Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
An Online Survey About Electroconvulsive Therapy in Japan During the COVID-19 Pandemic: Comparison of Early and Recent Stages
Authors Hirata R ![]() , Kawashima H
, Kawashima H ![]() , Tsuboi T
, Tsuboi T ![]() , Wada K, Takebayashi M
, Wada K, Takebayashi M ![]() , Suwa T
, Suwa T
Received 10 March 2022
Accepted for publication 26 May 2022
Published 28 June 2022 Volume 2022:18 Pages 1277—1285
DOI https://doi.org/10.2147/NDT.S365417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Taro Kishi
Risa Hirata,1 Hirotsugu Kawashima,1,5 Takashi Tsuboi,2,5 Ken Wada,3,5 Minoru Takebayashi,4,5 Taro Suwa1,5
1Department of Psychiatry, Kyoto University Hospital, Kyoto, Japan; 2Department of Neuropsychiatry, Kyorin University School of Medicine, Tokyo, Japan; 3Department of Psychiatry, Hiroshima Citizens Hospital, Hiroshima City Hospital Organization, Hiroshima, Japan; 4Department of Neuropsychiatry, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; 5ECT Committee, Japanese Society of General Hospital Psychiatry (JSGHP), Tokyo, Japan
Correspondence: Taro Suwa, Department of Psychiatry, Kyoto University Hospital, 54, Shogoin Kawahara-cho, Sakyo-ku, Kyoto-shi, Kyoto, Japan, Tel +81-75-751-3386, Fax +81-75-751-3246, Email [email protected]
Purpose: To provide an overview of how electroconvulsive therapy (ECT) practice in Japan has changed as the coronavirus disease 2019 (COVID-19) pandemic continues.
Patients and Methods: We surveyed healthcare institutions, primarily university and general hospitals, regarding changes in the number of patients undergoing ECT and infection control measures in the early (August 2020) and recent (August 2021) stages of the COVID-19 pandemic. Data for the early and recent stages were also compared between urban and non-urban areas.
Results: Among 32 facilities, the number of patients undergoing ECT decreased in 11 facilities (34.4%) from April 2020 to March 2021 compared with the previous year, whereas the number increased in 12 (37.5%) from April to June 2021 compared with the previous year. As of August 2021, some facilities had ongoing restrictions. Compared with non-urban facilities, the number of patients undergoing ECT decreased more in urban facilities, which also had more ECT restrictions. Maintenance ECT was used at the same rate as before the pandemic for 23 (82.1%) of 28 institutions. Regarding infection control measures, many facilities considered polymerase chain reaction testing before ECT and required all staff to wear surgical masks and eye shields during ECT.
Conclusion: The COVID-19 pandemic in Japan greatly affected the use of ECT in 2020; however, by the summer of 2021, infection control measures were relatively well established, the number of ECT cases stabilized and increased, and the decision to use ECT was again possible.
Keywords: electroconvulsive therapy, coronavirus disease 2019, pandemic, personal protective equipment, clinical decision making
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has had a substantial impact on medical practice,1,2 and the use of electroconvulsive therapy (ECT) as a general anesthetic procedure has been no exception. From the outset of the global pandemic, concerns have arisen worldwide about the disadvantages for patients who needed but were not able to receive ECT. In several countries with severe outbreaks of COVID-19, the number of ECT cases declined in 2020, and some facilities stopped ECT completely.3,4 In April 2020, a group of psychiatrists in the United States appealed vigorously to the medical community to support that ECT is an essential treatment modality, even with limited medical resources, and that some patients can only be effectively treated by ECT.5 Specialists in ECT then developed recommendations for the criteria to guide ECT introduction and infection control measures during the COVID-19 pandemic.6,7
In Japan, the total number of COVID-19 deaths was lower than that in most other countries, and the government did not enforce strict lockdowns throughout the pandemic.8,9 However, large increases in the number of COVID-19 infections occurred in five waves until October 2021 (Figure 1), which challenged the country’s ability to maintain essential medical services, including ECT. As in other countries, the rapid spread of COVID-19 infection caused confusion in clinical practice. The Japanese Society of General Hospital Psychiatry made its own recommendations regarding ECT during the pandemic,10 referring to the criteria proposed by ECT specialists as previously noted, and each facility decided on its criteria for introducing ECT and infection protection measures based on these domestic and international recommendations. However, the number of ECT cases and the degree of infection control required varied based on differences in infection status in different regions throughout Japan and at different time points throughout the pandemic, resulting in a wide range of approaches to the issue.
