")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Analysis of Closed Claims Among All Medical Specialties: Importance of Communication and Other Non-Clinical Contributing Factors
Authors Kusumoto F, Ross J , Wright D, Chazal RA , Anderson RE
Received 17 March 2023
Accepted for publication 24 October 2023
Published 29 February 2024 Volume 2024:17 Pages 411—422
DOI https://doi.org/10.2147/RMHP.S403710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Fred Kusumoto,1 Jacqueline Ross,2 Dan Wright,2 Richard A Chazal,3 Richard E Anderson2
1Heart Rhythm Service, Department of Cardiovascular Disease, Mayo Clinic, Jacksonville, FL, USA; 2The Doctors Company, Napa, CA, USA; 3Lee Health Heart and Vascular Institute, Fort Myers, FL, USA
Correspondence: Fred Kusumoto, Heart Rhythm Service, Department of Cardiovascular Disease, Mayo Clinic, 4500 San Pablo Ave, Jacksonville, FL, 32224, USA, Tel +1904 953-7277, Email [email protected]
Objective: Medical malpractice claims represent patient dissatisfaction of care delivered by their healthcare provider. Evaluation of contributing factors (CFs) associated with claims provides important information to optimize the patient–provider relationship.
Study Design: A total of 21,101 closed claims with 54,479 CFs (2.2 contributing factors per claim) from a large medical professional liability coverage provider were analyzed from 2010 to 2019.
Results: Four clinical CFs (technical performance, management of therapy, patient assessment, and patient factors) and four nonclinical CFs (communication between providers and patient, communication among providers, failure or delay in obtaining a consult, and insufficient documentation) were identified > 1,500 times. Nonclinical CFs increased as a percentage from 50% in the first part of the study period to 54% in the second part of the study period (p < 0.01), and were more frequent in cases associated with indemnity when compared to clinical CFs (Nonclinical: 57% vs 43%; p < 0.001). Poor communication as a CF increased steadily during the study period (3-year average; 2010– 2012: 777 CF/year vs 2017– 2019: 1207 CF/year; p < 0.001). In claims associated with high severity injury, poor communication among providers was more significant than poor communication between the provider and patient (63% vs 29%; p < 0.001), mainly due to failure to convey the severity of the patient’s condition. For non-surgical specialties except psychiatry, communication was the highest CF and the second or third CF for psychiatry or surgical specialties.
Discussion: Clinical and nonclinical CFs are equally important for malpractice claims. Communications issues are particularly important regardless of specialty. While focusing on clinical quality is important, implementing strategies that account for nonclinical issues, with a particular focus on communication, would have significant benefits particularly in an environment of increased consolidation of healthcare delivery systems.
Plain Language Summary: Nonclinical and clinical issues are equally common contributors underlying a malpractice claim, and nonclinical issues are more frequent in claims associated with indemnity.Communication-related (communication between the patient and the healthcare provider and communication among providers) contributing factors were the most observed nonclinical parameter and the incidence has steadily risen over the study decade.Current strategies in healthcare to improve communication have not been effective and developing systems and strategies that focus on communication and other nonclinical issues could significantly decrease future malpractice claims.
Keywords: closed claims, malpractice, professional liability, communication
Medical professional liability, more commonly referred to as medical malpractice has a significant impact on medicine.1–8 In one study from 1991 to 2005 of more than 40,000 physicians, the annual risk of a medical liability claim was 7.4% and the authors projected that 99% of physicians in high-risk specialties and 75% of physicians in low-risk specialties would face a malpractice claim by age 65 years.2 The absolute dollar contribution of malpractice to overall healthcare costs is low. However, claims represent a significant social cost and may be an important component for loss of trust between the patient and the medical system or healthcare provider and significant resources and time are necessary to close a claim (Pegalis and Bell, Choy, Beckman, Hickson 1994. In a United States based survey of patients, 21% said they directly experienced a medical error and 31% said they were involved in a “situation where an error occurred in someone else’s care”.7
The healthcare environment has changed dramatically with several overall trends including increased physician employment and team-based care delivery, larger and more diverse industries involved in healthcare, increased application of new technologies, and new financing strategies that incentivize care delivery in nontraditional settings and new organizational structures.9–11 These changes will have a greater impact on all aspects of medicine, including healthcare liability. Significant problems in healthcare liability that could arise from the evolving medical environment might include erosion of long-term stable relationships between an individual patient and care provider, poor communication within an organization or between different sites of care, and decreased institutional experience and expertise.
