Back to Journals » Journal of Pain Research » Volume 15
Acupuncture Based on Regulating Autonomic Nerves for the Prevention of Migraine Without Aura: A Prospective, Double-Dummy, Randomized Controlled Clinical Trial
Authors Zhou C ![]() , Bao J
, Bao J ![]() , Hu H
, Hu H ![]() , Ye S, Shao X
, Ye S, Shao X ![]() , Liang Y
, Liang Y ![]() , Fang J
, Fang J
Received 6 May 2022
Accepted for publication 26 July 2022
Published 4 August 2022 Volume 2022:15 Pages 2211—2221
DOI https://doi.org/10.2147/JPR.S372311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Chuanlong Zhou,1,* Jie Bao,2,* Hantong Hu,1 Siting Ye,3 Xiaomei Shao,4 Yi Liang,4 Jianqiao Fang4
1Department of Acupuncture, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2School of Basic Medical Sciences, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Tuina, the First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 4Key Laboratory of Acupuncture and Neurology of Zhejiang Province, the Third Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuanlong Zhou, Department of Acupuncture, the Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, XiHu District, Hangzhou, 310005, People’s Republic of China, Email [email protected]
Background: Migraine without aura (MWoA) is a nervous system disease, which is closely related to autonomic nerves dysfunction. As a popular non-pharmacological alternative treatment for preventing migraine, it remains unclear whether the acupuncture can prevent MWoA. Thus, this trial aims to evaluate the preventive effect and safety of the acupuncture method of stimulating acupoints that regulate autonomic nerves in MWoA patients.
Methods: This is a single-center, prospective, double-dummy, randomized controlled clinical trial. A total of ninety-six patients with MWoA are randomly allocated to acupuncture combined with the placebo group and sham acupuncture combined with the medication group in a 1:1 ratio. All subjects will receive intervention for 8 weeks and follow-up assessments three times (one month, three months, and six months in follow-up visiting). The frequency of acupuncture in both groups is three times a week for eight weeks. The primary outcome will be evaluated using a visual analog scale (VAS) and the number of migraine attacks per four weeks. The secondary outcome measures will include the migraine-specific quality of life (MSQOL) scale and headache needs assessment survey (HANA) questionnaire scale.
Results: The acupoint selection of this clinical trial is based on the combination of traditional Chinese medicine theory with modern medicine, thereby evaluating the efficacy and safety of the acupuncture method of stimulating acupoints that regulate autonomic nerves in the prevention of MWoA. The results may provide evidence of the beneficial effects of acupuncture on the prevention of MWoA by regulating autonomic nerves dysfunction.
Trial Registration: ClinicalTrials.gov NCT04766762.
Keywords: acupuncture, migraine without aura, autonomic nerves, randomized controlled clinical trial, protocol
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Xie has been published for this article.
Introduction
Migraine is a very common neurobiological headache disorder characterized by recurrent headaches, which ranks among the top disorders causing disability.1 The prevalence of migraine is approximately 14.7% worldwide, and the prevalence of chronic migraine ranges from 0 to 5.1%, usually estimated at 1.4 to 2.2%.2 It affects about 17% of women and 8% of men in Europe.3 Migraine is a heterogeneous disease with two major subtypes, namely, migraine with aura (MWA), and without aura (MWoA). Studies have confirmed different mechanisms underlying the variable subtypes.4 According to the International Classification of Headache Disorders-3rd edition (ICHD-3) from the International Headache Society,5 MWoA is defined as a recurrent headache disorder manifesting in attacks lasting 4–72 hours. Typical characteristics of the headache are unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity, and association with nausea and/or photophobia and phonophobia.
The pathogenesis of migraine remains inconclusive. Because the symptoms of autonomic nerves dysfunction are common in acute migraine attacks, some studies suppose that autonomic nerves dysfunction is an important pathophysiological mechanism of migraine attacks.6 The classical trigeminal vascular afferent pathway believes that migraine attacks are caused by disturbances in the brain’s sensory processing.7 Autonomic nerves dysfunction is very common in migraineurs and may occur either before or during migraine attacks, including nausea and vomiting, photophobia, palpitations, and flushing of the face,8 which is recognized as the diagnostic criteria for migraine. Moreover, the two attack mechanisms are closely related. The headache phase is driven by pain perception communicated from peripheral afferents to central control centers for pain. It is associated with the trigeminal nerve complex, where autonomic nerves are located.9 During a migraine attack, the patient’s sympathetic nerves system excites, while the parasympathetic nerves system is suppressed.10 To reduce migraine attack frequency and pain intensity, beta-blockers, such as propranolol and metoprolol, are widely used in clinical treatment.11 However, some patients do not take drugs as prescribed due to the side effects, such as paraesthesia, cognitive problems, dyspepsia, fatigue, dizziness, and so on.12 In addition, some patients cannot tolerate medication, and some are just not helped by it.
