Back to Journals » International Journal of Women's Health » Volume 15
Alternate Birth Strategies
Authors Whittington JR ![]() , Ghahremani T, Whitham M, Phillips AM, Spracher BN
, Ghahremani T, Whitham M, Phillips AM, Spracher BN ![]() , Magann EF
, Magann EF ![]()
Received 20 January 2023
Accepted for publication 11 July 2023
Published 21 July 2023 Volume 2023:15 Pages 1151—1159
DOI https://doi.org/10.2147/IJWH.S405533
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Julie R Whittington,1 Taylor Ghahremani,2 Megan Whitham,3 Amy M Phillips,2 Bethany N Spracher,4 Everett F Magann2
1Department of Obstetrics and Gynecology, Navy Medicine Readiness and Training Command Portsmouth, Portsmouth, VA, USA; 2Department of Obstetrics and Gynecology, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 3Department of Obstetrics and Gynecology, Virginia Tech Carilion School of Medicine, Roanoke, VA, USA; 4Department of Obstetrics and Gynecology, Edward via College of Osteopathic Medicine, Blacksburg, VA, USA
Correspondence: Everett F Magann, Department of Obstetrics and Gynecology, 4301 W. Markham St. Slot # 518, Little Rock, AR, 72205-7199, USA, Tel +1 501-686-8345, Fax +1 501-526-7820, Email [email protected]
Abstract: Community birth is defined as birth that occurs outside the hospital setting. Birthing in a birth center can be safe for certain patient populations. Home birth can also be safe in well-selected patient with a well-established transfer infrastructure should an emergency occur. Unfortunately, many areas of the United States and the world do not have this infrastructure, limiting access to safe community birth. Immersion during labor has been associated with decreased need for epidural and pain medication. Delivery should not occur in water due to concerns for infection and cord avulsion. Umbilical cord non-severance (also called lotus birth) and placentophagy should be counseled against due to well-documented risks without clear benefit. Birth plans and options should be regularly discussed during pregnancy visits.
Keywords: home birth, community birth, water birth, immersion in labor, placentophagy, maternal outcomes, perinatal outcomes
Background
The formalization of written birth plans in the 1980s has led to rapid uptake among the birthing population.1 Formulating a birth plan has become an important part of the birthing process for many pregnant patients. Patient satisfaction with the birth experience is variable and may depend on the number of requests, adherence to the formalized birth plan, route of delivery, and whether complications arose during or after delivery;2–4 however, the literature suggests that there is an overall higher satisfaction with this experience when a birth plan is employed.5,6 There is also a significant body of literature supporting that patients with birth plans may undergo fewer interventions in the labor process, which may be associated with a longer first stage of labor, but limited effect on overall labor duration.7,8
With the rise of employing birth plans to individualize care9 there have been growing interests in alternate birth choices outside of the traditional medical hospital birth experience. Our paper serves as a review of the more-commonly encountered alternative birth choices, literature review about these birthing methods and outcomes, and recommendations considering this review.9
Methods
A literature search was undertaken by a university librarian using the search engines PubMed and CINAHL. The searches were limited to English only. There was no limitation on the number of years search through 7/31/2022. The search terms used for the home birth section were “home” AND “birth OR childbirth” AND “planned” AND “outcome OR benefits OR complications OR adverse effects OR recommendations OR guidelines”. The searches undertaken for the other sections were “home birth” OR “water birth” OR “lotus birth” OR “placentophagy” AND “outcome OR benefits OR complications OR adverse effect OR recommendations OR guidelines”. Another search was undertaken with the terms “birth plans” encompassing various aspects of those plans. The searches identified 523 abstracts. All abstracts were read by two of the authors (JRW and EFM). Full articles were obtained for relevant articles. The references of the full articles were assessed for additional articles. There were 36 articles which are the basis of this review (Figure 1).
