Back to Journals » Journal of Pain Research » Volume 19
Acupuncture versus Sham Acupuncture for Migraine without Aura: A Systematic Review and Meta-Analysis
Authors Qi G, Li M, Zheng S, Xu X
Received 22 April 2026
Accepted for publication 16 June 2026
Published 10 July 2026 Volume 2026:19 616522
DOI https://doi.org/10.2147/JPR.S616522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Guoan Qi,1 Mengting Li,1 Shengen Zheng,2 Xu Xu3
1Traditional Chinese Medicine Clinic, Hangzhou Xiaoshan Hospital of Traditional Chinese Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Internal clinic, Shamen Town Health Clinic, Taizhou, Zhejiang, People’s Republic of China; 3Traditional Chinese Medicine Clinic, The People’s Hospital of Cangnan, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Xu Xu, Traditional Chinese Medicine Clinic, The People’s Hospital of Cangnan, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Migraine without aura is a disabling disorder for which acupuncture is commonly used as a preventive therapy. Sham-controlled randomized trials provide a more rigorous estimate of acupuncture-specific effects than comparisons with usual care. We evaluated the efficacy of acupuncture versus sham acupuncture in adults with migraine without aura.
Methods: We conducted a systematic review and meta-analysis of randomized sham-controlled trials. PubMed, Embase, Web of Science, CENTRAL, Scopus, and Wanfang were searched through 9 February 2026. The primary outcome was monthly migraine days (MMD). Secondary outcomes included migraine-specific quality of life (MSQ), pain intensity, and headache impact (HIT-6). Continuous outcomes were pooled as standardized mean differences (Hedges’ g) using random-effects REML models with Hartung–Knapp adjustment. Certainty of evidence was assessed using GRADE.
Results: Eight randomized trials involving 659 participants met the inclusion criteria. Compared with sham acupuncture, acupuncture reduced MMD (g = 0.46, 95% CI 0.27– 0.64; I2 = 0%) and pain intensity (g = 0.49, 95% CI 0.25– 0.72; I2 = 33%). MSQ showed a non-significant trend favoring acupuncture (g = 0.30, 95% CI − 0.01 to 0.62; I2 = 59%). HIT-6 scores also favored acupuncture (g = 0.58, 95% CI 0.02– 1.13), although heterogeneity was substantial (I2 = 80%). Sensitivity analyses did not materially alter the direction of effect. According to GRADE, certainty of evidence was low for MMD and pain intensity and very low for MSQ and HIT-6.
Conclusion: Acupuncture was associated with reductions in migraine frequency and pain intensity compared with sham procedures in adults with migraine without aura. However, evidence certainty ranged from low to very low, and findings for quality of life and headache impact remain uncertain. Larger multicenter trials with standardized sham procedures and longer follow-up are needed.
Trial Registration: The review protocol was registered in PROSPERO (CRD420261308589).
Keywords: migraine without aura, sham-controlled trial, acupuncture therapy, monthly migraine days, headache impact, meta-analysis
Introduction
Migraine without aura is a prevalent neurological disorder characterized by recurrent headache attacks that substantially impair daily functioning and quality of life. Although pharmacological therapies remain central to migraine management, their effectiveness is often limited by incomplete symptom control, adverse effects, and poor adherence in long-term preventive use. These limitations have prompted increasing interest in non-pharmacological strategies aimed at reducing migraine burden.1 Migraine also imposes a substantial economic burden through healthcare utilization, reduced workplace productivity, absenteeism, and presenteeism. Recent global estimates indicate that migraine remains one of the leading causes of disability among adults of working age, contributing significantly to both direct medical costs and indirect societal costs.1
Among these approaches, acupuncture has been widely adopted in clinical practice and evaluated in numerous randomized controlled trials. Some studies report clinically meaningful reductions in migraine frequency and symptom severity, while others demonstrate minimal differences compared with control interventions. This inconsistency has been reflected in guideline assessments and evidence syntheses, which often issue conditional recommendations and highlight variability in methodological rigor and reporting standards. A key methodological challenge in interpreting acupuncture research lies in distinguishing treatment-specific physiological effects from contextual and expectancy-related responses.2
Migraine without aura (MWoA) and migraine with aura are considered distinct clinical subtypes with differences in pathophysiological mechanisms, symptom presentation, and potentially treatment responsiveness. Migraine with aura is characterized by transient neurological symptoms associated with cortical spreading depolarization, whereas MWoA is primarily associated with activation of the trigeminovascular system.3 Restricting the present review to MWoA was intended to reduce clinical heterogeneity and provide more targeted evidence for this specific patient population.
Sham-controlled randomized trials provide a more rigorous framework for isolating specific treatment effects because they attempt to preserve blinding and control for procedural interaction.4 However, the interpretation of these trials remains complex. Sham acupuncture is not a uniform comparator and may involve superficial needling, non-penetrating devices, or needling at non-acupuncture locations, each potentially producing different degrees of physiological stimulation and placebo credibility.5 Moreover, many previous systematic reviews have combined heterogeneous comparators (eg, usual care or medication), mixed migraine subtypes, or non-placebo-controlled designs, limiting their ability to estimate the magnitude of acupuncture-specific effects under placebo-controlled conditions.
Consequently, uncertainty persists regarding whether acupuncture provides benefits beyond sham procedures in patients with migraine without aura.4 Clarifying this question is clinically important because it directly informs therapeutic recommendations and patient counseling regarding expected treatment benefit. Therefore, the present systematic review and meta-analysis was designed to synthesize evidence exclusively from randomized trials directly comparing acupuncture with sham acupuncture in adults with migraine without aura. We hypothesized that restricting analysis to placebo-controlled comparisons would provide a clearer estimate of acupuncture-specific clinical effects and reduce interpretive bias arising from heterogeneous comparator designs. To our knowledge, no previous systematic review has focused exclusively on sham-controlled randomized trials in adults with migraine without aura.
Methods
Eligibility Criteria
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement and the PRISMA-S extension for literature searches. The protocol was registered in the PROSPERO database (CRD420261308589) before study selection, data extraction, and statistical analyses.
