Back to Journals » Infection and Drug Resistance » Volume 19
Acute Q Fever in an Elderly Traveler with Multiple Comorbidities Diagnosed by Blood mNGS and Resolved with Omadacycline
Authors Li JZ ![]() , Guan SY, Zhang JF
, Guan SY, Zhang JF ![]() , Zheng JN
, Zheng JN
Received 18 March 2026
Accepted for publication 23 May 2026
Published 29 May 2026 Volume 2026:19 610202
DOI https://doi.org/10.2147/IDR.S610202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Ju-Zhang Li,1,* Si-Yao Guan,2,* Jian-Feng Zhang,1 Jiang-Nan Zheng1
1Department of Respiratory and Critical Care Medicine, Suzhou Ninth Hospital Affiliated to Soochow University (Suzhou Ninth People’s Hospital), Suzhou, People’s Republic of China; 2Department of Anesthesiology, Suzhou Ninth Hospital Affiliated to Soochow University (Suzhou Ninth People’s Hospital), Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian-Feng Zhang, Department of Respiratory and Critical Care Medicine, Suzhou Ninth Hospital Affiliated to Soochow University (Suzhou Ninth People’s Hospital), 2666 Ludang Road, Wujiang District, Suzhou, 215200, People’s Republic of China, Email [email protected] Jiang-Nan Zheng, Department of Respiratory and Critical Care Medicine, Suzhou Ninth Hospital Affiliated to Soochow University (Suzhou Ninth People’s Hospital), 2666 Ludang Road, Wujiang District, Suzhou, 215200, People’s Republic of China, Email [email protected]
Abstract: This article reports a case of acute Q fever in a 61-year-old man. The patient mainly presented with high fever and cough. Extensive multi-system investigations failed to identify an etiology. On the fourth day of admission, the diagnosis of acute Q fever was confirmed by rapid detection of Coxiella burnetii nucleic acid sequence by blood metagenomic Next-Generation Sequencing (mNGS). With the treatment of intravenous omadacycline, the fever was controlled within 24 hours and the clinical symptoms significantly improved. Subsequent sequential therapy with oral doxycycline was administered, and the patient was discharged successfully. This case highlights the value of mNGS in the rapid diagnosis of rare or zoonotic pathogens in patients with fever of unknown origin, especially in patients with potential exposure to endemic areas. Furthermore, the novel tetracycline antibiotic omadacycline, demonstrating favorable efficacy and safety despite the patient’s liver dysfunction, offers a valuable treatment option for rapid control of acute Q fever symptoms, especially in severe cases or those intolerant to doxycycline.
Keywords: Coxiella burnetii, next-generation sequencing, omadacycline, Q fever, zoonosis
Background
Q fever, caused by Coxiella burnetii, is an important global zoonosis. Inhalation of contaminated aerosols is the main mode of Coxiella burnetii infection in humans.1,2 Given the high infectivity and environmental resistance of Coxiella burnetii, the Centers for Disease Control and Prevention (CDC) in the USA has classified it as a category B potential bioterrorism agent.3 Q fever remains underappreciated, underreported, and understudied in many regions worldwide.1,4,5 Although often underrecognized, acute Q fever can lead to significant morbidity, including severe pneumonia and hepatitis. Approximately 1–5% of cases may progress to chronic Q fever, primarily presenting as endocarditis, with some investigations reporting this proportion exceeding 10%,2,6 which is associated with high mortality and long-term disability. Q fever imposes a considerable public health burden in endemic regions. The economic costs of Q fever include direct medical expenses for diagnosis, hospitalization, and prolonged antibiotic therapy, as well as indirect costs from lost productivity and disability. In outbreak settings, such as the large epidemic in the Netherlands (2007–2010), the societal impact was substantial, with over 4000 reported cases and enormous expenditures on healthcare, livestock culling, and public health interventions.7 As highlighted by the World Health Organization, the large-scale epidemics in Europe underscore Q fever’s potential to become a major public health concern.5,7 Despite evidence of widespread seropositivity in China (estimated 10% population exposure),8 Q fever is currently not recognized as a notifiable disease in China and receives little attention. Raising awareness of Q fever among clinicians and public health authorities is therefore essential to improve diagnosis, reduce chronic complications, and implement cost-effective surveillance strategies.
