Back to Journals » Journal of Pain Research » Volume 19
Acupuncture Therapy Combined with Core Stability Training for Chronic Nonspecific Low Back Pain: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Authors Li X, Yang X, Ye Q, Yang Y, Lu X ![]() , Yuan M, Zhou Y, Zhang J, Chen D
, Yuan M, Zhou Y, Zhang J, Chen D
Received 11 March 2026
Accepted for publication 19 May 2026
Published 26 May 2026 Volume 2026:19 606971
DOI https://doi.org/10.2147/JPR.S606971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Xu Li,1,* Xinyi Yang,2,* Qian Ye,3,4 Yun Yang,3,5 Xinyue Lu,1 Mengqian Yuan,1 Yuntao Zhou,6 Jiajia Zhang,1 Dong Chen1
1Department of Acupuncture and Rehabilitation, Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, People’s Republic of China; 2The First Clinical Medical College, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 3Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 4School of Acupuncture-Moxibustion and Tuina & School of Health Preservation and Rehabilitation, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 5School of Psychology, Nanjing Normal University, Nanjing, People’s Republic of China; 6School of Rehabilitation Medicine, Nanjing Medical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dong Chen, Email [email protected] Jiajia Zhang, Email [email protected]
Background: Chronic nonspecific low back pain (CNSLBP) is a common and disabling condition without identifiable specific pathoanatomical causes. Acupuncture therapy combined with core stability training (AT+CST) are widely used nonpharmacological interventions for CNSLBP. However, the effectiveness and safety of this combined intervention remains controversial. The present study conducted a network meta-analysis to rank the efficacy of different acupuncture modalities combined with core stability training and to identify the optimal treatment strategy, with the aim of informing health policy and guiding clinical practice.
Methods: Randomized controlled trials(RCTs) published from database inception to March 7, 2025, were systematically searched in PubMed, Embase, the Cochrane Library, Web of Science, China National Knowledge Infrastructure, VIP Database for Chinese Technical Periodicals, WANFANG Database, and SinoMed. Manual searches and reference tracking were performed. Pairwise meta-analyses and network meta-analyses were conducted using RevMan and ADDIS software, respectively, and standardized mean differences (SMDs) were calculated. The primary outcome was the Visual Analog Scale (VAS) score. The secondary outcome was the Oswestry Disability Index (ODI) score. Safety was defined as the incidence of adverse events(AEs).
Results: Thirty-two RCTs involving 2726 patients with CNSLBP were included. Available safety data suggested that reported AEs were generally mild, reversible, and infrequent; however, AE reporting was incomplete and heterogeneous across studies. Network meta-analysis indicated that moxibustion combined with unstable surface training ranked highly for reducing VAS scores, but this ranking was supported by limited evidence.
Conclusion: This study suggests that AT+CST may be more effective than single interventions for CNSLBP. Moxibustion combined with unstable surface training may be the optimal strategy, with a favorable safety profile. However, given the methodological limitations and heterogeneity of the current evidence, these findings should be interpreted cautiously. Future high-quality, multicenter RCTs are needed to validate these results.
Keywords: acupuncture therapy, core stability training, chronic nonspecific low back pain, network meta-analysis
Introduction
Low back pain (LBP) is one of the most common musculoskeletal disorders, characterized by high incidence, high recurrence, and substantial disability, with a trend toward affecting increasingly younger populations. A systematic review published in The Lancet (including 165 studies) reported a lifetime prevalence of 84% for LBP, identifying it as the leading cause of disability in 126 countries worldwide, with disability rates increasing significantly with age.1 The majority of patients with LBP present without a clearly identifiable pathoanatomical cause, and when symptoms persist for more than 12 weeks, the condition is defined as chronic nonspecific low back pain (CNSLBP).2 CNSLBP accounts for more than 85% of all LBP cases,3,4 and is typically characterized by persistent lumbosacral pain accompanied by restricted mobility, which often worsens after prolonged static posture or physical exertion. Long-standing chronic LBP is also associated with insomnia and psychological disturbances.5
Given the increasing concerns regarding adverse effects associated with pharmacological treatments for CNSLBP,6–9 non-pharmacological interventions have received growing attention. Although physical therapies, such as core stability training10–13and the McKenzie method,14,15 have demonstrated effectiveness, their benefits remain limited in some patients. Acupuncture, a key modality in traditional Chinese medicine, has been widely investigated in both basic and clinical research. Evidence suggests that acupuncture may relieve pain, regulate hormone secretion, harmonize qi and blood circulation, enhance the body’s self-healing capacity, and improve quality of life.16–18 The combination of acupuncture therapy and physical therapy may exert synergistic effects through multiple mechanisms, such as modulation of pain signaling pathways by acupuncture therapy and improvement of muscle function through physical rehabilitation, thereby potentially enhancing overall therapeutic efficacy.
Previous systematic reviews have evaluated acupuncture-related interventions or acupuncture combined with exercise-based therapies for CNSLBP. A systematic review published in 2017 assessed acupuncture and related nonpharmacological interventions for CNSLBP and suggested potential benefits in improving self-reported pain intensity and functional limitation; however, the findings were limited by methodological heterogeneity and generally low-quality evidence in some included studies.19 More recently, a systematic review published in 2024 examined acupuncture combined with core muscle exercise for CNSLBP and included 11 relevant studies, reporting that the combined intervention was superior to CST alone in improving pain and functional outcomes.20 Nevertheless, previous reviews mainly addressed whether acupuncture combined with CST was effective, but did not sufficiently clarify which specific combination of acupuncture modality and CST approach may provide the greatest clinical benefit.
This evidence gap is clinically important. In current practice, clinicians and policymakers still lack comparative evidence to guide the choice among different acupuncture-related therapies, such as manual acupuncture, electroacupuncture, moxibustion, and acupotomy, and different CST approaches, such as sling-based training and unstable surface training. Conventional pairwise meta-analyses are limited in their ability to simultaneously compare multiple interventions and generate comparative rankings. Network meta-analysis can integrate direct and indirect evidence within a unified framework, allowing comparison and ranking of multiple combined strategies. However, the comparative ranking, inconsistency assessment, safety profile, and robustness of different acupuncture therapy plus CST strategies remain insufficiently established.
Therefore, the present study conducted an updated systematic review and network meta-analysis of randomized controlled trials published up to March 7, 2025, to evaluate acupuncture therapy combined with CST for CNSLBP. This study aimed to compare and rank different combined intervention strategies in terms of pain relief, functional improvement, overall clinical effectiveness, and safety. By moving from the question of “whether the combined therapy is effective” to “which combined strategy may be more promising,” this review seeks to provide more clinically actionable evidence while recognizing the methodological limitations and uncertainty of the current evidence base.
Material and Methods
The present investigation adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)).21 The protocol has been previously registered on PROSEPERO (ID: CRD420251047683).
Methods
A comprehensive electronic search was conducted in eight Chinese and English databases, including PubMed, Embase, the Cochrane Library, Web of Science (WOS), China National Knowledge Infrastructure (CNKI), VIP Database for Chinese Technical Periodicals, WANFANG Database (WF), and SinoMed, from database inception to March 7, 2025.
The search strategy combined Medical Subject Headings (MeSH), subject terms, and free-text terms, covering four key domains: (1) low back pain, low back ache, lumbago; (2) acupuncture-related interventions, including acupuncture, moxibustion, electroacupuncture, electric acupuncture, fire needle, fire acupuncture, warm acupuncture, warm needle, needle-warming moxibustion, heat-sensitive moxibustion, auricular needling, ear needle, acupoint, etc.; (3) physical therapy–related interventions, including physical therapy, physiotherapy, manual therapy, exercise therapy, physical therapy modalities, rehabilitation, physical medicine, occupational therapy, and related truncation terms (eg., rehabilitati*physiotherap*exercis*training); and (4) study design terms, such as clinical trials as topic, randomized controlled trials, and controlled clinical trials.
The complete PubMed search strategy was subsequently adapted for use across the other databases (Supplementary File 1). The search strategy was designed and executed by an evidence-based medicine specialist with expertise in systematic review methodology.
Study Design
This review included all randomized controlled trials (RCTs) published in Chinese and English journals, as well as relevant master’s and doctoral theses. The following study types were excluded: non-randomized clinical studies, literature reviews, news reports, case reports, and trials comparing identical intervention protocols that differed only in treatment duration or frequency.
Participants
Eligible participants were patients clinically diagnosed with chronic nonspecific low back pain (CNSLBP) by a physician. No restrictions were imposed regarding sex, age, or ethnicity. Given that the included RCTs may have applied different diagnostic criteria, participants were required to meet at least one recognized authoritative diagnostic standard, such as the Criteria for Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine issued by the National Administration of Traditional Chinese Medicine.22 Patients were required to have a confirmed diagnosis of CNSLBP with a disease duration of at least 12 weeks and a history of recurrent low back pain. Physical examination findings typically included diffuse tenderness in the lumbosacral region, with tender points commonly located in the erector spinae muscles or lumbar transverse processes; muscle spasm characterized by lumbar muscle tension during examination; or palpable hypertrophy or induration. Laboratory examinations were generally unremarkable. The exclusion criteria were as follows: (1) cases not meeting the diagnostic criteria for CNSLBP; and (2) studies lacking clearly defined diagnostic criteria for CNSLBP or failing to specify explicit inclusion and exclusion criteria.
Types of Interventions
Clear criteria were established for the interventions in both the experimental and control groups: (1) Experimental group: Participants received acupuncture therapy combined with core stability training. Acupuncture therapy interventions included various modalities, such as manual acupuncture, moxibustion, electroacupuncture, fire needling, warm needling, needle-warming moxibustion, auricular acupuncture, and acupotomy. Core stability training encompassed different exercise approaches, including sling exercise therapy and other forms of therapeutic exercise. (2) control group: solely physical therapy or acupuncture therapy (using identical modalities to the intervention group), and placebo (sham acupuncture therapy or other placebo physical therapy). No restrictions were imposed on specific treatment parameters, such as acupoint selection, needling techniques, treatment duration, or frequency. The following studies were excluded: (1) studies with unavailable full texts and/or incomplete data; (2) interventions involving acupuncture combined with pharmacological approaches (eg., acupoint injection or water-injection therapy); (3) studies in which two or more distinct types of acupuncture therapies were simultaneously applied in both the experimental and control groups; (4) exercise interventions not specifically targeting core musculature; (5) studies involving special populations with distinct physiological or training characteristics (eg., professional athletes, postpartum women, or military personnel); (6) studies incorporating pharmacological treatments; and (7) duplicate publications.
