Back to Journals » International Journal of General Medicine » Volume 18
Analysis of Risk Factors for Acute First-Ever Ischemic Stroke in the Elderly Population of Eastern Liaoning Province: A Case-Control Study
Authors Liu WT, Yang ZC, Wang XH, Yang YJ, Liu C, Yan HB, Zhang YN, Wang J ![]() , He H
, He H ![]()
Received 17 December 2024
Accepted for publication 20 May 2025
Published 26 May 2025 Volume 2025:18 Pages 2715—2725
DOI https://doi.org/10.2147/IJGM.S512339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Satish Nair
Wen-Tao Liu,1 Zhi-Chao Yang,1 Xiao-Hui Wang,1 Yuan-Jiao Yang,1 Chen Liu,1 Han-Bing Yan,1 Ya-Nan Zhang,1 Jun Wang,1 Hui He1– 4
1Clinical Research Center, Liaoning Province Benxi Central Hospital, Benxi, Liaoning, 117000, People’s Republic of China; 2Department of Research and Development, Liaoning Province Benxi Clinical Bio-Bank, Benxi, Liaoning, 117000, People’s Republic of China; 3Training Department, China Medical University Benxi Central Hospital Postgraduate Training Workstation, Benxi, Liaoning, 117000, People’s Republic of China; 4Department of Research and Development, Shenyang Kati Health Consulting Co. LTD, Shenyang, Liaoning, 110101, People’s Republic of China
Correspondence: Hui He, Clinical Research Center, Liaoning Province Benxi Central Hospital, China Benxi Central Hospital Taizihe New City Campus, 120, Weining Avenue, Mingshan District, Benxi, Liaoning Province, 117000, People’s Republic of China, Tel +86-18941435621, Email [email protected]
Purpose: This study aimed to assess the risk factors for acute first-ever ischaemic stroke (IS) in the elderly population aged ≥ 60 years in the eastern part of Liaoning Province, China.
Patients and Methods: This retrospective case-control study was derived from the Benxi Clinical Biobank and the Thrombotic Chronic Non-Communicable Disease Cohort Study in Natural Populations in Eastern Liaoning (ChiCTR2300074593). We collected cases of acute IS in the elderly population and selected the corresponding controls in a 1:1 ratio for inclusion in the study. Data collection included sociodemographics, clinical characteristics, and laboratory characteristics. We used IBM SPSS Statistics V26.0 for Windows for descriptive statistical analysis and conditional logistic regression analysis to determine risk factors for IS.
Results: This study included 326 cases (163 pairs) of study subjects. The median age of the cases and controls was 65 years (62– 70). Both groups were predominantly 60– 69 years old in the age subgroups, 69.3% in the case group and 74.2% in the control group, with a p-value of 0.011; females in both groups accounted for 49.1% in the case group and 49.1% in the control group. Variables with P < 0.05 in the univariate analysis included current smoking, current alcohol consumption, fasting blood glucose, and hypertension. Variables statistically significant in the univariate analysis entered into the multivariate multifactorial analysis. The results showed that hypertension (OR, 1.977; 95% CI, 1.322– 2.956) and current alcohol consumption (OR, 1.549; 95% CI, 1.086– 2.210) were independent risk factors for acute first-ever IS in the elderly population aged ≥ 60 years.
Conclusion: Hypertension and current alcohol consumption are major risk factors for IS in an elderly population in eastern Liaoning Province.
Keywords: aged, risk factors, ischemic stroke, case-control studies
Introduction
According to the 2019 Global Burden of Disease study, stroke is the second leading cause of death and the third most common cause of disability globally,1 and the incidence and mortality rates of stroke in China are higher than the world average,2 with acute ischemic stroke (IS) accounting for 60%~80% of all stroke cases in China.3 In 2019 alone, there were 24.2 million current cases of IS, 2.9 million new cases, 1.03 million deaths due to IS, and 21.4 million disability-adjusted life-years (DALYs) due to IS.4 Comparison with the past 30 years reveals that IS’s prevalence and mortality rates in China’s elderly population have significantly increased.4 Therefore, the burden of disease caused by IS in China remains earnest, and with the aging of Chinese society, IS will become an essential public health problem.
Liaoning Province is located in northeastern China. The seventh national census in 2020 showed a resident population of 42,591,407.5 The proportion of people aged ≥60 years was 25.72%, which was the highest compared with other provinces in China.6 The crude prevalence of IS aged ≥40 years in Liaoning Province was 5.51% (602/10926) in rural areas7 and 4.8% in urban areas,8 which was significantly higher than the national crude prevalence of IS (1.79%).9 Whether this high prevalence is related to a local elderly population with specific IS risk factors deserves further exploration.
In several previous studies conducted on stroke-related risk factors in the elderly population, typical stroke risk factors mainly include hypertension, diabetes mellitus, heart disease, family history of stroke, smoking, and alcohol consumption.7,10–14 Another survey, which included 12 regions in northern China, also showed that hypertension was an independent risk factor for IS aged ≥40.9 Tu et al15 showed that hyperuricemia independently predicted the risk of stroke in the elderly population (Hazard Ratio: 2.32, 95% confidence interval [CI] 1.56–3.45).
However, there are no studies analyzing risk factors for acute first IS in the elderly population aged ≥60 years in the eastern part of Liaoning Province. In this study, we applied a case-control research method to investigate the risk factors for acute first IS in the elderly population in eastern Liaoning Province.