Methods
All closed claims from The Doctors Company (Napa, Ca) from 2010 to 2019 were included in the study and divided by specialty (Appendix Table 1). All claims were reviewed by specially trained clinical registered nurse analysts and aggregated into a database using the Comprehensive Risk Intelligence Tool (CRIT; CRICO Strategies, Cambridge, MA) structured taxonomy (Appendix Table 2). This evidence-based taxonomy identifies contributing factors that are classified into conceptual groupings, each with three different levels: category (a broad classification), subcategory, and detailed. The thirteen categories used are administrative, behavior, clinical environment, clinical judgment, communication, clinical systems, documentation, electronic health records, equipment, environmental, managed care, supervision, and technical skill. Within each of these broad categories of contributing factors, 46 specific subcategories have been identified. Subcategories were further classified as clinical factors if they involved the clinical skills of a healthcare provider or individual patient characteristics and included clinical assessment, patient condition, and technical skill, or nonclinical factors, if they pertained more to a system issue, such as communication, work conditions, and documentation (Appendix Table 2). A panel of 11 healthcare providers not involved in the study were used to define clinical vs nonclinical parameters. Any subcategory that did not receive more than 80% agreement was then discussed with final decision made by group consensus. Injury severity was also determined and calculated using the National Association of Injury Commissioners (NAIC) Injury Severity Scale and classified as low (NAIC Injury Scale 1–2), moderate (NAIC Injury Scale 3–5), or high (NAIC Injury Scale 6–9). All claims are also classified on whether an indemnity payment was provided. The database undergoes monthly internal quality reviews and an annual external audit by CRICO Strategies is also performed. To account for annual variability of closed claims, for temporal measures 3-year averages were used. Proportions between different groups were analyzed using a two-tailed z-test with a p value < 0.01 considered significant.
Results
Contributing Factors Associated with Claims
