38, P =0.020), pain duration (Odd Ratio=0.94, P =0.006), and local scars (Odd Ratio=0.07, P< 0.001). The presence and development of allodynia are associated with local sweating. The positive proportion of the Iodine-starch test between the T2-5 (50.0%) with the T6-11 (23.7%) had a statistically significant difference (χ2=5.36, P=0.021). 29.5% of patients at the T2-6 had obvious sweating, which was different from only sticky feelings at the T6-11 (70.5%, χ2=10.88, P=0.001). 19.2% of patients with residual scars and allodynia was significantly lower than 48.5% of patients without allodynia (χ2=15.28, P< 0.001).
Conclusion: This analysis suggests that local sweating is a concomitant symptom in dynamic allodynia, which imply the sympathetic nerves innervating the sweat glands of the skin were also involved during herpetic neuralgia. This may assist in the evaluation of dynamic allodynia and prove the role of sympathetic nerve intervention for herpetic neuralgia.
Keywords: herpetic neuralgia, mechanical dynamic allodynia, sweating, sympathetic nerves, peripheral sensitization
Introduction
Varicella zoster virus (VZV) is a neurotropic alpha-herpesvirus. After the primary infection (varicella), it enters a latent state in sensory, sympathetic, and parasympathetic neurons.1,2 Reactivation of VZV results in the spread of the infection to the epidermis, causing herpes zoster (HZ). HZ is often accompanied by pain, which is referred to as zoster-associated pain (ZAP) or postherpetic neuralgia (PHN). ZAP can be classified into three categories:3 (1) ongoing spontaneous burning pain; (2) brief recurrent shooting or electric shock-like pain;4 and (3) sharp, radiating pain of burning character evoked by light touch and other innocuous stimuli, known as mechanical allodynia (MA) or noxious stimuli (dynamic mechanical hyperalgesia).5,6 The first and second types of ZAP often cause extreme tenderness to touch and are worsened by tactile allodynia.7–9 According to quantitative sensory testing, approximately 27% of patients with PHN have preserved sensory functions but experience thermal hyperalgesia and mild MA. Another 25% of patients have lost both small and large fiber function, while 48% have lost small fiber function along with pinprick hyperalgesia, marked dynamic MA, and deep somatic allodynia.10 However, not all patients with PHN can be easily categorized into a specific category.11 In humans, both dynamic and static MA can be found in the affected dermatome of patients with acute HZ and PHN.12,13 Static MA is caused by light static pressure on the skin, while dynamic MA is caused by gentle stroking of the skin with a soft brush.14 In nearly 90% of cases, MA affects the affected and adjacent dermatomes.15,16 Dynamic MA is a prevalent symptom observed in both HZ and PHN. It can be so severe that it considerably decreases the patient’s quality of life.
MA is associated with both peripheral and central sensitization.16–20 Different subtypes of allodynia and hyperalgesia have separate mechanisms contributing to these reactions.19 In a large group of patients with PHN, various patterns of sensory dysfunction were detected, indicating heterogeneity.12 In individuals with neuropathic pain, static MA is believed to be mediated by unmyelinated primary afferents, while dynamic MA is mediated by myelinated primary afferents.14,21,22 These two types of MA represent distinct pathophysiological mechanisms.23 This implies that local MA may be accompanied by other symptoms. However, there is limited research on whether the development of MA around the lesion has other accompanying symptoms. Further investigation of the relationship between MA and local symptoms can improve our understanding of the underlying mechanisms and guide clinical therapeutic approaches. This cross-sectional analysis evaluated the relationship between MA and the various manifestations of locally involved tissues of herpetic neuralgia (HN) to gain a better understanding of the mechanisms related to VZV-induced peripheral sensitization.
Methods
Study Design
We conducted a cross-sectional study at the Zoster-associated Pain Research Center, Affiliated Tenth People’s Hospital of Tongji University.
The study protocol was reviewed and approved by the Affiliated Tenth People’s Hospital of Tongji University institutional review board (SHSY-IEC-KY-4.0/17-24). All procedures involving human participants were performed by the ethical standards of the institutional and national research committee and the 1964 Helsinki Declaration, its later amendments, or comparable ethical standards.
Inclusion Criteria
The study recruited patients diagnosed based on the European consensus-based (S2k) Guideline.24 Acute herpetic neuralgia (AHN) is defined as the intense pain in the affected nerve during acute zoster infection within 30 days, while subacute herpetic neuralgia (SHN) is defined as pain that persists 30 days or more after rash onset.25,26
Exclusion Criteria
Subjects who met the following criteria were excluded from this study: presentation or history of a serious or unstable medical or psychological condition that would compromise participation in the study, or confound the assessment of HN.
Patient Recruitment
Before study enrollment, the patients underwent a clinical examination and were assigned to complete baseline questionnaires.
Eligibility criteria included the following: a diagnosis of HN for at least half a month and no more than 24 months, 50–75 years of age, cutaneous and/or subcutaneous pain and/or other discomforts at the dermatomal T2 to T11 levels; or adjacent cutaneous dermatomes temporally and spatially associated with the HZ rash, and a pain score ≥ 4 on the 11-point NRS in the past 24 h, and pain area greater than or equal to one-third of the palm area of oneself.
Study Procedure
This cross-sectional study was conducted on 423 patients with trunk HN recruited between 2018 and 2022. To avoid the impact of high summer temperatures on body sweating, only patients from November of each year to April of the next year were investigated. Participants were provided a written explanation and their written consent was obtained.
