Back to Journals » Advances in Medical Education and Practice » Volume 13
African Medical Educators and Anatomy Teachers’ Perceptions and Acceptance of the Anatomage Table as an EdTech and Innovation: A Qualitative Study
Authors Owolabi J ![]() , Ojiambo R, Seifu D, Nishimwe A
, Ojiambo R, Seifu D, Nishimwe A ![]() , Masimbi O, Okorie CE
, Masimbi O, Okorie CE ![]() , Ineza D, Bekele A
, Ineza D, Bekele A
Received 16 January 2022
Accepted for publication 27 May 2022
Published 6 June 2022 Volume 2022:13 Pages 595—607
DOI https://doi.org/10.2147/AMEP.S358702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Joshua Owolabi,1 Robert Ojiambo,2 Daniel Seifu,3 Arlene Nishimwe,4 Ornella Masimbi,5 Chinonso Emmanuel Okorie,6 Darlene Ineza,4 Abebe Bekele7
1Department of Anatomy, Division of Basic Medical Science, University of Global Health Equity, Butaro, Rwanda; 2Department of Physiology, Division of Basic Medical Science, University of Global Health Equity, Butaro, Rwanda; 3Department of Biochemistry, Division of Basic Medical Science, University of Global Health Equity, Butaro, Rwanda; 4Division of Basic Medical Science, University of Global Health Equity, Butaro, Rwanda; 5The UGHE Simulation Centre, University of Global Health Equity, Butaro, Rwanda; 6Doctors without Borders, Brussels, Belgium; 7School of Medicine, University of Global Health Equity, Butaro, Rwanda
Correspondence: Joshua Owolabi, Department of Anatomy, Division of Basic Medical Science, University of Global Health Equity, Butaro, Rwanda, Tel +250 781164365, Email [email protected]
Background: This article presents a qualitative study of African anatomists and anatomy teachers on the Anatomage Table–a modern medical education technology and innovation, as an indicator of African anatomy medical and anatomy educators’ acceptance of EdTech. The Anatomage Table is used for digital dissection, prosection, functional anatomy demonstration, virtual simulation of certain functions, and interactive digital teaching aid.
Materials and Methods: Anatomy teachers [n=79] from 11 representative African countries, Ghana, Nigeria [West Africa], Ethiopia, Kenya, Rwanda [East Africa], Namibia [South Africa], Zambia [Southern Africa], Egypt [North Africa], and Sudan [Central Africa], participated in this study. Focus group discussions [FGDs] were set up to obtain qualitative information from stakeholders from representative institutions. In addition, based on the set criteria, selected education leaders and stakeholders in representative institutions participated in In-depth Interviews [IDIs]. The interview explored critical issues concerning their perceptions about the acceptance, adoption, and integration of educational technology, specifically, the Anatomage Table into the teaching of Anatomy and related medical sciences in the African continent. Recorded interviews were transcribed and analyzed using the Dedoose software.
Results: African anatomists are generally technology inclined and in favor of EdTech. The most recurring opinion was that the Anatomage Table could only be a “complementary teaching tool to cadavers” and that it “can’t replace the real-life experience of cadavers.” Particularly, respondents from user institutions opined that it “complements the traditional cadaver-based approaches” to anatomy learning and inquiry, including being a good “complement for cadaveric skill lab” sessions. Compared with the traditional cadaveric dissections a majority also considered it less problematic regarding cultural acceptability and health and safety-related concerns. The lifelikeness of the 3D representation is a major factor that drives acceptability.
Keywords: anatomy, Anatomage, educational technology, medical education, innovations, Africa
Background
Educational technology and innovations, abbreviated as EdTech, are becoming increasingly integral to the delivery of medical education globally. With technological and educational advancements, there have been significant shifts in the work culture and how much technology is being used to support work, including medical services. EdTech offers certain clear benefits and values to medical education, and evidence supports that it currently helps deliver very effective medical education. Further, medical care and services are benefiting from medical technology and innovations. Consequently, it is significant to integrate EdTech into medical education.
This study considered the perceptions of African anatomists and medical educators regarding their Anatomage Table use as educational technology, EdTech, in the teaching and education of medical and allied health students using qualitative research methods. This effort complements our previous efforts in considering the same population, obtaining quantitative data, and analyzing it. It is clear that the qualitative data and information obtained from the current study significantly and substantially add value to the existing data about African anatomists’ perceptions, opinions, and acceptance of educational technology in general. The study also considered factors that might favor or oppose the integration of the Anatomage Table as an EdTech into medical education on the continent. Representatives in African institutions, based on clearly defined inclusion and exclusion criteria, participated in this study. To the best of our knowledge, this would serve as one of the most extensive educational technology studies on the African continent in recent times. The primary aim of this study was to study African medical educators and anatomy teachers’ perception and acceptance of the Anatomage Table as a modern EdTech and innovation using a qualitative study approach. The qualitative study methods purposefully used provided quality insights into the subject of interest that is otherwise typically only explored by pure quantitative methods.
Review of Literatures
The Anatomage Table as an EdTech with Reported Educational Values and Benefits
Anatomy remains a fundamental basic medical science and an indispensable subject in the context of medical education.1 The Anatomage Table is an EdTech with reported educational values and benefits for teaching anatomical sciences and related basic medical sciences.2–5 The Anatomage Table has been used in different contexts and ways to deliver medical education or Anatomy teaching to medical, anatomical, and allied health students. Some specific ways in which this technology has been used include teaching aids to illustrate and present highly accurate human and other animals’ anatomy to trainees and students. It is also useful as an assessment tool as well as an EdTech that can deliver edutainment.6 The latter instance includes situations whereby students play games that test their knowledge and understanding of the body anatomy and functions, thus, enhancing their interest, learning, and critical reasoning. In certain other instances involving efforts to model the traditional anatomical dissections, the Anatomage Table has been used as a digital or virtual dissection facility. EdTech, especially its more advanced versions, can also be used to simulate specific body functions such as heartbeat, movement of the heart valves, blood flow, and the accompanying physiological attributes such as the EEG, all within the cardiovascular system. It is also possible to visualize the transport paths of food and air through the digestive and respiratory systems, respectively. A significant advantage of such a virtual or digital body over the traditional cadaveric observation and dissection is, therefore, the ability to simulate the physiological attributes associated with specific structures using the digital cadaver on the Anatomage Table. When it comes to EdTech and innovations that are currently significantly influencing anatomical sciences and education, the Anatomage Table stands out because it provides insight into how much benefit EdTech offers to the delivery of anatomy education to students and trainees. Continuous research efforts on EdTech, specifically Anatomage, are ongoing, and these efforts significantly add value and contribute to knowledge in this regard.
