Back to Journals » Drug, Healthcare and Patient Safety » Volume 18
Adverse Events Associated with Tirzepatide: Updated Pharmacovigilance Analysis Using FAERS (2022 Q1-2025 Q1) with an Adapted Time-to-Onset Method
Authors Gu S ![]()
Received 29 July 2025
Accepted for publication 3 January 2026
Published 8 January 2026 Volume 2026:18 556918
DOI https://doi.org/10.2147/DHPS.S556918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Siew Siang Chua
Saisai Gu
Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Saisai Gu, Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected]
Purpose: Tirzepatide, the first dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist with rapidly expanding clinical use, requires detailed post-marketing pharmacovigilance to monitor emerging safety signals. This study aims to identify and characterize specific adverse events (AEs) associated with tirzepatide utilizing FDA Adverse Event Reporting System (FAERS).
Patients and Methods: The datasets were cleaned and standardized using Python, a programming language for data processing, and MySQL, a database management system, to ensure accuracy and consistency before analysis. Subsequently, AE signals were detected via four quantitative disproportionality algorithms, sorted and categorized by demographics, gender, and clinical prioritization, with a modified Weibull model developed to analyze AE onset timing.
Results: A total of 67,305 cases (75.83% female) and 137,583 adverse events were identified related to tirzepatide. One hundred and forty-four AE signals showed statistically significant signals suggesting a potential association with tirzepatide, with several new including postmenopausal haemorrhage and menstrual disorder (implying regulatory interference on sex hormones), Wernicke’s encephalopathy and sleep disorder (malnutrition caused by low intake). Pancreatitis, impaired gastric emptying, dehydration and cholelithiasis carried higher risks with serious clinical outcomes. Sleep disorder, delayed gastric emptying, and medullary thyroid cancer are more common in males; starvation ketoacidosis and incorrect injection site, in females. The median time-to-onset (TTO) was 6.36 days (Interquartile Range (IQR) 0.85– 31.2) with the Weibull shape parameter (β) of 0.44, indicating an early failure profile.
Conclusion: This study uncovered new risks of tirzepatide, including AEs associated with skin, menstruation, psychiatric and nervous system. Median TTO was corrected to within a week, highlighting the need for early monitoring before clinicians prescribe tirzepatide, and special attention should be given to patients who have pre-existing digestive dysfunction, malnutrition, or a family history of thyroid disease.
Keywords: adverse events, adapted Weibull distribution, FAERS database, tirzepatide, GIP/GLP-1 receptor agonist
Introduction
Type 2 diabetes and obesity pose intertwined global public health crises, affecting over 1 billion people and driving rising rates of cardiovascular disease, liver failure, and premature mortality.1,2 Despite advances in pharmacotherapy, unmet needs persist: many patients fail to meet glycemic or weight-loss targets, and existing agents like glucagon-like peptide-1 (GLP-1) receptor agonists (eg, semaglutide) are limited by tolerability issues—particularly gastrointestinal3 (GI) adverse events in ~44% of users, leading to 4.3% treatment discontinuation.4
Tirzepatide, a novel receptor agonist binding to glucose-dependent insulinotropic polypeptide (GIP) in addition to GLP-1, has emerged as a transformative therapy.5 Its superiority arises from balanced agonism at GIP and GLP-1 receptors (co-expressed in pancreatic β-cells, hypothalamus, and brainstem nuclei) and a C20 fatty-diacid backbone that extends half-life via albumin binding, enabling weekly dosing.6,7 It outperformed semaglutide in HbA1c reduction, achieved average weight loss up to 20.9% at 72 weeks,8,9 and reduced the risk of cardiovascular death or worsening heart failure by 38%.10 These results propelled rapid regulatory approvals, as Mounjaro® (tirzepatide) for Type 2 diabetes (2022)11 and Zepbound® (tirzepatide) for obesity (2023).12 The rapid uptake of tirzepatide for obesity, beyond its initial diabetes indication, has expanded exposure to diverse populations with complex comorbidities; although it provides significant weight loss, cardiometabolic benefits, and improved life quality in non-diabetic obese individuals, a detailed pharmacovigilance analysis remains essential to assess its long-term safety and clinical application. The FDA Adverse Event Reporting System (FAERS)—a key post-marketing surveillance tool—aggregates global spontaneous AE reports, facilitating detection of rare/long-term risks.13 However, existing analyses of tirzepatide-related AEs (systematic reviews, cohorts, case–control studies) are outdated with limited data. Most of them covered periods before 2024 Q2,14,15 missing reports post the latest obesity indication approval.
Tirzepatide’s labeled safety profile primarily includes mild-to-transient GI disturbances (nausea: 30–40%, diarrhea: 20–25%, vomiting: 15–18%, constipation: 12–15%). Black box warnings highlight risks of medullary thyroid cancer and acute pancreatitis (incidence: 0.32–0.39%),16 implying that before medication administration, patients must undergo strict screening to exclude those with a (family) history of medullary thyroid cancer, a history of pancreatitis, and high-risk conditions (such as biliary tract diseases or hyperlipidemia). Given its expanding use and evolving risk profile, this study aims to provide an up-to-date, comprehensive safety analysis using 2022–2025 FAERS data, focusing on: 1) identifying novel signals via disproportionality screening; 2) characterizing AE distributions across gender differentiation and clinical priority; 3) applying modified Weibull distributions to determine time-to-onset patterns of AE signals in subgroups; 4) analyzing AE signals linked to severe outcomes. This work shall address critical gaps in tirzepatide pharmacovigilance, informing clinical practice and regulatory policies to enhance patient safety amid therapeutic expansion.
Materials and Methods
Data Source and Preprocess
This pharmacovigilance study extracted and analyzed tirzepatide-associated adverse events from FAERS database, covering the period from 2022 Q1 to 2025 Q1. Data were retrieved from the FDA official website (https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html), which provides a zip file containing seven dataset types.17 Raw data were standardized, transformed, and stripped of irrelevant fields using Python’s Pandas library. Processed datasets were imported into MySQL 8.0 for subsequent cleaning, merging, and screening. DEMO data were deduplicated under FDA-recommended criteria: retaining unique cases with the latest FDA_DT and PRIMARYID.18 DRUG reports were filtered by generic name (tirzepatide in DRUGNAME or PROD_AI fields) or trade name (Mounjaro or Zepbound in DRUGNAME), with only reports where tirzepatide was marked as the primary suspect19 (ROLE_COD = PS) retained to ensure reliability.