Measurements
All patients underwent a structured interview to assess the clinical and phenomenological characteristics of their pain sensations, such as location, scope descriptive characteristics, intensity using the Zoster Brief Pain Inventory (ZBPI),27 and changes in the skin, local sticky feeling, or local sweating at the affected region.
The first item of the ZBPI describing the pain at its worst in the last 24 h was evaluated from 0 (no pain) to 10 (worst pain imaginable). Zoster-related pain is generally described as continuous pain (burning, tightness, pressure), and/or paroxysmal pain (tingling, stabbing pain),4 and/or MA,5 and/or paresthesia (itching, numbness).26 This study focused on patients’ MA and distinguished it from other types of pain. Because the pain associated with HZ was located in the partial regions innervated by distal nerve branches instead of the entire nerve distribution,26 one unit of the pain scope in this study was defined as the whole palm area of the patient-self`s right hand. Subjects` perceived pain regions were mapped in a sagittal fashion from lateral to midline, and then their proportion of a unit was calculated.
The sticky is a feeling and sweating is a symptom in this study. To determine whether there is a local sticky feeling or sweating, patients were asked, “Do you have excessive localized sweating on the pain area for more than 1 week (yes or no) without any apparent cause?” The answer options were “No feeling”, “Local sticky feelings”, “Wipe it frequently”, and “Place napkins locally” (coded as 0, 1, 2, and 3, respectively). Those who answered “yes” to the question were further asked what kind of pain is there in the sweating area, and what is the range of sweating.
Cotton Swab Test
Mark the sticky feeling or sweating area and compare it with the pain range to see if it overlaps. Then the cotton on the head of the cotton swab 1–2cm was stretched and used the cotton tip lightly cutaneous brushed the target region. Subjects were asked to close their eyes and indicate the points at which they felt a pain in sensation. The investigator observed the local skin contraction.
Iodine-Starch Test
To identify the focal sweating areas, we administered the iodine-starch test by standard dermatologic practice,28 the 2% iodine was painted on the affected region, allowed to dry, then covered with cornstarch via a standard makeup applicator brush. The patient was supine for 20 minutes to observe sweating.
All the tests were performed in a quiet, air-conditioned room at 24–26 °C.
Data Analysis
The sample size was established at 386 HN based on the following assumptions: the prevalence of dynamic MA among PHN patients would be 38.5%, and 6.7% among control sites,29 with an alpha error of 0.05, and statistical power of 80%. The sample size estimation was calculated website http://powerandsamplesize.com.
We analyzed the participants’ sociodemographic and clinical characteristics and summarized the data using frequency counts, and descriptive statistics (mean, and standard deviation). Categorical variables were analyzed by the chi-square test, and continuous variables were expressed as mean ± SD with an independent-sample t-test.
The Chi-squared test was performed on the ordinal variables through the cross-classified tables, and the Goodman-Kruskal`s gamma coefficient and Somers`D were calculated to determine the correlation between MA and sticky or sweating. Binary logistic regression analyses were performed to identify multivariate predictors of MA. Standardized beta coefficients were reported for each predictor variable included in the final reduced models for direct comparisons between the predictor variables in the regression model and the criterion variable being studied. The odds ratio (OR) was calculated, and P < 0.05 was considered to indicate statistical significance. We performed the data analysis using the Statistics Package for Social Science (SPSS 22.00, IBM Inc., USA).
Results
Patient Characteristics
After excluding 37 individuals, the study period consisted of 386 individuals aged ≥50 years included in the analysis (Table 1 and Figure 1). During the study period, 46 individuals were diagnosed with AHN, 64 were SHN, and 276 were PHN. More than half (51.6%) were female, and the mean age was 63.8 ± 6.8 y. The average course of the disease was 10.6±7.3 m. The average pain score was 5.9±1.1. Of the 386 patients, 98 were affected at T2-5 and 288 at T6-11. No significant difference between the left and right sides. 42.2% of patients (163/386) showed local MA, and 131 (39.6%, 16 in the SHN, and 115 in the PHN) patients felt local sticky or had local sweating. 148 patients were left with local scars.