 |
Figure 1 Number of new positive coronavirus disease 2019 (COVID-19) cases for patients hospitalized in Japan (based on the website of the Ministry of Health, Labour and Welfare, “outbreaks in Japan, etc.” https://www.mhlw.go.jp/stf/covid-19/kokunainohasseijoukyou.html, accessed December 14, 2021). The first survey was conducted in August 2020 and the second survey in August 2021. The number of electroconvulsive therapy (ECT) cases from April to June 2020 was compared with that from April to June 2021, which approximately corresponds to the first and fourth waves, respectively, of the COVID-19 pandemic. |
ECT is widely used in Japan as well as other countries, and the number of ECTs being administered is increasing, with about 96,000 ECTs (0.76 per 1000 population) performed in 2019.11 The estimated number of ETCs performed in Canada is approximately 67,000 (2.11–2.13 per 1000 population). To the best of our knowledge, to date no studies have investigated how ECT practice in Japan has changed in response to the COVID-19 pandemic, the degree to which the impact of COVID-19 on ECT practices varied by region, and how the infection control measures of each facility changed in response to shifts in infection during the pandemic. Our study describes how facilities offering ECT have struggled during the COVID-19 pandemic in Japan. We surveyed healthcare institutions, primarily university and general hospitals, regarding the changes in the numbers of ECT cases and in their decisions related to ECT in each facility throughout the pandemic, from the first wave in April 2020, through the fourth wave in April–June 2021, to the fifth wave in August 2021. Based on these survey results, we discuss the best way to deliver the necessary treatment to patients who require ECT with appropriate protective measures and with an awareness of a next wave of pandemic in the future.
Materials and Methods
Survey Content
Two surveys were administered for this study. In the first survey, in August 2020, we used a mainly selective and partly descriptive questionnaire using Google forms12,13 (see Supplemental Digital Content 1). The questions were related to: 1) ECT delivery before the spread of COVID-19 infection; 2) protection measures for COVID infection for low- and high-risk cases; and 3) ECT delivery during COVID-19 pandemic. In these questions, the criteria for determining whether each case was at high risk for infection were determined by each facility. In the second survey conducted in August 2021, new questions were added, focusing on the changes in the situation after the first survey. To understand the changes between the early and recent stages of the pandemic, the numbers of patients who underwent ECT from April 2020 to March 2021 (during the pandemic) and from April 2019 to March 2020 (before the pandemic) were compared. Similarly, the number of patients undergoing ECT from April to June 2020 was compared with the number from April to June 2021.
Participants
The participants were ECT training facilities accredited by the Japanese Society of General Hospital Psychiatry (JSGHP) and facilities belonging to the members of the JSGHP ECT Committee. In both the first and second surveys, university and general hospitals accounted for more than 90% of the respondents. Of the 60 facilities contacted for the first survey, responses were collected from 46 facilities, of which 28 were university hospitals, 15 were general hospitals with beds, 2 were psychiatric hospitals, and 1 was a general hospital without beds. Out of the 61 facilities contacted for the second survey, responses were collected from 32 facilities, of which 21 were university hospitals, 9 were general hospitals with beds, 1 was a psychiatric hospital, and 1 was a general hospital without beds. A total of 28 facilities, comprising 20 university hospitals, 7 general hospitals with beds, and 1 general hospital without beds, responded to both the first and second surveys.
In addition, we compared the ECT cases throughout the pandemic waves in urban areas, where the impact of the pandemic was significant, with other non-urban areas. Facilities in urban areas were those located in the eight prefectures (Tokyo, Osaka, Kanagawa, Saitama, Aichi, Chiba, Hyogo, and Fukuoka) with more than 70,000 infected people as of December 13, 2021.13
Ethical Approval
This study has been granted an exemption by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine, and was conducted in compliance with the ethical standards set forth in the 1964 Declaration of Helsinki and its subsequent revisions.
Results
Change in the Number of Patients Undergoing ECT
Changes in the number of patients undergoing ECT throughout the COVID-19 pandemic are shown in Figure 2. The number of patients undergoing ECT decreased in 34.4% of facilities from April 2020 to March 2021 compared with the number from April 2019 to March 2020, whereas the number of patients undergoing ECT increased in 37.5% facilities from April to June 2021 compared with the number from April to June 2020. Urban areas had more facilities with a decrease in the number of patients between 2019 and 2020 than non-urban areas, whereas non-urban areas had more facilities with an increase between 2020 and 2021 than urban areas.
 |
Figure 2 Change in the number of electroconvulsive therapy (ECT) cases. The number of ECT cases was compared from April 2020 to March 2021 (during the pandemic) with that from April 2019 to March 2020 (before the pandemic). Similarly, the number of ECT cases from April to June 2020 (the early stage) was compared with that from April to June 2021 (the recent stage). |
In terms of the types of hospital, of the 21 university hospitals, the number of patients undergoing ECT decreased in 10 facilities (47.6%) from April 2020 to March 2021 compared with those from April 2019 to March 2020, whereas the number of patients undergoing ECT decreased in 8 facilities (38.1%) from April to June 2021 compared with those from April to June 2020. Of the 10 general hospitals, the number of patients undergoing ECT decreased in 2 facilities (20.0%) from April 2020 to March 2021 compared with those from April 2019 to March 2020, whereas the number of patients undergoing ECT decreased in 2 facilities (20.0%) from April to June 2021 compared with the number from April to June 2020. Trends in psychiatric hospitals could not be ascertained because only 1 facility responded.