Doxycycline is the first-line treatment for Q fever. Early diagnosis is crucial for patients to receive targeted anti-infective therapy and achieve better prognoses. However, Coxiella burnetii is a highly infectious obligate intracellular bacterium requiring biosafety level 3 (BSL-3) conditions for culture, which are not available in most clinical laboratories. Consequently, routine culture and phenotypic antimicrobial susceptibility testing are not feasible in most diagnostic settings and are not recommended in clinical practice. Alternative diagnostic methods, including indirect immunofluorescence assay (IFA), mini/portable qPCR, rapid diagnostic tests (RDTs), and rapid molecular testing, offer more accessible and cost-effective options for initial screening and diagnosis, particularly in resource-limited or remote endemic regions where Q fever is more prevalent. Compared with metagenomic Next-Generation Sequencing (mNGS), these methods are faster, require less infrastructure, and are more suitable for point-of-care testing. With the development of mNGS technology, more rare Coxiella burnetii infections have been identified in recent years. Although equitable access to mNGS remains a concern, it has unique advantages in detecting rare, unexpected, or co‑infecting pathogens without prior hypothesis, making it a valuable complementary tool in complex cases and for diagnosing emerging or rare infectious diseases. Omadacycline, a novel aminomethylcycline antibacterial agent, overcomes the ribosomal protection and efflux mechanisms of tetracycline resistance and has proven to be safe and effective for patients with community-acquired bacterial infection, including infection caused by atypical pathogens.9 However, clinical studies on its effectiveness for acute Q fever remain limited.
We report a case of acute fever of unknown origin in which blood mNGS rapidly confirmed the diagnosis of acute Q fever. The patient showed rapid symptom resolution following treatment with omadacycline and achieved a favorable prognosis. This case aims to illustrate the value of mNGS in the early diagnosis of zoonotic diseases in patients with fever of unknown origin, while also demonstrating the significant therapeutic effect of the novel tetracycline antibiotic omadacycline in acute Q fever, providing an important reference for treatment decisions in acute and severe Q fever cases.
Case
A 61-year-old man was admitted on January 24, 2026, with a 5-day history of cough, expectoration, and fever. He developed a high fever (up to 40°C) accompanied by rigors, myalgia, and headache, without upper respiratory catarrhal symptoms, chest pain, or dyspnea. He reported a recent short-term travel history to Shandong Province, China, but denied any specific tick bites or direct contact with livestock or animals. The patient is a retired factory worker with no occupational exposure to livestock or farming and resides in an urban area (Suzhou, Jiangsu Province, China). He denied any contact with individuals exhibiting similar symptoms, and no unexplained febrile illnesses were reported among his family members, or neighbors during the same period. He had no history of tick bites, raw milk consumption, or direct contact with cattle, sheep, or goats. His working habits had never involved handling animal products or visiting farms. Past medical history included hypertension and dilated cardiomyopathy, managed with sacubitril/valsartan, atorvastatin, and aspirin. He denied diabetes or history of infectious diseases.
Physical examination on admission: temperature 38.9°C, pulse 98 beats/min, respiratory rate 18 breaths/min, blood pressure 122/83 mmHg. He was conscious with clear mentation. No jaundice, petechiae, or rash was observed on the skin and mucosa. No superficial lymphadenopathy was palpable throughout the body. The pharynx was not congested, and tonsils were not swollen. Clear breath sounds were heard in both lungs without dry or moist rales. The heart rate was regular, with no pathological murmurs. The abdomen was soft and non-tender. Neurological examination was unremarkable.
The white blood cell count was normal with elevated neutrophil percentage (78.7%) and a significantly increased C-reactive protein (CRP, 54.25 mg/L). Procalcitonin and erythrocyte sedimentation rate were both within normal range. Liver function tests revealed significant hepatic injury with elevated transaminases (Alanine aminotransferase 131 U/L, Aspartate aminotransferase 100 U/L). Chest CT showed only old pulmonary nodules, linear opacities, and pleural thickening, without signs of consolidation. Cardiac ultrasound did not reveal any valvular vegetations. The abdominal ultrasound demonstrated intrahepatic calcifications, gallbladder polyps, and prostatic hyperplasia, with no additional abnormalities identified. Community-acquired infection was suspected, and empirical therapy with cefoxitin was initiated. However, the patient continued to experience recurrent high fever, with temperatures around 39°C.
Further investigations showed negative in nucleic acid amplification testing on throat swabs (covering COVID-19, influenza viruses A and B, rhinovirus, respiratory syncytial virus, adenovirus, and Mycoplasma pneumoniae). Serological screening for Epstein-Barr virus (EBV) infection, viral hepatitis, and common autoimmune disorders returned negative results. Blood culture showed negative. Microbiological nucleic acid PCR detection of sputum samples revealed Klebsiella pneumoniae, and sputum culture results also confirmed Klebsiella pneumoniae without Extended-Spectrum β-Lactamases. Given the lack of radiological evidence for typical bacterial pneumonia and the poor response to cefoxitin, this bacterium was considered a colonizer or a non-primary pathogenic organism.
