Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Age at Menarche and Its Association with Cardiovascular Disease in Women with Childhood-Onset Type 1 Diabetes (T1D)
Authors Ju J ![]() , El Khoudary SR, Buchanich JM, Orchard TJ, Costacou T
, El Khoudary SR, Buchanich JM, Orchard TJ, Costacou T ![]()
Received 12 November 2025
Accepted for publication 10 January 2026
Published 20 January 2026 Volume 2026:19 579879
DOI https://doi.org/10.2147/DMSO.S579879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Jinghui Ju,1 Samar R El Khoudary,1 Jeanine M Buchanich,2 Trevor J Orchard,1 Tina Costacou1
1Department of Epidemiology, School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA; 2Department of Biostatistics, School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA
Correspondence: Tina Costacou, Department of Epidemiology, School of Public Health, University of Pittsburgh, 130 N. Bellfield Ave, Pittsburgh, PA, 15213, USA, Email [email protected]
Objective: Early and delayed menarche are associated with increased cardiovascular disease (CVD) risk in the general population, but data are limited in type 1 diabetes (T1D). We thus examined the relationship between menarche age and CVD risk in women with childhood-onset T1D, representing the first study to evaluate the association between menarche timing and macrovascular disease risk in this population.
Methods: Female participants from the Pittsburgh Epidemiology of Diabetes Complications (EDC) prospective cohort study were categorized by menarche age: early (≤ 12 years), normal (13– 15 years), or delayed (≥ 16 years). Coronary artery disease (CAD) and major adverse cardiovascular events (MACE) were ascertained through clinical examination and surveys. Cox regression models were constructed to assess the relationship between menarche age and each outcome.
Results: At baseline, 320 participants were free of CAD and 319 were free of MACE (mean age, 27.8 years; T1D duration, 19.3 years; and median menarche age, 13 years). During 30 years of follow-up, 37.2% developed CAD and 31.3% MACE. A weak, non-significant, U-shaped pattern was observed between menarche age and both outcomes. In multivariable Cox models, compared with normal menarche, early menarche was significantly associated only with higher CAD risk (HR =1.71, 95% CI: 1.11– 2.64); no other significant associations were observed.
Conclusion: Among women with childhood-onset T1D, early menarche is associated with increased CAD risk.
Keywords: age at menarche, coronary artery disease, major adverse cardiovascular events, type 1 diabetes
Introduction
Recently, an increasing number of studies have focused on reproductive health and its influence on cardiovascular disease (CVD) risk in women. In the general population, early menarche has been associated with a greater risk of CVD1–6 and its risk factors,1,2,7–10 such as obesity, hypercholesterolemia, type 2 diabetes and decreased high-density lipoprotein cholesterol (HDL-C) level, in later life. Findings from Mendelian randomization studies11,12 and a mediation analysis13 suggest that the observed relationship between early menarche and elevated cardiometabolic risk in observational studies is partially mediated by excessive adiposity from childhood to adulthood. Evidence, however, also suggests that the association of age at menarche and CVD may not be linear.2,5,6,14–16 A large prospective study in the UK suggested a U-shaped relationship between age at menarche and coronary artery disease (CAD), with both early and late menarche timing increasing CAD risk.14 The Women’s Ischemia Syndrome Evaluation (WISE) study group also recently revealed that early (≤10 years) and late menarche (≥15 years) were both associated with increased risk of major adverse cardiac events (MACE) compared with the reference group with menarche at age 12.5 Indeed, delayed menarche has previously been associated with increased brachial artery diameter and reduced flow-mediated dilation in adulthood, indicating an impairment in the vascular endothelium and vascular function.17
Importantly, type 1 diabetes (T1D) appears to cause a delay in pubertal development through the effects of insulin deficiency and hyperglycemia on the hypothalamic–pituitary–gonadal (HPG) axis, leading to delayed menarche among girls with childhood-onset T1D.18,19 Thus, it is possible that in addition to the effect of early menarche, as seen in the general population, delayed menarche, which is more common in T1D, may also serve as a marker of adverse cardiometabolic health in this population. Indeed, delayed menarche was previously associated with a higher risk of nephropathy in women with T1D,20,21 a complication that contributes to increased CVD risk.22,23 Early menarche, on the other hand, may reflect adiposity-related mechanisms similar to those seen in the general population, as higher BMI z-scores have been consistently associated with younger menarche age.24–27
In the general population, pre-menopausal women typically have a lower risk of CVD compared to men. This lower risk is not seen in individuals with T1D, which means that women face a much higher relative risk of CVD due to T1D compared to men.28–32 However, the reason why T1D has a greater impact on CVD risk among women compared with men, and whether this may at least partly relate to age at menarche, is not well understood. We therefore assessed the association between age at menarche and the incidence of macrovascular complications, specifically CAD and MACE, among women with childhood-onset T1D. We hypothesized that both a younger and an older age at menarche are associated with a higher risk of macrovascular disease.
Materials and Methods
Study Population
The current analysis was based on female participants from the Pittsburgh Epidemiology of Diabetes Complications (EDC) prospective cohort study, a detailed description of which has been published previously.33,34 Briefly, EDC comprised individuals who were either diagnosed with childhood-onset T1D, or seen within a year of such diagnosis, at the Children’s Hospital of Pittsburgh between 1950 and 1980. A total of 658 participants (325 women) completed the EDC baseline assessment (1986–88) at a mean age of 28 years and a mean duration of diabetes of 19 years. The participants were subsequently followed with biennial surveys for 32 years and clinical examinations biennially for 10 years, and subsequently at the 18, 25, and 30-year follow-up. For participants who did not experience menarche before the baseline clinical visit (n=8), the visit following their first report of menstruation was used as their baseline. Participants who had CAD (n=4) or MACE (n=5) at their corresponding baseline or did not report age at menarche (n=1) were excluded. The final sample size included in the analysis was 324: 320 were evaluated for CAD, with 119 incident events during study follow-up, and 319 were assessed for MACE, with 100 incident events. The study was approved by the University of Pittsburgh Institutional Review Board.
