Back to Journals » Journal of Inflammation Research » Volume 19
Advanced Lung Cancer Inflammation Index (ALI) as an Independent Predictor for Bronchiectasis Exacerbation Risks
Authors Kwok WC, Tam TCC, Chan SKS, Choi EPH, Ho JCM
Received 18 November 2025
Accepted for publication 6 March 2026
Published 18 March 2026 Volume 2026:19 581623
DOI https://doi.org/10.2147/JIR.S581623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Wang Chun Kwok,1 Terence Chi Chun Tam,1 Shung Kay Samuel Chan,1 Edmond Pui Hang Choi,2 James Chung Man Ho1
1Division of Respiratory Medicine, Department of Medicine, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong; Queen Mary Hospital, Hong Kong Special Administrative Region, People’s Republic of China; 2School of Nursing, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: James Chung Man Ho, Department of Medicine, Queen Mary Hospital, 102 Pokfulam Road, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China, Tel +852 2255 4449, Email [email protected]
Purpose: Advanced lung cancer inflammation index (ALI), which is composed of the body mass index (BMI), serum albumin level, and blood neutrophil and lymphocyte levels, has been studied in various conditions, including cancers and non-malignant conditions, but not in bronchiectasis.
Patients and methods: A prospective cohort study of Chinese patients with non-cystic fibrosis (CF) bronchiectasis was conducted in Hong Kong to investigate the association between baseline ALI and the risk of bronchiectasis exacerbation. ALI was assessed as a continuous variable, in quartiles, and cutoff values were determined using receiver operator curve (ROC) analysis.
Results: A total of 148 Chinese patients were recruited, 60 of whom developed bronchiectasis exacerbation during the follow-up period. Lower baseline ALI was associated with an increased risk of bronchiectasis exacerbation in the follow-up period, with an adjusted odds ratio (aOR) of 1.06 (95% CI = 1.03– 1.09, p < 0.001) for every 10-unit decrease. The first to third quartiles of ALI were also associated with a significantly increased risk of bronchiectasis exacerbation, with aOR of 15.525 (95% CI = 3.927– 61.379) for Q1 (p < 0.001), 6.523 (95% CI = 1.730– 24.599) for Q2 (p = 0.006), and 7.272 (95% CI = 1.902– 27.800) for Q3 (p = 0.004). Patients with ALI less than 45.6 had a significantly increased risk of bronchiectasis exacerbation during the follow-up period, with an aOR of 3.829 (95% CI = 1.737– 8.442) (p< 0.001).
Conclusion: ALI can independently predicting the risk of future exacerbation in patients with non-CF bronchiectasis. Lower ALI was associated with an increased risk of bronchiectasis exacerbation, with a proposed cutoff value of 45.6.
Keywords: advanced lung cancer inflammation index, biomarkers, bronchiectasis, bronchiectasis exacerbation
Introduction
Bronchiectasis is marked by persistent neutrophilic inflammation of the airways.1–4 Among its clinical manifestations, exacerbations are both frequent and significant. Data from the European Multicenter Bronchiectasis Audit and Research Collaboration (EMBARC) Bronchiectasis Registry indicate that approximately half of bronchiectasis patients experience two or more exacerbations each year.5 These exacerbations adversely affect morbidity, quality of life, and mortality, in addition to raising healthcare costs.6–14 To assess disease severity, two well-established scoring systems are commonly used: the Bronchiectasis Severity Index (BSI)6,15 and the FACED score, which predicts five-year all-cause mortality. FACED score was built based on factors including forced expiratory volume in one second (FEV1), age, Pseudomonas aeruginosa colonization, disease extent and level of dyspnea; while body mass index (BMI) and exacerbation history were also included in BSI.15–18 However, these scoring tools primarily focus on clinical parameters and do not account for the inflammatory status of patients. Several inflammatory markers—such as high-sensitivity C-reactive protein, neutrophil-to-lymphocyte ratio (NLR), and systemic immune-inflammation index (SII)—have been investigated as possible prognostic biomarkers in bronchiectasis.19–21 Nevertheless, these markers do not incorporate patients’ clinical characteristics.
The advanced lung cancer inflammation index (ALI)—which incorporates BMI, albumin, and neutrophil-to-lymphocyte ratio (NLR)—is a systemic inflammation marker that was originally developed for patients with lung cancer.22,23 Its application has since broadened to include other types of cancer, such as esophageal, colorectal, pancreatic, and gastric cancers.24–27 More recently, ALI has also been proposed as a potential prognostic marker for non-malignant conditions, including hypertension, heart failure, coronary artery disease, diabetes mellitus, stroke, and chronic kidney disease (CKD).28–31 Recently, our group also reported that ALI could predict the risk of exacerbation of chronic obstructive pulmonary disease (COPD).32 There is similarities between COPD and bronchiectasis in the pathological mechanism while there are also major differences in these two diseases,33 for example the sex of the patients involves (predominantly male in COPD and more female in bronchiectasis), etiology (smoking as the predominant cause of COPD while post-infective causes predominates in bronchiectasis), radiological features, clinical course and treatment modalities. Hence, it will be interesting to assess if ALI has the same prognostic role in bronchiectasis as in COPD, while the findings in COPD cannot be directly extrapolated to bronchiectasis patients.
