Back to Journals » Patient Related Outcome Measures » Volume 14
Acceptability and Feasibility of Delivering Decision Aids to Veterans for Management of Knee Osteoarthritis – A Pilot Study
Authors Reilly CA ![]() , Rice ML
, Rice ML ![]() , Parker DJ
, Parker DJ ![]() , Goodney PP, Lurie JD, Ibrahim SA, Henderson ER
, Goodney PP, Lurie JD, Ibrahim SA, Henderson ER
Received 26 August 2022
Accepted for publication 1 March 2023
Published 22 March 2023 Volume 2023:14 Pages 49—55
DOI https://doi.org/10.2147/PROM.S386937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Clifford A Reilly,1 Makenna L Rice,2 Dylan J Parker,2 Philip P Goodney,3– 6 Jon D Lurie,3,4 Said A Ibrahim,7,8 Eric R Henderson2,4,6
1Larner College of Medicine, University of Vermont, Burlington, VT, USA; 2Department of Orthopaedic Surgery, Dartmouth Hitchcock Medical Center, Lebanon, NH, USA; 3The Dartmouth Institute for Health Policy and Clinical Practice, Dartmouth College, Hanover, NH, USA; 4Geisel School of Medicine, Dartmouth College, Hanover, NH, USA; 5Heart and Vascular Center, Dartmouth Hitchcock Medical Center, Lebanon, NH, USA; 6White River Junction VA Medical Center, US Department of Veterans Affairs, White River Junction, VT, USA; 7Zucker School of Medicine, Hofstra University/Northwell Health, Hempstead, NY, USA; 8Department of Medicine, Long Island Jewish Medical Center, New Hyde Park, NY, USA
Correspondence: Makenna L Rice, Department of Orthopaedic Surgery, Dartmouth Hitchcock Medical Center, 1 Medical Center Dr, Rubin 592, Lebanon, NH, 03756, USA, Tel +1 831 247-1106, Fax +1 603 653-3581, Email [email protected]
Introduction: Decision aids are effective tools in facilitating patient-centered care and patient involvement in the decision-making process. Given unique barriers to providing patient-centered care for Veterans, implementation of decision aids may improve overall quality of care. We aimed to assess the acceptability and feasibility of video-based and pamphlet-based decision aid use in Veterans with knee osteoarthritis.
Materials and Methods: Veterans considering treatment for knee osteoarthritis received either an online video-based aid, pamphlet-based aid, or both before their surgical consult. At their visit, patients completed written pre-visit and post-visit questionnaires. The pre-visit questionnaire included questions about the patient’s demographics, decision-making preferences, experiences using the assigned decision aids, and the Hip-Knee Decision Quality Instrument. The post-visit questionnaire assessed the patient’s overall experience with the decision-making process and how use of the decision aid influenced their discussion with the physician.
Results: All 16 patients who received the pamphlet-based aid reviewed the decision aid before their visit, compared to only five of the 12 patients who received the video-based aid. Thirteen of 20 patients indicated that they preferred to share treatment decision-making with their physician. Seventeen of 20 patients believed they would feel comfortable questioning the treatment recommendation of their surgeon after decision aid use. Most patients reported a positive experience using their decision aid, regardless of modality, and found it easily comprehensible and useful in visit preparation. A preference for a pamphlet-based aid was expressed by the majority of patients.
Conclusion: Veterans considering treatment for knee osteoarthritis are well prepared to engage in a patient-centered care experience. Most patients preferred sharing the decision-making process with their physician and felt comfortable questioning them about treatment recommendations. Decision aids helped Veterans feel more informed about their treatment options and improved engagement and discussion with their physician. Pamphlet-based aids were utilized more reliably than video-based aids.
Keywords: patient-centered care, shared decision-making, decision aid, knee osteoarthritis, military service
Introduction
Military service creates a unique environment for patients engaging in healthcare decision-making.1 Military law requires “the subordination of desires and interests of the individual” to the needs of nation and command, including many medical decisions.2,3 It is reasonable to hypothesize that the healthcare environment associated with military service may have a lasting effect on the way Veterans engage in healthcare decision-making after discharge and impede their access to patient-centered care.4,5 Patient-centered care occurs when the needs, values, and preferences of a well-informed patient are considered.6–9 Previous research has demonstrated that unique barriers exist around ensuring that patients are well informed about their treatment options in the Veteran population and that the Veteran population has lower average decision quality compared to the civilian population.4,10
Decision aids are effective tools in facilitating patient-centered care experiences by helping patients feel more informed regarding their treatment options, better understand their values, improve their perception of associated risks, and take a more active role in the decision-making process.11 However, given the unique barriers around providing patient-centered care in the Veteran population, we must evaluate how to best implement decision aids for those who have served. Because of these barriers to care and lower than average decision quality in this population, Veterans with knee osteoarthritis who are considering surgical treatment options offer an ideal population to study decision aid implementation.4,10 Knee osteoarthritis is classified as a preference-sensitive condition, in which there is more than one acceptable treatment option with substantial advantages and disadvantages for the patient to consider.6,12–14 Furthermore, knee osteoarthritis is common in Veterans and total knee replacement surgeries are associated with a high financial burden for the Veterans Administration. In 2014, 9153 Veterans underwent total knee replacement, resulting in an estimated cost burden of $284 million annually.15,16 The high incidence of and disability due to osteoarthritis further make this population and condition ideal for studying and identifying ways to improve healthcare decision-making in Veterans.