Types of Outcome Measures
This study aimed to identify the optimal intervention strategy of acupuncture therapy combined with core stability training for CNSLBP and to evaluate its safety.The primary outcome was the reduction in Visual Analog Scale (VAS) score after treatment. Secondary outcomes included the reduction in Oswestry Disability Index (ODI) score, the improvement in overall clinical effectiveness rate, and the incidence of adverse events (AEs). Pain relief and functional improvement were assessed based on changes in VAS and ODI scores and the proportion of patients achieving clinical effectiveness, while safety was evaluated according to the frequency of AEs. For included RCTs that used numerical rating scales or verbal rating scales, outcomes were converted to a standardized 0–10 VAS scale for analysis. All outcome assessments were restricted to the first evaluation time point immediately after completion of the treatment course.
Study Selection Process
All reviewers received standardized training prior to study selection. Literature management and classification were conducted using Zotero 6.0 software. Two investigators (XL and XY) independently performed literature searching, screening, and data extraction.The screening process consisted of three stages: (1) removal of duplicate and clearly irrelevant records using software, followed by manual verification; (2) secondary screening based on titles and abstracts; (3) full-text review of the remaining studies, with final eligibility determined strictly according to the predefined inclusion and exclusion criteria.After screening, the included studies were cross-checked for consistency. Any disagreements were resolved through discussion with a third investigator (QY) to reach consensus and ensure uniformity in the selection process.
Data Extraction
Data extraction was performed using Microsoft Excel spreadsheets and independently conducted by two investigators (XL and XY). The following information was extracted from each randomized controlled trial (RCT): (1) General study information and bibliometric data: title, first author, year of publication, country or region of study, and number of study arms. (2) Baseline characteristics of participants: mean age, sex distribution, source of cases, duration of disease, and sample size of the experimental and control groups. (3) Intervention details: detailed descriptions of the experimental and control interventions, treatment frequency, and treatment duration. (4) Outcome measures: including Visual Analog Scale (VAS) score, Oswestry Disability Index (ODI) score, overall clinical effectiveness rate, and incidence of adverse events (AEs). (5) Study design characteristics: methodological features related to risk of bias assessment (eg., randomization methods, allocation concealment), diagnostic criteria, and attrition or dropout rates.
Statistical Analysis
Statistical analyses were conducted using Review Manager (RevMan 5.4.1) and Stata 18.0 software. Mean difference (MD) was used as the effect size for continuous outcomes, and statistical significance was defined as P < 0.05 with a 95% confidence interval (CI) not including 0.When different measurement tools were used for the same outcome, standardized mean difference (SMD) with corresponding 95% CIs was calculated for pooled analysis. Statistical heterogeneity among studies was assessed using the Cochran Q test and quantified by the I2 statistic. A significance threshold of P = 0.1 for the Q test and an I2 value of 50% were used to evaluate heterogeneity. If I2 < 50%, a fixed-effects model was applied; if I2 > 50%, potential sources of heterogeneity were further explored before conducting pooled analysis. Results were presented as conventional meta-analysis forest plots. Network meta-analysis was performed to compare different treatment strategies in terms of VAS score, ODI score, and overall effectiveness rate, and results were presented using cumulative probability ranking plots. Based on comparisons of efficacy, safety, and overall effectiveness across interventions for CNSLBP, the relative ranking probabilities were calculated to identify the optimal treatment strategy and to provide evidence-based guidance for the combined use of acupuncture and core stability training. To distinguish between direct and indirect evidence for each comparison, the node-splitting method was applied. Finally, cumulative probability ranking plots were generated to determine the optimal strategy for reducing pain and disability in patients with CNSLBP.
Risk of Bias Assessment
The methodological quality of the included studies was independently assessed by two reviewers (XL and XY). After completing the evaluations, the results were cross-checked. Any discrepancies were resolved through discussion or, if necessary, adjudicated by a third reviewer (QY). The risk of bias of the included RCTs was evaluated using the Cochrane Reviewer’s Handbook (version 5.1.0) risk of bias tool. This tool assesses seven domains: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) completeness of outcome data, (6) selective reporting, and (7) other sources of bias. Each domain was judged as “low risk,” “high risk,” or “unclear risk.”
The overall risk of bias was determined according to the following criteria:23 a trial was considered to be at low risk of bias if all seven domains were rated as low risk, or if fewer than three domains were rated as unclear risk. A trial was considered at high risk of bias if more than two domains were rated as high risk. All other trials were classified as having an unclear overall risk of bias.
Assessment of Publication Bias
Comparison-adjusted or visually inspected funnel plots were constructed to assess potential reporting bias.
Sensitivity Analysis
Sensitivity analyses were performed by excluding small-sample studies (n < 60), large-sample studies (n > 200), or studies at high risk of bias to evaluate the robustness of the pooled results. When statistical heterogeneity was detected, sensitivity analysis was used to explore potential sources. If heterogeneity could not be eliminated and remained below 70%, a random-effects model was applied. Subgroup analyses were conducted following sensitivity analyses.
Patient and Public Involvement
Patients were not involved in the design, conduct, reporting, or dissemination of this study.
Results
Literature Search
A total of 8,791 records were initially identified through comprehensive database searching. After removal of duplicate records using NoteExpress software, 5,603 articles remained. Following screening of titles and abstracts, 137 studies were considered potentially eligible according to the predefined inclusion criteria. After full-text review, studies that did not meet the eligibility criteria were excluded, and a total of 32 randomized controlled trials (RCTs) were ultimately included. Among these, 30 studies were published in Chinese23–53and 2 were published in English.54,55 One study was included solely for methodological quality assessment but was not incorporated into the meta-analysis due to missing outcome data and unsuccessful attempts to contact the authors.24 The detailed study selection process and corresponding results are presented in Figure 1.
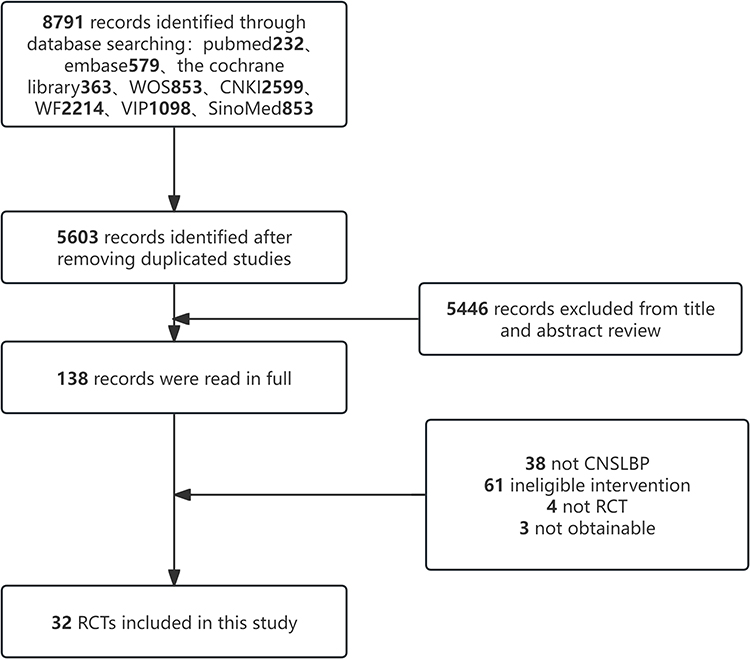 |
Figure 1 Flow chart of study selection. Bold numbers denote the number of records or studies at each stage. |
Characteristics of Included Studies
A total of 32 studies were included in this review. The earliest publications appeared in 2012 (two studies), while the highest annual publication output was observed in 2022, 2023, and 2024, with five studies each. The majority of trials were conducted in China (31/32)23–54and one study was conducted in Korea (1/32).55 Across the 32 RCTs, 2,726 patients with CNSLBP were included. The mean age of participants ranged from 27.23 to 65.21 years. A total of 49 participants were lost to follow-up or withdrew during the study period. The average disease duration ranged from 3 months to 6 years. Among all participants, 51.17% were male. There were no statistically significant differences in baseline characteristics (eg., age and sex) between the experimental and control groups, indicating good comparability. Thirteen types of acupuncture,27–31,37,39,41,43,52 electroacupuncture,32,49–51,54,55 acupotomy,25,26,33,40 fire needling,42 milli-fire needling,24 internal heat acupuncture,35 floating needle therapy,47 tendon acupuncture,38 warm needling moxibustion,34 meridian-sinew moxibustion,36 Du meridian moxibustion,46,53 herbal cake-separated moxibustion,45 and auricular acupressure therapy.48. Among these, manual acupuncture was the most frequently applied intervention (11 studies), followed by electroacupuncture (6 studies), acupotomy (4 studies), and Du meridian moxibustion (2 studies).
Acupoint Selection
Across the included studies, acupoint selection for CNSLBP demonstrated high consistency, generally based on the anatomical location of pain and the meridians associated with the painful region, particularly the Foot Taiyang Bladder Meridian and the Du Meridian. Acupoints were primarily located in the lumbosacral region, including Shenshu (BL23), Dachangshu (BL25), Yaoyangguan (GV3), Weizhong (BL40), Mingmen (GV4) and Ashi points, which are commonly regarded as fundamental points for the treatment of low back pain.
Different acupuncture modalities selected acupoints according to their specific therapeutic principles. For example, electroacupuncture commonly targeted bladder meridian points such as BL23, BL25, Guanyuanshu (BL26), and Zhibian (BL54) to enhance muscular stimulation. Floating needle therapy focused on identifying myofascial trigger points (MTrPs) around affected muscles rather than adhering strictly to traditional meridian points. Du meridian moxibustion was applied along the midline of the spine and adjacent Jiaji (EX-B2) points. Auricular acupuncture targeted corresponding auricular points related to the lumbosacral vertebrae, kidney, and bladder.