In terms of ECT restrictions, 20 facilities (62.5%) had never restricted ECT; 12 (37.5%) had temporary restrictions, and 3 (9.4%) had ongoing restrictions. Comparison between urban and non-urban areas showed that 9 (64.3%) in urban areas were temporarily restricted versus 3 (16.7%) in non-urban areas. As shown in Table 1, in August 2021 there were no longer any facilities that did not offer ECT to patients with a low risk of infection, and there was a slight increase in the number of facilities offering ECT to patients with a high risk of infection. Regarding the change in the decision to use ECT, in August 2020, 13 facilities (28.2%) used ECT only in severe patients requiring this treatment, whereas 4 (12.6%) did so in August 2021. Regarding the change in maintenance of patients undergoing ECT in the first wave of the pandemic in April 2020, the number of patients remained constant in 28 facilities (75.7%) and decreased in 7 (18.9%), whereas therapy was no longer offered in 2 facilities (5.4%). In the fourth wave in April–June 2021, the number of patients undergoing ECT remained constant in 23 facilities (82.1%) and decreased in 3 facilities (10.7%), whereas therapy was no longer offered in 2 facilities (7.1%).
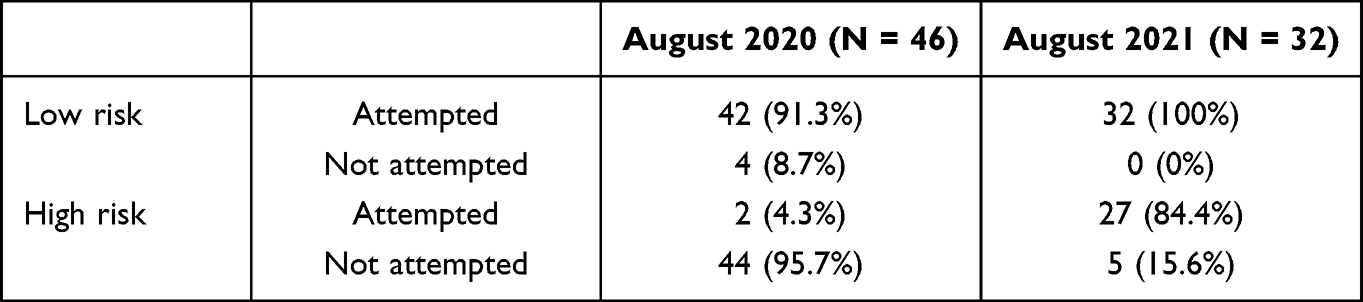 |
Table 1 Administration of Electroconvulsive Therapy in Cases with Low or High Risk for Coronavirus Disease 2019 Infection |
Infection Control Measures
At the time of the second survey in August 2021, all facilities had established infection control standards, and 28 facilities (87.5%) had hospital-wide standards. To develop infection control standards, one facility referred to the “Guide to the Treatment of New Coronavirus Infections, COVID-19” that was prepared by the Ministry of Health, Labor and Welfare and another referred to the “Use of Modified Electroconvulsive Therapy During the COVID-19 Pandemic” by the JSGHP ECT Committee.
Table 2 shows the infection control measures used by psychiatrists during administration of ECT in low-risk patients. An increased use of eye shields was noted in 2021 compared with 2020. The most common type of equipment used was a combination of surgical masks (non-N95 masks) and eye shields. The equipment used by anesthesiologists and other medical staff was similar to that of the psychiatrists (see Supplemental Digital Content 2). In addition, most respondents reported that their patients undergoing ECT wore a surgical mask to protect them from infection. Also mentioned were the infection control approaches of “covering the upper part of the body with plastic” and “using a head chamber.” As shown in Table 3, the other most common infection prevention measures were “polymerase chain reaction (PCR) testing” and “limiting the number of medical staff” during ECT administration.
