Back to Journals » Patient Preference and Adherence » Volume 16
Adherence to Optimal Breastfeeding Practices Among HIV-Positive Mothers in Kilimanjaro, Tanzania
Authors Philemon RN ![]() , Mmbaga BT
, Mmbaga BT ![]() , Bartlett J, Renju J, Mtuy TB, Mboya IB
, Bartlett J, Renju J, Mtuy TB, Mboya IB ![]() , Msuya SE
, Msuya SE ![]()
Received 23 October 2021
Accepted for publication 4 March 2022
Published 30 March 2022 Volume 2022:16 Pages 841—852
DOI https://doi.org/10.2147/PPA.S343213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Rune Nathaniel Philemon,1 Blandina T Mmbaga,1,2 John Bartlett,3 Jenny Renju,4,5 Tara B Mtuy,4,6 Innocent B Mboya,4,7,8 Sia E Msuya4,7,9
1Department of Pediatrics and Child Health, Kilimanjaro Christian Medical University College (KCMUCo) & Kilimanjaro Christian Medical Centre (KCMC), Moshi, Kilimanjaro, Tanzania; 2Department of Research, Kilimanjaro Clinical Research Institute (KCRI), Moshi, Kilimanjaro, Tanzania; 3Duke Global Health Institute, Duke University, Durham, NC, USA; 4Department of Epidemiology & Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College (KCMUCo), Moshi, Kilimanjaro, Tanzania; 5Department of Population Studies, Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine (LSHTM), London, UK; 6Faculty of Public Health and Policy and the Department of Global Health and Development, London School of Hygiene & Tropical Medicine (LSHTM), London, UK; 7Department of Community Health, Institute of Public Health, Kilimanjaro Christian Medical University College (KCMUCo), Moshi, Kilimanjaro, Tanzania; 8School of Mathematics, Statistics & Computer Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa; 9Department of Community Health, Kilimanjaro Christian Medical Centre (KCMC), Moshi, Kilimanjaro, Tanzania
Correspondence: Rune Nathaniel Philemon, Department of Pediatrics and Child Health, Kilimanjaro Christian Medical University College (KCMUCo) & Kilimanjaro Christian Medical Centre (KCMC), P O Box 2240, Moshi, Kilimanjaro, Tanzania, Tel +255 754 389 049, Email [email protected]
Purpose: We sought to assess how HIV-positive mothers enrolled in the PMTCT program adhere to breastfeeding recommendations concerning early initiation of breastfeeding (EIBF), ie, within one hour of birth, pre-lacteal feeds, exclusive breastfeeding until six months (EBF), and continued breastfeeding to one year of age. This study was designed to assess the practices in response to changing recommendations for breastfeeding in HIV, which have differed drastically over the years.
Patients and Methods: We recruited 524 mother-child pairs from 37 PMTCT clinics across Kilimanjaro, Tanzania. The 5 clinics with the highest patient load in each of the 7 districts of Kilimanjaro were chosen, plus the zonal and municipal referral hospitals. The children were below two years of age and currently in the PMTCT program. We administered a questionnaire to assess the mother’s practices in feeding the child. We used multiple logistic regression models to determine factors associated with EIBF, EBF, and continued breastfeeding.
Results: EIBF was achieved for 73.1% of babies. Cesarean delivery, low birth weight, and partner disclosure of HIV status were significant risk factors for not achieving EIBF. About 19% of children did not breastfeed exclusively. Of the 247 children ≥ 12 months old, 43.3% had stopped breastfeeding before 12 months. Counseling on ARV, having had > 2 pregnancies while HIV-positive and EBF were associated with breastfeeding until 12 months old. Using ART for more than two years decreased the odds of EBF and continued breastfeeding to 12 months of age.
Conclusion: Adherence to breastfeeding recommendations for HIV-positive women is suboptimal, particularly in aspects of recent changes in recommendations such as continuing breastfeeding for one year. There is a missed opportunity for interventions such as counseling, which has shown to favor adherence. Health education and counseling are needed for providers and mothers to keep them abreast with the frequently changing recommendations.
Keywords: early initiation, continued breastfeeding, exclusive breastfeeding, feeding recommendations
Introduction
Breastfeeding has long been the basis of infant nutrition. It has been shown to have many benefits beyond childhood for both the mother and the child.1,2 Breastfed children show better growth trends and have fewer diseases than non-breastfed infants.2 The World Health Organization (WHO) recommends that breastfeeding should be initiated within one hour of birth and that children be exclusively breastfed for the first six months of life.3,4 For children born to mothers infected with human immunodeficiency virus (HIV), the current recommendation is to introduce appropriate complementary feeds after six months of exclusive breastfeeding (EBF) and continue breastfeeding until the age of one year.3 Globally, these recommendations are yet to be realized, with 43% of newborns initiated within an hour of birth, 41% getting EBF, and only 70% being breastfed at one year.5
The current recommendations have been in place since 2010, but several varied recommendations have existed before this.6–8 Changes in breastfeeding recommendations that have been issued for HIV-positive women over the years have resulted in confusion that could have hindered optimal breastfeeding practices.9,10 In addition to this, other factors such as cultural practices involving pre-lacteal feeds and breastfeeding in public, myths around breast milk, childhood illnesses, and fear of transmitting HIV to the child may have led many mothers to not practice the recommended optimal breastfeeding practices.11 A mother’s knowledge of optimal breastfeeding recommendations also acts to influence their practices; however, many mothers have little knowledge on optimal breastfeeding, even in settings where breastfeeding is widely practiced.12,13 While having had a previous pregnancy and have previously received counseling appears to be a major influencer of knowledge and practice of optimal breastfeeding, not all mothers are getting counseling on infant feeding.12,13
Varying levels of knowledge regarding recommendations for the prevention of mother-to-child transmission (PMTCT) of HIV, a lack of universal counseling, and multiple other influencers of breastfeeding practices exist. Even though the current breastfeeding recommendations are known to work in research settings, it is important to know if mothers are adhering to these recommendations in real-world settings as this has implications on growth and development of the baby. This study explored how HIV-positive mothers adhere to PMTCT recommendations for optimal infant feeding in this varied environment. In this context, optimal breastfeeding was considered when initiation was within one hour, no prelacteal feeds were given, exclusive breastfeeding continued for 6 months, and the child was breastfed for 12 months as per WHO recommendations.3,4
Patients and Methods
Study Design
We conducted a cross-sectional study amongst women attending PMTCT services in Kilimanjaro region Northern Tanzania with children between one month and two years of age. The data was collected between August 2019 and April 2020. The principal aim of the study was to examine feeding practices that mothers had used regarding their child enrolled in the PMTCT program. We wanted to see whether their practices aligned with the optimal feeding recommendations given for PMTCT and what factors could be influencing their practices. The cross-sectional design allowed the capture of women who had children across different age groups and hence provides a picture of practices across the entire spectrum of the feeding recommendations.