Considering the patient’s travel history, along with persistent high fever, hepatic injury, and lack of response to beta-lactam antibiotics, a zoonotic infection was highly suspected. Further differential diagnosis was needed to identify infections caused by pathogens including Rickettsia spp., Brucella spp., Salmonella typhi, and Leptospira spp. However, none of the routine diagnostic assays for these pathogens, including IFA, mini/portable qPCR, or RDTs, were available at our institution. Therefore, on hospital day 3 (January 26, 2026), a blood sample was sent to Dinfectome Inc. (Nanjing, China) for mNGS analysis. On hospital day 4 (January 27, 2026), the mNGS report identified a significant number of specific nucleic acid sequences for Coxiella burnetii (DNA reads: 688, relative abundance 98.01%; RNA reads: 2935, relative abundance 99.8%). DNA and RNA sequencing were performed using independent and parallel workflows. The starting plasma input volume was identical for both DNA and RNA extractions. The read counts presented in the case report represent raw sequencing reads. After normalization according to the total sequencing yield, the standardized read counts for the DNA and RNA pipelines of Coxiella burnetii were 276 and 3830, respectively. For DNA mNGS, the proportions of human, microbial, and unclassified reads were 98.37%, 0.0019%, and 1.63%, respectively. For RNA mNGS, the corresponding proportions were 97.73%, 2.94%, and 2.27%, respectively. All microorganisms detected by mNGS are listed with detailed information in Table 1. The genome coverage map of Coxiella burnetii detected by DNA mNGS is shown in Figure 1. The overall genome coverage was 2.82%. Uniform coverage across the genome supports the specificity and reliability of the mNGS result. Antimicrobial resistance genes were simultaneously analyzed from mNGS data using the Resistance Gene Identifier (RGI) aligned against the Comprehensive Antibiotic Resistance Database (CARD), and no antimicrobial resistance genes were detected. These results strongly supported the diagnosis of acute Q fever. Detailed mNGS procedures have been supplemented in the Supplementary Material 1.
