")
Back to Journals » Cancer Management and Research » Volume 11
Acute myeloid leukemia patient with FLT3-ITD and NPM1 double mutation should undergo allogeneic hematopoietic stem cell transplantation in CR1 for better prognosis
Authors Huang Y, Hu J, Lu T, Luo Y, Shi J, Wu W, Han X, Zheng W, He J, Cai Z, Wei G, Huang H, Sun J
Received 25 November 2018
Accepted for publication 22 March 2019
Published 8 May 2019 Volume 2019:11 Pages 4129—4142
DOI https://doi.org/10.2147/CMAR.S194523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Beicheng Sun
Yan Huang,1–4* Juan Hu,1–4* Ting Lu,1–4 Yi Luo,1–4 Jimin Shi,1–4 Wenjun Wu,1–4 Xiaoyan Han,1–4 Weiyan Zheng,1–4 Jingsong He,1–4 Zhen Cai,1–4 Guoqing Wei,1–4 He Huang,1–4 Jie Sun1–4
1Bone Marrow Transplantation Center,the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310058, People’s Republic of China; 2Institute of Hematology, Zhejiang University, Hangzhou, Zhejiang 310058, People’s Republic of China; 3Zhejiang Province Engineering Laboratory for Stem Cell and Immunity Therapy, Zhejiang University, Hangzhou, Zhejiang 310058, People’s Republic of China; 4Stem Cell Institute, Zhejiang University, Hangzhou, Zhejiang 310058, People’s Republic of China
*These authors contributed equally to this work
Background: According to the recent National Comprehensive Cancer Network (NCCN) guidelines, the risk level in acute myeloid leukemia (AML) patients with FLT3-ITD and NPM1 double mutation (AMLFLT3-ITD+/NPM1+,) depends on the allelic ratio of FLT3-ITD. But despite a low or high allelic ratio of FLT3-ITD, AMLFLT3-ITD+/NPM1+, patients belong to the favorable or intermediate risk, for whom allogeneic stem cell transplantation is not obligated. However, some latest studies pointing out that NPM1 and FLT3-ITD double mutation patients showed an inferior prognosis, which have raised concern about the risk categorization and more effective treatment of AMLFLT3-ITD+/NPM1+, patients.
Methods: A total of 76 patients were selected for coexisting FLT3 and NPM1 mutations with normal cytogenetics. The prognostic risk factors were analyzed, and treatment strategies including allogeneic stem cell transplantati1on and chemotherapy were compared.
Results: In 76 AMLFLT3-ITD+/NPM1+, patients, 36.8% of patients had hyperleukocytosis (HL) and DNMT3A R882 mutation was the most common concomitant gene (23.7%). For 53 patients in the complete remission (CR), 22 had received allogeneic hematopoietic stem cell transplantation (allo-HSCT) on first complete remission (CR1). Patients in transplantation group had better overall survival (OS) and disease-free survival (DFS) than chemotherapy only (P=0.002 and 0.001, respectively). In multivariable Cox model analyses, HL and DNMT3A R882 mutation were independent adverse prognostic factors (all P<0.05) for AMLFLT3-ITD+/NPM1+, patients. Nevertheless, allo-HSCT was an independent good factor of OS and DFS (P=0.001 and 0.000; HR =0.173 and 0.138; 95% CI were 0.062–0.483 and 0.049–0.389). And allo-HSCT could moderately improve the poor prognosis of AML FLT3-ITD+/NPM1+/DNMT3A R882+,.
Conclusion: Although, AMLFLT3-ITD+/NPM1+, patients are categorized as favorable or intermediate risk levels according to recent NCCN and ELN guidelines, these patients should receive allo-HSCT in CR1 for a longer survival. AMLFLT3-ITD+/NPM1+, patients with DNMT3A R882 mutation had a very poor prognosis, and allo-HSCT could moderately improve their survival.
Keywords: FLT3-ITD, NPM1, DNMT3A R882, allo-HSCT
Introduction
FMS-like tyrosine kinase 3 (FLT3) belongs to the receptor tyrosine kinase class III, and is specifically expressed on hematopoietic progenitor cells. FLT3 plays a role in cell survival, proliferation and differentiation of hematopoietic progenitor cells.1 FLT3 gene is one of the most frequently mutated genes in acute myeloid leukemia (AML), and is reported in 25–30% of AML patients.2,3 There are two types of FLT3 mutation, internal tandem duplication of FLT3 (FLT3-ITD) and tyrosine kinase domain of FLT3 (FLT3-TKD). FLT3-ITD is the major type and reported among 20–30% AML patients,4 while FLT3-TKD in only found in about 7% AML patients.5–7 FLT3-ITD is associated with adverse disease features, including high initial peripheral white blood cell (WBC) count, high early recurrence rate and a low overall survival (OS) rate.3,5,8,9 According to NCCN and ELN, FLT3-ITD mutation with normal cytogenetics has a poor risk prognosis. NPM1 is a gene for expression of nucleophosmin, which belongs to nucleophosmin/nucleplasmin family of proteins.10 NPM1 mutations happen in 45–64% adult AML cases.11–14 With normal cytogenetics profile, AML with NPM1 mutation (AMLNPM1+) has a favorable prognosis, but when coexisted with FLT3-ITD, the risk level of AML depends on the allelic ratio (AR) of FLT3-ITD. NPM1 mutation with low AR of FLT3-ITD was considered as favorable-risk group, but when combined with high AR was classified as intermediate-risk group.15 Despite a low or high AR of FLT3-ITD, AMLFLT3-ITD+/NPM1+ patients belong to the favorable or intermediate risk according to the recent NCCN guidelines. These group of patients are not obligated to receive allo-HSCT. However, this risk classification on FLT3-ITD and NPM1 double mutated AML was not accepted by some clinicians, and several studies provided evidence that this type of AML is with unfavorable risks.16–21 What is the optimal treatment for AMLFLT3-ITD+/NPM1+ patients is also under investigation. In this study, we retrospectively analyzed the clinical features and risk factors of AMLFLT3-ITD+/NPM1+, and discussed whether hematopoietic stem cell transplantation is necessary after complete remission (CR).
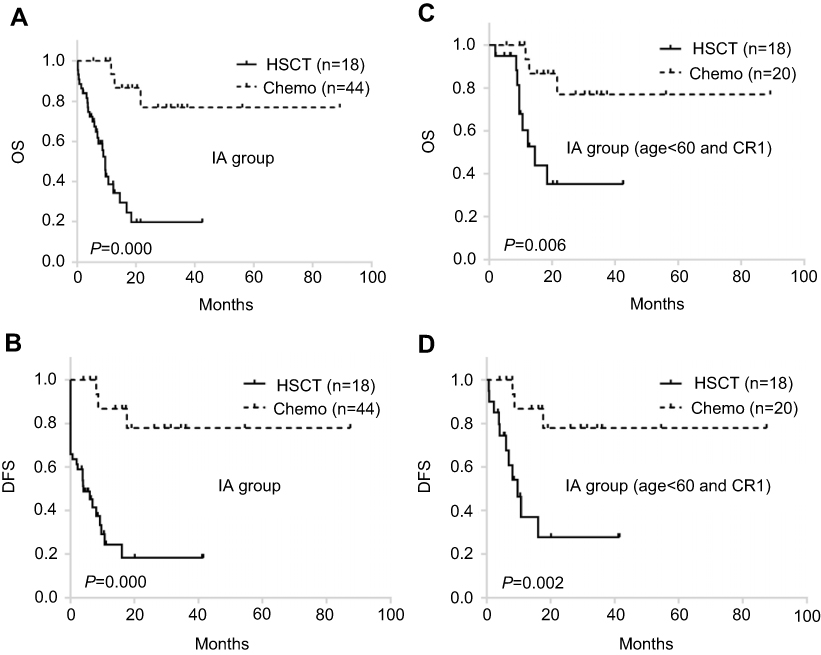 | Figure S1 Comparison of chemotherapy and allo-HSCT in AML FLT3-ITD+/NPM1+ patients received IA as induction regimen. (A, B) OS and DFS of all AML FLT3-ITD+/NPM1+ patients. (C,D) OS and DFS of the AML FLT3-ITD+/NPM1+ patients with age<60 years.Abbreviations: IA, idarubicin and cytarabine; OS, overall survival; DFS, disease-free survival; HSCT, hematopoietic stem cell transplantation; chemo, chemotherapy; |
Material and methods
Patients
We performed an individual patient data-based retrospective analysis of 76 patients evaluated at our hospital between July 2009 and March 2018, who were diagnosed as AML with positive mutation in FLT3-ITD and NPM1. Patients with acute promyelocytic leukemia were excluded. Written informed consent was obtained from all patients. This study was approved by the Human Research Ethics Committee of Zhejiang University. Details, such as patient age and sex, WBC counts at diagnosis, percentage of blast cells in bone marrow, AML French-American-British classification subtypes, karyotype, recurrent fusion genes such as PML-RARa; ETO; CBFβ and combined mutation genes as FLT3-ITD, NPM1, DNMT3A R882,CEBPA, KIT, IDH1/IDH2, TET2; treatment regimens, and response to therapy were reviewed. Hyperleukocytosis (HL) is defined as the peripheral WBC counts is above 100*109/L at diagnosing.