Study Site and PMTCT Program
The study was conducted in 37 PMTCT clinics across each of the seven districts of the Kilimanjaro region in Northern Tanzania. The district medical officer was asked to provide a list of clinics with the highest PMTCT client load in each district. The selected clinics were located in facilities varying from dispensaries to referral hospitals. All mothers had to provide written informed consent prior to enrolment in the study.
The PMTCT program aims at achieving HIV-free survival for children born to HIV-positive mothers by providing women and their families with access to HIV services such as testing, treatment, and support.14 All the PMTCT clinics offer counseling and testing services for HIV, dispense antiretrovirals (ARV), and provide counseling on infant feeding. The clinics also collect dry blood spot specimens from infants for PCR testing in zonal laboratories as part of the early infant diagnosis (EID) component of PMTCT. Infant growth and development monitoring is also incorporated into the PMTCT clinic to reduce the number of hospital visits for clients, allowing mothers to attend clinics on a monthly basis.14 We aimed to enroll all eligible mothers at each clinic during their routine clinic days; hence we visited each of the clinics for a minimum of one month. To avoid repetition of enrollment, we placed markers in files of enrolled clients to serve as identifiers. The mothers were interviewed by trained research assistants using the digitalized questionnaire. The questionnaire contained skip patterns and compulsory limits to ensure the data collected was complete and clean.
Study Population
We enrolled 524 mother-child pairs who were enrolled in any of the 37 selected PMTCT clinics. For each of the 7 districts of Kilimanjaro region where the study was conducted, we selected the five clinics with the highest patient load. We also included the municipal and zonal referral hospitals, as they have supervisory and training roles over the other clinics. We then invited all mothers with children enrolled in PMTCT were invited to participate in the study during their routine visits. All children had to be less than two years of age to be eligible. By looking at all children below two years of age, we could assess what was happening at the different feeding milestones. The women had to be the biological mothers of the children (guardians and fathers were not eligible) in order to provide more accurate first-hand information on the child’s breastfeeding history.
Study Tool, Users and Content
To capture the information, we used a questionnaire with open and closed-ended questions that we had developed. The questionnaire covered demographics, HIV history of the mother, as well as antenatal, delivery, and feeding history of the reference child. The questionnaire was developed in English, translated into Kiswahili (the language in which it was administered), then back-translated into English. The questionnaire was piloted on 30 women from clinics not participating in the study. The approved questionnaire was then loaded onto password-secured tablets for administration using Survey-CTOTM. Research assistants administered the questionnaires from the tablets in Kiswahili.
Data Analysis
We performed data analysis using Stata version 15.1. Frequencies and percentages summarized categorical variables while mean age and standard deviation for numeric variables. We used the logistic regression models to determine factors associated with breastfeeding practices, specifically timely breastfeeding initiation, exclusive breastfeeding up to six months, and continued breastfeeding up to twelve months. The selection of variables to include in the final model was performed using stepwise regression methods, ie, forward selection and backward elimination at a 10% threshold level. The final models had the factors significantly associated with breastfeeding practices at a 5% threshold level. Narrations were used to summarize reported reasons for not giving the child colostrum and to identify pre-lacteal feeds given to the baby before breastfeeding.
Results
Maternal and Child Background Characteristics
The mean age of the 524 mothers was 31.7 years (SD ± 6.6). The majority of the mothers were above 24 years of age (82.3%), had a primary school education (66.6%), and were married (45.2%). Concerning their HIV status, 71.4% reported having known their positive status for less than five years, and 53.6% had been using ART for two years or less.
For the children, the mean age was 10.3 months (SD ± 6.6). At birth, 93.3% of the children had normal birth weight (>2500g) (Table 1).
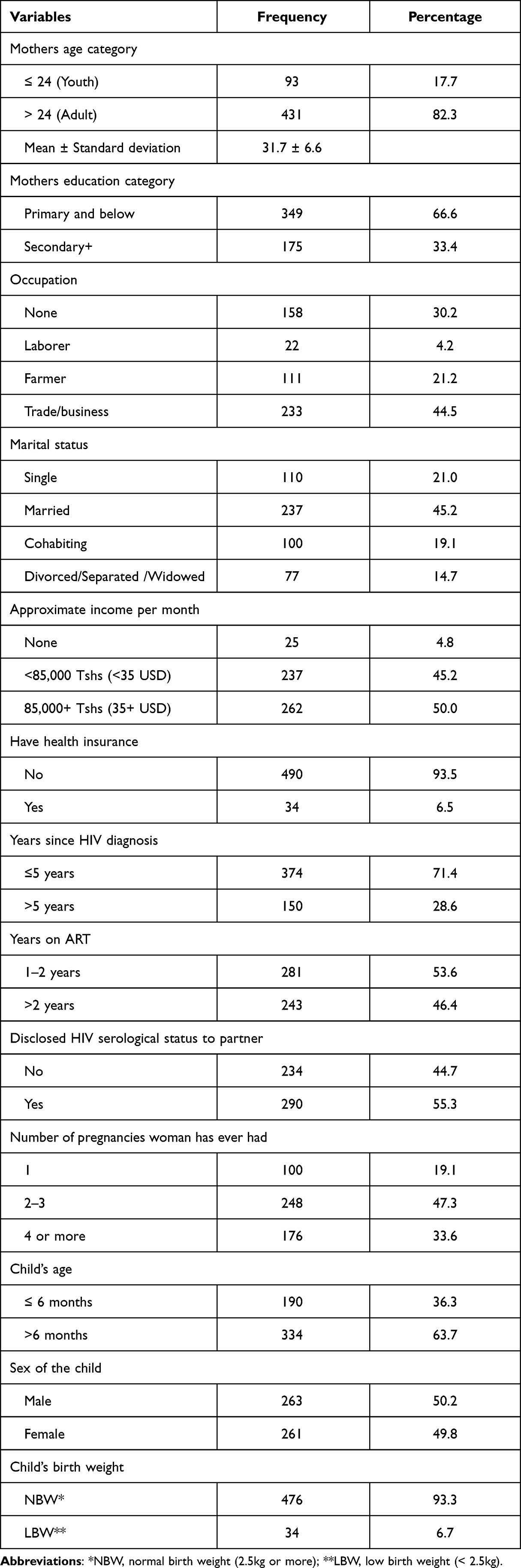 |
Table 1 Maternal Background Characteristics (N=524) |
Maternal Reproductive Characteristics
For 65.6% of the mothers, the reference child was their first while HIV-positive. 518 (98.9%) women reported having attended antenatal clinic (ANC) during their pregnancy with the reference child. For those that attended ANC, 263 (51.8) booked in the second trimester of their pregnancy, and 87.5% of the mothers attended at least four ANC visits. 97.3% of the mothers delivering at health facilities, counseling on breastfeeding was provided to 86.3% of women during ANC and 73.9% during postnatal clinics (Table 2). However, only 13.2% reported receiving breastfeeding support in terms of training on positioning the baby during breastfeeding and breastfeeding technique after delivery.
