Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Adherence to HPV-Based Cervical Cancer Screening: A Concept Analysis for Nursing and Midwifery Practice
Authors Lumia C ![]() , Fumagalli S, Martinelli M
, Fumagalli S, Martinelli M ![]() , Ausili D
, Ausili D ![]() , Nespoli A
, Nespoli A
Received 4 February 2026
Accepted for publication 17 March 2026
Published 1 May 2026 Volume 2026:19 601358
DOI https://doi.org/10.2147/JMDH.S601358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Cristina Lumia, Simona Fumagalli, Marianna Martinelli, Davide Ausili, Antonella Nespoli
School of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy
Correspondence: Cristina Lumia, School of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy, Tel +39 3881648481, Email [email protected]
Abstract: Human papillomavirus (HPV) infection is one of the most common sexually transmitted infections worldwide and a necessary cause of cervical cancer. Although HPV vaccination and HPV-based cervical cancer screening have strengthened prevention strategies, participation across screening and follow-up pathways remains suboptimal in many settings, limiting programme effectiveness and equity. For nurses and midwives - who play a central role in counselling, education, and community-based prevention - a clear conceptualization of adherence is essential to guide practice, research, and policy. This study aimed to analyze the concept of adherence to HPV-based cervical cancer screening and to propose an operationally useful framework for nursing and midwifery practice. A literature review of peer-reviewed studies addressing adherence to HPV-based or cervical cancer screening published between 1997 and 2025 (n = 38) was conducted using PubMed, CINAHL, and PsycINFO, and Walker and Avant’s concept analysis method was applied. Adherence was defined as the extent to which eligible individuals initiate, complete, and sustain participation in recommended cervical cancer screening pathways over time in accordance with established guidelines, including appropriate timing, test modality, follow-up, and repeat screening. Defining attributes were knowledge, awareness, and empowerment; key antecedents included education and social support; and consequences encompassed improved health outcomes, fewer complications, and reduced healthcare costs. Age, gender-related factors, and healthcare professionals’ counselling practices emerged as moderators influencing adherence behaviors, while anxiety, fear, and perceived lack of need acted as mediators shaping individual screening decisions. This concept analysis clarifies adherence as a complex phenomenon extending beyond a single screening event and supports the development of tailored, nurse- and midwife-led strategies to improve equitable cervical cancer prevention.
Keywords: cervical cancer screening, human papillomavirus, adherence, concept analysis, nursing, midwifery
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted infection worldwide, with estimates indicating that up to 90% of the population will acquire at least one HPV type during their lifetime.1 Although most infections are transient and resolve spontaneously within one to two years, persistent infection with high-risk genotypes can lead to the development of precancerous lesions and cervical cancer.2 The introduction of HPV vaccination and organised screening programmes has substantially reduced HPV-related morbidity and cervical cancer incidence in many countries.2–4
Alongside vaccination, cervical cancer screening has undergone a major transition from cytology-based Pap testing to HPV DNA-based strategies due to their higher sensitivity for detecting high-grade lesions.5 Updated international guidelines increasingly recommend HPV-based screening as the primary test, often combined with extended screening intervals and risk-stratified follow-up pathways.6,7 In low- and middle-income settings, innovative approaches such as self-sampling and screen-and-treat models have been promoted to address structural and geographical barriers and to improve access among underserved populations.8 However, regardless of the screening modality adopted, the effectiveness of cervical cancer prevention programmes depends not only on test performance but also on sustained participation throughout the entire screening pathway, including initial testing, triage, follow-up, and repeat screening over time.9,10
Adherence to HPV-based screening therefore represents a critical determinant of programme success. Despite the availability of effective screening tools, adherence remains suboptimal in many contexts. Recent evidence from European settings illustrates the magnitude of this gap. In Portugal, nearly 43.9% of women were found to be non-compliant with recommended cervical screening intervals,11 while up to 30% of women remaining under- or unscreened in Switzerland.12 Participation disparities are particularly pronounced among vulnerable populations; a meta-analysis of 18 European studies reported significantly lower screening uptake among migrant women compared with native populations (OR = 0.54).13 Moreover, recent population-based analyses suggest that non-adherence to cervical cancer screening increased following the COVID-19 pandemic, rising from 19.2% to 25.8% in the United States.14 Population-based data consistently show that a substantial proportion of cervical cancer cases occur among individuals who have not been screened or who have not completed recommended follow-up. In the United States, adherence to cervical cancer screening declined between 2005 and 2019, despite expanded access to preventive services.15 Comparable gaps have been reported across different health systems and population groups, highlighting persistent disparities between recommended screening pathways and real-world participation.15,16 Despite the extensive literature on screening uptake and participation, no unified conceptual framework of adherence specific to HPV-based cervical cancer screening pathways has been clearly established.
Across the literature, however, adherence to HPV or cervical cancer screening is inconsistently defined and variably operationalised. Studies refer to adherence using overlapping terms such as screening uptake, participation, compliance with recommended intervals, completion of follow-up after abnormal results, or continuity across repeated screening rounds.10,16,17 While these terms are often used interchangeably, they reflect distinct dimensions of screening behaviour. For example, screening uptake generally refers to initial participation, compliance refers to following recommended medical advice, and persistence describes continued engagement over time, whereas adherence encompasses the broader alignment of individual behaviours with recommended screening pathways. Operational indicators differ widely in terms of denominators, timeframes, inclusion of follow-up pathways, and handling of under- or over-screening. This heterogeneity limits comparability across studies, complicates evidence synthesis, and weakens the interpretability of adherence-related outcomes for clinicians and policymakers.