The objective of this pilot study was to field test the acceptability and feasibility of implementing knee osteoarthritis decision aids in the Veterans Affairs (VA) patient population. Like other pilot and feasibility studies, this study was designed to “guide the planning of a large-scale investigation”, in order to avoid unexpected challenges in the larger study.17 We specifically assessed the unique barriers and facilitators of implementation in the Veteran population in a rural setting, with special attention paid to the survey administration process and attrition rate. On a small scale, we examined whether the uptake of the decision aids influences decision quality in patients considering treatment options for knee osteoarthritis. We hypothesized that low-tech, pamphlet-based decision aids, compared to a video-based option, would be more acceptable with fewer barriers to implementation.
Materials and Methods
The study was approved by the Veteran’s Institutional Review Board of New England and is in compliance with the Declaration of Helsinki. We enrolled and consented 30 patients from 2015 to 2017 who were newly referred to the Veterans Affairs orthopaedic clinic with a diagnosis of knee osteoarthritis (ICD-9715.96). Using the same criteria in this pilot as the larger study, we excluded patients with prior joint replacement surgery, preexisting contraindications to surgical or nonsurgical treatments, inflammatory arthritis, knee pain with concomitant hip pain, or cognitive impairment precluding consent. Using a random number generator, a research coordinator assigned all 30 enrolled patients an online video-based decision aid (Emmi Solutions, Chicago, IL, USA),18 a pamphlet-based decision aid (Option GridTM, EBSCO Health, Ipswich, MA, USA),19 or both (Figure 1). Patients received their assigned decision aid(s) to review before their surgical consult and were asked to complete pre- and post-visit questionnaires20 and the Hip-Knee Decision Quality Instrument (HK-DQI).21 In attempt to reflect real technical limitations and increase generalizability to all Veterans, internet access was not a requirement for enrollment.
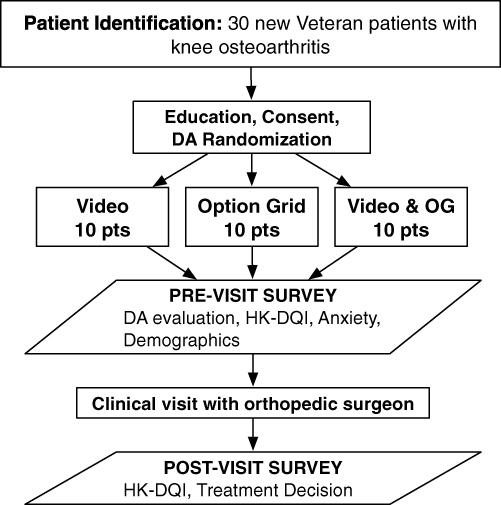 |
Figure 1 Pilot trial flow chart. Abbreviation: VA, Veterans Affairs; DA, Decision Aid; OG, Option Grid; HK-DQI, Hip-Knee Decision Quality Instrument. |
Decision Aids
Group 1 received an online video-based decision aid18 distributed via a unique online log-in code. Group 2 received a pamphlet-based decision aid.19 Group 3 received both decision aids. Participants were asked to review their assigned decision aid materials before their surgical consultation.
Study Measures
At the time of their surgical consultation, patients were administered paper pre-visit and post-visit questionnaires by a research coordinator (Supplemental Document).20 The pre-visit questionnaire included questions about the patient’s demographics, decision-making preferences, and experiences using the assigned decision aids. Patients were also administered the HK-DQI21 at the time of their pre-visit questionnaire. The HK-DQI is a validated instrument with 16 questions measuring the patients’ understanding of their condition, treatment options, treatment benefits, and associated risks of treatment.21 The post-visit questionnaire included questions about the patient’s overall experience with the decision-making process during their surgical consultation and how they feel the use of the decision aid prior to their visit influenced their discussion with the physician. While the surveys were administered in person at the time of their surgical consultation, completion of the surveys was not enforced or incentivized. All statistical analysis was completed using R statistical software,22 although as a pilot study intended to identify procedural challenges and attrition rate, minimal statistical analysis was performed.