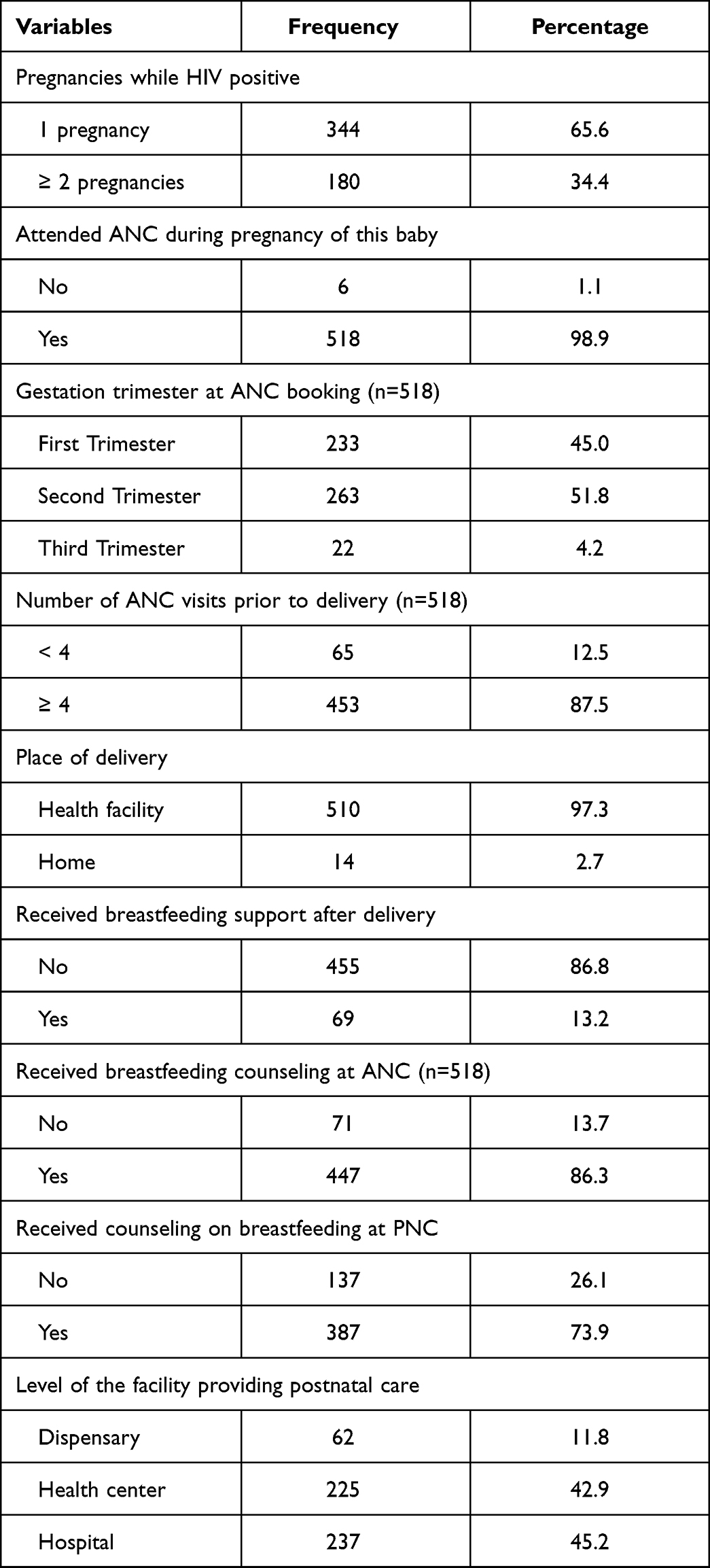 |
Table 2 Maternal Reproductive Characteristics (N=524) |
Breastfeeding Practices
The recommended initiation of breastfeeding within one hour of delivery was achieved for 73.1% of the children. Pre-lacteal feeds were given to 2.3% of the children, and 1.5% were not given colostrum. At the time of the study, 18.9% of the mothers were reported to have not conformed with exclusive breastfeeding. Two hundred forty-seven children were older than 12 months at the time of the study, and of these, 43.3% were reported to have ceased breastfeeding before the recommended age of 12 months (Figure 1).
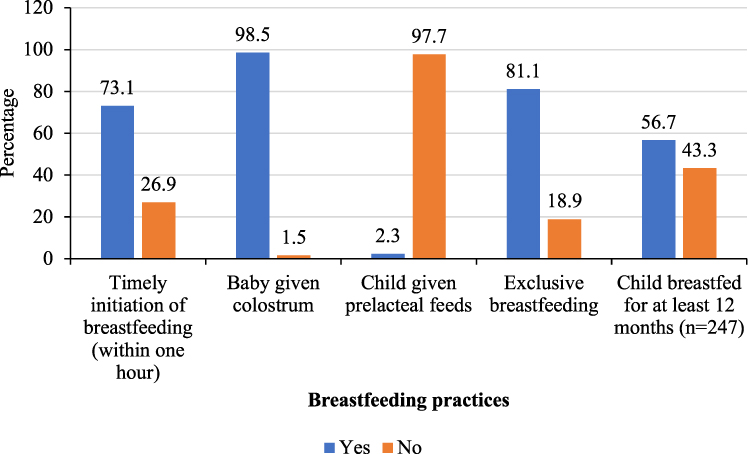 |
Figure 1 Breastfeeding practices. |
Of those that did not give colostrum, 2 said a nurse advised them not to give colostrum, 3 said it was because the baby was ill and had to be admitted, and 3 reported to have been told colostrum was “not good for the baby” or “was dirty milk”.