EdTech is Increasingly Adding Value to the Quality of Medical Education Delivery
According to Guze,7 EdTech currently helps meet certain critical challenges that medical education faces because of the rapid evolution of medical education training and delivery of care. The report identified specific contributions of EdTech through modeled practices, which include facilitating students’ acquisition of basic knowledge, helping with training on improving decision-making skills, helping to appreciate perceptual variation, contributing to improving the areas of skill coordination, helping with practicing for rare or critical events, training to enhance team learning, and improving psychomotor skills. Several medical educators and authors have also reported the importance and contributions of EdTech to the evolving landscape of medical education. It is clear that EdTech varies widely, and so is its application extensively, with various EdTech types having the potential to add value to medical education and training in different contexts. EdTech can significantly contribute to advancing medical education, improving care delivery, and training medical and allied health professionals.8–12
Qualitative study approaches in medical education are increasingly becoming popular and significant.13,14 The current study was purposefully designed to use a qualitative approach to explore the subject of interest, particularly because of the anticipated enriched perspective. It means the approach could be provided to other ongoing and previous efforts on the same subject area. Several authors have advocated for the escalating need to use qualitative study methods in medical education. It is also becoming increasingly clear that every important data and quality information might not be available in quantitative and quantified forms. For example, Chapman et al15 provided guidelines about the grounded theory use that involves the use of thematic analysis. The current study, consistent with these informed positions, adopted thematic analysis in analyzing the qualitative information obtained from the target population.13–16
Materials and Methods
Focus Group Discussion and in-Depth Interviews
The principles that guide the use of focus group discussions as a research method were followed as described by Dilshad and Latif.17 A set of 10 guide questions were used. In addition, at least 5 participants participated in a focus group discussion session. In each region or country, two focus groups were considered: One in a school that uses Anatomage and another in a school that was not using the Anatomage Table technology. A total population approach was used where all institutions that used the Anatomage Table in Africa were identified and approached through their leaders or contact persons. In each case of an institution that used the Anatomage Table, another institution in the same country or region with a similar attribute was identified as a match. The consenting institutions also had all anatomists and medical educators as participants after satisfying the inclusion criteria. IDIs were subsequently conducted with the head of the department, school management team, or Anatomage unit heads. Zoom meetings were scheduled on agreed dates for our overview meeting with the engaged team. The language of communication with the participants in all selected countries was English. The focus group interview and in-depth qualitative interview sessions were facilitated by the research assistant for the project (male) in partnership with a female member of the research team, while the principal investigator joined in as an observer. The participating interviewees were Anatomy teachers in the selected institutions who gave their informed consent to the Google survey form to participate in the qualitative study after completing the quantitative study questionnaire. All basic steps, principles, and standards or best practices were carefully observed with adequate reference to guides and previous works.18–23
Study Materials and Tools
The study tools we used in our quest to sufficiently answer the research objectives included:
- A set of pre-tested and validated Focused Group Discussion guide questions.
- A set of validated In-depth Interview guide questions.
Sample Size Determination
By design, each Anatomage-user institution was matched with another non-user in the same region; by implication, approximately half of the participants were users, and the other half were non-users. Only the consenting individuals in the target institutions participated in the research. Following their informed consent through an electronic Google form, a consenting population of all the participants in each surveyed institutional team participated in the focused group discussions. The sample size was set to at least 5 participants and a maximum of 12. The typical size of a focus group discussion is 6 to 12 participants; however, smaller groups were also allowed when the situation warranted. The same duration allowed for the FGD discussions was very informative, giving all participants of every group size enough time and opportunity to participate. A group of 3 to 4 participants was called a “mini-group.” A general rule of thumb is that the more experience and knowledge the participants have on the given subject, the smaller the group size. Figure 1 shows the map of Africa with the proportional distribution of respondents in African countries.