From 2010 to 2019, 21,201 closed claims were analyzed with a peak in total closed claims in 2014 but no significant temporal trend identified in claims associated with indemnity (Figures 1–3 Appendices). For all claims 54,479 contributing factors were identified (2.2 contributing factors per claim) with the distribution among the CRICO categories shown in Figure 1. Clinical Judgement and Technical skill were the largest single categories. However, other non-healthcare provider-related categories combined for the majority of contributing factors. Using the classification system developed by the study panel, 27,739 (51%) contributing factors were classified as nonclinical and 26,740 (49%) were classified as clinical. The most common specific contributing factors (>1500) are shown in Figure 2.
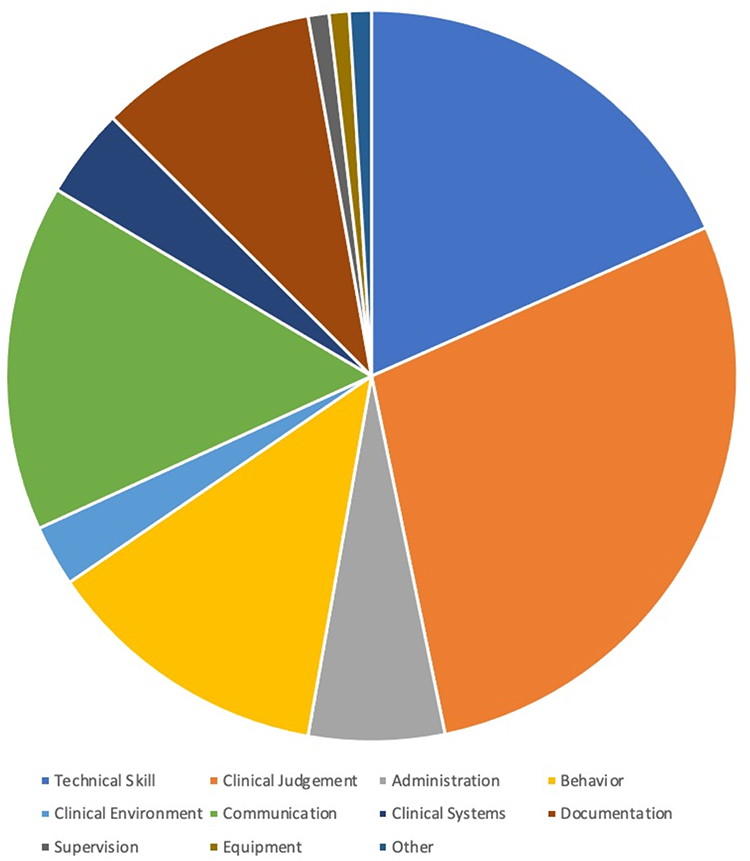 |
Figure 1 CRICO categories: Distribution of CRICO categories in the dataset. |
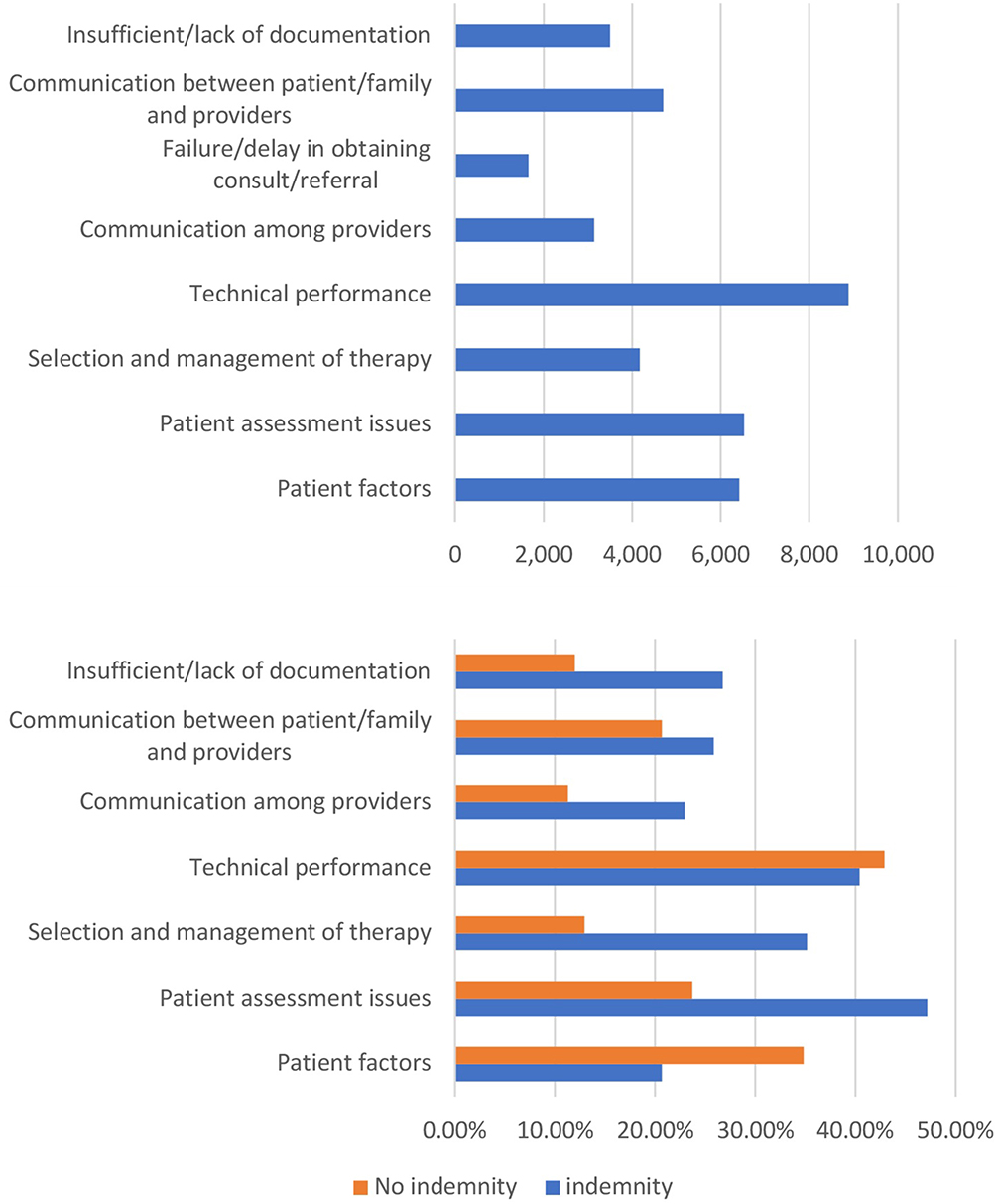 |
Figure 2 Contributing factors associated with closed claims (total and with and without indemnity) (Top) Individual contributing factors with a frequency >1500 over the 10-year study period grouped into nonclinical and clinical parameters. (Bottom) Individual contributing factors with a frequency >1500 over the 10-year study period grouped into nonclinical and clinical parameters further classified by whether the claim was associated with an indemnity payment. |
Clinical Contributing Factors
For those contributing factors identified >1500 times classified as clinical, technical performance was identified most frequently, followed by patient assessment issues and patient factors, and selection of therapy was identified the fewest number of times (Figure 2).
Nonclinical Contributing Factors
Nonclinical parameters were more heterogeneous, but documentation, delays in care, and communication between the provider and patient and among providers were most observed (Figure 2). Communication on expectations, inadequate informed consent, and poor rapport were the most important specific reasons identified for communication issues between the patient/family and provider (Figure 3). Failure to communicate the severity of a patient’s condition among providers accounted for the most common specific problem for communication among providers (p < 0.001). Other nonclinical factors not shown in the chart that were noted >1000 times included: staffing issues (1240), policy and protocol issues (1045), and patient monitoring (1441).