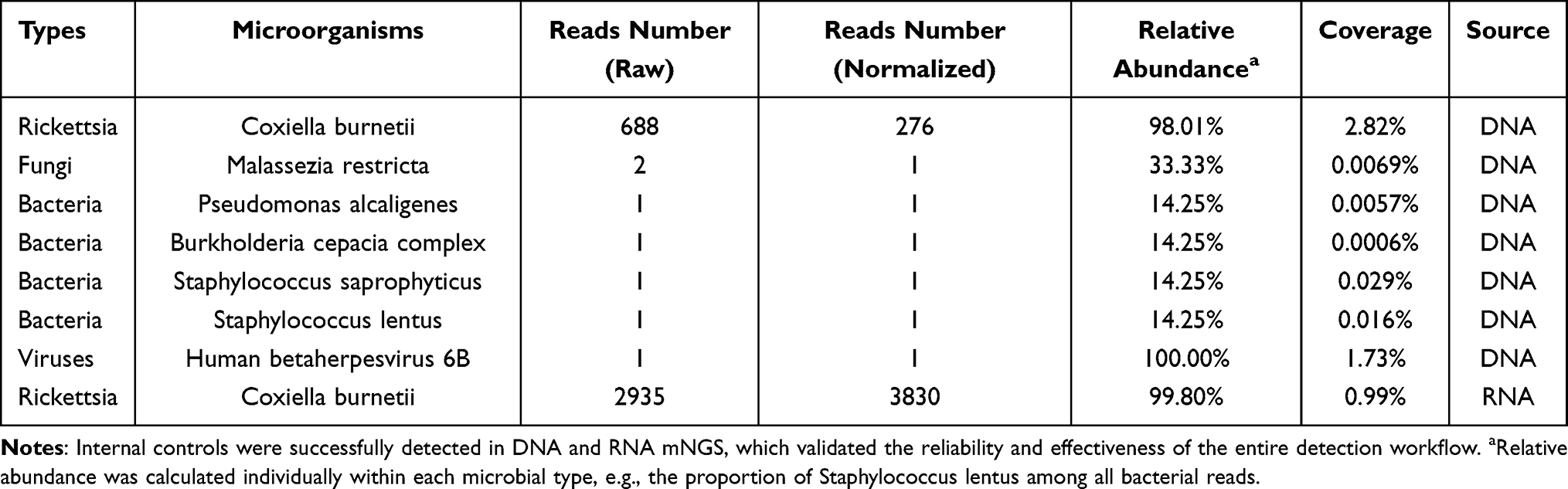 |
Table 1 mNGS Results |
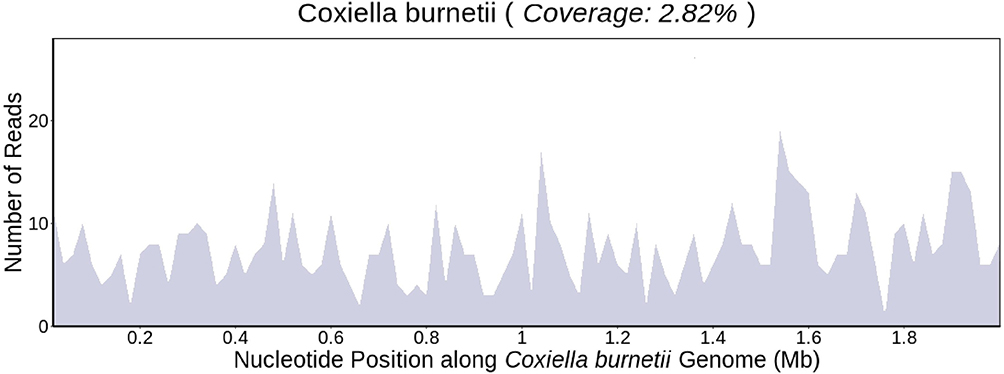 |
Figure 1 Genome coverage map of Coxiella burnetii based on DNA mNGS data. The x‑axis represents the nucleotide position along the Coxiella burnetii genome (in megabases, Mb), and the y‑axis indicates the number of sequencing reads. The blue shaded area illustrates the sequencing coverage across the genome. The overall genome coverage was 2.82%. Uniform coverage across the genome supports the specificity and reliability of the mNGS result. |
Upon confirmation of the diagnosis, cefoxitin was discontinued immediately. Considering the poor condition and abnormal liver function, we modified antibiotic therapy to intravenous omadacycline with a first dose of 200 mg, followed by 100 mg once daily. After switching therapy, the patient’s clinical symptoms (cough, fatigue, myalgia) improved significantly and his body temperature decreased markedly within 24 hours (Figure 2). Follow-up blood tests showed normalization of white blood cell count, decreased neutrophil percentage (43.8%), increased lymphocyte percentage (46.4%), and a significant drop in CRP to 13.34 mg/L. So, therapy was de-escalated from intravenous omadacycline to oral doxycycline for sequential treatment on February 1, 2026, to facilitate discharge. The patient was discharged in good condition on February 2, 2026. Follow-up after discharge confirmed sustained normal body temperature and absence of symptoms. Table 2 shows the laboratory examination during the disease course and follow-up of the patient. Figure 3 summarizes the clinical course of the patient over time.