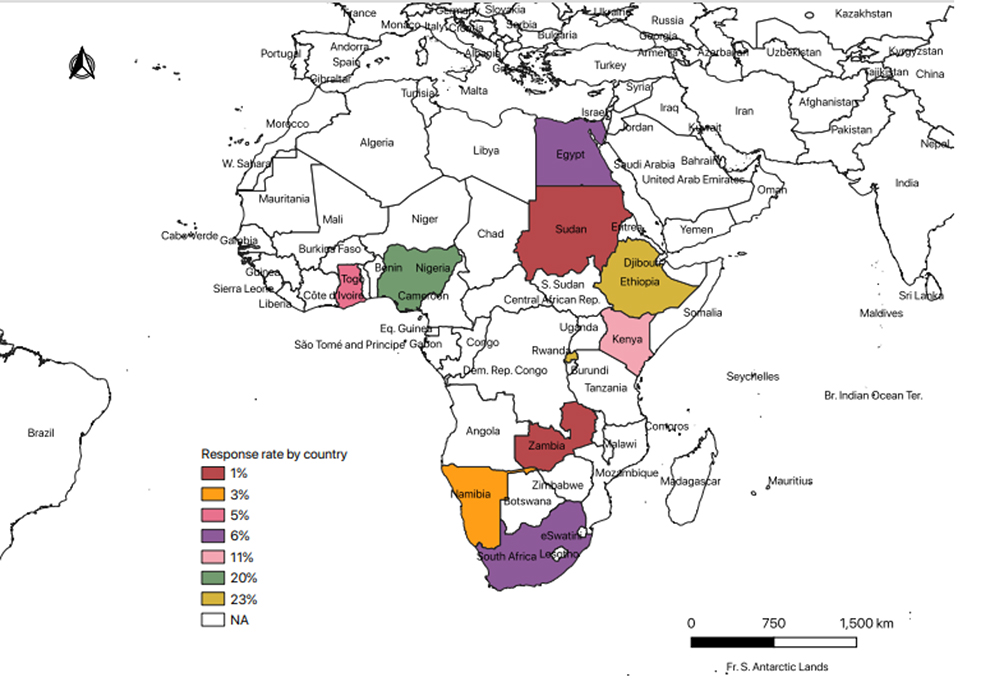 |
Figure 1 The map of Africa showing the proportional distribution of respondents in countries (only countries coloured participated). |
Inclusion and Exclusion Criteria
The general criteria for the selection of participants for this study were:
- Participants teach Anatomy or Anatomical science [whole or parts] to medical or allied health students in universities or allied health institutions.
- The institution where the participant teaches is accredited by the Government regulating agency on medical education or professional accreditors.
- Participant gives a documented informed consent.
Data Collection, Management, and Analysis
Qualitative data was collected via zoom meeting in the video and audio recorded formats and subsequently transcribed by the research assistant and other research team members into English, ensuring coded anonymity in the storage and handling of the files in compliance with privacy and confidentiality ethical codes. The text transcripts of the focused group discussion and in-depth interview recordings were coded, anonymized, and uploaded to Dedoose software version 8.3.47b for onward analysis. It uses the prepared code structure based on the research guide questions, study objectives, and recurrent cum dissenting themes observed from an interactive reading of the transcripts. A rigorous iterative process was used to summarize the emerging themes using a taxonomic presentation format.
Ethics, Informed Consent, and Confidentiality Statement
Participants indicated informed consent through an electronic form, which allowed them to register their informed consent and be contacted by the research team for the subsequent qualitative sessions(s). The communications and recruitment of participants were done with due recourse to ethical codes of respect for the dignity of participants, privacy and independence in voluntary choice, and sufficiently eliminating any form of power dynamics by authorities to influence subordinates. The Institutional Review Board of the University of Global Health Equity, where the research team resides, reviewed and approved the ethics of this research process [UGHE IRB #0085].
Results
Thematic Analysis of the Factors Facilitating and/or Could Facilitate Acceptance of/Interest in the Anatomage Table at Institutional Level
It is important to reiterate that this study is an effort by African researchers within the anatomical sciences community to obtain and share African perspectives and narratives of their contextual realities, formed opinions, and experiences on the Anatomage Table. This study followed a sequential explanatory design approach to get in proximity to an African narrative to support or develop the quantitative findings that we shared earlier.
The first question was for the respondents to share factors that promoted or might promote acceptance of the Anatomage Table in their current institution. The Dedoose was utilized to iteratively analyze the responses of the participants thematically. The theme summary was done using a taxonomic technique; the summary of what the respondents shared is presented in Figure 2. Attention was given to details in ensuring that no response was left uncaptured. The categorizing themes of the respondents’ self-documentation of the factors that facilitated or could facilitate acceptance or interest in the Anatomage Table include innovation, the impact of availability, technology age factors, training opportunities, integration considerations, awareness, and the drive of each institution’s management.
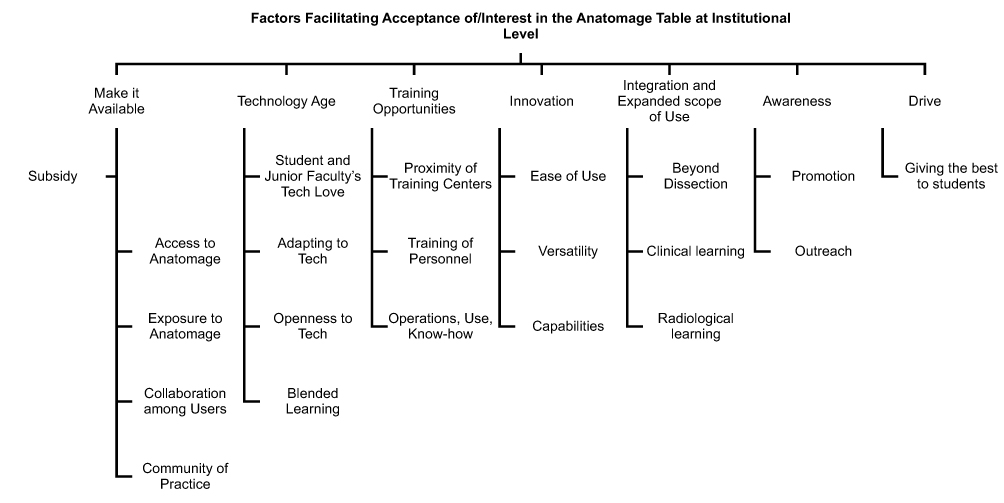 |
Figure 2 Taxonomic summary of the themes from the respondents’ response to the question on factors facilitating/could facilitate acceptance of/interest in the Anatomage Table at their own institution. |
In the words of one of the respondents, “make the Anatomage table available to us,” even if a subsidy arrangement was a representative theme. Respondents’ recurring opinion was that making it available within national, subnational, or regional reach will improve Anatomists’ curious access to it and would create an opportunity for more Anatomists and students as well as institutional management to be exposed to it. It will also develop easy awareness through promotional and outreach efforts to potential users. The exposures could encourage Anatomists to place a demand for it from institutional management. The impact of having more users within countries or regions of the continent could trigger user collaborations, which could help build up a community of practice for advancing the use of EdTech or digital technologies like the Anatomage Table in teaching, learning, and researching anatomical sciences. The respondents believed that a community of practice would help harness innovative intelligence and creative application possibilities toward advancing tech-based learning.