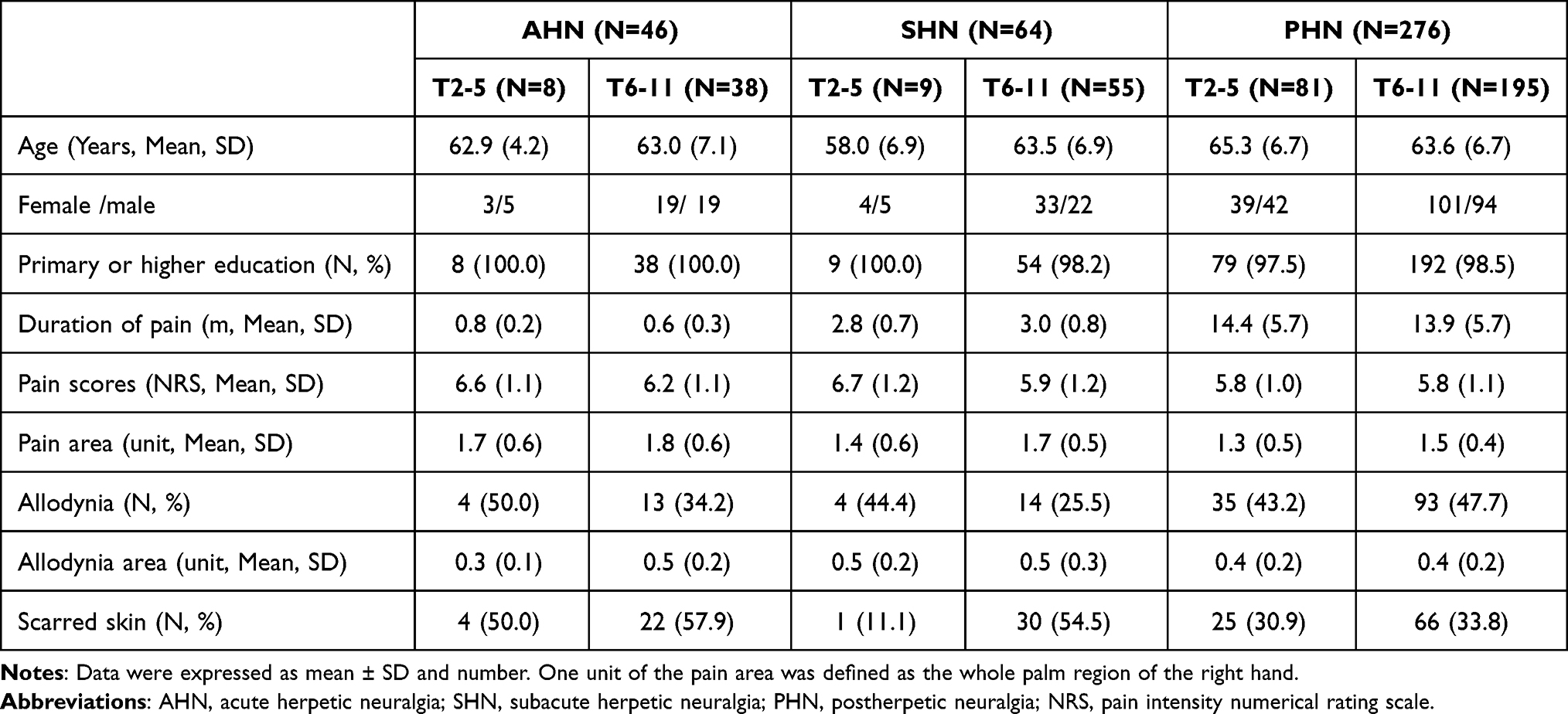 |
Table 1 Demographic, Clinical Characteristics of Patients with Torso Herpetic Neuralgia |
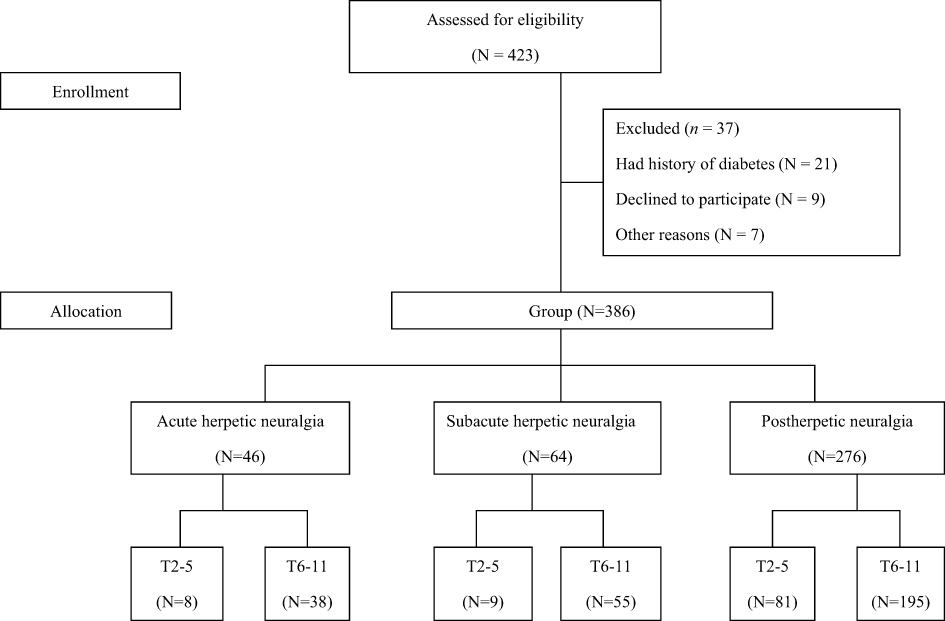 |
Figure 1 Flow chart of the study. |
The results of this study demonstrate that 37.0% (17/46) of patients with AHN experienced MA, 28.1% (18/64) of patients with SHN had MA, and 46.4% (128/276) of patients with PHN remained MA. There was no significant difference in the age distribution of MA.
In the acute stage, there were 17 patients suffered from MA. Only one had the local skin twitch induced by the cotton swab test, indicating that more participants at this stage were static MA. No local sticky feelings or sweating was found at this stage, and the iodine-starch test was negative. Another characteristic of this stage was that 26 patients had local skin scabs and scars, and only one patient suffered from MA.
In the subacute stage, 18 patients had MA, of which 16 had local skin twitching by the cotton swab test, which indicated that most participants at this stage were dynamic MA. Among 16 patients who responded to the cotton swab test, of which 15 subjects experienced local sticky feelings or sweating, and 4 patients had positive for the iodine starch test. Thirty-one patients had local scars, of which only 4 suffered from MA.