Unlike other inflammatory indices, ALI uniquely includes BMI, a simple and repeatable measurement, along with readily accessible blood-based biomarkers. This combination may provide a more holistic evaluation of systemic inflammation and body composition, both of which can be affected by severe illness. Notably, BMI is also a component of BSI, highlighting its prognostic significance in bronchiectasis. Additionally, serum albumin, another ALI component, reflects patients’ nutritional status, which can be compromised in the presence of major diseases. Integrating serum albumin, BMI, and NLR into a single scoring system like ALI could therefore enhance prognostic accuracy.
Given that bronchiectasis is characterized by chronic inflammation, additional studies are needed to further elucidate the prognostic significance of ALI in this disease.
Methods
This was a prospective, single-center cohort study conducted in Hong Kong. A total of 150 Chinese patients with non-cystic fibrosis (non-CF) bronchiectasis who were being followed at the designated bronchiectasis or respiratory clinic of the Department of Medicine, Queen Mary Hospital (QMH), were prospectively enrolled between February 9, 2023, and July 13, 2023. Participants were monitored for the occurrence of bronchiectasis exacerbations until February 28, 2025. Patients were excluded if they had coexisting airway disease (asthma/COPD), traction bronchiectasis secondary to interstitial lung disease (ILD), bronchiectasis due to allergic bronchopulmonary aspergillosis (ABPA), or those who lost to follow up. To confirm diagnoses, the investigators reviewed medical records and relevant radiological findings, ensuring that each case met the international consensus criteria for both the radiological and clinical diagnosis of bronchiectasis in adults.34 Patients’ data were accessed via the Electronic Patient Record (ePR) system of the Hong Kong Hospital Authority, which includes information from both outpatient and inpatient visits. Available data encompassed demographics, clinical documentation, investigation results, and treatment details.
Demographic information, clinical data, and investigation results were extracted from ePR. The primary outcome of the study was bronchiectasis exacerbation. Exacerbation of bronchiectasis was defined according to the consensus criteria for pulmonary exacerbations in adults with bronchiectasis.35 The criteria for bronchiectasis exacerbation included: [1] a worsening of ≥3 key symptoms for ≥48 hours, such as cough, sputum volume and/or consistency, sputum purulence, dyspnea and/or reduced exercise tolerance, fatigue and/or malaise, and hemoptysis; AND [2] a clinician’s judgment that a change in the patient’s bronchiectasis treatment was necessary.35 The secondary outcome was hospitalized bronchiectasis exacerbation, defined as an exacerbation meeting the aforementioned criteria that required inpatient care for at least 24 hours. Regular use of pharmacotherapy for bronchiectasis was defined as the continuous use of these medications for a minimum of 12 months during the study period. Baseline FACED scores were calculated for each patient, incorporating the following components: F—forced expiratory volume in 1 second (FEV1) in percentage predicted; A—age with cut-off at 70; C—chronic colonization by Pseudomonas aeruginosa; E—extent of bronchiectasis; and D—dyspnea (Assessed by Modified Medical Research Council (mMRC) Dyspnea Scale).17
ALI was calculated as follows: body mass index (kg/m2) × serum albumin level (g/dL)/neutrophil-to-lymphocyte ratio (NLR). Patients were categorized into four groups according to the quartiles of their ALI values.
The parameters required for calculating the ALI were obtained during the recruitment visit, when the patient had been clinically stable for at least 30 days following their most recent exacerbation that necessitated antibiotic treatment. The study was approved by the Institutional Review Board (reference number UW 22–656).
Sample Size Calculation
There was no published study on the association between ALI and bronchiectasis exacerbation risks. However, there was a study on the association between ALI and postoperative complications in patients undergoing lung resection for bronchiectasis.36 In this study, patients in the low ALI group had a higher proportion of requiring open thoracotomy (11.3% vs 38.8%) when compared to the high ALI group, which is a surrogate marker of negative outcome. Sample size calculation using the reported findings in this study suggested a sample size of 124 would have 95% power and an alpha of 0.05.
Statistical Analysis
Demographic and clinical variables were presented as actual frequencies or as means ± standard deviations. Baseline demographic and clinical characteristics were compared between patients with and without exacerbations during the follow-up period using two-sample t-test. Univariate and multi-variable logistic regression analysis were performed to assess the relationship between ALI and the risk of bronchiectasis exacerbation during follow-up. Age, baseline FACED score, sex, smoking status, use of bronchiectasis pharmacotherapy and the number of exacerbations in the preceding 1 year were included as covariates in the multi-variable analyses. Multi-collinearity among these variables was evaluated, with results provided in Supplementary Table 1; no evidence of multi-collinearity was found. Analyses of ALI were performed in three ways: as a continuous variable, by quartile grouping, and using the optimal cut-off determined by receiver operating characteristic (ROC) analysis. A p-value of < 0.05 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 28.0.
Results
A total of 150 Chinese patients with non-CF bronchiectasis were recruited. Two subjects were excluded because they were unable to perform body measurements for BMI assessment owing to their poor mobility. Sixty patients developed exacerbations of bronchiectasis during the follow-up period, with 22 requiring hospitalization. The mean follow-up interval was 21.9 ± 2.6 months. The patient selection flow diagram is shown in Figure 1.