Materials and Methods
Study Design and Population
This study is a retrospective case-control study. The study subjects were from the Benxi Clinical Bio-bank and the Cohort Study of Thrombotic Chronic Non-Communicable Diseases in Natural Populations in Eastern Liaoning (ChiCTR2300074593). The data were collected from May 2018 to July 2023. All case groups underwent a CT scan of the brain to exclude hemorrhage and, when possible, a magnetic resonance imaging (MRI) scan of the brain to confirm IS. Controls were individuals who were confirmed to be free of IS by cranial CT or MRI during the same period. The study complied with the Ethical Guidelines for Medical and Health Research Involving Human Subjects and the Declaration of Helsinki (revised by Brazil in 2013). It was approved by the Ethics Committee of Benxi Central Hospital, Liaoning Province, China (No. KY2022-033). Due to the retrospective design of this study, the Ethics Committee approved an exemption from informed consent for this project. Patient records and information were anonymized and de-identified before analysis.
The definition of IS was acute focal neurologic dysfunction due to vascular injury confirmed by clinical examination, cranial CT, and MRI for more than 24 hours.16 The diagnostic codes of IS were the International Classification of Diseases (ICD10), 10th edition, and patients with IS numbered according to the ICD numbers: I63.0, I63.1, I63.2, I63.3, I63.4, I63.5, I63.6, I63.8, and I63.9.17
Inclusion criteria for the case group were as follows: (1) age 60 years and older; (2) all patients with acute first IS stroke (IS diagnosed within 72 hours of admission within ≤5 days of onset), with CT or MRI brain imaging completed within 1 week of onset; (3) information on the main variables should be completed (missing values <10%).18
The exclusion criteria for the case group were as follows: (1) previous history of IS; (2) onset of illness had been more than 5 days; (3) severe cardiopulmonary and other vital organ diseases; (4) severe immune system diseases; (5) severe infections; (6) malignant tumors; (7) severe hemorrhagic tendency, active bleeding, or presence of hematological disorders; (8) history of neurological-related disorders other than hypertension and diabetes mellitus; and (9) Incomplete information.17
Inclusion criteria for the control group were (1) 60 years of age and older; (2) no abnormalities on cranial CT or MRI scans.
Exclusion criteria for the control group: (1) previous history of IS; (2) severe cardiopulmonary and other vital organ diseases; (3) severe immune system diseases; (4) severe infections; (5) malignant tumors; (6) severe hemorrhagic tendency, active bleeding, or the presence of hematological disorders; (7) other neurological disorders; and (8) incomplete data.The sex and age (±2 years) of each control group matched the cases.17
Definition of risk factors: (1) Hypertension was defined as (blood pressure ≥140/90 mm Hg, history of hypertension, or being treated with anti-hypertensive drugs);2
(2) Cardiac disease was defined as a history of current diagnosis of atrial fibrillation, cardiomyopathy, rheumatic heart disease, heart valve disease, heart failure, or ischemic heart disease;19 (3) Diabetes mellitus was defined by current US Food and Drug Administration criteria: fasting blood glucose ≥126 mg/dL (7.0 mmol/L) or 2-hour postprandial blood glucose ≥200 mg/dL (11.1 mmol/L) or glycosylated hemoglobin ≥6.5% (48 mmol/mol) or, for patients with typical symptoms of hyperglycemia or hyperglycemic crises, a random blood glucose ≥ 200 mg/dL (11.1 mmol/L)20 or self-reported previous diagnosis of diabetes mellitus by an internist or self-reported use of insulin or use of antidiabetic medications within the past two weeks; (4) Family history of stroke was defined as when the subject had a first-degree relative (maternal, paternal, or sibling) diagnosed with stroke;16 (5) The definition of Smoking status was current smokers (those who had smoked any tobacco in the past 12 months) and nonsmokers were those who had never smoked or had ever smoked in their lifetime;19 (6) Current drinkers were defined as participants who were currently drinking alcohol (any form of alcohol drinker), and non-drinkers were those who had never consumed alcohol or had ever consumed alcohol in their lifetime;19 (7) Uric acid levels were recorded in mg/dl, which can be converted to μmol/ L by multiplying by 59.485. Serum uric acid levels >7.0 mg/dl in men and >5.7 mg/dl in women were considered hyperuricemia.21
Data Collection
To ensure consistency of inclusion and enable follow-up, the Benxi Clinical Bio-bank exported monthly case data, screened hospitalized patients and medical examiners during the month, and finally collected data.
We screened cases as follows: screening time frame May 2018-June 2023. The case pools were screened: (1) patients aged ≥60 years were screened in the cohort, and (2) all patients with IS were selected according to ICD codes in the primary diagnosis, 508 consecutive patients were included, and (3) 233 eligible cases were obtained after exclusion according to the exclusion criteria.
The method of screening the control group in this study was as follows: The screening timeframe was May 2018-June 2023. (1) 3098 cases were selected from the cohort who had physical examinations without abnormalities in head CT; (2) 524 cases were screened for complete clinical information; (3) 233 cases were screened after duplicated entries; (4) 134 cases were screened for age ≥60 years; (5) 83 cases were finally obtained from the population that met the criteria based on the exclusion criteria; and (6) 377 cases of inpatients from the cohort who had a standard head CT and were ≥60 years of age were obtained from the cohort. We obtained 103 cases from the population that met the criteria after, according to the exclusion criteria: A total of 186 cases from the eligible population (physical examination + hospitalization) were included in the control group.
This study covered three dimensions of risk factors, including sociodemographic characteristics, clinical characteristics, and laboratory tests. Sociodemographic characteristics considered included gender, age, smoking, and alcohol consumption; clinical characteristics included hypertension, diabetes, heart disease, and a family history of stroke; and laboratory tests included fasting blood glucose and uric acid. Subsequently, data were backed up and archived as soft and hard copies to avoid loss. Using code numbers ensured Confidentiality rather than the names of study subjects.