Population
We included studies enrolling adults (≥18 years) diagnosed with migraine without aura according to recognized diagnostic criteria (eg, International Classification of Headache Disorders or equivalent clinical diagnostic standards) Studies including mixed headache populations were eligible only if data for migraine without aura could be extracted separately. Intervention: The intervention of interest was therapeutic acupuncture involving needle insertion at recognized acupuncture points, including manual acupuncture or electroacupuncture. Trials combining acupuncture with additional active therapies were excluded unless the independent effect of acupuncture could be isolated. Comparator: Eligible trials were required to use sham acupuncture designed to mimic the treatment procedure while minimizing specific therapeutic stimulation. Acceptable sham procedures included superficial needling, non-penetrating placebo devices, or needling at non-acupuncture points.
Studies using usual care, pharmacological therapy, waiting list, or no-treatment controls were excluded.
Outcomes: Studies were eligible if they reported at least one of the following predefined outcomes measured at the end of the treatment period. Monthly migraine days (MMD) is the primary outcome.
Secondary outcomes are Migraine-specific quality of life (MSQ), Pain intensity measured by visual analog scale (VAS) or equivalent scale, and Headache impact measured using HIT-6.
Study Design
Only randomized controlled trials were included. We excluded quasi-randomized trials, observational studies, conference abstracts without full text, protocols, animal studies, and duplicate datasets (the most complete report retained).
Information Sources and Search Strategy
A comprehensive search of PubMed, Embase, Web of Science Core Collection, Cochrane CENTRAL, Scopus, and Wanfang databases was conducted from inception to 9 February 2026. The search combined controlled vocabulary and free-text terms related to migraine without aura, acupuncture, sham/placebo acupuncture, randomized controlled trials. Outcome-specific terms were intentionally not used to maximize sensitivity. Reference lists of included studies and relevant reviews were manually screened for additional eligible trials. The full search strategies for each database are provided in Supplementary Appendix 1. Completed PRISMA 2020 is provided as Supplementary Appendix 2, and PRISMA-S checklists is provided as Supplementary Appendix 3.
Study Selection and Data Extraction
All retrieved records were imported into reference management software and duplicates removed.Two reviewers independently screened titles and abstracts, followed by full-text assessment of potentially eligible studies. Disagreements were resolved by discussion, and when necessary, consultation with a third reviewer. Extracted variables included: study characteristics (author, year, country), participant demographics, diagnostic criteria, acupuncture protocol (type, frequency, duration), sham procedure characteristics, outcome measures and assessment timepoints, sample size and attrition. For continuous outcomes, change-from-baseline values were preferentially extracted. If unavailable, post-treatment values were used. When required statistics were missing, they were derived using standard formulas. Data presented only in figures were extracted using WebPlotDigitizer.
Risk of Bias Assessment
Two reviewers independently assessed the risk of bias of the included randomized controlled trials using the Cochrane Risk of Bias 2.0 (RoB 2) tool. Five domains were evaluated: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of outcomes, and bias in selection of the reported results. Each domain and the overall study were judged as having low risk of bias, some concerns, or high risk of bias. Disagreements were resolved by discussion until consensus was reached.
Effect Measures
Continuous outcomes were pooled as standardized mean differences (Hedges’ g) with 95% confidence intervals to account for variability in measurement scales. When change-score standard deviations were unavailable, they were calculated using:  , with an assumed correlation coefficient r = 0.5.
, with an assumed correlation coefficient r = 0.5.
Data Synthesis and Statistical Analysis
Meta-analyses were performed using random-effects models with restricted maximum likelihood estimation (REML).
The Hartung–Knapp–Sidik–Jonkman adjustment was applied due to the small number of included studies.
Statistical heterogeneity was assessed using τ2 and I2 statistics.
Leave-one-out sensitivity analyses were conducted to evaluate robustness of pooled estimates.
Analyses were performed using Stata version 19.
Reporting Bias Assessment
Because fewer than 10 studies were included per outcome, funnel plot asymmetry tests were not considered reliable. Potential publication bias was therefore evaluated qualitatively by considering sample size distribution, study precision, and consistency of findings.
Certainty of Evidence
The certainty of evidence for each outcome was assessed using the GRADE framework across the domains of risk of bias, inconsistency, indirectness, imprecision, publication bias. Evidence was categorized as high, moderate, low, or very low certainty.
Results
Study Selection
The database search yielded 156 records from electronic sources, including PubMed (n = 23), Web of Science (n = 23), Embase (n = 28), the Cochrane Library (n = 32), Scopus (n = 31), and the Wanfang database (n = 19). After removal of 102 duplicate entries, 54 records remained for title and abstract screening, during which 40 were excluded.
Fourteen full-text reports were retrieved and assessed for eligibility. Six reports were subsequently excluded: three did not meet the predefined inclusion criteria and three lacked extractable data. Ultimately, eight randomized controlled trials were included in the systematic review and meta-analysis. The study selection process is summarized in the PRISMA 2020 flow diagram (Figure 1).