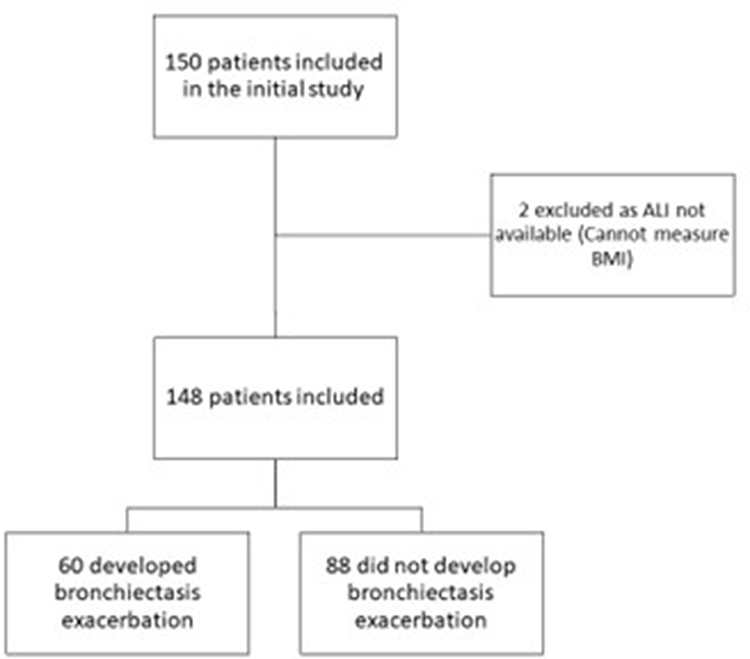 |
Figure 1 Patient selection flow diagram. |
Baseline Characteristics
The mean age of the include patients was 70.6 ± 10.0 years, with more females (71.6%) and never-smokers (88.5%). A total of 41 (27.7%) patients had Pseudomonas aeruginosa colonization. The mean baseline FEV1 was 1.75 ± 0.52 L (93.1 ± 20.6%). A total of 83 patients (56.1%) had more than 2 lobes involved by bronchiectasis. The mean ALI was 48.9 ± 22.1. The quartiles of ALI were Q1 (lowest): <343; Q2: 343–450; Q3: 450.1–577; Q4: > 577. The results are summarized in Table 1.
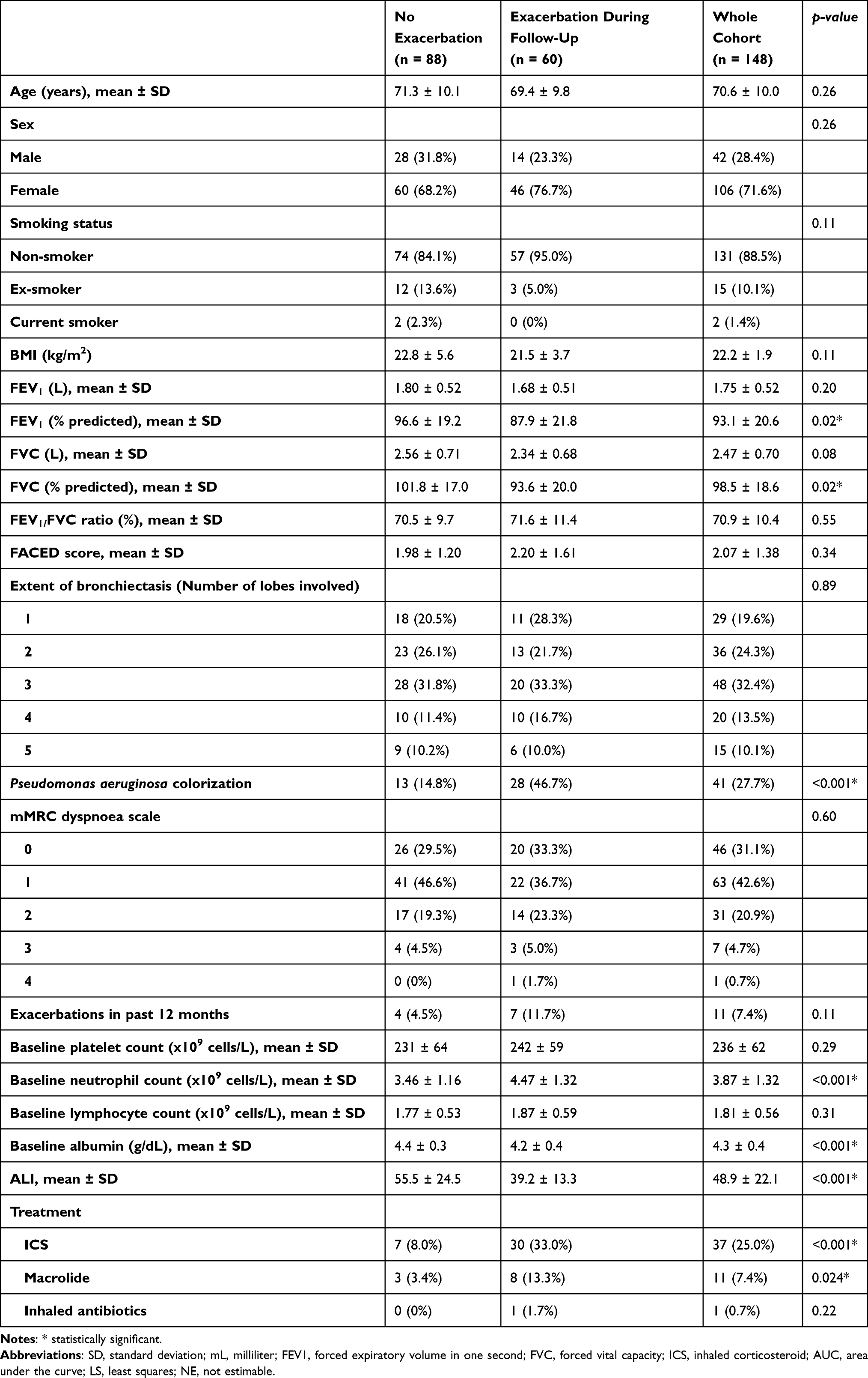 |
Table 1 Baseline Demographic and Clinical Characteristics |
Optimal ALI Cut-off Value to Predict the Risk of Total Bronchiectasis Exacerbation and Hospitalized Bronchiectasis Exacerbation
ROC analysis was performed to determine the optimal cut-off value for ALI in predicting total bronchiectasis exacerbation. At a cutoff of 45.6, the area under the curve (AUC) was 0.713 (95% confidence interval [CI] = 0.631–0.795; p < 0.001). The corresponding sensitivity and specificity were 60.2% and 71.7%, respectively, with a Youden index of 0.319 (Figure 2).