Sample Size Estimation
The sample size of cases and controls was estimated using PASS. Hypertension was a significant risk factor for IS from the literature. Due to the lack of studies on the prevalence of prior hypertension in the local study population, this study referred to the data in the literature and concluded that the prevalence of hypertension in the control population was 52.6%~61.24% (age ≥60 years),22,23 and the odds ratio (OR) for the risk of IS for the exposed factors was 2.55–4.9,18,24 with a confidence interval (CI) of 95% and a certainty of 90%. We estimated sample sizes of 75–199 for each case and control group.
Data Analysis
We used IBM SPSS Statistics V26.0 for Windows for all analyses and tested the normality of Measurement information. Measurement information that conformed to normal distribution was mean ± standard deviation. Comparisons between the two groups were paired t-tests. If they did not conform to a normal distribution, expressions were median and quartiles, and comparisons between the two groups were made using the Wilcoxon signed mean rank test. Frequencies or percentages expressed Count data and compared two groups using the paired-design chi-square test (McNemar). We constructed multivariate conditional logistic regression to assess the effect of risk factors on IS. Variables were included in the final regression model if they were significant in univariate analyses.25 P values <0.05 (two-tailed test) were considered statistically significant. Cases and controls were matched 1:1 by sex and age (±2 years).26 We removed Variables with missing values >10%. No interpolation was for data with ≤10% missingness.
Quality Control
Several measures to ensure the quality of the results included pretesting the questionnaire and standardizing it before the study began. We cleaned and standardized the raw medical data collected: (1) Data checking and cleaning: The raw data were summarized and sorted to form a display format of values, time, date, and complete and half corners for consistency. We removed and pretested the questionnaire and standardized it. Checking reproducibility and removing exact duplicate data; (2) Data standardization: calibration normalization of four elements: specimen type, test item name, test result unit, and test reference value. Before statistically analyzing the data, two quality controllers from the Bio-bank verified 10% until the error rate was less than 1% as qualified. They corrected the erroneous data and then backed up the data.
Result
The case group included 508 patients with acute first-ever IS, and the control group included 511 participants with no abnormal head CT findings during the same period. 326 (163 pairs) participants were included in this study after we matched the case and control groups 1:1 by sex and age±2. The study flow chart is in Figure 1.
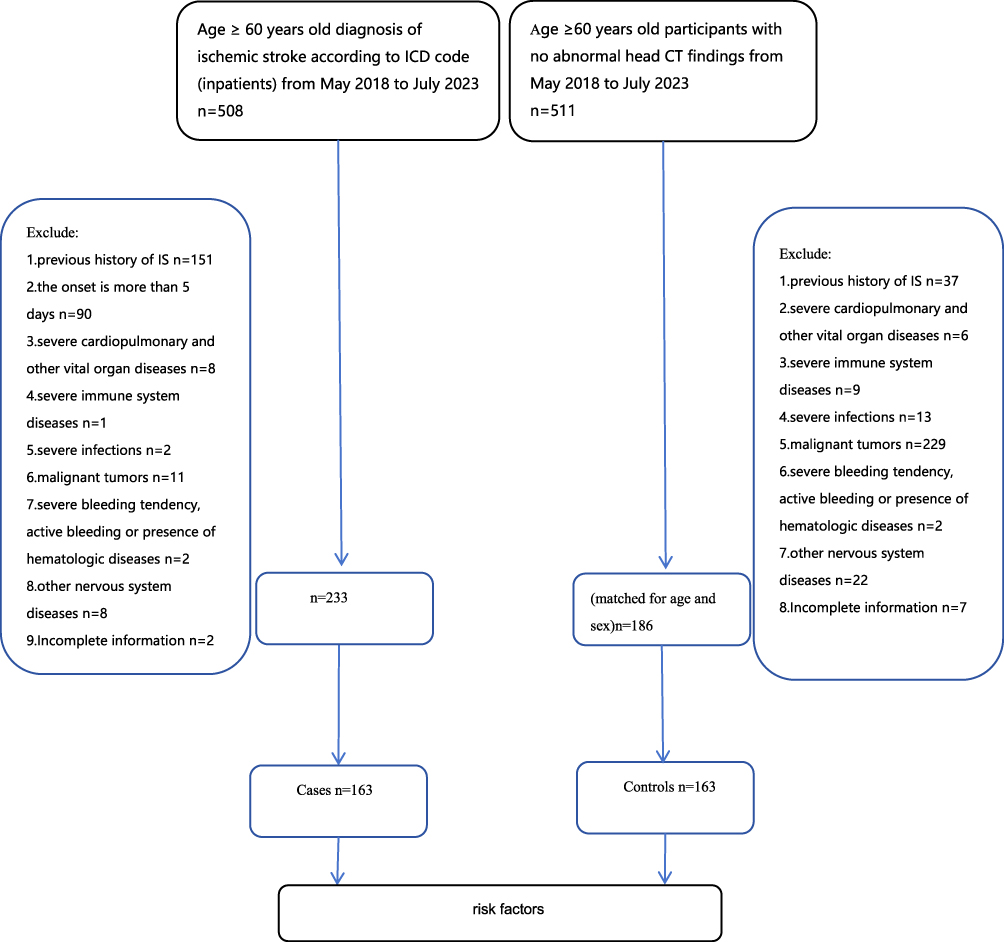 |
Figure 1 Study flow chart. Abbreviations: IS, ischemic stroke; ICD, International Classification of Diseases. |
Baseline Characteristics of the 2 Groups