In addition, for specific traditional Chinese medicine (TCM) syndrome patterns—such as cold-dampness, blood stasis, or kidney deficiency—acupoints along the Du Meridian or the Foot Shaoyin Kidney Meridian were added to enhance systemic regulation. Some studies were based on specialized theoretical frameworks, such as the meridian-sinew theory, selecting “tendon lesion points” (eg., secondary Shenshu, secondary Dachangshu, or secondary Yaoyan points) for electroacupuncture intervention.
Among the 32 included studies, 24 were two-arm trials,24,25,27,28,30–36,38,40–42,44–48,50–53,55 and 8 were three-arm trials.26,29,36,37,39,43,49,54 For three-arm trials in which two or more intervention arms met the inclusion criteria for the experimental group, the study was divided into separate pairwise comparisons for data analysis (Supplementary File 2).
Methodological Quality Assessment
Among the 32 included studies, 22 reported using randomization methods recommended by the Cochrane Handbook, including 20 studies employing a random number table, 1 using a coin-toss method, and 1 using computer-generated randomization; all of these were assessed as having a low risk of bias for random sequence generation. The remaining studies did not describe the method of randomization and were therefore rated as having an unclear risk. Only one study reported adequate allocation concealment and was assessed as low risk in this domain; the remaining studies did not provide relevant information and were rated as unclear risk. Two studies reported blinding of outcome assessors and were judged to be at low risk of bias. The other studies did not mention blinding procedures and were therefore rated as unclear risk. Eight studies reported participant dropout or attrition with incomplete outcome data; however, the reasons for attrition were clearly described and no significant between-group differences were observed. These studies were therefore assessed as having an unclear risk of bias. The remaining studies reported complete outcome data without attrition and were rated as low risk. All 32 included studies reported complete outcome data for the prespecified endpoints and were therefore judged as low risk for selective reporting. Two studies explicitly declared no conflicts of interest and were assessed as low risk in the “other bias” domain, whereas the remaining studies did not provide relevant information and were rated as unclear risk. None of the included studies reported additional potential sources of bias; therefore, all were assessed as unclear risk in this domain.The detailed results of the risk of bias assessment are presented in Figures 2 and 3.
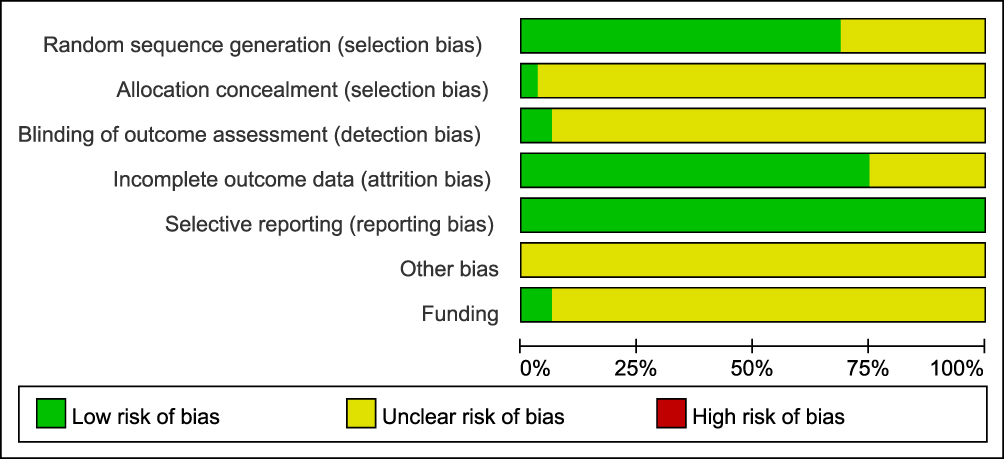 |
Figure 2 Risk of bias graph. |
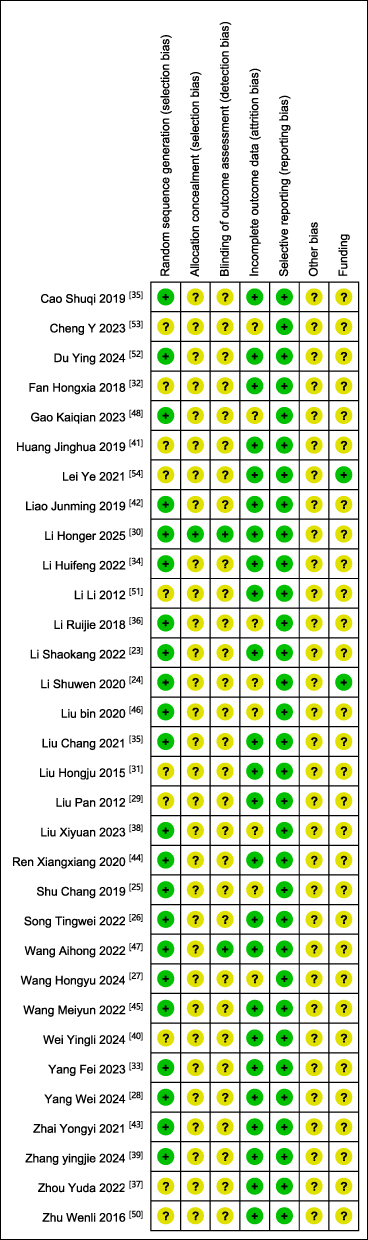 |
Figure 3 Risk of Bias summary. The green circle with a plus sign (+) indicates a low risk of bias, whereas the yellow circle with a question mark (?) indicates an unclear risk of bias due to insufficient or inadequately reported information. |
Meta-Analysis
VAS Score
AT + CST vs. AT
A total of 15 randomized controlled trials (RCTs) involving 1,003 participants were included to evaluate the efficacy of acupuncture therapy combined with core stability training (AT + CST) versus acupuncture therapy alone (AT) in reducing pain scores.26,29,30,32,33,36–38,43,44,49,51,52,54,55 Significant heterogeneity was observed across studies (I2 > 50%); therefore, a random-effects model was applied. The pooled results demonstrated that AT combined with CST was superior to acupuncture alone in reducing Visual Analog Scale (VAS) scores in patients with chronic nonspecific low back pain (CNSLBP) (15 RCTs, MD = −0.98, 95% CI [−1.23, −0.73]) (Figure 4).
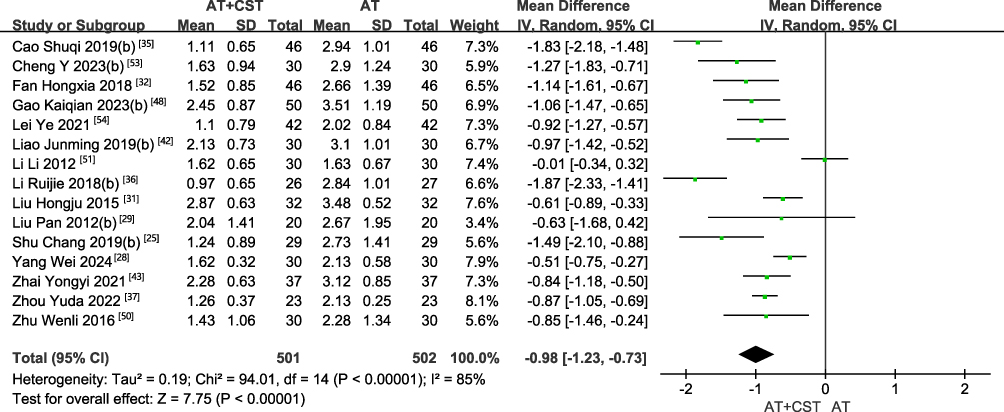 |
Figure 4 The forest plot of VAS scores after acupuncture therapy combined with core stability training versus acupuncture therapy alone for CNSLBP. AT+CST: acupuncture therapy combined with core stability training. The three-arm study was equally divided into two groups (a) and (b). |
To explore the potential sources of heterogeneity related to different acupuncture modalities, subgroup analyses were conducted according to acupuncture type. The included studies comprised 5 trials of acupuncture, 5 of electroacupuncture, 2 of acupotomy, 2 of specialized acupuncture techniques, and 1 of moxibustion. Subgroups of manual acupuncture, specialized acupuncture techniques, and moxibustion demonstrated substantial heterogeneity and were analyzed using random-effects models. In contrast, the electroacupuncture and acupotomy subgroups showed no significant heterogeneity and were analyzed using fixed-effects models. The results indicated that acupuncture (MD = −0.57, 95% CI [−0.92, −0.22]), electroacupuncture (MD = −0.89, 95% CI [−1.12, −0.66]), acupotomy (MD = −1.27, 95% CI [−1.64, −0.90]), specialized acupuncture techniques (MD = −1.35, 95% CI [−2.33, −0.37]), and moxibustion (MD = −0.98, 95% CI [−2.18, −1.48]) combined with core stability training were all superior to control interventions in reducing VAS scores. Heterogeneity analysis suggested that variations in acupuncture modality were likely one of the principal contributors to overall heterogeneity (Figure 5).
 |
Figure 5 The forest plot of VAS scores comparing different types of acupuncture combined with core stability training versus acupuncture therapy alone for CNSLBP. |
To further assess the influence of treatment duration on heterogeneity, subgroup analyses were conducted according to treatment length: <4 weeks (3 studies), 4–8 weeks (10 studies), and >8 weeks (2 studies). Significant heterogeneity persisted across subgroups (I2 > 50%), and random-effects models were applied. The pooled results showed that treatment duration <4 weeks (MD = −0.83, 95% CI [−1.30, −0.36]), 4–8 weeks (MD = −1.00, 95% CI [−1.33, −0.66]), and >8 weeks (MD = −1.11, 95% CI [−1.74, −0.49]) were all associated with significantly greater reductions in VAS scores compared with control interventions. However, no statistically significant heterogeneity was observed between the three duration subgroups (P = 0.76 > 0.05, I2 = 0%), indicating that treatment duration was not a major source of between-study heterogeneity. Similarly, subgroup analysis based on sample size demonstrated that study size was not a significant contributor to heterogeneity (Figure 6).
 |
Figure 6 The forest plot of VAS scores comparing different durations of acupuncture therapy combined with core stability training versus acupuncture therapy alone for CNSLBP. |
In summary, various acupuncture modalities combined with core stability training and different treatment durations were consistently more effective than acupuncture alone in reducing VAS scores. Nevertheless, heterogeneity analyses suggest that future studies should prioritize standardization of acupuncture interventions—particularly manual acupuncture, specialized acupuncture techniques, and moxibustion—to reduce inter-study variability and enhance the reliability of conclusions.