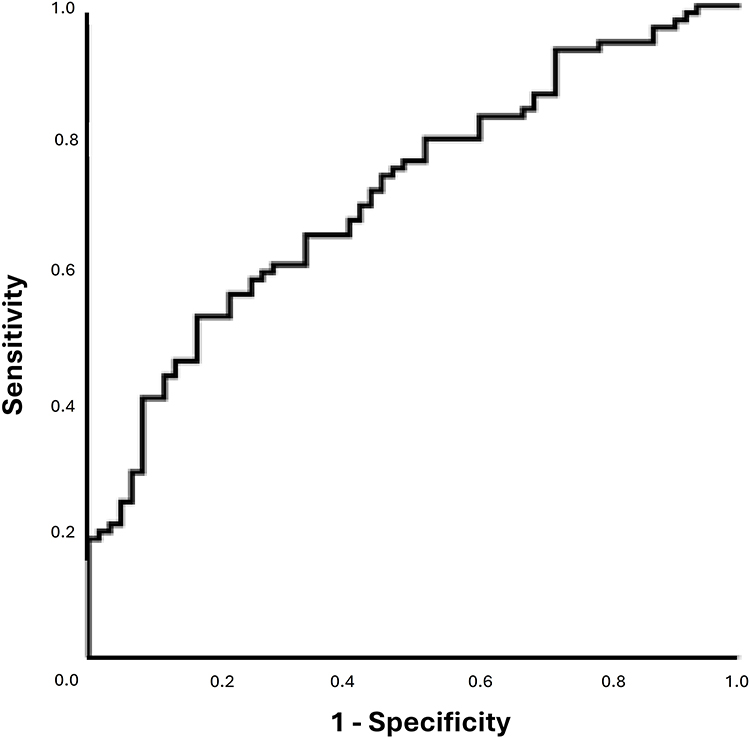 |
Figure 2 Receiver Operating Curve (ROC) for ALI and risk of total bronchiectasis exacerbation. |
ROC analysis was performed to determine the optimal cutoff value for ALI in predicting hospitalized bronchiectasis exacerbations. At the cut-off at 39.5, the AUC was 0.718 (95% CI = 0.610–0.826; p = 0.001). The corresponding sensitivity and specificity were 69.0% and 68.2%, respectively, with a Youden index of 0.372 (Figure 3).
 |
Figure 3 Receiver Operating Curve (ROC) for ALI and risk of hospitalized bronchiectasis exacerbation. |
Risk of Total Bronchiectasis Exacerbation and Baseline ALI
The lower baseline ALI, as a continuous variable, every ten-unit decrease was associated with an increased risk of total bronchiectasis exacerbation in the follow-up period, with an odds ratio (OR) of 1.05 (95% CI = 1.03–1.08, p <0.001) and an adjusted OR (aOR) of 1.06 (95% CI = 1.03–1.09, p <0.001).
Q1 to Q3 of ALI, when compared with Q4 (highest quartile), were associated with a significantly increased risk of total bronchiectasis exacerbation during the follow-up period, with OR of 9.389 (95% CI = 2.977–29.600; p< 0.001) for Q1, 6.063 (95% CI = 1.935–18.994; p = 0.002) for Q2, and 4.364 (95% CI = 1.384–13.761; p = 0.012) for Q3 (Table 2).