Factors Associated with Early Initiation of Breastfeeding
When we adjusted for other factors, mothers who had delivered by cesarean section (AOR=0.27, 95% CI 0.16, 0.45), delivered low birthweight babies (AOR=0.45, 95% CI 0.21, 0.98), disclosed their HIV serological status to partner (AOR=0.57, 95% CI 0.36, 0.89) were significantly less likely to have initiated breastfeeding within the first hour. Likewise, those who had known their positive status for more than five years (AOR=0.65, 95% CI 0.38, 1.09) were less likely to initiate breastfeeding within one hour, though this association was not statistically significant. Having had more than one pregnancy while HIV-positive (AOR=2.02, 95% CI 1.19, 3.43) was the only factor favoring EIBF with any statistical significance (Table 3).
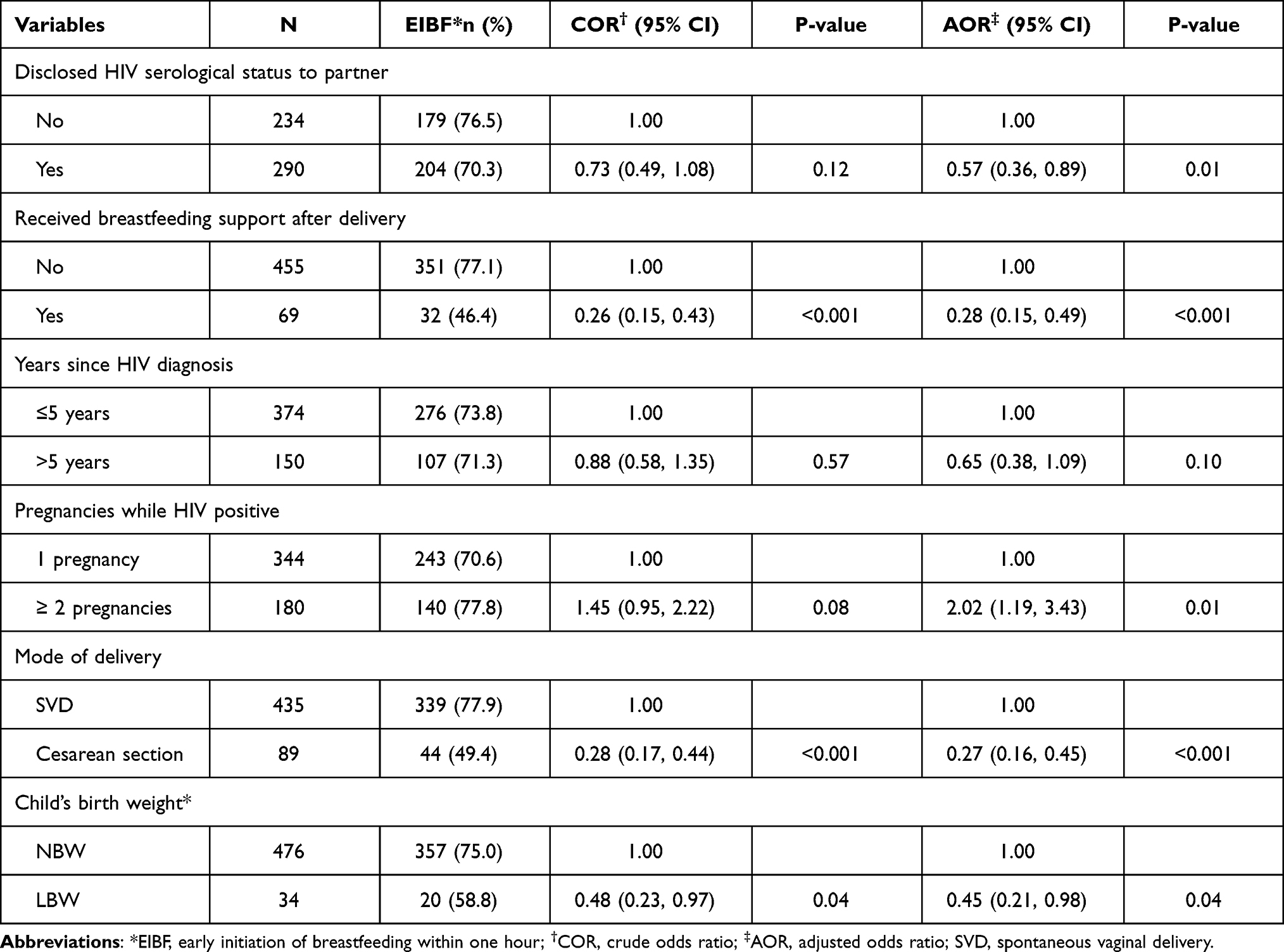 |
Table 3 Factors Associated with Breastfeeding Initiation Within One Hour After Birth (N=524) |
Factors Associated with Exclusive Breastfeeding Up to Six Months
Mothers who had had more than one pregnancy while HIV-positive were 1.97 times more likely to breastfeed exclusively than those who had only one (AOR=1.97, 95% CI 1.10, 3.53), adjusted for other factors. Having been diagnosed HIV-positive for more than five years (AOR=0.41, 95% CI 0.23, 0.74) and having four or more ANC visits (AOR=0.29, 95% CI 0.11, 0.74) were significantly associated with lower odds of breastfeeding exclusively for six months. The level of Health facility that the mother received her ANC care also showed a statistically significant association with EBF. Adjusted for other factors, those who received ANC from a dispensary (AOR=0.23, 95% CI 0.11, 0.48) or health center (AOR=0.53, 95% CI 0.31, 0.89) were less likely to practice EBF compared to those receiving care in hospitals (Table 4).