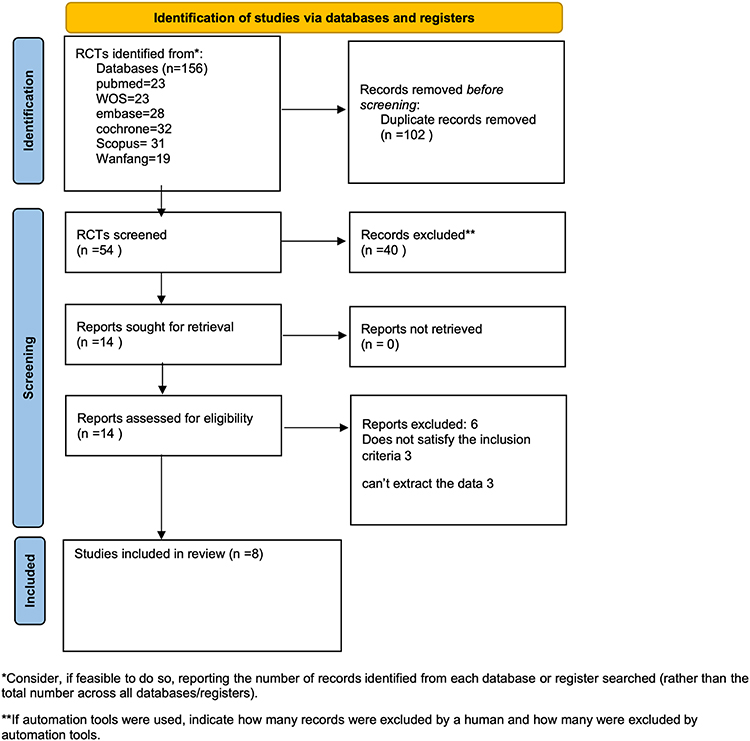 |
Figure 1 The PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Adapted from the PRISMA 2020 statement. ^17. |
Characteristics of Included Studies
Eight randomized controlled trials comparing acupuncture with sham acupuncture were included. All studies were conducted in China and enrolled adults diagnosed with migraine without aura. Across trials, sample sizes ranged from small single-center cohorts to larger parallel-group designs, with total participant numbers varying between 42 and 198 individuals.6,7 Participants were predominantly female, reflecting the known epidemiology of migraine, although the reported proportion varied across studies.8,9
Baseline demographic characteristics were generally comparable between acupuncture and sham groups within each trial. Mean participant age typically fell in the third to fourth decade of life, with some variability reflecting differences in recruitment settings.10,11 Baseline clinical measures indicated moderate migraine burden across studies, though reporting formats differed.7,12
Intervention protocols showed both consistency and methodological variation. Most trials employed manual acupuncture targeting fixed or standardized migraine-related acupoints,7–9,11,13 while one study incorporated electroacupuncture12 and another used intensified manual stimulation.6 Treatment schedules were typically structured around three sessions per week over four weeks, yielding 12 total sessions,10,13 whereas extended regimens involving 20 sessions over longer periods were also reported.6,11,12
Sham controls varied in design, including both penetrating and non-penetrating approaches intended to maintain participant blinding.8,9,13 Outcome assessments were performed at time points ranging from four to twenty weeks post-intervention, reflecting differences in study follow-up strategies.7,11 In terms of pain assessment, 7 articles used the Visual Analogue Scale (VAS), while 1 article did not specify the pain assessment tool used.6 Detailed participant characteristics, intervention parameters, and outcome reporting are summarized in Tables 1 and 2.