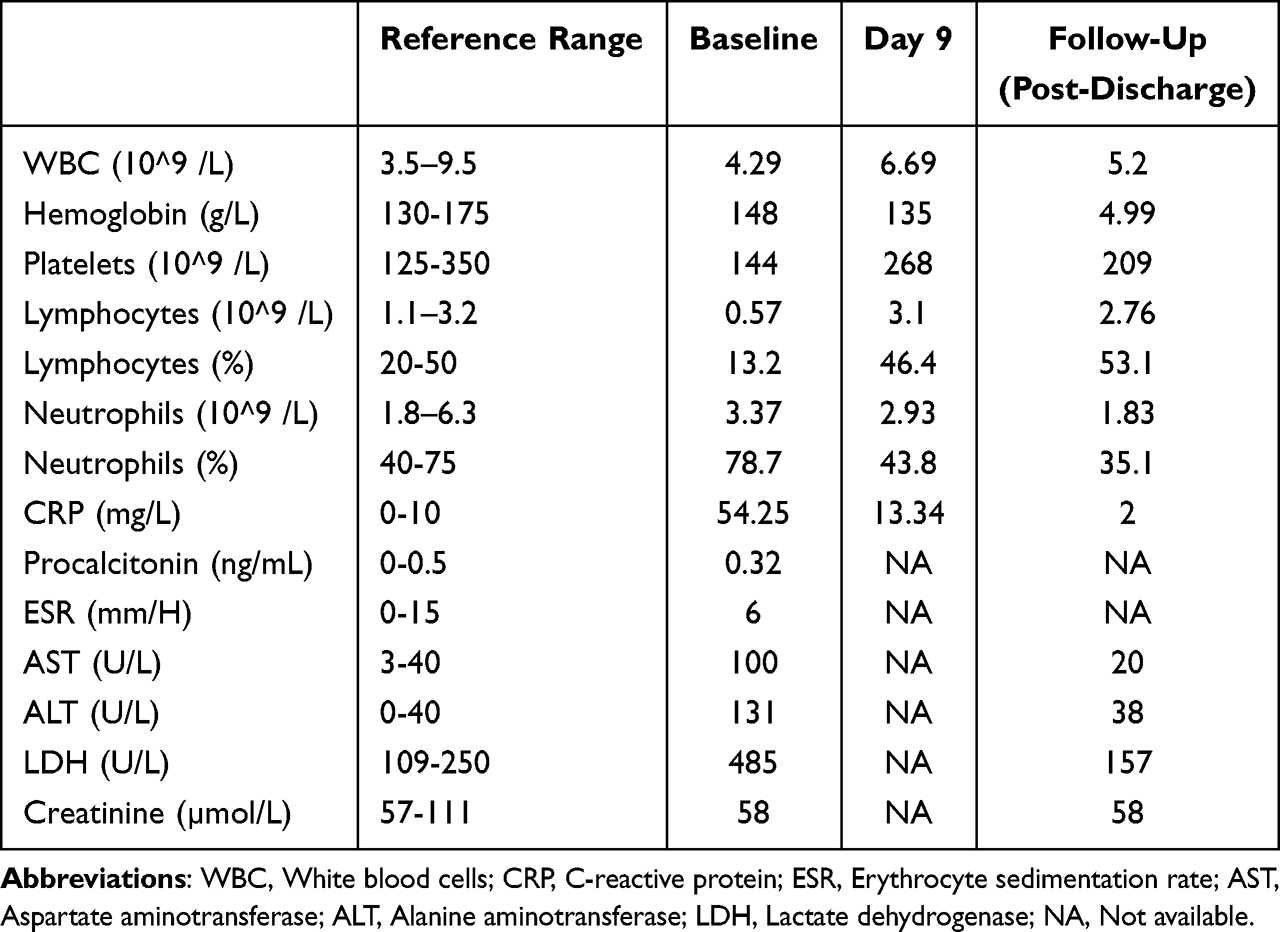 |
Table 2 Changes During Clinical Course of the Patient in the Laboratory Examination |
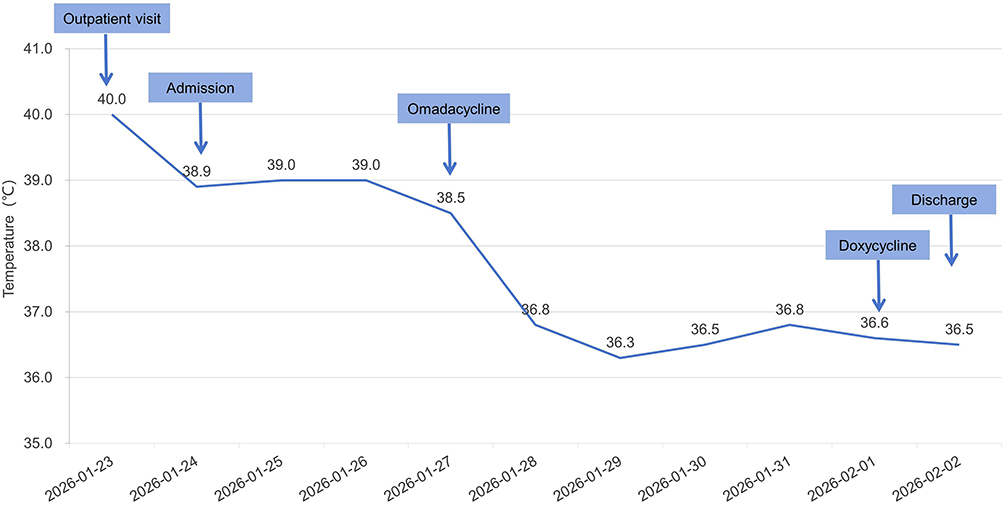 |
Figure 2 Trend of maximum body temperature. |
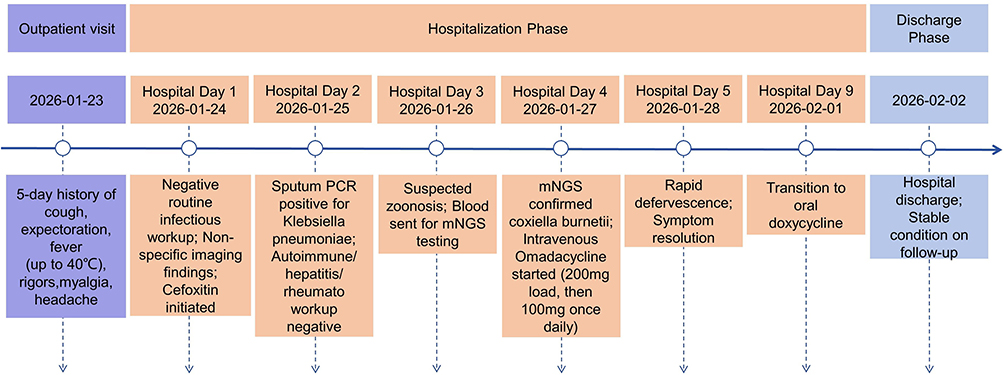 |
Figure 3 The clinical course of the patient with acute Q fever over time. |
Discussion
This case illustrates the successful management of acute Q fever facilitated by rapid diagnosis with mNGS. The patient in this case had a travel history to Shandong Province, an endemic area for several natural-focal diseases. Between 2010 and 2017, Shandong reported an annual average of 3.47 cases per million residents of four major diseases: severe fever with thrombocytopenia syndrome, human granulocytic anaplasmosis, endemic typhus, and scrub typhus, with farmers accounting for over 85% of cases.10 Rickettsial exposure is expected in eastern China due to frequent tick bites.11,12 However, the prevalence of Coxiella burnetii in Shandong remains unclear, and conventional diagnostic kits for Q fever, such as serologic and Coxiella burnetii–specific PCR reagents, are largely unavailable in primary healthcare settings. Rodents, livestock, and ticks serve as reservoirs and vectors for Coxiella burnetii. Infection can occur via aerosol inhalation or tick bites, complicating risk assessment even without direct animal contact.13 Previous reports from Shandong have described both acute and chronic Q fever cases diagnosed by mNGS, including in patients without apparent animal or tick exposure and in urban residents, where routine culture, PCR, or immunoassays failed to identify the pathogen.14,15 These observations highlight the diagnostic challenges of Q fever in China and underscore the value of mNGS for detecting fastidious pathogens when conventional testing is unrevealing.