Another recurring theme was recognizing the Anatomage Table as a product of the technology and suitable for this age of technological advancement and appreciation in medical education. Many participants from different African institutions and regions raised the students’ and junior faculty members’ love for technology and technology-based learning tools as a major basis of their acceptance and a possible leaning towards or interest in the Anatomage. The older Anatomy faculty members and the general staff believed that this age’s compelling necessity of adapting to or being open to new technology did or could favor acceptance or interest in the Anatomage Table. Most of the respondents across all the institutions acknowledged that the ongoing pandemic has further uncovered new technologies like the Anatomage enabled blended learning.
The availability of training opportunities on the technological operations, use, and know-how of the Anatomage Table was also pointed out as a factor that could facilitate acceptance or interest in the Anatomage. The respondents further highlighted that having Anatomage training centers located closer would be beneficial for training opportunities or helpful for improving acceptance or interest in the Anatomage. Institutions that already had the Anatomage acknowledged that training their personnel or staff members boosted appreciation, acceptance, and interest in utilizing the Anatomage Table as a teaching or learning tool.
The innovative edge of the Anatomage Table that they mentioned was the ease of its use, versatility, and capabilities regarding its application in teaching, learning, research, and students’ assessment. Besides, some of the respondents also stated the potential use of the Anatomage beyond anatomical dissection to fully leverage its capabilities to integrate clinical and radiological anatomy makes it more appealing to instructors in the applied anatomy units. They also shared that its capabilities for integrative basic medical sciences, clinical or surgical subjects, and radiological presentations give a broader scope of its use, facilitating its acceptance by decision-makers at the institutional leadership level. Finally, one key facilitating factor at both departmental and management levels for acceptance and acquisition of the Anatomage, as shared commonly by participants from user institutions in their own words, was the drive to “give the best learning opportunities to students.”
Thematic Analysis of the Factors That Hindered or Could Hinder Acceptance or Interest in the Anatomage Table at Institutional Level
The second question was for the respondents to share their opinion on the factors that hinder or might hinder acceptance of/interest in the Anatomage Table in their current institution. The Dedoose software was utilized to iteratively analyze the responses of the participants thematically. The summary of the themes was done using a taxonomic technique; the summary of what the respondents shared is presented in Figure 3. Attention was given to details in ensuring that no response was left uncaptured.
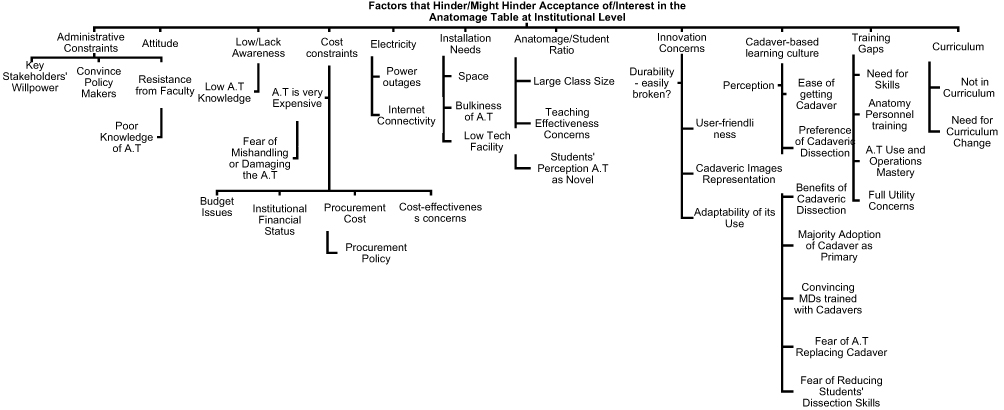 |
Figure 3 Taxonomic summary of the themes from the respondents’ response to the question on factors that hinder or might hinder the acceptance or interest in the Anatomage table at their own institution. |
The categorizing themes of the respondents’ self-documentation of the factors that hinder or could encourage acceptance or interest in the Anatomage Table include administrative constraints, attitude, cost constraints, low or lack of awareness, established cadaver-based learning culture, training gaps, curriculum, innovation concerns, installation needs, and electricity. The most recurring themes were cost and administrative constraints, teams being used to the cadaver-based learning culture, and training gaps. Paying attention to specific contexts helped us identify attitudes, installation needs, and important deterrents to acceptance.
Administrative constraints were mostly used to capture deterrent factors easily identifiable among those with the power to make decisions on acquiring or adopting the Anatomage Table. In their own words, these include the “willpower of key stakeholders,” the hurdle of “convincing institutional policymakers,” and possible “resistance from faculty or staff members” mostly due to “poor knowledge or awareness” about the Anatomy table. These factors are also greatly dependent on the “attitude” of the decision-makers.
The most mentioned category of hindering themes by respondents from almost all the institutions was the “cost constraint.” The sub-themes within this category, in their own words, include that the “Anatomy table is expensive,” and this is negatively reinforced by the “fear of mishandling or damaging” the table by the students. They identified further the dimensions of these constraints as budget issues and institutional financial status, which are foundational determinants of whether they can acquire it. The “procurement policy” of the school, as well as the “procurement cost” of the table, were also mentioned as deterrents, but above all the justification, the table’s “cost-effectiveness” was identified as a key hurdle to scale in convincing decision-makers.
Even after the Anatomage table is either donated or procured by any institution, a common African concern flagged by some of the respondents is electricity, considered in the dimensions of “power outages” extended to “internet connectivity struggles.” Closely related to these were the issues around “installation needs,” as one respondent mentioned. The various dimensions of this theme further identified by different respondents were “space needs,” which is important considering the “bulkiness of the table,” and the challenge of general “low technology facilities” in some institutions.