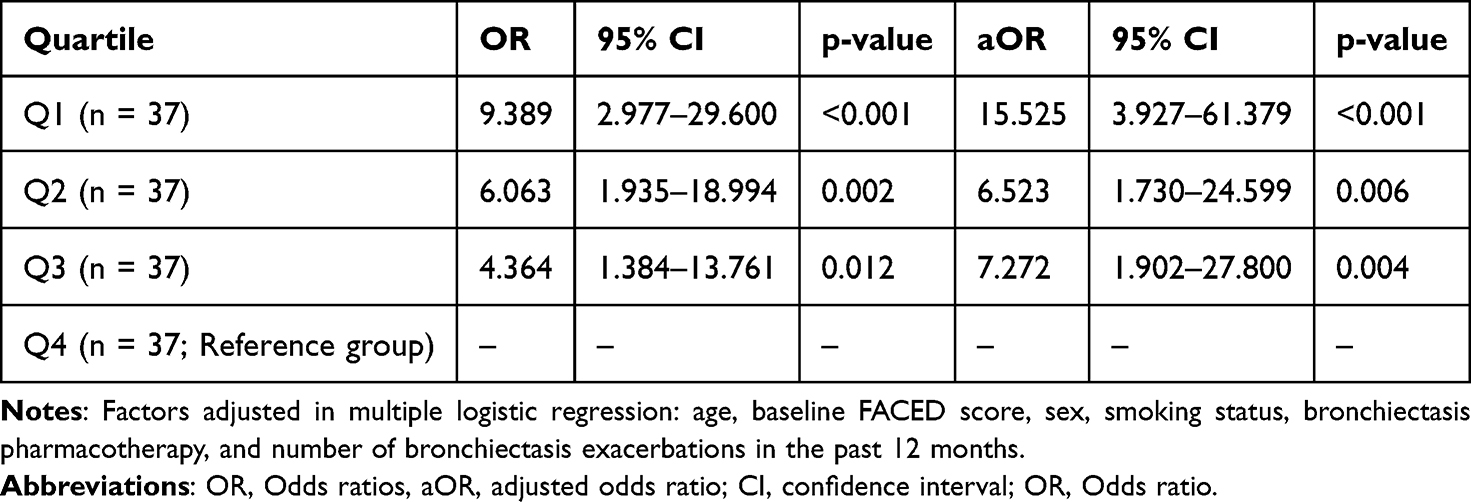 |
Table 2 Baseline ALI Level in Quartile and Risk of Total Bronchiectasis Exacerbation |
The aORs were 15.525 (95% CI = 3.927–61.379; p < 0.001) for Q1, 6.523 (95% CI = 1.730–24.599; p = 0.006) for Q2 and 7.272 (95% CI = 1.902–27.800; p = 0.004) for Q3.
Patients with ALI less than 45.6 (cut-off value determined by ROC analysis) had a significantly increased risk of total bronchiectasis exacerbation during the follow-up period, with an OR of 3.830 (95% CI = 1.892–7.755; p< 0.001) and aOR of 3.829 (95% CI = 1.737–8.442; p< 0.001).
Risk of Hospitalized Bronchiectasis Exacerbation and Baseline ALI
A lower baseline ALI as a continuous variable was associated with an increased risk of hospitalization bronchiectasis exacerbation during the follow-up period, with an OR of 1.005 (95% CI = 1.002–1.009; p = 0.003) and an aOR of 1.005 (95% CI = 1.001–1.009; p = 0.018) for every unit increase.
Q1 (lowest quartile) of ALI, compared with Q4 (highest quartile), was associated with a significantly increased risk of bronchiectasis exacerbation during the follow-up period, with OR of 11.571 (95% CI = 1.383–96.808; p = 0.024) for Q1, 9.931 (95% CI = 1.175–84.038; p = 0.035) for Q2, and 4.364 (95% CI = 0.464–41.056; p = 0.198) for Q3.
The aORs were 12.033 (95% CI = 1.279–113.217; p = 0.030) for Q1; 6.927 (95% CI = 0.748–64.1841; p = 0.088) for Q2 and 45.257 (95% CI = 0.521–53.025; p = 0.159) for Q3 (Table 3).
 |
Table 3 Baseline ALI Level in Quartile and Risk of Hospitalized Bronchiectasis Exacerbation |
Patients with ALI less than 39.2 (the cut-off value determined by ROC analysis) had a significantly increased risk of hospitalization bronchiectasis exacerbation during the follow-up period, with an OR of 4.053 (95% CI = 1.570–10.461; p = 0.004) and an aOR of 4.517 (95% CI = 1.434–14.227; p = 0.010).
Discussion
To the best of our knowledge, this is the first report on the role of ALI in predicting the risk of exacerbation of bronchiectasis. The findings were observed when ALI was assessed as a continuous variable, in quartiles and as a cut-off value determined by ROC. ALI was associated with both total and hospitalized exacerbations. Our results indicate that this easily accessible marker may have a role in predicting outcomes in bronchiectasis.
Although different scoring systems and biomarkers have been proposed for bronchiectasis, they have their own limitations. The BSI and FACED scores are well validated and most often used. However, these studies have mainly focused on established outcomes, such as the extent of bronchiectasis and bacterial colonization. However, the inflammatory state of bronchiectasis was not assessed using these scoring systems. BSI and FACED mainly based on the established outcomes in bronchiectasis like extent, lung function and colonization of bacteria, which are rather stable over time. BMI is included in BSI but not FACED. ALI has the advantage of incorporating inflammatory markers and BMI, which can reflect the dynamic process in bronchiectasis. It may also serve as the tool to monitor bronchiectasis, by observing the changes in BMI and inflammatory markers with time. While NLR, SII, and hs-CRP have been shown to predict bronchiectasis exacerbations, these biomarkers did not consider the nutritional status of patients with bronchiectasis. These markers only measure the inflammatory component but not BMI which is an important parameter, reflecting the nutritional status of these patients. ALI can serve as a simple, easily repeatable, and comprehensive biomarker of bronchiectasis. The calculation of ALI uses NLR in the denominator to represent inflammatory status, especially neutrophilic inflammation, which is a hallmark of bronchiectasis. BMI and albumin, forming the numerator, are essential nutritional indicators that often decline as chronic respiratory diseases progress.37 By incorporating systemic inflammation and nutritional parameters within a single scoring system, clinicians can easily prognosticate and monitor these patients. ALI can potentially serve as a simple and meaningful marker to reflect nutritional and inflammatory markers in bronchiectasis. Our study also suggested that ALI can predict bronchiectasis exacerbation as a continuous variable, in quartiles, and at a cut-off value, as determined by ROC analysis. In short, a lower ALI, which can result from worse nutritional status, a higher degree of neutrophilic inflammation, or both, is associated with an increased risk of bronchiectasis exacerbation.