For primary care professionals involved in preventive services, including nurses and midwives, unclear definitions and measures of adherence may hinder the identification of points at which individuals disengage from screening pathways and obscure which barriers are most amenable to intervention. Psychosocial factors such as risk perception, stigma, self-efficacy, fear, and perceived lack of need interact with social and health system determinants, including access to services, professional recommendation, and continuity of care.10,12,18–20 These interacting influences underscore adherence as a multidimensional phenomenon that extends beyond a single screening event.
A review is therefore warranted to clarify how adherence to HPV-based cervical cancer screening is conceptualised and measured across the literature. By synthesising existing definitions and operational approaches, and by identifying key conceptual gaps, this review aims to support clearer measurement, improve comparability across studies, and inform the development of targeted interventions within primary care and preventive health services.
Materials and Methods
Walker and Avant’s concept analysis method21 was applied, as it provides a structured and theory-driven approach for clarifying complex concepts and supporting their operational definition in health research. Following identification of adherence to HPV screening as the concept of interest, a comprehensive review of the literature was conducted to explore how the concept has been applied across midwifery, nursing, medicine, and the social sciences.
Two reviewers independently screened titles, abstracts, and full texts to ensure methodological rigor and reduce selection bias. Defining attributes, antecedents, and consequences of adherence were identified, together with model and contrary cases to illustrate the concept in practice. In addition, moderators and mediators were examined to capture the contextual and psychosocial complexity of adherence behaviours.22 These elements were analysed to support the conceptual clarification and definition of adherence to HPV-based cervical cancer screening according to Walker and Avant’s methodological framework.
The literature search was conducted in PubMed, CINAHL, and PsycINFO using the terms (“HPV screening” OR “human papillomavirus screening” OR “cervical cancer screening”) AND (adherence OR participation OR compliance). Database-specific controlled vocabularies, including MeSH terms, CINAHL Headings, and the APA Thesaurus of Psychological Index Terms, were combined with free-text keywords to enhance sensitivity and ensure comprehensive coverage (Table 1). The search covered publications from database inception to March 2025. No geographical restrictions were applied and only articles published in English were considered. Primary and secondary research publications were eligible for inclusion if they addressed adherence or participation in HPV-based or cervical cancer screening pathways and discussed conceptual, behavioural, or health system determinants of adherence. Grey literature, conference abstracts, editorials, pilot studies, and publications not directly relevant to screening adherence were excluded from the analysis. The study selection process is presented in the PRISMA flow diagram (Figure 1). Overall, 38 publications published between 1997 and 2025 met the inclusion criteria and were included in the analysis.
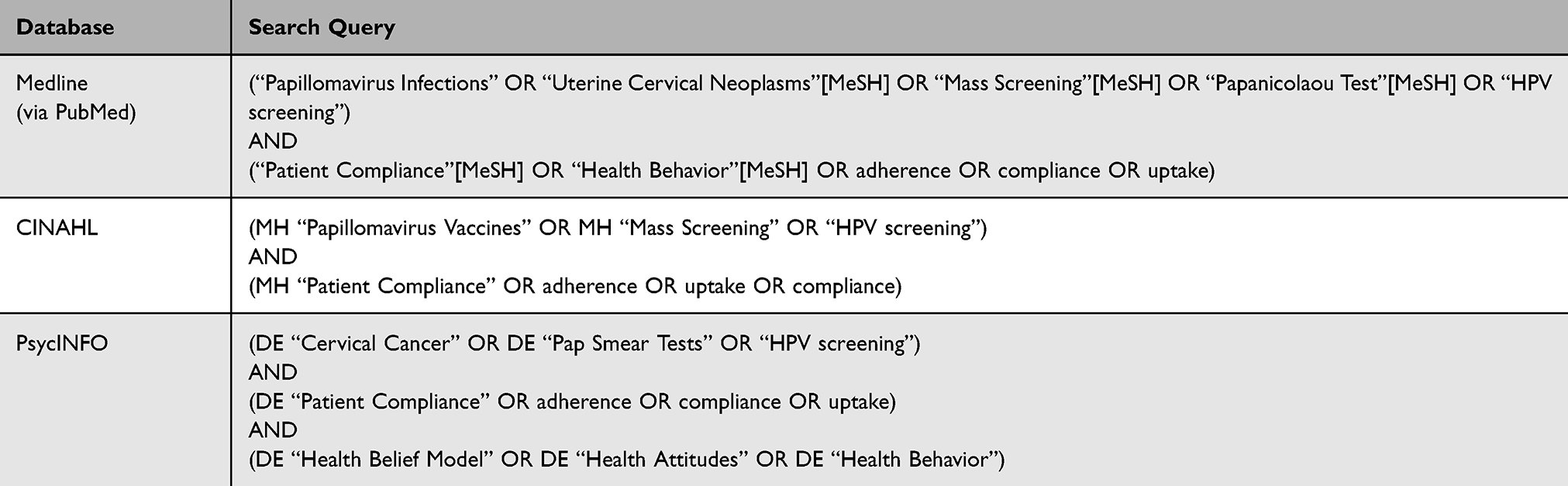 |
Table 1 Search Queries According to Each Database |
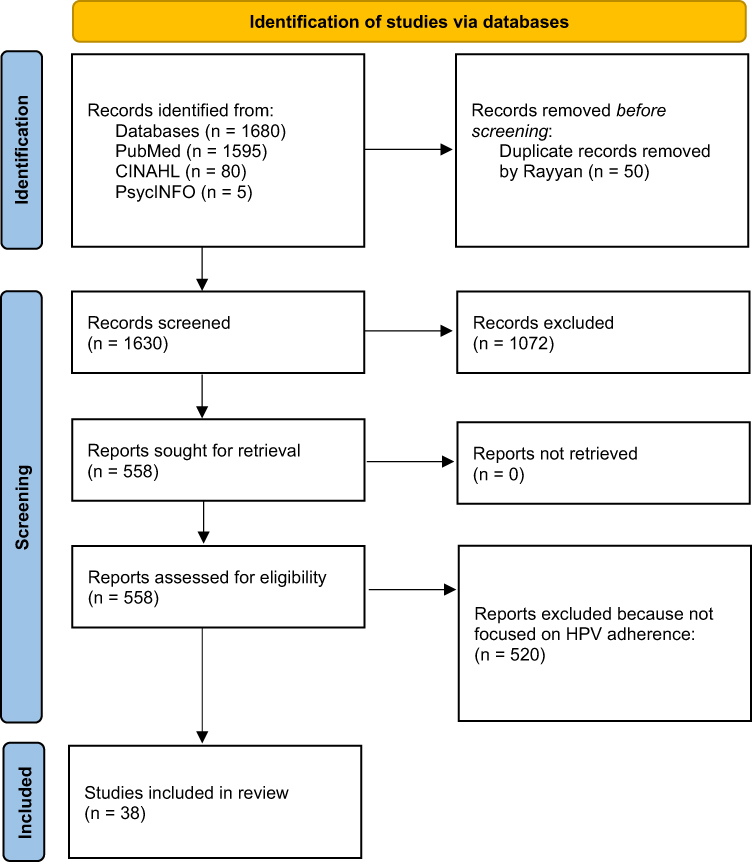 |
Figure 1 PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and final inclusion of studies in the concept analysis of adherence to HPV-based cervical cancer screening. |
Results
Defining and Identifying Adherence to HPV Screening
Adherence is defined as the proportion of the target population that follows current recommendations23 for cervical cancer screening and surveillance, including initiation of screening and completion of the recommended procedure. In the context of cancer screening, adherence is inherently multidimensional, as recommendations typically specify starting and stopping ages, screening modalities, and screening intervals.24 Consequently, adherence reflects not only participation prevalence and intervention efficacy, but also psychosocial and contextual factors influencing screening behaviours.25