Acupuncture, as a major part of traditional Chinese medicine, has been used in medical practice for more than 2000 years in China, with advantages of few side effects and low cost. The use of acupuncture has been proved to be effective and advantageous in alleviating chronic pain.13 However, there are controversies about the “placebo effect” and “specific effect” of acupuncture in the prevention of migraine.14 Our previous studies have proved that the acupuncture method of stimulating acupoints that can regulate autonomic nerves is an effective method for preventing MWoA attacks.15 But the quality and results of our previous experiment are inadequate. The control groups in that study were set differently and no western medicine group was set. Hence, this study with a better-designed protocol is conducted to confirm the curative effects of the acupuncture method of stimulating acupoints that can regulate autonomic nerves in the treatment of MWoA compared with flunarizine.
Materials and Methods
Study Design
This study is a single-center, prospective, double-dummy, and randomized controlled clinical trial (RCT). Ninety-six migraine patients will be randomly assigned to acupuncture combined with the placebo group and sham acupuncture combined with the medication group in a ratio of 1:1. The intervention will be performed for eight weeks with follow-up of three times (one month, three months, and six months after follow-up visiting). The frequency of treatment in both groups is three times a week for eight weeks. The study is enrolling participants now and is expected to end in February 2023.
The flow chart of the study process is shown in Figure 1 and the trial schedule of enrolment, treatments, and assessments is displayed in Table 1. The reporting of this study protocol is based on the SPIRIT reporting guidelines.
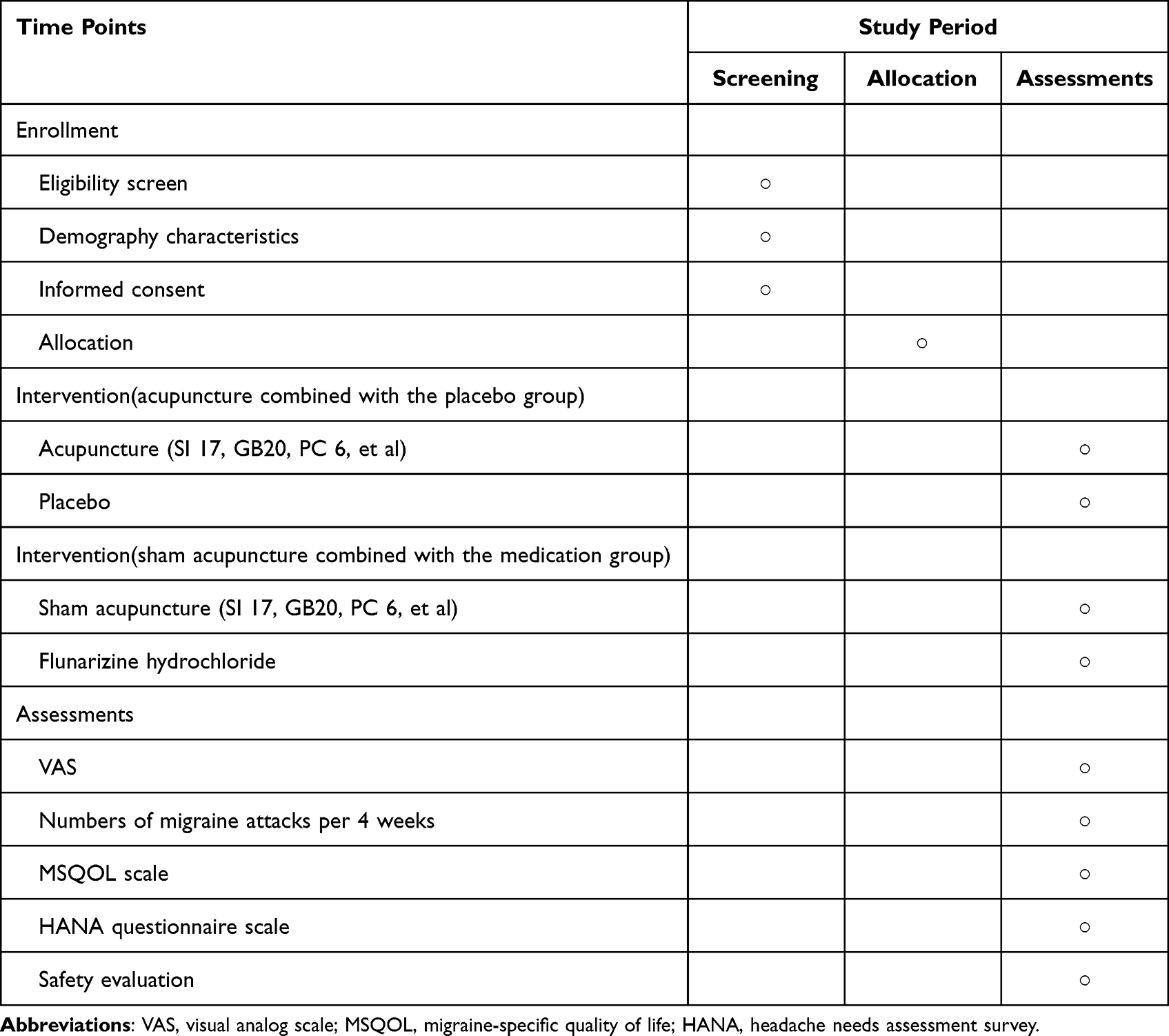 |
Table 1 Trial Schedule of Enrollment, Intervention and Assessments |
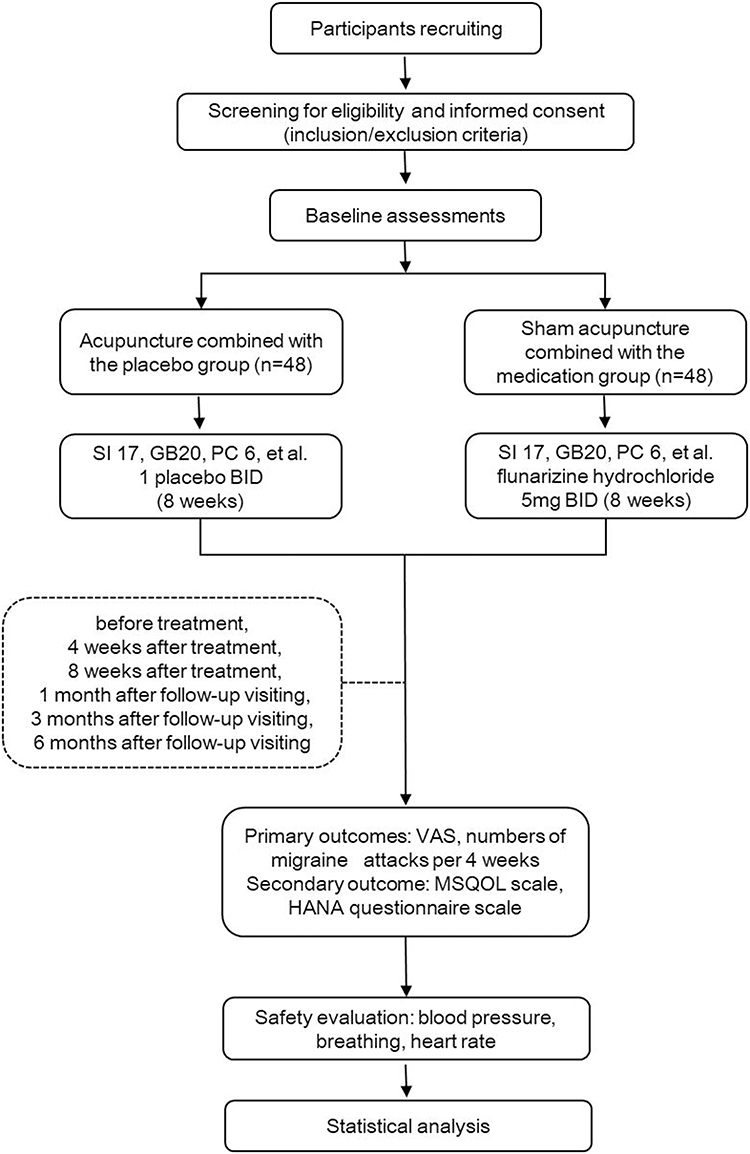 |
Figure 1 Study design flowchart. Abbreviations: VAS, visual analog scale; MSQOL, migraine-specific quality of life; HANA, headache needs assessment survey. |
Participants
Inclusion Criteria
(1) Patients meet the diagnostic criteria of migraine without aura specified in ICHD-3;
(2) 25 ≤ age ≤50 years, male or female;