Ascertainment of Exposure
Age at menarche was self-reported through survey forms using two questions: (1) “Have you started having menstrual periods?” and (2) “If yes, how old were you when your periods began?”. For 316 participants, the menarche age reported at the EDC study baseline was used. For the remaining eight participants who had not yet experienced menarche at baseline, their first reported menarche age from subsequent biennial surveys was used. Repeated assessments allowed the opportunity to cross-validate self-reported information and clarify discrepancies with the participant when possible. The mean and standard deviation (SD) of age at menarche were computed and participants were categorized into three menarche timing groups: early (≤12 years), normal (13–15 years), and delayed onset of menstruation (≥16 years). These categorizations were used given the participants’ median birth year of 1960, since earlier data indicates that women born in the 1960s in the United States typically experienced menarche at age 13 in the general population.35,36
Ascertainment of Outcome
Cardiovascular outcomes were ascertained based on both clinical examination as well as self-reported events in the medical survey forms and were further validated using medical records and/or death certificates during the 30-year follow-up. CAD was defined as the first appearance of confirmed myocardial infarction (MI, including clinical events and subclinical myocardial infarction on ECG, ie, Minnesota code 1.1 or 1.2), angiographic stenosis ≥50%, coronary revascularization, or CAD death. MACE was defined as the first appearance of CVD death, nonfatal MI (as above), or nonfatal stroke. The underlying cause of death was determined by a Mortality Classification Committee composed of at least two physician epidemiologists who reviewed death certificates, medical records, autopsy or coroner reports, and data from interviews with next-of-kin. Unlike CAD, MACE includes stroke and pertains to major adverse events caused by the disease process.37 Also, the direction and/or the strength of the associations between risk factors and the two conditions may differ.37,38 Thus, both outcomes were included in the current study.
Measurement of Covariates
Participant information regarding demographic, medical history, healthcare, lifestyle, and reproductive health were collected via self-administered survey forms. Physical activity was quantified as kilocalories expended on physical activity (ie, stairs climbed, city blocks walked, and light, moderate, and vigorous activity) per week collected through the modified Paffenbarger Physical Activity Questionnaire.39
At each clinical examination, weight (kg) and height (m) were measured and used to calculate BMI (kg/m2). Waist and hip circumference (cm) were calculated using the mean of two measurements, or the mean of three measurements if an additional measurement was performed due to a pre-specified difference (>0.5 cm) between the first two assessments. Following the Hypertension Detection and Follow-Up protocol,40 blood pressure was recorded using a random zero sphygmomanometer after a 5-minute rest to determine the presence of hypertension (ie, systolic blood pressure (SBP)/diastolic blood pressure (DBP) ≥140/90 mmHg, or the use of antihypertensive medications). During the initial 18 months of the study, stable HbA1 levels were assessed using the microcolumn cation exchange (Isolab, Akron, OH, USA). Subsequently, for the rest of the first 10-year follow-up, HbA1 was measured utilizing automated high-performance liquid chromatography (Diamat; Biorad, Hercules, CA, USA). There was strong concordance between the two assays (r = 0.95; Diamat HbA1 = - 0.18 + 1.00[Isolab HbA1]). To align the HbA1 measurements with the DCCT (Diabetes Control and Complications Trial) standard, a regression equation derived from duplicate assays was used (HbA1c = 0.14 + [0.83 × EDC HbA1]).41 Total cholesterol and triglycerides were measured enzymatically. HDL-C was measured using a modified precipitation technique according to the Lipid Research Clinics method.33,34 Three different timed urine samples (24-hour, overnight, and 4-hour clinic) were collected over a two-week period and assayed for albumin and creatinine to calculate the albumin excretion rate (AER). The median AER value from the three samples was utilized in analyses. Estimated glomerular filtration rate (eGFR) was determined using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation.42
Statistical Analysis
Descriptive analyses were performed to assess univariate differences by menarche timing group as well as by incident CAD and MACE. To assess participant characteristics related to age at menarche, a categorical variable for age at menarche was created (menarche timing groups: early: ≤12, normal: 13–15, delayed: ≥16). Multivariable Cox proportional hazards regression models with stepwise selection (significance levels for entry and stay: 0.25 and 0.15, respectively) were constructed to assess the relationship between age at menarche and each incident outcome, separately. Follow-up time was defined as the time in years from baseline to the time of incident outcome, for incident cases, or the end of follow-up for non-cases. Covariates were selected based on the results from descriptive analyses and existing knowledge from previous studies in the general population. The proportional hazards assumption was evaluated by graphical inspection. For variables that did not satisfy the proportional hazards assumption, time-dependent interaction terms were introduced to the models, alongside the fixed covariate term. The functional form of age at menarche and covariates was assessed by visual inspection of Martingale residuals. The examination revealed a U-shaped association between menarche age and MACE; thus, a quadratic term was included in the model alongside the linear form of the age at menarche. To ensure consistency in the statistical approach, a quadratic term was also tested for CAD. No significant deviations from a linear association were observed for CAD. Participants with missing covariate data (CAD: n=35, MACE: n=8) were excluded from the Cox regression analyses. Data analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC) and R version 4.1.3 (R Core Team, 2022). A two-tailed p-value of less than 0.05 was considered statistically significant.
Results
Of the 325 female participants of the EDC study, four participants had prevalent CAD and five participants had prevalent MACE at baseline (three had both conditions) and were excluded from analyses of the respective outcomes. An additional participant was excluded because of missing information on age at menarche. As a result, 320 and 319 women were included in the analysis for CAD (119 incident events, 37.2%) and MACE (100 incident events, 31.3%), respectively. Mean age was 27.8 years, mean T1D duration was 19.3 years, and the median age at menarche was 13 years. Included participants were divided into 3 menarche timing groups: early (≤12 years, n=104), normal (13–15 years, n=176) and delayed menarche (≥16 years, n=44). Most women (86.7%, 281/324) experienced menarche after the onset of T1D with only 13.3% (43/324) experiencing menarche before their diagnosis of T1D.
Baseline characteristics of women included in this analysis stratified by menarche timing are presented in Table 1. At baseline, women with delayed menarche had longer diabetes duration, higher AER, and were more likely to have hypertension, compared with the other groups. Additionally, women with normal menarche had higher eGFR compared to their counterparts. Notably, all women in the delayed menarche group were diagnosed with T1D before menarche. No other baseline characteristics were found to significantly differ across categories of age at menarche.