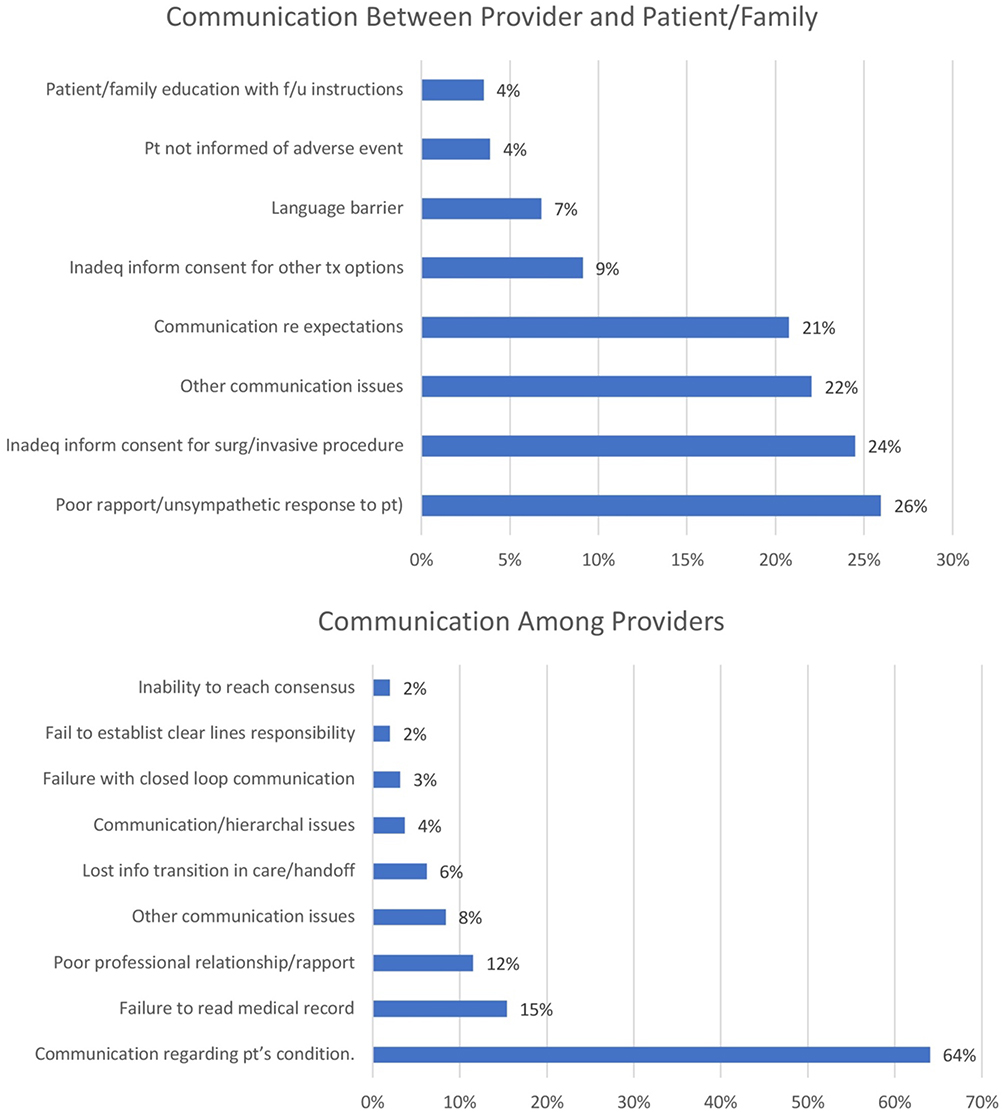 |
Figure 3 Specific communication problems (Top) Specific characteristics of communication problems between the patient/family and healthcare provider. (Bottom) Specific characteristics of communication problems among healthcare providers. |
Temporal Changes During the Study Period
For the six high frequency CRICO categories, technical skill, clinical environment, and clinical systems were observed at a relatively constant rate over the entire study period. Clinical judgement and documentation as contributing factors increased in the first part of the study period and then stabilized. Communication as contributing factor increased steadily during the study period due to increases in both communication between patient and provider and communication among providers (3 year average; 2010–2012: 777 CF/year vs 2017–2019: 1207 CF/year; p < 0.001), with a higher contribution by communication between patient and provider (Figure 4). Although overall counts are low (882), shift and off-hours conditions has increased dramatically as a contributing factor from an average of 31/year for 2010–2012 to 167/year for 2017–2019 (p < 0.001) (Figure 2 Appendix).