Interestingly, institutions with a well-established cadaver-based learning culture, as most reported by respondents from older generations of medical institutions, have a dismissive perception of Anatomage-based learning. In such contexts, other defining sub-themes identified as key deterrents include “ease of getting cadavers,” “preference of cadaveric dissection, appreciated benefits of cadaveric dissection,” and “institutional team majority’s adoption of cadavers” as the primary basis for learning or teaching Anatomy. Additionally, the “fear of Anatomage replacing cadaver” or the fear that Anatomage-based dissection could reduce the students’ dissection skills with time, which is key to surgical skillfulness at clinical stages, were also raised by the respondents, especially those from older schools. Finally, the uphill task of “convincing doctors who were trained entirely with cadavers” to accept or adopt the Anatomage was also mentioned by the participants.
The respondents, especially in western and eastern African regions, also brought the Anatomy curriculum externally regulated by designated bodies and internally influenced by the university’s standards. Since the Anatomage is novel, at least on the continent, they opined that the current curriculum being used had not integrated the Anatomage or a similar EdTech, and its effective use in teaching, assessments, and research, would need specific “changes in the curriculum.” Sadly, curriculum reviews do not happen regularly.
Thematic Analysis of the Respondents’ Personal Opinion on the Use of the Anatomage Table Technology in the Training of Medical and Allied Health Students
The last question sought the respondents’ individual opinions on the use of the Anatomage Table in the training of both medical and allied health students. The result of the iterative Dedoose analysis of the participants’ responses thematically summarized using a taxonomic technique is presented in Figure 4. Attention was given to details in ensuring that no response was left uncaptured. The categorizing themes of the respondents’ self-documentation of their concluding opinion of the Anatomage Table include that it is a timely, good, innovative technology, a digital medical education resource tool, and a complementing teaching tool to cadavers. It could supplement cadaveric dissection but not substitute it, or some believe could “solve shortages of cadavers” and has the potential to integrate anatomical science laboratory and classroom experiences.
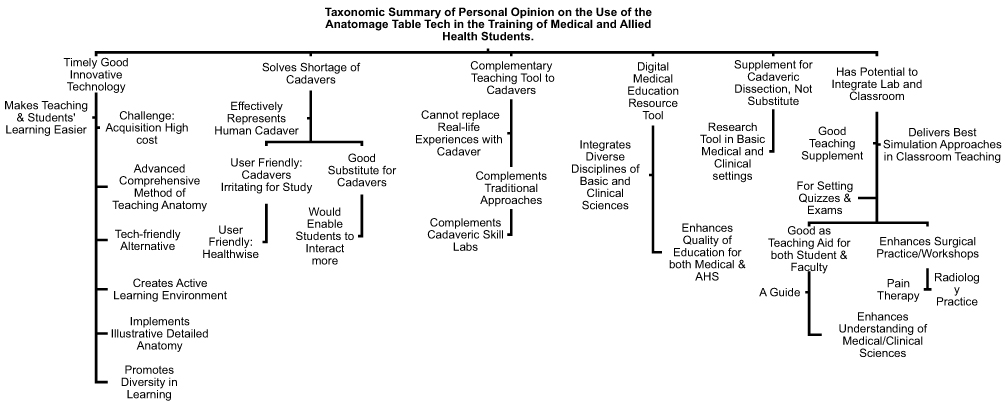 |
Figure 4 Taxonomic summary of the themes categorizing and capturing the respondent’s personal opinion on the use of the Anatomage Table in the training of medical and allied health students. |
The respondents believe that as a timely good innovative technology, the Anatomage Table “makes teaching and students’ learning easier,” serves as an “advanced comprehensive method of teaching anatomy,” a “tech-friendly alternative” that “implements illustrative detailed anatomy,” “promotes diversity in learning” and could better “create active learning environments” for medical and allied health students. However, respondents from every institution surveyed pointed out a major challenge, a “high acquisition cost.” In the words of a respondent from one of the institutions that have used it longest in Africa, the Anatomage can “solve shortages of a cadaver.” This was corroborated by their opinion that it “effectively represents human cadaveric images,” serves as a “good substitute for cadavers,” and is thought by even non-users to be a tool that “would enable students to interact more.” Besides, it could be more user-friendly with little or no associated health risks. Also, it might be more suitable for those that cadaver irritates during the study, according to respondents from both user and non-user schools.
The most recurring opinion was that the Anatomage Table could only be a “complementary teaching tool to cadavers” and that it “can’t replace real-life experience with cadavers.” Particularly, respondents from user institutions opined that it “complements the traditional cadaver-based approaches” to anatomy learning and inquiry, including being a good “complement for cadaveric lab” sessions. Furthermore, respondents from the schools with the most experience in using the table described it as a “supplement for cadaveric dissection, not a substitute” for it. They also shared that it is or could be a useful research tool in both basic medical and clinical stages. In addition, themes emerging from respondents’ institutions who are also users or who have been exposed to it described it as a digital medical education “resource tool” that “integrates diverse disciplines of basic medical and clinical sciences.”
Finally, those from user institutions opined that the Anatomage has the “potential to integrate both laboratory and classroom experience” in teaching and learning. The majority of user responses, including non-users, acknowledged it as a good supplementary anatomy teaching tool or EdTech. Specifically, a user shared that it “delivers the best simulation approaches for classroom teaching” and has been most helpful in setting standardized quizzes and exams for both medical and allied health students. Interestingly, the responses of the team from most experienced user institutions also shared that the Anatomage enhances surgical practice, hence useful for surgical workshops, citing examples in “pain therapy” and radiological practice. They endorsed it, in general, as a digital facility or EdTech that “enhances understanding of both medical and clinical sciences with anatomical inclination.”
Summary of Outcomes
The outcomes of the study include the following:
- Qualitative information about teachers’ perceptions and the influencing factors.