Evidence indicates that adherence encompasses both initial participation and sustained engagement over time. A population-based study among Chinese women demonstrated that vaccination status and sociocultural factors influenced both uptake and continuity of cervical cancer screening,16 highlighting the importance of social context in shaping adherence behaviours. Psychosocial factors further complicate adherence patterns. A prospective pilot study found that perceived risk and HPV awareness alone did not reliably predict follow-up adherence after abnormal screening results, suggesting that knowledge alone is insufficient to ensure continued participation.10
Age has also been associated with screening participation patterns. A national survey in the United States reported higher adherence among younger caregivers, potentially reflecting greater exposure to HPV awareness and prevention initiatives.18 Other studies have operationalized adherence using guideline-defined screening intervals, classifying deviations as under- or over-screening. Such approaches enable population-level quantification of adherence and facilitate comparisons across health systems.26
Notably, HPV vaccination has been associated with reduced adherence to subsequent screening, likely due to a perceived reduction in cancer risk.27 However, the magnitude of this association has been inconsistently quantified across studies, with limited reporting of effect measures such as odds ratios or risk differences. Most studies included in this review described the relationship qualitatively rather than providing pooled quantitative estimates. This finding underscores the need for clear communication and tailored follow-up strategies to reinforce the complementary role of vaccination and screening within cervical cancer prevention programmes.
The relationship between HPV vaccination and subsequent screening participation remains complex. While some studies suggest that vaccination may reduce perceived susceptibility and therefore decrease screening motivation, other research indicates that vaccinated individuals may demonstrate higher health awareness and preventive behaviours.28 This variability highlights the importance of clear communication strategies to ensure that vaccination is understood as complementary, rather than substitutive, to regular screening.
Essential Attributes
According to Walker and Avant,21 defining attributes represent the core characteristics of a concept and distinguish it from related phenomena. In the context of HPV screening adherence, the essential attributes identified were knowledge, awareness, and empowerment.
Knowledge plays a foundational role in promoting adherence to HPV screening programmes. Educational interventions have consistently been shown to improve understanding of HPV infection, cervical cancer risk, and screening procedures, thereby enhancing participation. A randomized controlled trial conducted in Turkey demonstrated that structured cervical cancer education significantly improved women’s knowledge and acceptance of HPV screening.29 Beyond content, the way information is communicated also matters. An experimental study showed that concise, evidence-based message framing improved women’s understanding of primary HPV testing and increased intention to participate.30
Awareness and empowerment further influence adherence by enabling individuals to interpret screening results, manage screening-related anxiety, and engage proactively with healthcare services. Informed women are better equipped to understand abnormal results and adhere to recommended follow-up and screening intervals.31 Community-based education addressing both cognitive and emotional dimensions fosters empowerment and sustained participation, even in the presence of cultural stigma and social barriers.32,33
Model Case and Contrary Case
Walker and Avant’s approach of concept analysis present the model case and the contrary case (Box 1) as a real-life example that illustrates the defining qualities of HPV screening adherence, as well as an example of what the concept is not. Both examples are authentic experiences.