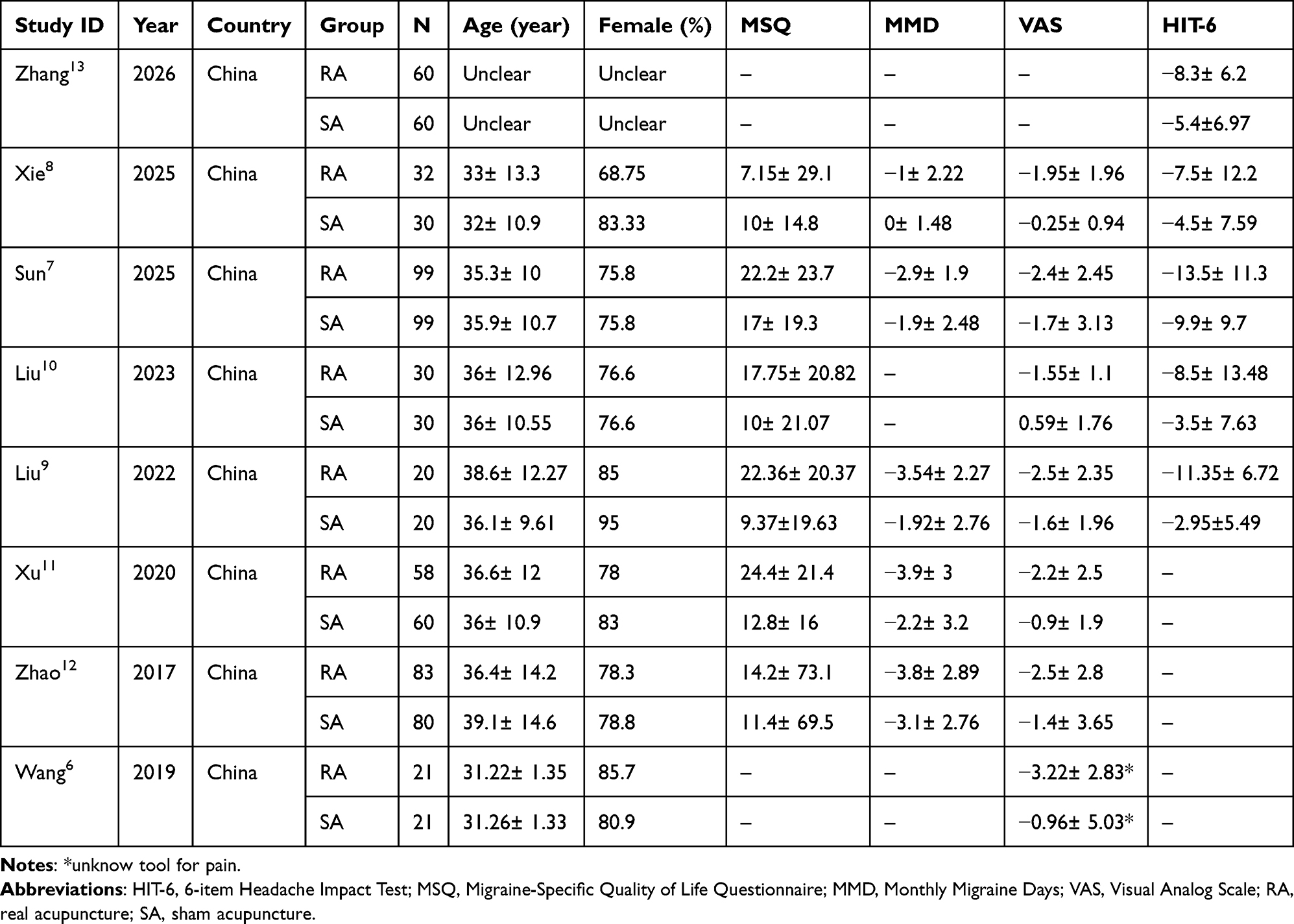 |
Table 1 Main Characteristics of the Included Randomized Controlled Trials |
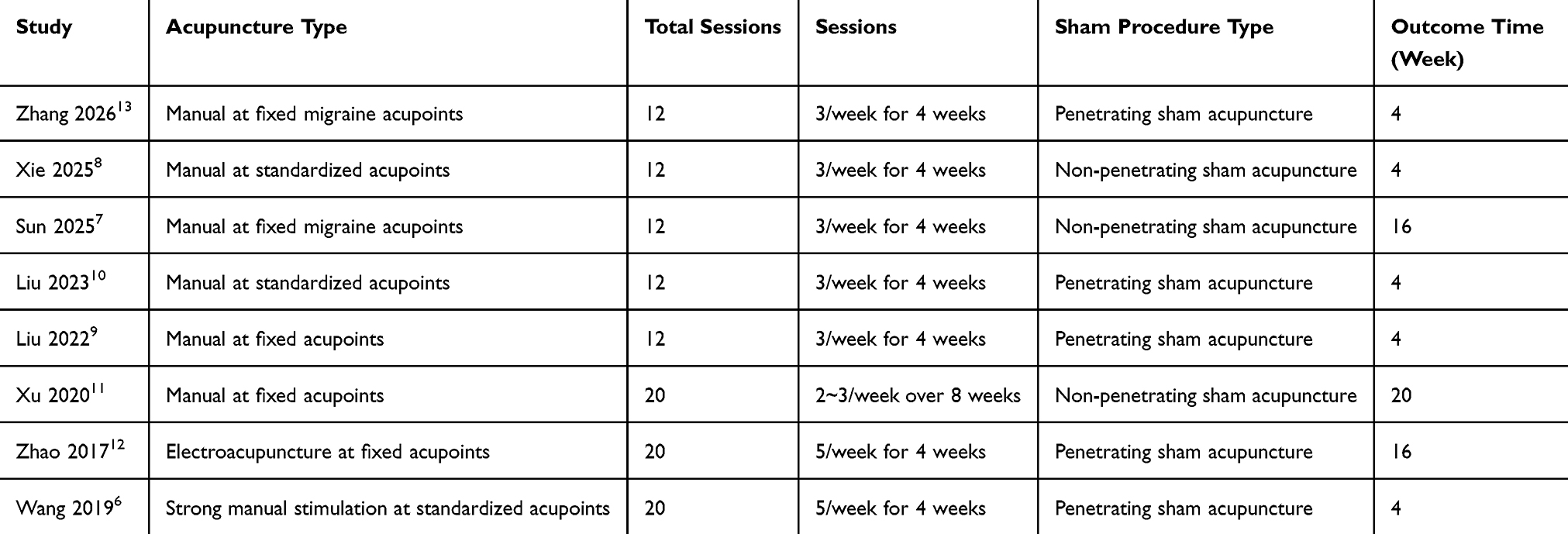 |
Table 2 Intervention Features of Included Acupuncture Trials |
Risk of Bias Assessment
Five domains were evaluated: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Most studies were judged as having low risk of bias in the measurement of outcomes, reflecting the use of validated migraine assessment tools and, in several trials, blinded outcome assessors. However, concerns remained regarding the randomization process and selection of the reported results, primarily because allocation concealment procedures and prespecified statistical analysis plans were not always fully reported. Bias due to deviations from intended interventions was generally low in studies using sham acupuncture controls and intention-to-treat analyses, although some concerns or high risk were identified in trials with inadequate blinding or insufficient reporting of adherence and analytical methods. Missing outcome data were generally well managed in larger trials but raised concerns in studies with post-randomization exclusions or incomplete reporting of attrition. Overall, most included studies were judged as having some concerns regarding risk of bias, while a minority were classified as high risk of bias, mainly because of inadequate reporting of randomization procedures, lack of blinding, non-intention-to-treat analyses, or incomplete handling of missing outcome data. Only a few trials met low-risk criteria across all RoB 2 domains (Figure 2 and supplementary table 1).
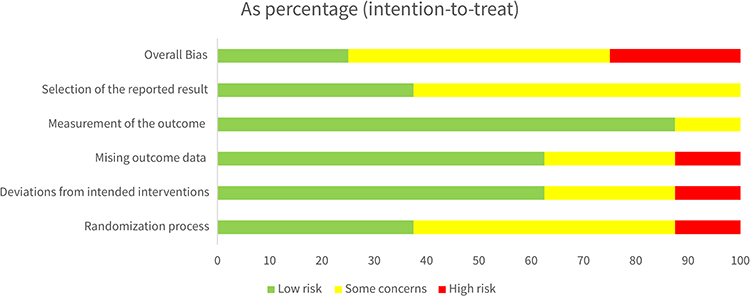 |
Figure 2 Graph for the risk of bias. |
Primary Outcomes
Mmd
Five trials reported monthly migraine days. Pooled analysis showed fewer migraine days with acupuncture compared with sham acupuncture (Hedges’ g = 0.46, 95% CI 0.27 to 0.64; I2 = 0%). Leave-one-out sensitivity analysis did not materially change the pooled estimate, the detail is shown in Figure 3A.
