Back to Journals » Journal of Pain Research » Volume 18
AI-Assisted Knee Infrared Imaging Based Acupuncture for Treating Knee Osteoarthritis: A Randomized Controlled Study Protocol
Authors Yang M, Qiu F, Xie X, Tao L, Zheng W, Wu Y, Xu Z, Xue Y ![]() , Cao Y
, Cao Y ![]()
Received 15 August 2025
Accepted for publication 5 November 2025
Published 19 November 2025 Volume 2025:18 Pages 6181—6195
DOI https://doi.org/10.2147/JPR.S560805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Muyun Yang,1,* Fengxi Qiu,2,* Xianfei Xie,3 Lin Tao,3 Weihong Zheng,4 Yufeng Wu,4 Zhaohong Xu,5 Yan Xue,2 Yuelong Cao1
1Characteristic Diagnosis and Treatment Technology Research Institution, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Department of Traditional Chinese Medicine, Shanghai Yangzhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), Shanghai, People’s Republic of China; 3Department of Orthopedics Ruijin Hospital, Shanghai JiaoTong University School of Medicine, Shanghai, People’s Republic of China; 4Department of Orthopedics, Zhongshan Hospital of Traditional Chinese Medicine, Guangdong, People’s Republic of China; 5School of Artificial Intelligence and Application, Shanghai Urban Construction Vocational College, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Xue, Email [email protected] Yuelong Cao, Email [email protected]
Background: The variability in acupoint selection limits the standardization of acupuncture for knee osteoarthritis (KOA) and is one of the important factors affecting treatment efficacy. Recent advancements in artificial intelligence (AI) and infrared imaging provide opportunities to enhance the precision and standardization of acupuncture.
Methods: This multicenter, single-blind, randomized controlled trial aims to evaluate whether AI-assisted personalized acupuncture is superior to traditional acupuncture and sham acupuncture in alleviating pain and improving joint function in patients with KOA. A total of 120 participants will be recruited from four hospitals in China and randomly assigned to three groups: the specific acupoint group (n=40), the conventional acupoint group (n=40), and the sham acupuncture group (n=40). All groups will receive acupuncture treatment twice a week for 8 weeks, with a total of 16 sessions. Outcome assessments will be conducted at baseline, week 8, and week 12. The AI system utilizes infrared imaging to identify heat-sensitive knee surface areas, and generates individualized acupoint prescriptions through internal decision analysis.
Discussion: The primary outcomes are knee pain (Numeric Rating Scale, NRS) and function (WOMAC subscale). Secondary outcomes include knee pain and stiffness (Western Ontario and McMaster Universities Osteoarthritis Index subscale, WOMAC subscale), quality of life (Short Form 12, SF-12), knee range of motion, Traditional Chinese Medicine (TCM) clinical efficacy, and inflammatory indicators (IL-1β, IL-6, and TNF-α). This trial is expected to provide high-quality evidence for the clinical value and standardization of AI-assisted acupuncture.
Trial Registration: This study has been registered with the Chinese Clinical Trial Registry (ChiCTR2400087106, July 19, 2024).
Keywords: knee osteoarthritis, koa, acupuncture, artificial intelligence, AI, infrared imaging
Background
Knee osteoarthritis (KOA) is a chronic degenerative joint disease characterized by the progressive deterioration of articular cartilage, resulting in pain, stiffness, and functional impairment.1 Epidemiological studies indicate that the prevalence of KOA increases significantly with age, affecting approximately 10% of men and 13% of women aged 60 years and older.2 This condition not only imposes significant limitations on physical function but also severely impacts quality of life, increases healthcare utilization, and poses a substantial economic burden.
Acupuncture, a cornerstone of Traditional Chinese Medicine (TCM), has been practiced for centuries and is widely used to alleviate pain and improve functional outcomes in patients with KOA.3–6 Its therapeutic mechanism involves the insertion of fine needles into specific acupoints, which are believed to stimulate the body’s natural healing processes and restore energy balance.7 Numerous studies8,9 have demonstrated the efficacy of acupuncture in reducing pain and improving joint function, with proposed mechanisms including the release of endogenous opioids, modulation of inflammatory pathways,10 and enhancement of local blood circulation. Despite its promising therapeutic effects, the variability in acupoint selection remains a significant limitation to its widespread application.
Traditional acupoint selection is predominantly based on the practitioner’s experience and TCM theoretical framework, leading to substantial individual variability and a lack of standardization.11,12 Evidence suggests that the effectiveness of acupuncture largely depends on the acupoints selected; however, the lack of reproducibility undermines the understanding of the therapeutic potential of acupuncture.13
In current acupuncture trials, acupoint selection for KOA can be categorized into local points, distal points, and combined approaches.14 Local points, such as Liangqiu (ST34), Zusanli (ST36), Neixiyan (EX-LE5), Dubi (ST35), Yinlingquan (SP9), Xuehai (SP10), and Yanglingquan (GB34),15 target localized symptoms like pain and stiffness around the knee joint. Distal points, such as Quchi (LI11), are selected based on the meridian theory to address systemic symptoms indirectly.16 Combined approaches integrate local and distal acupoints to treat both localized and systemic symptoms.17 In summary, these methods, are commonly based on empirical practice and traditional theories, lacking of scientific rigor and broad applicability.18
According to TCM, acupoints associated with specific conditions may exhibit sensitization, characterized by localized changes such as increased skin temperature, redness, swelling, or tenderness.19,20 Sensitized acupoints are thought to reflect underlying pathological changes, providing a potential basis for personalized acupoint selection. In previous work by our research team, infrared thermography was employed to study KOA patients, revealing that localized skin temperature patterns are closely related to clinical symptoms and inflammatory markers. These findings provided an objective foundation for developing individualized acupuncture protocols.21
In recent years, advancements in artificial intelligence (AI) have created new opportunities in precision medicine. By integrating AI algorithms with infrared imaging technology, it is possible to significantly enhance the standardization and personalization of acupuncture treatments. Portable devices equipped with infrared cameras can rapidly generate personalized acupoint selection protocols based on patients’ thermal profiles, addressing the limitations of traditional methods such as subjectivity and variability. This approach has the potential to offer more consistent and effective treatment options, improving clinical outcomes.22
This study aims to evaluate the effectiveness of AI-assisted acupoint selection based on and infrared image compared with traditional experience-based methods for treating KOA, laying the groundwork for the standardization and optimization of acupuncture practices and paving the way for broader clinical applications.
Method and Analysis
Study Design
This study is a multi-center, randomized, sham-controlled, parallel, participant- and assessor-blinded clinical trial. The study will be conducted simultaneously at four hospitals: Shanghai Yangzhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Hainan Branch of Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, and Zhongshan Hospital of Traditional Chinese Medicine. The trial is registered with the Chinese Clinical Trial Registry (ChiCTR2400087106). Figure 1 presents the flowchart for the trial process, while Table 1 details the schedule for enrollment, treatment, and assessment. Participants will be recruited through hospital outpatient clinics, community education campaigns, and online advertisements. Recruitment posters and brochures will be displayed in relevant departments such as orthopedics and traditional Chinese medicine. Interested individuals may contact the research team directly using the information provided in the materials, or be followed up by the study coordinator based on registration records to confirm eligibility and complete the screening process.