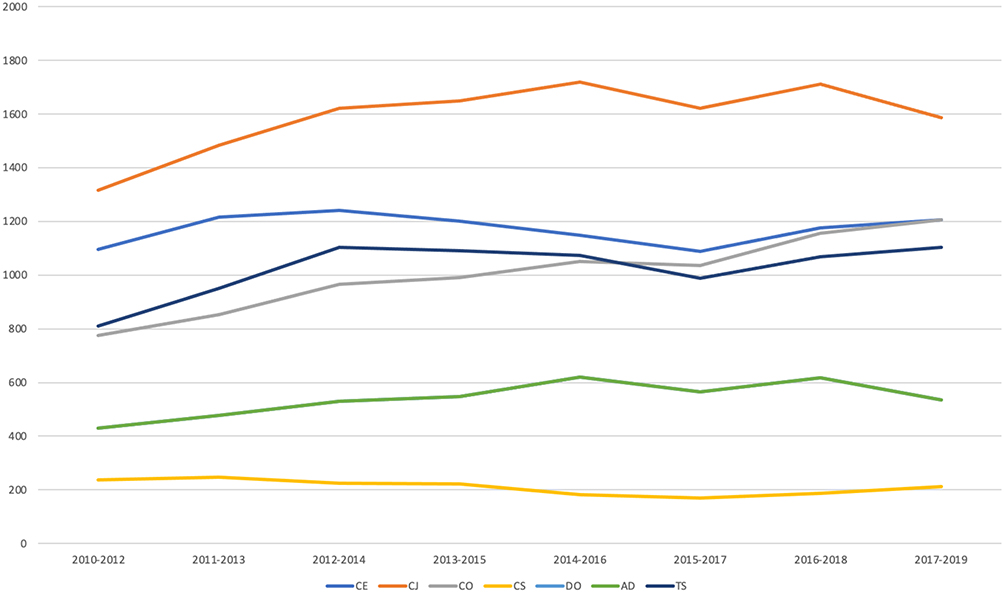 |
Figure 4 Temporal trends of contributing factors during the study period (Top) Temporal trends for the five largest CRICO categories during the study period. Running three-year averages were used to minimize the impact of annual variability. Communication was the only category of contributing factors that increased throughout the study period. (Bottom) Communication between the patient and provider and among providers both increased as contributing factors throughout the study period. |
Contributing Factors Based on Indemnity
Of all claims, 14,658 (69%) claims were not associated with indemnity and 31,624 contributing factors were identified (2.2 contributing factors per claim). For the remaining 6543 (31%) claims associated with indemnity payment 22,855 contributing factors were identified (2.8 contributing factors per claim) with 13,082 (57%) classified as nonclinical and 9773 (43%) classified as clinical. Nonclinical parameters were more frequent than clinical parameters in claims associated with indemnity payment when compared to all claims (Claims with indemnity: Nonclinical: 57% vs Clinical: 43%; All claims: Nonclinical: 51% vs Clinical: 49%; p < 0.001). The bottom panel in Figure 3 shows the commonly observed individual contributing factors separated by whether a claim was associated with an indemnity payment. One clinical parameter (patient factors) was less likely to be associated with indemnity payment. Two clinical parameters (selection and management of therapy (p < 0.001), patient assessment issues (p < 0.01)) and two nonclinical parameters (insufficient/lack of documentation (p < 0.01), communication among providers (p < 0.01)) were more likely to be associated with an indemnity payment. Communication issues were particularly important in those claims with high injury severity. For high injury severity, communication among providers was a contributing factor in 63% of claims with failure to convey the severity of the patient’s condition by far the largest specific problem (Figure 5).
 |
Figure 5 Injury severity and communication. (Top) Communication with other providers or with patients/family stratified by injury severity. (Bottom) Specific communication problems identified as contributing factors in closed claims analysis. Communication among providers was a contributing factor in high injury claims and mainly involved failure to convey the severity of a patient’s condition. |
Specialty Specific Differences
The largest number of claims were in the surgery specialties and the fewest in pediatrics (Figure 3 Appendix). When comparing surgical vs non surgical specialties collectively, technical performance was the most common contributing factor for surgical specialties and as expected was significantly more common when compared to the nonsurgical specialties (p < 0.0001) (Figure 6). Conversely, patient assessment (<0.0001), failure or delay in obtaining a consult (<0.001), and communication among providers (<0.001) were significantly more common contributing factors in nonsurgical specialties (Figure 6).
 |
Figure 6 Differences between surgical and nonsurgical specialties. Technical performance was a more common contributing factor for surgical specialties (p < 0.0001). When compared to surgical specialties, for nonsurgical specialties, patient assessment (p < 0.0001), failure/delay in obtaining a consult (p < 0.001), and communication among providers (p<0.01) were significantly more common. |
When surgical specialties were evaluated individually, technical performance was the most common contributing factor regardless of the surgical specialty. Patient factors were the next most observed contributing factor for orthopedics and other surgical specialties (surgical subspecialties other than neurosurgery and orthopedics), and collective communication issues were either the second or third most common contributing factor for all surgical specialties. Communication issues among providers accounted for 57% of communication problems for anesthesia, and 40–50% for general surgery (46%), obstetrics/gynecology (46%), and neurosurgery (42%).
For the individual nonsurgical specialties, the primary contributing factor was more heterogeneous: patient factors in psychiatry, patient assessment in radiology, and communication for the others. Communication among providers accounted for >60% of communication issues for emergency medicine, pathology, and radiology.
No specialty specific temporal trends were identified during the study period.
Discussion
Summary of Key Findings
Although older studies have reported a decrease in malpractice claims when the early 2000s are compared to the 1990’s, review of this dataset found that total closed claims and claims associated with indemnity have remained generally constant over the past decade despite a general decrease in the trend of adverse event rates in hospitalized patients.2,3,12 In the current study, nonclinical parameters are observed as commonly as clinical parameters. The contributing factors classified as nonclinical parameters are heterogeneous but documentation, communication between the patient and provider and communication among providers were observed most frequently. When considered collectively, communication is the most important nonclinical contributing factor and is more common in claims associated with indemnity, particularly in high injury claims. Communication issues are an important contributing factor for medical liability claims in all medical specialties and the most common contributing factor in nonsurgical specialties other than psychiatry.