Comparatively, 46.4% (128/276) of patients with PHN were MA subtypes, and 94.5% (121/128) of them had an obvious response to the cotton swab test, suggesting that most patients were dynamic MA. Among 121 patients with dynamic MA, 95 subjects had local sticky feelings or sweating. Only 31 patients with MA and local sticky feelings or sweating had positive for the iodine starch test (Table 2). 91 patients had local scars, and 24 of them remained MA.
 |
Table 2 Comparison of the Allodynia and Sticky Feeling for Patients with Torso Herpetic Neuralgia |
However, the results may be not directly comparable as in this study confounding variables were not considered in a multivariate design, ie study failed to take into account relevant clinical parameters simultaneously. Logistic regression techniques for analysis provide a perspective on the contribution of clinical parameters to the occurrence of MA.
Binary Logistic Regression Model
Firstly, chi-square analysis was performed on the categorical MA and other factors. The Goodman-Kruskal`s gamma coefficient was 0.907 (p<0.000), the Somers`D was 0.595 (p<0.000), and Spearman’s rank correlation coefficient was 0.615 (p<0.000) of MA between with ordinal sticky feelings or sweating, which suggested that this strong correlation between MA and sticky feelings or sweating was significantly present in the overall population.
The binary logistic regression model had statistical significance (chi-square = 234.03, P < 0.001; Cox & Snell R square = 0.46, Nagelkerke R square = 0.61, all P < 0.001). We checked whether the assumed model is correctly specified. The Hosmer-Lemeshow fitting degree test showed that the overall effect of model fitting was ideal, and there was no significant difference (chi-square = 9.80, P = 0.279). Using binary multivariate logistic analysis, 5 risk factors were identified that correlated best as predictors of MA: lesion location [odds ratio (OR) =2.46; P = 0.017]; pain duration (OR= 0.94; P = 0.006), pain intensity (OR = 1.38; P = 0.020), local sticky feelings or sweating (OR = 27.57, P < 0.001), and local scars (OR = 0.07, P <0.001, Figure 2).
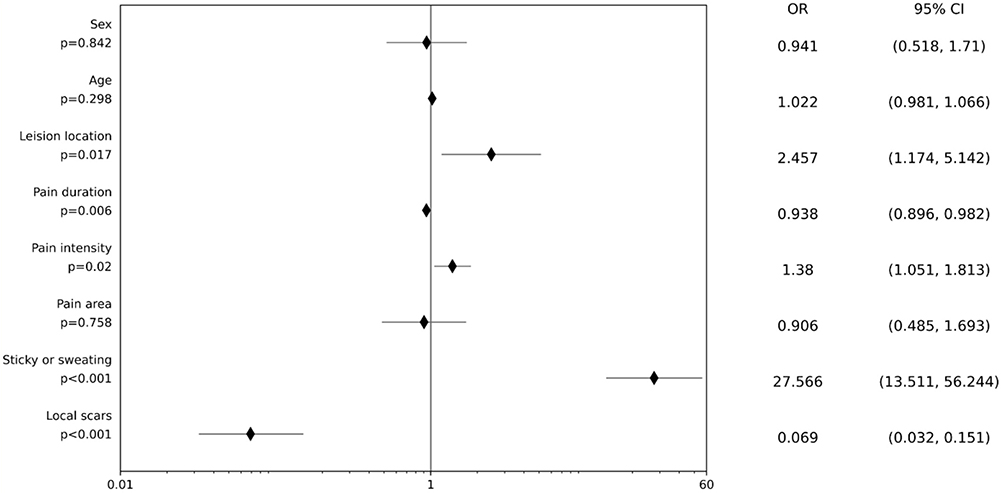 |
Figure 2 Parametric estimated value based on the collected data for binary logistic regression analyses. Abbreviations: OR, Odd Ratio; 95% CI, 95% confidence interval. |
Discussion
The majority of patients with PHN experience tactile allodynia, which is often the main clinical symptom.30,31 Touch-evoked allodynia is observed in 47% of PHN patients,32 while brush-evoked allodynia is present in 49% of PHN patients.33 In this study, 37.0% of patients experienced MA during the AHN phase, 28.1% had MA in the SHN stage, and 46.4% exhibited MA during the PHN phase. In general, dynamic MA is mediated by Aβ-fibers in pathological conditions, whereas static MA is mediated by various afferent types.34 Static MA is characterized by a decreased pain threshold. Previous research suggested that static MA by either touch sensors or sensitized mechanical nociceptors, depending on pathological conditions.21,35,36 Sensitized mechanical nociceptors rather show increased firing upon suprathreshold stimulation.34 Dynamic MA is commonly attributed to the activation of low-threshold Aβ fibers in most cases.37,38 However, in certain situations, unmyelinated, low-threshold mechanosensitive afferents also play a significant role in driving dynamic MA.39,40 Previous studies have indicated that abnormal sprouting of myelinated afferent fibers in the spinal dorsal horn is associated with MA in PHN.41 This abnormality leads to sensitization of C fibers, resulting in a lowered threshold for action potentials, increased discharge rate, and magnitude, ultimately causing spontaneous pain and allodynia mediated by the peripheral nervous system.17 Skin biopsies conducted on patients with PHN have shown a significant reduction in epidermal free nerve endings in the affected areas.42 As a result, Aβ fibers begin to sprout and establish connections with the spinothalamic tracts, which were previously responsible for transmitting pain signals through synapses with C fibers. This reorganization in the dorsal horn leads to the formation of interconnections between the spinothalamic tracts and pressure-related peripheral stimuli, ultimately causing allodynia mediated by the central nervous system.26
In our study population, we discovered that various factors were strongly linked to dynamic MA. These factors include lesion location (1:2.46), pain duration (1:0.94), pain intensity (1:1.38), and local scars (1:0.07). However, the most influential factor was found to be the presence of local sticky feelings or sweating (1:27.57).