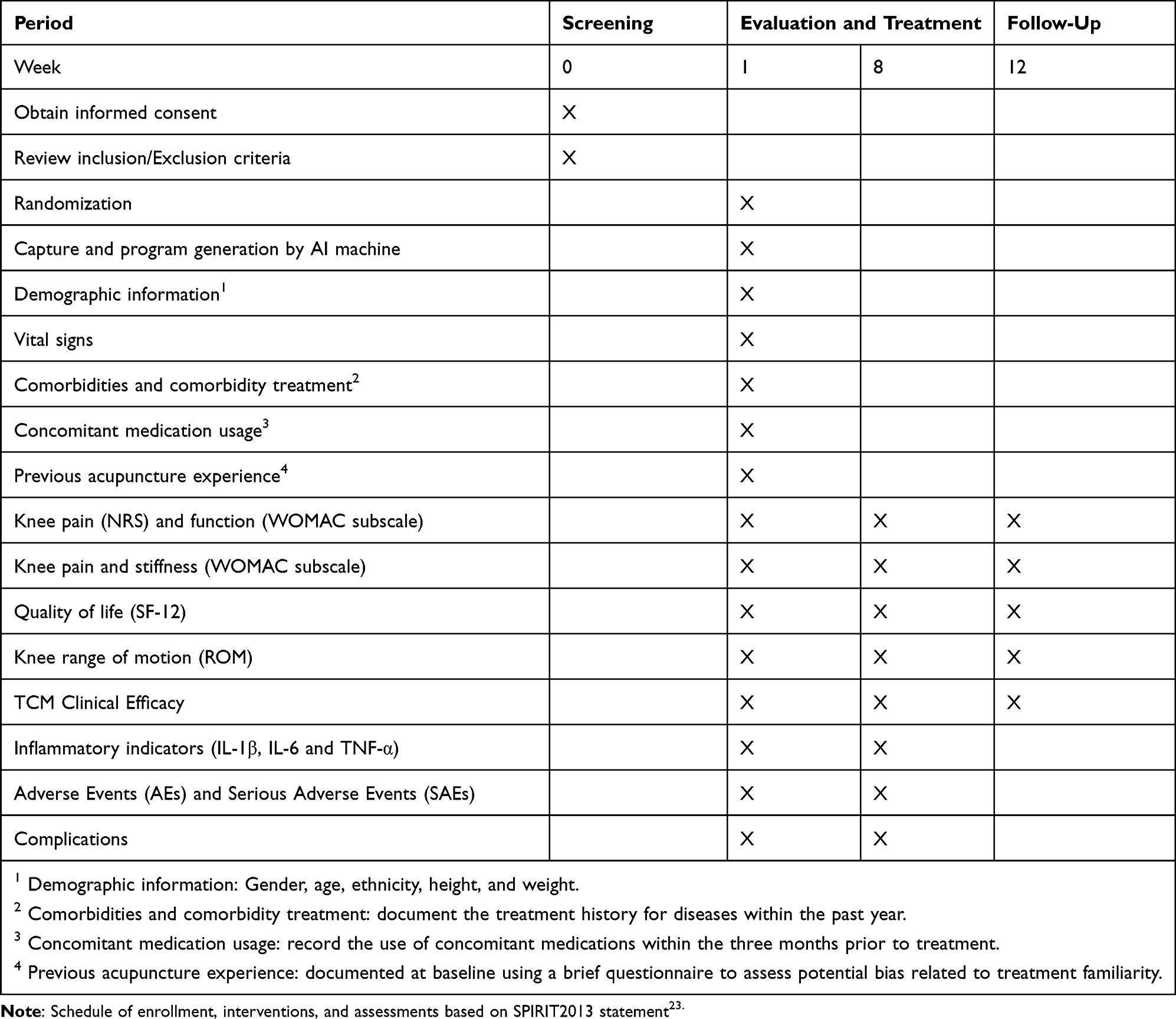 |
Table 1 Study Design Schedule |
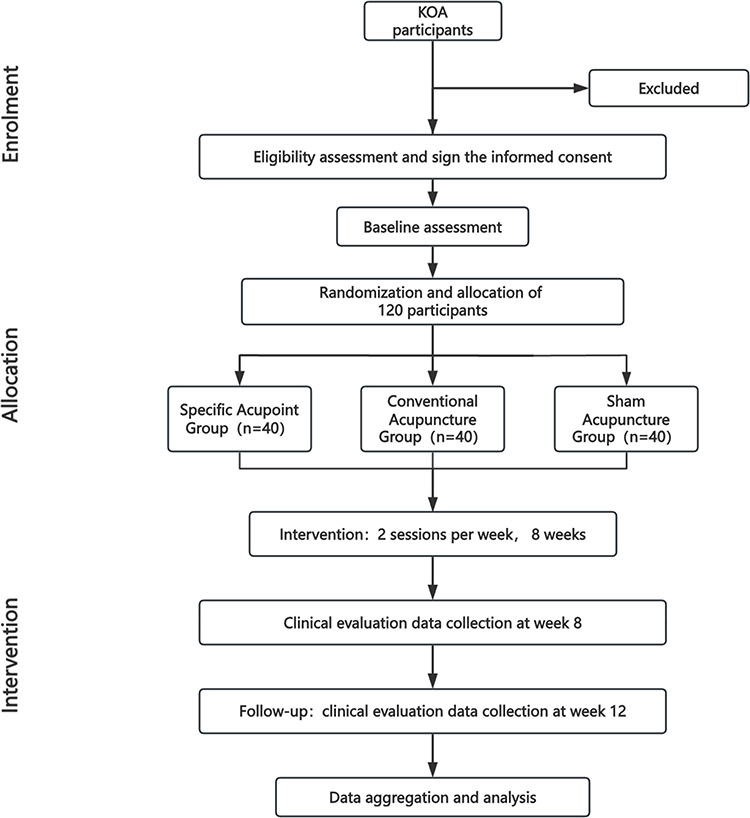 |
Figure 1 Flow chart of the study. |
Inclusion Criteria
Only patients who meet all of the following criteria will be recruited: (1) Meeting the clinical diagnostic criteria for KOA as defined by the American College of Rheumatology (ACR);24 (2) Age 50 years or older; (3) Knee pain lasting more than 3 months; (4) NRS pain score of 4 or higher out of 10; (5) Radiologic confirmation of KOA, classified as Kellgren-Lawrence grade II or III.25
Exclusion Criteria
Patients meeting any of the following criteria will not be eligible for inclusion: (1) History of systemic arthritis; (2) Have had knee surgery or are awaiting knee surgery; (3) Any other condition that affects the function of the lower extremities (eg, trauma, malignant tumors, neurological disorders); (4) Have received any knee injections (eg, adrenocorticotropic hormone, hyaluronic acid) within the past 6 months; (5) Current use of oral or injectable anticoagulant medications; (6) Used acupuncture therapy within the past 3 months; (7) Have any bleeding disorders. (8) Referred to a pain clinic or use of morphine or pethidine within the last 6 months; (9) Any other medical condition that makes them unsuitable for participation in a clinical trial (eg, kidney or liver disease, deep vein thrombosis); (10) Unable to provide written informed consent.
Discontinuation Criteria and Modification
During the trial, patients with KOA who meet any of the following criteria will be excluded from the study: (1) violation of the study protocol, such as taking the unauthorized types of analgesics without approval or receiving additional treatments that could interfere with the effectiveness of acupuncture; (2) withdrawal of consent to participate, indicating the patient no longer wishes to continue in the study; (3) missing more than 4 out of the 16 scheduled acupuncture sessions; or (4) the occurrence of a serious adverse event that, in the opinion of the medical team, warrants discontinuation of the patient’s participation.
Random Allocation
Eligible participants will be randomly assigned to three groups in a 1:1:1 ratio. An independent researcher, who is not involved in the trial, will generate the randomization sequence using SAS version 9.4, stratified by enrolling hospitals with random block sizes of 6. The randomization scheme is concealed using opaque envelopes, each labeled with a unique code and sealed before being handed over to the researchers for safekeeping. After a participant has met all selection criteria, signed the informed consent form,26 and completed the baseline assessments, the evaluator informs the acupuncturists. The acupuncturists will open the envelope according to the participant’s screening sequence number and then assign the participant to one of the three groups: the AI-assisted personalized acupoint group, the conventional acupuncture group, and the sham acupuncture group.