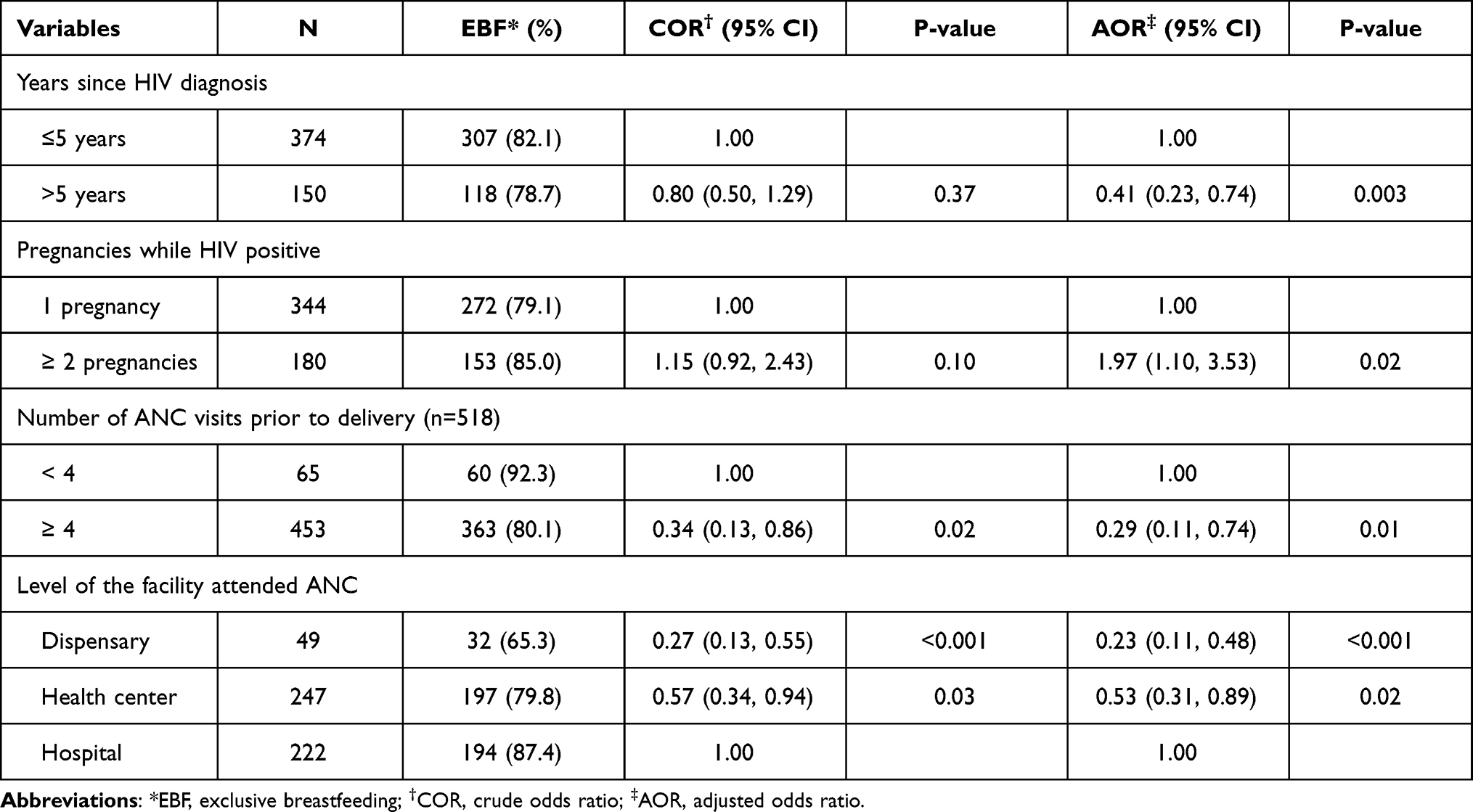 |
Table 4 Factors Associated with Exclusive Breastfeeding Up to Six Months (N=524) |
Factors Associated with Continued Breastfeeding Up to 12 Months
In the adjusted analysis, while mothers who had received ARV counseling during PNC were more likely to continue breastfeeding for up to 12 months (AOR=2.44, 95% CI 1.23, 4.84), and those who had used ART for more than two years were significantly less likely to do so (AOR=0.25, 95% CI 0.12, 0.54). Having had more than two pregnancies while HIV-positive (AOR=3.14, 95% CI 1.43, 6.88) and having successfully practiced EBF (AOR=4.00, 95% CI 2.03, 7.88) showed a statistically significant association within increased odds of practicing continued breastfeeding up to at least 12 months (Table 5).
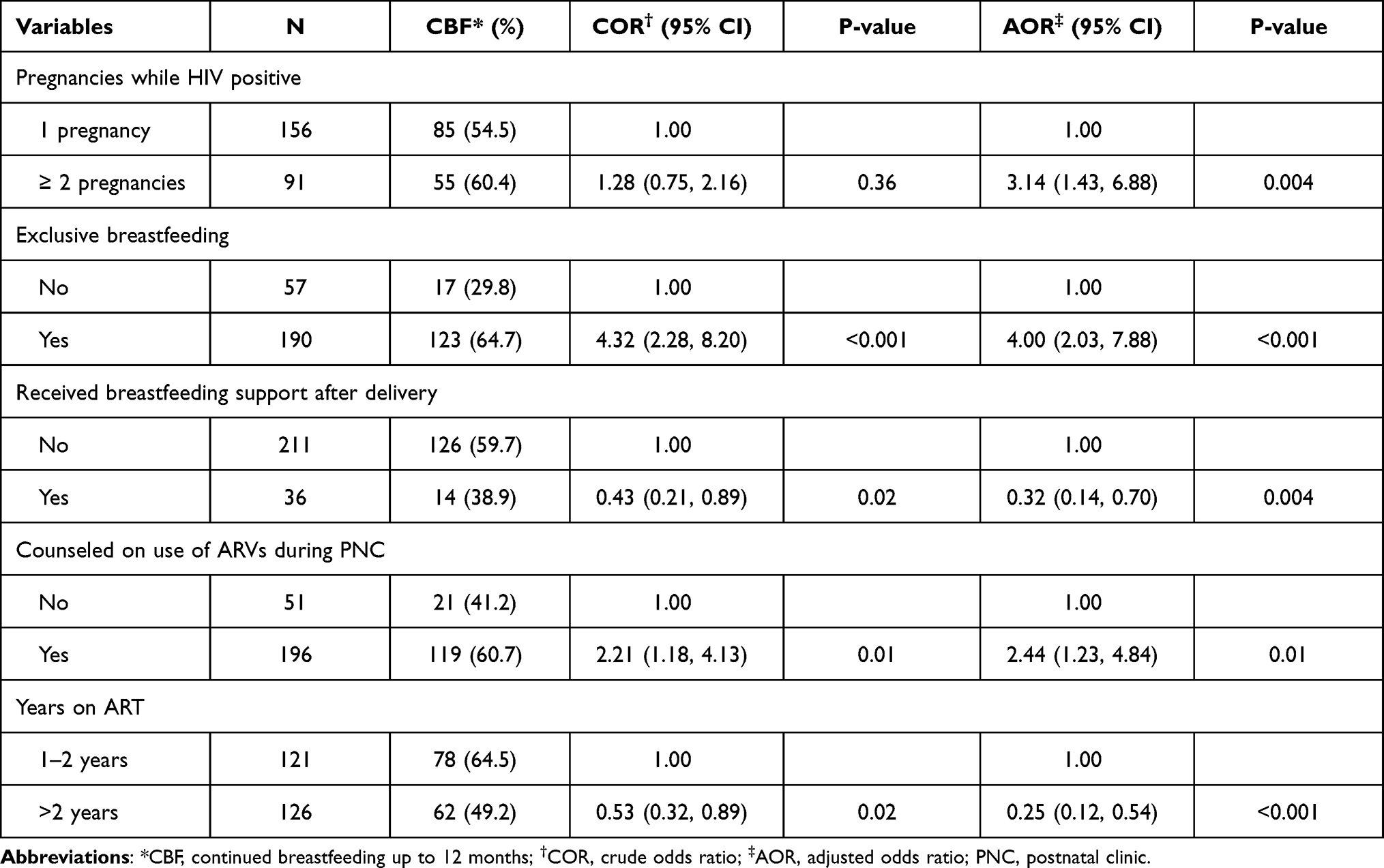 |
Table 5 Factors Associated with Continued Breastfeeding Up to 12 Months (N=247) |
Discussion
The study enrolled 524 mother-child pairs with children below 2 years of age receiving care in the PMTCT program. EIBF was found to be 73.1%, EBF was practiced for 81.1% of the children, and breastfeeding for 1 year was achieved for 56.7%. Restriction of colostrum and giving pre-lacteal feeds was reported for 1.5% and 2.3%, respectively.
In our study, the initiation of breastfeeding within one hour was achieved for 73.1% of children. Earlier studies in Kilimanjaro that looked at the general population (irrespective of HIV status) report the rate of EIBF to be 70%-71.1%.15,16 The difference in EIBF that we see in our study compared to these might result from the increased desire to exclusively breastfeed due to maternal HIV status and counseling given to the mothers. Another study from Moshi Municipality reported 83% of mothers to have achieved EIBF, but this was also in a general population and an urban setting.17 At the national level, it is reported that 53.5% of newborns are initiated on breastfeeding within one hour of birth, far below what was observed in the current study.18 However, our findings are not far from a study in Malawi, which reported EIBF to be 70% amongst HIV-positive women.19 A study from 2015 in Uganda reported that HIV-positive mothers are more likely to delay breastfeeding initiation.20 Though this does not seem to be the case in our setting, a study comparing EIBF in HIV-positive vs HIV-negative mothers in this setting would be needed to be certain. With EIBF being a predictor of successful EBF, a rate of 70% or even 83% raises concerns, given the importance of EBF.21 These figures are also likely to be overestimating the practice of EIBF as self-reported rates have been shown to do perhaps due to the subjectivity in the perception of time lapses.22 Thus, there is an urgent need to address these low rates. There is little evidence of what interventions could improve this situation, which is a key area for research, particularly in resource-limited settings.23 Setting-specific barriers on why women lack support to initiate breastfeeding despite high levels of facility delivery need to be explored and addressed.
In our study, EIBF among HIV-positive women was promoted by having two or more pregnancies and was deterred by breastfeeding support (guidance on how to breastfeed) after delivery, cesarean delivery, and low birth weight of the child. Other studies have also reported that illness of the child and cesarean delivery to be a deterrent of EIBF.15,17,20 Given the small number who report to have received breastfeeding support post-delivery, we postulate that these were mothers facing increased difficulty with breastfeeding. Although it is recommended that support be given to all mothers, it seems in our setting, this is not routine practice.