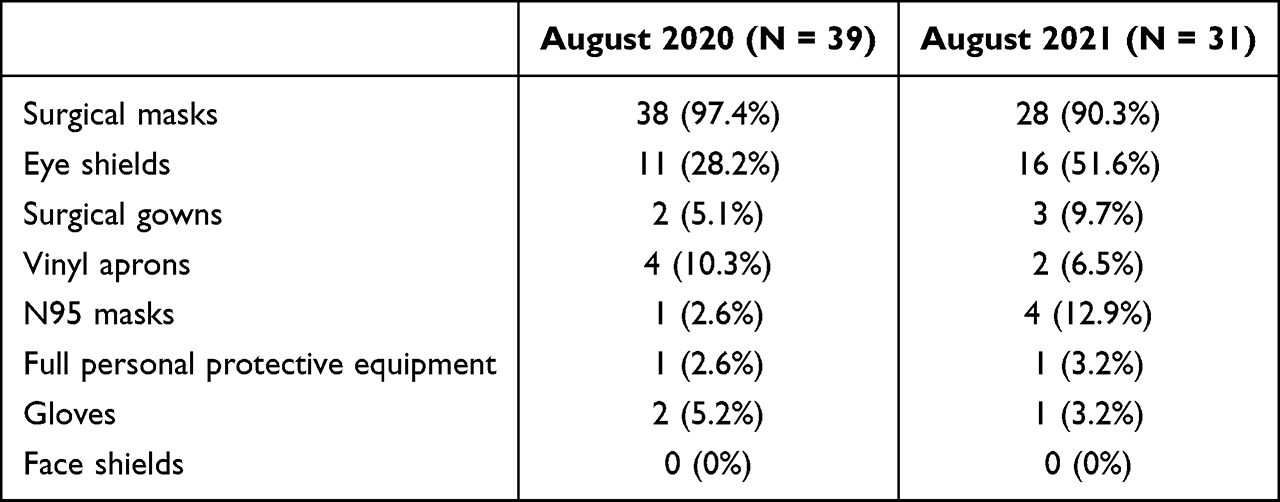 |
Table 2 Infection Control Measures Used by Psychiatrists for Electroconvulsive Therapy Cases with Low Risk of Coronavirus Disease 2019 Infection |
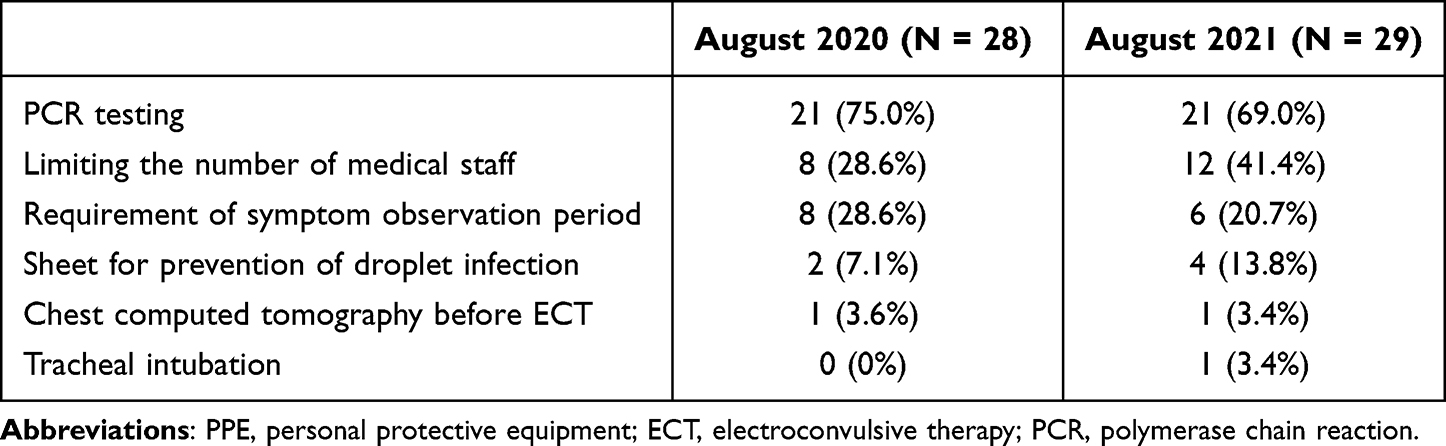 |
Table 3 Infection Control Measures Other Than PPE for ECT Patients |
The COVID-19 tests performed on admission at the time of the second questionnaire are shown in Table 4. More than 50% of the facilities performed PCR tests in all cases. In contrast, only a limited number of the facilities performed antigen and antibody tests. Moreover, some facilities required pre-hospital self-isolation for patients, which means staying indoors and completely avoiding contact with other people before their admission for ECT to avoid infection. At the time of the second survey, 6 facilities (18.7%) had a pre-hospital self-isolation requirement period, of which 4 (12.5%) mandated a period of 14 days.