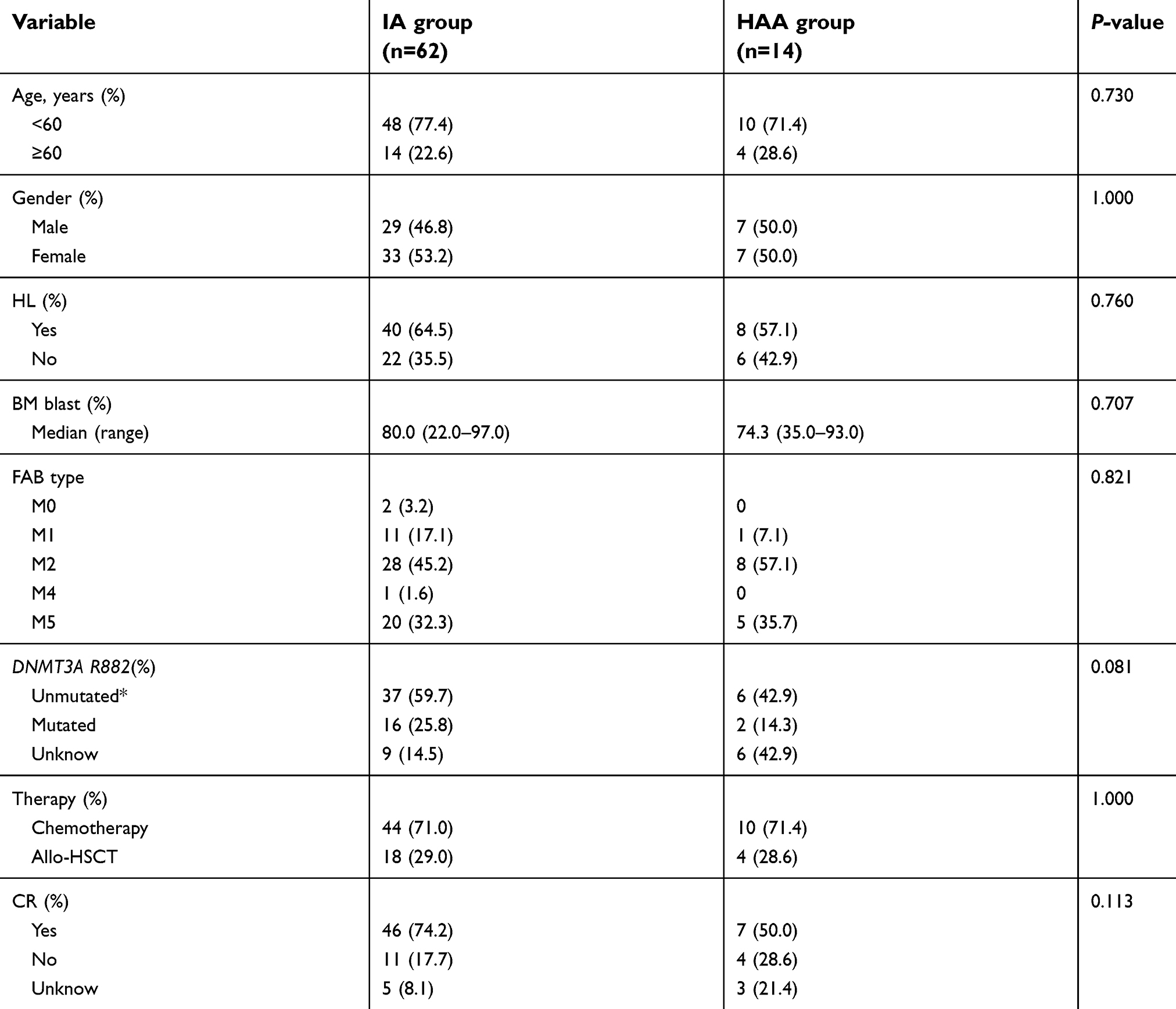
Part of the patients’ data is listed in Table 1.
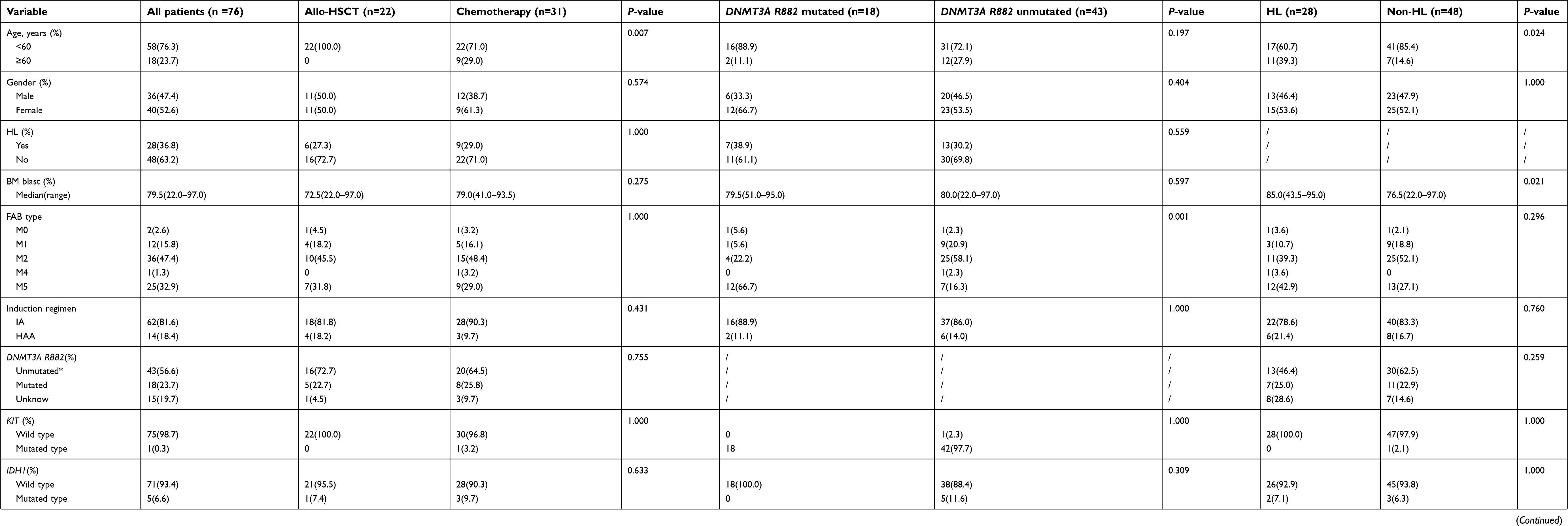
 | Table S1 Biological and clinical characteristics |
 | Table 1 Patients’ characteristics |
Gene mutation analyses
Bone marrow mononuclear cells were isolated and the DNA extracted using a DNA Extraction kit (Invitrogen, Shanghai, People's Republic of China). The forward primer of FLT3-ITD was 5ʹ-GCAATTTAG-GTATGAAAGCCAGC −3ʹ, the reverse primer is 5ʹ-CTTTCAGCATTTTGACGGCAACC-3ʹ. The forward primer of NPM1 gene is 5ʹ-TGTCTATGAAGTGTTGTGGTTCC-3ʹ, the reverse primer is 5ʹ-GGACAGCCAGATATCAACTG-3ʹ. The forward primer of DNMT3A gene is 5ʹ-GTAAAACGACGGCCAGT CCTCTCTCCCACCTTTCCTC-3ʹ, the reverse primer was 5ʹ-CAGGAAACAGCTATGACCCTGAGTGCCGGGTTGTTTAT-3ʹ. All PCR primers were linked with M13F/R universal primer. The total volume of the PCR reaction system was 20 µL, including 200 ng DNA, 20 pmol PCR primers, 25 mmol/L MgCl2, 2.5 mmol/L dNTP, 2 µL 10× PCR buffer, 0.2 µL HotTaq DNA polymerase (Qiagen, Shanghai, People's Republic of China). Reaction conditions: denaturation at 94°C for 5 mins, 94°C for 30 s, 58°C for 40 s and 72°C for 1 min for 35 cycles. PCR products were then sequenced by ABI 3500 Genetic Analyzer (Applied Biosystems). CEBPA, KIT, IDH1/IDH2 and TET2 mutations were analyzed by next-generation sequencing technology (San Valley Diagnostics).