(3) The frequency of migraine attacks in the past three months is more than twice a month;
(4) Pharmacotherapy and other treatments are not very effective for patients. Pharmacotherapy for migraine without aura has been stopped for at least one week;
(5) Participants can fully understand the study protocol and agree to sign written informed consent.
Exclusion Criteria
(3) Pregnant or lactating women;
(4) Patients have a spontaneous bleeding tendency, so it is not suitable for them to receive acupuncture;
(5) Patients have an allergic history of flunarizine hydrochloride or a history of depression;
(6) Patients are diagnosed with psychosis.
Participant Recruitment
This randomized, sham-controlled, patient and assessor-blinded trial will be conducted in The Third Affiliated Hospital of Zhejiang Chinese Medical University. The participants in this study will be recruited from the outpatient department via advertisement on hospital-based electronic social media platforms and poster distribution in the public areas of hospitals with the details of this study and contact information.
The research object will be conducted through preliminary screening by contacting a research assistant in the field. The potentially eligible participants will be registered and make an appointment with a designated physician to check the inclusion and exclusion criteria. The patients who conform to all inclusion criteria but not exclusion criteria will be invited to participate in the study and provide details about this RCT. All participants will be required to sign an informed consent form and their comprehensive information.
The baseline assessment will be performed by the same physician and recorded in the case report form (CRF). All participants will receive eight weeks of treatment and six months of follow-up. The assessment points in time are before treatment, four weeks after treatment, eight weeks after treatment, one month after follow-up visiting, three months after follow-up visiting, and six months after follow-up visiting. Each participant will be given a schedule of intervention dates and follow-up appointments performed by an uninformed research assistant.
Besides, all participants will be asked to keep a headache diary including the date, duration, and intensity of each migraine attack, as well as the use of rescue medication, throughout the treatment and follow-up period.