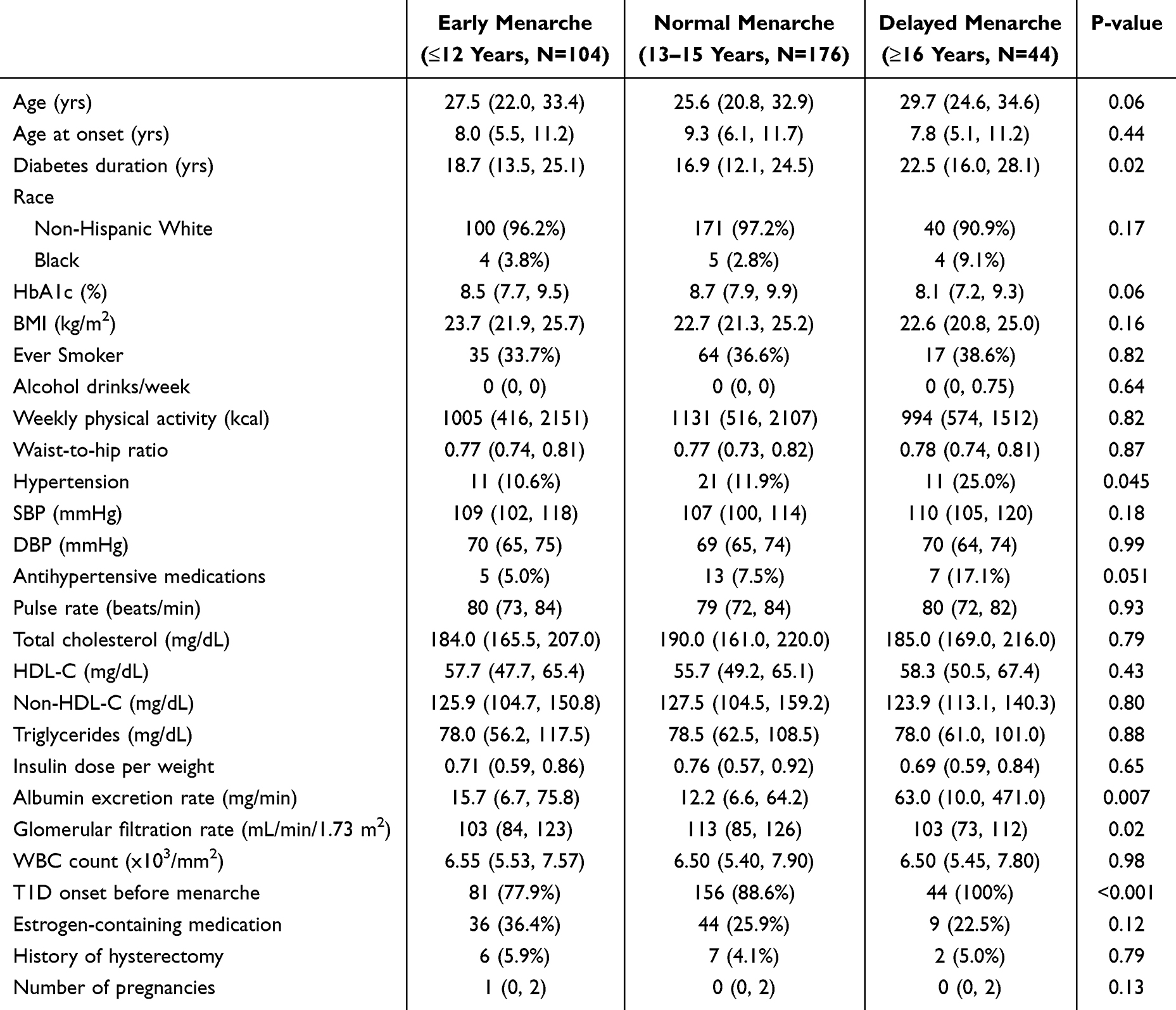 |
Table 1 Baseline Characteristics of Female EDC Participants by Menarche Timing Group (n=324) |
Table 2 describes differences in baseline characteristics of participants by CAD incidence and by MACE incidence. Women who developed CAD within the study follow-up period were older at baseline, had longer diabetes duration, larger waist-to-hip ratio, higher SBP, pulse rate and white blood cell (WBC) count, lower eGFR and higher AER, as well as a worse lipid profile (ie, higher total cholesterol, non-HDL-C, and triglycerides). Additionally, they were more likely to have a history of smoking, use estrogen-containing medications, and to have a higher number of pregnancies. The overall distribution of age at menarche (continuous variable) did not differ significantly by incident CAD status (p=0.38). Compared to incident cases, a greater proportion of women without a CAD event were in the normal menarche timing group, although this did not reach statistical significance (p=0.05). Similar patterns in baseline characteristics emerged when comparing participants by incident MACE as those observed for CAD. In addition, women who developed MACE were less physically active and more likely to have undergone hysterectomy than those who did not develop MACE.