This study discovered that patients frequently reported experiencing moisture and stickiness in the area affected by MA, which was found to be a concomitant symptom of dynamic MA (OR= 27.57, p<0.001), indicating the involvement of sympathetic nerves that innervate the sweat glands of the skin. The positive proportion of the Iodine-starch test between the T2-5 region (50.0%, 17/34) with the T6-11 region (23.7%, 15/76) showed a statistically significant difference (χ2=5.36, P=0.021). The results of the iodine starch test, which indicated the area of sweating,43 provide evidence of increased sweating rather than just a sticky feeling in this study. In the case of PHN, 29.5% of patients (15/31 at the T2-5 and 13/64 at the T6-11) experienced noticeable sweating, causing their underwear to cling to the skin and requiring the use of napkins. Additionally, in the study, 70.5% (16/31 at the T2-5 and 51/64 at the T6-11) of patients reported experiencing only sticky feelings. Importantly, the local sticky or sweating sensation in the T2-5 region was distinct from that in the T6-11 region (χ2=10.88, P=0.001). The production of sweat is regulated by signals transmitted from the central nervous system to the peripheral nervous system, specifically the autonomic nervous system (ANS). As individuals age, the number of eccrine sweat glands in their body decreases,44 with the most significant decline occurring around the age of 70 years.45 VZV DNA is not only found in cranial nerve ganglia and dorsal root ganglia (DRG) but also the sympathetic and parasympathetic ganglia as well as in the enteric nervous system of most humans.46,47 Importantly, thoracic sympathetic ganglia (TSG) supply postganglionic fibers to the skin, blood vessels, and internal organs and also connect to dorsal root ganglia via gray communicating rami. Therefore, the reactivation of VZV from both TSG and DRG, followed by the spread of the virus to the skin, could potentially result in virus-induced dysfunction of the autonomic nerves.48 Previous studies have shown a close correlation between sympathetic nerves and the pathology of HN.49 This can result in abnormal sensation and autonomic symptoms due to increased sympathetic outflow to the skin and collateral sprouting in the peripheral nerve fibers.50 The findings of this study strongly suggest that there is a focal abnormal function of these glands. The increased sweating at the T2-5 region was associated with the distribution of apocrine glands, while the increased sticky feelings at the T6-11 region were linked to the distribution of eccrine glands. VZV infection has been reported to cause segmental hyperhidrosis (exaggerated sweating particularly after eating)51 or segmental anhidrosis (loss of sweating)52 at the skin rash. Skin biopsy results have revealed a reduction in the density of innervation of the epidermis, the dermal-epidermal junction, and the eccrine sweat glands in PHN skin.53 The observed segmental hyperhidrosis may be caused by abnormal activation of sympathetic nerve function, which controls the sweat glands.54 Autonomic symptoms and allodynia are often experienced by migraine patients.55,56 Allodynia is more frequently developed in migraineurs with autonomic symptoms compared to those without autonomic manifestations.56 Prolonged peripheral sensitization appears to trigger the trigeminal-autonomic reflex in some migraineurs leading to the development of autonomic symptoms.56 The cause of sweating disturbance in patients with HN could be due to VZV-induced dysfunction of sweat glands.51,52 This study found that 80.3% of patients with segmental hyperhidrosis had dynamic MA in both the SHN and PHN phases, along with local sticky or even sweating. The presence of both dynamic MA and local sweating in the same region suggests that these symptoms may be simultaneously caused by different mechanisms.
The study found that the location of the lesion was a significant factor associated with MA (OR=2.46, P =0.017). However, there was no significant difference in the incidence of local sticky feelings or sweating between the T2-5 region (34/39) and the T6-11 region (76/107, χ2= 0.54, P=0.462) in both SHN and PHN. To differentiate between local sweating or sticky feeling, the trunk was divided into two parts: the T2-5 region, which is near the axillary sweat gland, and the T6-11 region, which is the thoracoabdominal region without the apocrine glands. In this study, 80.3% (110/137) of patients with dynamic MA experienced local sticky feelings or sweating, while patients with static MA did not report this complaint. Additionally, 21 subjects with other pain also reported local sticky feelings or sweating. In patients with allodynia, the reported maximal pain and the location of maximal allodynia on sensory examination largely overlapped.57 Age (OR = 1.02; P = 0.298), gender (OR =0.94; P = 0.842), and pain area (OR = 0.91; P = 0.758) did not have a statistically significant effect on MA in this study (Figure 2).