Pre-lacteal feeds and withholding of colostrum are associated with early cessation of breastfeeding.24 These are not common practices in our setting, however, we found some myths surrounding these practices, and some reported that they were steered into these malpractices by healthcare workers. The presence of such beliefs has been reported in the general population. If Healthcare workers share and propagate these misconceptions, they can undermine the messages of the PMTCT program.11,25
Eighty-one percent of the mothers in our study reported having practiced EBF with the reference child. This is relatively high compared to previous studies in the region, which had reported rates of 55% and the national average of 58.6%.18,26 The proportion of EBF in this study is in keeping with reports from other parts of Tanzania and Africa.19,27–29 Like with EIBF; we found that having had more than two pregnancies while HIV-positive significantly increased the odds of EBF. We speculate that the mothers with more deliveries draw upon their previous experiences to overcome the challenges of EBF. The emphasis put on EBF for HIV-positive mothers and their repeated clinic visits might also have a role to play.
Surprisingly, and in keeping with the situation for EIBF, those with a longer duration since HIV diagnosis were less likely to practice EBF. We could not determine why in this study, but speculate that those women exposed to pre-option B+ recommendations, which recommended different durations of EBF at different time points and encouraged replacement feeding, are less likely to adhere to current EBF recommendations.8,9 A higher number of ANC visits also appears to decrease odds of EBF. However, other studies have reported increased ANC visits to have the opposite effect.30 We speculate that mothers with a high number of ANC visits are more likely to have health complications and, hence, less compliant, something demonstrated in other settings.31 Our study found higher-level health facility delivery to have better EBF practice compared to lower-level facilities. More staff available for counseling and more conducive environments for counseling in higher-level facilities might be the reason for this trend.32
We found that 56.7% of the infants 1-year-old or more were breastfed until one year as recommended.6 This is lower than the global average, previously estimated at 73.3%, and less than studies in Malawi where they reported continued breastfeeding to be 91%.2,19 It is also well below the national average for breastfeeding at one year in Tanzania, estimated at 92.4%.18 The lower continued breastfeeding rate is not a regional problem, as estimates for the general public in Kilimanjaro are reported to be 92.3%, close to the national average.18 We think this reflects HIV-positive mothers being over-cautious and untrusting of the PMTCT recommendations, hence stopping breastfeeding early to avoid transmission. It raises the question of where these mothers are getting the information they trust. Some studies clearly show that mothers are more likely to accept what they get from their peers than health workers when faced with contradicting information.33 Given that only 64.9% of HIV-positive mothers have good knowledge of PMTCT and that only 71.4% could identify the recommended duration of breastfeeding, there is a need to identify the source of information these mothers use.13 It is also important to establish the reasons behind their reliance on these sources.