Treatments
All 76 patients adopted the IA scheme (idarubicin and cytarabine; 62cases) or HAA scheme (harringtonine, aclacinomycin and cytarabine; 14cases) for induced chemotherapy. After achieving CR, they were then treated with another course of IA or HAA, and then all patients were treated with intermediate-dose cytarabine (2.0/m2) for 2–3 courses, coupled with standard dose chemotherapies composed with aclacinomycin, cytarabine, etoposide, harringtonine, idarubicin and mitoxantrone as consolidation chemotherapies. When relapsed, patients were treated with FLAG (fludarabine/cytarabine/granulocyte colony-stimulating factor) or the CLAG (cladribine/cytarabine/granulocyte colony-stimulating factor), or decitabine+CAG (cytarabine, aclacinomycin and granulocyte colony-stimulating factor) for re-induction therapy. Twenty-two patients received allogeneic hematopoietic stem cell transplantation (allo-HSCT) at CR1. We adopted a myeloablative pretreatment scheme based on busulfan, cyclophosphamide before transplantation, and used mycophenolate combined with cyclosporine A plus methotrexate to prevent graft-versus-host disease (GVHD). For those patients who received HLA-haploidentical allo-HSCT, antithymocyte globulin was added to prevent GVHD.
Statistical analyses
SPSS Statistics (Version 23.0. Armonk, NY: IBM Corp.) was used for statistical analyses. We used a chi-square test for comparisons between sample rates including clinical characteristics, protocol and CR rate. OS and disease-free survival (DFS) were analyzed by the Kaplan–Meier method, risk factor analysis was analyzed by Cox Regression method, and the log-rank test was adopted to compare differences between groups. The P-value <0.05 was considered to be significantly different.
Results
Biological and clinical characteristics
We identified 76 AML patients coexistent with FLT3-ITD and NPM1 mutations. All patients were with normal conventional cytogenetics. The median age was 50 years (range, 14–71 years) with elderly patients (≥60 years) accounted for 23.7%. The male/female ratio was 0.9. The median percentage of bone marrow blast was 79.5% (range, 22.0–97.0%). WBC counts ranged from 1.6 to 229.6×109/L with a median of 62.2×109/L, and 36.8% of patients were hyper-leukocytosis at diagnosis. 18/76 (23.7%) detected DNMT3A R882 mutation, and 15/76 (19.7%) patients were not detected or unknown. In order to remove the effects from CEBPA, patients with CEBPA double mutation were excluded. KIT, IDH1, IDH2 and TET2 mutations were also detected and the incidence rates were of no differences between transplantation and chemotherapy groups.
OS and DFS
After induction chemotherapy, 53/76 (69.8%) of patients obtained CR, 15/76 (19.7%) did not reach CR and 8/76 (10.5%) were unknown. Twenty-two patients underwent allo-HSCT at CR1 (Table 1). The median follow-up time was 20 months for all patients. At the end of the follow-up, 42 (55.3%) patients died and 19/53 (35.8%) relapsed. The median DFS time for all AMLFLT3-ITD+/NPM1+ patients was 8.1 months (range, 0–87.4 months), the median OS time was 12.2 months (range, 0.2–89.2 months) (Figure 1). To clarify the better treatment for these AMLFLT3-ITD+/NPM1+patients, allo-HSCT group (n=22) vs chemotherapy group (n=31) were compared. Transplantation group has better DFS and OS than chemotherapy group (medium OS: not reach vs 14.5 months, P=0.002; medium DFS: not reach vs 9.3 months, P=0.001) (Figure 2A and B). Among 44 patients received CR who were younger than 60 years. Transplant still significantly improved the prognosis (medium OS: not reach vs 12.3 months, P=0.004; medium DFS: not reach vs 8.1months, P=0.002) (Figure 2C and D).
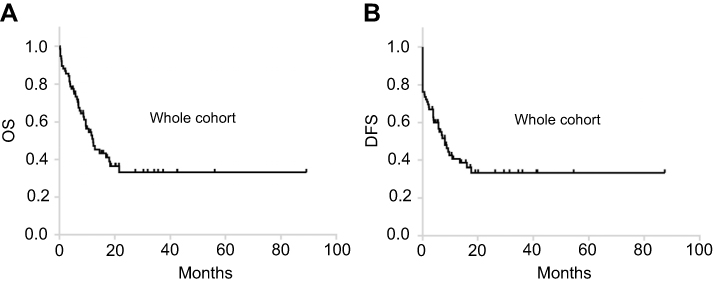 | Figure 1 Prognostic analysis of all 76 patients. (A) Overall survival of all 76 AMLFLT3-ITD+/NPM1+ patients. (B) Disease-free survival of all 76 AMLFLT3-ITD+/NPM1+ patients. Abbreviations: OS, overall survival; DFS, disease-free survival. |
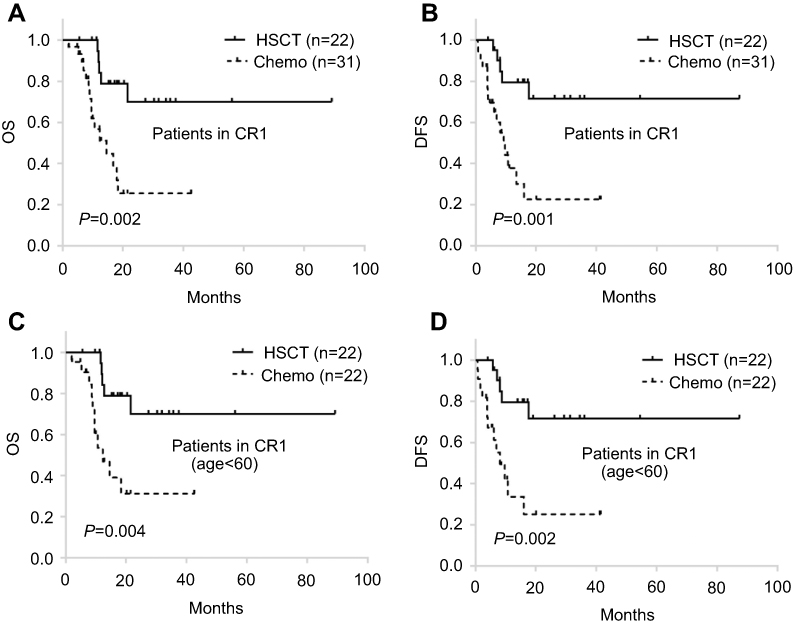 | Figure 2 Comparison of chemotherapy and allo-HSCT in patients received CR1. (A, B): OS and DFS of the 53 AMLFLT3-ITD+/NPM1+ patients received CR1. (C, D) OS and DFS of the 44 AMLFLT3ITD+/NPM1+patients (age<60 years) received CR1.Abbreviations: OS, overall survival; DFS, disease-free survival; HSCT, hematopoietic stem cell transplantation; chemo, chemotherapy; CR1, first complete remission. |
Our study also showed that several AML-related gene mutations were co-existed in AMLFLT3-ITD+/NPM1+ patients, including DNMT3A R882 (18/23.7%), IDH2 (7/9.2%), IDH1 (5/6.6%), TET2 (4/5.3%) and KIT (1/0.3%). The incidence rates of all above gene mutations were equal in chemotherapy and transplantation groups (all P>0.05). Thus, the result that allo-HSCT had better prognosis than chemotherapy alone for AMLFLT3-ITD+/NPM1+ patients was not interfered by concomitant mutations.