AT + CST vs. CST
A total of 23 randomized controlled trials (RCTs) involving 1,841 participants were included to evaluate the efficacy of acupuncture therapy combined with core stability training (AT + CST) versus core stability training (CST) alone in reducing pain scores.25–28,30,31,34–37,39–43,45–50,53,54 In two studies conducted by Huifeng Li et al35 and Hongyu Wang et al28 the Numeric Rating Scale (NRS) used the same measurement range as the Visual Analog Scale (VAS), and the post-treatment outcomes were reported as mean differences; therefore, these studies were incorporated into the present analysis. Significant heterogeneity was observed among studies (I2 > 50%), and a random-effects model was applied. The pooled results demonstrated that AT combined with CST was superior to CST alone in reducing VAS scores in patients with chronic nonspecific low back pain (CNSLBP) (24 RCTs, MD = −1.25, 95% CI [−1.47, −1.03]) (Figure 7).
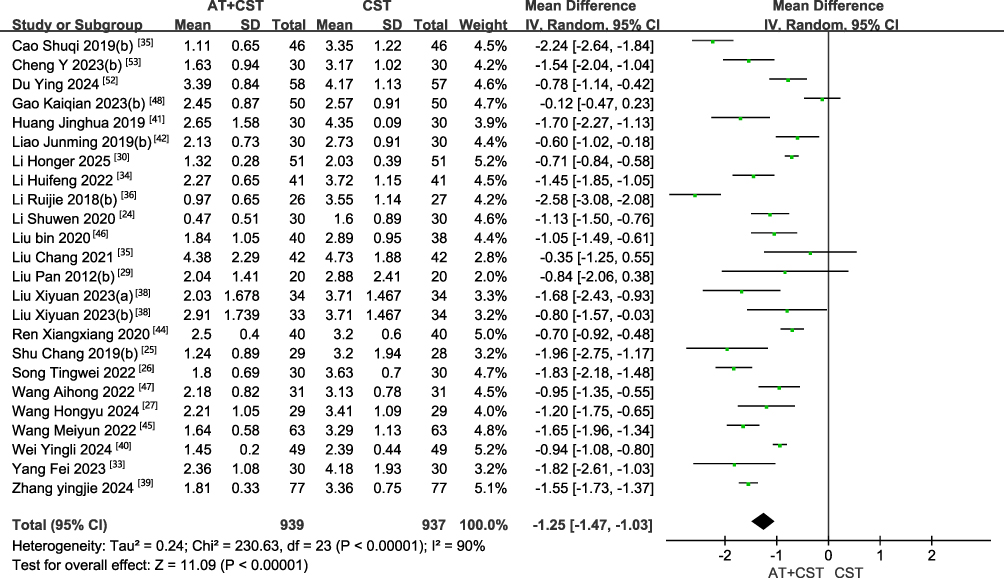 |
Figure 7 The forest plot of VAS scores after acupuncture therapy combined with core stability training versus core stability training alone for CNSLBP. |
To explore whether differences in CST modalities contributed to heterogeneity, subgroup analyses were conducted according to the type of core stability training. The included studies comprised 14 trials of traditional core stability training, 6 of unstable surface training, and 3 of comprehensive core training. Substantial heterogeneity was observed within each subgroup; therefore, random-effects models were applied. The results indicated that traditional core stability training (MD = −1.04, 95% CI [−1.27, −0.82]), unstable surface training (MD = −1.64, 95% CI [−2.23, −1.04]), and comprehensive core training (MD = −1.51, 95% CI [−2.06, −0.95]) combined with acupuncture were all superior to control interventions in reducing VAS scores. Heterogeneity analysis suggested that variations in core stability training modalities were not the primary source of between-study heterogeneity (Figure 8).
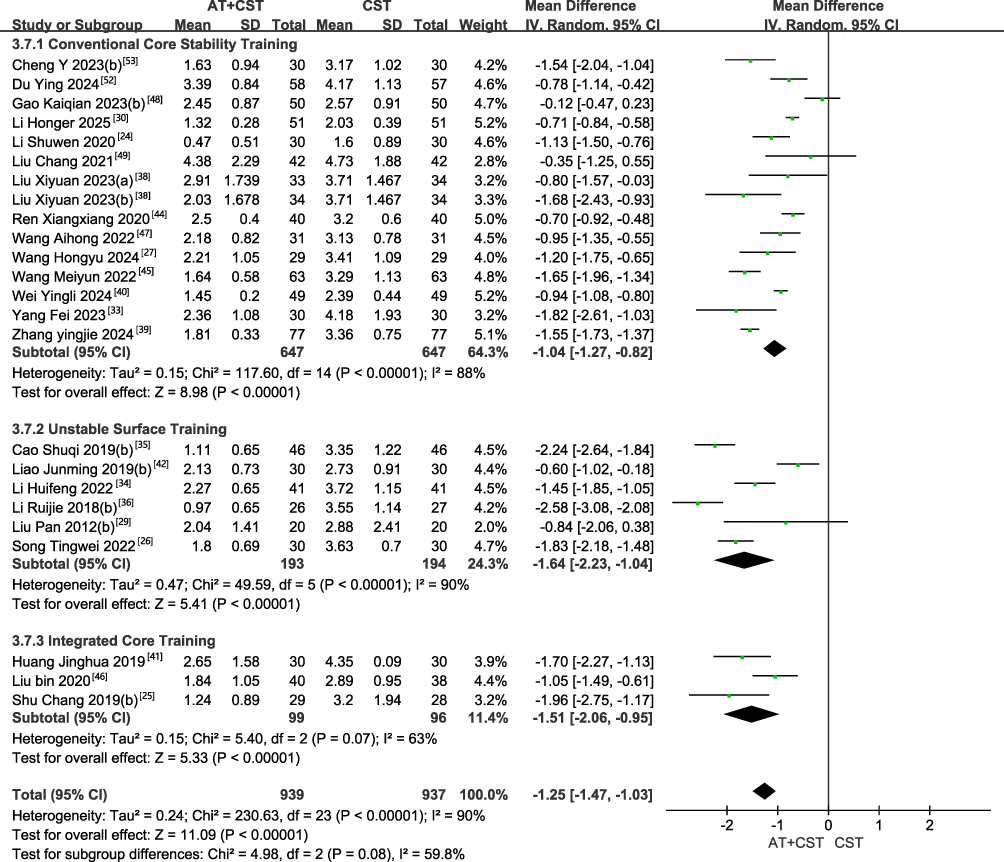 |
Figure 8 The forest plot of VAS scores comparing different types of core stability training combined with acupuncture therapy versus core stability training alone for CNSLBP. |
To further assess the impact of treatment duration on heterogeneity, subgroup analyses were performed according to treatment length: <4 weeks (7 studies), 4–8 weeks (15 studies), and >8 weeks (2 studies). Significant heterogeneity persisted across studies (I2 > 50%), and random-effects models were used. The pooled results showed that treatment duration <4 weeks (MD = −1.28, 95% CI [−1.60, −0.96]), 4–8 weeks (MD = −1.21, 95% CI [−1.57, −0.85]), and >8 weeks (MD = −1.47, 95% CI [−2.27, −0.67]) were all associated with significantly greater reductions in VAS scores compared with control interventions. However, no statistically significant heterogeneity was observed among the three duration subgroups (P = 0.84 > 0.05, I2 = 0%), indicating that treatment duration was not a major contributor to overall heterogeneity. Similarly, subgroup analyses based on sample size demonstrated that study size was not a significant source of heterogeneity (Figure 9).
 |
Figure 9 The forest plot of VAS scores comparing different durations of acupuncture therapy combined with core stability training versus core stability training alone for CNSLBP. |
In summary, acupuncture combined with core stability training was consistently superior to core stability training alone in reducing VAS scores. This combined intervention provides robust evidence-based support as a more effective treatment strategy for CNSLBP and warrants broader application in clinical practice.
ODI Score
AT + CST vs. AT
The Oswestry Disability Index (ODI) was used to assess functional disability related to low back pain. Among the 15 randomized controlled trials (RCTs) included in this comparison, 8 studies26,32,38,43,44,52,54,55 reported ODI outcomes. Significant heterogeneity was observed across studies (I2 = 90% > 50%); therefore, a random-effects model was applied. The pooled analysis demonstrated that acupuncture therapy combined with core stability training (AT + CST) was superior to acupuncture alone (AT) in reducing ODI scores among patients with chronic nonspecific low back pain (CNSLBP) (MD = −4.80, 95% CI [−6.96, −2.65]) (Figure 10).
 |
Figure 10 The forest plot of ODI scores after acupuncture therapy combined with core stability training versus acupuncture therapy alone for CNSLBP. |
AT + CST vs. CST
Among the 23 randomized controlled trials (RCTs) included in this comparison, 14 studies25–27,31,35,39,41–43,45–47,50,54 reported outcomes using the Oswestry Disability Index (ODI). Significant heterogeneity was observed among studies (I2 = 92% > 50%); therefore, a random-effects model was applied. The pooled analysis demonstrated that acupuncture therapy combined with core stability training (AT + CST) was superior to core stability training (CST) alone in reducing ODI scores in patients with chronic nonspecific low back pain (CNSLBP) (MD = −6.47, 95% CI [−7.99, −4.95], Z = 8.34, P < 0.00001) (Figure 11). These findings indicate that, compared with CST alone, the addition of acupuncture to core stability training resulted in an additional mean reduction of 4.32 points in ODI scores, with highly statistically significant differences.