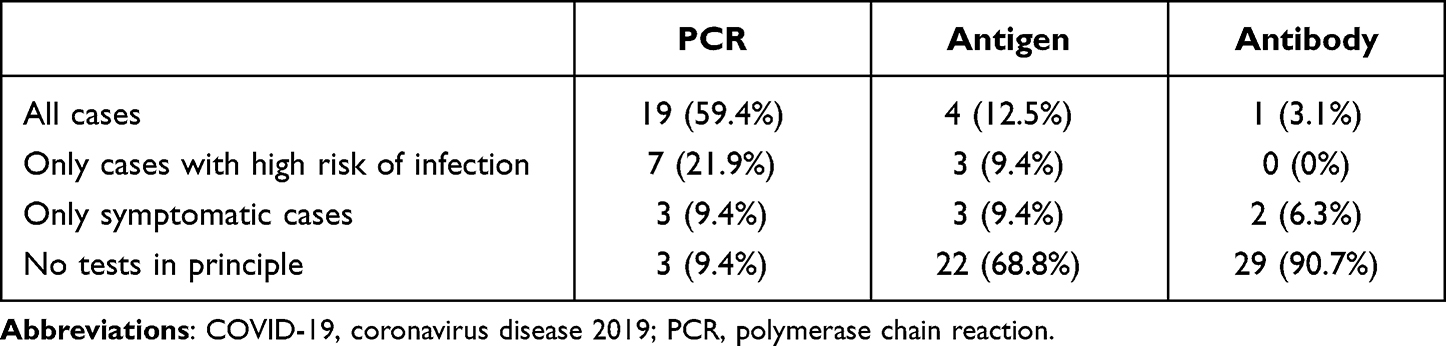 |
Table 4 Tests for COVID-19 Performed on Admission (August 2021) |
Discussion
Number of ECT Procedures
The number of ECT procedures was less affected in Japan than that in several other countries.3,4,14–16 According to a previous paper from Canada, between mid-March and mid-May 2020, the number of ECT procedures in that country decreased in 64% of facilities, with procedures completely stopped in 27% of facilities.3 In the United Kingdom and Ireland in April 2020, 88% of facilities reported a decrease in the number of ECT procedures and 24% had stopped completely, and in July 2020, 78% of facilities still reported a decrease in the number of procedures.4 The lower impact of the pandemic on ECT practices in Japan may be due to the relatively small number of infected people and few restrictions on movement in the society such as lockdowns. Each time that the COVID-19 infection spread, the Japanese government introduced a state of emergency, but the stay-at-home guidelines were voluntary. Non-essential businesses were asked to close, but rarely faced penalties for not complying.17
A comparison of urban and non-urban areas in Japan shows a marked decline in the number of patients undergoing ECT and enforcement restrictions in urban areas. The recovery in the number of patients undergoing ECT in urban areas during the fourth wave in April–June 2021 was slower than in the first wave in April 2020, suggesting that the impact of the pandemic may be prolonged in urban areas.
Maintenance ECT
In August 2021, more than 80% of facilities were using maintenance ECT at the same rate as before, but some were still restricted in their use. There is an urgent need to resume maintenance ECT to reach pre-pandemic levels, with priority given to patients at high risk of relapse. In a follow-up study of 81 patients for whom maintenance ECT was abruptly discontinued because of the COVID-19 pandemic, 36 patients (44.44%) relapsed within a 6-month observation period.18 In another study, the relapse rate also increased when the treatment was continued with a decreased frequency.19 Patients at higher risk of relapse were those with diagnoses other than major depressive disorder (ie, bipolar disorder, schizophrenia, schizoaffective disorder) and those with shorter intervals between maintenance ECT treatments. These findings clearly indicate that maintenance ECT is an essential treatment for which the accessibility to and frequency of administration should be stable, even in the pandemic.
Infection Control Measures During ECT
Most facilities considered PCR testing before ECT if a patient was suspected to be infected with COVID-19. This strategy is recommended by several past reports.6,10,20 Furthermore, many facilities required all staff to wear surgical masks and eye shields during ECT. Some studies recommend the use of gloves, gowns, or head covers, in addition to masks and eye shields,6,10,20–26 so it may be necessary to consider their use in Japan for future responses to infection and pandemic.