In 76 AMLFLT3-ITD+/NPM1+ patients, 18 patients were also detected as DNMT3A R882 mutation positive, with a percentage of 23.7%, which is similar to reports which is about 20% in all AML patients.22 Depending on having DNMT3A R882 mutation or not, AMLFLT3-ITD+/NPM1+ patients were divided into AMLFLT3-ITD+/NPM1+/DNMT3A R882+group (n=18) and AMLFLT3-ITD+/NPM1+/DNMT3A R882-group (n=43). AMLFLT3-ITD+/NPM1+/DNMT3A R882+ patients had worse OS and DFS than AMLFLT3-ITD+/NPM1+/DNMT3A R882- patients (medium OS: 9.5 months vs not reach, P=0.007; medium DFS: 6.1 months vs not reach, P=0.002) (Figure 3A and B). There was no statistical difference in CR rate between DNMT3A R882 mutated group and DNMT3A R882 unmutated group (72.2% vs 83.7%, P=0.319, Table 1), but the cumulative incidence (CI) of relapse in the DNMT3A R882 mutated group was significantly higher than the unmutated group (P=0.009) (Figure 5A). This indicates that DNMT3A R882 mutation can increase the relapse rate of AMLFLT3-ITD+/NPM1+ patients, and the reduced survival of AMLFLT3-ITD+/NPM1+/DNMT3A R882+group was caused by the high relapse rate but not the poor CR rate. To further investigate how to improve the poor prognosis of AMLFLT3-ITD+/NPM1+/DNMT3A R882+ patients, we compared the OS and DFS in allo-HSCT and chemotherapy alone therapies. Results showed that allo-HSCT can significantly improve the OS and DFS both in AMLFLT3-ITD+/NPM1+/DNMT3A R882+group and in AMLFLT3-ITD+/NPM1+/DNMT3 R882-group (both P<0.001, Figure 3C–F). However, in AMLFLT3-ITD+/NPM1+/DNMT3A R882+patients, the advantage in allo-HSCT group was not obvious, the 1-year OS rate was still <30%.
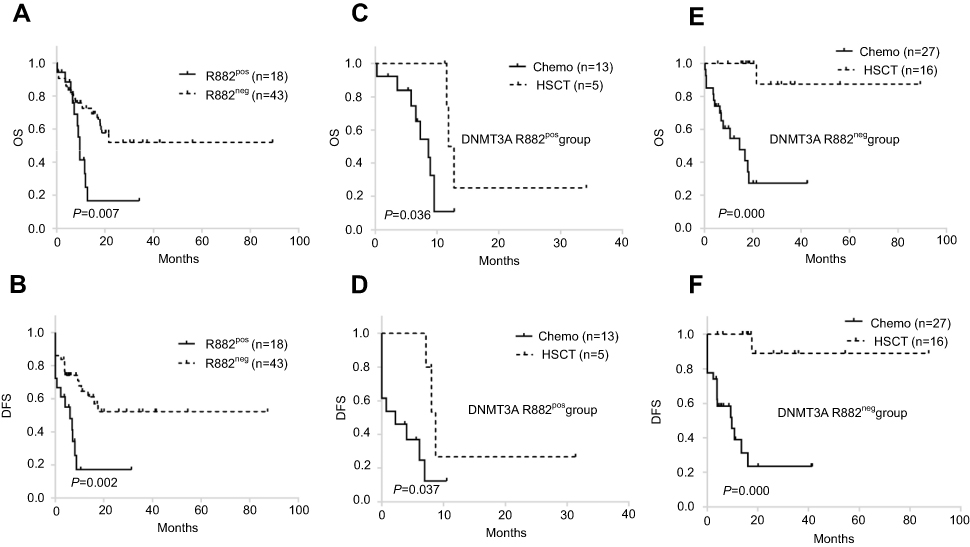 | Figure 3 Comparison of outcome in different mutation groups. (A, B) OS and DFS of AMLFLT3-ITD+/NPM1+/DNMT3A R882+ vs. AMLFLT3-ITD+/NPM1+/DNMT3A R882-in 61 patients. (C, D) Comparison of the survival of chemotherapy group and allo-HSCT group in 18 AMLFLT3-ITD+/NPM1+/DNMT3A R882+ patients. (E, F) Comparison of the survival of chemotherapy group and allo-HSCT group in 43 AMLFLT3ITD+/NPM1+/DNMT3A R882-patients.Abbreviations: OS, overall survival; DFS, disease-free survival; pos, positive; neg, negative; HSCT, hematopoietic stem cell transplantation; chemo, chemotherapy. |
We also noticed that 28/76 patients had HL. The prognosis of HL group (n=28) vs. non-HL group (n=48) were analyzed, which showed that the HL group had worse OS and DFS (medium OS: 6.9 months vs 18.0 months, P=0.008; medium DFS: 3.8 months vs 13.5 months, P=0.009, Figure 4A and B). Patients with HL had significantly worse CR rate than those with non-HL (53.6% vs 79.2%, P=0.005) (Table 1), and there was no significant difference in CI of relapse rates between these two groups (P=0.371) (Figure 5B). So that the poor survival in HL group is majorly caused by the inferior CR rate but not a high relapse rate. Allo-HSCT could prolong OS and DFS, no matter whether patients are with HL. (all P<0.05) (Figure 4C–F). There is no significant difference (P=0.306) on the ratio of HL patients between allo-HSCT and chemotherapy groups, thus the better prognosis of AMLFLT3-ITD+/NPM1+ patients achieved in allo-HSCT group is not caused by a lower ratio of HL patients.