Randomization and Blinding
The subjects will be randomly divided into two groups: the acupuncture combined with the placebo group and the Sham acupuncture combined with the medication group in a 1:1 ratio.
To remain blind in the trial, none of the patients will be told which group they have been assigned to. All of the patients participated in this study; principal investigators and research staff will remain blinded to all patients’ randomization assignments throughout the study. Follow-up evaluators and statisticians who would not be involved in clinical management would be blinded throughout the study. It is unable to blind acupuncture practitioners in this study because of the practical application of acupuncture techniques.
To ensure the success of the blind test, several common approaches of acupuncture would be performed for patients from both groups: skin sterilized with 75% alcohol; usage of disposable and sterile steel needles (1.5-inch needle, 0.25×40 mm); needles inserted into the skin for 10 to 15 mm and remain for 30 minutes; no moxibustion or electrical stimulation; bilateral acupoints; 10 to 12 needles each time; DeQi obtained by 5 to 10 times of lifting, thrusting, and twirling the needles; twenty-four times of acupuncture or sham acupuncture over eight weeks (three times per week). In addition, the placebo appeared the same as flunarizine.
Intervention
All participants will accept real or fake acupuncture for eight weeks. The frequency of an intervention is three times a week. Each participant will be arranged in a separate room for thirty minutes during each session. To ensure the accuracy and consistency of the treatment provided, all acupuncturists participating in the study must be practicing physicians. Simultaneously, possible adverse reactions during the study will be recorded.
In case of intolerable acute migraine attacks during the trial, the participants will be allowed to take rescue medication, and the name and the dosage of the medication will be documented in detail in the patient’s diary.
Acupuncture Combined with the Placebo Group
This group will include 48 patients. Patients in this group will receive acupuncture combined with a placebo. Participants are in the supine position. The bilateral Tianrong (SI 17) acupoints are needled for 1–1.5 inches with the direction tilted back 45±5 degrees. The bilateral Fengchi (GB 20) acupoints are needled for 0.5–1 inch with the direction tilted to the nose. The bilateral Neiguan (PC 6) acupoints are also needled for 0.5–1 inch with the straight direction. The locations of the acupoints are displayed in Table 2. In addition, 4–6 additional acupoints can be identified according to different syndrome types of patients. The needles maintain for thirty min, the treatment frequency is three times per week, and the treatment duration lasts eight weeks. Meanwhile, the daily dosage of placebo is one capsule BID and the treatment duration also lasts eight weeks.
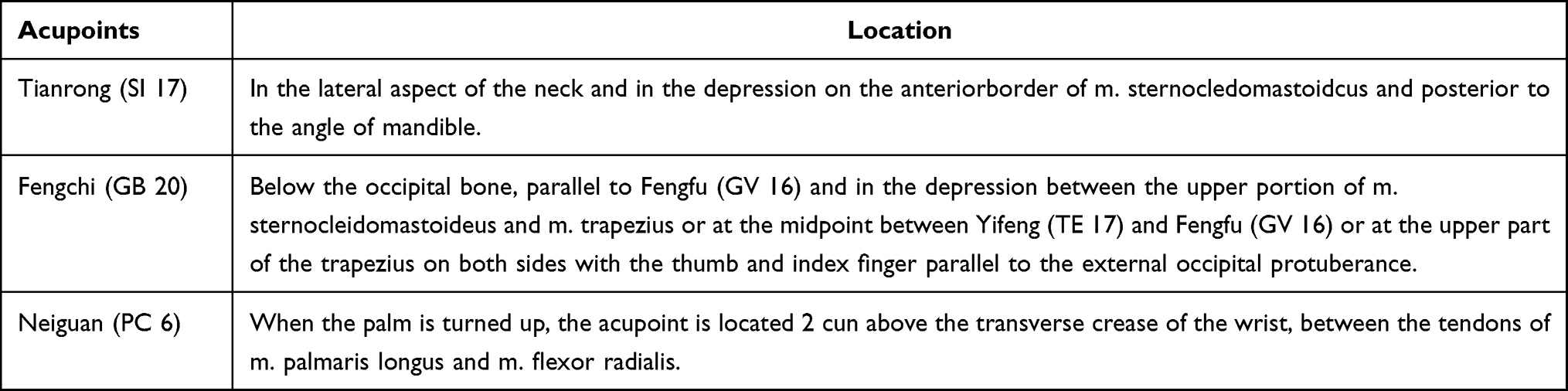 |
Table 2 Locations of Acupuncture Acupoints |
Sham Acupuncture Combined with Medication Group
This group will include forty-eight patients. Participants in this group will receive sham acupuncture plus flunarizine hydrochloride. Participants are in the supine position, and sham acupuncture is conducted. The bilateral Tianrong (SI 17) acupoints, Fengchi (GB 20) acupoints, and Neiguan (PC 6) acupoints are selected, and 4–6 additional acupoints can be identified according to the syndrome type of the participants. The needles are kept for thirty min, the treatment frequency is three times per week, and the treatment duration lasts eight weeks. Moreover, the daily dosage of flunarizine hydrochloride is 5mg BID and the treatment duration also lasts eight weeks.