Another less common, but potentially effective, strategy is to cover the upper bodies of patients or to use ECT head chambers for them. Some reports suggest that if bag-mask ventilation (BMV) is needed for a significant desaturation, it may be helpful to cover the patient’s head with a plastic sheet22–24 and to place a breathing circuit filter between the mask and valve.24,25 Because BMV is a known aerosolizing procedure,26 routine BMV should not be provided prior to ECT.23 In one chart review study, when patients were pre-oxygenated with a non-rebreather mask for 3–5 minutes, more than 50% of them did not require BMV and electroencephalography seizure duration did not decrease significantly.27
ECT for Patients Not at Low Risk of COVID-19 Infection
Our study revealed an increase in the use of ECT in patients who were not at low risk of infection in 2021. This finding may be explained by widespread awareness of the safety of ECT using proper infection control. It is conceivable that urgent cases for ECT included these patients groups: those at high risk of suicide, those rapidly deteriorating physically due to psychiatric symptoms, older adults with co-morbidities, or those with respiratory disease who have severe psychiatric symptoms but for whom pharmacotherapy is difficult, and other patients who, without ECT, are at risk of serious harm to themselves or others, including COVID-19 infection.10,28,29 Successful cases of ECT for urgent patients not at low risk of infection and even for infected patients have been reported.30–34 For example, ECT in symptomatic patients has been reported in the United Kingdom in a 67-year-old man diagnosed with a major depressive episode with catatonic features. The patient presented with fever and decreased oxygen saturation prior to ECT and was found to be COVID-19 positive. Treatment for pneumonia was initiated, and 4 later the patient underwent ECT twice weekly for a total of six sessions. Infection control measures for this case included all staff wearing N95 masks, caps, visors, gowns, plastic aprons, shoe covers, and three pairs of gloves, and equipment was thoroughly disinfected before the next procedure. Glycopyrronium was also administered prior to treatment to inhibit respiratory secretion. During the procedure, BMV was avoided, intubation was performed after the use of an oxygen mask, and the psychiatrist and psychiatric nurse left the room during intubation and extubation.32 The infection control procedures in this case were practiced as recommended in other papers.35,36 To our best knowledge, no cases of ECT have been reported for infected people in Japan as of December 2021. In situations for which ECT must be performed in infected patients, it is necessary to implement ECT while taking sufficient infection control measures, referring to prior approaches used for cases globally.
Future Prospects for ECT in the Pandemic
In the COVID-19 pandemic, some cases of unfortunate outcomes occurred due to the inability to perform ECT.37,38 Of note, there was one case in which ECT was effective for neuropsychiatric symptoms in COVID-19.39 All these reports reaffirm the importance of ECT. We must continue to provide ECT to as many eligible patients as possible with appropriate infection control measures. It is not possible to predict how the widespread use of vaccines,40,41 the development of oral drugs,42 and the emergence of mutant43,44 strains for COVID-19 will affect the pandemic in the future. Therefore, it may still take some time before we will be able to offer ECT in the same way we did pre-pandemic.
Study Limitations
This report has certain noteworthy limitations. The survey results may have been biased because this questionnaire only covered JSGHP training facilities and ECT committee members’ facilities. These facilities were relatively experienced in ECT practice, and most of them were general hospitals, including university hospitals. In a nationwide survey of psychiatric institutions in 2010, ECT was performed in 356 facilities and 217 facilities were psychiatric hospitals.45 We have not fully assessed the status of ECT implementation in psychiatric hospitals. In addition, the criteria regarding whether each case was at high risk for infection were not uniform, as they were based on each facility’s standards throughout the survey. Moreover, the exact number of ECT cases could not be determined because the question regarding the number of cases offered answer options with a number range, such as “1–5 cases,” for ease of answering the questionnaire. Furthermore, the second survey covered the beginning of the fifth wave of the COVID-19 pandemic, which had the largest number of infections. Therefore, it is not possible to make a simple comparison with the first questionnaire, which was conducted during the period of convergence of the COVID-19 infection. Finally, it was unclear whether there was a shortage of anesthesiologists in Japan during the study period. Other countries reported that several cases of ECT were stopped due to a shortage of anesthesiologists, especially in the early stages of infection,3,37 and a survey that includes the perspective of anesthesiologists is needed in the future.
Conclusion
To the best of our knowledge, this study is unique because it analyzes the course of more than 1 year during the COVID-19 pandemic from 2020 to 2021. This survey showed that ECT was heavily affected by the pandemic in 2020, but by the summer of 2021, the number of ECT cases and the decisions to use ECT were returning almost to previous levels, with infection control measures in place.
Disclosure
Dr Hirotsugu Kawashima reports I received lecture fees from Otsuka, Dainippon-Sumitomo, Eisai, Meiji-Seika Pharma. Dr Takashi Tsuboi reports personal fees from Dainippon Sumitomo, personal fees from Takeda Pharmaceutical, personal fees from Pfizer, personal fees from Yoshitomi Yakuhin, personal fees from Tsumura, personal fees from Otsuka Pharmaceutical, personal fees from Mochida Pharmaceutical, personal fees from Kyowa Pharmaceutical, personal fees from Meiji-Seika Pharma, personal fees from Eisai, personal fees from Mitsubishi Tanabe Pharma, personal fees from MSD, personal fees from Shionogi, outside the submitted work; The authors declare no other conflicts of interest in this work.
References
1. Iyengar KP, Vaishya R, Bahl S, et al. Impact of the coronavirus pandemic on the supply chain in healthcare. Br J Health Care Manag. 2020;26:1–4.