Patient characteristics (gender, age, weight, reporting country, annual AE amount, outcome, and indication) were analyzed using DEMO data. AEs in REAC data were normalized and coded using Medical Dictionary for Regulatory Activities (MedDRA, version 28.0).20 Meanwhile, WHO Vigilance (https://www.vigiaccess.org/), a database aggregating anonymized individual case safety reports on medicinal products from member states, pharmaceutical companies and healthcare professionals worldwide, was used as a supplemental control. The author queried (2025–07-06) and selected results on AE distribution at SOC level to strengthen the robustness of this study’s findings.
Data Mining Algorithms and Statistical Analysis
Data from the DEMO, DRUG, and REAC files were merged and linked to the MedDRA dictionary to derive the corresponding SOC information. Four algorithms were used to detect potential signals at the preferred term (PT) and SOC levels, including two mean difference methods [Reporting Odds Ratio (ROR),21 Proportional Reporting Ratio (PRR)22] and two Bayesian models [Bayesian Confidence Propagation Neural Network (BCPNN),23 Multi-item Gamma Poisson Shrinker (MGPS)]. ROR provides a consistent, low-bias risk ratio estimate; PRR assesses relative risk but is prone to false positives; BCPNN remains stable with small sample sizes and MGPS, via polynomial distribution and Bayesian adjustment, better handles sparse data and identifies multidimensional/rare signals.23,24 All four algorithms are used to measure the association between the relevant drug (in comparison with other drugs) and specific adverse reactions. Meanwhile, the gender-differentiated AE signals were also illustrated using PRR and the adjusted p value (the Benjamini–Hochberg correction of Fisher’s exact p value, AEs with adjusted p < 0.001 were selected). The elements for calculation and the formula with respective thresholds were presented in Supplemental Table S1–2 The AEs that satisfied all four algorithms were recognized as valuable signals, and to reduce false positives, only AE signals with at least 3 reports were selected. These methods were also applicable in subgroup analysis.
Clinical Prioritization of Signals
Among AE signals, those prone to serious adverse reactions and requiring special attention were further identified using a previously published method.25 This approach leverages the European Medicines Agency (EMA)’s Designated Medical Event (DME) and Important Medical Event (IME, version 28.0) lists (available at https://www.ema.europa.eu/en/human-regulatory-overview/research-development/pharmacovigilance-research-development/eudravigilance/eudravigilance-system-overview) to prioritize suspected AE reports. Briefly, a semiquantitative score method composed of 5 parts was applied to rank the priority: number of AE reports, ROR, mortality rate, DME or IME, and biological plausibility.26,27 By summing up the scores of each item for the PT signals, their priority was divided into three levels: weak (0–4), moderate (5–7), and strong (8–10).
Time-to-Onset Analysis
Time-to-onset (TTO) was calculated as the interval between tirzepatide initiation (EVENT_DT in DEMO files) and adverse event occurrence (START_DT in THER files).28 The Weibull distribution was modified to handle TTO data recorded as 0: these values were randomly reassigned to x/24 via Python’s random library, where x is a random integer between 1 and 24. This method enhances fitting accuracy and reliability compared to prior approaches that either excluded 0 data or treated it as a near-zero value.23 Stability was confirmed through repeated calculation. To ensure data quality, cases with incomplete dates, missing values, multiple START_DT entries, or START_DT preceding tirzepatide’s approval date (2022–05-13) were excluded. TTO profiles were evaluated at both the case and SOC levels using the median (interquartile range, IQR), min–max, and Weibull shape parameter.
AE Signals with Serious Outcomes
To exclude ambiguous data, only records with available OUTC_COD as death (DE), life-threatening (LT), hospitalization (HO), disability (DS), or other serious events (OT) were selected and taken as serious outcomes. Tirzepatide-associated cases were linked to available OUTC_COD reports to analyze the proportion of PTs leading to serious outcomes. Given the limited number of such reports, only AEs with an association ratio over 30% to severe outcomes were included. In addition, the demographic profile of AE signals was analyzed.
Results
Descriptive Analysis
From 5,521,211 patient records in the DEMO files (2022 Q1–2025 Q1), 4,758,917 valid records were retained after deduplication and exclusion of deleted cases by FDA. During this period, there were 24,883,081 medication records, of which 67,305 identified tirzepatide as the primary suspect (PS) and were matched to valid DEMO records. Then, 137,583 adverse reaction reports with standardized preferred terms were extracted from a total of 19,146,450 REAC records (Figure 1).
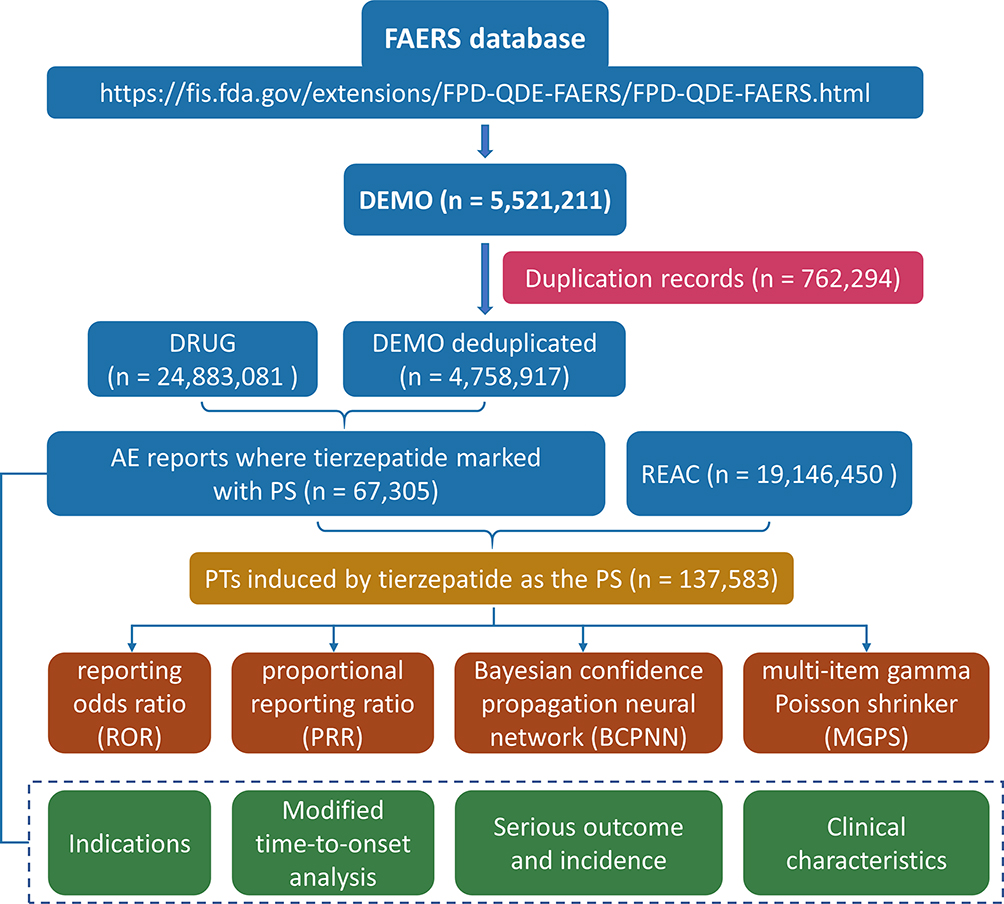 |
Figure 1 The schematic diagram of the analytical framework for this study. |
Demographic characteristics of tirzepatide-associated AEs are summarized in Table 1. Of 57,281 cases with gender data, females predominated (n=43,438, 75.83%) versus males (n=13,843, 24.17%). Age distribution showed a concentration in >24 and ≤79 years: 26.55% (>24 and ≤44), 53.30% (>44 and ≤64), and 18.39% (>64 and ≤79). Among 2,585 cases with weight records, 72.07% weighed over 80 kg. Top 5 indications for tirzepatide included 2 glucose-control-related (48.61%) and three weight-control-related (31.87%). Most cases were reported from the United States (95.26%). These findings were consistent with the query result for tirzepatide from WHO Vigilance (Figure S1). AE reports surged annually from 2022 onward: 3,109 (2022), 15,776 (2023), and 37,214 (2024). The vast majority (93.87%) of the reporters were consumers. Due to the substantial amount of missing outcome data in FAERS, only 9,266 cases had available outcome data, and 98.22% of them were recorded as serious outcomes in this study.