Outcome Measurements
Primary Outcomes
(1) Pain intensity
Pain intensity will be measured by a VAS.16 Using a horizontal ruler of 10 cm, “0” represents no pain, and “10” stands for unbearable pain.
(2) Numbers of migraine attacks per four weeks.
The number of migraine attacks is assessed by patients’ pain diary.
Measuring time points: before treatment, four weeks after treatment, eight weeks after treatment, one month after follow-up visiting, three months after follow-up visiting, and six months after follow-up visiting.
Secondary Outcome Measure
(1) Migraine-specific Quality of life (MSQOL)
Quality of life will be measured by the MSQOL scale17 that consists of 20 items, each of which is rated using a response scale with four categories (1 = very much and 4 = not at all). The data were then standardized to a range of values from 0–100, where 0 represents the worst health status experienced by the participants and 100 stands for the best health status. If reporting a score on a scale, the unabbreviated scale title, the minimum, and maximum values, and whether higher scores mean a better or worse outcome should be included. The WHO believes that an individual’s needs for life and the extent of those needs should be included in quality of life assessment, involving personal goals, standards, concerns, and expectations influenced by a particular culture and values.18 The language used in the MSQOL scale is based on the language used by migraine patients. This method is patient-oriented, so it provides more meaningful assessment values.17
(2) Headache needs assessment survey (HANA) questionnaire scale.
HANA questionnaire scale19 to assess the frequency and impact of migraine. This short, practical survey focuses on the impact of migraine on an individual’s health and daily life and reflects the severity of the disorder suffered by migraine sufferers. HANA meets the validity criteria and has good internal consistency, reliability, structural validity, and responsiveness. A good correlation between frequency and degree of distress suggests that both issues are important to patients and have different weights.
Safety Evaluation
Adverse events will be monitored during the whole observation period. In addition, safety evaluations will be conducted including blood pressure, breathing, and heart rate.
Sample Size Calculation
We used the method used in previous studies, and the effective rate in the acupuncture group was eighty percent,15 compared with sixty-seven percent20 in the control group. The ratio of the acupuncture group to the control group was 1:1. According to the two-sided test of SAS 9.4 software, the sample size required for each group was thirty-nine cases, the significance level (α) was 0.05 and the power (1-β) was 0.80. Thus, there are ninety-six subjects in Acupuncture combined with the placebo group and Sham acupuncture combined with the medication group, and the withdrawal rate was about 20%.
Quality Control
It is necessary to establish a standard acupuncture procedure, which will govern the identification, registration, and treatment of participants. Acupuncture doctors with clinical experience are trained to ensure the consistency of acupuncture operations. A corresponding data security monitoring plan will be developed. All adverse events are recorded in detail, properly handled, and followed up until the adverse events are resolved. Moreover, all adverse events are reported to the Ethics committee promptly.
Data Management
All researchers, including acupuncturists, data managers, data collectors, data entry personnel, outcome assessors, and statisticians will receive professional training on the overall procedure and data management. During the recruitment period, the data collector will record the baseline characteristics of participants in CRFs, and the data manager will check all data. After the treatment and follow-up phases completion, data for all participants will be filled out and recorded on the original CRF, followed by independent Excel sheets by two data entry personnel. The two sets of data are then cross-checked by the data manager to ensure accuracy. If any discrepancies are found, they will be corrected according to the original CRF and marked on it. All paper documents will be kept in a locked filing cabinet, while electronic files will be stored on a special computer that will be password protected. Only leading researchers have access to the files. All research documents, both paper and electronic, will be preserved for at least 5 years after publication.
Statistical Analysis
Data values will be presented by mean ± standard deviation, 95% confidence intervals (CI), or percentage. Statistical analysis will be performed using the two-tailed test with a significance level of 5%. At baseline, the t-test or Wilcoxon ran-sum test will be used to compare differences between groups. If there are baseline characteristics (eg frequency and intensity of migraine at baseline) showing statistical significance between groups, analysis of covariance (ANOVA) or logistic regression will be used for analysis and adjustment of baseline characteristics. For changes in the number of migraine days, the baseline number of migraine days will be used as a covariance to compare the differences between the last two time points in the groups. For VAS scores, ANOVA with repeated measures will be used to compare inter-group and intra-group differences. In the case of proportion, the Chi-square test will be applied. All analyses will be performed using the SPSS software program (version 26.0).
Publication Policy
The study group will publish the results when the data analysis is complete. All reports and publications should protect the integrity of the main objectives of the research. Any data on blind concealment failures will not be published until the results are published. The Steering Committee will discuss recommendations regarding the timing and possible meetings for the submission of these endpoint data. The major results will be presented through publications such as papers, conference abstracts, and clinical trial registries. The data set analyzed in the current study is available on request from the corresponding author.
Ethical Considerations
The protocol has been approved by the Institutional Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval number: ZSLL-KY-2020-006-02) and our study will follow the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. All subjects will be requested to sign informed consent. Consent may be obtained from the corresponding author if necessary. In the consent form, participants will be asked if they agree to use their data once they opt-out of the trial. Participants will also be required to obtain permission from the research team to share relevant data with participating university members. This experiment does not involve the collection of biological specimens for storage. Furthermore, participants’ personal information will be kept strictly confidential.