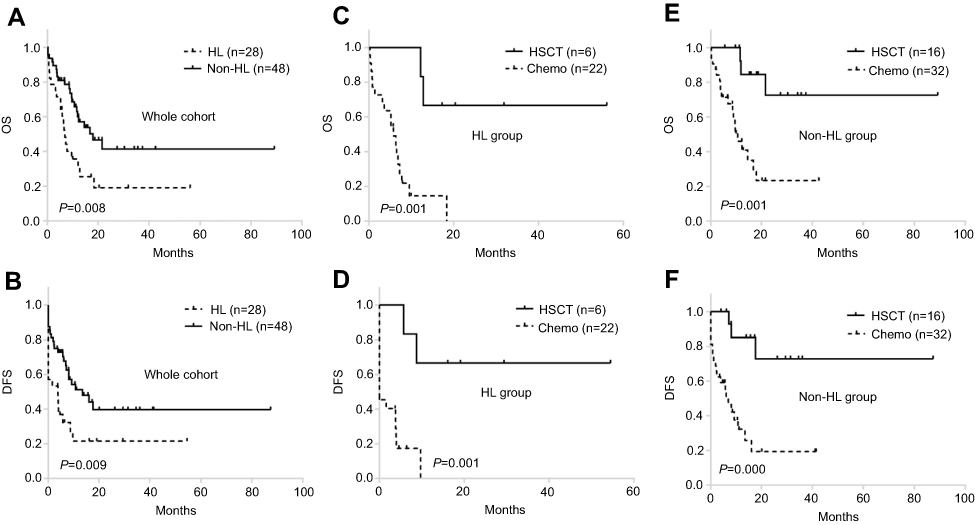 | Figure 4 Comparison of outcome in different clinical groups associated with HL. (A, B) OS and DFS of HL vs. non-HL in all 76 patients. (C, D) Comparison the survival of chemotherapy group and allo-HSCT group in 28 patients with HL. (E, F) Comparison the survival of chemotherapy group and allo-HSCT group in 48 patients with non-HL.Abbreviations: OS, overall survival; DFS, disease-free survival; HSCT, hematopoietic stem cell transplantation; chemo, chemotherapy; HL, hyperleukocytosis. |
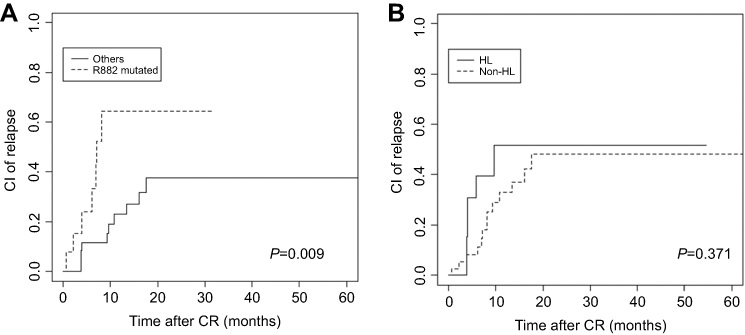 | Figure 5 Comparison of relapse rate in different biological and clinical groups. (A) CI of relapse between AMLFLT3-ITD+/NPM1+/DNMT3A R882+and AMLFLT3-ITD+/NPM1+/DNMT3A R882-in 49 patients received CR (P=0.009). (B) CI of relapse between HL and Non-HL in 53 patients received CR (P=0.371).Abbreviations: CI, cumulative incidence; HL, hyperleukocytosis; CR, complete remission. |
Risk factors for OS and DFS
Risk factors as age, gender, WBC (HL or Non-HL), treatment (allo-HSCT or chemotherapy), combined mutated genes including DNMT3A R882, IDH1, IDH2, TET2 and KIT were evaluated with univariate analysis (Table 2). Only factors with a P-value of <0.2 in the univariate analysis were included in the multivariate analysis model. Multivariate Cox model analysis (Table 3) showed that age ≥60, with HL, and DNMT3A R882 mutation were independent risk factors for OS of AML FLT3-ITD+/NPM1+ patients (P=0.005, 0.042 and 0.001; HR=3.035, 1.994 and 4.339; 95% CI were 1.395–6.601,1.027–3.872 and 1.798–10.474, respectively). HL and DNMT3A R882 mutation also were independent risk factors for DFS (P=0.015 and 0.003; HR =2.327 and 3.435; 95% CI were 1.177–4.603 and 1.514–7.793, respectively). Allo-HSCT was an independent benefit factor of both OS and DFS (P=0.001 and 0.000; HR=0.173 and 0.138; 95% CI were 0.062–0.483 and 0.049–0.389, respectively). None of the other factors, including sex, IDH1, IDH2, TET2 and KIT mutation were found significantly associated with OS and/or DFS in multivariate analysis.
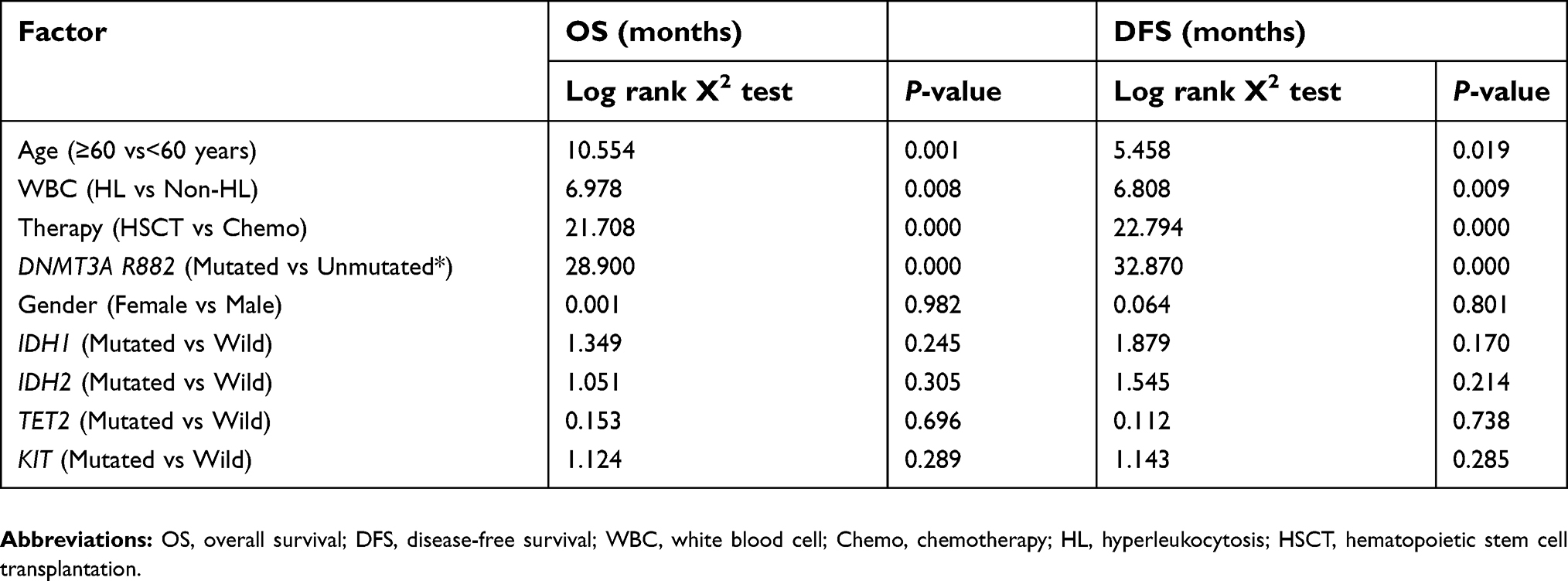 | Table 2 Analysis of risk factors of FLT3-ITD and NPM1 double mutated AML |
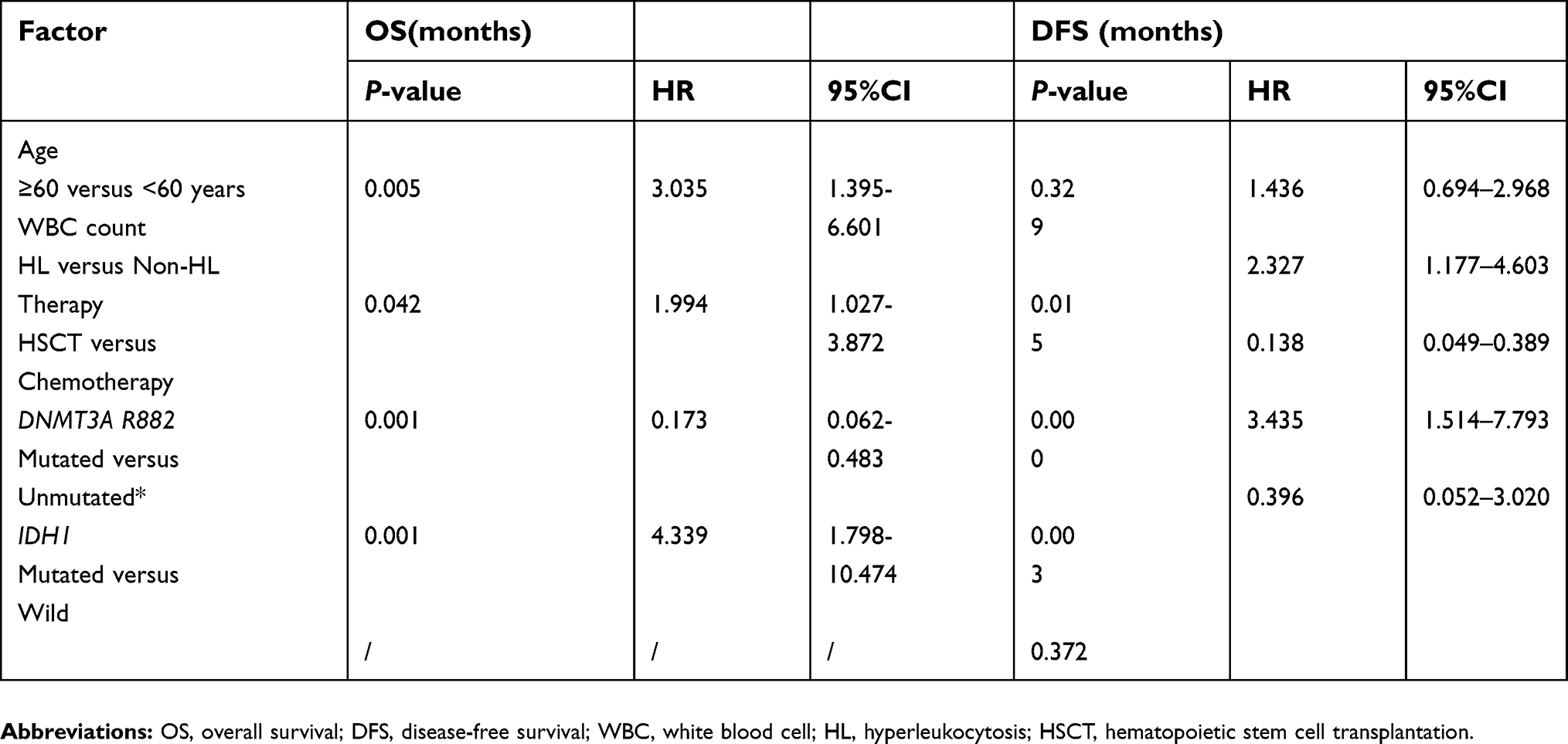 | Table 3 Multivariate Cox model analysis of FLT3-ITD and NPM1 double mutated AML |
A major concern was then raised, how about the survival of AML FLT3-ITD+/NPM1+ patients without three risk factors including age ≥60, HL and DNMT3A R882 mutation? With statistical analysis on 24 AML FLT3-ITD+/NPM1+patients without either of three risk factors, the Kaplan–Meier curve showed that allo-HSCT had a trend of better OS than chemotherapy without significant difference (P=0.054), but the DFS could be significantly prolonged after allo-HSCT (P=0.032). This indicates that allo-HSCT can be recommended for all the AML FLT3-ITD+/NPM1+patients, no matter they show above three risk factors or not (Figure 6).
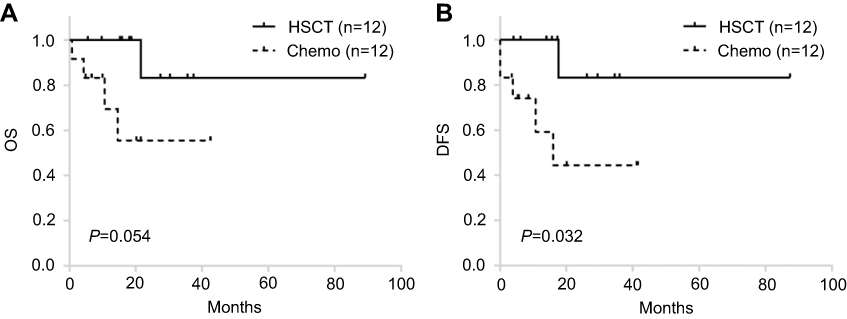 | Figure 6 Comparison of chemotherapy and allo-HSCT in AMLFLT3-ITD+/NPM1+patients without three risk factors including age ≥60, HL and DNMT3A R882 mutation. (A, B) OS and DFS of 24 AMLFLT3-ITD+/NPM1+/DNMT3A R882-patients younger than 60 years old and without HL.Abbreviations: OS, overall survival; DFS, disease-free survival; HSCT, hematopoietic stem cell transplantation; chemo, chemotherapy. |
Discussion
According to NCCN 2018 and ELN 2017 guidelines, the risk level in AMLFLT3-ITD+/NPM1+ dependents on the AR of FLT3-ITD mutation. Below 0.5 is defined as low AR. When FLT3-ITD’s AR is low, AMLFLT3-ITD+/NPM1+ falls to low risk, when FLT3-ITD’s AR is high, this type of AML falls to intermediate risk. In this study, we did not detect the AR of FLT3-ITD, because this laboratory examination is not a regular item in our hospital and its cost is high. But according to guidelines, with either low or high FLT3-ITD AR, patients with FLT3-ITD and NPM1 double mutations fall in low or intermediate risk levels, for them allo-HSCT is not obligated.