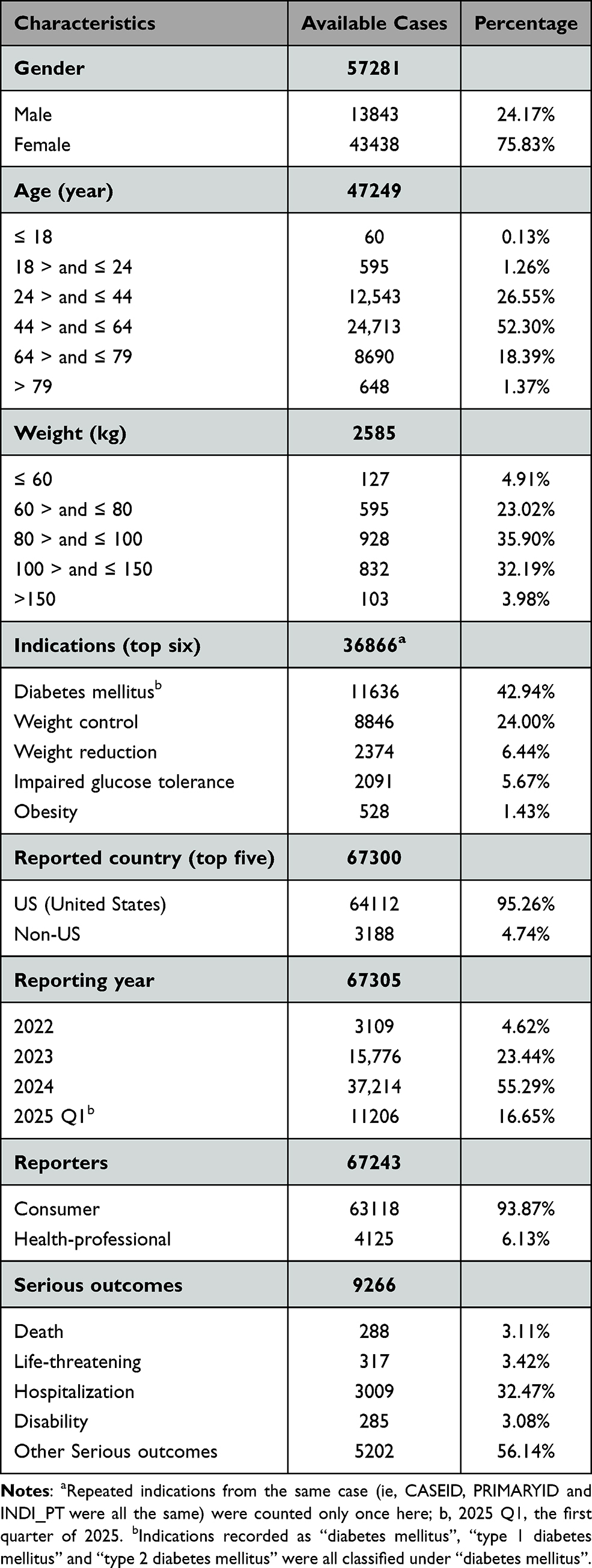 |
Table 1 Demographic Characteristics of Cases Associated with Tirzepatide (2022 Q1 ~ 2025 Q1) |
Disproportionality Analysis
Among all the 137583 PTs involving 26 SOC categories, significant SOCs related to tirzepatide which met at least one of the four algorithms were Injury, poisoning and procedural complications (SOC:10022117, n = 39065, ROR = 2.63), General disorders and administration site conditions (SOC:10018065, n = 34930, ROR = 1.62), Gastrointestinal disorders (SOC: 10017947, n = 26395, ROR = 2.66), and Metabolism and nutrition disorders (SOC:10027433, n = 4551, ROR = 1.77) (Table S3).
A total of 144 tirzepatide-related AE signals in 17 SOCs were detected in this work. Most of them were consistent with the side effects specified in the instruction manual, such as gastrointestinal disorders, local discomfort caused by drug devices, and adverse symptoms related to blood glucose fluctuations. However, some new adverse effects were identified simultaneously. The 14 new PT signals (not specified in the instructions for tirzepatide and not disclosed in previous studies) are listed in Table 2, such as postmenopausal haemorrhage (n = 46, ROR: 9.92), menstrual disorder (n = 37, ROR: 2.85), skin sensitization (n = 17, ROR: 9.43), anorexia nervosa (n = 5, ROR: 10.31), sleep disorder (n = 120, ROR: 4.0), Wernicke’s encephalopathy (n = 7, ROR: 6.7), muscle atrophy (n = 77, ROR: 3.0), neck mass (n = 22, ROR: 3.5) and lymph node pain (n = 27, ROR: 6.28).