Blinding
In this study, acupuncturists providing the treatment are unable to be blinded; they are fully aware of the treatment allocation to ensure proper administration according to the assigned group. However, participants in the study are blinded, and the outcome assessors and statisticians are completely unaware of the randomization and do not participate in the treatment process. To ensure effective blinding, participants will be treated in separate rooms to prevent communication regarding their treatment protocols. Furthermore, all participants underwent the capture and AI program generation before treatment, regardless of whether they were in the conventional or sham group. From the patient’s point of view, they all accepted the acupuncture treatment plan provided by the machine after evaluation. Therefore, it was impossible to distinguish which acupoints were used in treatment or sham control. Acupuncturists will not disclose any information about the treatment programs to the participants. Group assignments will remain concealed from both outcome assessors and data analysts. Unblinding will only occur after the completion of data analysis. In the data summary stage, the three separation principles of researcher, operator, and statisticians will be implemented.
Sample Size
We aim to detect a minimal clinically important difference (MCID) of 6 units in the WOMAC function (0–68 scale)27 and 1.8 units in the NRS pain score (0–10 scale).28 Based on previous clinical data,29 we expect a standard deviation of 12.0 for function and 3.0 for pain. ANCOVA (Analysis of Covariance) will be used, assuming baseline-to-12-week correlations of 0.70 for function and 0.50 for pain. To detect a 6-unit difference in function with 90% power at a two-sided alpha of 0.05, 32 participants per group are required. This sample size also provides 85.8% power to detect a 1.8-unit change in pain. Allowing for a 20% dropout rate, we will enroll a total of 120 participants (40 per group: specific acupoint, conventional acupoint, and sham acupuncture). In summary, this sample size ensures adequate power to detect clinically meaningful differences in the co-primary outcomes—WOMAC function and NRS pain scores—thereby supporting a robust evaluation of AI-assisted personalized knee infrared imaging acupuncture versus conventional and sham acupuncture in patients with KOA.
Concurrent Treatments
We will record the clinical history of any diagnosed diseases other than those listed in the exclusion criteria, along with current medications being taken. During the trial, participants will be advised to avoid using additional therapies to relieve knee pain. However, for ethical considerations, Celebrex (celecoxib) may be used as a standardized rescue medication when necessary. The recommended dosage is 200 mg per day (one 0.2 g tablet, Pfizer Inc)., with a maximum continuous use of five days. All rescue medication use will be documented in detail, including the medication name, dosage, frequency, timing, and time to pain relief.
Assessment of Safety
Throughout the trial, AEs will be monitored and documented using standardized safety assessment forms, capturing the timing, severity, frequency, and duration of each event. Common AEs associated with acupuncture include dizziness, bleeding, pain, hematoma, and other potentially serious reactions. Although no definitive cases of acupuncture-induced infection have been reported in the literature, local skin infections may still occur due to needle penetration of the subcutaneous layer, even after proper skin disinfection. If an infection is suspected, the needle will be removed immediately, and appropriate skin care and etiological evaluation will be conducted in consultation with the dermatology department. Antibiotic therapy will be initiated if necessary. Adverse events related to the use of Celebrex, including potential gastrointestinal and cardiovascular side effects, will also be carefully monitored.30 For any AE, immediate emergency measures will be taken, and details will be thoroughly recorded in the Case Report Form (CRF). In the event of a SAE, the research ethics committee will determine whether the participant should be withdrawn from the study. Participants may voluntarily withdraw at any time if they experience discomfort or adverse reactions. If unblinding is required for the clinical management of an SAE, the principal investigator will perform emergency unblinding according to a predefined protocol, and all relevant documentation will be submitted to the ethics committee for review. To minimize loss to follow-up, participants will receive a modest transportation subsidy and regular follow-up reminders. For those who withdraw or are lost to follow-up, the reasons for withdrawal and available clinical data will be collected as far as possible and included in the Intention-To-Treat (ITT) analysis when applicable. No independent Data Monitoring Committee (DMC) has been established for this trial due to its small scale, short duration, and low-risk nature. Instead, internal monitoring will be performed by the principal investigator and research coordinators, with regular auditing of data completeness and adverse events reporting. The research team has no financial conflict of interest with the study sponsor.
Interventions
This trial is divided into three groups: the specific acupoint group, the conventional acupuncture group, and the sham acupuncture group, receiving acupuncture based on AI-assisted infrared image based acupoints, conventional acupoints, or sham acupoints, respectively. Apart from the experimental scheme, patients will be advised not to use any other methods for the treatment of KOA. The knees of all subjects were captured using AI machine information collection and infrared images at baseline information collection, followed by different interventions based on randomized groups. To ensure data consistency across all four participating centers, all infrared imaging devices will undergo standardized calibration before the initiation of the trial and regular recalibration every three months, following the manufacturer’s technical specifications. Imaging sessions will be conducted in temperature-controlled rooms maintained at 24±1°C and a relative humidity of 45–60%, without direct sunlight or strong airflow. Prior to image acquisition, participants will rest quietly in the imaging room for at least 15 minutes to achieve thermal equilibrium. All centers will use the same infrared imaging device model (Shanghai Dashi Medical Technology Co., Ltd.) and follow a unified operating protocol to minimize inter-site variability and ensure data comparability. The AI-assisted acupoint selection strategy is presented in Figure S1, while the machine’s appearance is shown in Figure S2A. All needling procedures at each center are performed by a designated TCM practitioner with at least 10 years of clinical experience and rigorous training. Each hospital has three acupuncturists, who are responsible for only one type of acupuncture treatment according to a randomized treatment protocol provided by independent researchers. Before the study, all practitioners are required to attend the operational training for this trial, and the four acupuncturists responsible for the same group of four hospitals will be trained together to standardize the treatment protocols. All groups are required to retain the needles for 30 minutes after needling. The acupuncture treatment will be continued for 8 weeks, 2 times a week. Participants will be contacted by phone prior to each treatment day to remind them of their scheduled session.
To enhance adherence, participants will receive text message or phone call reminders before each scheduled session. Attendance will be recorded, and adherence will be defined as completion of at least 12 of 16 sessions. If adherence falls below 75%, the case will be reviewed. During the trial, use of other KOA treatments (eg, physiotherapy, herbal medicine, other acupuncture therapies) will be prohibited and monitored via patient self-report and regular check-ins. For ethical considerations, participants in the sham acupuncture group will be offered active acupuncture treatment after the completion of the study.
Specific Acupoint Group
The AI system provides precise acupuncture point program for this group by analyzing infrared thermal images of the knee. The logic of the system from data acquisition to program generation is demonstrated in Figure 2. The system calculates the average temperature for each of the five regions of the knee: middle, upper inner, lower inner, upper outer, and lower outer. The diagram of the knee joint region division is provided in Figure S2B. Using the primary acupuncture points and corresponding meridians of different sensitive regions, combined with clinical experience and literature reports, the system establishes acupuncture prescription rules for the sensitized areas of KOA. It finally forms a comprehensive acupuncture point scheme based on the corresponding TCM meridians for these regions, integrating commonly used and clinically experienced points, with all selected acupoints listed in Table S1, and the acupuncture point program is displayed on the smartphone interface as shown in Figure S2C. During acupuncture treatment, patients are required to lie supine on the treatment bed, maintaining stillness and adopting a comfortable posture throughout the entire process. Before treatment commences, the TCM doctor first disinfects the acupoints locally with 75% alcohol and then inserts disposable acupuncture needles (0.25mm in diameter, 40mm in length, Yunlong, Wujiang, China) vertically into designated acupoints to a depth of 25 to 40 millimeters. Subsequently, acupoints are stimulated through lifting, thrusting, and rotating motions until the patient experiences the Deqi sensation. The term “Deqi” refers to a composite sensation (such as numbness, soreness, or heaviness) that is felt after needle insertion and manual stimulation, and is believed to be crucial to acupuncture efficacy.