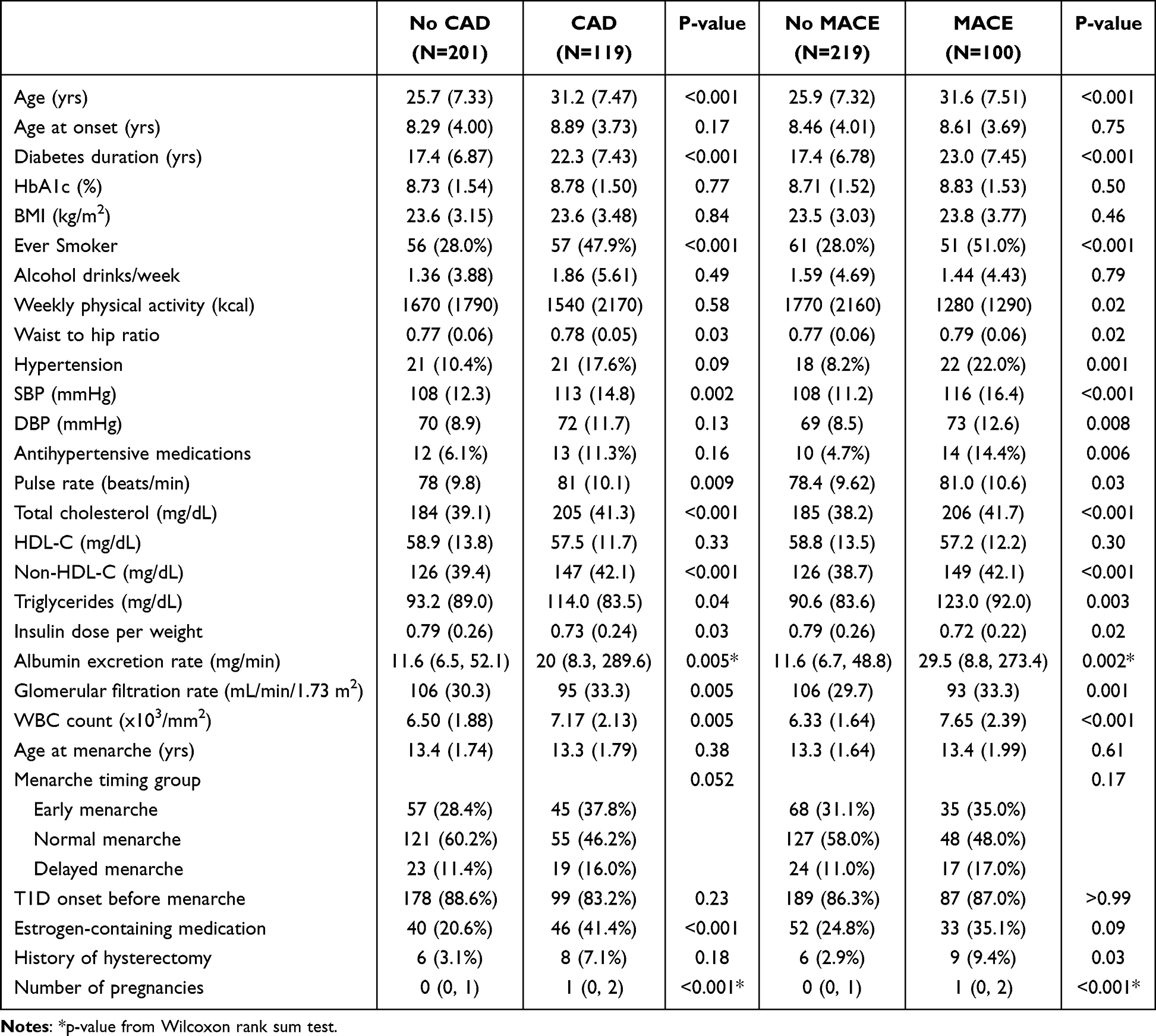 |
Table 2 Baseline Characteristics of Female EDC Participants by Cumulative Incidence of CAD and MACE |
The unadjusted hazard ratios for both CAD and MACE by age at menarche suggested a U-shaped relationship (Figures 1 and 2, respectively). The results of Cox regression analyses for CAD and MACE are shown in Table 3 (Model 1, for age at menarche as a continuous variable, also allowing for a quadratic term, and Model 2, for age at menarche as a categorical variable). In multivariable Cox models, the quadratic term for age at menarche was not selected for inclusion in the mo although age at menarche as a continuous variable was included, it was not significantly associated with risk of CAD (Model 1: HR =0.88, 95% CI: 0.78–1.00, p=0.06). When using the categorical variable, compared to menarche between 13–15 years, early menarche (≤12 years) was significantly associated with greater risk of CAD (Model 2: HR =1.71, 95% CI: 1.11–2.64, p=0.01), although the risk associated with delayed menarche was not statistically significant (HR =1.25, 95% CI: 0.66–2.36, p=0.50). Other baseline participant characteristics associated with the risk of CAD comprised T1D duration, smoking history, HbA1c, SBP, non-HDL-C, WBC count, eGFR, use of estrogen-containing medications, and pregnancy number (Model 2).
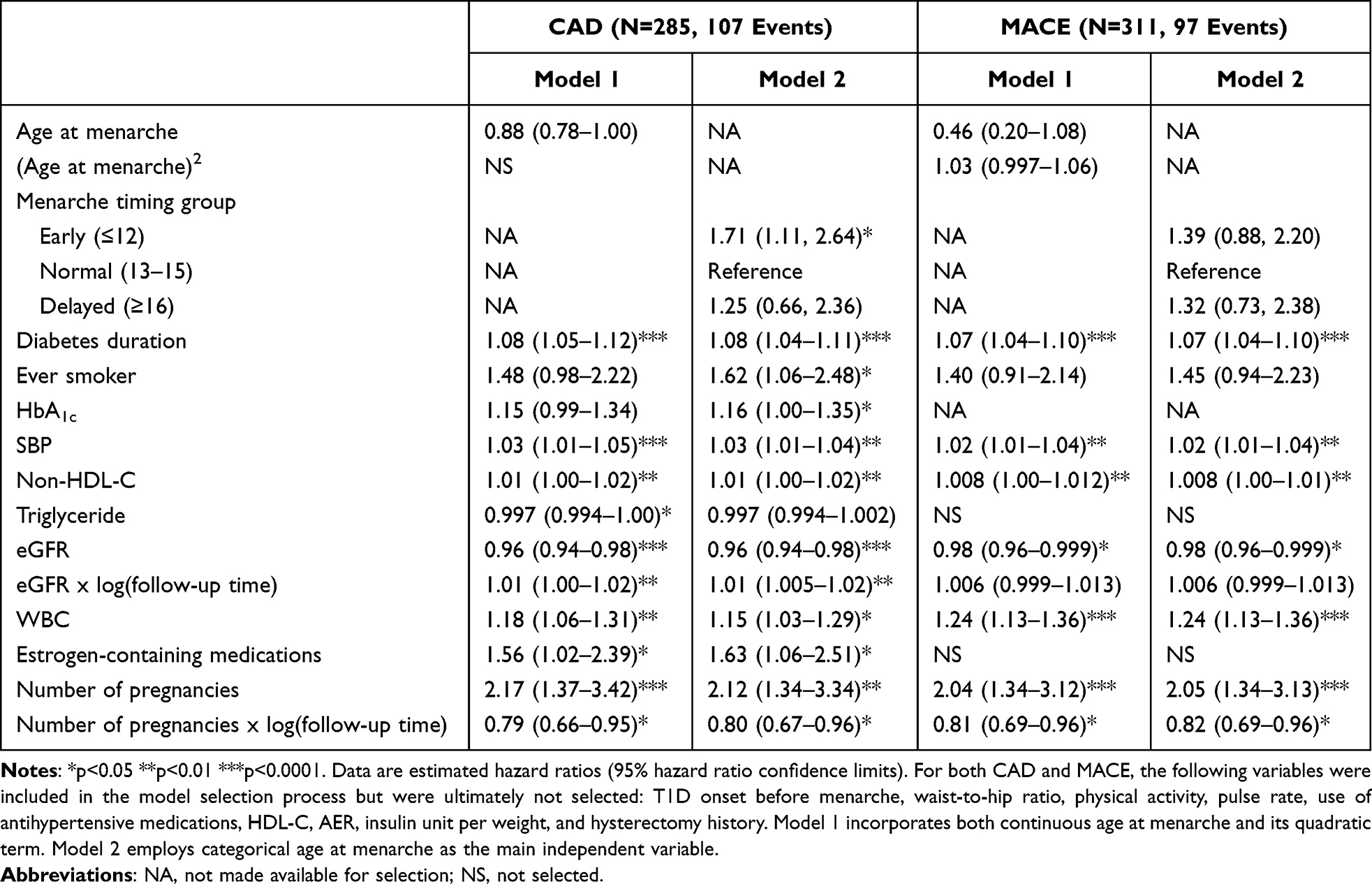 |
Table 3 Multivariable Cox Proportional Hazards Regression Results for Incident CAD and MACE Among Women with T1D in the EDC Study |
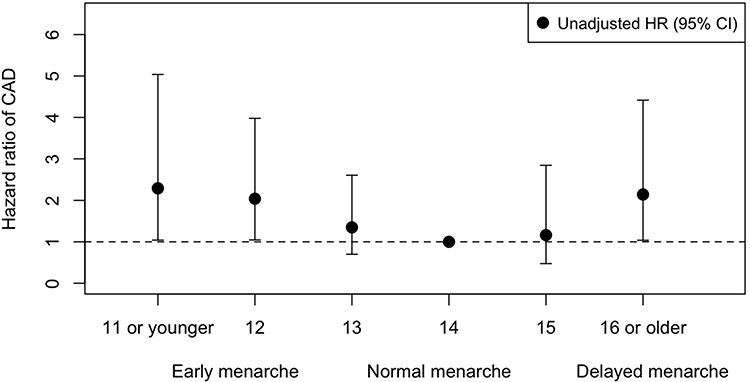 |
Figure 1 Unadjusted HR (95% CI) for CAD by age at menarche. |
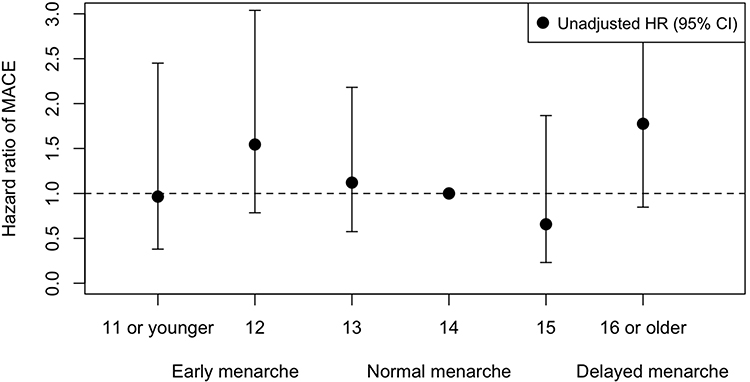 |
Figure 2 Unadjusted HR (95% CI) for MACE by age at menarche. |
In multivariable Cox models for MACE although the quadratic term for age at menarche (along with the linear form) was selected for inclusion into the model, neither term reached statistical significance (Model 1: linear term p=0.075, quadratic term p=0.08). Using the categorical variable for age at menarche, neither early nor late menarche was significantly associated with CAD risk compared to normal menarche timing. The covarying factors associated with MACE were similar to those identified for CAD. Importantly, no significant interactions were detected between age at menarche and other covariates for either outcome. Moreover, replacing T1D duration with age yielded similar results.
Discussion