This study has given a portrait of breastfeeding practice among HIV-positive women across the Kilimanjaro region, capturing both rural and urban mothers and their practices. However, since the information is self-reported and not from direct observation, it must be acknowledged that the findings are likely to be an overestimation of practice, which is a key limitation in this sort of study.22 With this limitation in mind, the need for action is further emphasized as the reality might be worse than what we have found in this study.
Conclusion
Mothers in the PMTCT program seem to be faring much better than the general population regarding EIBF and EBF though they have not reached the intended target. Continued breastfeeding until one year appears to be an even greater challenge. The failure of women in the PMTCT program to adhere to the guidelines could mean that providers are failing to take the opportunity to address challenges the women are facing. It could also mean that mothers are choosing not to follow the advice of the providers, which opens the question as to where they are getting the advice they follow. There is thus a need to explore the interaction between mothers and healthcare providers in terms of what they are being told and examine the sources of alternative information that influences their breastfeeding practices.
Abbreviations
ART, antiretroviral therapy; ARV, antiretrovirals; ANC, antenatal clinic; EBF, exclusive breastfeeding; EIBF, early initiation of breastfeeding; EID, early infant diagnosis; HIV, human immunodeficiency virus; LBW, low birth weight; NBW, normal birth weight; PMTCT, prevention of mother to child transmission; PNC, postnatal clinic; SVD, spontaneous vaginal delivery.
Data Sharing Statement
Data can be obtained by request from the authors.
Ethics
This study was conducted in accordance with the Helsinki declaration. The Kilimanjaro Christian Medical University College Research Ethics Committee provided ethical permission (certificate number 2434) for the study. The regional medical officer for Kilimanjaro, as well as the district Medical officers and the heads of participating clinics, approved the conduct of the study in their respective domains. Research assistants approached the mothers during routine clinic visits and asked for their participation in the study. Mothers were informed about the purpose of the study, the nature of data intended to be collected, and the intended use of the data. Mothers who agreed to participate were asked to sign a consent form prior to data collection.
Acknowledgments
This work was supported through the DELTAS Africa Initiative grant # DEL-15-011 to THRiVE-2. The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS) ’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust grant # 107742/Z/15/Z and the UK government. The views expressed in this publication are those of the author (s) and not necessarily those of AAS, NEPAD Agency, Wellcome Trust or the UK government.
This study was also supported by the United States National Institutes of Health Medical Education Partnership Initiative-Junior Faculty (MEPI-JF) Award D43TW10138.
Dr. Bartlett receives salary support from the Duke University Center for AIDS Research P30AI64518 and the Fogarty International Center D43 TW009595.
We also wish to extend our gratitude to the regional medical office for Kilimanjaro, the district medical officers, the facilities where this study took place, and all the study participants.
Disclosure
Dr. Rune Philemon reports grants from THRiVE-2 and MEPI-JF during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Williams AM, Suchdev PS. Assessing and improving childhood nutrition and growth globally. Pediatr Clin North Am. 2017;64(4):755–768. doi:10.1016/j.pcl.2017.03.001
2. Victora CG, Bahl R, Barros AJD, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/s0140-6736(15)01024-7
3. World Health Organization. United Nations Children’s Fund. Guideline: updates on HIV and infant feeding: The duration of breastfeeding, and support from health services to improve feeding practices among mothers living with HIV. Geneva: World Helath Organization; 2016.
4. World Health Organization. Breastfeeding; 2021. Available from: https://www.who.int/health-topics/breastfeeding#tab=tab_1.
5. World Health Organizations, United Nations Children’s Fund. Global breastfeeding scorecard, 2019: increasing commitment to breastfeeding through funding and improved policies and programmes 2019; 2019. Available from: https://apps.who.int/iris/handle/10665/326049.
6. Sint TT, Lovich R, Hammond W, et al. Challenges in infant and young child nutrition in the context of HIV. AIDS. 2013;27:S169–S177. doi:10.1097/qad.0000000000000089
7. Setegn T, Haile D, Biadgilign S. Adherence to WHO breastfeeding guidelines among HIV positive mothers in Southern Ethiopia: implication for intervention. Pediatric Health Med Ther. 2015;87. doi:10.2147/phmt.s82356
8. Dunkley E, Ashaba S, Burns B, et al. “I beg you … breastfeed the baby, things changed”: infant feeding experiences among Ugandan mothers living with HIV in the context of evolving guidelines to prevent postnatal transmission. BMC Public Health. 2018;18(1). doi:10.1186/s12889-018-5081-x
9. Horwood C, Haskins L, Engebretsen I, Connolly C, Coutsoudis A, Spies L. Are we doing enough? Improved breastfeeding practices at 14 weeks but challenges of non-initiation and early cessation of breastfeeding remain: findings of two consecutive cross-sectional surveys in KwaZulu-Natal, South Africa. BMC Public Health. 2020;20(1). doi:10.1186/s12889-020-08567-y
10. Lang’at PC, Ogada I, Steenbeek A, et al. Infant feeding practices among HIV-exposed infants less than 6 months of age in Bomet County, Kenya: an in-depth qualitative study of feeding choices. Arch Dis Child. 2018;103(5):470–473. doi:10.1136/archdischild-2017-314521
11. Mgongo M, Hussein TH, Stray-Pedersen B, Vangen S, Msuya SE, Wandel M. Facilitators and barriers to breastfeeding and exclusive breastfeeding in Kilimanjaro Region, Tanzania: a qualitative study. Int J Pediatr. 2019;2019:8651010. doi:10.1155/2019/8651010
12. Hashim TH, Mgongo M, Katanga J, et al. Predictors of appropriate breastfeeding knowledge among pregnant women in Moshi Urban, Tanzania: a cross-sectional study. Int Breastfeed J. 2016;12(1). doi:10.1186/s13006-017-0102-4
13. Philemon RN, Mmbaga BT, Bartlett J, et al. Do women enrolled in PMTCT understand the recommendations: a case study from Kilimanjaro. Patient Prefer Adherence. 2021;15:1301–1309. doi:10.2147/ppa.s307847