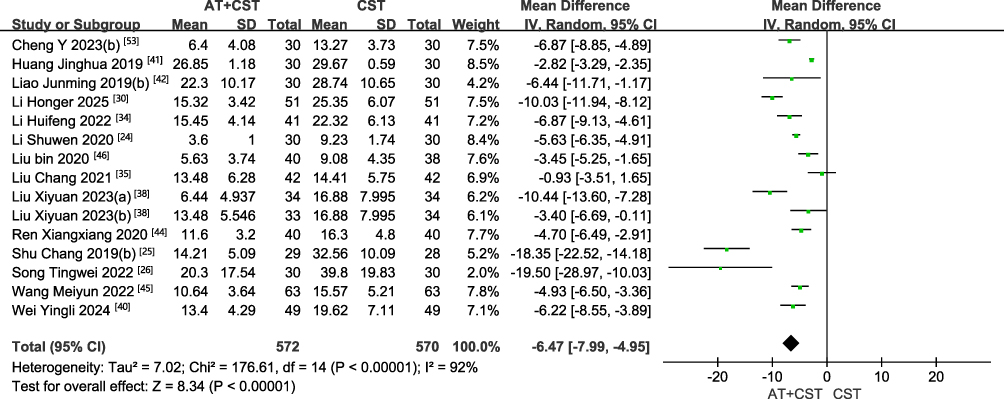 |
Figure 11 The forest plot of ODI scores after acupuncture therapy combined with core stability training versus core stability training alone for CNSLBP. |
Clinical Effectiveness Rate
AT + CST vs. AT
Among the 15 randomized controlled trials (RCTs) included in this comparison, 5 studies30,36,37,43,54 reported overall clinical effectiveness rates. No significant heterogeneity was observed among the studies (I2 = 0%, P = 0.61); therefore, a fixed-effects model was applied. The pooled analysis showed that, compared with acupuncture alone, acupuncture therapy combined with core stability training (AT + CST) significantly improved the overall clinical effectiveness rate by 14% (MD = −0.14, 95% CI [−0.21, −0.07], Z = 4.05, P < 0.0001) (Figure 12). These results indicate that the addition of core stability training to acupuncture therapy significantly enhances clinical effectiveness in patients with chronic nonspecific low back pain.
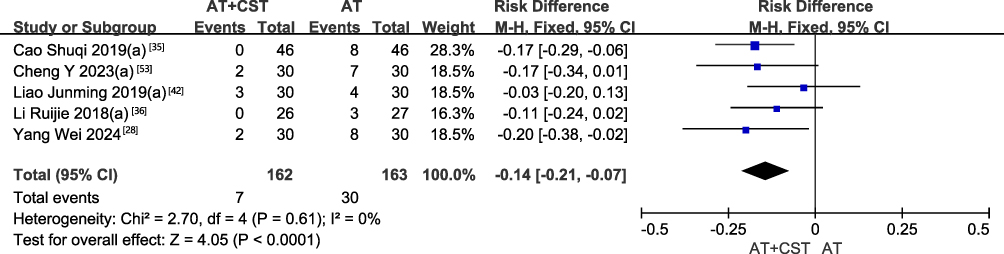 |
Figure 12 The forest plot of clinical effectiveness rate after acupuncture therapy combined with core stability training versus acupuncture therapy alone for CNSLBP. |
AT + CST vs. CST
Among the 23 randomized controlled trials (RCTs) included in this comparison, 15 studies25,27,28,34–37,39–43,50,53,54 reported overall clinical effectiveness rates. No significant heterogeneity was detected among the studies (I2 = 0%, P = 0.71); therefore, a fixed-effects model was applied. The pooled results demonstrated that, compared with core stability training (CST) alone, acupuncture therapy combined with core stability training (AT + CST) significantly reduced the risk of treatment failure by 71% (or, correspondingly, significantly increased the clinical effectiveness rate) (MD = 0.29, 95% CI [0.21, 0.41], Z = 7.15, P < 0.0001) (Figure 13). These findings indicate that acupuncture therapy combined with core stability training confers a significant and consistent advantage over CST alone in improving overall clinical effectiveness in patients with chronic nonspecific low back pain.
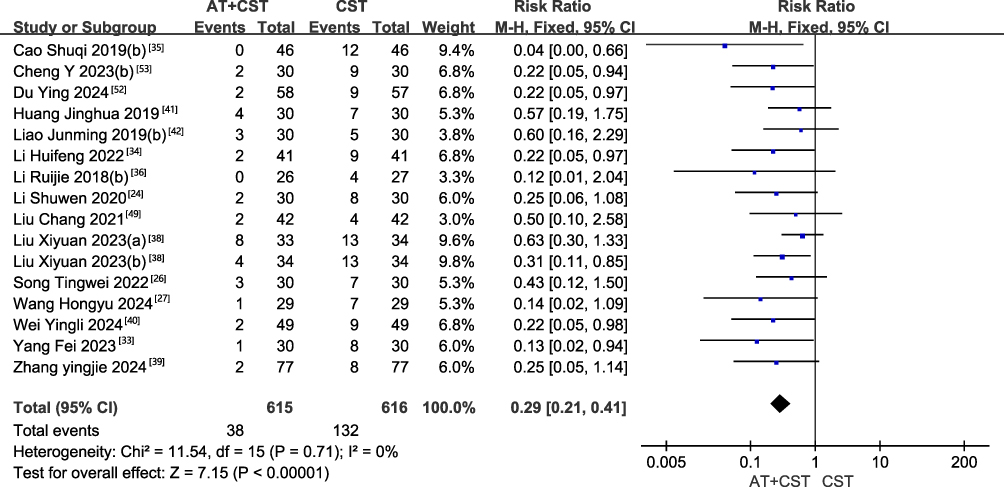 |
Figure 13 The forest plot of clinical effectiveness rate after acupuncture therapy combined with core stability training versus core stability training alone for CNSLBP. |
Network Meta-Analysis
Figure 14 presents the network plots of the different intervention comparisons. For the Visual Analog Scale (VAS) outcome, 31 randomized controlled trials (RCTs) involving a total of 2,614 participants were included, covering 20 distinct intervention strategies (Figure 14a). Among all intervention nodes, the traditional core stability training (CST) alone group had the largest sample size, followed by the unstable surface training alone group. The most frequently investigated comparisons were electroacupuncture versus traditional CST, manual acupuncture versus traditional CST, and manual acupuncture versus unstable surface training. For the Oswestry Disability Index (ODI) outcome, 18 RCTs comprising 1,525 participants were included, involving 17 different intervention strategies (Figure 14b). Consistent with the VAS network, the traditional CST alone group had the largest sample size, and the comparison between manual acupuncture and traditional CST accounted for the highest proportion of studies.
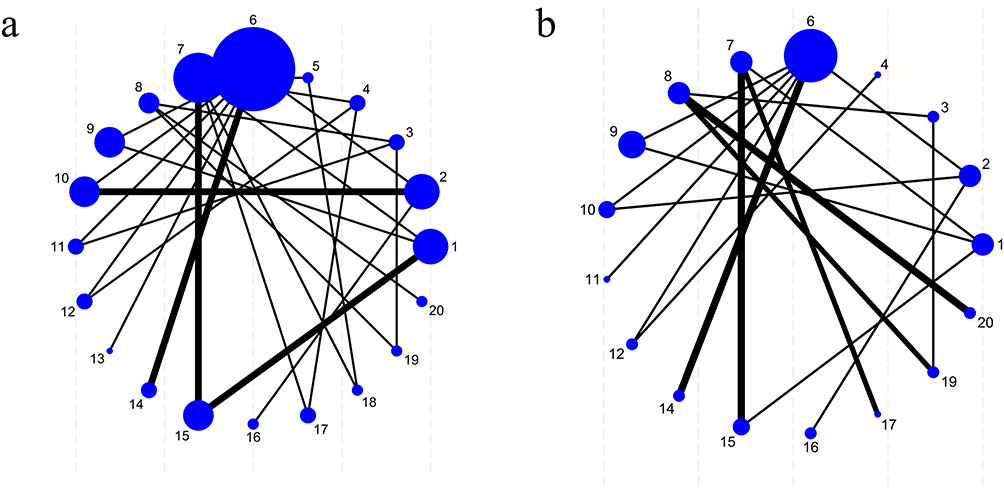 |
Figure 14 Network Evidence Map. (a) VAS; (b) ODI; 1: Acupuncture; 2: Electroacupuncture; 3: Acupotomy; 4: Specialized acupuncture techniques; 5: Moxibustion; 6: Traditional core stability training; 7: Unstable surface training; 8: Comprehensive core training; 9: Acupuncture combined with Traditional core stability training; 10: Electroacupuncture combined with Traditional core stability training; 11: Acupotomy combined with Traditional core stability training; 12: Specialized acupuncture techniques combined with Traditional core stability training; 13: Auricular acupressure combined with Traditional core stability training; 14: Moxibustion combined with Traditional core stability training; 15: Acupuncture combined with Unstable surface training; 16: Electroacupuncture combined with Unstable surface training; 17: Specialized acupuncture techniques combined with Unstable surface training; 18: Moxibustion combined with Unstable surface training; 19: Acupotomy combined with Comprehensive core training; 20: Specialized acupuncture techniques combined with Comprehensive core training. |
The validity of network meta-analysis depends on the internal consistency of the evidence network, meaning that direct and indirect evidence should be in agreement. In the present study, inconsistency was assessed using the node-splitting method (Supplementary File 3). The results showed no statistically significant differences between direct and indirect comparisons for any split node (P > 0.05), indicating no evidence of inconsistency within the network. Model convergence was also evaluated, and the results demonstrated good convergence, with a potential scale reduction factor (PSRF) equal to 1 (Supplementary File 4).