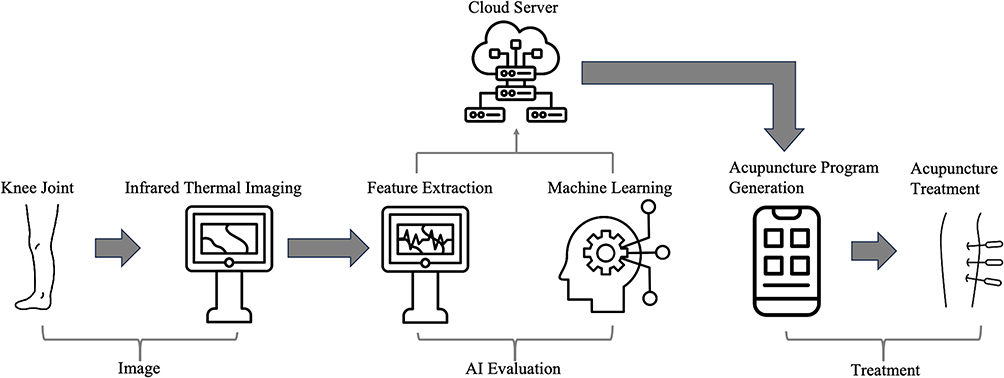 |
Figure 2 The logic of the system from data acquisition to program generation. |
Conventional Acupuncture Group
When choosing the conventional acupuncture points, we will determine the locations of the acupoints using the nomenclature and locations of acupuncture points specified in the National Standard of the People’s Republic of China (GB/T 12346–2006) including SP9 (Yinlingquan), GB34 (Yanglingquan), EX-LE4 (Neixiyan), ST36 (Zusanli), BL40 (Weizhong), SP10 (Xuehai) and ST34 (Liangqiu), which are mainly located around the knee (Table 2). Furthermore, an Ashi acupoint (where the patient feels the most pain) will be added based on the patient’s condition. Practitioners also need to lift, thrust, and rotate needles to make patients feel Deqi when inserting acupuncture needles.
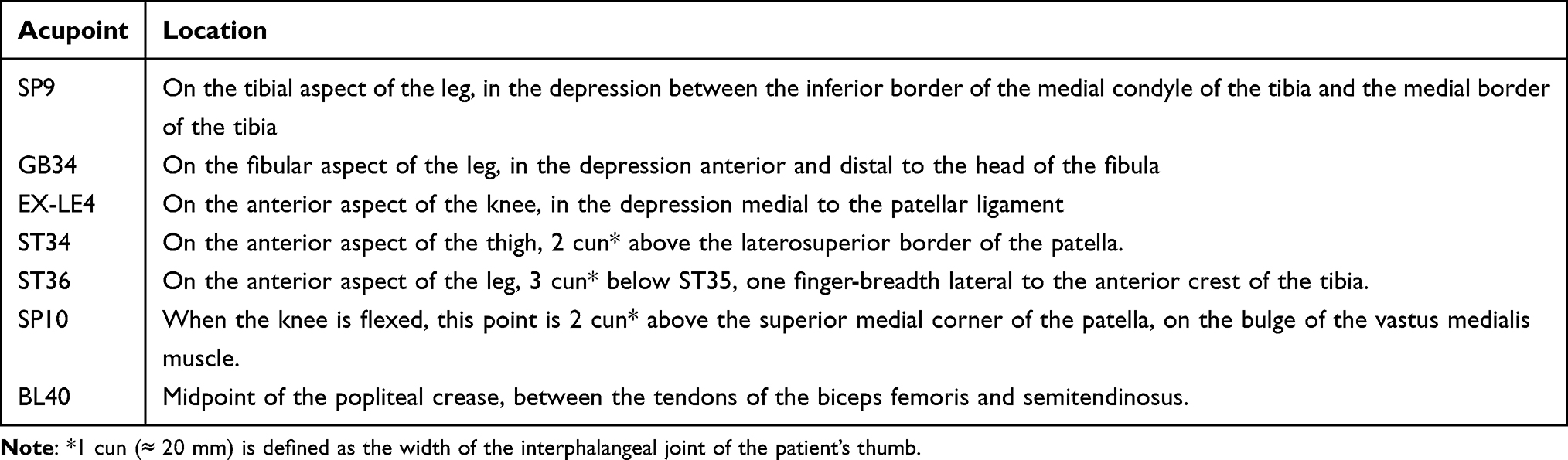 |
Table 2 Locations of Acupoints for Conventional Acupuncture Group |
Sham Acupuncture Group
Sham acupuncture will be administered at eight predefined non-acupuncture points located away from recognized meridians, acupoints, nerve bundles, motor points, and myofascial trigger points (see Table 3). The procedure will mirror that of the other groups, except that needles will be inserted superficially (<5 mm) without manual stimulation or elicitation of the Deqi sensation.31
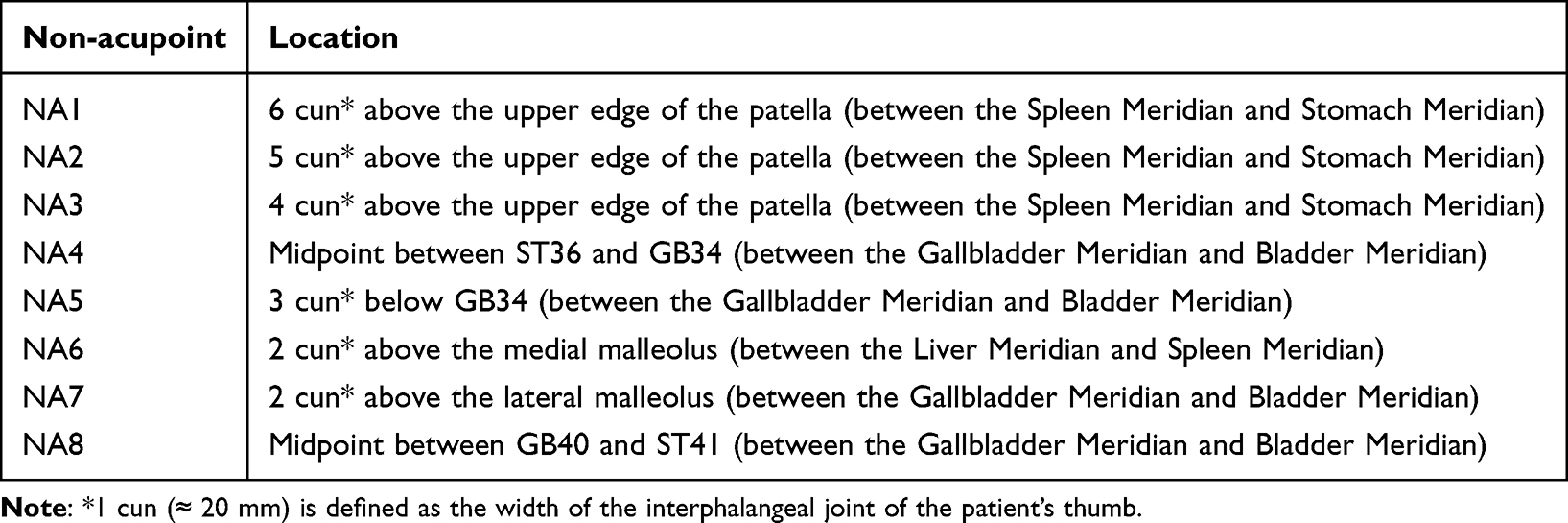 |
Table 3 Locations of Non-Acupoints for Sham Acupuncture Group |
Outcome Measures
In cases where both knees meet the inclusion criteria, the knee with greater pain will be selected as the target knee for both intervention and analysis. Only the target knee will receive acupuncture treatment to avoid potential cross-intervention effects. If both knees are symptomatic but only one meets the inclusion criteria, the intervention and evaluation will still be limited to that single knee (see Table 4).