 |
Figure 1 Flow diagram for identifying articles eligible for inclusion. |
Alternative Birth Plans - Community Birth
Community birth is a birth that is accomplished either in a detached birthing center or at home instead of in the hospital setting. In 2017, one out of every 61 births occurred out of the hospital and the incidence has increased since 2004.10 During the COVID-19 pandemic.11 In women who had significant psychological stress associated with contracting COVID-19, there was an increased preference for community birth.12 In a small cohort of parturients who chose home birth after a prior in-hospital birth, dissatisfaction with the hospital birthing experience and avoidance of intervention were noted to be common factors in their choice.13
There are multiple studies showing increased neonatal risks associated with home birth. A large retrospective cohort study using data from the Centers for Disease Control from 2010 to 2017 stratified location of birth (hospital versus home) supervised by certified nurse-midwives noted there was an increase in neonatal mortality noted with home births (odds ratio 2.90, 95% CI 2.17–3.89).14 It is remarkable that, again with the pandemic, there has been a 37.33% increase in community breech births, and there was an increase in Apgar scores of 0–3 by 35.9%.15 The increased risk associated with home births is even more pronounced with direct-entry midwives (OR 3.81, 95% CI 3.12–4.65).16 Direct-entry midwives are midwives who are certified professional midwives who did not complete nursing training first.14 This would imply that the risk is not only related to the training of the birth attendant, but to the location of birth. In a retrospective case control study out of Hawaii, the rate of hypoxic-ischemic encephalopathy was higher in neonates after planned home birth (OR 2.77, 95% CI 1.05–6.87). This difference in HIE rates was even more pronounced after adjusting for risk factors (OR 11.56 95% CI 1.37–118.77).17 In a retrospective cohort study of planned out-of-hospital births in Oregon, there was increased risk of perinatal mortality after adjusting for maternal characteristics and medical conditions (OR 2.43, 95% CI 1.37–4.3).18 There was also an increased risk of neonatal seizures in this study. Wasden et al published a case–control study in 2017 that noted a 21-fold increased risk of hypoxemic ischemic encephalopathy when home birth was planned.19 Even though hypoxemic ischemic encephalopathy and neonatal seizures are rare events, the gravity of these complications puts the safety of home birth into serious question.
In contrast, other studies show no difference in neonatal outcomes based on planned delivery location. Nethery et al reviewed births in Washington from 2015 to 2020. In a well-established, integrated community midwifery program with women within professional association guidelines, there was no difference in outcomes between planned home birth and planned birth center birth (both are considered out-of-hospital births) amongst low-risk patients.20 In a systematic review and meta-analysis of home birth versus hospital birth for low-risk women, there was no difference in neonatal morbidity or mortality. However, there was decreased risk of cesarean delivery OR 0.607 (95% CI 0.553–0.667), shoulder dystocia OR 0.287 (95% CI 0.133–0.618), and postpartum hemorrhage 0.692 (95% CI 0.634–0.755) in the planned home birth group.21 It is also notable that none of the studies in this systematic review and meta-analysis were completed in the United States.
In women with prior cesarean delivery who planned home birth in the United States compared to women with prior cesarean delivery who planned hospital delivery, there was a notable increased risk of Apgar scores of 0 (relative risk 9.04, 95% CI 4–20.39) and neurologic dysfunction (relative risk 11.19, 95% CI 5.13–24.29).22 Another study of CDC data from 2016 to 2020 noted significantly increased risk for adverse outcomes for breech deliveries and twin deliveries (OR 8.88, 95% CI 7.7–10.3 and OR 2.8, 95% Ci, 2.2–3.4, respectively).23 In contrast, in a national prospective cohort study in England, the babies of higher risk women with planned hospital birth had increased risk of NICU admission; there was no difference in neonatal morbidity or mortality.24 This must be interpreted with caution, given the robust transfer system in place in England. It is also notable that proximity to hospital likely plays a role in morbidity, especially in the United States. Way et al reviewed United States birth data from 2010 to 2017 and found that neonates delivered in a rural setting were associated with increased risk of infant mortality with rural home and birth center births (aRR 1.62 95% CI 1.42–1.85 and aRR 1.33, 95% CI 1.05–1.68 respectively).25
Community birth may be associated with decreased risk of cesarean delivery and obstetric intervention. However, community birth is associated with adverse neonatal outcomes in multiple studies. There is extensive debate in the obstetric community regarding safety of community birth and where the optimal place for birthing is. Grunebaum et al noted that advocates for home birth look at absolute risk of incidents. Absolute risk of neonatal death and HIE are indeed low with planned community birth. However, when referencing exceedingly important outcomes including neonatal death and hypoxic ischemic encephalopathy, any increased risk (including relative risk) must be considered.26
In conclusion, planned community birth may be safe for low-risk pregnancies with highly organized transfer capabilities.27 However, birthing people must be thoroughly informed about the risk of severe neonatal morbidity with community birth. In addition, many, if not most, areas of the United States are without such highly organized transfer capabilities. Parturients considering out of hospital birth should also meet the eligibility criteria outlined here in Table 1 and voice understanding of the counseling on risk.