Based on the Surface Under the Cumulative Ranking Curve (SUCRA) values, the interventions were ranked as follows: Moxibustion + unstable surface training > Specialized acupuncture techniques + unstable surface training > Acupotomy + comprehensive core training > Acupuncture + unstable surface training > Specialized acupuncture techniques + comprehensive core training > Acupuncture + traditional core stability training > Unstable surface training > Comprehensive core training > Acupotomy > Specialized acupuncture techniques > Moxibustion > Electroacupuncture + traditional core stability training > Traditional core stability training > Manual acupuncture > Electroacupuncture > Acupotomy + traditional core stability training > Specialized acupuncture techniques + traditional core stability training > Auricular acupressure + traditional core stability training > Moxibustion + traditional core stability training > Electroacupuncture + unstable surface training (Supplementary File 5 and Figure 15).
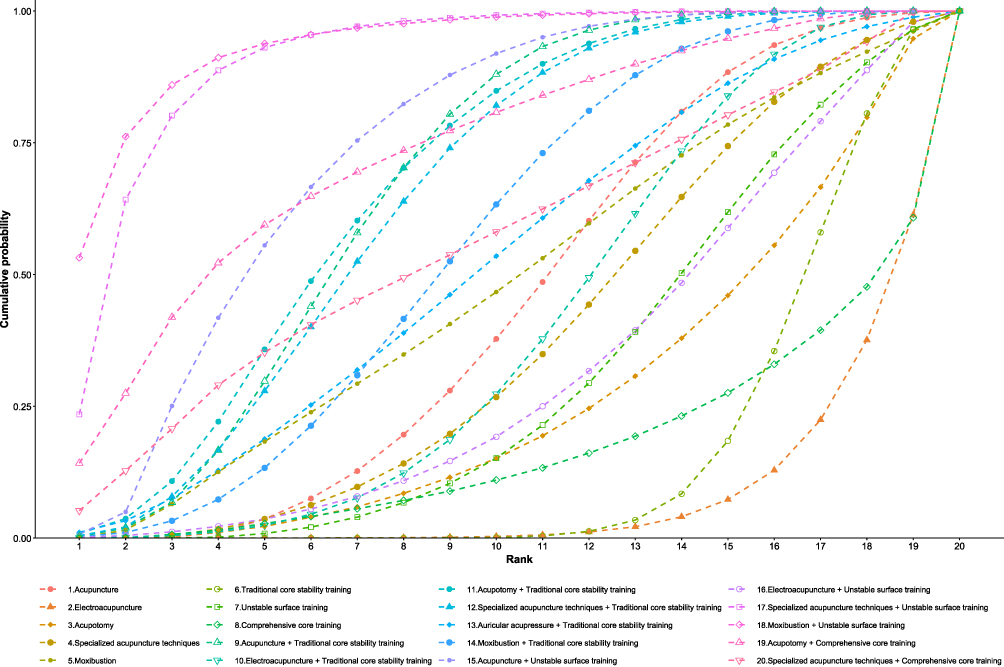 |
Figure 15 The Cumulative ranking plot (SUCRA) of VAS score improvement for different acupuncture therapies, core stability training, and their combination. |
Because the evidence network for the Oswestry Disability Index (ODI) did not form a fully connected structure and therefore did not meet the fundamental assumptions required for network meta-analysis (Figure 14b), a descriptive analysis was conducted for ODI outcomes instead.
Publication Bias
Publication bias was assessed by constructing comparison-adjusted funnel plots (Figures 16 and 17). Because the evidence network for the Oswestry Disability Index (ODI) did not form a fully connected structure, network comparison–adjusted funnel plot analysis could not be performed for this outcome; therefore, a conventional funnel plot was generated and analyzed instead (Figures 17). The funnel plots for both the Visual Analog Scale (VAS) and ODI outcomes demonstrated that most study points were symmetrically distributed on either side of the central line and were primarily concentrated in the middle region. This pattern suggests that the included studies generally had moderate sample sizes and that the overall risk of publication bias was relatively low.
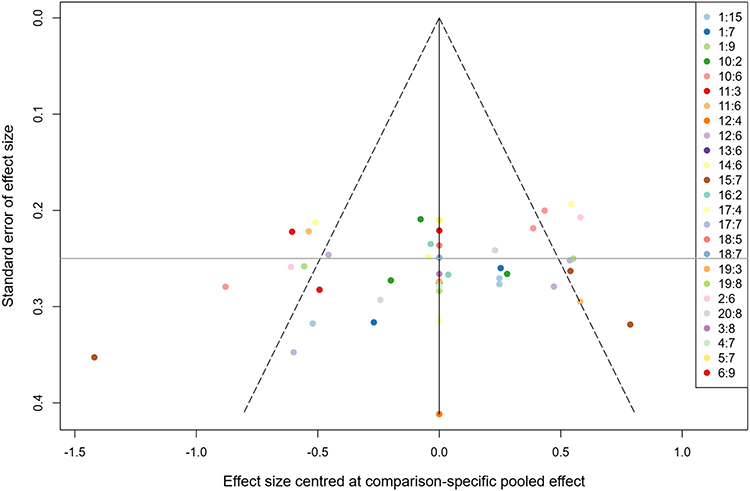 |
Figure 16 Funnel plot of network meta-analysis in VAS score. 1: Acupuncture; 2: Electroacupuncture; 3: Acupotomy; 4: Specialized acupuncture techniques; 5: Moxibustion; 6: Traditional core stability training; 7: Unstable surface training; 8: Comprehensive core training; 9: Acupuncture combined with Traditional core stability training; 10: Electroacupuncture combined with Traditional core stability training; 11: Acupotomy combined with Traditional core stability training; 12: Specialized acupuncture techniques combined with Traditional core stability training; 13: Auricular acupressure combined with Traditional core stability training; 14: Moxibustion combined with Traditional core stability training; 15: Acupuncture combined with Unstable surface training; 16: Electroacupuncture combined with Unstable surface training; 17: Specialized acupuncture techniques combined with Unstable surface training; 18: Moxibustion combined with Unstable surface training; 19: Acupotomy combined with Comprehensive core training; 20: Specialized acupuncture techniques combined with Comprehensive core training. |
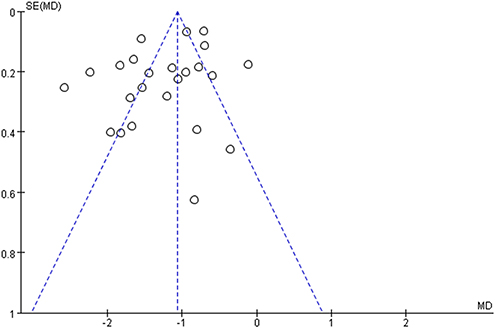 |
Figure 17 Funnel plot of meta-analysis in ODI score. |
Discussion
In recent years, an increasing number of studies have investigated acupuncture combined with core stability training for the treatment of chronic nonspecific low back pain (CNSLBP). Most have suggested beneficial effects on pain relief and functional improvement. However, the combinations of acupuncture modalities (eg., manual acupuncture, electroacupuncture, acupotomy) and core stability training approaches (eg., traditional core stability training, unstable surface training, comprehensive core training) vary considerably. Suboptimal therapeutic strategies may not only compromise clinical recovery in patients with CNSLBP but also lead to inefficient use of healthcare resources. Therefore, the present study conducted a systematic review and network meta-analysis (NMA) to identify the most effective combined treatment strategy for CNSLBP, thereby providing evidence-based guidance for clinical practice.
In this study, 32 randomized controlled trials (RCTs) evaluating acupuncture combined with core stability training for CNSLBP were assessed for methodological quality using the Cochrane risk-of-bias tool. Across the seven domains—including random sequence generation, allocation concealment, and blinding procedures—only two studies were rated as having a low overall risk of bias, while 30 studies (93.75%) were classified as having unclear risk. These findings indicate that the current body of evidence is still limited by methodological shortcomings. To mitigate the potential impact of bias on the study conclusions, sensitivity analyses were conducted. The pooled results remained largely consistent across most key comparisons, suggesting that the overall findings demonstrate a reasonable degree of robustness and strengthening confidence in the primary conclusions.
Furthermore, this study conducted both pairwise meta-analyses and network meta-analysis (NMA) based on 32 randomized controlled trials involving 2,726 patients with chronic nonspecific low back pain (CNSLBP). The findings demonstrated that acupuncture therapy combined with core stability training (AT + CST) was significantly superior to acupuncture therapy alone (AT) or core stability training alone (CST) in reducing Visual Analog Scale (VAS) scores, improving Oswestry Disability Index (ODI) scores, and increasing overall clinical effectiveness rates. In the network meta-analysis, moxibustion combined with unstable surface training ranked highly for reducing VAS scores. This result may reflect the potential complementary effects of thermal stimulation and proprioceptive or neuromuscular training. Moxibustion may provide local thermal stimulation and may be associated with pain-relieving effects, while unstable surface training challenges postural control and may enhance deep trunk muscle activation and lumbar stability. From a mechanistic perspective, the superiority of moxibustion combined with unstable surface training may be attributed to its dual effects: localized thermal stimulation and neuromuscular functional reconstruction. Previous studies have suggested that moxibustion may increase pain thresholds by improving local blood circulation, modulating inflammatory mediators, and regulating neural excitability.56 Meanwhile, unstable surface training facilitates activation of deep core musculature and enhances neuromuscular control, thereby improving lumbar stability and reducing the mechanical basis of pain.57 Recent evidence comparing active, passive, and combined physiotherapy approaches in chronic low back pain has highlighted the importance of active rehabilitation strategies.58 This is consistent with our finding that combined interventions involving core stability training may improve pain and functional outcomes. The combination of these modalities may therefore produce synergistic effects at both the “analgesia” and “functional restoration” levels. However, caution is warranted in interpreting these findings. These conclusions are based on limited evidence and a small number of studies. Therefore, further high-quality randomized controlled trials are needed to validate these results. Specialized acupuncture techniques combined with unstable surface training also demonstrated favorable analgesic effects. In contrast, electroacupuncture combined with unstable surface training ranked relatively lower in the present analysis. These findings imply that within the “acupuncture + training” paradigm, the training platform (eg., unstable surface) alone does not guarantee equivalent analgesic enhancement across all acupuncture modalities. Rather, the analgesic advantage may depend on the interaction between the type of stimulation and the form of training. For example, the thermal effects of moxibustion—improving local circulation and modulating myofascial tension—may synergize more effectively with deep stabilizing muscle recruitment induced by unstable surface training, thereby resulting in superior pain relief.