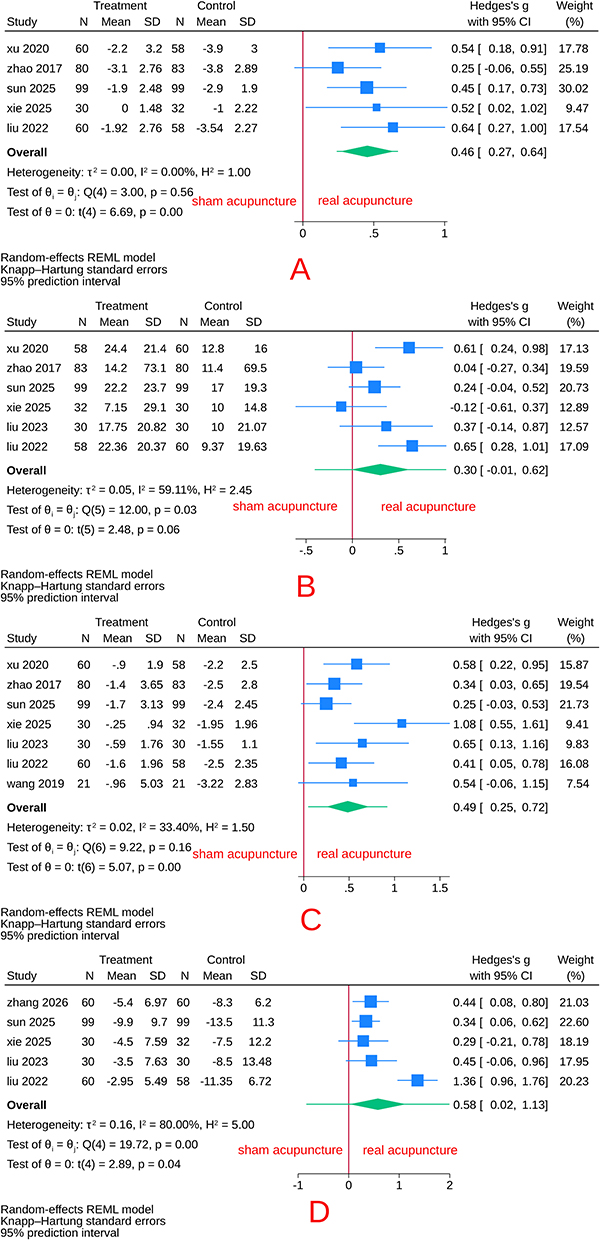 |
Figure 3 Forest plot of acupuncture versus sham acupuncture, using a random-effects REML model with Hartung–Knapp adjustment: (A) for MMD outcome; (B) for MSQ outcome; (C) for pain intensity outcome; (D) for HIT-6 outcome. |
Subgroup analyses by sham type and treatment duration produced estimates like the overall model, indicating no meaningful effect modification. Leave-one-out sensitivity analyses yielded consistent results, confirming the stability and robustness of the pooled MMD estimate, the details are shown in Table 3 and Table 4. The observed reduction in monthly migraine days may be clinically meaningful because even modest reductions in attack frequency can improve daily functioning and reduce medication use.
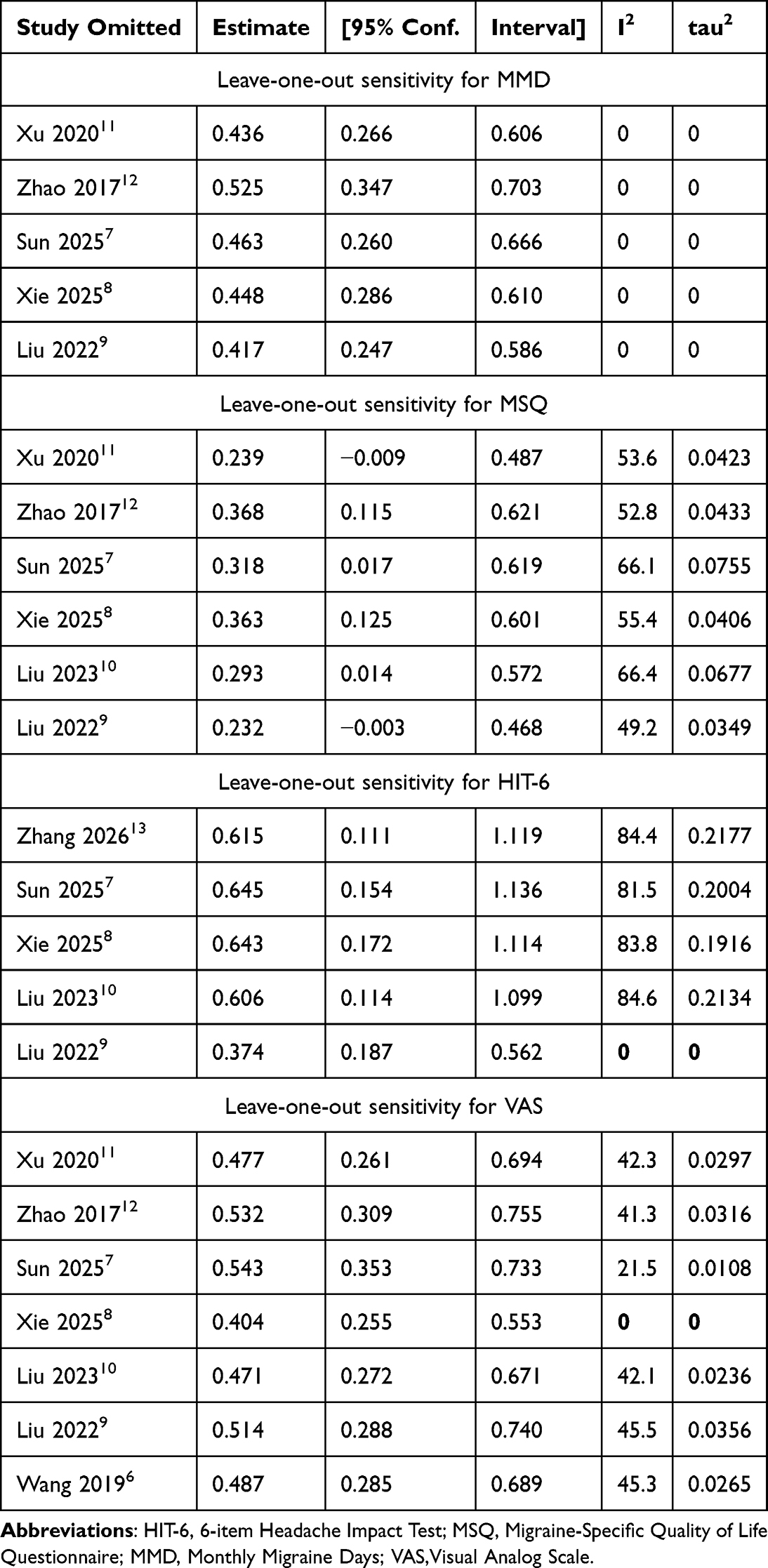 |
Table 3 Sensitivity Analysis for All Outcomes |
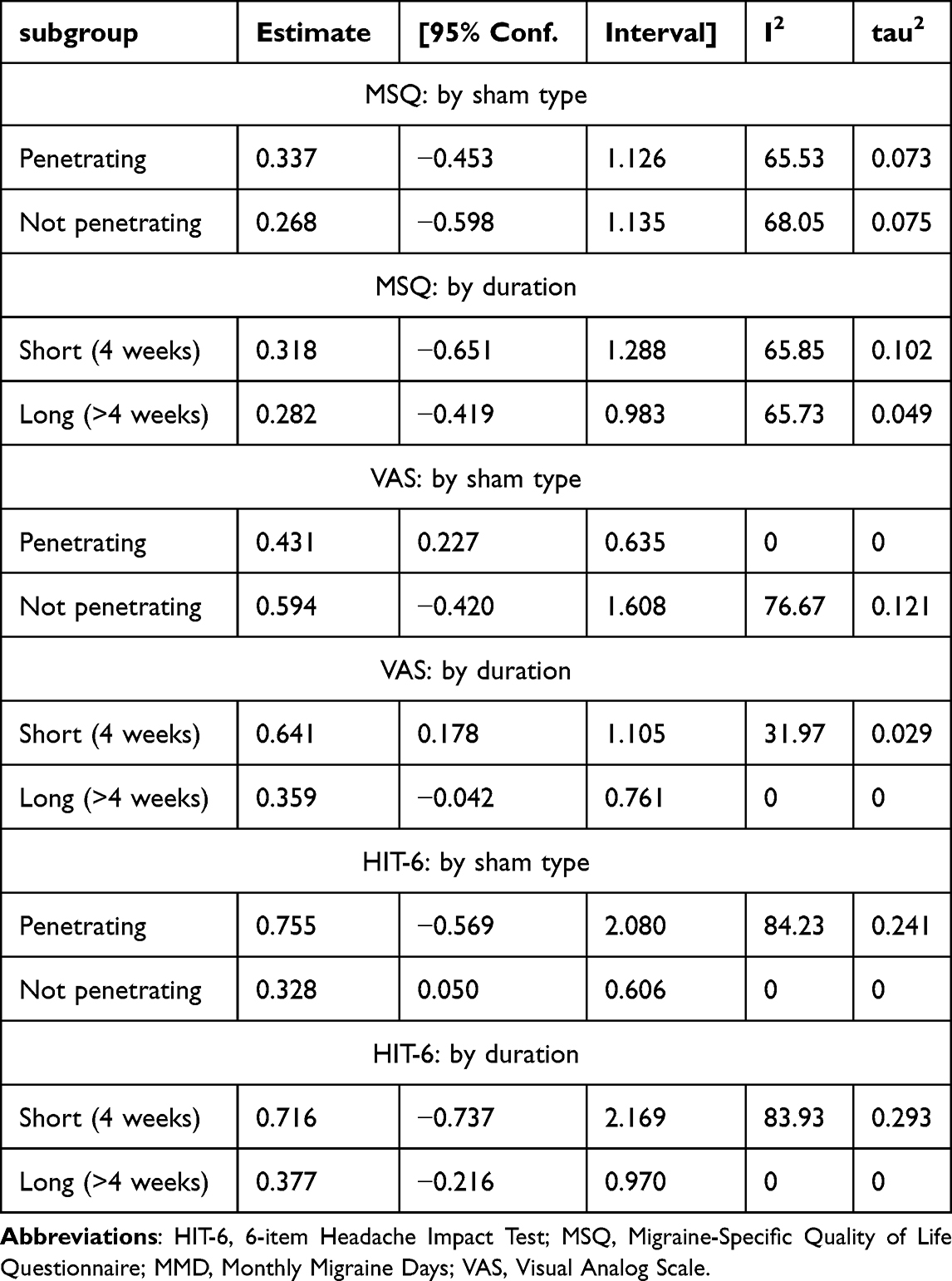 |
Table 4 Subgroup Analysis for All Outcomes |
Secondary Outcomes
Msq
Six trials reported MSQ. The pooled analysis showed a modest improvement favoring acupuncture compared with sham acupuncture, although the overall effect did not reach conventional statistical significance (Hedges’ g = 0.30, 95% CI −0.01 to 0.62). Moderate heterogeneity was observed (I2 = 59%), which is shown in Figure 3B. Subgroup analyses by sham design and treatment duration yielded estimates comparable to the overall model, and sensitivity analyses suggested variability across individual trials without altering the direction of effect (Table 3; Table 4). While the pooled effect size was relatively small, improvements in migraine-specific quality of life may still be clinically meaningful, particularly for patients experiencing substantial impairment in daily activities. Nevertheless, the observed benefit should be interpreted cautiously because between-study heterogeneity was moderate and the certainty of evidence was very low.
Pain Intensity