Patients without obvious skin lesions in the acute stage, or those with skin healing in the later stage were found to be more prone to developing MA in this study. This suggests that patients with good skin conditions were more susceptible to MA. It is important to note that HZ is self-limiting in nature.58,59 The presence of scars indicated the severity of the VZV infection during the acute stage. As the disease progresses, the skin gradually heals from the damage caused by VZV. Our study revealed that local scarring was a significant factor associated with MA (OR=0.07, P<0.001). The proportion of patients with residual scarring and MA was significantly lower compared to those experiencing other types of pain during the same disease course and in the affected dermatome. Among patients with MA, 19.2% (4/18 in the SHN and 24/128 in the PHN) had scars, while 48.5% (94/194) of patients in the SHN (27/46) and PHN (67/148) without MA had local scars, showing had a significant difference (χ2=15.28, P<0.001). According to Inomata’s reports, the severity of dermal denervation in scarred skin is associated with the development of postherpetic allodynia and hyperalgesia. However, the decrease in epidermal nerve density in scarred and stimulated skin may not be associated with postherpetic allodynia and hyperalgesia.31 The results of this study were inconsistent with those of Inomata’s.31
Our study findings indicated that pain intensity (OR=1.38, P =0.02) and pain duration (OR=0.94, P =0.006) were significant factors associated with MA. The majority of patients with PHN experience MA and its severity is closely correlated with the intensity of continuing pain.31,53 Our study also found that patients with MA often experience higher levels of pain. MA, which refers to pain associated with typically non-painful stimuli, is a prominent feature of PHN.16 Additionally, MA during the acute stage of HZ is strongly linked to the development of PHN.29,60 While a few patients may experience static MA without sticky feelings or sweating within one month, our study revealed that after a period of over a month, 93.8% (137/146) of patients in the SHN and PHN stages experienced dynamic MA, as evidenced by a clear response to the cotton swab test. Static MA is more common in the early stage, while dynamic MA tends to persist for up to 24 months and is more prevalent in the late stage. Sasaki’s research also supports our observations, suggesting that dynamic MA becomes more apparent after the herpetic pain stage and gradually increases as the lesion heals.23
This study revealed a correlation between local abnormal sweating or sticky sensations and dynamic MA in HN, indicating the involvement of sympathetic nerves that innervate the sweat glands in the skin. These findings serve as a valuable tool for identifying and evaluating static and dynamic MA, which can aid in the assessment of dynamic MA and support the use of sympathetic nerve intervention for HN. Further investigations are required to gain a better understanding of the role of MA conditions in the development of changes in central or peripheral sensitization. These investigations should focus on identifying clinical variables that may indicate an increased risk of MA signs in HN. To estimate the etiological contribution of MA, a prospective cohort study would be more suitable than a case-control study.
Conclusions
This study discovered that individuals experiencing local abnormal sweating or sticky sensations were associated with dynamic MA in HN. This suggests that the sympathetic nerves that innervate the sweat glands in the skin are involved in the occurrence of dynamic MA during the HN. These findings provide a useful indicator for identifying and evaluating static and dynamic MA, which in turn may aid in the evaluation of dynamic MA and support the use of sympathetic nerve intervention for HN.
To better understand the role of MA conditions in the development of changes in central or peripheral sensitization, further investigations are necessary. These investigations should focus on identifying clinical variables that may be associated with an elevated risk for MA signs of HN. A prospective cohort study, rather than a case-control study, is needed to estimate the etiologic contribution of MA.
Funding
This study was supported by the National Natural Science Foundation of China (81771209) for Gang Xu. The funders had no role in study design, data collection, data analysis, manuscript preparation, and publication decisions.
Disclosure
None of the authors has any financial or personal conflict of interest to disclose.
References
1. Como CN, Pearce CM, Cohrs RJ, Baird NL. Interleukin-6 and type 1 interferons inhibit varicella zoster virus replication in human neurons. Virology. 2018;522:13–18. doi:10.1016/j.virol.2018.06.013
2. Gilden DH, Gesser R, Smith J, et al. Presence of VZV and HSV-1 DNA in human nodose and celiac ganglia. Virus Genes. 2001;23:145–147. doi:10.1023/a:1011883919058
3. Anosike UG, Ouko I, Mwaura AW, Ongidi I, Mbonu CC. Phenotypes and genotypes in postherpetic neuralgia drug therapy: a narrative mini-review. Clin J Pain. 2022;38:536–540. doi:10.1097/AJP.0000000000001045
4. Niv D, Maltsman-Tseikhin A. Postherpetic neuralgia: the never-ending challenge. Pain Pract. 2005;5:327–340. doi:10.1111/j.1533-2500.2005.00035.x
5. Petersen KL, Rice FL, Farhadi M, Reda H, Rowbotham MC. Natural history of cutaneous innervation following herpes zoster. Pain. 2010;150:75–82. doi:10.1016/j.pain.2010.04.002
6. Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371:1526–1533. doi:10.1056/NEJMcp1403062
7. O’Connor KM, Paauw DS. Herpes zoster. Med Clin North Am. 2013;97:503–522. doi:10.1016/j.mcna.2013.02.002
8. Silva JR, Lopes AH, Talbot J, et al. Neuroimmune-glia interactions in the sensory ganglia account for the development of acute herpetic neuralgia. J Neurosci. 2017;37:6408–6422. doi:10.1523/JNEUROSCI.2233-16.2017
9. Devor M. Rethinking the causes of pain in herpes zoster and postherpetic neuralgia: the ectopic pacemaker hypothesis. Pain Rep. 2018;3:e702. doi:10.1097/PR9.0000000000000702
10. Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle based on sensory profiles. Pain. 2017;158(2):261–272. doi:10.1097/j.pain.0000000000000753
11. Forstenpointner J, Rice ASC, Finnerup NB, Baron R. Up-date on clinical management of postherpetic neuralgia and mechanism-based treatment: new options in therapy. J Infect Dis. 2018;218:S120–S126. doi:10.1093/infdis/jiy381
12. Pappagallo M, Oaklander AL, Quatrano-Piacentini AL, Clark MR, Raja SN. Heterogenous patterns of sensory dysfunction in postherpetic neuralgia suggest multiple pathophysiologic mechanisms. Anesthesiology. 2000;92:691–698. doi:10.1097/00000542-200003000-00013
13. Haanpaa M, Laippala P, Nurmikko T. Pain and somatosensory dysfunction in acute herpes zoster. Clin J Pain. 1999;15:78–84.