It is noteworthy that some studies did not merely adopt an empirical “acupuncture + training” combination, but instead incorporated specific theoretical frameworks—such as meridian-sinew theory, the cervico-lumbar co-treatment theory, tension balance theory, and movement pattern correction theory—to systematically design acupoint selection and exercise prescriptions. For example, studies grounded in the cervico-lumbar co-treatment concept or the global kinetic chain theory selected cervical acupoints or targeted upstream muscle groups in addition to lumbar interventions.39 Meanwhile, studies based on movement pattern correction or exercise-acupuncture theory emphasized the synchronous application of acupuncture stimulation with specific motor tasks to facilitate reconstruction of central–peripheral motor control pathways.41
Regarding heterogeneity, this study found that variations in acupuncture modality contributed substantially to treatment heterogeneity. This may be partly attributable to insufficient standardization in acupoint selection and needling techniques across trials.
Because the evidence network for the Oswestry Disability Index (ODI) outcome did not form a fully connected structure and thus did not meet the fundamental assumptions for network meta-analysis, a descriptive analysis was performed for ODI results. The findings indicated that, compared with single-modality interventions, combined treatment strategies incorporating core stability training generally demonstrated greater improvements in ODI scores. This suggests that such integrative approaches may have advantages in ameliorating low back pain–related functional disability. Overall, the direction of ODI improvement was consistent with the results of the VAS network meta-analysis, indicating that comprehensive acupuncture-based interventions may not only relieve pain but also promote functional recovery.
In addition, this study systematically reviewed reports of adverse events among the 32 included randomized controlled trials. Overall, most studies did not provide standardized safety reports on adverse reactions, offering only brief records with inconsistent reporting formats. Therefore, a quantitative summary analysis of adverse events cannot be conducted. The most commonly reported adverse events included transient exacerbation of pain, local soreness or distension, and occasional vasovagal reactions (eg., dizziness, chest discomfort, cold sweating). Pain aggravation was typically observed shortly after acupuncture or acupotomy procedures, or during the early stages of core stability training due to inappropriate load adjustment. These symptoms generally manifested as temporary muscle soreness or transient worsening of baseline pain and resolved spontaneously within hours to days without specific intervention. In studies involving acupotomy or stronger stimulation techniques, a few cases of needle-related syncope were reported, along with rare instances of mild bleeding or local subcutaneous bruising. All resolved after brief rest in the supine position or simple symptomatic management, with no serious sequelae. No studies reported major adverse events such as severe infection, nerve injury, or permanent functional impairment. For core stability or motor control training, most studies did not report specific adverse reactions, suggesting good tolerability when exercises were performed under appropriate supervision. Taken together, adverse events associated with acupuncture-related interventions and core stability training were generally mild, reversible, and infrequent, with no serious safety concerns identified. Overall, acupuncture combined with core stability training appears to be a safe and acceptable therapeutic approach for the management of chronic nonspecific low back pain.
Strengths
This study has several notable strengths. First, to ensure comprehensive literature retrieval, we searched eight major Chinese and English databases in addition to conducting manual searches.Second, it compared multiple acupuncture therapies and CST approaches within a unified evidence network, extending beyond previous pairwise meta-analyses that mainly assessed whether combined therapy was effective. Finally, the study considered not only pain and functional outcomes but also overall clinical effectiveness, safety, model consistency, and treatment ranking. These features may provide useful preliminary evidence for clinicians when considering combined nonpharmacological strategies for CNSLBP.
Limitations
Several limitations should be acknowledged. First, 31 of the 32 included studies were conducted in China (with only one study from Korea), and most participants were of Asian ethnicity. Therefore, the generalizability of the findings to Western populations—considering potential differences in musculoskeletal characteristics and lifestyle factors—may be limited. Additionally, we extracted baseline data and the first post-treatment outcome only. Variations in treatment duration and intervention cycles across studies may have introduced bias, and the absence of long-term follow-up data (eg., 6-month or 1-year recurrence rates) prevents definitive conclusions regarding the sustained effects of AT + CST. Second, although we rigorously assessed methodological quality using the Cochrane risk-of-bias tool, the overall quality of included trials was moderate to low. This may partly reflect the inherent challenges of acupuncture research, where double-blinding of practitioners and participants is often impractical, potentially increasing the risk of performance and detection bias. Third, heterogeneity was detected in several pairwise meta-analyses. Although random-effects models were applied, the pooled estimates may still be subject to imprecision. Fourth, because the ODI evidence network was not fully connected (with some interventions lacking direct or indirect comparisons), only descriptive analysis could be conducted, and precise ranking was not feasible. Fifth, several studies did not report key technical details—such as needling depth, needle retention time, or specific intensity parameters of core training—and some lacked detailed descriptions of acupuncture procedures, limiting reproducibility in clinical practice. Finally, a notable limitation is the ranking of “Moxibustion + Unstable surface training” as the top intervention, which was based on limited evidence. Although network meta-analysis allows the incorporation of indirect evidence, the SUCRA value for this node may be unstable because of the small number of contributing studies.
Conclusion
This study suggests that AT+CST may be more effective than single interventions for CNSLBP. Moxibustion combined with unstable surface training may represent the optimal strategy, offering good safety profiles and thus may be promising. Although methodological limitations exist, the current evidence supports its clinical application. International research teams urgently need to conduct high-quality, multicenter randomized controlled trials (RCTs) to verify whether these findings are applicable to non-Asian populations. Meanwhile, Given the methodological limitations, heterogeneity, short-term outcome assessment, and regional concentration of the current evidence, future high-quality, multicenter randomized controlled trials are needed to validate these findings.
Abbreviations
LBP, Low back pain; CNSLBP, chronic nonspecific low back pain; GRADE,Grading of Recommendations Assessment, Development and Evaluation; WOS, Web of Science; CNKI, China National Knowledge Infrastructure; VIP, CQVIP; WF, WANFANG Database; MeSH, Medical Subject Headings; RCTs, randomized controlled trials; VAS, Visual Analog Scale; ODI, Oswestry Disability Index; AEs,adverse events; MD, Mean difference; CI, confidence interval; SMD, standardized mean difference; MTrPs, myofascial trigger points; TCM,traditional Chinese medicine; AT, acupuncture therapy; CST, core stability training; 95% CI, 95% confidence interval; PSRF, potential scale reduction factor; SUCRA, surface under the cumulative ranking area; NMA, network meta-analysis.
Author Contributions
XL and XY designed and registered the project. XL, XY, and QY screened the literature. XL,QY and YY extracted the relevant data and evaluated the quality of RCTs. XL and XY conducted the statistical analysis of the data. XL and XY drafted the manuscript. XL, YZ, JZ DCMY and MY supervised the implementation of the entire study and provided guidance. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Fourth Batch Peak Academic Talents Training Project, Jiangsu Provincial TCM Hospital (k2026yrc52).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–23. doi:10.1016/S0140-6736(16)30970-9
2. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379(9814):482–491. doi:10.1016/S0140-6736(11)60610-7
3. Lurie JD. What diagnostic tests are useful for low back pain. Best Pract Res Clin Rheumatol. 2005;19(4):557–575. doi:10.1016/j.berh.2005.03.004
4. Koes BW, Van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. BMJ. 2006;332(7555):1430–1434. doi:10.1136/bmj.332.7555.1430
5. Aroke EN, Wiggins AM, Hobson JM, et al. The pace of biological aging helps explain the association between insomnia and chronic low back pain. Mol Pain. 2023;19:17448069231210648. doi:10.1177/17448069231210648
6. Whittle SL, Richards BL, Husni E, Buchbinder R. Opioid therapy for treating rheumatoid arthritis pain. Cochrane Database Syst Rev. 2011. doi:10.1002/14651858.CD003113.pub3
7. Buch MH, Emery P. New therapies in the management of rheumatoid arthritis. Curr Opin Rheumatol. 2011;23(3):245–251. doi:10.1097/BOR.0b013e3283454124
8. Solomon DH, Rassen JA, Glynn RJ, et al. The comparative safety of opioids for nonmalignant pain in older adults. Arch Intern Med. 2010;170(22):1979–1986. doi:10.1001/archinternmed.2010.450
9. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015;162(4):276–286. doi:10.7326/M14-2559
10. Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–2803. doi:10.1007/s00586-018-5673-2
11. Deodato M, Saponaro S, Šimunič B, Martini M, Murena L, Buoite Stella A. Trunk muscles’ characteristics in adolescent gymnasts with low back pain: a pilot study on the effects of a physiotherapy intervention including a postural reeducation program. J Man Manip Ther. 2024;32(3):310–324. doi:10.1080/10669817.2023.2252202
12. Shamsi MB, Rezaei M, Zamanlou M, Sadeghi M, Pourahmadi MR. Does core stability exercise improve lumbopelvic stability (through endurance tests) more than general exercise in chronic low back pain? A quasi-randomized controlled trial. Physiother Theory Pract. 2016;32(3):171–178. doi:10.3109/09593985.2015.1117550
13. Fischer SC, Calley DQ, Hollman JH. Effect of an exercise program that includes deadlifts on low back pain. J Sport Rehabil. 2021;30(4):672–675. doi:10.1123/jsr.2020-0324
14. Namnaqani FI, Mashabi AS, Yaseen KM, Alshehri MA. The effectiveness of McKenzie method compared to manual therapy for treating chronic low back pain: a systematic review. J Musculoskelet Neuronal Interact. 2019;19(4):492–499.