- Qualitative information about the teachers’ acceptance of Anatomage technology by teachers.
- Qualitative information about factors that influence acceptance or otherwise.
Discussion
African Anatomists on Factors That Could Facilitate Acceptance and Interest in the Anatomage Table at Individual and Institutional Levels
The consensus from the participant’s responses in the current study was that they were interested in using educational technology, specifically the Anatomage Table, in their teaching and training activities. Most of the participants generally value Anatomage as an EdTech, and they believed that it is consistent with advancements and trends in medical education globally. They further identified several factors that could promote their use of the Anatomage Table and any other form of educational technology. To avail Anatomage Table at an affordable cost was a major consideration. Another vital consideration is user training and promoting EdTech’s benefits amongst stakeholders, including educators, administrators, and students. The implication would be that resource allocation, especially to support medical education in African institutions, should place adequate priorities on EdTech. Many respondents did not think that the institutions lacked the financial capacity to procure Anatomage or other EdTech products, innovations, and facilities, but rather they are not prioritized. It would also point to the need to engage institutional leadership and decision-makers. It might be practical and convenient to do a cost analysis that proposes an adequate perspective on the required investment versus the benefits that Anatomage or any other EdTech would offer to the institutions to support the medical education and training delivery. The fact that these participants generally believed that the benefits would justify the cost is an important consideration.
Another key consideration arising from the consensus of the participants would be the need to provide training opportunities for anatomists and medical educators for Anatomage use. It was apparent from the responses that many people were not familiar with technical skills and know-how on using the Anatomage optimally or the educational principles that justify and support its use. The implication of this observation, therefore, includes the need for adequate investment of efforts and resources in training-the-trainer programs. Medical education courses should be promoted in the African continent, and these programs should emphasize, amongst other considerations, the value of EdTech, including the Anatomage and pedagogical principles that support the deployment of educational technology. Interestingly, it was difficult for certain stakeholders in the education industry to appreciate the fact that educational technologies are not mere creative products and innovations but are supported by quality educational research and principles and created with vital consideration to specific educational principles and requirements. Therefore the need to connect the use of these products to various theories and principles of education will not only help to enlighten users and potential users but also help them appreciate the need to integrate EdTech into medical education. EdTech’s use in alignment with educational principles has become integral to quality education delivery rather than being merely peripheral and complementary.11,24,25 We, therefore, advocate for training-the-trainer courses that would consider EdTech and educational principles as well as best practices that support their uses.
African Anatomists on the Factors That Hinder Acceptance and Interest in the Anatomage Table at Institutional Level
Expectedly, anatomists identified multiple factors that could limit their interest and opportunities to acquire educational technology such as the Anatomage Table and use the same to train medical and allied health science students. The factors included constraints to acquiring educational technologies at the administrative level, the perceived prohibitive cost of the technology, limited system thinking, and limited infrastructural support, among others. An effort to probe further what is considered as administrative constraints included not just the procurement cost of this technology but the fact that in certain instances, the relatively senior academics or leaders in the university systems who make key decisions are not always tech-inclined and might not make decisions that typically favor EdTech. The university administrative system is typically hierarchical, with most senior administrators being senior academics. Therefore, it is not unexpected that their appreciation for EdTech might reflect lags relative to the current trends and advancements, especially based on their impression of the current age relative to their age of training. Anatomists, therefore, flagged this as a major constraint and indicated that often administrators might typically be reluctant to invest in EdTech and extend its procurement.
In addition, there are specific instances where these anatomists also indicated that having a tech-inclined administrator made all the difference. The implication of this would be that continuous effort should be made to create awareness of the benefit of EdTech to medical and university education and training and continuously engage education administrators on the importance of EdTech and the need to embrace the culture of technology, especially in tertiary institutions. This, by extension, will positively influence the cost factor as these administrators and stakeholders will no longer consider the face value of what EdTech costs but values that such facilities add to medical education in the long run. Other considerations would also include the fact that EdTech products, such as the Anatomage, are fast becoming a necessity. Furthermore, there is a need to promote the practice of system thinking where stakeholders, including teachers within the university systems and the administrators and leaders, will critically consider the value and benefits of EdTech in alignment with global trends and advancement. As such, they will make vital decisions to promote innovations and technology not just as byproducts of the education system but as useful tools and materials to deliver modern education and produce students who value technology and innovation. It is clear that more than ever before, trainees in medical scientists and allied health professionals need to be tech-inclined, tech-complaint, and tech-literate, and this culture should be enshrined in the academic institutions that are responsible for their training. It is also consistent with global trends and informed opinions worldwide.7,26–30
African Anatomists on the Use of the Anatomage Table in the Training of Medical and Allied Health Students
It is clear from the current study that African anatomists are largely tech-inclined and interested in embracing EdTech, and more specifically, in this instance, the Anatomage Table, to support their teaching and training of students. It is also equally important to mention that certain previous opinions were likely based on the perceived impressions about what African medical educators think about the Anatomage Table or EdTech in general. However, the current effort presents empirical evidence to support that African anatomists and medical educators are tech-inclined, with an interest and enthusiasm to integrate technology into the processes of delivering medical education to students and trainees. These findings also present a clear position about how African anatomists would prefer to integrate this technology into their systems.