2. Emanuel EJ, Persad G, Upshur R, et al. Fair allocation of scarce medical resources in the time of Covid-19. N Engl J Med. 2020;382:2049–2055. doi:10.1056/NEJMsb2005114
3. Demchenko I, Blumberger DM, Flint AJ, et al. Electroconvulsive therapy in Canada during the first wave of COVID-19: results of the what happened national survey. J ECT. 2021. 38(1):52.
4. Braithwaite R, Chaplin R, Sivasanker V. Effects of the COVID-19 pandemic on provision of electroconvulsive therapy. BJPsych Bull. 2021;46(3):1–4.
5. Espinoza RT, Kellner CH, McCall WV. Electroconvulsive therapy during COVID-19: an essential medical procedure-maintaining service viability and accessibility. J ECT. 2020;36:78–79. doi:10.1097/YCT.0000000000000689
6. Bryson EO, Aloysi AS. A strategy for management of electroconvulsive therapy patients during the COVID-19 pandemic. J ECT. 2020;36:149–151. doi:10.1097/YCT.0000000000000702
7. International Society for ECT and Neurostimulation. Position statement on ECT as an essential procedure during COVID-19. Available from: https://www.isen-ect.org/covid-19-essential-procedure.
8. Karako K, Song P, Chen Y, et al. Overview of the characteristics of and responses to the three waves of COVID-19 in Japan during 2020–2021. BioSci Trends. 2021;15:1–8. doi:10.5582/bst.2021.01019
9. Oh Y. Characteristics and challenges of Japan’s corona response measures: an international comparative perspective. NIRA opin. 2021;57(2021):1–12.
10. JSGHP ECT Committee. Use of modified electroconvulsive therapy during the COVID-19 pandemic. Available from: http://psy.umin.ac.jp/content/document/ECT_under_COVID-19. pdf Accessed June 17, 2022. (Japanese).
11. Ministry of Health, Labour and Welfare. NDB open data. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000177182.html.
12. Google. Google forms. Available from: https://www.google.com/intl/en/forms/about/#overview.
13. Kumar K, Naik L. How to create an online survey using google forms. Int J Libr Inf Stud. 2016;6:118–126.
14. The Ministry of Health, Labour and Welfare. Publication of infection status by region. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/newpage_00016.html.
15. Grover S, Mehra A, Sahoo S, et al. Impact of COVID-19 pandemic and lockdown on the state of mental health services in the private sector in India. Indian J Psychiatry. 2020;62:488–493. doi:10.4103/psychiatry.IndianJPsychiatry_568_20
16. Grover S, Mehra A, Sahoo S, et al. State of mental health services in various training centers in India during the lockdown and COVID-19 pandemic. Indian J Psychiatry. 2020;62:363–369. doi:10.4103/psychiatry.IndianJPsychiatry_567_20
17. Looi M-K. Covid-19: Japan declares state of emergency as Tokyo cases soar. BMJ. 2020;369:m1447. doi:10.1136/bmj.m1447
18. Lambrichts S, Vansteelandt K, Crauwels B, et al. Relapse after abrupt discontinuation of maintenance electroconvulsive therapy during the COVID‐19 pandemic. Acta Psychiatr Scand. 2021;144:230–237. doi:10.1111/acps.13334
19. Methfessel I, Besse M, Belz M, et al. Effectiveness of maintenance electroconvulsive therapy-evidence from modifications due to the COVID‐19 pandemic. Acta Psychiatr Scand. 2021;144:238–245. doi:10.1111/acps.13314
20. Naik SS, Gowda GS, Shivaprakash P, et al. Homeless people with mental illness in India and COVID-19. Lancet Psychiatry. 2020;7:e51–e52. doi:10.1016/S2215-0366(20)30286-8
21. Colbert SA, McCarron S, Ryan G, et al. Immediate impact of coronavirus disease 2019 on electroconvulsive therapy practice. J ECT. 2020;36:86–87. doi:10.1097/YCT.0000000000000688
22. Gil-Badenes J, Valero R, Valentí M, et al. Electroconvulsive therapy protocol adaptation during the COVID-19 pandemic. J Affect Disord. 2020;276:241–248. doi:10.1016/j.jad.2020.06.051
23. Ramakrishnan VS, Kim YK, Yung W, et al. ECT in the time of the COVID-19 pandemic. Australas Psychiatry. 2020;28:527–529. doi:10.1177/1039856220953705
24. Lapid MI, Seiner S, Heintz H, et al. Electroconvulsive therapy practice changes in older individuals due to COVID-19: expert consensus statement. Am J Geriatr Psychiatry. 2020;28:1133–1145. doi:10.1016/j.jagp.2020.08.001