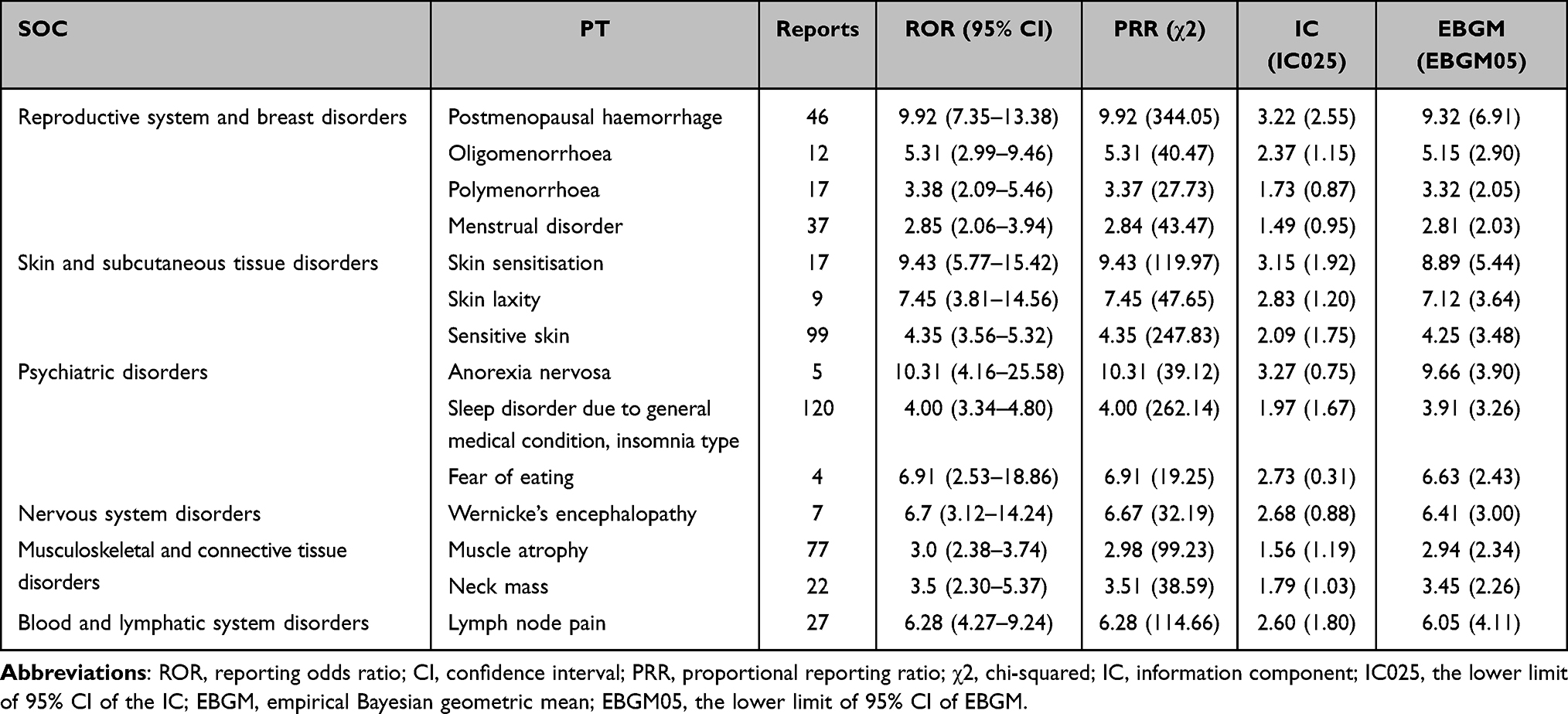 |
Table 2 Unexpected Adverse Events of Tirzepatide at the PT Level |
Gender-Differentiated AE Signals
For the overall AEs with available gender data, females still constituted the majority at the SOC level, with 78.5% for injury, poisoning and procedural complications (n = 36,152), 80.5% for general disorders and administration site conditions (n = 31240) and 73.3% for gastrointestinal disorders (n = 21,770) (Figure 2A). The volcano map in Figure 2B shows gender differentiation among AEs related to tirzepatide. The dots represent each AE and the marked are significant ones (PRR > 16 and the adjusted p value < 0.05), where blue dots indicate notable AEs in males and red dots in females. Beyond injection site abnormalities observed in both genders, males exhibit a higher prevalence of sleep disorders, delayed gastric emptying, and medullary thyroid cancer, whereas females are more prone to starvation ketoacidosis and incorrect injection sites.
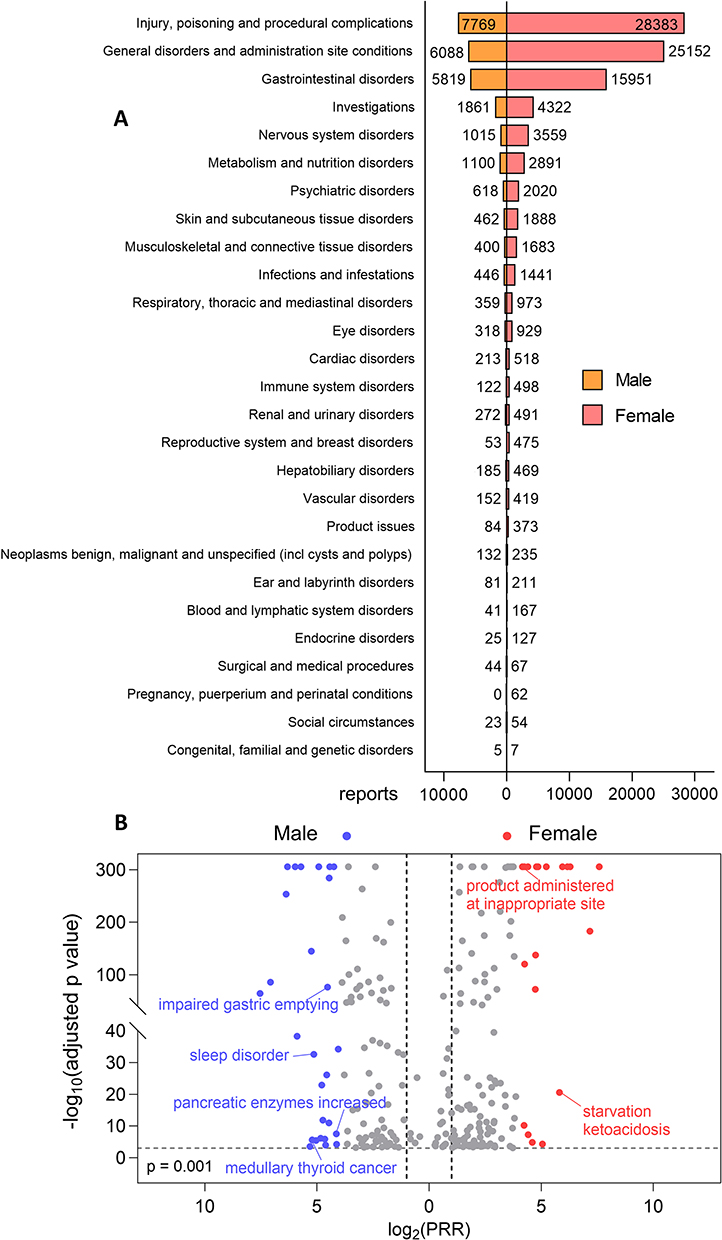 |
Figure 2 (A) Distribution of AE reports with available gender information presented at the SOC level. (B) Gender-differentiated AE signals. The vertical coordinate indicates the adjusted p value after -log10 conversion. The marked dots are significant ones (blue for male and red for female).PRR, proportional reporting ratio. |
Clinical Prioritization of Signals
As shown in Table S4, 9 were classified as IME and 2 as DME with the analysis of the 85 most frequent PT signals (occurrence >30). Pancreatitis is noted as a significant adverse effect as marked in the label. Clinical priority scores were distributed as: 12 weak, 72 moderate, and 1 strong. Forty-seven PTs from Gastrointestinal disorders and General disorders and administration site conditions scored exceeding 6, primarily due to high report volume, elevated ROR scores, and strong association with tirzepatide administration, such as impaired gastric emptying, eructation, flatulence, small intestinal obstruction and injection site discomfort.