Acute Q fever often presents as nonspecific fever with or without pneumonia or hepatitis. Traditional diagnosis relies on serology (eg., rise in Phase II antibodies), which has a window period (typically 1–4 weeks post-infection), leading to potential diagnostic delay in early stages.2 In contrast, mNGS has demonstrated excellent diagnostic power in rare and emerging infectious diseases, providing early etiological evidence and enabling timely treatment. In the present case, mNGS enabled rapid confirmation of Coxiella burnetii, overcoming the limitations of serology and guiding timely targeted therapy. However, mNGS cannot reliably distinguish between viable microorganisms and residual genetic material from dead microbes. In our case, both DNA- and RNA-based mNGS detected Coxiella burnetii sequences, with 688 and 2,953 reads, respectively. As Coxiella burnetii is a DNA pathogen, the presence of its RNA reads may suggest active transcription and possible metabolic activity. Nevertheless, this conclusion is tentative, and the ability to differentiate active infection from residual nucleic acids based on RNA read counts requires further validation. Importantly, mNGS was performed within one week of fever onset, before targeted therapy was initiated. The patient’s rapid defervescence and clinical improvement within 24 hours after omadacycline therapy, along with negative imaging for chronic foci (endocarditis), supported acute Q fever.
Doxycycline is the first-line oral agent for acute Q fever. However, intravenous options are limited for severe cases, patients unable to tolerate oral medication, or those requiring rapid symptom control. Omadacycline, a novel intravenous tetracycline-class agent, exhibits a broad spectrum covering atypical pathogens, including rickettsiae.9,16 In this case, switching to intravenous omadacycline resulted in rapid and effective fever control, demonstrating its clinical efficacy. Notably, the patient had liver injury on admission, which was possibly related to prior medications or the infection itself. Omadacycline was used safely and effectively in this context. Compared to doxycycline, omadacycline has fewer reports of significant hepatotoxicity, and its pharmacokinetic profile allows for use without dose adjustment in renal impairment, making it a potentially preferable option for infected patients with hepatic or renal comorbidities.17,18 Therefore, omadacycline can be considered an effective alternative or preferred intravenous regimen for severe Q fever, patients intolerant to oral doxycycline, or those with hepatic/renal impairment.
A recent case report by Nie et al also used NGS (targeted NGS of bronchoalveolar lavage fluid) and omadacycline for Q fever.16 Our case differs in several important ways. First, unlike most previously reported Q fever cases that occurred in farmers, our patient was a retired factory worker with no occupational animal exposure but had a travel history to Shandong Province, a potential endemic area. This highlights that Q fever should be suspected in travelers, even without traditional risk factors. Second, our patient had dilated cardiomyopathy, liver dysfunction, and negative imaging, underscoring the value of unbiased blood mNGS when clinical clues are lacking. Third, this is the first report to simultaneously detect both DNA and RNA reads of Coxiella burnetii from a single blood sample. The presence of RNA reads may indicate active transcription, helping differentiate acute infection from residual nucleic acids, though this finding requires further validation. Fourth, this is the first acute Q fever case diagnosed by blood mNGS in Suzhou, Jiangsu Province. These distinctive features highlight the value of blood mNGS for rapid diagnosis of Q fever in travelers from potential endemic areas, even without direct animal contact. Blood mNGS is non-invasive, unbiased, and can assess pathogen viability when clinical clues are lacking. Omadacycline is a safe and effective alternative to doxycycline in high-risk patients with multiple comorbidities.