The key theme remained that these stakeholders in medical education would want to integrate the Anatomage Table into the educational system as a complementary tool or facility. They did not think that this EdTech should replace their traditional practice of cadaveric dissection. It is not unexpected, as many anatomists would think that cadaveric dissection is a gold standard for teaching gross anatomy, as well as a traditional pedagogical practice.31,32 The strength of this technology from anatomists’ positions and assertions, therefore, included its alignment with advancements and realities that have come with the age of technology, ease of use, and potential of the technology to add value to their efforts significantly. For medical educators or anatomists some of the related reasons are not far-fetched because it was clear that cadavers are readily available to anatomists and medical educators in many African institutions. While we did not extensively probe the source of cadavers, it would be interesting to note that previous reports have indicated that most African institutions do not depend on traditional body donors or bequest programs. Alternative special arrangements supported by governments and institutional stakeholders enable institutions to access the supply of cadavers to medical schools for dissections and other forms of anatomical demonstrations.33–35
It will be important, therefore, to further explore in the future how African medical schools acquire cadavers for dissection other than the conventional bequest program as obtainable in other parts of the world, especially the developed countries. Therefore, since cadavers are readily available, it will not be unexpected for most anatomists to hold their position that cadaver dissection should be retained as a traditional anatomical practice. To this end, they would determine that EdTech rather provides alternatives for digital dissections, simulations, and all other benefits that cadaver offers. It should also be noted that some participants indicated that despite the relative assurance of availability of cadavers, there are times or seasons of cadaver shortages. They, therefore, believed that EdTech might complement their Anatomy teaching when such shortages occur. The implications of not having an alternative to cadaveric dissection during such seasons of shortages would be that students lose the opportunity to dissect, creating a deficiency in meeting the specific objectives in certain aspects of their training.
We also did not unravel any major absolute cultural restrictions to the use of cadavers from the participants’ responses who did not consider the availability of cadavers as a critical challenge. However, the reluctance of individuals to bequest their bodies is tied to lack of awareness, limited education about the nature and benefits of body donors, bequest programs, and traditional and superstitious beliefs about the need for people to have their bodies in peace after death and for the bodies to be buried. While such reluctance, attributed to the traditional superstitious beliefs, could be said to be largely based on a lack of orientation, education, and awareness about the value of body bequest program to anatomical sciences and medical education, we could not find specific instances where based on beliefs and culture people were barred or prevented from dissecting cadavers. Therefore, such reluctance and restrictions were not institutional but individual and cultural. EdTech can clearly help since it has no such restrictions.
This study also identified from the experiences of anatomists and medical educators in certain parts of Africa that instances where cadaver dissections were impractical based on specific events in their past existed. Recent and prominent instances included cases where cadaver dissections were suspended due to the Ebola outbreak in certain African countries over a significant period. Epidemiological measures to prevent the spread of the deadly Ebola virus included the need to cremate bodies and reduce contact with such bodies, thus, necessitating stopping cadaver dissections altogether. It might be logical, however, to think that there could have been alternative sources of cadavers apart from bodies that died of Ebola. Contrarily, the lack of bequest programs and instituted cadaver procurement programs might have necessitated the decision to cancel cadaveric dissection altogether to reduce risk. It is, therefore, important to mention that in such instances, the availability of educational technology such as the Anatomage Table could become a very important avenue to sustain quality teaching since such EdTech offers quality digital and technological alternatives to the traditional cadaver dissection. The Covid-19 pandemic-related social and physical distancing measures, especially in 2020 and 2021, had also affected, stopped, or limited cadaver dissection in many medical schools.36 However, there were specific reports where institutions that continued medical education seamlessly switched to digital and virtual dissections and demonstrations with significant successes because of their ability to model the traditional cadaver dissection and demonstration using EdTech or digital technology. To ensure optimal performance of EdTechs, the ASIC Framework has been published, emphasizing the need to consider four major factors, including adaptation [A], standardization [S], integration [I], and compliance with regulations, principles, and standards [C] to support medical education and training.37
Conclusion
We, therefore, conclude that African anatomists and medical educators embrace EdTech to support medical education, specifically, the teaching of anatomical sciences to medical and allied health science students. It is believed that efforts to promote the EdTech integration into the teaching and training systems would include leadership and administrative support, availability of resources and funding, supportive infrastructural setup, and an enabling and EdTech-supportive culture of training and learning. Acquisition of competencies, particularly through the training-The-trainer programs, will also help. Continuous effort should therefore be used to promote the integration of EdTech into medical and allied health science training programs in Africa.
Acknowledgments
Special thanks to the DVC Academic office for technical support, the UGHE HR for hiring the RA, the UGHE’s Finance Department for the financial management of the grant, and the UGHE’s BMS Division for technical and administrative support. It is very important to specially acknowledge all the African anatomists, professional society stakeholders, and academic leaders in the African countries who participated in the study.
Funding
This project was funded by the UGHE Dean’s Seed Research Grant, UG0365.413, in 2020.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Turney BW. Anatomy in a modern medical curriculum. Ann R Coll Surg Engl. 2007;89(2):104–107. doi:10.1308/003588407X168244
2. Anatomage. Anatomage table- the world first and only virtual dissection table. Available from: https://www.anatomage.com/table/.
3. Fyfe G, Fyfe S, Dye D, Radley-Crabb H. Use of Anatomage tables in a large first year core unit. In Carter H, Gosper M, Hedberg J (Eds).
4. Ruiz V. The Anatomage table – visualizing life size anatomy. Available from: http://streetanatomy.com/2013/06/13/the-anatomage-table-visualizing-life-size-anatomy/.
5. Periya SN, Moro C. Applied learning of anatomy and physiology: virtual Dissection tables within medical and health sciences education. Bangkok Med J. 2019;15(1):121–127. doi:10.31524/bkkmedj.2019.02.021
6. Martín JG, Mora CD, Henche SA. Possibilities for the use of Anatomage (the anatomical real body-size table) for teaching and learning anatomy with the students. Biomed J Sci Tech Res. 2018;4(4):94. doi:10.26717/BJSTR.2018.04.001094
7. Guze PA. Using technology to meet the challenges of medical education. Trans Am Clin Climatol Assoc. 2015;126:260–270.
8. Saffari Z, Takmil F, Arabzadeh R. The role of educational technology in medical education. J adv med educ prof. 2014;2(4):183.