Time-to-Onset of Tirzepatide-Related Adverse Events
Merging EVENT_DT (DEMO) and START_DT (THER) yielded 3,485 valid duration records, including 1,405 with a TTO of 0 days. These 0-day records—indicating the same day post-administration—were randomly reassigned using the aforementioned strategy, with stability confirmed (Table S5). Weibull distribution fitting of the optimized data showed a median onset time of 6.36 days (IQR 0.85–31.2 days) (Table S6). Most AEs occurred within the first week (62.28%) or month (75.5%) of initial treatment (Figure 3). Weibull shape parameter analysis yielded a β value of 0.44 (0.42–0.45), indicating an early failure pattern.
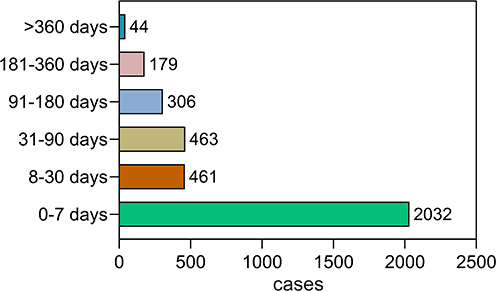 |
Figure 3 TTO distribution of cases with tirzepatide as the primary suspect drug. |
In line with common sense, TTO analysis at SOC level (Table 3) showed immune system disorders had the shortest median TTO (2.16 [0.24–12.38] days), followed by injury, poisoning, and procedural complications (3.12 [0.35–17.73] days). For several SOCs with the highest number of adverse reactions, the median TTOs were all less than one week such as administration site conditions (4.91 [0.63–24.88] days) and gastrointestinal disorders (5.57 [0.75–27.09] days). SOCs with median TTO exceeding 1 month included surgical/medical procedures (38.9 [9.13–121.93] days), hepatobiliary disorders (43.63 [10.75–131.63] days), and thyroid carcinogenesis (benign/malignant, 48.9 [9.99–171] days). Weibull shape parameter for all SOCs yielded values <1 (0.4–0.63), confirming the early failure pattern.
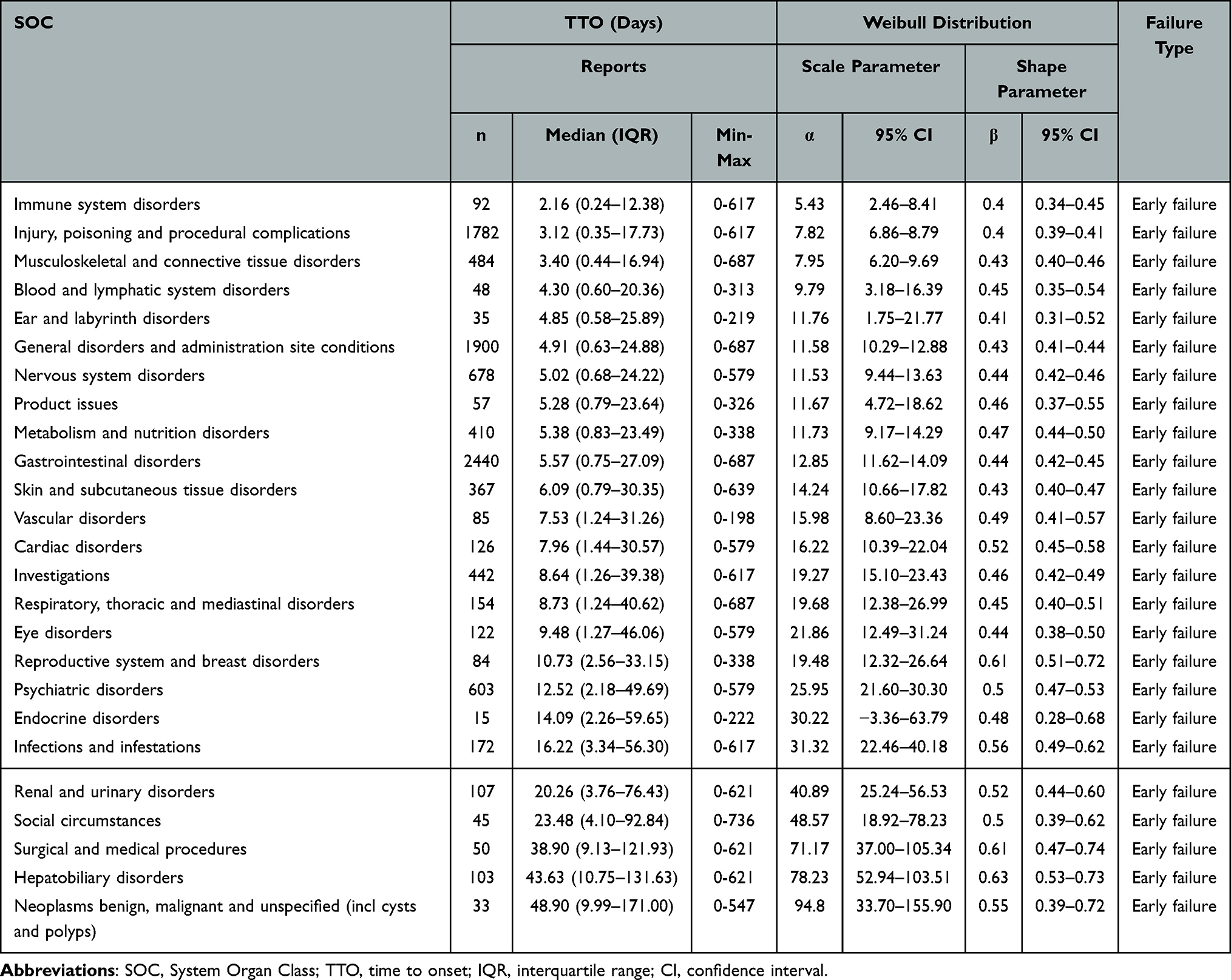 |
Table 3 Results of Time-to-Onset Analysis of Tirzepatide-Related AEs at SOC Level (Sorted by Median) |
AE Signals That Leading to Serious Outcomes
Certain PTs are more likely to lead to serious consequences. This study also analyzed the proportion of PTs related to tirzepatide that ultimately result in serious outcomes. We conducted statistics on the PTs with a frequency of serious outcomes exceeding 3 records, an occurrence proportion over 50%, and showing significant signals (EBGM05 > 2). Among these PTs, the most frequent SOCs were metabolism and nutrition disorders, hepatobiliary disorders and gastrointestinal disorders including AE signals of pancreatitis, impaired gastric emptying, cholelithiasis and dehydration with an occurrence quantity exceeding 100 (Table S7). The findings should alert patients with such adverse reactions in the real world. Among these AEs, females still account for the majority (59.9%, Figure S2). However, the female-to-male ratio has decreased compared to that of all AEs (2.27 vs 3.14 in Table 1, p < 0.001), indicating that males are more likely to experience severe outcomes when developing such adverse reactions. In addition, adverse reactions of tirzepatide in patients over 64 years old or weighing >100 kg are more likely to result in serious outcomes (Figure S2, compared with Table 1). This is consistent with real-world situations where overweight and elderly patients often exhibit age-related physiological changes and increased susceptibility to AEs, indicating higher-risk subgroups requiring targeted monitoring.