 |
Table 1 Eligibility Criteria and Recommended Contraindications to Home Birth |
Alternative Birth Plans – Immersion During Labor and Delivery
Water birth refers to delivery of the neonate into the water while the birthing person is immersed in water (Figure 2). The American College of Obstetricians and Gynecologists discourages use of the term “water birth” in favor of immersion in the second stage of labor.28 This allows for clarification of the stage at which water is utilized and where birth occurs (on land or in water). Immersion in warm water has been used for both pain relief and relaxation and has been used in both the first and second stage of labor.29 Immersion in water may help pain by allowing the parturient to move more freely than on land and position themselves comfortably. It may also help with pain by inhibiting pain signaling pathways.29
 |
Figure 2 Water birth or immersion illustration. |
A recent systematic review and meta-analysis found that immersion during the first stage of labor has been found to have many benefits including decreased utilization of pain medication, shorter labor, and fewer interventions including episiotomy.30 Of note, there does not appear to be a difference between spontaneous vaginal delivery, cesarean delivery, or operative vaginal delivery rates between women who use hydrotherapy in the first stage of labor compared to those who do not.29
In a retrospective cohort study by Hodgson et al, immersion during the second stage of labor was associated with a decrease in the risk of third- and fourth-degree lacerations and a decrease in the risk of neonatal morbidity compared to conventional birth.31 However, there was no significant difference in the length of the second stage of labor between groups.31 Another retrospective cohort study of 6264 water births by Aughey et al found reduced risk of neonatal intensive care unit admission and postpartum hemorrhage with immersion in the second stage of labor.11 Aughey et al also noted that water birth was less common in black or Asian women and those from areas of increased socioeconomic deprivation.11 Birthing people who are socioeconomically disadvantaged may not have the same access or opportunities to alternative birthing or birth plans.
In a retrospective cohort study of United States birth center birth in which immersion was utilized, Snapp et al found decreased risk for pharmacologic pain medication, episiotomy, genital lacerations, prolonged first or second stage, shoulder dystocia and maternal hemorrhage.32 They did note increased risk of cord avulsion with immersed birth.32 The authors suggested that excessive traction may occur on the cord as the neonate is brought up and out of the water, causing avulsion. Preston et al specifically examined the risk of obstetric anal sphincter injury with immersed birth compared to land birth. They noted an odds ratio of 2.1 (95% confidence interval 1.5–2.94) for 3rd or 4th degree perineal lacerations.33 Thus, there is conflicting data regarding risks of perineal injuries with water birth. There may be increased risk of perineal injury due to lack of controlled delivery of the fetal head.
In a retrospective study of 58 deliveries that occurred in water, there was increased risk of postpartum hemorrhage associated with immersion during the second stage of labor compared to conventional birth.16 There were no differences in neonatal outcomes between groups.16 In a study of 17,530 water births compared to 17,530 propensity-score matched land births, the investigators found increased incidence in maternal infection rate and neonatal cord avulsion with immersion in the second stage of labor. However, the investigators also found improved outcomes for maternal and neonatal hospitalization. Otherwise, there were no differences between delivery on land compared to delivery in water.34
Much of the concern around water birth comes from case reporting of adverse neonatal outcomes. Vanderlaan and Hall performed a systematic review of case reports and found associations with adverse neonatal outcomes. The authors noted a pattern of waterborne pathogens and caution that protocols must be in place to ensure clean water supply and appropriate birthing tubs are utilized. They also encourage a high index of suspicion for waterborne pathogens when pediatricians are caring for infants born in the water.35 The authors also note cord avulsion has been a cause for neonatal morbidity and that delivering providers carefully manage the cord.35
The American College of Nurse Midwives (ACNM) put forth guidelines to support access to hydrotherapy and immersed second stage of labor.36 They establish eligibility criteria and outline contraindications for water immersion for labor and birth as seen in Table 2. The ACNM also give precautions including infection control measures, universal personal protective equipment, available emergency equipment, regularly scheduled emptying and cleaning of the birthing tub.