14. Ochoa JL, Yarnitsky D. Mechanical hyperalgesias in neuropathic pain patients: dynamic and static subtypes. Ann Neurol. 1993;33:465–472. doi:10.1002/ana.410330509
15. Nurmikko T, Bowsher D. Somatosensory findings in postherpetic neuralgia. J Neurol Neurosurg Psychiatry. 1990;53:135–141. doi:10.1136/jnnp.53.2.135
16. Kost RG, Straus SE. Postherpetic neuralgia--pathogenesis, treatment, and prevention. N Engl J Med. 1996;335:32–42. doi:10.1056/NEJM199607043350107
17. Fields HL, Rowbotham M, Baron R. Postherpetic neuralgia: irritable nociceptors and deafferentation. Neurobiol Dis. 1998;5:209–227. doi:10.1006/nbdi.1998.0204
18. Stucky CL, Mikesell AR. Cutaneous pain in disorders affecting peripheral nerves. Neurosci Lett. 2021;765:136233. doi:10.1016/j.neulet.2021.136233
19. Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014;13:924–935. doi:10.1016/S1474-4422(14)70102-4
20. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101:259–301. doi:10.1152/physrev.00045.2019
21. Field MJ, Bramwell S, Hughes J, Singh L. Detection of static and dynamic components of mechanical allodynia in rat models of neuropathic pain: are they signalled by distinct primary sensory neurones? Pain. 1999;83:303–311. doi:10.1016/s0304-3959(99)00111-6
22. Yamamoto W, Sugiura A, Nakazato-Imasato E, Kita Y. Characterization of primary sensory neurons mediating static and dynamic allodynia in rat chronic constriction injury model. J Pharm Pharmacol. 2008;60:717–722. doi:10.1211/jpp.60.6.0006
23. Sasaki A, Serizawa K, Andoh T, Shiraki K, Takahata H, Kuraishi Y. Pharmacological differences between static and dynamic allodynia in mice with herpetic or postherpetic pain. J Pharmacol Sci. 2008;108:266–273. doi:10.1254/jphs.08154fp
24. Gross GE, Eisert L, Doerr HW, et al. S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. J Dtsch Dermatol Ges. 2020;18:55–78. doi:10.1111/ddg.14013
25. Arani RB, Soong SJ, Weiss HL, et al. Phase specific analysis of herpes zoster associated pain data: a new statistical approach. Stat Med. 2001;20:2429–2439.
26. Dworkin RH, Gnann JW, Oaklander AL, Raja SN, Schmader KE, Whitley RJ. Diagnosis and assessment of pain associated with herpes zoster and postherpetic neuralgia. J Pain. 2008;9:S37–44. doi:10.1016/j.jpain.2007.10.008
27. Coplan PM, Schmader K, Nikas A, et al. Development of a measure of the burden of pain due to herpes zoster and postherpetic neuralgia for prevention trials: adaptation of the brief pain inventory. J Pain. 2004;5:344–356. doi:10.1016/j.jpain.2004.06.001
28. Solish N, Bertucci V, Dansereau A, et al. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol Surg. 2007;33:908–923. doi:10.1111/j.1524-4725.2007.33192.x
29. Kramer S, Baeumler P, Geber C, et al. Somatosensory profiles in acute herpes zoster and predictors of postherpetic neuralgia. Pain. 2019;160:882–894. doi:10.1097/j.pain.0000000000001467
30. Buonocore M, Gatti AM, Amato G, Aloisi AM, Bonezzi C. Allodynic skin in post-herpetic neuralgia: histological correlates. J Cell Physiol. 2012;227:934–938. doi:10.1002/jcp.22804
31. Inomata Y, Gouda M, Kagaya K, et al. Association of denervation severity in the dermis with the development of mechanical allodynia and hyperalgesia in a murine model of postherpetic neuralgia. Anesth Analg. 2013;116:722–729. doi:10.1213/ANE.0b013e31827d139a
32. Johnson RW, Wasner G, Saddier P, Baron R. Herpes zoster and postherpetic neuralgia: optimizing management in the elderly patient. Drugs Aging. 2008;25:991–1006. doi:10.2165/0002512-200825120-00002
33. Maier C, Baron R, Tolle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain. 2010;150:439–450. doi:10.1016/j.pain.2010.05.002
34. La JH, Chung JM. Peripheral afferents and spinal inhibitory system in dynamic and static mechanical allodynia. Pain. 2017;158:2285–2289. doi:10.1097/j.pain.0000000000001055
35. Eijkelkamp N, Linley JE, Torres JM, et al. A role for Piezo2 in EPAC1-dependent mechanical allodynia. Nat Commun. 2013;4:1682. doi:10.1038/ncomms2673
36. Brenneis C, Kistner K, Puopolo M, et al. Phenotyping the function of TRPV1-expressing sensory neurons by targeted axonal silencing. J Neurosci. 2013;33:315–326. doi:10.1523/JNEUROSCI.2804-12.2013
37. Gracely RH, Lynch SA, Bennett GJ. Painful neuropathy: altered central processing maintained dynamically by peripheral input. Pain. 1992;51:175–194. doi:10.1016/0304-3959(92)90259-E