14. Prevention of Mother to Child Transmission of HIV Pocket Guide; 2012.
15. Ali F, Mgongo M, Mamseri R, George JM, Mboya IB, Msuya SE. Prevalence of and factors associated with early initiation of breastfeeding among women with children aged < 24 months in Kilimanjaro region, northern Tanzania: a Community-based cross-sectional study. Int Breastfeed J. 2020;15(1). doi:10.1186/s13006-020-00322-8
16. Kiwango F, Mboya IB, John B, Hashim T, Msuya SE, Mgongo M. Prevalence and factors associated with timely initiation of breastfeeding in Kilimanjaro region, northern Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1). doi:10.1186/s12884-020-03209-y
17. Lyellu HY, Hussein TH, Wandel M, Stray-Pedersen B, Mgongo M, Msuya SE. Prevalence and factors associated with early initiation of breastfeeding among women in Moshi municipal, northern Tanzania. BMC Pregnancy Childbirth. 2020;20(1). doi:10.1186/s12884-020-02966-0
18. Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], Tanzania Food and Nutrition Centre (TFNC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS) [Zanzibar] and UNICEF. Tanzania National Nutrition Survey using SMART Methodology (TNNS) 2018. Dar es Salaam, Tanzania: MoHCDGEC, MoH, TFNC, NBS, OCGS, and UNICEF; 2018. Available from: https://www.unicef.org/tanzania/media/2141/file/Tanzania%20National%20Nutrition%20Survey%202018.pdf.
19. Flax VL, Hamela G, Mofolo I, Hosseinipour MC, Hoffman I, Maman S. Infant and young child feeding counseling, decision-making, and practices among HIV-infected women in malawi’s option B+ prevention of mother-to-child transmission program: a mixed methods study. AIDS Behav. 2016;20(11):2612–2623. doi:10.1007/s10461-016-1378-x
20. Kalisa R, Malande O, Nankunda J, Tumwine JK. Magnitude and factors associated with delayed initiation of breastfeeding among mothers who deliver in Mulago hospital, Uganda. Afr Health Sci. 2016;15(4):1130. doi:10.4314/ahs.v15i4.11
21. Group NS. Timing of initiation, patterns of breastfeeding, and infant survival: prospective analysis of pooled data from three randomised trials. Lancet Global Health. 2016;4(4):e266–75. doi:10.1016/s2214-109x(16)00040-1
22. Tahsina T, Hossain AT, Ruysen H, et al. Immediate newborn care and breastfeeding: EN-BIRTH multi-country validation study. BMC Pregnancy Childbirth. 2021;21(S1). doi:10.1186/s12884-020-03421-w
23. Balogun OO, O’Sullivan EJ, McFadden A, et al. Interventions for promoting the initiation of breastfeeding. Cochrane Database Syst Rev. 2016;2016(11). doi:10.1002/14651858.cd001688.pub3
24. Patil CL, Turab A, Ambikapathi R, et al. Early interruption of exclusive breastfeeding: results from the eight-country MAL-ED study. J Health Popul Nutr. 2015;34:10. doi:10.1186/s41043-015-0004-2
25. Tuthill EL, Chan J, Butler LM. Challenges faced by health-care providers offering infant-feeding counseling to HIV-positive women in sub-Saharan Africa: a review of current research. AIDS Care. 2015;27(1):17–24. doi:10.1080/09540121.2014.951310
26. Rasheed MH, Philemon R, Kinabo GD, Maxym M, Shayo AM, Mmbaga BT. Adherence to exclusive breastfeeding and associated factors in mothers of HIV-exposed infants receiving care at Kilimanjaro Christian Medical Centre, Tanzania. East Afr Med J. 2018;2(1):33–42. doi:10.24248/eahrj.v2i1.565
27. Aishat U, David D, Olufunmilayo F. Exclusive breastfeeding and HIV/AIDS: a crossectional survey of mothers attending prevention of mother-to-child transmission of HIV clinics in southwestern Nigeria. Pan Afr Med J. 2015;21:309. doi:10.11604/pamj.2015.21.309.6498
28. Williams AM, Chantry C, Geubbels EL, et al. Breastfeeding and complementary feeding practices among HIV-exposed infants in coastal Tanzania. J Hum Lact. 2016;32(1):112–122. doi:10.1177/0890334415618412
29. Jahanpour O, Msuya SE, Todd J, Stray-Pedersen B, Mgongo M. Increasing trend of exclusive breastfeeding over 12 years period (2002–2014) among women in Moshi, Tanzania. BMC Pregnancy Childbirth. 2018;18(1). doi:10.1186/s12884-018-2104-7
30. Dagnew AB, Tewabe T, Birhie A, et al. Factors associated with compliance with world health organization-recommended infant-feeding practices by mothers with HIV infection in Northwest Ethiopia. Curr Ther Res Clin Exp. 2019;91:39–44. doi:10.1016/j.curtheres.2019.100568
31. Majra JP, Silan VK. Barriers to early initiation and continuation of breastfeeding in a tertiary care institute of Haryana: a qualitative study in nursing care providers. J Clin Diagn Res. 2016;10(9):LC16–LC20. doi:10.7860/JCDR/2016/19072.8559
32. Kinshella M-LW, Prasad S, Hiwa T, et al. Barriers and facilitators for early and exclusive breastfeeding in health facilities in Sub-Saharan Africa: a systematic review. Global Health Res Policy. 2021;6(1). doi:10.1186/s41256-021-00206-2
33. Mgongo M, Hussein TH, Stray-Pedersen B, Vangen S, Msuya SE, Wandel M. “We give water or porridge, but we don’t really know what the child wants:” a qualitative study on women’s perceptions and practises regarding exclusive breastfeeding in Kilimanjaro region, Tanzania. BMC Pregnancy Childbirth. 2018;18(1). doi:10.1186/s12884-018-1962-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.