However, some clinicians view the NCCN and ELN recommendation with skepticism. In two published validation studies,16,17 when comparing low FLT3-ITD AR patients with high AR, no significant differences of survival were found in AMLNPM1+ patients. Moreover, in a large group of AML patients,18 low FLT3-ITD AR with NPM1 mutated AML, which was classified in NCCN as favorable risk level, should be considered as intermediate-risk group. And the similar conclusion was also reported by Liu et al19. Besides, some studies indicated that allo-HSCT improves the prognosis in NPM1 mutated AML with FLT3-ITD low AR.19–21 Moreover, Patel et al23 reported that high variant allele frequency of NPM1 predict poor outcomes in de novo AML, even after undergoing hematopoietic stem cell transplantation. And the effect of high NPM1 variant allele frequency on prognosis was not affected by the level of FLT-ITD AR. These findings directly challenge the prognostic risk stratification of FLT3-ITD and NPM1 double-mutated AML. What is the optimal treatment for this type of AML is obscure too.
In order to know more about the FLT3-ITD and NPM1 mutation double positive AML, we studied 76 AML FLT3-ITD+/NPM1+ patients. Our result did not support that AMLFLT3-ITD+/NPM1+ patients have favorable prognosis: the median DFS time for all AMLFLT3-ITD+/NPM1+ patients was 8.1 months (range, 0–87.4 months), the median OS time was 12.2 months (range, 0.2–89.2 months). Allo-HSCT group had significantly prolonged OS and DFS of AML FLT3-ITD+/NPM1+ patients than chemotherapy alone. Here, as age was not balanced between transplantation and chemotherapy groups, we analyzed 44 patients in chemotherapy group who were younger than 60 years with all the 22 patients in transplantation group who are younger than 60. And the results also showed that allo-HSCT can significantly improve the prognosis in AML FLT3-ITD+/NPM1+ patients. (Figure S1) We further analyzed the impact of induction regimen on prognosis. Among 76 patients, 62 patients received IA scheme and 14 adopted homoharringtonine-based induction regimens (HAA). After remission, all patients were treated with intermediate-dose cytarabine (2.0/m2) for 2–3 courses and coupled with standard dose chemotherapies such as AAE, IAE, AA and MAE. Previous reports showed the assessment of intermediate-dose cytarabine monotherapy vs. intermediate-dose cytarabine combination treatment of standard dose chemotherapies did not present a significant difference with respect to RFS and OS.24 Thus, no matter which standard dose chemotherapies were used, all patients can be considered as to be received with consolidation treatments equally. The only difference is the induction chemotherapy. Thus, we divided patients of chemotherapy group into two sub-groups: IA group (62 cases) and HAA group (14 cases) (Table S1). According to the K-M survival analysis, we found that the IA group achieved a better prognosis than the HAA group (data not shown). Then, we compared consolidation chemotherapy with transplantation in IA group, the median OS for chemotherapy group is 9.5 months, median DFS is 4months, while transplantation group was not reached for both OS and DFS (both P=0.000) (Figure S1A and B). In order to balance the age, 38 patients aged younger than 60 years old were analyzed, and the result still supported that allo-HSCT can improve patients’ OS and DFS than consolidation chemotherapy did (P=0.006 and 0.002, respectively) (Figure S1C and D). There were only four patients adopted SCT in HAA group. As SCT had better OS and DFS in IA group, we could say transplantation improved survival in HAA group. Thus, transplantation group should have better survival than chemotherapy group in a whole. Also, after excluded three risk factors including age ≥60, HL and DNMT3A R882, allo-HSCT still showed better survival than chemotherapy. Thus, our result supported that AML FLT3-ITD+/NPM1+ patients, with either low or high FLT3-ITD AR, accept allo-HSCT at CR1 to improve their survival.