The median age of the case and control groups was 65 years (interquartile spacing: 62–70 years). Among the age subgroups, 60–69 had the highest proportion in both groups. The proportion of people aged 60–69 years was 69.3% in the case group and 74.2% in the control group; the proportion of women in both groups was 49.1%; and the median fasting blood glucose in the case group was 5.82 (range: 5.15–8.13). The median fasting blood glucose in the control group was 5.7 (5.05–6.81). The difference in fasting blood glucose between the two groups was statistically significant (P=0.018). There were 54 current smokers in the case group (33.3%). There were 30 current smokers in the control group (18.5%). The difference in smoking prevalence between the two groups was significant (P<0.001); there were 41 cases of current alcohol drinkers in the case group, accounting for 25.3%. In the control group, there were 17 cases of current alcohol consumption, accounting for 10.5%. The difference in the rate of alcohol consumption between the two groups was significant (P<0.001). There were 132 cases of hypertension in the case group, accounting for 81%. There were 90 cases of hypertension in the control group, accounting for 55.2%. The difference in the prevalence of hypertension between the two groups was significant (P<0.001). The rest of the baseline characteristics were not statistically different. (Table 1)
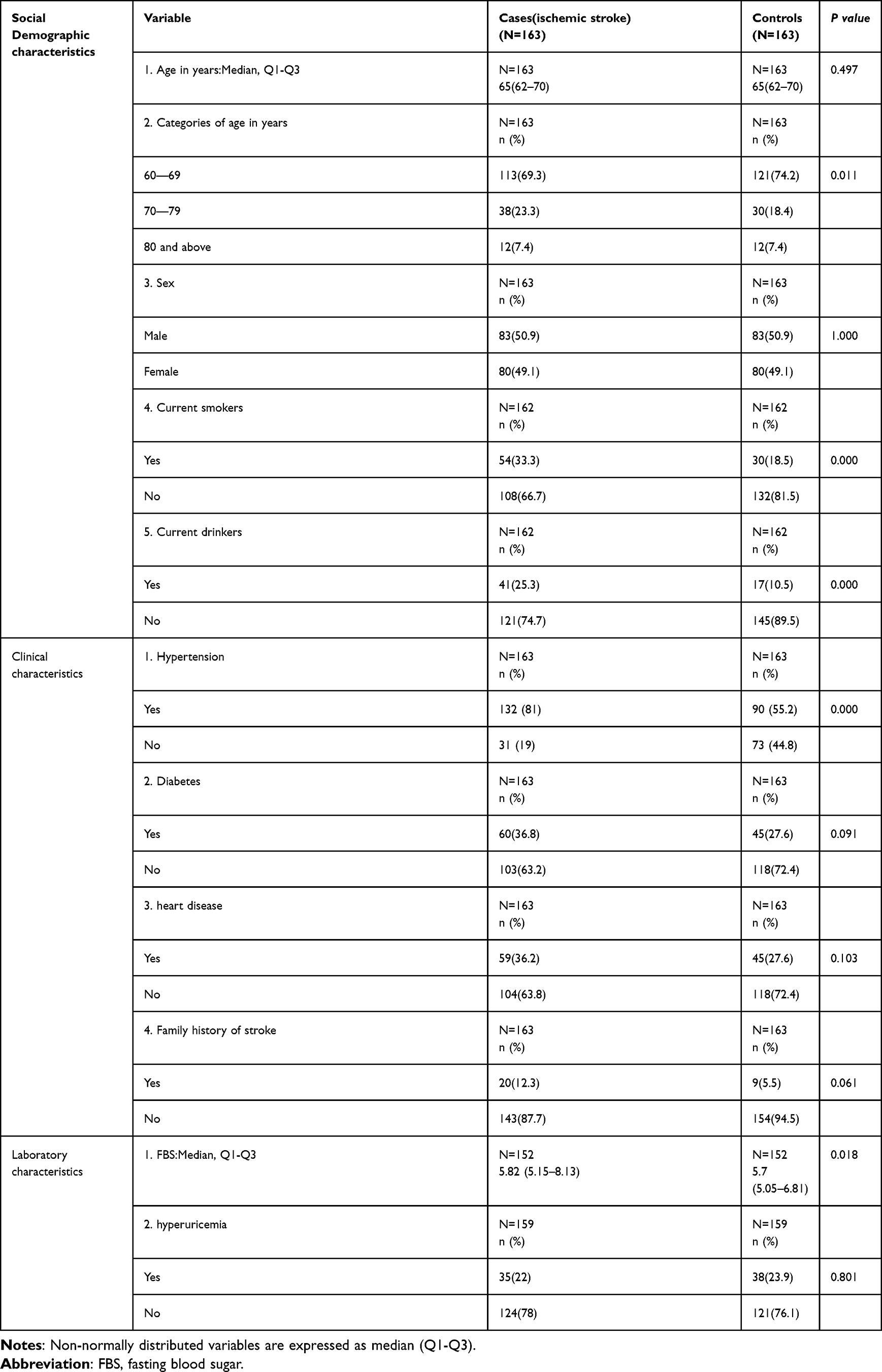 |
Table 1 Baseline of the Two Groups |
This study also analyzed demographic information such as race, marital status, and residence. (Supplementary Table 1) None of these factors were statistically significant in the univariate analysis and did not enter into the final multivariate analysis process.(Supplementary Table 2)
Risk Factors for IS in Univariate Analysis
The uncorrected OR for current smoking was 1.43 (95% CI: 1.035–1.989). The prevalence of smoking was 33.3% in the case group and 18.5% in the control group. The difference between the two groups was statistically significant (P=0.03); the uncorrected OR for current alcohol consumption was 1.56 (95% CI: 1.095–2.223). The rate of alcohol consumption was 25.3% in the case group and 10.5% in the control group. The difference between the two groups was statistically significant (P<0.05); the uncorrected OR for fasting blood glucose was 1.064 (95% CI: 1.010–1.121). The difference between the two groups was statistically significant (P<0.05); the uncorrected OR for hypertension was 1.995 (95% CI: 1.349–2.950). The prevalence of hypertension was 81% in the case group and 55.2% in the control group. The difference between the two groups was statistically significant (P=0.001). (Table 2)
 |
Table 2 Univariate Analysis of the Two Groups |
Risk Factors for IS at Multivariate Analysis
Variables with P<0.05 in the univariate analysis included current smoking, current alcohol consumption, fasting blood glucose, and hypertension, and the method of variable selection was stepwise screening. The results of the multifactorial analysis showed that hypertension (OR, 1.977; 95% CI, 1.322–2.956) and current alcohol consumption (OR, 1.549; 95% CI, 1.086–2.210) were independent risk factors for IS in the elderly population aged ≥60 years. (Table 3).