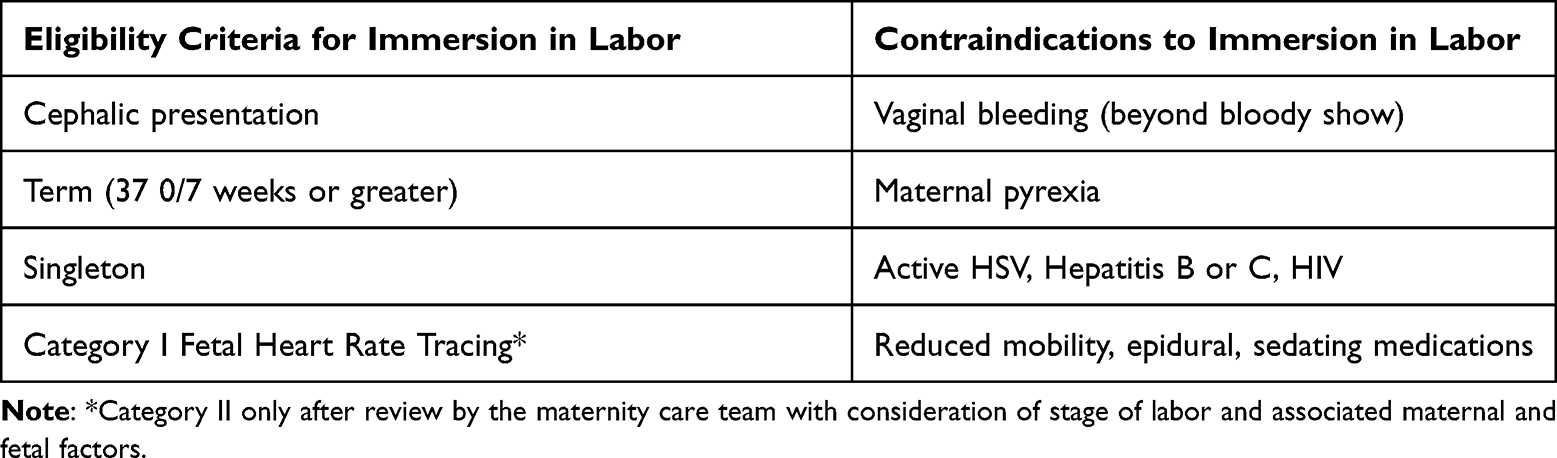 |
Table 2 Eligibility Criteria and Contraindications to Immersion in Labor and Birth |
Currently, the American College of Obstetricians and Gynecologists and the American Academy of Pediatrics consider delivery in water to be experimental and state that immersed delivery should only occur in the context of clinical trials.28,37 Furthermore, immersed delivery should be regulated and evidence-based to minimize maternal and neonatal risks. Birthing people considering water birth should be counseled on the risks and benefits of immersion in labor and delivery and only deliver in a center or hospital with rigorous cleaning standards.
Alternative Birth Plans – Umbilical Cord Non-Severance (Lotus Birth)
A lotus birth refers to the practice of non-severance of the umbilical cord at the time of birth. The umbilical cord and placenta are left attached to the newborn and allowed to dry and fall off naturally which can take anywhere from 3 to 10 days (Figure 3). The third stage of labor is managed passively with no uterotonics administered and traction is not applied to the cord. Once the placenta is delivered, it is washed, dried, and processed with a mixture of salt and herbs to facilitate drying and decrease odor and bacterial growth. Lavender and rosemary are commonly used. The placenta is then placed in a container that allows for air circulation.