Clinical Vs Nonclinical Factors
Clinical parameters such as selection and management of therapies, patient assessment issues, and patient factors are important contributing factors for medical professional liability claims and technical performance is particularly important in surgical specialties. Prior studies have focused on clinical factors such as diagnostic errors and technical performance of a procedure.3,4 However, this analysis demonstrates that nonclinical factors are as common as clinical factors in all medical specialties and although the nonclinical factors are heterogeneous and require a multipronged approach, efforts for healthcare providers and systems to design processes that systematically address nonclinical issues will be critical in the evolving healthcare environment. This issue may become even more important given the consolidation of health systems over the past decade and the dramatic increase in the employed healthcare providers model (Neprash, Mulstein).
Communication
Prior studies have noted the importance of communication between the patient and provider as an underlying factor for a malpractice claim.13–16 For this reason, several strategies have been suggested or implemented to improve communication between patient and provider with mixed results.15–18 Our analysis confirms that communication between the patient and provider is critical and in addition, the importance of communication is generalizable to all medical specialties. However, despite profession-wide recognition of this issue, communication has unfortunately continued to increase as a contributing factor for malpractice claims over the past decade. The study also provides additional detail with lack of rapport, communication about expectations, and inadequate consent as the primary specific communication problems between patient and provider. Many possible reasons for this trend exist including erosion in individual relationships between patient and healthcare provider due to financial pressure, less time spent together, and increased fractionation of the medical system. Communication problems may accelerate in new care models with intervention. While technology has provided new ways for patients to communicate with healthcare providers, it is unclear whether new communication strategies will establish necessary trust. While all acknowledge the importance of trust between the patient and provider, trust has multiple components and difficult to measure.19 However, most studies have shown that the foundation for developing trust is good communication between the patient and healthcare provider.20
Our study also found that communication among providers, particularly for nonsurgical specialties, is an important component of communication failures and is as common as between patient and provider with failure to communicate on the severity of the patient’s condition the overwhelming specific problem. This issue is even more common in those claims associated with indemnity, particularly in claims associated with high injury. Communication among providers was a particularly important contributing factor in emergency medicine, pathology, and radiology.
Electronic communication models may facilitate communication among providers in systems which could be particularly relevant as delivery of more complex care spreads to more areas that are physically separated. Studies have provided mixed, though generally positive results on the use of digital strategies to facilitate communication between healthcare facilities.21,22 The electronic health records could also be used as an auditing tool to confirm and document communication, whether between the patient and provider, among providers, or between facilities.23
Communication among providers increased as a contributing factor over the study period despite government mandates that have led to widespread adoption of the electronic health record and the emergence of sophisticated communication technologies. This finding could be due to fractionation in the medical environment with no widely accepted system or standard. Improved communication among providers could be facilitated by multiple strategies. For example, while medical school curriculum usually includes education on communication between the patient and provider, interprofessional communication training could also systematically be implemented. In addition, an important part of leadership training is developing communication skills, and institutions or state medical boards could require this type of training as part of obtaining privileging or licensing. Finally, wide adoption of a standardized communication strategy could be useful. Within the hospital, using a SBAR (Situation, Background, Assessment, Recommendations) approach may be beneficial for inpatient hand-offs, though the data has been mixed particularly when extended from the classroom to the clinical setting.24–26 Regardless, a structured communication strategy that focused on conveying the severity of the patient’s condition could be beneficial given the results of the present analysis. Finally, communication among providers including failure/delay in obtaining a consult was particularly important for nonsurgical specialties, suggesting that designing strategies that facilitate communication with surgical specialties would be particularly beneficial.
Claims not associated with indemnity more commonly had patient associated contributing factors and technical performance contributing factors were equally prevalent in claims without indemnity and claims with indemnity. In contrast, patient assessment issues, lack of documentation, and communication issues, particularly among providers were more common in claims associated with indemnity. It appears these contributing factors were less defensible or tolerated and blame ultimately placed on the healthcare provider.
Implications and Policy Recommendations
Postgraduate education for healthcare providers has historically focused on the clinical aspects of medicine. While these educational opportunities will have an impact on clinical parameters such clinical judgement and technical expertise, they are not designed to improve patient factors or nonclinical parameters. Reducing intrinsic patient factors will require a nationwide commitment to public health initiatives. Strategies that address nonclinical factors could have important benefits. For example, documentation has long been recognized as a contributing factor in medical malpractice claims and is valuable with increased transparency of electronic health records.27 Although inadequate documentation continues to be a contributing factor, its incidence appeared to plateau over the last half of the study period. However, increasing demands on healthcare providers may lead to erosion of any gains that prior programs designed to improve documentation have made. Artificial intelligence using large language models may become a tool for synthesizing conversation between a patient and provider into a comprehensive clinical note that could also confirm appropriate documentation but at this point widespread application will require further study and potential regulatory oversight.28–30
As the medical environment changes rapidly and patients begin receiving more care via new methods (eg, telemedicine,) and receive medical care in a team-based setting, nonclinical factors may become even more important as contributing factors leading to patient dissatisfaction and a resulting claim.1,9,10,31 As care is delivered in different settings among multiple providers-for example ambulatory surgical centers or the hospital at home,11,32 developing effective communication strategies among all stakeholders will be critical. In addition, although the absolute numbers are relatively low, shift and off hours problems increased dramatically over the study period and may become even more important in the aftermath of the COVID-19 pandemic and continued financial pressures on medical providers and facilities.