Seven trials contributed data on pain intensity, six trials measured by VAS and one trial did not mention which tool they used. Acupuncture demonstrated a significant reduction in pain compared with sham treatment (Hedges’ g = 0.49, 95% CI 0.25 to 0.72), with low to moderate heterogeneity (I2 = 33%), which is shown in Figure 3C. Subgroup analyses produced similar estimates. Sensitivity analyses indicated that between-study heterogeneity for VAS was primarily driven by the one study.8 When this trial was excluded, statistical heterogeneity was eliminated (I2 = 0%) while the pooled effect size remained comparable to the primary estimate, indicating that the observed treatment benefit was not dependent on a single study. The magnitude of pain reduction suggests a potentially clinically relevant improvement in symptom burden.
Hit-6
Five trials evaluated headache impact using the HIT-6 scale. The pooled estimate indicated a significant benefit of acupuncture over sham acupuncture (Hedges’ g = 0.58, 95% CI 0.02 to 1.13). Substantial heterogeneity was observed (I2 = 80%) (Figure 3D). Subgroup analyses yielded effect estimates comparable to the primary model. Sensitivity analyses identified one study9 as the principal contributor to heterogeneity. Removal of this trial reduced heterogeneity to negligible levels (I2 = 0%) without materially changing the direction or magnitude of the pooled effect, supporting the robustness of the overall finding (Table 3 and Table 4). The observed improvement in headache impact may be clinically meaningful, although interpretation should be cautious given the substantial heterogeneity.
GRADE Level
According to the GRADE assessment, the certainty of evidence ranged from low to very low across outcomes (Table 5). Evidence for MMD and pain intensity was rated as low certainty, primarily due to unclear randomization methods in some trials, the small number of contributing studies, and imprecision due to limited sample sizes. The certainty for MSQ and HIT-6 was judged very low, reflecting additional concerns related to heterogeneity and imprecision. No serious issues of indirectness were identified (Table 5).