In the current study, we assessed the longitudinal relationship of age at menarche with incident CAD and MACE in women with childhood-onset type 1 diabetes. Our analysis revealed a weak U-shaped relationship between age at menarche and the risk of both CAD and MACE; however, the quadratic terms did not attain statistical significance in the multivariable Cox regression models. Rather, our results indicated that only early menarche was linked to an elevated risk of developing CAD. Specifically, experiencing menarche by the age of 13 years was associated with a 1.7 times higher risk of CAD compared to reaching menarche between 13–15 years of age.
The relationship between menarche age and CAD has been examined in several large population-based cohorts within the general population,2,14–16 suggesting both early and delayed menarche were associated with a higher risk of incident CAD. However, findings from the China Kadoorie Biobank study6 showed no significant association between menarche timing and CAD risk. Evidence regarding age at menarche and incident MACE is scarce. The Women’s Ischemia Syndrome Evaluation (WISE) study group5 revealed a J-shaped relationship among middle-aged women. Compared to those who began menstruating at age 12, both early menarche (≤10 years) and late menarche (≥15 years) were found to be associated with increased risk of MACE.5 Comparable evidence is very limited in the T1D population. However, similar with existing data in the general population, our findings indicate possible weak, U-shaped relationships between menarche age and both CAD and MACE, particularly reinforcing the association between early menarche and increased CAD risk, providing insights within the T1D population for the first time.
In light of these findings regarding the association between menarche timing and CVD risk, researchers have attempted to elucidate the mechanisms underlying these observations. Based on results from Mendelian randomization studies11,12 and a mediation analysis,13 the observed relationship between early menarche and elevated CAD risk appears to be partially explained by excessive adiposity persisting from childhood into adulthood. Specifically, it was found that early menarche is causally related with increased adult BMI11 but does not independently influence the risk of cardiometabolic diseases.12 Studies conducted in the T1D population suggest that a greater BMI z-score or BMI standard deviation score is associated with younger age at menarche.24–27 Although no significant correlation between BMI and menarche age was observed in the current study, the absence of information on BMI around the onset of menstruation for most participants precludes any conclusions regarding the role of childhood obesity in those with early menarche. Future studies should investigate whether the association between early menarche (linked to adiposity) and increased CAD risk, as observed in the general population, is also present in women with T1D.