9. Moran J, Briscoe G, Peglow S. Current technology in advancing medical education: perspectives for learning and providing care. Acad Psychiatry. 2018;42(6):796–799. doi:10.1080/10447310802546716
10. Han ER, Yeo S, Kim MJ, Lee YH, Park KH, Roh H. Medical education trends for future physicians in the era of advanced technology and artificial intelligence: an integrative review. BMC Med Educ. 2019;19:460. doi:10.1186/s12909-019-1891-5
11. Owolabi J, Bekele A. Implementation of innovative educational technologies in teaching of anatomy and basic medical sciences during the COVID-19 pandemic in a developing country: the COVID-19 silver lining? Adv Med Educ Pract. 2021;12:619–625. doi:10.2147/AMEP.S295239
12. Tuma F. The use of educational technology for interactive teaching in lectures. Ann Med Surg. 2021;62:231–235. doi:10.1016/j.amsu.2021.01.051
13. Watkins DC. Qualitative research: the importance of conducting research that doesn’t “count”. Health Promot Pract. 2012;13(2):153–158. doi:10.1177/1524839912437370
14. Cristancho SM, Goldszmidt M, Lingard L, Watling C. Qualitative research essentials for medical education. Singapore Med J. 2018;59(12):622–627. doi:10.11622/smedj.2018093
15. Chapman AL, Hadfield M, Chapman CJ. Qualitative research in healthcare: an introduction to grounded theory using thematic analysis. J R Coll Physicians Edinb. 2015;45(3):201–205. doi:10.4997/JRCPE.2015.305
16. Sawatsky AP, Ratelle JT, Beckman TJ. Qualitative research methods in medical education. Anesthesiology. 2019;131(1):14–22. doi:10.1097/ALN.0000000000002728
17. Dilshad RM, Latif MI. Focus group interview as a tool for qualitative research: an analysis. Pak J Soc Sci. 2013;33:191–198.
18. Merton RK, Fiske M, Kendall PL. The Focused Interview: A Manual of Problems and Procedures. Glencoe: Free Press; 1956.
19. Patton PQ. Qualitative Research & Evaluation Methods. Thousand Oaks: Sage Publications; 2002.
20. Stewart DW. Focus groups. In: Frey BB, eds. The SAGE Encyclopedia of Educational Research, Measurement, and Evaluation. 2018:687–692.
21. Carey MA, Asbury JE. Focus Group Research. Walnut Creek: Left Coast Press; 2012.
22. Sim J, Waterfield J. Focus group methodology: some ethical challenges. Qual Quant. 2019;53(1):3003–3022. doi:10.1007/s11135-019-00914-5
23. Wheeler K. What is an in-depth interview? SAGE Research Methods; 2021. Available from: https://www.doi.org/10.4135/9781529763119.
24. Alkhowailed MS, Rasheed Z, Shariq A, et al. Digitalization plan in medical education during COVID-19 lockdown. Inform Med Unlocked. 2020;20:100432. doi:10.1016/j.imu.2020.100432
25. Owolabi J, Bekele A. Medical educators’ reflection on how technology sustained medical education in the most critical times and the lessons learnt: insights from an African medical school. Digit Health. 2021;7:20552076211059358. doi:10.1177/20552076211059358
26. Salter G. Factors affecting the adoption of educational technology. In: Howard C, Boettcher J, Justice L, Schenk K, Rogers P, Berg G, eds. Encyclopedia of Distance Learning. IGI Global; 2005:922–929. doi:10.4018/978-1-59140-555-9.ch133
27. Wiecha J, Heyden R, Sternthal E, Merialdi M. Learning in a virtual world: experience with using second life for medical education. J Med Internet Res. 2010;12(1):e1. doi:10.2196/jmir.1337
28. Azizi SM, Khatony A. Investigating factors affecting on medical sciences students’ intention to adopt mobile learning. BMC Med Educ. 2019;19:381. doi:10.1186/s12909-019-1831-4
29. Lin HC, Tu YF, Hwang GJ, Huang H. From precision education to precision medicine: factors affecting medical staff s intention to learn to use AI applications in hospitals. Educ Techno Soc. 2021;24(1):123–137.
30. Dawidziuk A, Kawka M, Szyszka B, Wadunde I, Ghimire A. Global access to technology-enhanced medical education during the COVID-19 pandemic: the role of students in narrowing the gap. Global Health. 2021;9(1):10–14. doi:10.9745/GHSP-D-20-00455
31. Ghosh SK. Human cadaveric dissection: a historical account from ancient Greece to the modern era. Anat Cell Biol. 2015;48(3):153–169. doi:10.5115/acb.2015.48.3.153
32. Chia T, Oyeniran OI. Anatomy education in Nigeria: challenges and prospects. J Contemp Med Educ. 2019;9(3):61–65. doi:10.5455/jcme.20190531113058
33. Akinola OB. Formal body bequest program in Nigerian medical schools: when do we start? Anat Sci Ed. 2011;4:239–242. doi:10.1002/ase.226
34. Mazyala EJ, Revocatus M, Manyama M, et al. Human bodies bequest program: a wake-up call to Tanzanian medical schools”. Adv Anat. 2014;2014:1–6. doi:10.1155/2014/940472
35. Habicht JL, Kiessling C, Winkelmann A. Bodies for anatomy education in medical schools: an overview of the sources of cadavers worldwide. Acad Med. 2018;93(9):1293–1300. doi:10.1097/ACM.0000000000002227
36. Onigbinde OA, Ajagbe AO, Oyeniran OI, Chia T. Post-COVID-19 pandemic: standard operating procedures for gross anatomy laboratory in the new standard. Morphologie. 2021;105(350):196–203. doi:10.1016/j.morpho.2020.10.004
37. Owolabi JO. Proposing a framework guide for the integration of educational technologies and innovations into the teaching of anatomy and medical sciences: the ASIC framework. Adv Med Educ Pract. 2021;12:1277–1282. doi:10.2147/AMEP.S338262
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.