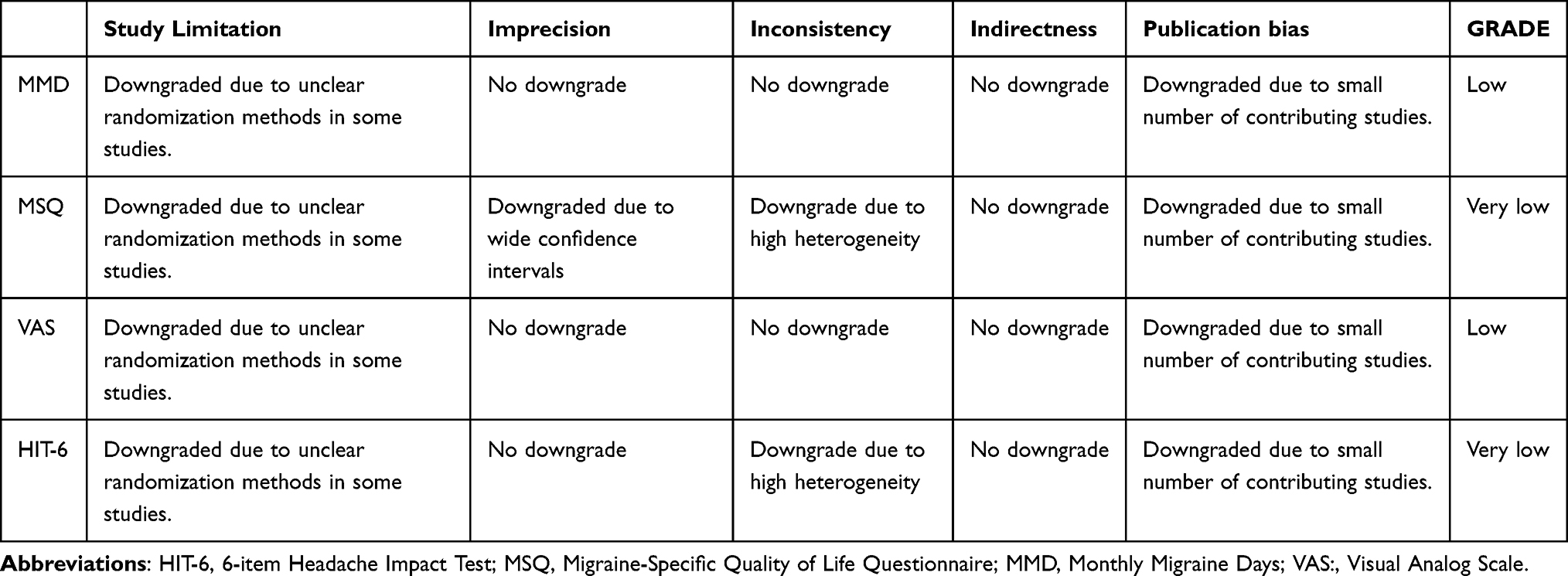 |
Table 5 GRADE Level |
Discussion
This systematic review synthesized sham-controlled randomized trials evaluating acupuncture for migraine without aura. The pooled analyses showed that acupuncture was associated with reductions in monthly migraine days and pain intensity compared with sham procedures, with similar directional effects observed for headache impact. Improvements in migraine-specific quality of life were less certain. However, the certainty of evidence ranged from low to very low, indicating that the magnitude of benefit should be interpreted cautiously.
Our findings should be interpreted in the context of previous evidence syntheses. Xu et al also reported favorable effects of acupuncture for migraine without aura.14 However, unlike the previous review, the present study was restricted exclusively to sham-controlled randomized trials, providing a more specific estimate of acupuncture-related effects beyond placebo responses. In addition, several randomized trials published after 2017 were included, and risk of bias and certainty of evidence were evaluated using the Cochrane RoB 2 tool and GRADE methodology.
The stability of the pooled estimates in sensitivity analyses suggests that the observed effects were not driven by a single influential study, but this should not be interpreted as confirmation of a definitive treatment effect because methodological limitations remained across trials. For outcomes with substantial heterogeneity (MSQ and HIT-6), removal of individual studies in sensitivity analyses markedly reduced I2 without altering the direction of effect, indicating that between-study variability was driven by specific trial characteristics rather than random statistical fluctuation. Trials employing penetrating or intensified sham procedures tended to show smaller between-group differences, suggesting partial physiological activity of the control intervention as a plausible contributor to heterogeneity. Differences in sham design, treatment intensity, and follow-up duration may contribute to variability in treatment estimates. Another important limitation is the heterogeneity of sham acupuncture designs. Included trials used superficial needling, non-penetrating placebo devices, and needling at non-acupuncture locations. Although subgroup analyses were performed, the available evidence remains insufficient to determine whether different sham procedures produce systematically different effect estimates. Future studies should adopt standardized sham acupuncture protocols to improve comparability across trials.
Sham-controlled designs attempt to distinguish specific physiological effects from contextual and expectancy effects, yet this distinction remains challenging in acupuncture research. Previous trials have reported both clinically meaningful differences and minimal separation between real and sham procedures,11 and emerging neuroimaging-based studies further support specific therapeutic effects.13 Structured subgroup and sensitivity analyses have been shown to stabilize pooled estimates despite underlying variability, and removal of influential studies rarely alters overall conclusions.15 Our results follow this pattern, suggesting that the observed treatment effects are unlikely to be driven by single-study influence.
However, evidence remains mixed. Earlier rigorously conducted trials found minimal differences between real and sham acupuncture in migraine day reduction, highlighting the influence of control design and methodological rigor.13 Current guideline assessments continue to issue conditional recommendations, citing variability in reporting standards and procedural transparency.16 These uncertainties underscore the need for more standardized protocols and clearer reporting frameworks.
Several limitations should be considered when interpreting these results. First, the overall number of sham-controlled trials remains limited, which constrains precision and increases vulnerability to publication bias. Second, reporting of randomization and allocation procedures was inconsistent in several studies, contributing to downgrades in evidence certainty. Third, heterogeneity in sham methodology, treatment intensity, and follow-up duration complicates direct comparison across trials, particularly for patient-reported outcomes. An important limitation is that all eight included trials were conducted in China. Consequently, the findings may not be fully generalizable to other ethnic populations, healthcare systems, or acupuncture practice settings. Multinational and multicenter randomized trials are needed to determine whether similar treatment effects can be observed across different cultural and clinical contexts.