The reasons behind the association between late menarche and an increased risk of CAD are not yet well understood. Some researchers have introduced the notion that the link between delayed menarche and increased CAD risk might be related to a shorter duration of exposure to the cardioprotective effects of estrogen,2,17 as late menarche has been linked to early natural menopause.15 However, the WISE study group reported that the association between menarche age and MACE was not attenuated by adjustment for the duration of exposure to estrogen.5 We have previously shown that women with T1D are more likely to experience delayed menarche compared with non-diabetic women.43 It is therefore possible that certain conditions, such as childhood-onset T1D, cause both delayed menarche and cardiovascular outcomes. Indeed, previous research has linked late menarche with impaired vascular endothelium and vascular function in adulthood.17 Moreover, there is evidence suggesting that delayed menarche is associated with an increased risk of nephropathy in T1D,20,21 which has been shown to substantially increase CVD risk.22
It is important to mention that how menarche age was categorized by researchers could have affected its association with studied outcomes. Assuming an adequate sample size, utilizing finer-grained categories, particularly at the extremes, could pronounce the increased risk associated with both early and late menarche. Additionally, the time period studies were conducted could have also influenced the categorization of age at menarche, since age at menarche has declined over the years.27,44 Future studies should focus on the origins of late menarche, including conditions such as polycystic ovarian syndrome, excessive exercise, and childhood undernutrition, in order to provide further insights into the mechanisms behind the association between late menarche and the risk of CVD.
It is known that T1D affects the reproductive health of female patients, leading to delayed puberty and menarche due to the effects of insulin deficiency and hyperglycemia on the HPG axis.19 Similar to the general population, girls with T1D have shown a trend toward earlier menarche.44,45 In the present analysis, the median birth year of female study participants was 1960 and the median age at menarche was 13 years, similar to the previously estimated age at menarche (~12.8 years) for US women born in the 1960s in the general population.35,36 In individuals with T1D, later menarche has been linked to earlier diabetes onset,20,43,44 worse glycemic control,24,46 and lower BMI.25,26,45 Consequently, girls who develop T1D before experiencing menarche, especially at a younger age and with less well-controlled blood glucose levels, may be more prone to experiencing delayed menarche. In our cohort, 13.6% experienced menarche at the age of 16 years or later. On the other hand, early menarche was also common in our cohort of T1D (32.1%), especially among those who experienced menarche before T1D onset. In the general population, early menarche is thought to contribute to an elevated CVD risk through its impact on adulthood obesity.11–13 Whether this also applies to the T1D population remains to be investigated. Other factors associated with an increased risk of CAD and MACE, generally included diabetes duration, smoking status, HbA1c, SBP, lipid profiles, WBC count, renal function, use of estrogen-containing medications, and the number of pregnancies. The increased risk of CVD associated with an increasing number of pregnancies in this population may relate to adverse pregnancy outcomes accompanied by a rise in pregnancy attempts, which has been related to underlying health issues and complications in T1D.47
Our study is the first study to evaluate the relationship of menarche timing with CAD and MACE in women with childhood-onset type 1 diabetes. The distinct associations noted for CAD and MACE may be explained by the incorporation of stroke and the exclusion of coronary revascularization within the MACE outcome. Notably, unlike CAD, where revascularization can be influenced by various objective and subjective factors, MACE refers to adverse events caused by the disease process and are often referred to as “hard” events.
Limitations of the current study deserving to be mentioned include the relatively small sample of 324 women with T1D, as compared with the large population-based cohorts in the general population discussed above.2,6,14–16 Moreover, as only a small proportion (13%) of women in this analysis developed T1D after menarche, we were unable to examine how timing of menarche in relation to the onset of T1D affected outcomes. Another limitation arises from the absence of racial diversity; as 96% of participants were non-Hispanic whites, our findings cannot be generalized to broader racial and ethnic groups. Additionally, as the majority of female participants in the EDC study had already experienced menarche prior to study entry, information on covariates at the time of menarche was not available. Therefore, the question of whether these associations are independent of other factors, particularly BMI, that impact menarche timing remains unanswered. Although menarche is a memorable event in a woman’s life, the possibility of recall bias cannot be excluded. However, it is unlikely that errors in recalling age at menarche would be differential by subsequent outcome status. Future studies should address the limitations mentioned above to help further our understanding of the role of age at menarche in women with T1D. While menarche age is a possible surrogate of nutritional status, physical activity, and childhood obesity, its routine collection as part of gynecologic history in everyday clinical practice suggests its potential value in predicting women’s cardiovascular risk during later life, both in the T1D population and the general population.
In conclusion, our results suggest that among women with childhood-onset T1D, early menarche is associated with a higher risk of CAD. Delayed menarche was not significantly associated with either CAD or MACE. Given the adverse impact of CAD, should future studies confirm the general population findings on the role of early menarche on the development of CAD also in T1D, early menarche could be considered as a clinical marker for CAD risk prediction. Taking advantage of the widespread availability of electronic health records in the era of medical data digitalization, early identification of individuals at elevated cardiovascular risk could facilitate more proactive monitoring and targeted interventions in the T1D population, ultimately improving both longevity and quality of life.
Declaration of Generative AI in Scientific Writing
During the preparation of this work J. J. used ChatGPT in order to improve language. After using this tool, all authors reviewed and edited the content as needed, and take full responsibility for the content of the publication.
Data Sharing Statement
The original data for this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principles of the Declaration of Helsinki as revised in 2008. All procedures performed in studies involving human participants were in accordance with the ethical standards of the responsible institutional and national research committee on human experimentation and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The study was approved by the University of Pittsburgh Institutional Review Board (IRB980707).
Acknowledgments
We are indebted to study participants and staff for their invaluable contributions to the EDC study. Funding sources: this research was supported by the National Institutes of Health Grant DK34818 and by the Rossi Memorial Fund.
Author Contributions
Jinghui Ju: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft, Writing – review & editing, Visualization. Samar R. El Khoudary: Methodology, Writing – review & editing. Jeanine M. Buchanich: Methodology, Writing – review & editing. Trevor J. Orchard: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. Tina Costacou: Conceptualization, Funding acquisition, Methodology, Writing – review & editing, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or relationships that could be perceived as conflict of interest.