HL is defined as the WBC count above 100,000/mm3 in peripheral blood at the initial diagnosis. In this study, the proportion of patients with HL at initial diagnosis of AMLFLT3-ITD+/NPM1+ patients accounted for 36.8%, which is higher than the ratio in de novo AML patients (5–20%) reported in the previous literature.25–28 Moreover, HL was found to be an independent risk factor for AMLFLT3-ITD+/NPM1+. Patients with HL suffered shorter OS and DFS than non-HL. The high ratio of HL may be one of the causes of poor survival of AMLFLT3-ITD+/NPM1+ patients. It is generally believed that AML patients presented with HL have a particularly dismal prognosis because of 1) A higher risk of early death resulting from HL complications, including disseminated intravascular coagulation, tumor lysis syndrome, and leukostasis; 2) a higher probability of relapse and death in the long run.25,29–31 In this study, we found that the CI of relapse rate of HL did not differ from that of non-HL. But patients with HL had significantly worse CR rate than with non-HL. So the poor OS and DFS of HL group is not related to the higher relapse rate, but could the lower CR rate.
This study also revealed that 23.7% of AMLFLT3-ITD+/NPM1+ patients were also positive for DNMT3A R882 mutation. Among the six combined mutational genes including DNMT3A R882, IDH1, IDH2,TET2 and KIT, only DNMT3A R882 was the independent risk factor for OS and DFS of AML FLT3-ITD+/NPM1+ patients. Ley et al’s study showed that in the de novo AML patients, the co-occurrence between mutations in FLT3, DNMT3A, and NPM1 was the most prominent,32 and this triple-mutation represent a novel subtype of AML for the distinct molecular characteristics. Loghavi et al found that 20% of de novo AML have DNMT3A, NPM1 and FLT3 mutation coexistence.33 A large number of studies reported that DNMT3A mutation predicts poor outcome.32–37 Kumar et al found that DNMT3A R882 mutation plays an important role in normal chromosome AML patients’ prognosis and clinical outcomes in the presence of NPM1 and FLT3 mutations.38 Although various DNMT3A mutations have been identified in AML, R882 is the most frequent, accounting for 70–80% of all DNMT3A mutations.39 DNMT3A R882 mutation was widely accepted as a poor prognostic factor in AML patients.40–42 The effect of non-R882 mutation was not very clear, some studies showed that both R882 and non-R882 mutations of DNMT3A appeared to be associated with a negative prognostic impact on OS.22,43 Here, we only present the data with DNMT3A R882 mutation. Our results showed that AMLFLT3-ITD+/NPM1+/DNMT3A R882+ patients had significant worse outcomes than AMLFLT3-ITD+/NPM1+/DNMT3A R882- patients. Although the survival was only moderately increased, allo-HSCT can give better OS and DFS in AMLFLT3-ITD+/NPM1+/DNMT3A R882+ patients. We also found that there was no difference of CR rate between AML FLT3-ITD+/NPM1+/DNMT3A R882+ and AML FLT3-ITD+/NPM1+/DNMT3A R882- patients, but AML FLT3-ITD+/NPM1+/DNMT3A R882+patients had a higher relapse rate. Thus, the poor survival of AML FLT3-ITD+/NPM1+/DNMT3A R882+AML patients may be due to the higher relapse rate.
We concluded that AMLFLT3-ITD+/NPM1+ is associated with an unfavorable survival. Age ≥60, with HL at diagnosing, and DNMT3A R882 mutation were independent risk factors for FLT3-ITD and NPM1 double mutated AML. Allo-HSCT can improve the survival of AMLFLT3-ITD+/NPM1+ patients. Thus, although AMLFLT3-ITD+/NPM1+ patients were considered with favorable to intermediate risk, they should undergo allo-HSCT at CR1. Further studies need to be done to know better of this type of AML.
Acknowledgment
This study was supported by two grant from the China National Natural Science Foundation Council (81372031 and 8140080).
Disclosure
The authors report no conflicts of interest in this work.
References
1. El Fakih R, Rasheed W, Hawsawi Y, Alsermani M, Hassanein M. Targeting FLT3 mutations in acute myeloid leukemia. Cells. 2018;7(1). doi:10.3390/cells7010004
2. Kindler T, Lipka DB, Fischer T. FLT3 as a therapeutic target in AML: still challenging after all these years. Blood. 2010;116(24):5089–5102. doi:10.1182/blood-2010-04-261867
3. Bullinger L, Valk PJ. Gene expression profiling in acute myeloid leukemia. J Clin Oncol. 2005;23(26):6296–6305. doi:10.1200/JCO.2005.05.020
4. Frohling S, Scholl C, Levine RL, et al. Identification of driver and passenger mutations of FLT3 by high-throughput DNA sequence analysis and functional assessment of candidate alleles. Cancer Cell. 2007;12(6):501–513. doi:10.1016/j.ccr.2007.11.005
5. Thiede C, Steudel C, Mohr B, et al. Analysis of FLT3-activating mutations in 979 patients with acute myelogenous leukemia: association with FAB subtypes and identification of subgroups with poor prognosis. Blood. 2002;99(12):4326–4335.
6. Yamamoto Y, Kiyoi H, Nakano Y, et al. Activating mutation of D835 within the activation loop of FLT3 in human hematologic malignancies. Blood. 2001;97(8):2434–2439.
7. Meshinchi S, Alonzo TA, Stirewalt DL, et al. Clinical implications of FLT3 mutations in pediatric AML. Blood. 2006;108(12):3654–3661. doi:10.1182/blood-2006-03-009233
8. Govedarovic N, Marjanovic G. Frequency and prognostic impact of FLT3/ITD mutation in patients with acute myeloid leukaemia. J BUON. 2011;16(1):108–111.
9. Canaani J, Labopin M, Huang XJ, et al. T-cell replete haploidentical stem cell transplantation attenuates the prognostic impact of FLT3-ITD in acute myeloid leukemia: a report from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Am J Hematol. 2018;93(6):736–744. doi:10.1002/ajh.25082
10. Heath EM, Chan SM, Minden MD, Murphy T, Shlush LI, Schimmer AD. Biological and clinical consequences of NPM1 mutations in AML. Leukemia. 2017;31(4):798–807. doi:10.1038/leu.2017.30
11. Thiede C, Koch S, Creutzig E, et al. Prevalence and prognostic impact of NPM1 mutations in 1485 adult patients with acute myeloid leukemia (AML). Blood. 2006;107(10):4011–4020. doi:10.1182/blood-2005-08-3167
12. Schnittger S, Schoch C, Kern W, et al. Nucleophosmin gene mutations are predictors of favorable prognosis in acute myelogenous leukemia with a normal karyotype. Blood. 2005;106(12):3733–3739. doi:10.1182/blood-2005-06-2248
13. Chou WC, Tang JL, Lin LI, et al. Nucleophosmin mutations in de novo acute myeloid leukemia: the age-dependent incidences and the stability during disease evolution. Cancer Res. 2006;66(6):3310–3316. doi:10.1158/0008-5472.CAN-05-4316
14. Boissel N, Renneville A, Biggio V, et al. Prevalence, clinical profile, and prognosis of NPM mutations in AML with normal karyotype. Blood. 2005;106(10):3618–3620. doi:10.1182/blood-2005-05-2174
15. Doehner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
16. Boddu PC, Kadia TM, Garcia-Manero G, et al. Validation of the 2017 European LeukemiaNet classification for acute myeloid leukemia with NPM1 and FLT3-internal tandem duplication genotypes. Cancer. 2018;125:1091–1100.