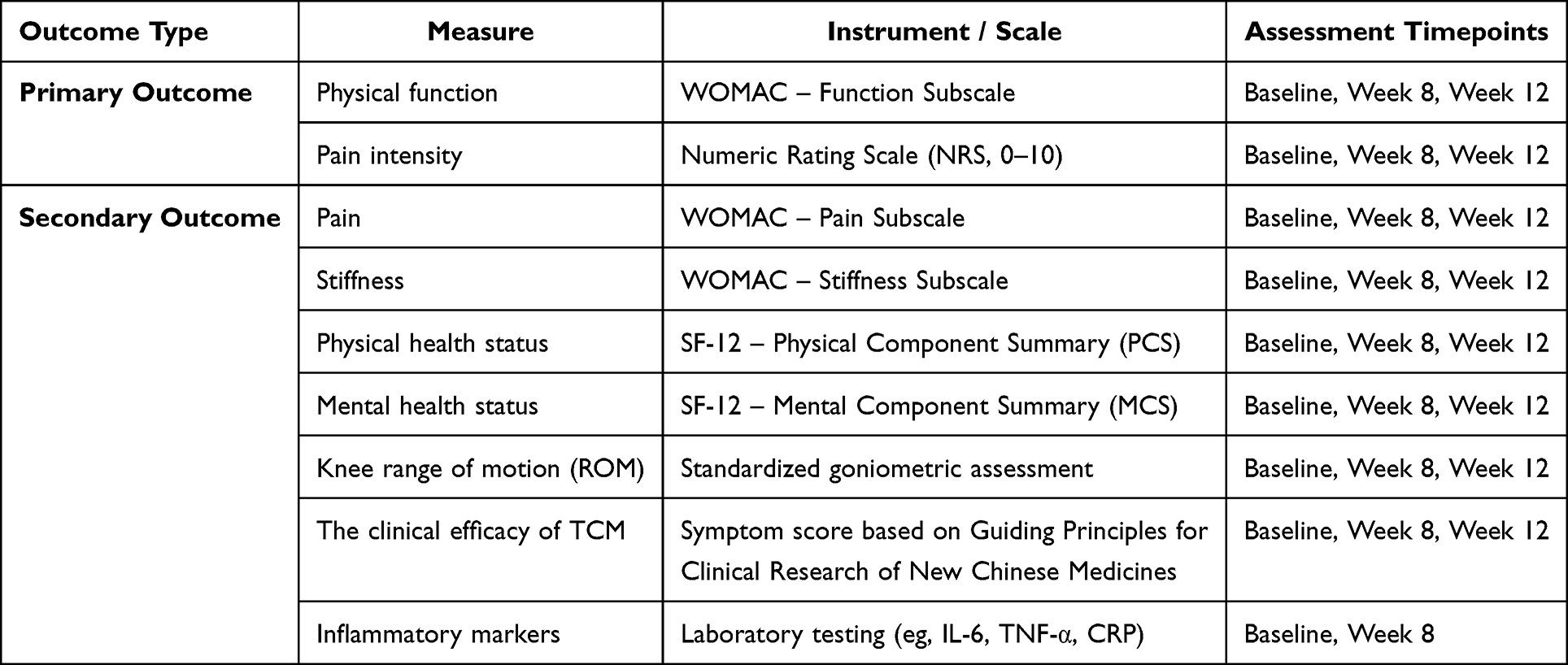 |
Table 4 Summary of Outcome Measures |
Primary Outcomes
Knee function and pain are defined as co-primary outcomes in this study. Functional status was assessed using the function subscale of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC, Likert 3.1 version), and knee pain was evaluated using the Numeric Rating Scale (NRS).32 The WOMAC function subscale includes 17 items assessing difficulty in performing daily activities.33 Each item is scored on a 5-point Likert scale: none (0), mild (1), moderate (2), severe (3), and extreme (4), with total scores ranging from 0 to 68. Higher scores indicate worse knee function.34 For patients with bilateral knee involvement, the more severely affected side was used for scoring. Pain was assessed based on average knee pain experienced over the past week, using an 11-point NRS ranging from 0 (no pain) to 10 (worst imaginable pain). Pain levels were further categorized as: 1–3=mild (does not affect sleep), 4–6=moderate (slightly affects sleep), 7–9=severe (prevents sleep or causes awakening), and 10=extreme pain.35 Patients rated their pain by selecting the number that best matched their experience.
Secondary Outcomes
- The WOMAC subscales for knee pain (5 items, score range 0–20) and stiffness (2 items, score range 0–8) will be used for assessment. For patients with bilateral knee involvement, the more severely affected side will be scored. Patients will report their average knee pain and stiffness over the past week.
- The SF-12 questionnaire will be used to assess patients’ quality of life,36 covering both physical and mental health domains. It consists of 12 items, each scored across a range of responses, with higher scores reflecting better health status. The SF-12 produces two summary scores: the Physical Component Summary (PCS) and the Mental Component Summary (MCS), both standardized to a population mean of 50 and a standard deviation of 10. This provides a comprehensive evaluation of physical and mental health functioning across multiple dimensions.
- Knee ROM is a key functional assessment that evaluates the movement range of the knee joint. It is commonly used in assessing knee conditions such as osteoarthritis, post-operative rehabilitation, and other disorders affecting joint mobility. Knee ROM includes flexion, extension, internal rotation, and external rotation. To measure knee mobility, we used a multifunctional movable angle ruler with a 180-degree steel angle (double arm’s length 250 mm, YMD, Y282), as shown in Figure S2D. For active ROM measurement, patients were instructed to move their knee independently, while for passive ROM measurement, the researcher assisted the patient in moving the knee while the patient remained immobile.
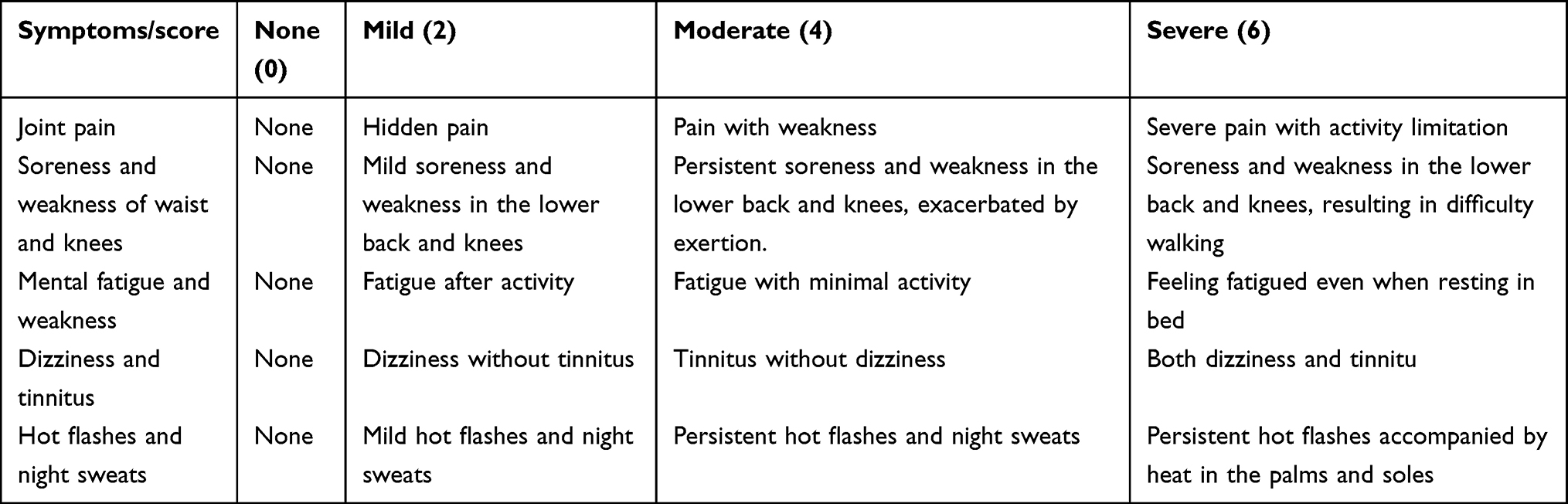
- The clinical efficacy of TCM will be assessed based on the Guiding Principles for Clinical Research of New Chinese Medicines.37 Treatment efficacy for KOA will be evaluated by scoring five primary TCM symptoms before and after treatment (refer to Table 5). The percentage reduction in symptom scores will be used to determine efficacy, with classifications defined as follows: Clinical Cure is defined as the disappearance or near disappearance of TCM clinical symptoms and signs, with a symptom score reduction of ≥95%; Significantly Effective indicates marked improvement, with a score reduction of 70% to <95%; Effective refers to general improvement, with a score reduction of 30% to <70%; and Ineffective is defined as no significant improvement or worsening of symptoms and signs, with a score reduction of <30%.