Moreover, the present case underscores a broader issue: the lack of awareness of Q fever among medical professionals in China. Despite seroepidemiological evidence of widespread exposure, Q fever is not a notifiable disease and receives little attention in clinical practice. Enhancing medical knowledge about Q fever, including its epidemiology, diverse clinical presentations, and diagnostic options, is essential for timely diagnosis and treatment, thereby preventing chronic complications and reducing unnecessary healthcare costs. Moreover, as a zoonosis with environmental reservoirs, Q fever cannot be effectively controlled by human health measures alone. The One Health approach, which integrates human, animal, and environmental health through multisectoral collaboration, is crucial for the surveillance, prevention, and control of neglected zoonotic diseases.19 Coordinated strategies should include animal surveillance, data sharing between public health and veterinary sectors, strengthening of laboratory infrastructure, and environmental monitoring. Such an approach not only helps prevent Q fever outbreaks but also reduces the overall public health burden of emerging and re‑emerging zoonoses.
Several limitations should be acknowledged. First, we acknowledge that IFA for phase II antibodies is the gold standard for confirming acute Q fever after exclusion of potential differential diagnoses. Serological confirmation was not performed because Coxiella burnetii-specific IFA was unavailable at our institution. Although the clinical presentation and rapid response to therapy strongly support acute Q fever, the lack of reference serology is a limitation. Therefore, while mNGS provided rapid and compelling molecular evidence for Coxiella burnetii infection, the lack of serological confirmation should be interpreted with caution. Future studies would benefit from integrating both molecular and serological methods to enhance diagnostic accuracy for Q fever. Second, based solely on molecular data, we cannot completely rule out prior subclinical exposure instead of acute infection, though the clinical course argues for the latter. Third, for DNA pathogens, while concurrent detection of DNA and RNA reads from blood may suggest active transcription and therefore viable organisms, the RNA threshold required to distinguish active infection from residual microbial material remains unknown. This uncertainty applies to all molecular diagnostics, and our observation should be considered hypothesis‑generating. Fourth, from a public health perspective, unbiased blood mNGS may not be cost‑effective for routine use in non‑endemic areas, and in such settings, targeted NGS (tNGS) combined with IFA may offer a more practical approach. In resource‑limited or remote endemic regions, alternative rapid diagnostic tools (RDTs, mini/portable qPCR, rapid molecular testing) are more accessible and affordable. Finally, as a single case report, our findings require validation in larger studies.
Conclusion
In patients with fever of unknown origin and a history of travel to potential endemic areas (eg., Shandong Province, China), Q fever should be considered. For diagnosis, mNGS enables rapid, unbiased pathogen detection, facilitating early diagnosis and targeted treatment. However, in resource-limited endemic regions, rapid diagnostic tools (RDTs, mini/portable qPCR, rapid molecular testing) are more practical, and in non-endemic areas, tNGS combined with IFA may represent a more cost-effective alternative to unbiased mNGS. For control, raising awareness of Q fever among medical professionals and implementing the One Health approach that integrates human, animal, and environmental surveillance are essential for timely diagnosis, prevention, and control of neglected zoonotic diseases. Regarding treatment, intravenous omadacycline demonstrated good efficacy in rapidly controlling symptoms of acute Q fever, with an acceptable safety profile in patients with hepatic injury, making it a valuable option among therapeutic approaches, especially for severe cases or special patient populations.
Artificial Intelligence Assistance Statement
During the preparation of this article, the authors used ChatGPT (GPT-4) and DeepSeek (DeepSeek-V3.2) for the purposes of language refinement, translation assistance, and grammatical improvement. Following the use of these tools, the authors reviewed and edited the content as needed and take full responsibility for the final version of the manuscript.
Data Sharing Statement
All the data generated or analyzed during this study are available from the corresponding author Jiang-Nan Zheng ([email protected]) on reasonable request.
Statement of Ethics
The study was approved by the Ethics Committee of Suzhou Ninth Hospital Affiliated to Soochow University (Jiangsu, China; Approval No. KYLW2026-031-01). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
We appreciate the mNGS sequencing and interpretation provided by Dinfectome Inc., Nanjing, China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Suzhou Ninth People’s Hospital Youth Research Fund (YK202504, YK202524) and Gusu Health Talent Training Project (GSWS2024066).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jemilehin FO, Okunlade AO, Adesola RO, Obiechefu HC, Ahmed AO. Q fever in the 21st century: uncovering diagnostic, epidemiological, and one health gaps in a re-emerging zoonosis. Res Vet Sci. 2026;201:106060. doi:10.1016/j.rvsc.2026.106060
2. Perez-Arellano JL, Curbelo J, Carranza-Rodriguez C. A comprehensive review of the mechanisms of human Q fever: pathogenesis and pathophysiology. Pathogens. 2025;14(6):589. doi:10.3390/pathogens14060589
3. Anderson A, Bijlmer H, Fournier PE, et al. Diagnosis and management of Q fever--United States, 2013: recommendations from CDC and the Q fever working group. MMWR Recomm Rep. 2013;62(RR–03):1–8.