 |
Figure 3 Lotus birth illustration. |
The practice was named after Clair Lotus Day who, while pregnant in 1974, observed that chimpanzees do not always separate their placentas from their newborns. At the time of her delivery, she brought this model to the human birth experience and did not cut the umbilical cord of her child. Reasons for choosing to have a lotus birth vary but are often cited as promoting maternal-infant bonding through uninterrupted skin-to-skin contact, honor to the placenta, and belief that there is a spiritual relationship between the newborn and the placenta.38 Advocates also believe the fetus and placenta formed from the same cell and are thus a single unit and if left attached a considerable amount of blood will be transferred to the newborn.39
A 2019 qualitative study by Gonenc et al describes the experience of 9 women who had a lotus birth in Turkey. One birth was at home while the other eight occurred in a hospital setting. The participants reported the reasons for choosing lotus birth were desire for the most natural birth process and the belief that cutting the cord was an interruption of the spiritual relationship between the newborn and the placenta which was disrespectful to the placenta. Overall, the participants reported a positive experience and that they would choose it again and recommend it to others.39 Other positive perceptions included strengthening of the maternal-infant bond, promotion of breastfeeding, and a peaceful, calm newborn. The reported negative experiences included perception by family, friends, and healthcare professionals and lack of resources when making their decision to have a lotus birth. Their biggest concerns were how to carry the newborn and placenta together and ensure no pulling on the cord, fear of infection and jaundice.39 Most participants hid or buried the placenta after separation. There were no reported newborn infections and 1 report of jaundice.39
While there are no research studies evaluating the neonatal benefits of lotus birth, there are case reports of identified risks. The placenta, once delivered, is considered a non-viable organ which becomes colonized with bacteria and may increase the risk of adverse outcomes. In 2015, Tricarico et al reported on an infant with persistent jaundice related to idiopathic neonatal hepatitis associated with umbilical cord non-severance. The infant was admitted on day of life 3 at which time the umbilical cord was cut. However, the infant continued to have poor fetal growth and poor feeding and was readmitted on DOL 25. Mild hypertransaminasemia persisted until 18 months of age.40 In 2017, Baker et al reported on a term neonate who developed S. epidermidis sepsis after umbilical cord non-severance. Symptoms displayed by the neonate included lethargy, poor feeding, and rhythmic twitching of the lower extremities. S. epidermidis was noted on placental pathology with no evidence of chorioamnionitis.41
Svendenkrans reported on an infant who had delayed cord clamping for 50 minutes during which time the placenta was placed below the level of the infant. The child lost a large volume of blood and developed hypovolemic shock thus highlighting that delayed cord clamping can be acutely dangerous as well.42
In contrast, Zinsser et al reported on 3 lotus births that occurred outside of the hospital setting and had no infections.43 Additionally, Monroe et al reported 6 in–hospital lotus births and none experienced neonatal infection.38 Two of the 6 received phototherapy for jaundice. Three of the 6 severed the umbilical cord prior to hospital discharge. This study also collected data on other newborn interventions in these 6 patients and found they were less likely to allow routine newborn care including lower rates of hepatitis B vaccination (16.7% vs 86.4%), erythromycin eye ointment (50% vs 94.1%), and intramuscular vitamin K administration (33.3 vs 97.7%) when compared to typical newborn services at the institution.38
While there is plenty of evidence-based research to support the benefit of delayed cord clamping, studies reporting positive or negative neonatal health outcomes with umbilical cord non-severance are lacking. The American College of Obstetricians and Gynecologist as well as the American Academy of Pediatrics do not have formal statements on lotus birth. Despite these deficiencies, women who choose to pursue lotus birth should receive information on the potential risks and benefits to the newborn and mother. Continued research around lotus birth should be pursued in efforts to best treat patients who choose to have a lotus birth.
Alternative Birth Plans – Placentophagy
Placentophagy is the consumption of the placenta after birth. This ritual of placenta consumption is commonly observed in non-human mammals and more recently has gained in popularity in humans since the 1970s.44 Placental tissue can be eaten raw, cooked, dehydrated, or processed for encapsulation which is the most common method of consumption.44–46 The reasoning driving motivation for consumption is because hormones (oxytocin, estrogen, progesterone, placental lactogen, ACTH, CRH) trace elements (copper, iron, selenium, zinc) amino acids, B vitamins, cytokines, and growth factors have been identified in placental tissue. Proposed benefits include improved mood, prevention of postpartum depression, increased breast milk production, reduction of postpartum bleeding, increased energy, and improvement in overall nutrition.46–50 Despite these claims, there is currently no information in the literature that the consumption of placental tissue in any form is beneficial in humans. Suggested risks of placental consumption include transmission of pathogens, endocrine effects, thromboembolic events, environmental toxins, and immunological responses.51
Due to the lack of any substantial benefits in evidence-based literature to date and the potential risks, expert option recommends against placentophagy.
Conclusion/Relevance
We offer the following best practices for the utilization of birth plans:
- Discuss birth plans and preferences with all pregnant people
- Start discussion and documentation of birth plans early in gestation
- Determine what is safe or feasible in the birthing facility
- Recommend against home birth unless birthing person meets criteria and there is a robust transfer program
- Consider supporting immersion in water in labor if rigorous cleaning standards are in place
- Recommend against umbilical cord non-severance and placentophagy due to infectious concerns
This requires open communication with the provider and the patient.52 There are demonstrated benefits to a patient having a plan for birth, and it can be viewed as a surrogate for shared decision-making and informed consent.53 It may also underscore a patient’s health literacy surrounding birth.53 There is no doubt that the process of birth is important but can also be unpredictable. Some authors have suggested renaming the idea to birth preferences, to help mitigate the belief that birth can always be planned.54,55
Ethics
This manuscript does not use human subject research or human subject data, it is a review of the history and trends in birth planning and safety guidelines. This work does not fall under the oversight of the Institutional Review Board of the University of Arkansas for Medical Sciences.