 |
Table 3 Risk Factors for Ischemic Stroke at Multivariate Analysis |
Results of the Multiplicative Interaction Between Hypertension and Current Drinking
For the results of the multifactorial analysis, we performed an interaction analysis.27,28 The results showed no multiplicative interaction between hypertension and current alcohol consumption (OR = 0.558, 95% CI, 0.238–1.312). (Supplementary Table 3)
Discussion
Our study identified hypertension and current alcohol consumption as significant risk factors for the first-ever IS in an elderly population aged ≥60 years in the eastern part of Liaoning Province, China.
The participants in our study were predominantly an elderly population, as the risk of IS continues to increase with age, and several mechanisms could explain this phenomenon. First, aging leads to metabolic disorders increases the secretion of pro-inflammatory factors, impairs the anti-inflammatory system, disrupts the energy balance of the central nervous system, and undermines the integrity of the neurovascular system. Second, aging alters cerebrovascular structure, damages arterial endothelial cells, and disrupts cerebrovascular self-regulation.29 China has a larger elderly population than other countries, and its aging population is one of the largest in the world,30 so there is an urgent need to find geographically specific risk factors for IS in the elderly population.
In our study, 132 patients with IS had hypertension, accounting for 81% of all IS patients. Studies in different regions of China have reported similar figures, which ranged from 72.7% in northern China,9 78.3% in rural northeast China,27 and 57.3% in southwestern China,31 all of which have found hypertension to be the most important risk factor for the development of IS in the Chinese elderly population. Similarly, worldwide, several studies have found hypertension to be a common risk factor for IS in the elderly population.24,32–34
There are some regional differences in the prevalence of hypertension in the Chinese natural population. We believe that the emergence of hypertension as the most important risk factor for IS in the elderly population is closely related to the environment and lifestyle habits of the population studied here. The natural environment influences the eastern part of Liaoning, and local people like to eat pickled foods. According to a survey, the salt intake (11.7 g/person/d) and sodium intake (5 g/person/d) of the residents of Liaoning province exceeded the maximum recommended daily amount (5 g/person/d of salt and two g/person/d of sodium), which was higher than that of other cities in China,35 which led to the prevalence of hypertension among the residents (aged 35–70 years) of nearly half of the population.36 Our current study showed that the prevalence of hypertension in the elderly population in the control group was 55.2%. This finding shows that the prevalence of hypertension is higher among the elderly in the natural population of the region. Moreover, a study reported that only 47.4% of hypertensive patients over 40 years of age in Northeastern China were aware of their elevated blood pressure, and the control rate was only 10.2%.37 Therefore, strict primary and secondary prevention measures for hypertension are recommended in this region to minimize the occurrence of IS in the elderly.
In our study, current alcohol consumption was another important risk factor for the first-ever IS in the elderly population aged ≥60 years in eastern Liaoning Province. Alcohol consumption was present in 25.3% of IS patients. A meta-analysis showed that chronic alcohol consumption is a risk factor for stroke in Asian populations.38 Previous studies have also produced controversial results regarding the importance of this factor. Certain studies have identified chronic heavy drinking as a risk factor for IS,39–41 and one study found that reducing alcohol intake to mild to moderate levels significantly reduced the incidence of IS compared with persistent alcohol abuse.42 However, other studies have reached the opposite conclusion.43,44 Chronic heavy drinking is a risk factor for many chronic diseases, such as hypertension and diabetes,44,45 which increase the risk of IS. It is worrying that China has become the country with the highest per capita consumption of alcohol46 and that a higher proportion of males in the Northeast region are heavy drinkers than residents of other regions.47 Heavy alcohol consumption in the region’s population may be due to the cold weather and drinking culture in the Northeast. In a systematic analysis of the Global Burden of Disease 2020 study, IS in people aged 65 years and older was found to result in 14.2% (13.5–14.9) and 16.0% (15.2–16.7) of all alcohol-related disability-adjusted life-years (DALYs) in men and women.48 Therefore, limiting alcohol consumption and seeking healthy drinking patterns may play an indirect role in preventing the occurrence of IS.
The present study found that although hypertension and current alcohol consumption were each significantly associated with IS, their interaction was not significant. The reason may be that the sample size was small enough to reveal the interaction. Future studies need larger sample sizes to explore whether there is an interaction between hypertension and current alcohol consumption in their effects on IS risk in older adults. (Supplementary Tables 1–3)
The results of this study are consistent with those of another previous case-control study (INTERSTROKE 2007–2015),18 which included populations from 32 countries in Asia, the Americas, Europe, Australia, and the Middle East and Africa, and concluded that the global burden of stroke, including IS, is mainly attributable to potentially modifiable risk factors. Of the ten modifiable risk factors for stroke identified in the INTERSTROKE study, our study confirmed that hypertension and alcohol consumption were two significant risk factors. The odds ratio for hypertension in our study was equal to 1.977 compared with 2.78 in the INTERSTROKE study; similarly, for alcohol consumption, the OR for heavy or occasional heavy drinking was 2.14 in the INTERSTROKE study, and the OR for drinking, defined in our study as participants currently consuming alcohol (any form of alcohol drinkers), was 1.549.