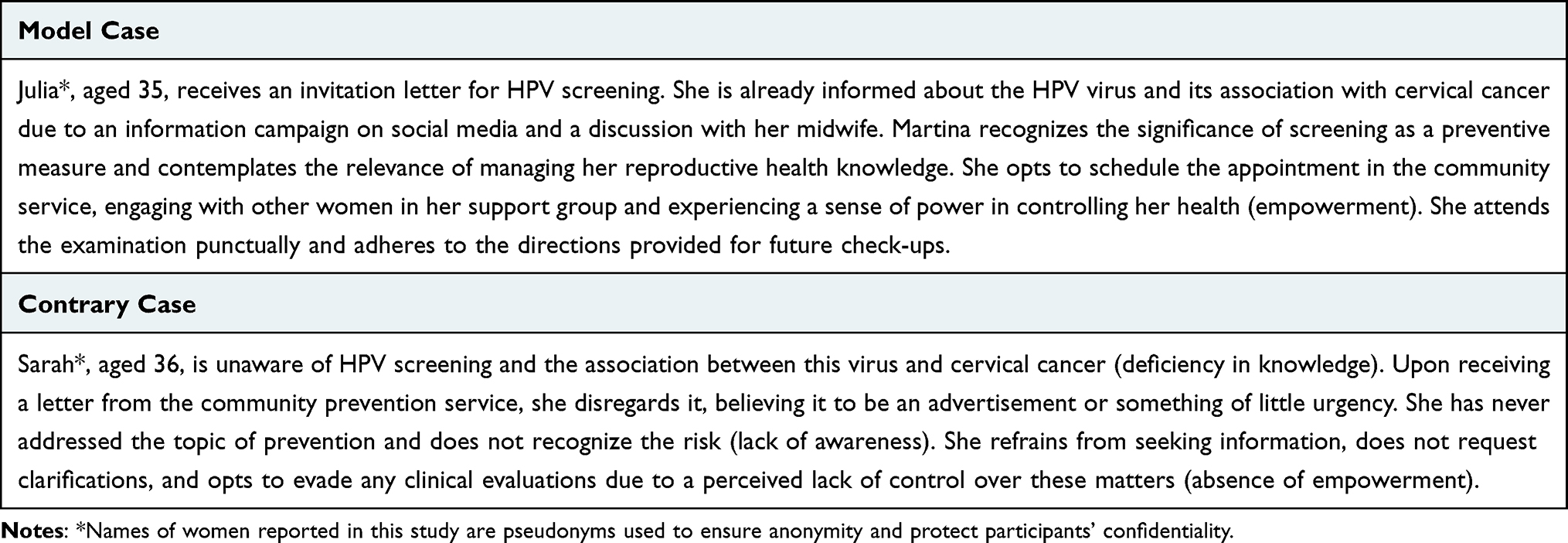 |
Box 1 Model Case and Contrary Case of HPV Screening Adherence |
Antecedents
Antecedents are events or conditions that must occur before the concept can manifest.21 Social support and education emerged as key antecedents of adherence to HPV screening. These factors are closely intertwined with HPV-related stigma, which is rooted in the association between HPV and sexually transmitted infections and can negatively affect screening behaviours.33–36
Social Support
Social support, including emotional, informational, and instrumental assistance from family members, peers, community organisations, and healthcare professionals, plays a critical role in facilitating adherence. Supportive networks promote health information exchange, normalize preventive behaviours, and reinforce adherence to screening recommendations.37 In contrast, women with limited social support or social isolation may experience reduced motivation to engage in screening due to lack of encouragement and reinforcement.38
Education
Education and schooling strongly influence adherence to cervical cancer screening. Lower educational attainment is associated with reduced participation, likely reflecting disparities in health literacy and access to accurate information. Evidence shows that women with limited formal education are significantly less likely to undergo screening compared with those with higher educational levels.39 Higher health literacy mediates the relationship between education and screening participation by enabling informed decision-making and engagement with preventive health services.40,41
Consequences
Consequences refer to outcomes that arise as a result of the concept.21 Adherence to HPV screening has important implications for health outcomes, complications, and healthcare costs.
Improving Health
The primary objective of screening is to improve patient-relevant health outcomes rather than simply identify disease.42 HPV-based screening facilitates early detection and management of precancerous lesions, contributing to reduced cervical cancer incidence and mortality, particularly when combined with effective health education.43
Reducing Complications
Adherence to screening recommendations enables timely identification of cervical abnormalities and early intervention, thereby preventing disease progression and reducing treatment-related complications.44
Reducing Costs
From a health system perspective, adherence to screening generates substantial cost savings by preventing advanced disease requiring complex and expensive treatment. Cost-effectiveness analyses demonstrate that HPV-based screening programmes reduce long-term healthcare expenditures while improving survival outcomes.45
Moderators and Mediators
Identifying moderators and mediators is essential to understanding the mechanisms and contextual conditions influencing adherence behaviours. Moderators identified included age, gender, and healthcare professionals, while mediators included anxiety, fear, and perceived lack of need.
Age-related differences in HPV epidemiology and screening recommendations may shape adherence patterns.18 Gendered communication has historically framed HPV as a women’s issue, despite high HPV prevalence among men and the role of men as reservoirs of infection.46 Gender-diverse populations may face additional barriers to screening, including discomfort with conventional procedures and limited availability of inclusive services.47
Healthcare professionals play a central moderating role. Clear recommendations, effective communication, and continuity of care are consistently associated with higher screening adherence.20 Anxiety and fear - particularly following abnormal results - can mediate adherence by discouraging future participation if not appropriately addressed.48
Discussion
Although the reviewed studies consistently highlighted similar determinants of screening behaviour, important variations emerged in how adherence was conceptualized and operationalized across settings. In particular, some studies defined adherence as a single screening event, whereas others conceptualized it as sustained engagement across the entire screening and follow-up pathway. These inconsistencies reinforce the need for a unified conceptual framework capable of integrating behavioural, psychosocial, and health system determinants.
Implication for Midwifery and Nursing
The concept analysis of adherence to HPV screening clarified the theoretical and operational elements of this construct, highlighting its complexity and multidimensional nature (Figure 2). A clear and consistent understanding of adherence is essential for nurses and midwives, who play a central role in designing and implementing strategies aimed at addressing barriers to screening participation, supporting informed decision-making, and encouraging sustained engagement in screening programs. Midwives and nurses are optimally positioned to advocate for individuals eligible for screening.