Discussion
This trial is designed as a single-center, prospective, double-dummy RCT that aims to investigate whether the acupoint selection method has a positive effect on the frequency of migraine attacks, pain, and related symptoms. If proven effective, the technique could offer a new idea for prevention and treatment for migraine sufferers, or at least for migraine without aura. Moreover, it may provide some material for discussing the mechanism of migraine.
Migraine belongs to the category of “headwind” in traditional Chinese medicine. At present, there are pieces of literature and clinical experience supporting acupuncture in the treatment of migraine,21 with definite curative effects. Some literature has made statistics on acupuncture acupoint selection for migraine. The results showed that more than 130 acupoints have been selected for treating migraine,22 and a variety of acupuncture methods and therapies have been involved in the past fifty years. The complexity of acupoint selection and treatment has affected the promotion and application of acupuncture.23 Therefore, it is a complicated problem how to select acupoints and arrange experiments when the pathogenesis of migraine is uncertain.7 In this experiment, we aim to optimize the following aspects to explore the study of acupuncture prevention of migraine.
Selection of Acupoints
The classical trigeminal afferent pathway theory believes that migraine is caused by disturbances in sensory processing.7 Autonomic nerves dysfunction is discussed as a pathogenetic factor in migraine. Symptoms, such as nausea and vomiting, photophobia, heart palpitations, or flush on the face8 are likely to occur before or during migraine attacks. Therefore, acupoint selection based on the regulation of autonomic nerves function may be a better treatment for migraine.
Fengchi (GB 20) acupoint had been demonstrated to have a beneficial influence on the autonomic nerves system in migraineurs with a reduction of the low-frequency power of heart-rate variability related to the clinical effect.24 Acupuncture at Tianrong (SI 17) Point has long been reported to have significant efficacy in the treatment of migraine.25 Our previous study discussed the ancient literature basis of treating migraine by Tianrong acupoint.26 Moreover, modern medicine thinks that the depth of Tianrong acupoint is near the cervical ganglia of the sympathetic trunk.27 It is useful to intervene in the autonomic nerves system function of the cervical sympathetic plexus and bidirectional regulation of the cerebral artery blood flow velocity for the treatment of migraine.28 Acupuncture at Neiguan (PC6) acupoint also significantly enhanced vagus nerve activity and had a relatively specific effect on heart rate variability.29 In previous studies, it has been found that the sympathetic and parasympathetic nerve activities of migraine patients are lower than those of normal people. Acupuncture can improve the activity of autonomic nerves function.15
In addition, based on the research principles of the real world of TCM, 4–6 acupoints would be applied according to the syndrome type of the subjects. TCM Zheng (syndrome) is a basic concept in its theory. It is generally composed of a relatively fixed set of internally related symptoms and signs that can reveal the essence of a certain stage or a certain type of disease, and “bian zheng lun zhi” (syndrome differentiation) is the most fundamental theory in TCM treatment,30 characterized as holistic with emphasis on the interaction between human individuals31 and their environments. Therefore, the innovation of this study lies in the combination of traditional Chinese medicine theory with modern medicine for acupoint selection. It aims to discuss the intervention and regulation of acupoint selection in patients with MWoA from a clinical research point of view.
Experimental Design and Blinding
In this study, we will select a blunt pointed dummy needle that is similar in shape to the actual needle. During the treatment, the fake needles will penetrate a sticky pad that reaches the skin surface but not into the tissue, so the subjects will still feel the pain of the “acupuncture”, ensuring the treatment is blind. This method had been proved to have good application prospects in previous studies. The pragmatic placebo needle is a valid control for acupuncture research. It produces a good subject blinding effect with a similar appearance to conventional acupuncture needles and no tissue penetration when applied.32
In terms of the selection of fake acupuncture methods, some scholars believe that Chinese people have a strong belief in the “DeQi” during acupuncture treatment.33 This also involves the specificity of acupoint stimulation or the selection of some acupoint specificity, which may affect the observation of efficacy.34,35 If the sham acupuncture chose to Pierce the skin, the sham acupuncture produces a greater effect than placebo compared to non-treatment and may include the intervention effect of the real placebo effect combined with acupuncture.36–38 However, the research team believes that the current improvement of acupuncture needles is mainly to make patients feel painless, but on this basis, it must have a curative effect. Hence, in the control group, we adopted sham acupuncture (acupuncture skin) combined with real drug treatment, which is more in line with the real-world clinical simulations of acupuncture. Patients from both groups receive acupuncture and drug treatment, and it is not easy to distinguish different groups by communication, which is more consistent with the blind method.
For acupuncture clinical trials, many scholars have made great efforts in designing the control group,39–41 but there may still be many problems in the actual operation. In this study, the acupuncturists would receive standardized training ahead to achieve blindness as much as possible. For example, operation in the control group, answers to the patients’ questions about “DeQi” and questions involving oral drugs or placebo, would all be carried out.