Our study and the INTERSTROKE study also compared other study variables. We found that although the prevalence of diabetes mellitus was higher in the case group (36.8%) than in the control group (27.6%), it was not significantly associated with IS. This result may be related, on the one hand, to the small sample size and, on the other hand, to the high prevalence of diabetes mellitus among the elderly in the natural population of the Northeast.49 Regarding whether smoking was associated with the occurrence of IS, 33.3% of the smokers in the case group were higher than in the control group (18.5%). However, this factor was not statistically significant in IS. We analyzed the reasons for this and need to further analyze the smoking status according to the duration and number of cigarettes per day to examine this association correctly. Given that smoking is associated with an increased risk of adverse inpatient outcomes in patients with acute IS,50 increased smoking cessation is necessary. Differences between the results of this study and those of the INTERSTROKE study may be related to differences in the selection of control subjects (hospital-based or community-based), the choice of study population, the method of risk factor assessment, and differences in the prevalence of risk factors between populations in different regions.18
In the present study, we also observed that the rate of family history of heart disease and stroke was higher in the case group than in the control group. At the same time, the mean values of fasting blood glucose also showed a trend of being higher in the case group than in the control group, but these differences did not reach statistical significance. It also turns out that the rate of hyperuricemia was not substantially more significant in the case group (22%) than in the control group (23.9%), with no statistical difference between the two groups. This negative result is likely due to the study’s limited sample size.
Strengths of this study. First, we successfully collected first-episode IS cases within 5 days of onset, a time window that ensured the reliability and timeliness of the data. Second, using a matched case-control design method effectively enhanced the credibility of the study results.
This study provides an evidence-based basis for preventing and controlling IS in the elderly population in eastern Liaoning Province, but there are some limitations. First, as a single-center and small sample size case-control study, the generalisability of its findings may be limited. We plan to expand the sample size in future studies to validate this finding. Second, as this was a retrospective study, we had relatively limited access to information to meticulously categorize alcohol intake into mild, moderate, and severe, as well as did not obtain data on hypertension control, thus preventing an in-depth stratified analysis and in the future, we may consider conducting a prospective study to explore this issue further. In addition, several studies have shown that dyslipidemia and obesity are risk factors for IS51,52 and that statin interventions given to patients with dyslipidemia with good adherence can reduce the risk of stroke.53 We did not include obesity and lipid variables in the final statistical analysis. Finally, this study was geographically limited to the eastern part of Liaoning Province, and therefore, its results may not be more generalizable to other regions or populations.
Conclusion
This study demonstrates that hypertension and current alcohol consumption are major risk factors for IS in the elderly population in eastern Liaoning Province. The high prevalence of hypertension and current alcohol consumption as potential and modifiable risk factors in patients with IS highlights the urgency of developing and implementing a national control plan. The program should focus on raising public awareness of these risk factors and on effective interventions to reduce their occurrence and improve their control.
Data Sharing Statement
The dataset generated and analyzed during the current study is not publicly available due to patient privacy restrictions and ongoing data collection for research purposes but are available from the corresponding author (Hui He, [email protected]) on reasonable request.
Acknowledgments
The authors would like to thank the people and organizations involved in this study. This work was supported by the Benxi City 2023 Innovative Topics Research Project (No. BKYW2301).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Feigin VL, Stark BA, Johnson CO. Global. regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/s1474-4422(21)00252-0
2. Wang H, Wu M, Tu Q, Li M. Risk factors for stroke in a population of central China: a cross-sectional study. Medicine. 2022;101(46):e31946. doi:10.1097/md.0000000000031946
3. Liu L, Nguyen TN, Chen HS. Endovascular treatment for acute ischemic stroke in China: a study protocol for a prospective, national, multi-center, registry study. Front Neurol. 2023;14:1171718. doi:10.3389/fneur.2023.1171718
4. Ye Y, Zhu YT, Zhang JC, et al. Burden and attributable risk factors of ischemic stroke in China from 1990 to 2019: an analysis from the global burden of disease study 2019. Front Neurol. 2023;14:1216777. doi:10.3389/fneur.2023.1216777
5. National Bureau of Statistics. Bulletin of the seventh national population census (No. 3). 2021.
6. National Bureau of Statistics. Bulletin of the seventh national population census (No. 5). 2021. Available online: http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/202106/t20210628_1818824.html.