However, ALI did have its own disadvantages. While ALI included important and easily available nutritional and inflammatory markers, it did not include other well reported prognostic factors in bronchiectasis, such as lung function, symptoms and bacterial colonization. Also, whether replacing NLR with SII, or adding hs-CRP to it may enhance its prognostic role is also worth assessing. In the future, it is worthwhile to assess the incorporation of ALI into FACED/BSI to enhance the performance of these well reporting scoring systems.
Exacerbation of bronchiectasis is one of the most common sequelae. Assessing patients’ risk of bronchiectasis exacerbation is crucial when considering new drug treatments.38–40 The use of scoring systems and biomarkers will facilitate clinicians to stratify the exacerbation of the disease and offer timely management. These findings suggest that ALI has potential as an independent prognostic factor in forecasting exacerbations in bronchiectasis. The observed values in this study can be explained by the fact that ALI incorporates factors representing both the pathophysiology and general health of bronchiectasis patients. This also underscores the need for clinicians to focus on both disease severity and the nutritional decline—evident through low BMI and albumin—that accompanies chronic inflammation in bronchiectasis. Whether nutritional support and therapy can help bronchiectasis patients is also worth studying, but the importance of maintaining good overall health status should not be overemphasized. The simplicity of ALI makes it a practical tool for routine evaluation and serial monitoring of disease progression in bronchiectasis patients.
Knowing the role of various biomarkers, such as ALI, in relation to the prognosis of bronchiectasis, such as exacerbation risk, they can be incorporated into a new scoring system. The addition of biomarkers, including ALI, to the new scoring system could provide insight into patients’ nutritional and inflammatory states and aid in predicting outcomes such as the risk of exacerbations. This could help clinicians to better understand the severity and risks of bronchiectasis by incorporating disease extent, nutritional status, and inflammatory markers into this novel scoring system, which can more precisely affect bronchiectasis in multiple dimensions. Apart from exacerbation risks, symptoms, quality of life, lung function, and survival should be assessed using this scoring system.
Our study had some limitations. First, it involved the QMH as the only center. QMH, a tertiary medical center in Hong Kong affiliated with The University of Hong Kong, houses a respiratory unit that receives referrals from healthcare facilities across the region. It also features a dedicated bronchiectasis clinic for comprehensive management of patients with bronchiectasis. Second, lung function tests were performed at different time points in the different patients. Only one ALI measurement was obtained from the included patients during the recruitment visit. As BMI and blood parameters can change over time, serial ALI measurements and assessment of their role in bronchiectasis should be considered in a separate study. A follow up study on serial ALI measurement and the long-term outcome such as development of other system complications, evolution of bronchiectasis over time and mortality shall be considered. Only Chinese patients were included in this study, which affects their generalizability While baseline FACED score was adjusted, which included Pseudomonas aeruginosa colonization as one of the component, the colonization from other micro-organisms were not measured by FACED score with potential residual confounding. Using BSI instead of FACED score may overcome this issue as it includes the colonization from other micro-organisms as the component. But it also introduced the potential issue of multi-collinearity as BMI is also included in BSI. Finally, the study included only a small number of participants. Having a small sample size and low event number resulted in a wide CI in the results reported, despite statistical significance being reached. A large-scale study, especially multi-national multi-centre study involving patients of different ethnicities and clinical characteristics, is important to test the observations noted in this study. Ideally, the results should be validated using an external data source to confirm the findings of this study.
Conclusion
ALI has the potential to serve as a biomarker for predicting exacerbation risk in bronchiectasis patients. Reduced ALI was associated with an elevated risk of exacerbation in bronchiectasis patients. The proposed cut-off value was 45.6 for bronchiectasis exacerbation and 39.2 for hospitalized bronchiectasis exacerbation. The prognostic significance of ALI in bronchiectasis should be confirmed through external validation in a separate cohort.
Data Sharing Statement
All available data are presented in the manuscript and no additional data are provided. Due to the ethical restrictions imposed by the Institutional Review Board (IRB) regulations and rules on patient data privacy in this study, supporting research data were not available upon request.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of the University of Hong Kong and the Hospital Authority of Hong Kong West Cluster (UW 22-656). Informed consent was obtained from all the participants. This study was conducted in accordance with the principles of the Declaration of Helsinki. The study was reported in accordance with the RECORD reporting guidelines.
Acknowledgments
We thank Hospital Authority for providing clinical data essential to this study.