Discussion
Adverse Events Associated with Tirzepatide
Prior to its approval, tirzepatide garnered significant interest in preclinical and controlled clinical trials. Beyond its primary indications for diabetes and weight management, tirzepatide demonstrates additional therapeutic benefits, including reducing all-cause cardiovascular risk in patients with diabetes and obesity, as well as improving blood pressure and lipid profiles—specifically lowering low-density lipoprotein cholesterol and triglycerides.10,29 Tirzepatide’s mechanism of action could induce a state of passive calorie restriction and malnutrition, which may cause metabolic and digestive disturbances and even neuropsychiatric effects, such as anorexia nervosa, sleep disorder, muscle atrophy and Wernicke’s encephalopathy (indicating vitamin B1 deficiency)–newly identified AEs in this study. This mechanistic insight helps contextualize the frequent reporting of neurological and psychiatric adverse events within the FAERS database.30 Moreover, skin sensitization may stem from the administration route of tirzepatide or immune responses triggered by peptide drugs. AEs of the reproductive system may result from the regulatory interference of tirzepatide on the hypothalamic-pituitary-gonadal (HPG) axis.31 Additionally, since GLP-1 is highly expressed in thyroid C cells, tirzepatide may stimulate the proliferation of these cells,32,33 which could lead to neck mass or lymph node pain.
After its approval, there have been several pharmacovigilance studies on tirzepatide. The typical side effects mentioned in the manual have been widely verified in the real world, such as gastrointestinal disorders, diabetic-related eye diseases, thyroid cancer, hepatobiliary disorders and so on. These side effects from the top three SOCs are described as mild or weak in the label, but sometimes they can become quite troublesome.34 For instance, as mentioned above, pancreatitis, acute kidney injury, intestinal obstruction, dehydration, cholelithiasis, and anorexia all have a high probability of leading to serious outcomes. Consequently, clinicians should provide comprehensive medication education, particularly to patients with relevant comorbidities, outlining preventive measures and management strategies for potential adverse effects.
Gender-Differentiated AE Signals
The findings regarding gender-differentiated AE signals of tirzepatide provide critical insights into personalized pharmacovigilance, aligning with emerging evidence on sex-related disparities in the safety profiles of GLP-1 receptor agonists.35 Except for the gender difference among patients who originally used tirzepatide, the predominance of females in several SOCs may stem from multiple interrelated factors. Physiologically, females often exhibit heightened sensitivity to peptide-based therapeutics due to differences in drug-metabolizing enzyme activity and hormonal fluctuations, which could modulate AE susceptibility.36 Additionally, non-biological factors such as sex-specific differences in injection technique proficiency or healthcare-seeking behavior for mild AEs may contribute to the observed gender imbalance in reporting.35
The Time-to-Onset Analysis
TTO measures the interval between medication initiation and the first occurrence of an adverse drug reaction (ADR). It is critical for causality assessment, as a plausible TTO strengthens the drug-event association. TTO pattern analysis aids in safety signal detection, risk period identification, distinguishing ADRs from concurrent illnesses, and refining safety monitoring. The TTO median indicates the typical time-to-reaction, defining monitoring windows and characterizing ADR patterns. In Weibull distribution analysis, the shape parameter (β) reveals the ADR hazard pattern: β < 1 signifies early failure (eg, hypersensitivity), contrasting with β ~ 1 (random failures, eg, chemotherapies) or β > 1 (wear-out failures, eg, cumulative toxins).15,37 Previous studies reported a tirzepatide-related median TTO of 23 (7–90) days and a Weibull β of 0.63 (95% CI: 0.61–0.66),38 which shows considerable inconsistency with the present finding (β = 0.44). Given the minimum TTO taken as 1, improper handling of TTO=0 cases in calculations may explain this deviation, and the same issue can also be noted in other tirzepatide studies.15,39 Moreover, a report that added 0.5 to all samples before inputting them into the calculation also showed inaccuracies.40
Since the proportion of TTO=0 data in the database is not negligible—accounting for approximately 30% in this study—the innovative value reassignment method for TTO=0 data proposed herein showed greater rationality and rigor and enhanced analytical reliability. This has a significant impact on evaluating the fitting parameters of the AE occurrence model, particularly for acute-onset AEs that demand urgent intervention. The enhanced robustness of the Weibull fitting stability (Table S5) further validates this approach, especially the identification of an early failure pattern that guides intensive initial surveillance. Besides, the author conducted TTO analysis from a multi-dimensional perspective, revealing that while immune-, injury-, gastrointestinal-, and neurovascular-related adverse events occur earlier, hepatobiliary disorders and thyroid carcinogenesis may occur later—differences requiring attention in patient monitoring.