7. Tian YM, Jing L, Lin M, et al. Prevalence and risk factors of ischemic stroke in rural areas of Liaoning province. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48(2):148–153. doi:10.3760/cma.j.issn.0253-3758.2020.02.011
8. Xing L, Jing L, Tian Y, et al. Epidemiology of stroke in urban northeast China: a population-based study 2018–2019. Int J Stroke. 2021;16(1):73–82. doi:10.1177/1747493019897841
9. Li Y, Zhang X, Sang H, et al. Urban-rural differences in risk factors for ischemic stroke in northern China. Medicine. 2019;98(21):e15782. doi:10.1097/md.0000000000015782
10. Ren Z, Fu X. Stroke risk factors in United States: an analysis of the 2013-2018 national health and nutrition examination survey. Int J Gen Med. 2021;14:6135–6147. doi:10.2147/ijgm.S327075
11. Ma LY, Wang XD, Liu S, et al. Prevalence and risk factors of stroke in a rural area of northern China: a 10-year comparative study. Aging Clin Exp Res. 2022;34(5):1055–1063. doi:10.1007/s40520-021-02028-1
12. Milionis HJ, Liberopoulos E, Goudevenos J, Bairaktari ET, Seferiadis K, Elisaf MS. Risk factors for first-ever acute ischemic non-embolic stroke in elderly individuals. Int J Cardiol. 2005;99(2):269–275. doi:10.1016/j.ijcard.2004.01.013
13. Xia X, Yue W, Chao B, et al. Prevalence and risk factors of stroke in the elderly in Northern China: data from the national stroke screening survey. J Neurol. 2019;266(6):1449–1458. doi:10.1007/s00415-019-09281-5
14. Satue E, Vila-Corcoles A, Ochoa-Gondar O, et al. Incidence and risk conditions of ischemic stroke in older adults. Acta Neurol Scand. 2016;134(4):250–257. doi:10.1111/ane.12535
15. Tu W, Wu J, Jian G, et al. Asymptomatic hyperuricemia and incident stroke in elderly Chinese patients without comorbidities. Eur J Clin Nutr. 2019;73(10):1392–1402. doi:10.1038/s41430-019-0405-1
16. Ganguly SS, Gujjar AR, Al Harthi H, et al. Risk factors for ischaemic stroke in an Omani community: a case-control study. Sultan Qaboos Univ Med J. 2021;21(4):585–590. doi:10.18295/squmj.4.2021.043
17. Li X, Wang Y, Xu J. Development of a machine learning-based risk prediction model for cerebral infarction and comparison with nomogram model. J Affect Disord. 2022;314:341–348. doi:10.1016/j.jad.2022.07.045
18. O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–775. doi:10.1016/s0140-6736(16)30506-2
19. Sarfo FS, Ovbiagele B, Akpa O, et al. Risk factor characterization of ischemic stroke subtypes among West Africans. Stroke. 2022;53(1):134–144. doi:10.1161/strokeaha.120.032072
20. ElSayed NA, Aleppo G, Aroda VR, et al. 2. classification and diagnosis of diabetes: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S19–s40. doi:10.2337/dc23-S002
21. Chen-Xu M, Yokose C, Rai SK, Pillinger MH, Choi HK. Contemporary prevalence of gout and hyperuricemia in the United States and decadal trends: the national health and nutrition examination survey, 2007-2016. Arthritis Rheumatol. 2019;71(6):991–999. doi:10.1002/art.40807
22. Ren Y, Shi J, Qiao Y, et al. Epidemiological status quo of hypertension in elderly population in Changchun, China: a cross-sectional study. BMJ Open. 2022;12(3):e053086. doi:10.1136/bmjopen-2021-053086
23. Okati-Aliabad H, Ansari-Moghaddam A, Kargar S, Mohammadi M. Prevalence of hypertension and pre-hypertension in the Middle East region: a systematic review & meta-analysis. J Hum Hypertens. 2022;36(9):794–804. doi:10.1038/s41371-021-00647-9
24. Libruder C, Ram A, Hershkovitz Y, et al. The contribution of potentially modifiable risk factors to acute ischemic stroke burden - comparing young and older adults. Prev Med. 2022;155:106933. doi:10.1016/j.ypmed.2021.106933
25. Alhazzani AA, Mahfouz AA, Abolyazid AY, Awadalla NJ. Risk factors of the first-time stroke in the Southwest of Saudi Arabia: a case-control study. Brain Sci. 2021;11(2):222. doi:10.3390/brainsci11020222
26. Jones RH, Beber SA, Adhiyaman A, et al. No association between growth hormone therapy and upper extremity physeal tension injuries: a matched case-control study. Clin Orthop Relat Res. 2025;483(3):527–532. doi:10.1097/CORR.0000000000003248
27. Wang C, Du Z, Ye N, et al. Hyperlipidemia and hypertension have synergistic interaction on ischemic stroke: insights from a general population survey in China. BMC Cardiovasc Disord. 2022;22(1):47. doi:10.1186/s12872-022-02491-2
28. Azam S, Peng C, Rosner BA, et al. Plasma C-peptide mammographic features and risk of breast cancer. NPJ Breast Cancer. 2024;10(1):91. doi:10.1038/s41523-024-00702-x
29. Liu L, Fan Y, Wang Z, et al. Disparity in risk factors of ischemic stroke in four coastal-area hospitals in China. Heliyon. 2024;10(2):e24745. doi:10.1016/j.heliyon.2024.e24745
30. You Y, Wang J, Teng W, Ma G, Liu P. Blood pressure and noncommunicable diseases in middle-aged and older adults in China. PLoS One. 2018;13(11):e0206635. doi:10.1371/journal.pone.0206635
31. Yi X, Luo H, Zhou J, et al. Prevalence of stroke and stroke related risk factors: a population based cross sectional survey in southwestern China. BMC Neurol. 2020;20(1):5. doi:10.1186/s12883-019-1592-z
32. Malek EG, Elbejjani M, Abbas R, Abed Al Ahad M, Isma’eel H, Makki A. TOAST classification and risk factors of ischemic stroke in Lebanon. Acta Neurol Scand. 2020;141(4):294–300. doi:10.1111/ane.13201