17. Harada Y, Nagata Y, Kihara R, et al. Prognostic analysis according to the 2017 ELN risk stratification by genetics in adult acute myeloid leukemia patients treated in the Japan Adult Leukemia Study Group (JALSG) AML201 study. Leuk Res. 2018;66:20–27. doi:10.1016/j.leukres.2018.01.008
18. Versluis J, In ‘T Hout FE, Devillier R, et al. Comparative value of post-remission treatment in cytogenetically normal AML subclassified by NPM1 and FLT3-ITD allelic ratio. Leukemia. 2017;31(1):26–33. doi:10.1038/leu.2016.183
19. Liu SB, Qiu QC, Bao XB, et al. Pattern and prognostic value of FLT3-ITD mutations in Chinese de novo adult acute myeloid leukemia. Cancer Sci. 2018;109(12):3981–3992. doi:10.1111/cas.13835
20. Sakaguchi M, Yamaguchi H, Najima Y, et al. Prognostic impact of low allelic ratio FLT3-ITD and NPM1 mutation in acute myeloid leukemia. Blood Adv. 2018;2(20):2744–2754. doi:10.1182/bloodadvances.2018020305
21. Oran B, Cortes J, Beitinjaneh A, et al. Allogeneic transplantation in first remission improves outcomes irrespective of FLT3-ITD allelic ratio in FLT3-ITD-positive acute myelogenous leukemia. Biol Blood Marrow Transplant. 2016;22(7):1218–1226. doi:10.1016/j.bbmt.2016.03.027
22. Yuan XQ, Peng L, Zeng WJ, Jiang BY, Li GC, Chen XP. DNMT3A R882 mutations predict a poor prognosis in AML: a meta-analysis from 4474 patients. Medicine. 2016;95(18):e3519. doi:10.1097/MD.0000000000004864
23. Patel SS, Kuo FC, Gibson CJ, et al. High NPM1-mutant allele burden at diagnosis predicts unfavorable outcomes in de novo AML. Blood. 2018;131(25):2816–2825. doi:10.1182/blood-2018-01-828467
24. Magina KN, Pregartner G, Zebisch A, et al. Cytarabine dose in the consolidation treatment of AML: a systematic review and meta-analysis. Blood. 2017;130(7):946–948. doi:10.1182/blood-2017-04-777722
25. Rollig C, Ehninger G. How I treat hyperleukocytosis in acute myeloid leukemia. Blood. 2015;125(21):3246–3252. doi:10.1182/blood-2014-10-551507
26. Canaani J, Labopin M, Socie G, et al. Long term impact of hyperleukocytosis in newly diagnosed acute myeloid leukemia patients undergoing allogeneic stem cell transplantation: an analysis from the acute leukemia working party of the EBMT. Am J Hematol. 2017;92(7):653–659. doi:10.1002/ajh.24737
27. Byrd JC, Mrozek K, Dodge RK, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood. 2002;100(13):4325–4336. doi:10.1182/blood-2002-03-0772
28. Porcu P, Danielson CF, Orazi A, Heerema NA, Gabig TG, McCarthy LJ. Therapeutic leukapheresis in hyperleucocytic leukaemias: lack of correlation between degree of cytoreduction and early mortality rate. Br J Haematol. 1997;98(2):433–436.
29. Dixit A, Chatterjee T, Mishra P, et al. Disseminated intravascular coagulation in acute leukemia at presentation and during induction therapy. Clin Appl Thromb Hemost. 2007;13(3):292–298. doi:10.1177/1076029607302435
30. Porcu P, Cripe LD, Ng EW, et al. Hyperleukocytic leukemias and leukostasis: a review of pathophysiology, clinical presentation and management. Leuk Lymphoma. 2000;39(1–2):1–18. doi:10.3109/10428190009053534
31. Porcu P, Farag S, Marcucci G, Cataland SR, Kennedy MS, Bissell M. Leukocytoreduction for acute leukemia. Ther Apher. 2002;6(1):15–23.
32. Ley TJ, Miller C, Ding L, et al. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med. 2013;368(22):2059–2074. doi:10.1056/NEJMoa1301689
33. Loghavi S, Zuo Z, Ravandi F, et al. Clinical features of de novo acute myeloid leukemia with concurrent DNMT3A, FLT3 and NPM1 mutations. J Hematol Oncol. 2014;7:74. doi:10.1186/s13045-014-0074-4
34. Marcucci G, Metzeler KH, Schwind S, et al. Age-related prognostic impact of different types of DNMT3A mutations in adults with primary cytogenetically normal acute myeloid leukemia. J Clin Oncol. 2012;30(7):742–750. doi:10.1200/JCO.2011.39.2092
35. Gale RE, Lamb K, Allen C, et al. Simpson‘s paradox and the impact of different DNMT3A mutations on outcome in younger adults with acute myeloid leukemia. J Clin Oncol. 2015;33(18):2072–2083. doi:10.1200/JCO.2014.59.2022
36. Ley TJ, Ding L, Walter MJ, et al. DNMT3A mutations in acute myeloid leukemia. N Engl J Med. 2010;363(25):2424–2433. doi:10.1056/NEJMoa1005143
37. Tie R, Zhang T, Fu H, et al. Association between DNMT3A mutations and prognosis of adults with de novo acute myeloid leukemia: a systematic review and meta-analysis. PLoS One. 2014;9(6):e93353. doi:10.1371/journal.pone.0093353
38. Kumar D, Mehta A, Panigrahi MK, Nath S, Saikia KK. DNMT3A (R882) mutation features and prognostic effect in acute myeloid leukemia in Coexistent with NPM1 and FLT3 mutations. Hematol Oncol Stem Cell Ther. 2018;11(2):82–89. doi:10.1016/j.hemonc.2017.09.004
39. Koya J, Kataoka K, Sato T, et al. DNMT3A R882 mutants interact with polycomb proteins to block haematopoietic stem and leukaemic cell differentiation. Nat Commun. 2016;7:10924. doi:10.1038/ncomms10924
40. Gaidzik VI, Schlenk RF, Paschka P, et al. Clinical impact of DNMT3A mutations in younger adult patients with acute myeloid leukemia: results of the AML Study Group (AMLSG). Blood. 2013;121(23):4769–4777. doi:10.1182/blood-2012-10-461624
41. Ahn JS, Kim HJ, Kim YK, et al. DNMT3A R882 mutation with FLT3-ITD positivity is an extremely poor prognostic factor in patients with normal-karyotype acute myeloid leukemia after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2016;22(1):61–70. doi:10.1016/j.bbmt.2015.07.030
42. Renneville A, Boissel N, Nibourel O, et al. Prognostic significance of DNA methyltransferase 3A mutations in cytogenetically normal acute myeloid leukemia: a study by the Acute Leukemia French Association. Leukemia. 2012;26(6):1247–1254. doi:10.1038/leu.2011.382
43. Thol F, Damm F, Ludeking A, et al. Incidence and prognostic influence of DNMT3A mutations in acute myeloid leukemia. J Clin Oncol. 2011;29(21):2889–2896. doi:10.1200/JCO.2011.35.4894
Supplementary materials
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.