Results
Thirty patients were initially enrolled and randomized into three groups of ten patients each. However, only twenty patients completed study questionnaires at their consultation (Table 1). The other ten patients either missed their consultation or declined participation on the day of their visit. The highest rate of attrition was in Group 1, where four of ten patients completed the study. Eight of ten patients each from Groups 2 and 3 completed the study.
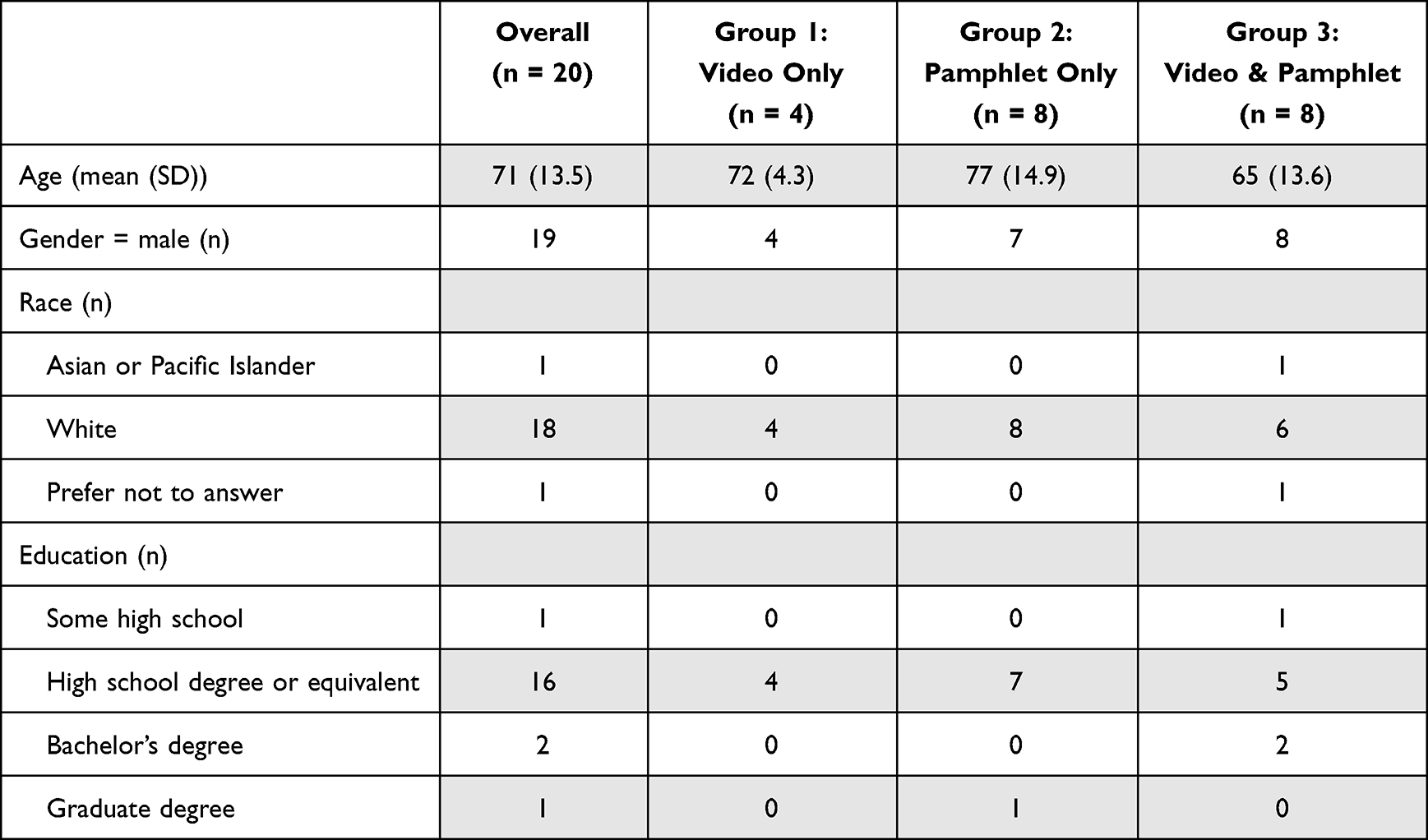 |
Table 1 Demographics by Decision Aid Group |
Decision-Making Preference
Overall, 13 of 20 patients indicated that they preferred to share the responsibility for making a treatment decision with their physician, four preferred to make the final decision after considering their physician’s opinion, two preferred to make the decision without physician input, and one preferred that the physician makes the final decision after seriously considering their opinion. No patients preferred physician-only decision-making. Similarly, 17 of 20 patients either agreed or strongly agreed with the statement “I believe I will feel comfortable questioning the treatment recommendation of my surgeon when I meet him/her today.” Two patients were neutral about the statement and one patient disagreed with the statement.