- The detection of inflammatory indicators was conducted by collecting fasting venous blood samples (2 mL) from participants in both groups before and after treatment. The samples were centrifuged, and the assays were performed strictly following the instructions provided in the reagent kit manual. Optical density (OD) values were measured at a wavelength of 450 nm using a microplate reader. A standard curve was plotted with the standard concentrations as the x-axis and the corresponding OD values as the y-axis. Based on this curve, the serum levels of interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) were calculated.

Table 5 Chinese Medicine Clinical Symptom Score
Statistical Analysis
The primary analysis of this study will follow the Intention-to-Treat (ITT) principle. The Full Analysis Set (FAS), serving as the primary analysis population, will include all randomized participants, analyzed according to their original group assignment, regardless of adherence to the intervention protocol. Participants who were randomized but did not receive any treatment or who lack all post-randomization efficacy data will be excluded from the FAS in accordance with standard practice. The Per-Protocol Set (PP) will be used for secondary or sensitivity analyses. It will include participants with valid baseline data who completed the assigned intervention and follow-up as per protocol, and who met all inclusion criteria without violating any exclusion criteria. The Safety Analysis Set (SAS) will consist of all randomized participants who received at least one treatment session and will be used to evaluate adverse events and treatment-related safety. Continuous variables will be summarized as means ± standard deviations, while categorical variables will be expressed as frequencies (percentages). Differences in mean changes from baseline for each outcome will be compared between groups using a mixed-effects linear regression model, with baseline outcome scores as covariates. The model will include fixed effects for group, time, and their interaction, and random intercepts for participants to account for within-subject correlations. Least squares mean differences and 95% confidence intervals will be estimated for each group at each time point. Interaction terms will be assessed to determine whether treatment effects vary over time. Post-hoc pairwise comparisons will be conducted to examine between-group differences and within-group changes. Given the inclusion of multiple secondary outcomes (eg, WOMAC subscales, SF-12, and inflammatory markers), appropriate corrections for multiple comparisons—such as the Bonferroni adjustment—will be applied to control for Type I error and ensure the robustness of statistical inferences.A two-tailed p value <0.05 will be considered statistically significant unless otherwise adjusted. Sensitivity analyses will adjust for Celebrex use and participants’ previous acupuncture experience, both of which will be included as covariates to control for potential confounding. In addition, exploratory subgroup analyses will be conducted to investigate potential effect modifiers. Subgroups will be stratified by baseline disease severity (Kellgren–Lawrence grade II vs III), age (<65 vs ≥65 years), and previous acupuncture experience. These analyses aim to explore differential treatment responses across patient subgroups and enhance the precision and clinical relevance of the findings. All statistical analyses will be performed using SPSS for Windows (Version 21.0, SPSS, Chicago, IL, USA).
Discussion
Our study lies on the explanatory-pragmatic continuum. The explanatory component of the research derives from the rigorous sham-controlled design, which aimed at isolating the specific physiological effects of acupuncture beyond placebo. At the same time, the fact that our study targeted the primary clinical outcomes of pain and function in OA and was consistent with commonly used interventions over 8 weeks brings a pragmatic aspect to our study. Furthermore, our investigation combines traditional concepts of acupuncture with innovative methodologies, including thermosensitive mechanisms and AI-assisted acupoint selection. While traditional acupoint selection often relies on the subjective expertise of practitioners, our study incorporates objective measures, such as infrared imaging to detect thermal variations, combined with AI algorithms to optimize acupoint selection. The AI system used in this study is built upon a rule-based decision tree model, employing a structured if–then logic framework. Its core algorithm is derived from consensus opinions of experienced traditional Chinese medicine (TCM) practitioners. By encoding clinical expertise and interpretation principles of infrared thermographic images, the system analyzes knee infrared images to generate personalized acupoint prescriptions.Prior to the formal initiation of this clinical trial, we conducted a preliminary validation study involving infrared thermographic data from 30 patients with knee osteoarthritis. In that study, the prescriptions generated by the AI system were independently compared with those formulated by two senior acupuncture experts, who were blinded to the AI output. The results showed an agreement rate of over 80%, with no significant clinical discrepancies observed, providing preliminary evidence for the system’s reliability and clinical potential. Furthermore, to ensure the safety and appropriateness of the treatment plans, all AI-generated prescriptions in this study are reviewed and confirmed by licensed acupuncture physicians before being implemented. Such an approach not only increases the precision of the intervention but also establishes a more systematic and reproducible framework for acupuncture therapy.
Moreover, the current version of the AI model focuses on identifying thermosensitive regions and mapping them to corresponding meridians, rather than performing direct TCM syndrome differentiation. However, the rule base underlying the algorithm was developed based on expert consensus that integrates acupoint selection principles applicable across the common syndrome patterns of KOA, such as “cold-damp obstruction”, “qi and blood stagnation” and “liver-kidney deficiency”. This design ensures a degree of adaptability across varying clinical manifestations. In future iterations, we plan to incorporate syndrome-specific diagnostic information (eg, symptoms, tongue, and pulse data) into the AI framework to enable syndrome-guided, individualized acupoint selection and further enhance clinical precision.
Additionally, the AI system applied in this study does not rely on absolute temperature values, but rather identifies thermally sensitized areas by analyzing the relative temperature differences within each predefined region of the knee. The system automatically detects the highest and lowest temperature points in each region to locate the most thermally active zones. To address the potential interference caused by excessive local heating in patients with severe inflammation, a thermal normalization and outlier correction process has been incorporated into the algorithm. Specifically, when abnormally high temperatures are detected in a localized region, the system automatically limits the influence of these outlier pixels and applies spatial smoothing to ensure that the identified acupoints align with anatomically valid positions. This design minimizes potential misidentification due to extreme temperature elevations while maintaining clinical interpretability and acupoint accuracy. This strategy ensures that even with slight fluctuations in ambient temperature, the relative thermal distribution remains stable across regions, thereby enhancing the robustness, consistency, and generalizability of thermal data interpretation in various clinical settings. This study aims to address critical challenges in acupuncture research by introducing an AI-assisted, evidence-based methodology for acupoint selection. By combining modern technology with traditional practices, this research seeks to enhance the reliability, reproducibility, and therapeutic efficacy of acupuncture for KOA.