Author Contributions
Conceptualization: W.C.K.; Methodology: W.C.K.; Validation: S.S.K.C., T.C.C.T.; Formal analysis: W.C.K.; Investigation: W.C.K., E.P.H.C.; Data Curation: W.C.K.; Writing - Original Draft: W.C.K., E.P.H.C., S.S.K.C., T.C.C.T., J.C.M.H.; Writing - Review & Editing: W.C.K., E.P.H.C., S.S.K.C., T.C.C.T., J.C.M.H.; Visualization: W.C.K., E.P.H.C., J.C.M.H.; Supervision: J.C.M.H.; Project administration: W.C.K., J.C.M.H.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chan SC, Leung VO, Ip MS, Shum DK. Shed syndecan-1 restricts neutrophil elastase from alpha1-antitrypsin in neutrophilic airway inflammation. Am J Respir Cell Mol Biol. 2009;41(5):620–11. doi:10.1165/rcmb.2008-0185OC
2. Bedi P, Davidson DJ, McHugh BJ, Rossi AG, Hill AT. Blood neutrophils are reprogrammed in bronchiectasis. Am J Respir Crit Care Med. 2018;198(7):880–890. doi:10.1164/rccm.201712-2423OC
3. Finch S, Shoemark A, Dicker AJ, et al. Pregnancy zone protein is associated with airway infection, neutrophil extracellular trap formation, and disease severity in bronchiectasis. Am J Respir Crit Care Med. 2019;200(8):992–1001. doi:10.1164/rccm.201812-2351OC
4. Keir HR, Shoemark A, Dicker AJ, et al. Neutrophil extracellular traps, disease severity, and antibiotic response in bronchiectasis: an international, observational, multicohort study. Lancet Respir Med. 2021;9(8):873–884. doi:10.1016/S2213-2600(20)30504-X
5. Chalmers JD, Aliberti S, Polverino E, et al. The EMBARC European Bronchiectasis Registry: protocol for an international observational study. ERJ Open Res. 2016;2(1). doi:10.1183/23120541.00081-2015
6. Chalmers JD, Goeminne P, Aliberti S, et al. The bronchiectasis severity index. An international derivation and validation study. Am J Respir Crit Care Med. 2014;189(5):576–585. doi:10.1164/rccm.201309-1575OC
7. Chalmers JD, Smith MP, McHugh BJ, Doherty C, Govan JR, Hill AT. Short- and long-term antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med. 2012;186(7):657–665. doi:10.1164/rccm.201203-0487OC
8. Kapur N, Masters IB, Chang AB. Longitudinal growth and lung function in pediatric non-cystic fibrosis bronchiectasis: what influences lung function stability? Chest. 2010;138(1):158–164. doi:10.1378/chest.09-2932
9. Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3). doi:10.1183/13993003.00629-2017
10. Sheehan RE, Wells AU, Copley SJ, et al. A comparison of serial computed tomography and functional change in bronchiectasis. Eur Respir J. 2002;20(3):581–587. doi:10.1183/09031936.02.00284602
11. Seitz AE, Olivier KN, Steiner CA, Montes de Oca R, Holland SM, Prevots DR. Trends and burden of bronchiectasis-associated hospitalizations in the United States, 1993-2006. Chest. 2010;138(4):944–949. doi:10.1378/chest.10-0099
12. Ringshausen FC, de Roux A, Pletz MW, Hamalainen N, Welte T, Rademacher J. Bronchiectasis-associated hospitalizations in Germany, 2005-2011: a population-based study of disease burden and trends. PLoS One. 2013;8(8):e71109. doi:10.1371/journal.pone.0071109
13. McDonnell MJ, Aliberti S, Goeminne PC, et al. Comorbidities and the risk of mortality in patients with bronchiectasis: an international multicentre cohort study. Lancet Respir Med. 2016;4(12):969–979. doi:10.1016/S2213-2600(16)30320-4
14. Beijers RJ, van den Borst B, Newman AB, et al. A multidimensional risk score to predict all-cause hospitalization in community-dwelling older individuals with obstructive lung disease. J Am Med Dir Assoc. 2016;17(6):508–513. doi:10.1016/j.jamda.2016.01.007
15. Martinez-Garcia MA, de Gracia J, Vendrell Relat M, et al. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Eur Respir J. 2014;43(5):1357–1367. doi:10.1183/09031936.00026313
16. Rosales-Mayor E, Polverino E, Raguer L, et al. Comparison of two prognostic scores (BSI and FACED) in a Spanish cohort of adult patients with bronchiectasis and improvement of the FACED predictive capacity for exacerbations. PLoS One. 2017;12(4):e0175171. doi:10.1371/journal.pone.0175171
17. Martinez-Garcia MA, Athanazio RA, Giron R, et al. Predicting high risk of exacerbations in bronchiectasis: the E-FACED score. Int J Chron Obstruct Pulmon Dis. 2017;12:275–284. doi:10.2147/COPD.S121943
18. Menendez R, Mendez R, Polverino E, et al. Factors associated with hospitalization in bronchiectasis exacerbations: a one-year follow-up study. Respir Res. 2017;18(1):176. doi:10.1186/s12931-017-0659-x
19. Kwok WC, Ho JCM, Lam DCL, et al. Baseline neutrophil-to-lymphocyte ratio as a predictor of response to hospitalized bronchiectasis exacerbation risks. Eur Clin Respir J. 2024;11(1):2372901. doi:10.1080/20018525.2024.2372901
20. Kwok WC, Teo KC, Lau KK, Ho JC. High-sensitivity C-reactive protein level in stable-state bronchiectasis predicts exacerbation risk. BMC Pulm Med. 2024;24(1):80. doi:10.1186/s12890-024-02888-z