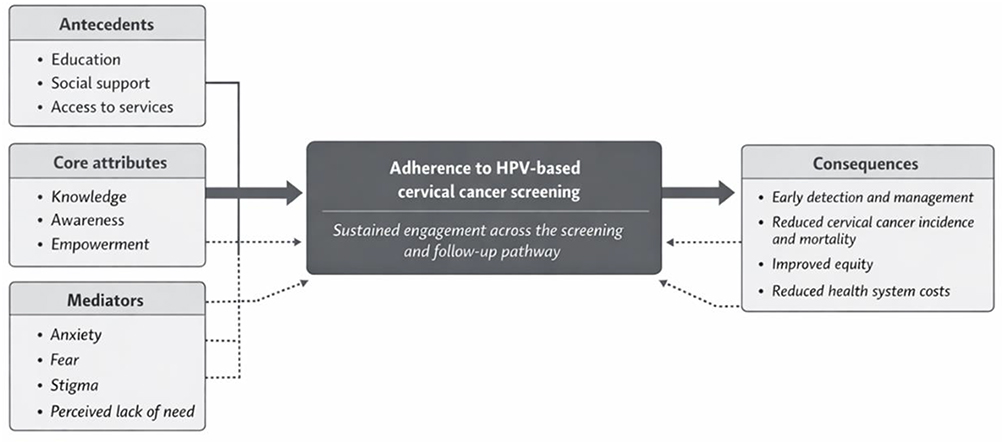 |
Figure 2 Conceptual framework of adherence to HPV-based cervical cancer screening showing antecedents, defining attributes, mediators, and consequences influencing sustained engagement across the screening pathway. Solid arrows represent the primary conceptual pathway linking antecedents and core attributes to adherence to HPV-based cervical cancer screening and its consequences. Dotted arrows indicate indirect or contextual influences, highlighting mediating factors that may facilitate or hinder adherence along the screening and follow-up pathway. |
Midwives and nurses can improve adherence to cervical cancer screening through direct patient interaction, culturally sensitive communication, and targeted educational interventions: community-based education has been shown to increase cervical cancer screening participation from 3.2% to 67.6% in target populations.49 These healthcare professionals frequently represent the primary - and sometimes the only - point of contact for women accessing reproductive healthcare.50 Their role in counselling, promoting, and directly implementing screening processes is therefore crucial in mitigating barriers that lead to inadequate adherence.
Midwives are the specialists tasked with educating and supporting women involved in screening initiatives. Beyond the technical execution of the screening procedure, it is essential that women understand how participation contributes to their own health and to broader public health outcomes. Midwives often maintain close relationships with women and families and therefore play an important role in the entire counselling process. Strengthening the role of midwives in the prevention of HPV-related infections may contribute to improved screening uptake.51 Training midwives to perform adequate sample collection for cervical cancer screening may also challenge prevailing perceptions that restrict this task to physicians, promoting a more inclusive distribution of screening responsibilities.52 Certified nurse-midwives have successfully integrated cervical cancer screening into their practice, demonstrating that appropriate training and certification can enable nurses to deliver high-quality preventive care. The expansion of these roles is particularly relevant in areas with limited physician availability, where task-sharing approaches may substantially increase population coverage.53 Moreover, midwives’ knowledge of cervical cancer prevention has been associated with increased participation in screening programmes.54
Providing nurses and midwives with up-to-date knowledge of HPV screening methods, together with appropriate tools and clinical guidelines, is essential for effective implementation of these tests. This combined emphasis on education and resource allocation enables midwives and nurses to perform screening activities with greater confidence, thereby enhancing adherence.55 Ultimately, health systems that prioritize nurse-led screening initiatives are likely to achieve higher participation rates and contribute to reductions in cervical cancer incidence.55 Compared with existing conceptual models of screening adherence in preventive health literature, recent studies have emphasized the role of multidimensional determinants influencing participation in preventive screening programs. For example, recent research has highlighted how behavioural, social, and health system factors interact to shape adherence to preventive screening pathways. While these approaches contribute to understanding participation in preventive care, the framework proposed in this concept analysis specifically conceptualizes adherence within HPV-based cervical cancer screening as a longitudinal process that includes initiation, follow-up, and sustained participation over time.56
The conceptual framework proposed in this study may also support the development of practical assessment tools for use in primary care settings. For example, the defining attributes, antecedents, and mediators identified in this concept analysis could be translated into structured checklists or brief assessment instruments to help nurses and midwives identify barriers to screening adherence during routine consultations. Such tools could guide targeted counselling strategies addressing knowledge gaps, perceived risk, emotional barriers, and access to services. Addressing emotional barriers such as anxiety and fear is also essential for improving adherence to cervical cancer screening. Evidence suggests that nurse- and midwife-led counselling strategies can mitigate these barriers through clear risk communication, empathetic dialogue, and the use of tailored educational materials. Practical approaches may include brief motivational interviewing techniques, reassurance regarding the screening procedure, normalization of screening-related concerns, and structured follow-up reminders. These strategies can help women better understand the purpose of screening, reduce uncertainty related to test results, and increase confidence in participating in recommended screening pathways.
Future research should focus on the empirical validation and operationalization of this framework in clinical practice. In particular, further studies are needed to explore adherence barriers and facilitators among gender-diverse populations, including transgender and non-binary individuals eligible for cervical cancer screening, who remain underrepresented in the current literature.
Compared with existing adherence models in cancer screening literature, which often focus primarily on initial uptake, the framework proposed in this study emphasizes adherence as a longitudinal process encompassing initiation, follow-up, and continued participation over time. By integrating behavioural, contextual, and health system determinants, this model provides a more comprehensive representation of adherence within HPV-based screening pathways.