Limitations
As indicated in Table 1, the predominance of consumer self-reported cases (93.87%) introduces numerous missing data and inherent reporting bias, including overreporting of mild or non-specific AEs (eg, fatigue, bloating), underreporting of severe but less recognizable events (eg, early-stage cholelithiasis). Consequently, analyses of gender, weight, outcomes, and TTO are necessarily restricted to the subset of cases with available information. Furthermore, the majority of tirzepatide adverse event reports originate from the United States, reflecting relatively limited contributions from other regions. This geographic imbalance implies that FAERS-derived analyses may not fully represent the global patient population. Although search results in WHO Vigilance corroborated findings on patient demographics and SOC distribution of AEs, the regional reporting bias remains an inherent limitation of spontaneous reporting systems.
Secondly, the disproportionality analyses identify statistical associations, which may be confounded by unmeasured factors such as doses, treatment duration, concurrent medications, underlying comorbidities or lifestyle factors. Causality cannot be established due to the observational, spontaneous reporting nature of FAERS. Thus, the identified signals reflect potential safety concerns requiring further prospective cohort studies or randomized controlled trials designed to establish causality. Besides, FAERS does not capture the total number of patients exposed to tirzepatide, nor does it provide data on exposure duration or dosage levels across the population. As a result, this study can only report the frequency and proportional distribution of AEs, not their true incidence. This limitation hinders comparisons of AE risk between tirzepatide and other GLP-1 receptor agonists.
Conclusion
This study does not declare explicit risks, still findings highlight 14 new signals warranting further investigation, including postmenopausal haemorrhage, menstrual disorder, skin sensitization, sleep disorder, Wernicke’s encephalopathy, muscle atrophy, neck mass and lymph node pain. It is crucial to monitor AEs related to the nervous system and metabolism and gastrointestinal tract particularly within the first week after administration, and later within a month for reproductive and endocrine system disorders. Pancreatitis, impaired gastric emptying, small intestinal obstruction, cholelithiasis, dehydration, ketoacidosis and hypoglycaemic unconsciousness could lead to serious outcomes. This work shall provide a useful method for more accurate TTO analyses of pharmacovigilance and improve patient safety in clinical practice of tirzepatide. In addition, the research findings may inform drug development by guiding personalized dosing, updating drug labeling, advancing targeted pharmacovigilance tools, and expanding clinical trial inclusion of vulnerable subgroups (eg, elderly, high-weight patients).
Ethics Statement
The study was carried out in accordance with the Declaration of Helsinki after the approval from the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Ethical code: [2024] LSZ (0682)).
Acknowledgments
The author appreciates the assistance provided by Fengli Li in language polishing.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38–13. doi:10.1001/jama.2023.24945
2. Alfaris N, Waldrop S, Johnson V, Boaventura B, Kendrick K, Stanford FC. GLP-1 single, dual, and triple receptor agonists for treating type 2 diabetes and obesity: a narrative review. EClinicalMedicine. 2024;75102782. doi:10.1016/j.eclinm.2024.102782
3. Wharton S, Calanna S, Davies M, et al. Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg in adults with overweight or obesity, and the relationship between gastrointestinal adverse events and weight loss. Diabetes Obesity Metab. 2022;24(1):94–105. doi:10.1111/dom.14551
4. Borner T, Pataro AM, Doebley SA, et al. Hypophagia and body weight loss by tirzepatide are accompanied by fewer GI adverse events compared to semaglutide in preclinical models. Sci Adv. 2025;11(25):eadu1589. doi:10.1126/sciadv.adu1589
5. Nauck MA, DAlessio DA. Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regrading glycaemic control and body weight reduction. Cardiovascul Diabetol. 2022;21(1):169. doi:10.1186/s12933-022-01604-7
6. Zhou Q, Zhao F, Zhang Y, Yang D, Wang M-W. Structural pharmacology and mechanisms of GLP-1R signaling. Trends Pharmacol Sci. 2025;46(5):422–436. doi:10.1016/j.tips.2025.03.003
7. Martin JA, Czeskis B, Urva S, Cassidy KC. Absorption, distribution, metabolism, and excretion of tirzepatide in humans, rats, and monkeys. Eur J Pharm Sci. 2024;202106895. doi:10.1016/j.ejps.2024.106895
8. Venniyoor A. Tirzepatide once weekly for the treatment of obesity. New Engl J Med. 2022;387(15):1433–1434. doi:10.1056/NEJMc2211120
9. Ciudin A, Johansson E, Zimner-Rapuch S, et al. Indirect comparative efficacy and safety of tirzepatide 10 and 15 mg versus semaglutide 2.4 mg for the management of obesity and overweight in patients with type 2 diabetes. Diabetes Obesity Metab. 2025:1–11. doi:10.1111/dom.16508
10. Packer M, Zile MR, Kramer CM, et al. Tirzepatide for heart failure with preserved ejection fraction and obesity. New Engl J Med. 2025;392(5):427–437. doi:10.1056/NEJMoa2410027
11. Syed YY. Tirzepatide: first approval. Drugs. 2022;82(11):1213–1220. doi:10.1007/s40265-022-01746-8
12. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205–216. doi:10.1056/NEJMoa2206038
13. Song Q, Gao S, Tan Y. Adverse events associated with gepants: a pharmacovigilance analysis based on the FDA adverse event reporting system. J Headache Pain. 2025;26(1):147. doi:10.1186/s10194-025-02091-3
14. Godfrey H, Leibovit-Reiben Z, Jedlowski P, Thiede R. Alopecia associated with the use of semaglutide and tirzepatide: a disproportionality analysis using the FDA adverse event reporting system (FAERS) from 2022 to 2023. J Eur Acad Dermatol Venereol. 2025;39(2):e153–e154. doi:10.1111/jdv.20197
15. He L, Li Q, Yang Y, et al. Pharmacovigilance study of GLP-1 receptor agonists for metabolic and nutritional adverse events. Front Pharmacol. 2024;15(8):1416985. doi:10.3389/fphar.2024.1416985