4. Maki CK, Truong TT, Salzer JS, et al. Coxiella burnetii infections identified by molecular methods, United States, 2006-2023. Emerg Infect Dis. 2025;31(4):861–863. doi:10.3201/eid3104.241214
5. Pustahija T, Medic S, Vukovic V, et al. Epidemiology of Q fever in Southeast Europe for a 20-Year period (2002-2021). J Epidemiol Glob Health. 2024;14(3):1305–1318. doi:10.1007/s44197-024-00288-4
6. El Zein S, Challener DW, Ranganath N, Khodadadi RB, Theel ES, Abu Saleh OM. Acute coxiella burnetii infection: a 10-year clinical experience at a tertiary care center in the United States. Open Forum Infect Dis. 2024;11(6):ofae277. doi:10.1093/ofid/ofae277
7. Eldin C, Melenotte C, Mediannikov O, et al. From Q fever to coxiella burnetii infection: a paradigm change. Clin Microbiol Rev. 2017;30(1):115–190. doi:10.1128/CMR.00045-16
8. El-Mahallawy HS, Lu G, Kelly P, et al. Q fever in China: a systematic review, 1989-2013. Epidemiol Infect. 2015;143(4):673–681. doi:10.1017/S0950268814002593
9. Stets R, Popescu M, Gonong JR, et al. Omadacycline for community-acquired bacterial pneumonia. N Engl J Med. 2019;380(6):
10. Chen R, Kou Z, Xu L, et al. Analysis of epidemiological characteristics of four natural-focal diseases in Shandong Province, China in 2009-2017: a descriptive analysis. PLoS One. 2019;14(8):e0221677. doi:10.1371/journal.pone.0221677
11. Qin XR, Han HJ, Han FJ, et al. Rickettsia japonica and novel rickettsia species in ticks, China. Emerg Infect Dis. 2019;25(5):992–995. doi:10.3201/eid2505.171745
12. Zhang R, Zhao A, Wang X, Zhang Z. Diversity of tick species on domestic animals in Shandong Province, China, using DNA barcoding. Exp Appl Acarol. 2017;73(1):79–89. doi:10.1007/s10493-017-0161-7
13. Zhao GP, Wang YX, Fan ZW, et al. Mapping ticks and tick-borne pathogens in China. Nat Commun. 2021;12(1):1075. doi:10.1038/s41467-021-21375-1
14. Li D, Liu H, Liu M, et al. Delayed diagnosis of acute Q fever, China. Emerg Infect Dis. 2022;28(12):2580–2582. doi:10.3201/eid2812.221118
15. Wang S, Xu K, Wang G. Delayed diagnosis of persistent Q fever: a case series from China. BMC Infect Dis. 2024;24(1):591. doi:10.1186/s12879-024-09484-w
16. Nie C, Zhu Y, Zhou H, et al. Omadacycline in the treatment of severe Q fever pneumonia during an influenza epidemic: a case report with literature review. Front Med. 2025;12:1626115. doi:10.3389/fmed.2025.1626115
17. Zhang A, Sun Y, Zuo M, et al. Physiologically based pharmacokinetic model for predicting omadacycline pharmacokinetics and pharmacodynamics in healthy and hepatic impairment populations. Clin Ther. 2024;46(8):629–635. doi:10.1016/j.clinthera.2024.06.014
18. Berg JK, Tzanis E, Garrity-Ryan L, et al. Pharmacokinetics and safety of omadacycline in subjects with impaired renal function. Antimicrob Agents Chemother. 2018;62(2). doi:10.1128/AAC.02057-17
19. Meurer IR. The importance of medical knowledge about Q fever in the context of timely diagnosis and treatment and the use of the one health approach in combating this and other neglected zoonotic diseases. Infect Drug Resist. 2025;18:5007–5008. doi:10.2147/IDR.S567142
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Coxiellosis in Livestock: Epidemiology, Public Health Significance, and Prevalence of Coxiella burnetii Infection in Ethiopia
Robi DT, Demissie W, Temteme S
Veterinary Medicine: Research and Reports 2023, 14:145-158
Published Date: 18 August 2023
Crescentic Glomerulonephritis and Portal Hypertension with Chronic Q Fever: A Case Report and Comprehensive Literature Review
Yao Y, Zhao H, Lu H, Liu X, Liu H, Fu Z, Li C, Zhou F, Hou W, Shi S
Infection and Drug Resistance 2024, 17:4599-4605
Published Date: 23 October 2024
An Atypical Pneumonia Case of Quinolone-Refractory Chlamydia Pneumoniae Successfully Treated With Omadacycline
Tong J, Zhou L, Chen Y, Xu L, Wang J
Infection and Drug Resistance 2025, 18:2357-2363
Published Date: 7 May 2025
Coxiella burnetii Should Not Be Ignored: Two Cases of Q Fever Pneumonia Diagnosed by Metagenomic Next-Generation Sequencing
Yao J, Zhang J, Zheng L, Fang W, Lang Y
Infection and Drug Resistance 2025, 18:6227-6239
Published Date: 27 November 2025