References
1. Prentice P, Viner RM. Pubertal timing and adult obesity and cardiometabolic risk in women and men: a systematic review and meta-analysis. Int J Obes Lond. 2013;37(8):1036–11. doi:10.1038/ijo.2012.177
2. Lakshman R, Forouhi NG, Sharp SJ, et al. Early age at menarche associated with cardiovascular disease and mortality. J Clin Endocrinol Metab. 2009;94(12):4953–4960. doi:10.1210/jc.2009-1789
3. Okoth K, Chandan JS, Marshall T, et al. Association between the reproductive health of young women and cardiovascular disease in later life: umbrella review. BMJ. 2020;371:m3502.
4. Chen L, Hu Z, Wang X, et al. Age at menarche and menopause, reproductive lifespan, and risk of cardiovascular events among chinese postmenopausal women: results from a large national representative cohort study. Front Cardiovasc Med. 2022;9:870360. doi:10.3389/fcvm.2022.870360
5. Lee JJ, Cook-Wiens G, Johnson BD, et al. Age at menarche and risk of cardiovascular disease outcomes: findings from the national heart lung and blood institute-sponsored women’s ischemia syndrome evaluation. J Am Heart Assoc. 2019;8(12):e012406. doi:10.1161/JAHA.119.012406
6. Yang L, Li L, Millwood IY, et al. Age at menarche and risk of major cardiovascular diseases: evidence of birth cohort effects from a prospective study of 300,000 Chinese women. Int J Cardiol. 2017;227:497–502. doi:10.1016/j.ijcard.2016.10.115
7. Janghorbani M, Mansourian M, Hosseini E. Systematic review and meta-analysis of age at menarche and risk of type 2 diabetes. Acta Diabetol. 2014;51(4):519–528. doi:10.1007/s00592-014-0579-x
8. Zheng Y, Wen TS, Shen Y, Hu H. Age at menarche and cardiovascular health: results from the NHANES 1999-2016. Menopause. 2020;28(1):18–24. doi:10.1097/GME.0000000000001653
9. Hu C, Zhang Y, Zhang J, et al. Age at menarche, ideal cardiovascular health metrics, and risk of diabetes in adulthood: findings from the REACTION study. J Diabetes. 2021;13(6):458–468. doi:10.1111/1753-0407.13128
10. Asrullah M, L’Hoir M, Feskens EJM, Melse-Boonstra A. Trend in age at menarche and its association with body weight, body mass index and non-communicable disease prevalence in Indonesia: evidence from the Indonesian Family Life Survey (IFLS). BMC Public Health. 2022;22(1):628. doi:10.1186/s12889-022-12995-3
11. Gill D, Brewer CF, Del Greco MF, et al. Age at menarche and adult body mass index: a Mendelian randomization study. Int J Obes Lond. 2018;42(9):1574–1581. doi:10.1038/s41366-018-0048-7
12. Cao M, Cui B. Negative effects of age at menarche on risk of cardiometabolic diseases in adulthood: a mendelian randomization study. J Clin Endocrinol Metab. 2020;105(2):515–522. doi:10.1210/clinem/dgz071
13. Bubach S, Horta BL, Goncalves H, Assuncao MCF. Early age at menarche and metabolic cardiovascular risk factors: mediation by body composition in adulthood. Sci Rep. 2021;11(1):148. doi:10.1038/s41598-020-80496-7
14. Canoy D, Beral V, Balkwill A, et al. Age at menarche and risks of coronary heart and other vascular diseases in a large UK cohort. Circulation. 2015;131(3):237–244. doi:10.1161/CIRCULATIONAHA.114.010070
15. Day FR, Elks CE, Murray A, Ong KK, Perry JR. Puberty timing associated with diabetes, cardiovascular disease and also diverse health outcomes in men and women: the UK Biobank study. Sci Rep. 2015;5:11208. doi:10.1038/srep11208
16. Peters SA, Woodward M. Women’s reproductive factors and incident cardiovascular disease in the UK Biobank. Heart. 2018;104(13):1069–1075. doi:10.1136/heartjnl-2017-312289
17. Schnabel RB, Biener MP, Wilde S, et al. Sex differences in noninvasive vascular function in the community. J Hypertens. 2013;31(7):1437–1446. doi:10.1097/HJH.0b013e328360f755
18. Codner E, Merino PM, Tena-Sempere M. Female reproduction and type 1 diabetes: from mechanisms to clinical findings. Hum Reprod Update. 2012;18(5):568–585. doi:10.1093/humupd/dms024
19. Thong EP, Codner E, Laven JSE, Teede H. Diabetes: a metabolic and reproductive disorder in women. Lancet Diabetes Endocrinol. 2020;8(2):134–149. doi:10.1016/S2213-8587(19)30345-6
20. Harjutsalo V, Maric-Bilkan C, Forsblom C, Groop PH, FinnDiane Study G. Age at menarche and the risk of diabetic microvascular complications in patients with type 1 diabetes. Diabetologia. 2016;59(3):472–480. doi:10.1007/s00125-015-3816-0
21. Yi Y, Denic-Roberts H, Rubinstein D, Orchard TJ, Costacou T. Effect of age at menarche on microvascular complications among women with type 1 diabetes. Diabet Med. 2019;36(10):1287–1293. doi:10.1111/dme.13936
22. Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37(10):2864–2883. doi:10.2337/dc14-1296
23. Thomas MC, Zoungas S, Hanssen NMJ, McAuley SA, Cooper ME. Kidney disease: the forgotten legacy of type 1 diabetes. Diabetes Care. 2025;48(8):1299–1308. doi:10.2337/dci25-0028
24. Danielson KK, Palta M, Allen C, D’Alessio DJ. The association of increased total glycosylated hemoglobin levels with delayed age at menarche in young women with type 1 diabetes. J Clin Endocrinol Metab. 2005;90(12):6466–6471. doi:10.1210/jc.2005-0349
25. Rohrer T, Stierkorb E, Grabert M, et al. Delayed menarche in young German women with type 1 diabetes mellitus: recent results from the DPV diabetes documentation and quality management system. Eur J Pediatr. 2008;167(7):793–799. doi:10.1007/s00431-007-0590-0
26. Pereira KC, Pugliese BS, Guimaraes MM, Gama MP. Pubertal development in children diagnosed with diabetes mellitus type 1 before puberty. J Pediatr Adolesc Gynecol. 2015;28(1):66–71. doi:10.1016/j.jpag.2014.08.009