21. Kwok WC, Tam TCC, Lam DCL, MSM I, JCM H. Systemic immune-inflammation index in predicting hospitalized bronchiectasis exacerbation risks and disease severity. J Thorac Dis. 2024;16(5):2767–2775. doi:10.21037/jtd-23-1392
22. Mountzios G, Samantas E, Senghas K, et al. Association of the advanced lung cancer inflammation index (ALI) with immune checkpoint inhibitor efficacy in patients with advanced non-small-cell lung cancer. ESMO Open. 2021;6(5):100254. doi:10.1016/j.esmoop.2021.100254
23. Jafri SH, Shi R, Mills G. Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): a retrospective review. BMC Cancer. 2013;13:158. doi:10.1186/1471-2407-13-158
24. Huo C, Liu Y, Xie F, Zhao L, Huang H, Feng Q. Advanced lung cancer inflammation index predicts the outcomes of patients with non-metastatic gastric cancer after radical surgical resection. J Gastrointest Oncol. 2023;14(3):1653–1654. doi:10.21037/jgo-23-315
25. Topkan E, Mertsoylu H, Ozdemir Y, et al. Prognostic usefulness of advanced lung cancer inflammation index in locally-advanced pancreatic carcinoma patients treated with radical chemoradiotherapy. Cancer Manag Res. 2019;11:8807–8815. doi:10.2147/CMAR.S222297
26. Feng JF, Huang Y, Chen QX. A new inflammation index is useful for patients with esophageal squamous cell carcinoma. Onco Targets Ther. 2014;7:1811–1815. doi:10.2147/OTT.S68084
27. Shibutani M, Maeda K, Nagahara H, et al. The prognostic significance of the advanced lung cancer inflammation index in patients with unresectable metastatic colorectal cancer: a retrospective study. BMC Cancer. 2019;19(1):241. doi:10.1186/s12885-019-5468-9
28. Li X, Wang Q, Wu F, Ye Z, Li Y. Association between advanced lung cancer inflammation index and chronic kidney disease: a cross-sectional study. Front Nutr. 2024;11:1430471. doi:10.3389/fnut.2024.1430471
29. Fan W, Zhang Y, Liu Y, et al. Nomograms based on the advanced lung cancer inflammation index for the prediction of coronary artery disease and calcification. Clin Appl Thromb Hemost. 2021;27:10760296211060455. doi:10.1177/10760296211060455
30. Yuan X, Huang B, Wang R, Tie H, Luo S. The prognostic value of advanced lung cancer inflammation index (ALI) in elderly patients with heart failure. Front Cardiovasc Med. 2022;9:934551. doi:10.3389/fcvm.2022.934551
31. Tu J, Wu B, Xiu J, et al. Advanced lung cancer inflammation index is associated with long-term cardiovascular death in hypertensive patients: national health and nutrition examination study, 1999-2018. Front Physiol. 2023;14:1074672. doi:10.3389/fphys.2023.1074672
32. Kwok WC, Leung SHI, Tam TCC, Chau CH, Lam FM and Ho JCM. The Role of Advanced Lung Cancer Inflammation Index in Predicting COPD Exacerbation Risks. Int J Chron Obstruct Pulmon Dis. 2026;21:1–12. doi:10.2147/COPD.S559800
33. Athanazio R. Airway disease: similarities and differences between asthma, COPD and bronchiectasis. Clinics. 2012;67:335–1343. doi:10.6061/clinics/2012(11)19
34. Aliberti S, Goeminne PC, O’Donnell AE, et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: international consensus recommendations. Lancet Respir Med. 2022;10(3):298–3062. doi:10.1016/S2213-2600(21)00277-0
35. Hill AT, Haworth CS, Aliberti S, et al. Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research. Eur Respir J. 2017;49(6). doi:10.1183/13993003.00051-2017
36. Gu Y, Zhang C, Miao J-B, et al. The association of the advanced lung cancer inflammation index with postoperative complications in patients undergoing lung resection for bronchiectasis. J Thoracic Dis. 2025;17(6):3577–3589. doi:10.21037/jtd-2024-2271
37. Bone AE, Hepgul N, Kon S, Maddocks M. Sarcopenia and frailty in chronic respiratory disease. Chron Respir Dis. 2017;14(1):85–99. doi:10.1177/1479972316679664
38. Chalmers JD, Shteinberg M, Mall MA, et al. Cathepsin C (dipeptidyl peptidase 1) inhibition in adults with bronchiectasis: AIRLEAF, a Phase II randomised, double-blind, placebo-controlled, dose-finding study. Eur Respir J. 2025;65(1). doi:10.1183/13993003.01551-2024
39. Chalmers JD, Loebinger MR, Teper A, et al. Brensocatib in patients with bronchiectasis: subgroup analyses from the WILLOW trial. ERJ Open Res. 2025;11(1). doi:10.1183/23120541.00505-2024
40. Johnson ED, Long MB, Perea L, et al. Broad Immunomodulatory effects of the dipeptidyl-peptidase-1 inhibitor brensocatib in bronchiectasis: data from the phase 2, double-blind, placebo-controlled WILLOW trial. Am J Respir Crit Care Med. 2025. doi:10.1164/rccm.202408-1545OC
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of Advanced Lung Cancer Inflammation Index in Predicting COPD Exacerbation Risks
Kwok WC, Leung SHI, Tam TCC, Chau CH, Lam FM, Ho JCM
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:559800
Published Date: 31 January 2026