Thermosensitive acupoints are specific regions that exhibit increased sensitivity to thermal stimulation, often associated with local temperature elevations due to inflammation or pathological changes. Research has shown that temperature variations in these regions may reflect underlying lesions. For example, studies by Japanese scholar Kohei Akabane indicated that monitoring temperature along meridians can help identify acupuncture points associated with pathological conditions.38 Studies on heat-sensitive moxibustion for KOA have shown that this treatment significantly alleviates pain and reduces pro-inflammatory cytokine levels, such as TNF-α, IL-1, and IL-6. A randomized controlled trial comparing conventional moxibustion and heat-sensitive moxibustion found the latter to be more effective in improving clinical symptoms, lowering inflammatory marker levels, and reducing adverse reaction rates.39 This provides a scientific basis for acupuncture therapy. Based on these findings, our proposed AI-assisted infrared imaging acupuncture system uses localized infrared imaging to detect thermal variations and map them to the corresponding meridians. Based on the identified meridian, the system selects appropriate acupoints from a pre-defined pool of acupoints associated with that meridian, providing a balance between precision and holistic intervention. This method transcends the traditional focus on local acupuncture points alone by incorporating a systematic approach to optimize acupuncture point selection across the entire body.
Traditional acupoint selection in acupuncture often relies on the practitioner’s expertise and theoretical knowledge. While this approach can be effective, it lacks the systematic and reproducible framework necessary for widespread clinical application. To address these limitations, our proposed system integrates AI with infrared imaging technology to capture temperature variations in the knee joint and analyze them using AI algorithms. This allows the identification of the most suitable acupoints for treatment based on localized temperature changes, combined with meridian theory in TCM to establish correlations between pathological regions and meridians. Compared to traditional methods that rely heavily on practitioner experience, this system offers the potential to reduce subjectivity and variability in acupoint selection, thereby aiming to improve standardization and reproducibility in acupuncture treatment. Moreover, if its effectiveness can be validated, this innovative technology could enhance the accuracy of acupoint selection, optimize treatment efficiency, and bolster the credibility and acceptance of acupuncture therapy in clinical medicine. By merging modern technology with TCM principles, this approach paves the way for the development of personalized and scientifically grounded acupuncture treatment strategies.
In this study, the design of the intervention groups was carefully crafted to reflect both traditional practices and modern innovations, ensuring a robust comparison to evaluate the efficacy of AI-assisted personalized acupuncture. In the conventional acupuncture group, the points primarily target pain and functional dysfunction localized around the knee joint, such as SP9, GB34, and ST36, combined with patient-specific Ashi points. This group reflects the most commonly used protocols in clinical practice, ensuring a reliable comparison with the specific and sham groups. To rigorously assess the specific effects of acupuncture, the sham acupuncture group was designed with strict controls. Non-acupoints located away from recognized meridians were selected, with needle insertion limited to 5 mm and no Deqi sensation induced. The “Deqi” sensation, characterized by soreness, numbness, heaviness, or distention, represents a distinct neurosensory phenomenon rather than a local inflammatory response. Mechanistically, Deqi arises from the activation of Aδ and C afferent fibers and the subsequent modulation of central pain inhibitory and autonomic pathways. While mild, transient changes in local microcirculation and neuroimmune signaling may accompany Deqi, these responses differ fundamentally from the immune-mediated cascade underlying inflammation. Emerging evidence suggests that Deqi may indirectly modulate inflammatory activity by influencing neuroimmune balance, which could contribute to symptom improvement in KOA. However, Deqi itself does not indicate tissue inflammation but reflects effective neural engagement during acupuncture stimulation. While we acknowledge that even superficial needling at non-acupoint locations may elicit certain physiological responses, these measures were deliberately chosen to minimize the specific therapeutic effects associated with acupuncture. Importantly, this approach is consistent with internationally accepted standards for sham-controlled acupuncture trials and serves as a reasonable and widely adopted comparator that preserves participant blinding while minimizing physiological interference as much as possible.40,41
Besides, we chose an intervention period of 8 weeks, with two sessions per week based on evidence from previous studies that this schedule is sufficient to produce measurable improvements in chronic conditions such as KOA. Two primary outcomes, including the NRS for pain and the WOMAC function subscale, were chosen to comprehensively assess the effect of treatment on both symptom relief and functional improvement. This approach ensures a balanced assessment of subjective and objective therapeutic benefits.
In short, by designing a rigorous research protocol, including controlling for nonspecific effects and employing sham acupuncture in the control group, we aim to provide reliable evidence to assess this technology’s scientific and clinical value. If the study is successfully implemented and yields the expected results, it would provide modern scientific support for traditional acupuncture therapy while offering a novel non-pharmacological treatment option for KOA patients. This innovative approach, grounded in rules and evidence, promises to modernize and enhance the credibility of traditional acupuncture treatment.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author Yan Xue upon reasonable request from qualified researchers.
Ethics Approval and Informed Consent
The study protocol (Version 2.0, dated January 26, 2024) has been approved by the Ethics Committee of Shanghai Yangzhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center) (2023-040), the Ethics Committee of Shuguang Hospital affiliated with Shanghai University of Traditional Chinese Medicine (2024-1525-108-01), the Ethics Committee of Zhongshan Hospital of Traditional Chinese Medicine (2024ZSZY-LL-KY-008), and the Ethics Committee of the Hainan Branch of Ruijin Hospital affiliated with Shanghai Jiao Tong University School of Medicine (Hainan Boao Research-Based Hospital) (KY2024-007).
Prior to randomization, all participants were required to provide written informed consent. The consent process was conducted face-to-face by trained research staff and included a comprehensive explanation of the study’s purpose, procedures, potential risks and benefits, and participant rights. Participants were explicitly informed that the study involves the use of an AI system to assist in acupoint selection based on infrared imaging. The AI system’s function as a non-autonomous decision-support tool was clarified, and participants were assured that all treatments would be administered by licensed acupuncture physicians. Ample time was provided for participants to ask questions, and participation was entirely voluntary, with the right to withdraw at any time without penalty. All participants signed the informed consent form only after confirming full understanding and agreement. This study adheres to the ethical principles outlined in the Declaration of Helsinki.
Acknowledgments
The authors would like to sincerely thank all participants, research staff, and supporting institutions for their valuable cooperation and contributions to the development of this study protocol.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, development of the protocol, methodology refinement, or manuscript preparation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Neither patients nor the public were involved in the development of this clinical trial protocol.
Funding
The National Natural Science Foundation of China (82305269,82274553), Clinical Research Project of Shanghai Municipal Health Commission (20224Y0209), Research Physicians Innovation and Transformation Ability Training Project of Shanghai Hospital Development Center (SHDC2023CRS045), National Key Clinical Specialty Discipline Construction Project of China(Z155080000004), Shanghai Research Center of Rehabilitation Medicine (Top Priority Research Center of Shanghai) (2023ZZ02027), Shanghai Hospital Development Center Foundation—Shanghai Municipal Hospital Rehabilitation Medicine Specialty Alliance (SHDC22023304,SHDC22026304), Traditional Chinese Medicine Research Project of Shanghai Municipal Health Commission (2024QN063), Hospital Management Project of Shanghai Hospital Association (X2024032), Special Fund for Promoting High-Quality Industrial Development (2024-GZL-RGZN-02034)and Shanghai Municipal Health Commission Smart Healthcare Special Project (2025ZHYL028).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Salman LA, Ahmed G, Dakin SG et al. Osteoarthritis: a narrative review of molecular approaches to disease management. Arthritis Res Ther. 2023;25(1):27. doi:10.1186/s13075-023-03006-w
2. Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: part I. Caspian J Intern Med. 2011;2(2):205–212.