27. Gohlke B, Reschke F, Lanzinger S, et al. Time trends towards earlier puberty in boys and girls with type 1 diabetes: insights from the German Diabetes Prospective Follow-up (DPV) registry, 2000 to 2021. Diabetes Obes Metab. 2024;26(1):293–300. doi:10.1111/dom.15315
28. Miller RG, Mahajan HD, Costacou T, Sekikawa A, Anderson SJ, Orchard TJ. A contemporary estimate of total mortality and cardiovascular disease risk in young adults with type 1 diabetes: the pittsburgh epidemiology of diabetes complications study. Diabetes Care. 2016;39(12):2296–2303. doi:10.2337/dc16-1162
29. Livingstone SJ, Looker HC, Hothersall EJ, et al. Risk of cardiovascular disease and total mortality in adults with type 1 diabetes: scottish registry linkage study. PLoS Med. 2012;9(10):e1001321. doi:10.1371/journal.pmed.1001321
30. Soedamah-Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, Colhoun HM. High risk of cardiovascular disease in patients with type 1 diabetes in the U.K.: a cohort study using the general practice research database. Diabetes Care. 2006;29(4):798–804. doi:10.2337/diacare.29.04.06.dc05-1433
31. Kalyani RR, Lazo M, Ouyang P, et al. Sex differences in diabetes and risk of incident coronary artery disease in healthy young and middle-aged adults. Diabetes Care. 2014;37(3):830–838. doi:10.2337/dc13-1755
32. Harjutsalo V, Thomas MC, Forsblom C, Groop PH, FinnDiane Study G. Risk of coronary artery disease and stroke according to sex and presence of diabetic nephropathy in type 1 diabetes. Diabetes Obes Metab. 2018;20(12):2759–2767. doi:10.1111/dom.13456
33. Orchard TJ, Dorman JS, Maser RE, et al. Factors associated with avoidance of severe complications after 25 yr of IDDM. Pittsburgh epidemiology of diabetes complications study I. Diabetes Care. 1990;13(7):741–747. doi:10.2337/diacare.13.7.741
34. Orchard TJ, Dorman JS, Maser RE, et al. Prevalence of complications in IDDM by sex and duration. Pittsburgh epidemiology of diabetes complications study II. Diabetes. 1990;39(9):1116–1124. doi:10.2337/diab.39.9.1116
35. McDowell MA, Brody DJ, Hughes JP. Has age at menarche changed? Results from the National Health and Nutrition Examination Survey (NHANES) 1999-2004. J Adolesc Health. 2007;40(3):227–231. doi:10.1016/j.jadohealth.2006.10.002
36. Nichols HB, Trentham-Dietz A, Hampton JM, et al. From menarche to menopause: trends among US Women born from 1912 to 1969. Am J Epidemiol. 2006;164(10):1003–1011. doi:10.1093/aje/kwj282
37. Matsunaga M, Yatsuya H, Iso H, et al. Similarities and differences between coronary heart disease and stroke in the associations with cardiovascular risk factors: the Japan Collaborative Cohort Study. Atherosclerosis. 2017;261:124–130. doi:10.1016/j.atherosclerosis.2017.03.003
38. Muhammad IF, Borne Y, Zaigham S, et al. Comparison of risk factors for ischemic stroke and coronary events in a population-based cohort. BMC Cardiovasc Disord. 2021;21(1):536. doi:10.1186/s12872-021-02344-4
39. Kriska AM, LaPorte RE, Patrick SL, Kuller LH, Orchard TJ. The association of physical activity and diabetic complications in individuals with insulin-dependent diabetes mellitus: the Epidemiology of Diabetes Complications Study--VII. J Clin Epidemiol. 1991;44(11):1207–1214. doi:10.1016/0895-4356(91)90153-Z
40. Detection H. The hypertension detection and follow-up program: hypertension detection and follow-up program cooperative group. Prev Med. 1976;5(2):207–215. doi:10.1016/0091-7435(76)90039-6
41. Prince CT, Becker DJ, Costacou T, Miller RG, Orchard TJ. Changes in glycaemic control and risk of coronary artery disease in type 1 diabetes mellitus: findings from the Pittsburgh Epidemiology of Diabetes Complications Study (EDC). Diabetologia. 2007;50(11):2280–2288. doi:10.1007/s00125-007-0797-7
42. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
43. Yi Y, El Khoudary SR, Buchanich JM, et al. Women with Type 1 diabetes (T1D) experience a shorter reproductive period compared with nondiabetic women: the Pittsburgh Epidemiology of Diabetes Complications (EDC) study and the Study of Women’s Health Across the Nation (SWAN). Menopause. 2021;28(6):634–641.
44. Schweiger B, Klingensmith GJ, Snell-Bergeon JK. Menarchal timing in type 1 diabetes through the last 4 decades. Diabetes Care. 2010;33(12):2521–2523. doi:10.2337/dc10-0872
45. Codner E, Barrera A, Mook-Kanamori D, et al. Ponderal gain, waist-to-hip ratio, and pubertal development in girls with type-1 diabetes mellitus. Pediatr Diabetes. 2004;5(4):182–189. doi:10.1111/j.1399-543X.2004.00059.x
46. Rohrer T, Stierkorb E, Heger S, et al. Delayed pubertal onset and development in German children and adolescents with type 1 diabetes: cross-sectional analysis of recent data from the DPV diabetes documentation and quality management system. Eur J Endocrinol. 2007;157(5):647–653. doi:10.1530/EJE-07-0150
47. Costacou T, Rubinstein D, Orchard TJ. Prediction of adverse pregnancy outcomes among women with type 1 diabetes. Diabetes. 2018;67(1):1630–P.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibrinogen is Associated with Clinical Adverse Events in Patients with Psoriasis and Coronary Artery Disease
Zhao L, Zeng Y, Sun L, Zhang Z, Yang K, Li Z, Wang M, Zhou X, Yang W
Journal of Inflammation Research 2023, 16:4019-4030
Published Date: 12 September 2023
The Clinical Significance and Prognostic Value of Inflammatory Hematological Indices in Young Patients with Coronary Artery Disease
Sun J, Qi S, Yu M, Lei S, Han W, Wu S, Zhou Y, Shi D
Journal of Inflammation Research 2026, 19:582913
Published Date: 13 June 2026