Abbreviations
MWoA, migraine without aura; VAS, visual analog scale; MSQOL, migraine-specific quality of life; HANA, headache needs assessment survey; MWA, migraine with aura; ICHD-3, International Classification of Headache Disorders-3rd edition; RCT, randomized controlled clinical trial; CRF, case report form; CI, confidence intervals.
Data Sharing Statement
All data will be available upon reasonable request.
Trial Status
Participant recruitment started from March 1, 2021, and the study completion date is estimated to be February 2023.
Consent
A consent form including the study procedures, possible risks, and rights will be provided to each participant before enrolling in this trial.
Acknowledgments
The authors would like to appreciate the participation of included subjects who will be involved in this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Zhejiang Traditional Chinese Medicine Science and Technology Plan Project (No. 2020ZB125) and Zhejiang Province Medical and Health Care Key Project (No.2022KY237) provided funding.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Silberstein SD. Migraine. Lancet. 2004;363(9406):381–391. doi:10.1016/S0140-6736(04
2. Natoli J, Manack A, Dean B, et al. Global prevalence of chronic migraine: a systematic review. Cephalalgia. 2009:599–609. doi:10.1111/j.1468-2982.2009.01941.x
3. Stovner LJ, Hagen K. Prevalence, burden, and cost of headache disorders. Curr Opin Neurol. 2006;19(3):281–285. doi:10.1097/01.wco.0000227039.16071.92
4. Kincses ZT, Vereb D, Farago P, et al. Are Migraine With and Without Aura Really Different Entities? Front Neurol. 2019;10:982. doi:10.3389/fneur.2019.00982
5. Headache Classification Committee of the International Headache Society (IHS); The International Classification of Headache Disorders. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
6. Shechter AL, Silberstein SD, Stewart WF, et al. Migraine and autonomic nervous system function: a population-based, case-control study. Neurology. 2002;58(3):422–427. doi:10.1212/wnl.58.3.422
7. Goadsby PJ, Holland PR, Martins-Oliveira M, et al. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017. doi:10.1152/physrev.00034.2015
8. Miglis MG. Migraine and autonomic dysfunction: which is the horse and which is the jockey? Curr Pain Headache Rep. 2018;22(3):1–7. doi:10.1007/s11916-018-0671-y
9. Qubty W, Patniyot I. Migraine pathophysiology. Pediatr Neurol. 2020;107:1–6. doi:10.1016/j.pediatrneurol.2019.12.014
10. Gass JJ, Glaros AG. Autonomic dysregulation in headache patients. Appl Psychophysiol Biofeedback. 2013;38(4):257–263. doi:10.1007/s10484-013-9231-8
11. Sarchielli P, Granella F, Prudenzano MP, et al. Italian guidelines for primary headaches: 2012 revised version. j Headache Pain. 2012;13(2):31–70. doi:10.1007/s10484-013-9231-8
12. Dekker F, Dieleman J, Neven AK, et al. Preventive treatment for migraine in primary care, a population-based study in the Netherlands. Cephalalgia. 2013;33(14):1170–1178. doi:10.1177/0333102413490343
13. Han J-S. Acupuncture analgesia: areas of consensus and controversy. Pain. 2011;152(3):S41–S48. doi:10.1016/j.pain.2010.10.012
14. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444–1453. doi:10.1001/archinternmed.2012.3654
15. Chuan-long Z, Jie B, Xiao-mei S, et al. Randomized controlled study of different acupoints selection principles based on autonomic nerve function in patients with migraine without aura. China J Traditional Chin Med Pharmacy. 2021;36(1):5.
16. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16(1):87–101. doi:10.1016/0304-3959(83)90088-X
17. Patrick DL, Hurst BC, Hughes J. Further development and testing of the migraine‐specific quality of life (MSQOL) measure. Headache. 2000;40(7):550–560. doi:10.1046/j.1526-4610.2000.00086.x
18. Szabo S. The World Health Organisation Quality of life (WHOQOL) assessment instrument. Quality Pharmacoeconomics Clin Trials. 1996;355–362. doi:10.1016/0277-9536(95)00112-k
19. Cramer JA, Silberstein SD, Winner P. Development and validation of the Headache Needs Assessment (HANA) survey. Headache. 2001;41(4):402–409. doi:10.1046/j.1526-4610.2001.111006402.x
20. Bussone G, Cerbo R, Martucci N, et al. Alpha-Dihydroergocryptine in the prophylaxis of migraine: a multicenter double-blind study versus flunarizine. Headache. 1999;39(6):426–431. doi:10.1046/j.1526-4610.1999.3906426.x
21. Urits I, Patel M, Putz ME, et al. Acupuncture and its role in the treatment of migraine headaches. Neurol Therapy. 2020;9(2):375–394. doi:10.1007/s40120-020-00216-1
22. Qin C, Fanrong L, Hui Z, et al. Study on the classification and application of acupoints on acupuncture in treating migraine. Zhejiang J Traditional Chin Med. 2013;1:854.