25. Araujo RF, de Oliveira Quites L. Occupational team safety in ECT practice during the COVID-19 pandemic. Rev Bras Anestesiol. 2021;70:687–688. doi:10.1016/j.bjan.2020.10.002
26. Purushothaman S, Fung D, Reinders J, et al. Electroconvulsive therapy, personal protective equipment and aerosol generating procedures: a review to guide practice during coronavirus disease 2019 (COVID-19) pandemic. Australas Psychiatry. 2020;28:632–635. doi:10.1177/1039856220953699
27. Luccarelli J, Fernandez-Robles C, Fernandez-Robles C, et al. Modified anesthesia protocol for electroconvulsive therapy permits reduction in aerosol-generating bag-mask ventilation during the COVID-19 pandemic. Psychother Psychosom. 2020;89:314–319. doi:10.1159/000509113
28. Baghai TC, Möller H-J. Electroconvulsive therapy and its different indications. Dialogues Clin Neurosci. 2008;10:105–117. doi:10.31887/DCNS.2008.10.1/tcbaghai
29. Tor P-C, Tan J, Loo C. Model for ethical triaging of electroconvulsive therapy patients during the COVID-19 pandemic. BJPsych Bull. 2021;45:175–178. doi:10.1192/bjb.2020.99
30. Boland X, Dratcu L. Electroconvulsive therapy and COVID-19 in acute inpatient psychiatry: more than clinical issues alone. J ECT. 2020;36:223–224. doi:10.1097/YCT.0000000000000708
31. Grover S, Sinha P, Sahoo S, et al. Electroconvulsive therapy during the COVID-19 pandemic. Indian J Psychiatry. 2020;62:582–584. doi:10.4103/psychiatry.IndianJPsychiatry_335_20
32. Braithwaite R, McKeown HL, Lawrence VJ, et al. Successful electroconvulsive therapy in a patient with confirmed, symptomatic covid-19. J ECT. 2020;36:222–223. doi:10.1097/YCT.0000000000000706
33. Hassani V, Amniati S, Kashaninasab F, et al. Electroconvulsive therapy for a patient with suicide by drinking bleach during treatment of COVID-19: a case report. Anesth Pain Med. 2020;10:e107513. doi:10.5812/aapm.107513
34. Martinez-Roig M, Arilla-Aguilella JA, Bono-Ariño MC, et al. ECT: a decision to decrease risks during COVID-19 pandemic. Rev Psiquiatr Salud Ment. 2021. doi:10.1016/j.rpsm.2021.04.004
35. Sienaert P, Lambrichts S, Popleu L, et al. Electroconvulsive therapy during COVID-19-times: our patients cannot wait. Am J Geriatr Psychiatry. 2020;28:772–775. doi:10.1016/j.jagp.2020.04.013
36. Thiruvenkatarajan V, Dharmalingam A, Armstrong-Brown A, et al. Uninterrupted anesthesia support and technique adaptations for patients presenting for electroconvulsive therapy during the COVID-19 era. J ECT. 2020;36:156–157. doi:10.1097/YCT.0000000000000707
37. Tor PC, Phu AHH, Koh DSH, et al. Electroconvulsive therapy in a time of COVID-19. J ECT. 2020;36:80–85. doi:10.1097/YCT.0000000000000690
38. Sagué-Vilavella M, Gil-Badenes J, Baldaquí Baeza N, et al. The other victims of COVID-19: the value of electroconvulsive therapy. J ECT. 2021;37:e1–e2. doi:10.1097/YCT.0000000000000718
39. Austgen G, Meyers MS, Gordon M, et al. The use of electroconvulsive therapy in neuropsychiatric complications of COVID-19: a systematic literature review and case report. J Acad Consult-Liaison Psychiatry. 2022;63:86–93. doi:10.1016/j.jaclp.2021.07.010
40. Gursel M. COVID‐19 vaccine inequity: high time to calibrate the global moral compass. Eur J Immunol. 2021;51:2705–2707. doi:10.1002/eji.202170125
41. Mori H, Naito T. A rapid increase in the COVID-19 vaccination rate during the Olympic and Paralympic games 2021 in Japan. Hum Vaccin Immunother. 2021;18(1):2010440.
42. Mahase E. Covid-19: molnupiravir reduces risk of hospital admission or death by 50% in patients at risk, MSD reports. BMJ. 2021;375:n2422. doi:10.1136/bmj.n2422
43. Karim SSA, Karim QA. Omicron SARS-CoV-2 variant: a new chapter in the COVID-19 pandemic. Lancet. 2021;398:2126–2128. doi:10.1016/S0140-6736(21)02758-6
44. Torjesen I. Covid-19: omicron may be more transmissible than other variants and partly resistant to existing vaccines, scientists fear. BMJ. 2021;375:n2943. doi:10.1136/bmj.n2943
45. Okumura M, Samejima T, Awata S, et al. Current status of electroconvulsive therapy (ECT) in Japan: what is needed in general hospital psychiatry from the results of a nationwide survey. Gen Hosp Psychiatry. 2010;22:105–118. In Japan.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.