Limitations and Strengths
This concept analysis has several limitations. First, the available literature on adherence to HPV-based and Pap-based cervical cancer screening remains fragmented, with limited integration of quantitative and qualitative evidence. In addition, no formal methodological quality appraisal of the included publications was conducted, as the primary aim of this concept analysis was conceptual clarification rather than evidence synthesis. Although this approach is consistent with Walker and Avant’s methodological framework, the absence of a structured quality assessment may limit the ability to evaluate the methodological robustness of the studies informing the identified attributes and antecedents. Another limitation concerns the limited representation of gender-diverse populations in the existing literature, which constrains a comprehensive understanding of adherence across the full spectrum of individuals eligible for cervical cancer screening. Addressing this gap represents an important priority for future research.
Despite these limitations, a key strength of this study lies in the comprehensive synthesis of existing definitions and operational approaches to adherence. By integrating conceptual, behavioural, and contextual dimensions, this analysis proposes a unified framework that may support more consistent measurement, facilitate research translation, and inform service planning in cervical cancer prevention.
Conclusion
Measuring adherence to HPV screening is essential for understanding its epidemiology and for designing effective cervical cancer prevention strategies. Adherence is shaped by interacting individual, psychosocial, and system-level factors, including health literacy, access to services, and quality of patient–provider interactions. By clarifying defining attributes, antecedents, moderators, mediators, and consequences, this concept analysis provides a theoretically grounded framework that may support the development of targeted interventions and standardized assessment tools. Future research should focus on the empirical validation of the proposed framework and on examining adherence across diverse clinical, gender, and sociocultural contexts.
Beyond its conceptual contribution, the proposed framework may also inform policy and programme development aimed at improving the effectiveness and equity of cervical cancer screening initiatives. By supporting more consistent measurement of adherence and guiding targeted interventions, this framework may contribute to reducing disparities in screening participation and strengthening population-level prevention strategies.
Acknowledgments
The authors would like to thank the members of the research group for their valuable intellectual input, constructive discussions, and ongoing support throughout the development of this manuscript. Their interdisciplinary perspectives and collaborative engagement contributed meaningfully to the conceptual refinement of this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kobayashi O, Kamata S, Okuma Y, et al. Carcinogenesis and epidemiology of cervical cancer: the hallmark of human papillomavirus-associated cancer. J Obstet Gynaecol Res. 2024;50(Suppl 1):25–11. doi:10.1111/jog.15997
2. World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem; 2020.
3. Ashique S, Hussain A, Fatima N, et al. HPV pathogenesis, various types of vaccines, safety concern, prophylactic and therapeutic applications to control cervical cancer, and future perspective. Virusdisease. 2023;34(2):1–19. doi:10.1007/s13337-023-00824-z
4. Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health. 2016;4(7):e453–63. Erratum in: Lancet Glob Health. 2017 Jul;5(7)e662doi: 10.1016/S2214-109X(17)30186-9. doi:10.1016/S2214-109X(16)30099-7
5. Tatar O, Thompson E, Naz A, et al. Factors associated with human papillomavirus (HPV) test acceptability in primary screening for cervical cancer: a mixed methods research synthesis. Prev Med. 2018;116:40–50. doi:10.1016/j.ypmed.2018.08.034
6. Akgör U, Temiz BE, Gültekin M. Prevention of gynecological cancers: cervical cancer screening in Turkey: a role model for the world. Curr Opin Obstet Gynecol. 2025;37(1):30–36. doi:10.1097/GCO.0000000000000998
7. Lew JB, Simms K, Smith M, et al. Effectiveness modelling and economic evaluation of primary HPV screening for cervical cancer prevention in New Zealand. PLoS One. 2016;11(5):e0151619. doi:10.1371/journal.pone.0151619
8. Goldstein A, Gersh M, Skovronsky G, Moss C. The future of cervical cancer screening. Int J Womens Health. 2024;16:1715–1731. doi:10.2147/IJWH.S474571
9. Paolino M, Gago J, Pera AL, et al. Adherence to triage among women with HPV-positive self-collection: a study in a middle-low income population in Argentina. Ecancermedicalscience. 2020;14:1138. doi:10.3332/ecancer.2020.1138
10. Buick C, Murphy KJ, Howell D, Metcalfe K. Understanding the role of oncogenic human papillomavirus (HPV) status on adherence behaviors among women with abnormal cervical cytology. BMC Womens Health. 2021;21(1):29. doi:10.1186/s12905-020-01168-2
11. Costa JM, Pimentel AL, Duarte I, et al. Barriers to cervical cancer screening: a cross-sectional study of non-adherent Portuguese women. BMC Prim Care. 2025;26(1):406. doi:10.1186/s12875-025-03121-4
12. Murtas M, Rolland-Guillard L, Hu K, et al. Autoprélèvement HPV et dépistage du cancer du col utérin [HPV self-sampling and cervical cancer screening]. Rev Med Suisse. 2025;21(935):1827–1831. French. doi:10.53738/REVMED.2025.21.935.47907
13. Rosato I, Dalla Zuanna T, Tricarico V, et al. Adherence to cervical cancer screening programs in migrant populations: a systematic review and meta-analysis. Int J Environ Res Public Health. 2023;20(3):2200. doi:10.3390/ijerph20032200
14. Bilalaga MM, Gaddipati G, Devkota A, et al. HPV knowledge and non-adherence to cervical cancer screening before and following the COVID-19 pandemic in the United States. PLOS Glob Public Health. 2025;5(9):e0004800. doi:10.1371/journal.pgph.0004800
15. Winer RL, Lin J, Anderson ML, et al. Strategies to increase cervical cancer screening with mailed human papillomavirus self-sampling kits: a randomized clinical trial. JAMA. 2023;330(20):1971–1981. doi:10.1001/jama.2023.21471
16. Choi HC, Leung K, Wu JT. Cervical screening among Chinese females in the era of HPV vaccination: a population-based survey on screening uptake and regular screening following an 18-year organized screening program. J Gynecol Oncol. 2024;35(2):e20. doi:10.3802/jgo.2024.35.e20
17. Shin M. Understanding over- and under-screening of cervical cancer among a national sample of commercially insured women: implications for health equity. JCO Oncol Pract. 2023;19(Suppl 11):451. doi:10.1200/OP.2023.19.11_suppl.451
18. Kim J, Dove MS, Dang JHT. Sociodemographic factors associated with HPV awareness/knowledge and cervical cancer screening behaviors among caregivers in the U.S. BMC Womens Health. 2022;22(1):335. doi:10.1186/s12905-022-01918-4
19. Christy SM, Winger JG, Mosher CE. Does self-efficacy mediate the relationships between social-cognitive factors and intentions to receive HPV vaccination among young women? Clin Nurs Res. 2019;28(6):708–725. doi:10.1177/1054773817741590
20. Peterson CE, Silva A, Goben AH, et al. Stigma and cervical cancer prevention: a scoping review of the U.S. literature. Prev Med. 2021;153:106849. doi:10.1016/j.ypmed.2021.106849