Limitations
One limitation of this study is that only closed claims were evaluated, and it should be emphasized that there is no evidence to suggest that a claim is an indicator of healthcare delivery that does not reach the medical standard of care.5 Nonetheless, a malpractice claim does suggest that the relationship between the patient and the healthcare provider has been compromised. The focus of this study is to identify contributing factors that lead to loss of trust. Although defining clinical vs nonclinical parameters will vary based on individual interpretation, the data show the importance of nonclinical parameters as contributing factors to loss of trust. This review is limited to closed claims data from one medical professional liability company; however, The Doctor’s Company is one of the two largest medical malpractice carriers in the United States and cover healthcare providers from the entire range of medical specialties and different practice structures. Although, large databases such as The National Practice Data Bank provide a comprehensive list of claims against healthcare providers, they have limited information on the underlying cause other than the primary allegation.33
Further Research and Conclusions
The current study identifies important contributing factors associated with medical professional liability. While clinical parameters such as patient characteristics, judgement on therapy choice, and skilled technical performance are important, nonclinical parameters are just as common. Of nonclinical parameters, communication between patient and provider and among providers are the most frequently observed, particularly in claims associated with high injury. Unfortunately, communication issues have continued to steadily increase despite recognition of this problem decades ago. Specifically, when communicating with patients, healthcare providers should focus on developing an environment of trust and rapport, ensuring appropriate discussion of treatment options and obtaining consent, and providing clear expectations. Overall health policies at government, state, facility, and individual provider levels must focus on nonclinical parameters, particularly on developing strategies that will facilitate and incentivize communication among providers for best patient care.
Data Sharing Statement
The data that support the findings of this study are available from The Doctors Company, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of The Doctors Company.
Ethical Statement
The study was reviewed by the Mayo Clinic Institutional Review Board and in accordance with the Code of Federal Regulations, 45 CFR 46.102, noted that the research does not require IRB review nor that patient consent was required for this study. Permission was granted by The Doctors Company to access and publish this data. All guidelines from the Declaration of Helsinki were followed. All authors agree on the content of the manuscript.
Consent for Publication
Patient consent for publication not applicable as the data does not include access or publication of individual patient information. This was confirmed by the Institutional Review Board.
Acknowledgement
The authors would like to acknowledge the support provided by Brenda Hindle MS, MBA and Laura Kline MBA for this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any agency in the public, commercial or not for profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Austin C, Kusumoto F. Updates in medical professional liability: a primer for electrophysiologists. J Interv Card Electrophysiol. 2019;56(2):151–158. doi:10.1007/s10840-018-0453-9
2. Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011;365(7):629–636. doi:10.1056/NEJMsa1012370
3. Mello MM, Chandra A, Gawande AA, Studdert DM. National costs of the medical liability system. Health Aff. 2010;29(9):1569–1577. doi:10.1377/hlthaff.2009.0807
4. Seabury S, Chandra A, Lakdawalla D, Jena AB. Defense costs of medical malpractice claims. N Engl J Med. 2012;366(14):1354–1356. doi:10.1056/NEJMc1114805
5. Jena AB, Schoemaker L, Bhattacharya J, Seabury SA. Physician spending and subsequent risk of malpractice claims: observational study. BMJ. 2015;4:351.
6. Carrier ER, Reschovsky JD, Katz DA, Mello MM. High physician concern about malpractice risk predicts more aggressive diagnostic testing in office-based practice. Health Aff. 2013;32(8):1383–1391. doi:10.1377/hlthaff.2013.0233
7. NORC at the University of Chicago and IHI/NPSF Lucian Leape Institute. Americans’ Experiences with Medical Errors and Views on Patient Safety. Cambridge, MA: Institute for Healthcare Improvement and NORC at the University of Chicago; 2017.