23. White A, Resch K, Chan J, et al. Acupuncture for episodic tension-type headache: a multicentre randomized controlled trial. Cephalalgia. 2000;20(7):632–637. doi:10.1111/j.1468-2982.2000.00097.x
24. Bäcker M, Grossman P, Schneider J, et al. Acupuncture in migraine: investigation of autonomic effects. Clin J Pain. 2008;24(2):106–115. doi:10.1097/AJP.0b013e318159f95e
25. Deping L, Anle H. Clinical observation on 100 cases of migraine treated by acupuncture at Tianrong Point. Zhejiang J Traditional Chin Med. 1995;1:856.
26. Chuan-long Z, Jie B, Xiao-mei S, et al. Theoretical discussion of point Tianrong (SI17) for treating migraine China. J Traditional Chin Med Pharmacy. 2019;1(3):3.
27. Dawei Y, Zhibin L, Daren Z, et al. Application Manual of Acupoint Anatomy. Vol. 10. Bafang Culture Enterprise Company; 2001.
28. Weiquan J, Peigen K, Jiamei J, et al. Symmetry changing of MFV and BEAM were investigated in migraine without aura with Tianrong acupoint treatment. J Brain Nervous Dis. 2002;10(5):282–284.
29. Miao Y, Wei S, Changchun W, et al. Effect of Needling PC6 on HRV of DCAN Patients. J Clin Acupuncture Moxibustion. 2019;35(5):3.
30. Zeng -X-X, Bian Z-X, Wu T-X, et al. Traditional Chinese medicine syndrome distribution in chronic hepatitis B populations: a systematic review. Am J Chin Med. 2011;39(6):1061–1074.
31. Preeti L, Magesh K, Rajkumar K, et al. Recurrent aphthous stomatitis. J Oral Maxillofacial Pathol. 2011;15(3):252–256. doi:10.4103/0973-029X.86669
32. Liu B, Xu H, Ma R, et al. Effect of blinding with a new pragmatic placebo needle: a randomized controlled crossover study. Medicine. 2014;93:27. doi:10.1097/MD.0000000000000200
33. Liu L. Acupuncture as prophylaxis for chronic migraine: a protocol for a single-blinded, double-dummy randomised controlled trial. BMJ open. 2018;8(5):e020653. doi:10.1136/bmjopen-2017-020653
34. White P, Lewith G, Berman B, et al. Reviews of acupuncture for chronic neck pain: pitfalls in conducting systematic reviews. Rheumatology. 2002;41(11):1224–1231. doi:10.1093/rheumatology/41.11.1224
35. White A, Filshie J, Cummings T. Clinical trials of acupuncture: consensus recommendations for optimal treatment, sham controls and blinding. Complement Ther Med. 2001;9(4):237–245. doi:10.1054/ctim.2001.0489
36. Lundeberg T, Lund I, Näslund J, et al. The Emperors sham–wrong assumption that sham needling is sham. Acupuncture Med. 2008;26(4):239–242. doi:10.1136/aim.26.4.239
37. Linde K, Niemann K, Meissner K. Are sham acupuncture interventions more effective than (other) placebos? A re-analysis of data from the Cochrane review on placebo effects. Complementary Med Res. 2010;17(5):259–264. doi:10.1159/000320374
38. Hróbjartsson A, Gøtzsche PC. Placebo interventions for all clinical conditions. Cochrane Database Sys Rev. 2004;1(2):847. doi:10.1002/14651858.CD003974.pub2
39. Zhang CS, Tan HY, Zhang GS, et al. Placebo devices as effective control methods in acupuncture clinical trials: a systematic review. PLoS One. 2015;10(11):e0140825. doi:10.1371/journal.pone.0140825
40. Dincer F, Linde K. Sham interventions in randomized clinical trials of acupuncture - review. Complement Ther Med. 2003;11(4):235–242. doi:10.1016/s0965-2299(03
41. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chin Med. 2009;4(1):1–9. doi:10.1186/1749-8546-4-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Pain and Function in Patients with Nonspecific Low Back Pain: Study Protocol for an Up-to-Date Systematic Review and Meta-Analysis
Li Y, Liu Y, Zhang L, Zhai M, Li L, Yuan S, Li Y
Journal of Pain Research 2022, 15:1379-1387
Published Date: 10 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Effectiveness of Pharmacopuncture in Patients with Lumbar Spinal Stenosis: A Protocol for a Multi-Centered, Pragmatic, Randomized, Controlled, Parallel Group Study
Lee JY, Park KS, Kim S, Seo JY, Cho HW, Nam D, Park Y, Kim EJ, Lee YJ, Ha IH
Journal of Pain Research 2022, 15:2989-2996
Published Date: 23 September 2022
Central Mechanism of Acupuncture Treatment in Patients with Migraine: Study Protocol for Randomized Controlled Neuroimaging Trial
Jia J, Yan C, Zheng X, Shi A, Li Z, Xu L, Hui Z, Chen Y, Cao Z, Wang J
Journal of Pain Research 2023, 16:129-140
Published Date: 18 January 2023
The Opioid-Sparing Effect of Acupuncture After Abdominal Surgery: A Systematic Review and Meta-Analysis Protocol
Joo C, Kim KH, Jang BH, Huang CW, Kang JW, Lee JD, Lee S, Lee S
Journal of Pain Research 2023, 16:1095-1101
Published Date: 29 March 2023