3. Lv ZT, Shen LL, Zhu B, et al. Effects of intensity of electroacupuncture on chronic pain in patients with knee osteoarthritis: a randomized controlled trial. Arthritis Res Ther. 2019;21(1):120. doi:10.1186/s13075-019-1899-6
4. Hinman RS, McCrory P, Pirotta M, et al. Acupuncture for chronic knee pain: a randomized clinical trial. JAMA. 2014;312(13):1313–1322. doi:10.1001/jama.2014.12660
5. Shan WS, Chi Ho CV. Acupuncture: filling the effectiveness gaps in Western medicine? Br J Gen Pract. 2011;61(587):374–375. doi:10.3399/bjgp11X572607
6. Chen J, Guo H, Pan J, et al. Efficacy of acupuncture combined with active exercise training in improving pain and function of knee osteoarthritis individuals: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1):921. doi:10.1186/s13018-023-04403-2
7. Smith CA, Collins CT, Levett KM et al. Mesgarpour B: acupuncture or acupressure for pain management during labour. Cochrane Database Syst Rev. 2020;2(2):CD009232. doi:10.1002/14651858.CD009232.pub2
8. Jia P, Liu J, Li L, et al. Acupuncture for knee osteoarthritis with sensitized acupoints: results from a pilot, feasibility randomized controlled trial. Pilot Feasibility Stud. 2020;6:144. doi:10.1186/s40814-020-00687-x
9. Atalay SG, Durmus A, Gezginaslan O. The effect of acupuncture and physiotherapy on patients with knee osteoarthritis: a randomized controlled study. Pain Physician. 2021;24(3):E269–E278. doi:10.36076/ppj.2021/24/E269
10. Wang M, Liu W, Ge J et al. The immunomodulatory mechanisms for acupuncture practice. Front Immunol. 2023;14:1147718. doi:10.3389/fimmu.2023.1147718
11. Zhao JP, Chen S, Marmori F, et al. Disease location identification as a major guide to acupoint selection. Chin J Integr Med. 2013;19(12):894–899. doi:10.1007/s11655-013-1650-0
12. Zhang Q, Fang J, Chen L, et al. Different kinds of acupuncture treatments for knee osteoarthritis: a multicentre, randomized controlled trial. Trials. 2020;21(1):264. doi:10.1186/s13063-019-4034-8
13. Gang WJ, Xiu WC, Shi LJ, et al. Factors associated with the magnitude of acUpuncture treatment effectS (famous): a meta-epidemiological study of acupuncture randomised controlled trials. BMJ Open. 2022;12(8):e060237. doi:10.1136/bmjopen-2021-060237
14. Chen H, Shi H, Gao S, et al. Durable effects of acupuncture for knee osteoarthritis: a systematic review and meta-analysis. Curr Pain Headache Rep. 2024;28(7):709–722. doi:10.1007/s11916-024-01242-6
15. Cai FH, Li FL, Zhang YC, et al. Research on electroacupuncture parameters for knee osteoarthritis based on data mining. Eur J Med Res. 2022;27(1):162. doi:10.1186/s40001-022-00795-9
16. Yu WZ, Huang CM, Ng HP, et al. Distal acupoints outperform proximal acupoints in treating knee osteoarthritis: a randomized controlled trial. Evid Based Complement Alternat Med. 2021;2021:4827123. doi:10.1155/2021/4827123
17. Tam LS, Leung PC, Li TK, et al. Acupuncture in the treatment of rheumatoid arthritis: a double-blind controlled pilot study. BMC Complement Altern Med. 2007;7:35. doi:10.1186/1472-6882-7-35
18. Godson DR, Wardle JL. Accuracy and precision in acupuncture point location: a critical systematic review. J Acupunct Meridian Stud. 2019;12(2):52–66. doi:10.1016/j.jams.2018.10.009
19. Lin L, Jia F, Zhongyong L, et al. Clinical observation of thermal moxibustion in treating 50 cases of angina pectoris. J New Chin Medi. 2011;43(12):82–84.
20. Yan C, Yan X, Ding J, et al. Literature mining and clinical verification of sensitized acupoints in knee osteoarthritis treatment. Shanghai J Traditional Chin Med. 2021;55(08):13–16.
21. Yan X, Hongyang H, Ding J, et al. Study on the correlations between local skin surface temperature of knee joint, clinical symptoms and inflammatory factors in patients with knee osteoarthritis. Mod. J. Integr. Tradit. Chin. West. Med. 2019;28(36):3991–3994+4054.
22. Wang Y, Shi X, Efferth T et al. Artificial intelligence-directed acupuncture: a review. Chin Med. 2022;17(1):80. doi:10.1186/s13020-022-00636-1
23. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
24. Vicky D, Win Min O, Changhai D et al. Evaluation and treatment of knee pain: a review. JAMA. 2023;330(16).
25. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
26. World medical a: world medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
27. Tubach F, Ravaud P, Baron G, et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and Hip osteoarthritis: the minimal clinically important improvement. Ann Rheum Dis. 2005;64(1):29–33. doi:10.1136/ard.2004.022905
28. Bellamy N, Carette S, Ford PM, et al. Osteoarthritis antirheumatic drug trials. III. Setting the delta for clinical trials--results of a consensus development (Delphi) exercise. J Rheumatol. 1992;19(3):451–457.
29. Hinman RS, McCrory P, Pirotta M, et al. Efficacy of acupuncture for chronic knee pain: protocol for a randomised controlled trial using a Zelen design. BMC Complement Altern Med. 2012;12:161. doi:10.1186/1472-6882-12-161
30. Huang H, Liu R, Shao J et al. Biomechanically based Fu’s subcutaneous needling treatment for senile knee osteoarthritis: protocol for a randomized controlled trial. J Orthop Surg Res. 2024;19(1):394. doi:10.1186/s13018-024-04878-7
31. Li PS, Peng XM, Niu XX, et al. Efficacy of acupuncture for endometriosis-associated pain: a multicenter randomized single-blind placebo-controlled trial. Fertil Steril. 2023;119(5):815–823. doi:10.1016/j.fertnstert.2023.01.034
32. Farrar JT, Young JP Jr, LaMoreaux L et al. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
33. Roos EM, Klassbo M, Lohmander LS. WOMAC osteoarthritis index. Reliability, validity, and responsiveness in patients with arthroscopically assessed osteoarthritis. Western Ontario and MacMaster Universities. Scand J Rheumatol. 1999;28(4):210–215. doi:10.1080/03009749950155562
34. Shen ZD, Yu HM, Wang JT et al. Modified western ontario and mcmaster university osteoarthritis index scale used in patients with knee osteoarthritis. Zhonghua Yi Xue Za Zhi. 2019;99(7):537–541. doi:10.3760/cma.j.issn.0376-2491.2019.07.012
35. Hawker GA, Mian S, Kendzerska T et al. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–252.
36. Lam CL, Tse EY, Gandek B. Is the standard SF-12 health survey valid and equivalent for a Chinese population? Qual Life Res. 2005;14(2):539–547. doi:10.1007/s11136-004-0704-3
37. Xiaoyu Z. Guiding Principles for Clinical Research of New Drugs of Traditional Chinese Medicine Trial Implementation (in Chinese). Beijing: China Pharmaceutical Science and Technology Publishing House; 2002.
38. Medicine SUoTC: Acupuncture. Meridian Theory: Shaohua Cultural Service Center; 1970.
39. Ji L, Shuang L. Effect of heat-sensitive moxibustion on pain and expressions of tnf-α and il-1 in patients with KOA. J. Clin. Acupunct. Moxi. 2020;36(06):55–58.
40. Lundeberg T, Lund I. Are reviews based on sham acupuncture procedures in fibromyalgia syndrome (FMS) valid? Acupunct Med. 2007;25(3):100–106. doi:10.1136/aim.25.3.100
41. Moffet HH. Sham acupuncture may be as efficacious as true acupuncture: a systematic review of clinical trials. J Altern Complem Med. 2009;15(3):213–216. doi:10.1089/acm.2008.0356
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.