38. Campbell JN, Raja SN, Meyer RA, Mackinnon SE. Myelinated afferents signal the hyperalgesia associated with nerve injury. Pain. 1988;32:89–94. doi:10.1016/0304-3959(88)90027-9
39. Liljencrantz J, Bjornsdotter M, Morrison I, et al. Altered C-tactile processing in human dynamic tactile allodynia. Pain. 2013;154:227–234. doi:10.1016/j.pain.2012.10.024
40. Seal RP, Wang X, Guan Y, et al. Injury-induced mechanical hypersensitivity requires C-low threshold mechanoreceptors. Nature. 2009;462:651–655. doi:10.1038/nature08505
41. Pan HL, Khan GM, Alloway KD, Chen SR. Resiniferatoxin induces paradoxical changes in thermal and mechanical sensitivities in rats: mechanism of action. J Neurosci. 2003;23:2911–2919. doi:10.1523/JNEUROSCI.23-07-02911.2003
42. Oaklander AL. The density of remaining nerve endings in human skin with and without postherpetic neuralgia after shingles. Pain. 2001;92:139–145. doi:10.1016/s0304-3959(00)00481-4
43. Rzany B, Bechara FG, Feise K, Heckmann M, Rapprich S, Worle B. Update of the S1 guidelines on the definition and treatment of primary hyperhidrosis. J Dtsch Dermatol Ges. 2018;16:945–952. doi:10.1111/ddg.13579
44. Wilke K, Martin A, Terstegen L, Biel SS. A short history of sweat gland biology. Int J Cosmet Sci. 2007;29:169–179. doi:10.1111/j.1467-2494.2007.00387.x
45. Yonemoto Y. Studies on measurements of the scalp tissue of the Japanese adult (II). Okajimas Folia Anat Jpn. 1968;45:143–163. doi:10.2535/ofaj1936.45.4_143
46. Nagel MA, Rempel A, Huntington J, Kim F, Choe A, Gilden D. Frequency and abundance of alphaherpesvirus DNA in human thoracic sympathetic ganglia. J Virol. 2014;88:8189–8192. doi:10.1128/JVI.01070-14
47. Kennedy PG, Grinfeld E, Gow JW. Latent varicella-zoster virus is located predominantly in neurons in human trigeminal ganglia. Proc Natl Acad Sci USA. 1998;95:4658–4662. doi:10.1073/pnas.95.8.4658
48. Sakakibara R, Sawai S, Ogata T. Varicella-zoster virus infection and autonomic dysfunction. Auton Neurosci. 2022;242:103018. doi:10.1016/j.autneu.2022.103018
49. Makharita MY. Prevention of post-herpetic neuralgia from dream to reality: a ten-step model. Pain Phys. 2017;20:E209–E220.
50. Hakusui S, Iwase S, Mano T, Takahashi A. 皮膚交感神経活動の著明なこう進をきたした minor reflex sympathetic dystrophyの1例 [A microneurographic analysis of minor reflex sympathetic dystrophy with increased skin sympathetic activity--report of a case]. Rinsho Shinkeigaku. 1990;30:668–671. Japanese.
51. Bourgeois P, Morren MA. Frey’s syndrome after herpes zoster virus infection in a 2-year-old girl. Pediatr Dermatol. 2015;32:e184–185. doi:10.1111/pde.12604
52. Kurihara K, Tsushima T, Tokura Y. Idiopathic segmental anhidrosis associated with varicella. J Dermatol. 2017;44:211–212. doi:10.1111/1346-8138.13455
53. Rowbotham MC, Yosipovitch G, Connolly MK, Finlay D, Forde G, Fields HL. Cutaneous innervation density in the allodynic form of postherpetic neuralgia. Neurobiol Dis. 1996;3:205–214. doi:10.1006/nbdi.1996.0021
54. Fujimoto T. Pathophysiology and treatment of hyperhidrosis. Curr Probl Dermatol. 2016;51:86–93. doi:10.1159/000446786
55. Ekizoglu E. Autonomic symptoms and allodynia in migraine. Noro Psikiyatr Ars. 2018;55:197–198. doi:10.29399/npa.23345
56. Barbanti P, Aurilia C, Dall’Armi V, Egeo G, Fofi L, Bonassi S. The phenotype of migraine with unilateral cranial autonomic symptoms documents increased peripheral and central trigeminal sensitization. A case series of 757 patients. Cephalalgia. 2016;36:1334–1340. doi:10.1177/0333102416630579
57. Rowbotham MC, Fields HL. Post-herpetic neuralgia: the relation of pain complaint, sensory disturbance and skin temperature. Pain. 1989;39:129–144. doi:10.1016/0304-3959(89)90001-8
58. Sengupta S. Cutaneous herpes zoster. Curr Infect Dis Rep. 2013;15:432–439. doi:10.1007/s11908-013-0356-y
59. Werner RN, Nikkels AF, Marinovic B, et al. European consensus-based (S2k) guideline on the management of Herpes Zoster - guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), part 1: diagnosis. J Eur Acad Dermatol Venereol. 2017;31:9–19. doi:10.1111/jdv.13995
60. Haanpää M, Laippala P, Nurmikko T. Allodynia and pinprick hypesthesia in acute Herpes Zoster, and the development of postherpetic neuralgia. J Pain Symptom Manage. 2000;20:50–58. doi:10.1016/s0885-3924(00)00149-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.