21. Walker L, Avant K. Strategies for Theory Construction in Nursing.
22. Bennett JA. Mediator and moderator variables in nursing research: conceptual and statistical differences. Res Nurs Health. 2000;23(5):415–420. doi:10.1002/1098-240x(200010)23:5<415::aid-nur8>3.0.co;2-h
23. Kew GS, Koh CJ. Strategies to improve persistent adherence in colorectal cancer screening. Gut Liver. 2020;14(5):546–552. doi:10.5009/gnl19306
24. Chubak J, Hubbard R. Defining and measuring adherence to cancer screening. J Med Screen. 2016;23(4):179–185. doi:10.1177/0969141316630766
25. Vernon SW. Participation in colorectal cancer screening: a review. J Natl Cancer Inst. 1997;89(19):1406–1422. doi:10.1093/jnci/89.19.1406
26. Shin MB, Axeen S, Cole AM, et al. Nonadherence to cervical cancer screening guidelines in commercially Insured US Adults, 2013-2021. JAMA Network Open. 2025;8(12):e2548512. doi:10.1001/jamanetworkopen.2025.48512
27. Garrido CO, Coşkun RA, Lent AB, et al. Use of cervical cancer preventive services among US women aged 21-29: an assessment of the 2010 Affordable Care Act rollout through 2018. Cancer Causes Control. 2020;31(9):839–850. doi:10.1007/s10552-020-01325-w
28. Akinwumiju A, Amadi I, Ishola F, et al. Human papillomavirus (HPV) and HPV vaccine awareness among US adults with depression and anxiety: a nationally representative analysis using Health Information National Trends Survey (HINTS) data. Cureus. 2025;17(10):e95218. doi:10.7759/cureus.95218
29. Öztaş H G, Işik K. The effect of cervical cancer education given to women in Turkey on knowledge, attitudes, and health beliefs: a randomized controlled study. Public Health Nurs. 2025;42(1):363–373. doi:10.1111/phn.13456
30. Ogden SN, Leskinen EA, Sarma EA, et al. Effects of message framing on cervical cancer screening knowledge and intentions related to primary HPV testing. Cancer Prev Res. 2021;14(9):839–844. doi:10.1158/1940-6207.CAPR-20-0622
31. Waller J, Waite F, Marlow L. Awareness and knowledge about HPV and primary HPV screening among women in Great Britain: an online population-based survey. J Med Screen. 2024;31(2):91–98. doi:10.1177/09691413231205965
32. Oketch SY, Kwena Z, Choi Y, et al. Perspectives of women participating in a cervical cancer screening campaign with community-based HPV self-sampling in rural western Kenya: a qualitative study. BMC Womens Health. 2019;19(1):75. doi:10.1186/s12905-019-0778-2
33. Rosser JI, Njoroge B, Huchko MJ. Changing knowledge, attitudes, and behaviors regarding cervical cancer screening: the effects of an educational intervention in rural Kenya. Patient Educ Couns. 2015;98(7):884–889. doi:10.1016/j.pec.2015.03.017
34. Ginjupalli R, Mundaden R, Choi Y, et al. Developing a framework to describe stigma related to cervical cancer and HPV in western Kenya. BMC Womens Health. 2022;22(1):39. doi:10.1186/s12905-022-01619-y
35. Vahabi M, Mishra G, Pimple S, et al. Effectiveness of family-centred sexual health education and HPV self-sampling in promoting cervical cancer screening among hard-to-reach indian women in rural and tribal areas: a community-based pilot study. BMC Public Health. 2023;23(1):671. doi:10.1186/s12889-023-15602-1
36. Foster S, Carvallo M, Song H, Lee J, Lee J. When culture and health collide feminine honor endorsement and attitudes toward catch-up HPV vaccinations in college women. J Am Coll Health. 2023;71(5):1454–1462. doi:10.1080/07448481.2021.1935970
37. Gillies C, Allen-Scott LK, Nykiforuk CIJ, et al. Social capital interventions for human papillomavirus (HPV) immunization and cervical cancer screening: a rapid review. Can Commun Dis Rep. 2024;50(7–8):260–273. doi:10.14745/ccdr.v50i78a04
38. Moudatsou MM, Kritsotakis G, Alegakis AK, et al. Social capital and adherence to cervical and breast cancer screening guidelines: a cross-sectional study in rural Crete. Health Soc Care Community. 2014;22(4):395–404. doi:10.1111/hsc.12096
39. Parikh S, Brennan P, Boffetta P. Meta-analysis of social inequality and the risk of cervical cancer. Int J Cancer. 2003;105(5):687–691. doi:10.1002/ijc.11141
40. Johnson NL, Head KJ, Scott SF, Zimet GD. Persistent disparities in cervical cancer screening uptake: knowledge and sociodemographic determinants of Papanicolaou and human papillomavirus testing among women in the United States. Public Health Rep. 2020;135(4):483–491. doi:10.1177/0033354920925094
41. Kim K, Han HR. Potential links between health literacy and cervical cancer screening behaviors: a systematic review. Psychooncology. 2016;25(2):122–130. doi:10.1002/pon.3883
42. Bell NR, Grad R, Dickinson JA, et al. Better decision making in preventive health screening: balancing benefits and harms. Can Fam Physician. 2017;63(7):521–524.