15. Lam OT, Strenger DM, Chan-Fee M, Pham PT, Preuss RA, Robbins SM. Effectiveness of the McKenzie method of mechanical diagnosis and therapy for treating low back pain: literature review with meta-analysis. J Orthop Sports Phys Ther. 2018;48(6):476–490. doi:10.2519/jospt.2018.7562
16. Liu L, Skinner M, McDonough S, Mabire L, Baxter GD. Acupuncture for low back pain: an overview of systematic reviews. Evid Based Complement Alternat Med. 2015;2015:328196. doi:10.1155/2015/328196
17. Mu J, Furlan AD, Lam WY, Hsu MY, Ning Z, Lao L. Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst Rev. 2020;12(12):CD013814. doi:10.1002/14651858.CD013814
18. Lu L, Zhang Y, Ge S, et al. Evidence mapping and overview of systematic reviews of the effects of acupuncture therapies. BMJ Open. 2022;12(6):e056803. doi:10.1136/bmjopen-2021-056803
19. Yeganeh M, Baradaran HR, Qorbani M, Moradi Y, Dastgiri S. The effectiveness of acupuncture, acupressure and chiropractic interventions on treatment of chronic nonspecific low back pain in Iran: a systematic review and meta-analysis. Complement Ther Clin Pract. 2017;27:11–18. doi:10.1016/j.ctcp.2016.11.012
20. Li X, Zhai G, Zhang H, et al. Clinical efficacy of acupuncture therapy combined with core muscle exercises in treating patients with chronic nonspecific low back pain: a systematic review and meta-analysis of randomized controlled trials. Front Med. 2024;11:1372748. doi:10.3389/fmed.2024.1372748
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
22. Spinal Cord and Spine Professional Committee Research Group, Chinese Association of Rehabilitation Medicine. Expert consensus on acute/chronic nonspecific low back pain in China. Chin J Spine Spinal Cord. 2016;26(12):1134–1138.
23. Ye L, Jiaqi Z, Jianchao W, Zhaohui F, Liang Y, Xiaohui Z. Comparative efficacy and safety of anti-vascular endothelial growth factor regimens for neovascular age-related macular degeneration: systematic review and Bayesian network meta-analysis. Ther Adv Chronic Dis. 2020;11:2040622320953349. doi:10.1177/2040622320953349
24. Shaokang L, Jie Z, Xiaowen C, Sen Z, Sheqing L, Yuanxiao F. Core stability training combined with acupuncture in treatment of chronic nonspecific low back pain: a prospective randomized controlled trial. Acupuncture Res. 2022;47(2):160–164. doi:10.13702/j.1000-0607.201050
25. Shuwen L, Xiangdong T, Guangyu Z, et al. Observation of the curative effect of acupotomy combined with lumbar and back muscle core stability training on chronic nonspecific low back pain. Mod J Integr Tradit Chin Western Med. 2020;29(13):1401–1404,1409.
26. Chang S. Observation of the Efficacy of Needle Scalpel Therapy Combine Core Stability Training in the Treatment of Chronic Non-Specific Low Back[Dissertation]. Zhejiang:University of Traditional Chinese Medicine. 2020.
27. Tingwei S, Zhiqiang K. Clinical observation on acupuncture at the four-side points around the umbilicus combined with core muscle training under suspension for nonspecific low back pain. JETCM. 2022;31(12):2194–2196.
28. Hongyu W, Xinjie Y, Xiaoyan Q. Research on acupuncture combined with motor control training for chronic non-specific low back pain. TCM Res. 2024;37(12):55–58.
29. Wei Y, Jinzhong T, Songtao L, et al. Clinical observation of acupuncture combined with sling exercise therapy for nonspecific low back pain. JHunan Univer Chin Med. 2024;44(4):600–605.
30. Pan L. Clinical Observation of Acupuncture Combined with Scale of Exercise Therapy in the Treatment of Nonspecific Chronic Low Pain[Dissertation]. Shandong: Shandong University of Traditional Chinese Medicine; 2013.
31. Honger L, Shaowen L, Yindi L, Jiexuan L, Aiguo X, Shuxiong L. Observation on the clinical efficacy of tension balance acupuncture combined with core muscle training in treating chronic nonspecific low back pain. Tianjin J Traditional Chin Med. 2025;42(2):158–162.
32. Hongju L, Sigang Z, Yunfeng Q, Ling D, Ting Q, Yunlong F. Observation on the therapeutic effect of lumbar core stability training combined with electroacupuncture in treating chronic nonspecific low back pain. Chin J Rehabilit. 2015;4:296–297.
33. Hongxia F, Guohui Z, Airong N, Yingjie Z, Yuanmei L, Shujie T. Clinical observation on the treatment of nonspecific low back pain with small needle knife combined with core stability training. China Health Care Nutr. 2018;28(25):10.
34. Fei Y, Peng L, Ruixiang Z. Effects of warm acupuncture combined with core stability training on patients with nonspecific low back pain. Med J Chin People’s Health. 2023;35(4):107–110.
35. Huifeng L, Songhe M, Ming S. The clinical efficacy of inner heat needle therapy in patients with chronic nonspecific low back pain and its impact on inflammatory factors. Sichuan J Physiol Sci. 2022;44(6):1046–1048,1056.
36. Shuqi C, Baoqiang D, XIngxing L, et al. Effect of combined acupuncture and moxibustion and core stability training on pain,function and muscular endurance in patients with chronic non - specific low back pain. Chinese Archives Traditional Chin Med. 2019;37(4):911–914.
37. Ruijie L, Baoqiang D, Xingxing L, Zuqi S, Jiaoping H, Miao Z. Clinical observation of the treatment of chronic nonspecific low back pain with tendon and traditional cardiac stability training. J Liaoning Univer Tcm. 2018;20(6):60–63.
38. Yuda Z, Xiaoqin L, Bei C, Wei J, Yong D, Xiuming D. Superficial needle therapy combined with core stability training for chronic non-specific low back pain: a report of 23 cases. Zhejiang J Tradit Chin Med. 2022;57(4):290.
39. Xiyuan L. Clinical Observation on Acupuncture Treatment of Chronic Non-Specific Low Back Pain Based on the Theory of Treating Neck and Waist Simultaneously[dissertation]. Liaoning: Liaoning University of Traditional Chinese Medicine. 2024.
40. Yingjie Z, Guoqing L, Feng Z. Acupuncture knife combined with core stability training based on jingjin theory in the treatment of 77 cases of chronic non-specific low back pain. China J Tradition Chin Med Pharm. 2024;31(4):693–695.
41. Yingli W, Yuandong C, Yuanqin M, Yuqin W, Liugang T, Tai L. Effect of motor acupuncture based on movement pattern adjustment theory in the treatment of non-specific low back pain. J Clin Med Pract. 2024;28(21):100–104.
42. Jinghua H. Clinical observation on fire needle therapy combined with core muscle strength training for chronic non-specific low back pain. J Pract Tradit Chin Med. 2019;35(7):860–861.
43. Junming L. The Clinical Study of Core Training Combined with Acupuncture for Chronic Non-Specific Low Back Pain. Guangzhou:Guangzhou University of Chinese Medine; 2019.
44. Yongyi Z, Yanhong C, Haokun X. Effects of core stability exercise on β-Endorphin and cortisol levels in patients with chronic non-specific low back pain. J Cervicodynia Lumbodynia. 2021;42(1):100–102.
45. Xiangxiang R, Ying C, Xiaojie Y. Clinical observation on chronic non-specific low back pain of kidney deficiency and blood stasis type treated with herbal-cake-separated moxibustion combined with core strength training. China J Tradition Chin Med Pharm. 2020;27(5):801–802.
46. Meiyun W, Dongming Z, Wenqing H. Clinical study on modified du meridian moxibustion combined with core stability training for chronic non-specific low back pain. Chin Manipulation and Rehabil Med. 2022;13(15):8–11.
47. Bin L, Rui Z, Kang H, Jun Q, Xing T. Clinical observation on floating needle therapy combined with lumbar and abdominal core muscle training in treating chronic non-specific low back pain. J Shandong Univer Tcm. 2020;44(05):544–549.
48. Aihong W. Ecological momentary assessment of auricular point acupressure combined with core stability training in the treatment of chronic low back pain. J Cervicodynia Lumbodynia. 2022;43(2):258–261.
49. Kaiqian G, Fengzhou X, Jianhua L, Fafa D, Chao L, Xi W. Therapeutic efficacy of electroacupuncture combined with core stability training for chronic nonspecific low back pain and analysis of treatment course optimization. J Cervicodynia Lumbodynia. 2023;44(2):235–238.
50. Chang L, Baoqiang D, Yu F, et al. Obsercation on the intervention effect of electroacupuncture focus of tendon combined with waist core strength training on chronic non-specific low back pain. Asia-Pacific Tradit Med. 2021;17(6):59–61.
51. Wenli Z, Daoming X, Jing L, Wenzhong W. Clinical effects of the combination of electric acupuncture and core muscular training on nonspecific low back pain. Chin J Rehabilit. 2016;31(4):283–285.
52. Li L, Wenwen F, Haifeng L, Chao L. Clinical comparative study of conventional acupuncture and acupuncture combined with lumbar and abdominal muscle training in the treatment of nonspecific low back pain. Chinese Journal of Rehabilitation Medicine. 2012;27(5):475–476.
53. Ying D, Xiaohua M, Yaoguang G. Application effects of long snake moxibustion combined with core stable exercise training in patients with chronic nonspecific low back pain. Med J Chin People’s Health. 2024;36(11):81–84.
54. Cheng Y, Yu Y, Wang Y, et al. Effects of lumbar-pelvic training combined with electroacupuncture on chronic nonspecific low back pain. Medicine. 2023;102(29):e34407. doi:10.1097/MD.0000000000034407
55. Ye L, Liu C, Jiang C, Cao Y. Core training under suspension exercise therapy on treatment of low back pain. Rev Soc Bras Med Trop. 2022;55:e0336B2021.
56. Chen F-Q, Ge J-F, Leng Y-F, Li C, Chen B, Sun Z-L. Efficacy and safety of moxibustion for chronic low back pain: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2020;39:101130. doi:10.1016/j.ctcp.2020.101130
57. Jung M, Rein N, Fuchs B. Physical therapy for chemotherapy-induced peripheral neuropathy in pediatric oncology. Klin Padiatr. 2016;228(6–07):313–318. doi:10.1055/s-0042-111692
58. Baroncini A, Maffulli N, Manocchio N, et al. Active and passive physical therapy in patients with chronic low-back pain: a level I Bayesian network meta-analysis. J Orthop Traumatol. 2025;26(1):66. doi:10.1186/s10195-025-00885-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.