Acknowledgments
This work was prepared as part of her official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government”. Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person’s official duties. Where possible, we attempt to use the preferable terms birthing person, birthing people, and pregnant people and gender-neutral pronouns in lieu of gender-specific terminology. When studies were cited, women may be specified and thus will be used when referencing those studies.
Funding
There was no funding for this project.
Disclosure
EFM does the Assessment of Amniotic Fluid Volume chapter in UpToDate. JRW is a military service member. All other authors report no conflicts of interest in this work.
References
1. Simkin PE, Reinke CA. Planning Your Baby’s Birth. Minneapolis, MN: International Childbirth Education Association; 1980.
2. Jolles MW, Vries M, Hollander MH, et al. Prevalence, characteristics, and satisfaction of women with a birth plan in The Netherlands. Birth. 2019;46(4):686–692. doi:10.1111/birt.12451
3. Mei JY, Afshar Y, Gregory KD, et al. Birth plans: what matters for birth experience satisfaction. Birth. 2016;43(2):144–150. doi:10.1111/birt.12226
4. Alba-Rodríguez R, Coronado-Carvajal MP, Hidalgo-Lopezosa P. The birth plan experience-a pilot qualitative study in Southern Spain. Healthcare. 2022;10(1):95. doi:10.3390/healthcare10010095
5. Mirghafourvand M, Mohammad Alizadeh Charandabi S, Ghanbari‐Homayi S, et al. Effect of birth plans on childbirth experience: a systematic review. Int J Nurs Pract. 2019;25(4):e12722. doi:10.1111/ijn.12722
6. Webb R, Ayers S, Bogaerts A, et al. When birth is not as expected: a systematic review of the impact of a mismatch between expectations and experiences. BMC Pregnancy Childbirth. 2021;21(1):475. doi:10.1186/s12884-021-03898-z
7. Afshar Y, Mei JY, Gregory KD, et al. Birth plans-Impact on mode of delivery, obstetrical interventions, and birth experience satisfaction: a prospective cohort study. Birth. 2018;45(1):43–49. doi:10.1111/birt.12320
8. Hidalgo-Lopezosa P, Cubero-Luna AM, Jiménez-Ruz A, et al. Association between birth plan use and maternal and neonatal outcomes in Southern Spain: a case-control study. Int J Environ Res Public Health. 2021;18(2):456. doi:10.3390/ijerph18020456
9. Divall B, Spiby H, Nolan M, et al. Plans, preferences or going with the flow: an online exploration of women’s views and experiences of birth plans. Midwifery. 2017;54:29–34. doi:10.1016/j.midw.2017.07.020
10. MacDorman MF, Declercq E. Trends and state variations in out-of-hospital births in the United States, 2004–2017. Birth. 2019;46(2):279–288. doi:10.1111/birt.12411
11. Aughey H, Jardine J, Moitt N, et al. Waterbirth: a national retrospective cohort study of factors associated with its use among women in England. BMC Pregnancy Childbirth. 2021;21(1):256. doi:10.1186/s12884-021-03724-6
12. Preis H, Mahaffey B, Lobel M. The role of pandemic-related pregnancy stress in preference for community birth during the beginning of the COVID-19 pandemic in the United States. Birth. 2021;48(2):242–250. doi:10.1111/birt.12533
13. Bernhard C, Zielinski R, Ackerson K, et al. Home birth after hospital birth: women’s choices and reflections. J Midwifery Womens Health. 2014;59(2):160–166. doi:10.1111/jmwh.12113
14. Grünebaum A, McCullough LB, Orosz B, et al. Neonatal mortality in the United States is related to location of birth (hospital versus home) rather than the type of birth attendant. Am J Obstet Gynecol. 2020;223(2):254.e1–254.e8. doi:10.1016/j.ajog.2020.01.045