8. Jena AB, Chandra A, Lakdawalla D, Seabury S. Outcomes of medical malpractice litigation against US physicians. Arch Intern Med. 2012;172(11):892–894. doi:10.1001/archinternmed.2012.1416
9. Casale PN, Perez C, Hagan EP, Roiland RA, Saunders RS. Aligning care and payment for chronic cardiovascular conditions. J Am Coll Cardiol. 2021;78(23):2377–2381. doi:10.1016/j.jacc.2021.09.1368
10. Kusumoto FM, Hao SC, Slotwiner DJ, et al. Arrhythmia care in a value-based environment: past, present, and future: developed and endorsed by the Heart Rhythm Society (HRS). Heart Rhythm. 2018;15(2):e5–e15. doi:10.1016/j.hrthm.2017.10.041
11. Maniaci MJ, Maita K, Torres-Guzman RA, et al. Provider evaluation of a novel virtual hybrid hospital at home model. Int J Gen Med. 2022;15:1909–1918. doi:10.2147/IJGM.S354101
12. Eldridge N, Wang Y, Metersky M, et al. Trends in adverse event rates in hospitalized patients, 2010–2019. JAMA. 2022;328(2):173–183. doi:10.1001/jama.2022.9600
13. Neprash HT, Chernew ME, Hicks AL, et al. Association of financial integration between physicians and hospitals with commercial health care prices. JAMA Intern Med. 2015;175(12):1932–1939. doi:10.1001/jamainternmed.2015.4610
14. Muhlestein DB, Smith NJ. Physician consolidation: rapid movement from small to large group practices, 2013–15. Health Aff. 2016;35(9):1638–1642. doi:10.1377/hlthaff.2016.0130
15. Kachalia A, Sands K, Niel MV, et al. Effects of a communication-and-resolution program on hospitals’ malpractice claims and costs. Health Aff. 2018;37(11):1836–1844. doi:10.1377/hlthaff.2018.0720
16. Klitzman R. Improving education on doctor-patient relationships and communication: lessons from doctors who become patients. Acad Med. 2006;81(5):447–453. doi:10.1097/01.ACM.0000222271.52588.01
17. Cole SA. Reducing malpractice risk through more effective communication. Am J Manag Care. 1997;3(4):649–653.
18. Barrier PA, Li JT, Jensen NM. Two words to improve physician-patient communication: what else? Mayo Clin Proc. 2003;78(2):211–214. doi:10.4065/78.2.211
19. Merenstein Z, Shuemaker JC, Phillips RL. Measuring Trust in Primary Care. Milbank Q. 2023;101(3):841–880. doi:10.1111/1468-0009.12654
20. Serhan O, Moise A, Guadagno E, Issa AM, Poenaru D. Exploring trust development in families of children towards surgical and emergency care providers: a scoping review of the literature. J Pediatr Surg. 2023;58(5):871–878. doi:10.1016/j.jpedsurg.2023.01.022
21. Avoka CK, McArthur E, Banke-Thomas A. Interventions to improve obstetric emergency referral decision making, communication and feedback between health facilities in sub-Saharan Africa: a systematic review. Trop Med Int Health. 2022;27(5):494–509. doi:10.1111/tmi.13747
22. Danhausen K, Diaz HL, McCain MA, McGinigle M. Strengthening interprofessional collaboration to improve transfers between a freestanding birth center and an academic medical center. J Midwifery Womens Health. 2022;67(6):753–758. doi:10.1111/jmwh.13437
23. Huilgol YS, Adler-Milstein J, Ivey SL, Hong JC. Opportunities to use electronic health record audit logs to improve cancer care. Cancer Med. 2022;11(17):3296–3303. doi:10.1002/cam4.4690
24. Coolen E, Engbers R, Draaisma J, Heinen M, Fluit C. The use of SBAR as a structured communication tool in the pediatric non-acute care setting: bridge or barrier for interprofessional collaboration? J Interprof Care. 2020;15:1–10. doi:10.1080/13561820.2020.1816936
25. Lo L, Rotteau L, Shojania K. Can SBAR be implemented with high fidelity and does it improve communication between healthcare workers? A systematic review. BMJ Open. 2021;11(12):e055247. doi:10.1136/bmjopen-2021-055247
26. Khazen M, Mirica M, Carlile N, Groisser A, Schiff GD. Developing a Framework and electronic tool for communicating diagnostic uncertainty in primary care: a qualitative study. JAMA Network Open. 2023;6(3):e232218. doi:10.1001/jamanetworkopen.2023.2218
27. Greenlaw J. Documentation of patient care: an often-underestimated responsibility. Law Med Health Care. 1982;10(4):172–174. doi:10.1111/j.1748-720X.1982.tb01708.x
28. Meskó B, Topol EJ. The imperative for regulatory oversight of large language models (or generative AI) in healthcare. NPJ Digit Med. 2023;6(1):120. doi:10.1038/s41746-023-00873-0
29. Falcetta FS, de Almeida FK, Lemos JCS, Goldim JR, da Costa CA. Automatic documentation of professional health interactions: a systematic review. Artif Intell Med. 2023;137:102487. doi:10.1016/j.artmed.2023.102487
30. Clough RA, Sparkes WA, Clough OT, Sykes JT, Steventon AT, King K. Transforming healthcare documentation: harnessing the potential of AI to generate discharge summaries. BJGP Open. 2023;1:2.
31. Zaki MM, Jena AB, Chandra A. Supporting value-based health care - aligning financial and legal accountability. N Engl J Med. 2021;385(11):965–967. doi:10.1056/NEJMp2105625
32. Ranum D, Beverly A, Shapiro FE, Urman RD. Leading causes of anesthesia-related liability claims in ambulatory surgery centers. J Patient Saf. 2021;17(7):513–521. doi:10.1097/PTS.0000000000000431
33. Wermuth HR, Sergent SR. The national practitioner data bank. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.