16. Zeng Q, Xu J, Mu X, Shi Y, Fan H, Li S. Safety issues of tirzepatide (pancreatitis and gallbladder or biliary disease) in type 2 diabetes and obesity: a systematic review and meta-analysis. Front Endocrinol. 2023;14:1214334. doi:10.3389/fendo.2023.1214334
17. Liu F, Zheng JX, Wu XD. Clinical adverse events to dexmedetomidine: a real-world drug safety study based on the FAERS database. Front Pharmacol. 2024;151365706. doi:10.3389/fphar.2024.1365706
18. Yu M, Zhou L, Cao M, Ji C, Zheng Y. Post-marketing drug safety surveillance of enfortumab vedotin: an observational pharmacovigilance study based on a real-world database. Front Immunol. 2024;151397692. doi:10.3389/fimmu.2024.1397692
19. Chen X, Jiang Y, Zhu H, Tian M. Mining and evaluation of adverse event signals for capmatinib based on the FAERS database. Front Pharmacol. 2024;151417661. doi:10.3389/fphar.2024.1417661
20. Wang J, Zhang Z, Liu X, et al. Exploring novel adverse events of nefecon. Kidney Int Rep. 2024;9(9):2705–2717. doi:10.1016/j.ekir.2024.07.006
21. Anand K, Ensor J, Trachtenberg B, Bernicker EH. Osimertinib-induced cardiotoxicity: a retrospective review of the FDA Adverse Events Reporting System (FAERS). JACC CardioOncol. 2019;1(2):172–178. doi:10.1016/j.jaccao.2019.10.006
22. Omar NE, Fahmy Soliman AI, Eshra M, Saeed T, Hamad A, Abou-Ali A. Postmarketing safety of anaplastic lymphoma kinase (ALK) inhibitors: an analysis of the FDA Adverse Event Reporting System (FAERS). ESMO open. 2021;6(6):100315. doi:10.1016/j.esmoop.2021.100315
23. Gao W, Yu J, Sun Y, et al. Adverse events in the nervous system associated with blinatumomab: a real-world study. BMC Med. 2025;23(1):72. doi:10.1186/s12916-025-03913-6
24. Wang X, Chen H, Han S, Li L, Chen H, Yang B. The real-world analysis of adverse events with teduglutide: a pharmacovigilance study based on the FAERS database. Front Pharmacol. 2024;151404658. doi:10.3389/fphar.2024.1404658
25. Zou C, Wang X, Huang R, Hu H. Real-world safety profile of etelcalcetide in dialysis-related secondary hyperparathyroidism: a pharmacovigilance analysis of FAERS data. Renal Failure. 2025;47(1):2523575. doi:10.1080/0886022x.2025.2523575
26. Shu Y, Ding Y, Liu L, Zhang Q. Cardiac adverse events associated with quetiapine: disproportionality analysis of FDA adverse event reporting system. CNS Neurosci Ther. 2023;29(9):2705–2716. doi:10.1111/cns.14215
27. Zhang W, Chen Y, Yao Z, Ouyang M, Sun M, Zou S. Post-marketing pharmacovigilance of canakinumab from the FDA Adverse Event Reporting System (FAERS). Pharmaceuticals. 2025;18(1):114. doi:10.3390/ph18010114
28. Nie W, Wu X, Xia Y, Zheng L, Lu H. Reported psychiatric adverse events among isotretinoin users: monitoring priorities from a 20-year FDA Adverse Event Reporting System database study. J Am Acad Dermatol. 2025;93(1):64–72. doi:10.1016/j.jaad.2025.02.072
29. Forzano I, Varzideh F, Avvisato R, Jankauskas SS, Mone P, Santulli G. Tirzepatide: a systematic update. Int J Mol Sci. 2022;23(23):14631. doi:10.3390/ijms232314631
30. Wang M, Yang Z, Yan M, Liu S, Xiao S. Depression and suicide/self-injury signals for weight loss medications: a disproportionality analysis of semaglutide, liraglutide, and tirzepatide in FAERS database. J Affective Disorders. 2025;389119670. doi:10.1016/j.jad.2025.119670
31. Stefanakis K, Kokkorakis M, Mantzoros CS. The impact of weight loss on fat-free mass, muscle, bone and hematopoiesis health: implications for emerging pharmacotherapies aiming at fat reduction and lean mass preservation. Metabolism. 2024;161:156057. doi:10.1016/j.metabol.2024.156057
32. Sande CM, Tondi I, Livolsi VA. The thyroid pathologist meets therapeutic pharmacology. Endocrine Pathol. 2023;34(1):48–56. doi:10.1007/s12022-023-09749-1
33. Bezin J, Gouverneur A, Pénichon M, et al. GLP-1 receptor agonists and the risk of thyroid cancer. Diabetes Care. 2023;46(2):384–390. doi:10.2337/dc22-1148
34. Guirguis A, Chiappini S, Papanti PG, et al. Exploring the association between suicidal thoughts, self-injury, and GLP-1 receptor agonists in weight loss treatments: insights from pharmacovigilance measures and unmasking analysis. Eur Neuropsychopharmacol. 2024;82:82–91. doi:10.1016/j.euroneuro.2024.02.003
35. Inceu GV, Craciun A-E, Ciobanu DM, et al. Real-world sex differences in response to treatment with glucagon-like peptide-1 receptor agonists: analysis of single-center outpatient case series. Medicina. 2025;61(8):1343. doi:10.3390/medicina61081343
36. Zhang Z, Li J, Zheng J, Liang Y, Ma L, Su L. Tirzepatide safety in type 2 diabetes: a disproportionality analysis of adverse events using the FDA FAERS database. Endocr Connections. 2025;14(7):e250205. doi:10.1530/EC-25-0205
37. Liu J, Xue L, Fang X, et al. Drug-associated hyperprolactinemia: a comprehensive disproportionality analysis based on the FAERS database. Eur J Pharmacol. 2025;996:177551. doi:10.1016/j.ejphar.2025.177551
38. Ou Y, Cui Z, Lou S, et al. Analysis of tirzepatide in the US FDA adverse event reporting system (FAERS): a focus on overall patient population and sex-specific subgroups. Front Pharmacol. 2024;151463657. doi:10.3389/fphar.2024.1463657
39. Huo Y, Ma M, Liao X. Data mining study on adverse events of tirzepatide based on FAERS database. Expert Opin Drug Saf. 2025;24(6):675–683. doi:10.1080/14740338.2024.2376686
40. Cai X, Chen G, Wang H, Wang L, Hu C. Pharmacovigilance insights into drug-associated venous thromboembolism. Int J Surg. 2025;1–31. doi:10.1097/js9.0000000000002931
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unveiling the Hidden Risks: An Update Decade-Long Analysis of Abraxane-Related Adverse Events from the FAERS Database
Zhao YC, Li X, Wang CQ, Jiao Y, Shen YN, Wang TJ, Zhang CH
International Journal of Nanomedicine 2024, 19:11847-11858
Published Date: 14 November 2024
Risk Factors for Drug-Induced Acute Generalized Exanthematous Pustulosis(AGEP) from 2004 to 2024: A Real-World Study Based on the FAERS
Que H, Zheng X, Li X, Wang W
Clinical, Cosmetic and Investigational Dermatology 2025, 18:2835-2845
Published Date: 28 October 2025
Risk Signals of Antibody-Drug Conjugates in Bladder Cancer: A Real-World FAERS Study
Liu J, Li G, Yang J, Sun B, Guo S
Clinical Epidemiology 2025, 17:995-1009
Published Date: 28 November 2025