Despite these constraints, the current synthesis provides converging evidence that acupuncture may offer clinically meaningful reductions in migraine burden compared with sham interventions. The stability of pooled estimates across sensitivity analyses suggests that the treatment signal is reproducible, although the certainty of evidence remains modest. Future research should prioritize larger multicenter trials with standardized sham protocols, transparent methodological reporting, and longer follow-up intervals to clarify durability of effect. From a broader perspective, these findings support the integration of rigorously evaluated non-pharmacological therapies into migraine management strategies, particularly when individualized patient preferences and treatment tolerability are considered.
Conclusion
In summary, this systematic review and meta-analysis suggests that acupuncture was associated with reductions in migraine frequency and symptom burden compared with sham procedures in patients with migraine without aura. However, the certainty of evidence ranged from low to very low, and the observed effects should therefore be interpreted as suggestive rather than confirmatory. The findings indicate a possible treatment benefit, but they do not establish a definitive therapeutic effect beyond placebo-related influences. The consistency observed across sensitivity analyses suggests a stable statistical pattern, while underscoring the need for cautious interpretation. Well-designed, larger sham-controlled trials with standardized methodologies and longer follow-up are required before firm clinical recommendations can be made.
AI Use Statement
Generative AI (ChatGPT) was used solely for language editing and manuscript preparation. All data extraction, statistical analyses, interpretation of results, and final manuscript content were performed and verified by the authors.
Abbreviation
GRADE, Grading of Recommendations Assessment, Development and Evaluation; HIT-6, 6-item Headache Impact Test; HKSJ, Hartung–Knapp–Sidik–Jonkman; MMD, monthly migraine days; MSQ, Migraine-Specific Quality of Life Questionnaire; MWoA, migraine without aura; REML, restricted maximum likelihood; RoB, risk of bias; SMD, standardized mean difference; VAS, visual analog scale.
Data Sharing Statement
The data extracted from the included studies and used in all analyses are provided within the article and its supplementary materials. The PRISMA 202017 and PRISMA-S checklists,18 along with the full search strategies, are available as supplementary files. Analytic code was not publicly shared but is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Not applicable. This study was a systematic review and meta-analysis of previously published studies and did not involve direct participation of human subjects.
Acknowledgments
The authors would like to thank all participants and research staff who contributed to the included randomized controlled trials and made this study possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lu Y, Li QY, Gan L, et al. The global and regional burden and trends of migraine from 1990 to 2021: global Burden of Disease Study 2021. Front Neurol. 2025;16:1686288. doi:10.3389/fneur.2025.1686288
2. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. BMJ. 2008;336(7651):999–13. doi:10.1136/bmj.39524.439618.25
3. Charles A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. 2018;17(2):174–182. doi:10.1016/S1474-4422(17)30435-0
4. Nie Y, Jing R, Song Z, Zheng H. Utility of acupuncture therapy for adult chronic daily headache prophylaxis: a systematic review and meta-analysis. Med Sci Monit. 2026;32:e952359. doi:10.12659/MSM.952359
5. Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis. Cochrane Database Syst Rev. 2009;1:CD001218. doi:10.1002/14651858.CD001218.pub2
6. Wang Y. Randomized. women’s health research. 2019;11.21.
7. Sun M, Xie C, Wang Y, et al. The prophylactic effect of acupuncture for migraine without aura: a randomized, sham-controlled, clinical trial. J Evid Based Med. 2025;18(3). doi:10.1111/jebm.70059
8. Xie C, Zhang Z, Zhang Y, et al. Multi-spatial voxel-scale modulation of acupuncture on abnormal brain activity in migraine patients without aura: a randomized study neuroimaging trial. Brain Behav. 2025;15(5). doi:10.1002/brb3.70536
9. Liu L, Lyu T, Fu MY, et al. Changes in brain connectivity linked to multisensory processing of pain modulation in migraine with acupuncture treatment. NeuroImage Clin. 2022;36.
10. Liu L, Qi W, Wang Y, et al. Circulating exosomal microRNA profiles in migraine patients receiving acupuncture treatment: a placebo-controlled clinical trial. Front Mol Neurosci. 2023;15.
11. Xu S, Yu L, Luo X, et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: multicentre, randomised clinical trial. BMJ. 2020;368. doi:10.1136/bmj.m697
12. Zhao L, Chen J, Li Y, et al. The long-term effect of acupuncture for migraine prophylaxis a randomized clinical trial. JAMA Intern Med. 2017;177(4):508–515. doi:10.1001/jamainternmed.2016.9378
13. Zhang X, Chen Q, Liu Y, et al. Acupuncture for migraine without aura and connection-based efficacy prediction: a randomized clinical trial. JAMA Network Open. 2026;9(1):e2555454. doi:10.1001/jamanetworkopen.2025.55454
14. Xu J, Zhang FQ, Pei J, Ji J. Acupuncture for migraine without aura: a systematic review and meta-analysis. J Integr Med. 2018;16(5):312–321. doi:10.1016/j.joim.2018.06.002
15. Xu L, Xiang L, Pan L, et al. A Bayesian network meta-analysis of non-pharmacological interventions for neonatal pain management: a clinical effectiveness comparison. Front Pediatr. 2025;13:1547308. doi:10.3389/fped.2025.1547308
16. Cui S, Wang X, Luo Z, et al. Acupuncture recommendations for migraine in headache treatment guidelines: a systematic review. Bull World Health Organ. 2025;103(11):685–95b. doi:10.2471/BLT.25.293420
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
18. Rethlefsen ML, Kirtley S, Waffenschmidt S, et al. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst Rev. 2021;10(1):39. doi:10.1186/s13643-020-01542-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Acupuncture in Treating Nape Back Myofascial Pain Syndrome: a Comprehensive Systematic Review and Meta-Analysis
Zhang P, Zhang Y, Guo M
Journal of Pain Research 2025, 18:1667-1681
Published Date: 29 March 2025
Acupuncture-Based Interventions for Sleep Outcomes in Patients with Postherpetic Neuralgia: A Systematic Review and Meta-Analysis
Zhang J, Zhang J, Chen J, Li Z, Liu X, Chen S
Journal of Pain Research 2026, 19:613776
Published Date: 19 June 2026