43. Sumarmi S, Hsu YY, Cheng YM, Lee SH. Factors associated with the intention to undergo Pap smear testing in the rural areas of Indonesia: a health belief model. Reprod Health. 2021;18(1):138. doi:10.1186/s12978-021-01188-7
44. Watson M, Benard V, King J, et al. National assessment of HPV and Pap tests: changes in cervical cancer screening, National Health Interview Survey. Prev Med. 2017;100:243–247. doi:10.1016/j.ypmed.2017.05.004
45. Mandelblatt JS, Lawrence WF, Gaffikin L, et al. Costs and benefits of different strategies to screen for cervical cancer in less-developed countries. J Natl Cancer Inst. 2002;94(19):1469–1483. doi:10.1093/jnci/94.19.1469
46. Bruni L, Albero G, Rowley J, et al. Global and regional estimates of genital human papillomavirus prevalence among men: a systematic review and meta-analysis. Lancet Glob Health. 2023;11(9):e1345–e1362. doi:10.1016/S2214-109X(23)00305-4
47. Peitzmeier SM, Agénor M, Bernstein IM, et al. “It can promote an existential crisis”: factors influencing Pap test acceptability and utilization among transmasculine individuals. Qual Health Res. 2017;27(14):2138–2149. doi:10.1177/1049732317725513
48. Maissi E, Marteau TM, Hankins M, et al. The psychological impact of human papillomavirus testing in women with borderline or mildly dyskaryotic cervical smear test results: 6-month follow-up. Br J Cancer. 2005;92(6):990–994. doi:10.1038/sj.bjc.6602411
49. Nisha M, Bateson D, Saville M, et al. The role of non-medical providers in increasing access to cervical screening: a scoping review. BMJ Glob Health. 2025;10(8):e019041. doi:10.1136/bmjgh-2025-019041
50. Morse RM, Brown J, Ríos López EJ, et al. Challenges associated with follow-up care after implementation of an HPV screen-and-treat program with ablative therapy for cervical cancer prevention. BMC Public Health. 2024;24(1):2121. doi:10.1186/s12889-024-19436-3
51. Stoyanova E, Kamburova M, Minerva E. Confidence in midwives in prevention of HPV-associated diseases in Bulgaria. Popul Med. 2023;5(Supplement):A1815. doi:10.18332/popmed/165376
52. Mutyaba T, Mmiro FA, Weiderpass E. Knowledge, attitudes and practices on cervical cancer screening among the medical workers of Mulago Hospital, Uganda. BMC Med Educ. 2006;6:13. doi:10.1186/1472-6920-6-13
53. Murphy PA, Schwarz EB, Dyer JM. Cervical cancer screening practices of certified nurse-midwives in the United States. J Midwifery Womens Health. 2008;53(1):11–18. doi:10.1016/j.jmwh.2007.06.014
54. Tchounga BK, Jaquet A, Coffie PA, et al. Cervical cancer prevention in reproductive health services: knowledge, attitudes and practices of midwives in Côte d’Ivoire, West Africa. BMC Health Serv Res. 2014;14:165. doi:10.1186/1472-6963-14-165
55. Kress CM, Sharling L, Owen-Smith AA, et al. Knowledge, attitudes, and practices regarding cervical cancer and screening among Ethiopian health care workers. Int J Womens Health. 2015;7:765–772. doi:10.2147/IJWH.S85138
56. Terrinoni M, Golia D’Augè T, Mascellino G, et al. Human papillomavirus across the reproductive lifespan: an integrative review of fertility, pregnancy outcomes, and fertility-sparing management. Medicina. 2025;61(8):1499. doi:10.3390/medicina61081499
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient and Staff Satisfaction and Experience While Transforming Health Center Systems
Whelihan K, Modica C, Bay RC, Lewis JH
Risk Management and Healthcare Policy 2022, 15:2115-2124
Published Date: 11 November 2022
Disparities in Healthcare-Seeking Behavior and Decision Preference Among Hispanics: A Comparative Study Across Races/Ethnicities, SES, and Provider Types
Lin C, Mella-Velazquez A, Braund WE, Tu P
Journal of Multidisciplinary Healthcare 2024, 17:3849-3862
Published Date: 8 August 2024
The Impact of Patients’ Engagement in the Prevention of Surgical Site Infections: A Systematic Review
A’aqoulah A, Alomran MF, Alhumaid N, El-Metwally A, Kalmey F
Infection and Drug Resistance 2025, 18:5761-5770
Published Date: 6 November 2025
The Paradox of Education and the Failure of Communication: A Cross-Sectional Study of Topical Corticosteroid Phobia and Its Impact on Treatment Adherence Among Urban Primary Care Patients in Shenzhen, China
Huang J, Chen W, Ma L, Wen Z, Shi M, Hong F, Hou S
Patient Preference and Adherence 2026, 20:584646
Published Date: 25 March 2026