15. Grünebaum A, Bornstein E, Katz A, et al. Worsening risk profiles of out-of-hospital births during the COVID-19 pandemic. Am J Obstet Gynecol. 2022;226(1):137–138. doi:10.1016/j.ajog.2021.11.1346
16. Neiman E, Austin E, Tan A, et al. Outcomes of waterbirth in a US hospital-based midwifery practice: a retrospective cohort study of water immersion during labor and birth. J Midwifery Womens Health. 2020;65(2):216–223. doi:10.1111/jmwh.13033
17. Buchanan C, Kuo S, Minton L, et al. Neonatal hypoxic ischemic encephalopathy and planned home birth. J Midwifery Womens Health. 2022;67(1):69–74. doi:10.1111/jmwh.13309
18. Snowden JM, Caughey AB, Cheng YW. Planned out-of-hospital birth and birth outcomes. N Engl J Med. 2016;374(22):2190–2191. doi:10.1056/NEJMc1602337
19. Wasden SW, Chasen ST, Perlman JM, et al. Planned home birth and the association with neonatal hypoxic ischemic encephalopathy. J Perinat Med. 2017;45(9):1055–1060. doi:10.1515/jpm-2016-0292
20. Nethery E, Schummers L, Levine A, et al. Birth outcomes for planned home and licensed freestanding birth center births in Washington state. Obstet Gynecol. 2021;138(5):693–702. doi:10.1097/AOG.0000000000004578
21. Rossi AC, Prefumo F. Planned home versus planned hospital births in women at low-risk pregnancy: a systematic review with meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2018;222:102–108. doi:10.1016/j.ejogrb.2018.01.016
22. Grünebaum A, McCullough LB, Arabin B, et al. Serious adverse neonatal outcomes such as 5-minute Apgar score of zero and seizures or severe neurologic dysfunction are increased in planned home births after cesarean delivery. PLoS One. 2017;12(3):e0173952. doi:10.1371/journal.pone.0173952
23. Grünebaum A, Bornstein E, Katz A, et al. An immutable truth: planned home births in the United States result in avoidable adverse neonatal outcomes. Am J Obstet Gynecol. 2022;226(1):138–140. doi:10.1016/j.ajog.2021.11.1347
24. Li Y, Townend J, Rowe R, et al. Perinatal and maternal outcomes in planned home and obstetric unit births in women at ‘higher risk’ of complications: secondary analysis of the Birthplace national prospective cohort study. Bjog. 2015;122(5):741–753. doi:10.1111/1471-0528.13283
25. Way EA, Carwile JL, Ziller EC, et al. Out-of-hospital births and infant mortality in the United States: effect measure modification by rural maternal residence. Paediatr Perinat Epidemiol. 2022;36(3):399–411. doi:10.1111/ppe.12862
26. Grünebaum A, McCullough LB, Arabin B, et al. Critical appraisal of the proposed defenses for planned home birth. Am J Obstet Gynecol. 2019;221(1):30–34. doi:10.1016/j.ajog.2019.01.205
27. Committee on Obstetric Practice. Committee opinion no. 697: planned home birth. Obstet Gynecol. 2017;129(4):e117–e122. doi:10.1097/AOG.0000000000002024
28. American College of Obstetricians and Gynecologists. Committee opinion no. 679: immersion in water during labor and delivery. Obstet Gynecol. 2016;128(5):e231–e236.
29. Cluett ER, Burns E, Cuthbert A. Immersion in water during labour and birth. Cochrane Database Syst Rev. 2018;5(5):Cd000111.
30. Burns E, Feeley C, Hall PJ, Vanderlaan J. Systematic review and meta-analysis to examine intrapartum interventions, and maternal and neonatal outcomes following immersion in water during labour and waterbirth. BMJ Open. 2022;12(7):e056517.