33. Sadeq A, Baraka MA, Hamrouni A, Elnour AA. Retrospective cohort study on risk factors for developing ischemic stroke. Pharm Pract. 2022;20(3):2682. doi:10.18549/PharmPract.2022.3.2682
34. Pastuszak Ż, Koźniewska E, Stępień A, Piusińska-Macoch A, Czernicki Z, Koszewski W. Importance rating of risk factors of ischemic stroke in patients over 85 years old in the Polish population. Neurol Neurochir Pol. 2018;52(1):88–93. doi:10.1016/j.pjnns.2017.11.007
35. Hipgrave DB, Chang S, Li X, Wu Y. Salt and sodium intake in China. JAMA. 2016;315(7):703–705. doi:10.1001/jama.2015.15816
36. Li W, Gu H, Teo KK, et al. Hypertension prevalence, awareness, treatment, and control in 115 rural and urban communities involving 47 000 people from China. J Hypertens. 2016;34(1):39–46. doi:10.1097/hjh.0000000000000745
37. Zhang FL, Guo ZN, Xing YQ, Wu YH, Liu HY, Yang Y. Hypertension prevalence, awareness, treatment, and control in northeast China: a population-based cross-sectional survey. J Hum Hypertens. 2017;32(1):54–65. doi:10.1038/s41371-017-0003-4
38. Chen X, Zhou L, Zhang Y, et al. Risk factors of stroke in Western and Asian countries: a systematic review and meta-analysis of prospective cohort studies. BMC Public Health. 2014;14(1):776. doi:10.1186/1471-2458-14-776
39. Jeong SM, Lee HR, Han K, et al. Association of change in alcohol consumption with risk of ischemic stroke. Stroke. 2022;53(8):2488–2496. doi:10.1161/strokeaha.121.037590
40. Jones SB, Loehr L, Avery CL, et al. Midlife alcohol consumption and the risk of stroke in the atherosclerosis risk in communities study. Stroke. 2015;46(11):3124–3130. doi:10.1161/strokeaha.115.010601
41. Larsson SC, Wallin A, Wolk A, Markus HS. Differing association of alcohol consumption with different stroke types: a systematic review and meta-analysis. BMC Med. 2016;14(1):178. doi:10.1186/s12916-016-0721-4
42. Kang DO, Lee DI, Roh SY, et al. Reduced alcohol consumption and major adverse cardiovascular events among individuals with previously high alcohol consumption. JAMA Network Open. 2024;7(3):e244013. doi:10.1001/jamanetworkopen.2024.4013
43. Gan Y, Feng J, Zhu Y, et al. Association between alcohol consumption and the risk of stroke in middle-aged and older adults in China. Drug Alcohol Depend. 2021;229(Pt B):109134. doi:10.1016/j.drugalcdep.2021.109134
44. Li Z, Bai Y, Guo X, Zheng L, Sun Y, Roselle AM. Alcohol consumption and cardiovascular diseases in rural China. Int J Cardiol. 2016;215:257–262. doi:10.1016/j.ijcard.2016.04.095
45. Wu X, Liu X, Liao W, et al. Prevalence and characteristics of alcohol consumption and risk of type 2 diabetes mellitus in rural China. BMC Public Health. 2021;21(1):1644. doi:10.1186/s12889-021-11681-0
46. Tang Z, Ding Y, Zhang W, et al. Epidemiological characteristics of alcohol-related liver disease in China: a systematic review and meta-analysis. BMC Public Health. 2023;23(1):1276. doi:10.1186/s12889-023-15645-4
47. Wang Q, Zhang Y, Wu C. Alcohol consumption and associated factors among middle-aged and older adults: results from China health and retirement longitudinal study. BMC Public Health. 2022;22(1):322. doi:10.1186/s12889-022-12718-8
48. Bryazka D, Reitsma MB, Griswold MG. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the global burden of disease study 2020. Lancet. 2022;400(10347):185–235. doi:10.1016/s0140-6736(22)00847-9
49. Wang R, Zhang P, Li Z, et al. The prevalence of pre-diabetes and diabetes and their associated factors in Northeast China: a cross-sectional study. Sci Rep. 2019;9(1):2513. doi:10.1038/s41598-019-39221-2
50. Hu G, Gu H, Jiang Y, et al. Revisiting the smoking paradox in acute ischemic stroke patients: findings from the Chinese stroke center alliance study. J Am Heart Assoc. 2023;12(16):e029963. doi:10.1161/jaha.123.029963
51. Azeez TA, Yaria J, Adetunji TA. Stroke and dyslipidaemia in Africa: a meta-analysis of case-control studies. J Thromb Thrombolysis. 2023;56(1):188–195. doi:10.1007/s11239-023-02823-9
52. Shiozawa M, Kaneko H, Itoh H, et al. Association of body mass index with ischemic and hemorrhagic stroke. Nutrients. 2021;13(7):2343. doi:10.3390/nu13072343
53. Jeong W, Joo JH, Kim H, Jang SI, Park EC. Association between statin adherence and the risk of stroke among South Korean adults with hyperlipidemia. Nutr, Metab Cardiovasc Dis. 2022;32(3):560–566. doi:10.1016/j.numecd.2021.12.010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Prospective Study of Stroke Characteristics, Risk Factors, and Mortality in a Tertiary Hospital of Northern Ethiopia
Gidey K, Hailu A
International Journal of General Medicine 2023, 16:5051-5061
Published Date: 3 November 2023
Exploration of the Shared Gene Signatures and Molecular Mechanisms Between Ischemic Stroke and Atherosclerosis
Ban R, Huo C, Wang J, Zhang G, Zhao X
International Journal of General Medicine 2024, 17:2223-2239
Published Date: 19 May 2024
Predicting Early Dysphagia in Acute Ischemic Stroke Using an Explainable Machine Learning Model
Li Y, Yu S, Yu X, Tian B, Tang J, Qu H, Zhang Y
International Journal of General Medicine 2025, 18:7341-7356
Published Date: 5 December 2025