31. Hodgson ZG, Comfort LR, Albert AAY. Water birth and perinatal outcomes in British Columbia: a retrospective cohort study. J Obstet Gynaecol Can. 2020;42(2):150–155. doi:10.1016/j.jogc.2019.07.007
32. Snapp C, Stapleton SR, Wright J, et al. The experience of land and water birth within the American Association of Birth Centers Perinatal Data Registry, 2012–2017. J Perinat Neonatal Nurs. 2020;34(1):16–26. doi:10.1097/JPN.0000000000000450
33. Preston HL, Alfirevic Z, Fowler GE, et al. Does water birth affect the risk of obstetric anal sphincter injury? Development of a prognostic model. Int Urogynecol J. 2019;30(6):909–915. doi:10.1007/s00192-019-03879-z
34. Bovbjerg ML, Cheyney M, Caughey AB. Maternal and neonatal outcomes following waterbirth: a cohort study of 17 530 waterbirths and 17 530 propensity score-matched land births. Bjog. 2022;129(6):950–958. doi:10.1111/1471-0528.17009
35. Vanderlaan J, Hall P. Systematic review of case reports of poor neonatal outcomes with water immersion during labor and birth. J Perinat Neonatal Nurs. 2020;34(4):311–323. doi:10.1097/JPN.0000000000000515
36. Kennedy L. A model practice template for hydrotherapy in labor and birth. J Midwifery Womens Health. 2017;62(1):120–126. doi:10.1111/jmwh.12587
37. Papile L-A, Baley JE, Benitz W. Immersion in water during labor and delivery. Pediatrics. 2014;133(4):758–761. doi:10.1542/peds.2013-3794
38. Monroe KK, Rubin A, Mychaliska KP, et al. Lotus birth: a case series report on umbilical nonseverance. Clin Pediatr (Phila). 2019;58(1):88–94. doi:10.1177/0009922818806843
39. Gönenç İM, Aker MN, Ay E. Qualitative study on the experience of lotus birth. J Obstet Gynecol Neonatal Nurs. 2019;48(6):645–653. doi:10.1016/j.jogn.2019.08.005
40. Tricarico A, Bianco V, Di Biase AR, et al. Lotus birth associated with idiopathic neonatal hepatitis. Pediatr Neonatol. 2017;58(3):281–282. doi:10.1016/j.pedneo.2015.11.010
41. Baker AN, Rao LM, Yeganeh N. Case 3: seizures in a 2-day-old Infant. NeoReviews. 2017;18(7):e445–e447. doi:10.1542/neo.18-7-e445
42. Svedenkrans J, Aquilano G, Pettersson K. A case of severe infant-to-placenta hemorrhage in association with prolonged delayed cord clamping. Am J Case Rep. 2020;21:e925116. doi:10.12659/AJCR.925116
43. Zinsser LA. Lotus birth, a holistic approach on physiological cord clamping. Women Birth. 2018;31(2):e73–e76. doi:10.1016/j.wombi.2017.08.127
44. Botelle R, Willott C. Borth attitudes and placentophagy: a thematic discourse analysis of discussions on UK parenting forums. BMC Pregnancy Childbirth. 2020;20(1):134.
45. Coyle CW, Hulse KE, Wisner KL, Driscoll KE, Clark CT. Placentophagy: therapeutic miracle on myth? Arch Womens Ment Health. 2015;18(5):673–680.
46. Satmbough K, Hernandex A, Sunn S, Adeyemi-Fowode O. Maternal Placentophagy as a Possible Cause of Breast Buding and Vaginal Bleeding in a Breast-Fed 3-Month-Old infant. J Pediatr Adolesc Gynecol. 2019;32(1):78–79.
47. Farr A, Chervenak FA, McCullough LB, Grunebaum A. Placentophagy among women planning community births in the United States: Frequency, rationale and associated neonatal outcomes. Birth. 2019;46(1):201–202.
48. Farr A, Chervenak FA, McCullough LB, Baergen RN, Grunebaum A. Human placentophagy: a review. Am J Obstet Gynecol. 2018;218(4):e401.1–e401.11.
49. Placentophagy HHE. Lotus Birth, and Other Placenta Practices: What Does the Evidence Tell Us? J Perinat Neonatal Nurs. 2019;33(2):99–102.
50. Morris E, Slomp C, Hippman C, et al. A Matched Cohort Study of Postpartum Placentophagy in Women with a History of Mood Disorders: No Evidence for Impact on Mood, Energy, Vitamin B12 Levels, or Lactation. J Obstet Gynaecol Can. 2019 Sep;41(9):1330–1337.
51. Hayes EH. Consumption of the Placenta in the Postpartum Period. J Obstet Gynecol Neonatal Nurs. 2016;45(1):78–89.
52. Aragon M, Chhoa E, Dayan R, et al. Perspectives of expectant women and health care providers on birth plans. J Obstet Gynaecol Can. 2013;35(11):979–985. doi:10.1016/S1701-2163(15)30785-4
53. Pinheiro A, Sardo D. P10 the birth plan as an instrument of health literacy. Eur J Public Health. 2019;29(Supplement_2). doi:10.1093/eurpub/ckz095.007
54. Kearsley R, Plaat F. When expectation and reality clash: birth plans and the anaesthetist. Int J Obstet Anesth. 2021;46:102964. doi:10.1016/j.ijoa.2021.102964
55. Medeiros RMK, Figueiredo G, Correa ÁC, et al. Repercussions of using the birth plan in the parturition process. Rev Gaucha Enferm. 2019;40:e20180233. doi:10.1590/1983-1447.2019.20180233
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.