Decision Aid Use Adherence
Twelve total patients received the video-based aid, four from Group 1 and eight from Group 3. Five of 12 patients successfully viewed the video-based aid before their visit; seven of 12 patients were unable to view the video-based aid. Of the seven who were unable to view the aid, four lacked internet access and three stated they had insufficient free time to view the aid.
Sixteen total patients received the pamphlet-based aid, eight from Group 2 and eight from Group 3. All 16 patients reported that they read the pamphlet in its entirety before their visit. The difference in aid completion when comparing pamphlet-based and video-based aids was considerable.
Decision Aid Preference
Patients reported a positive experience using their decision aid, regardless of their decision aid group. Across all groups, 14 of 20 patients reported that the decision aids were easy to comprehend; 6 of 20 patients felt neutral. Similarly, 13 of 20 patients reported that the aids assisted in visit preparation; 7 of 20 patients felt neutral. Finally, 8 of 20 patients reported that the aids decreased pre-visit anxiety; 12 of 20 patients felt neutral.
Two Group 1 patients indicated the video-based aid provided an appropriate amount of information; the other two were neutral about the amount of information. One Group 2 patient preferred more information, four indicated the pamphlet-based aid provided the right amount of information, and three were neutral about the information amount. One Group 3 patient preferred more information, five believed it was an appropriate amount of information, and two were neutral about the information amount provided in both the video- and pamphlet-based aids.
Three of four Group 1 patients indicated they would prefer a pamphlet-based aid over the video-based aid; one indicated they would prefer the video-based aid. Two of eight Group 2 patients indicated they would prefer a video-based aid over the pamphlet-based aid; five indicated they would prefer the pamphlet-based aid and one indicated no preference. Seven of eight Group 3 patients indicated they would prefer the pamphlet alone and one indicated they would prefer both the video- and the pamphlet-based aids; none indicated preference for the video alone.
Decision Aid – Discussion Facilitation
Two of four Group 1 patients indicated the video-based aid “helped them talk with their physician;” the remaining two were neutral about discussion facilitation. Similarly, four of eight Group 2 patients indicated the pamphlet-based aid facilitated discussion and four were neutral. Seven of eight Group 3 patients indicated that both aids facilitated discussion; one was neutral.
Decision Aid – Decision-Making
When asked if the information helped them make a treatment choice, one Group 1 patient indicated the video-based aid was helpful; three were neutral. Three of eight Group 2 patients indicated the pamphlet-based aid was helpful; four were neutral, and one patient indicated the aid was unhelpful. Seven of eight Group 3 patients indicated the aids were helpful; one was neutral.
Decision Aid – Decision Confidence
Sixteen of twenty patients indicated they had confidence in their treatment decision; four patients were neutral about decision confidence. Of the four neutral patients, two were from Group 1, one from Group 2, and one from Group 3.
Hip-Knee Decision Quality Instrument (HK-DQI)
The HK-DQI knowledge scores for Groups 1–3 were 65%, 58%, and 50%, respectively; decision process scores for Groups 1–3 were 60%, 67%, and 65%, respectively. These differences were not significant; however, this study was not powered nor intended to assess statistical significance of the data collected.
Discussion
In this sample of Veterans considering treatment for knee osteoarthritis who were referred to orthopedic clinic, we found that Veterans are open to engaging in a patient-centered care experience. None of the patients in this study preferred the decision-making responsibility to be placed entirely on the physician and the majority of patients preferred to share the responsibility equally with their physician. Similarly, the majority of patients did not feel uncomfortable questioning their physician about treatment recommendations.
We observed lower levels of successful decision aid use for the video-based decision aid. The majority of patients who received the video-based aid encountered barriers that prevented them from watching the video before their orthopaedic consultation. Furthermore, the group that received only the video-based decision aid had the highest attrition rate. While this high attrition rate is a limitation of this study, it also may be indicative of the barriers Veterans experienced around viewing the video-based decision aid. The pamphlet-based decision aid had an adherence rate of 100%, which suggests that the pamphlet format is easier for Veterans to access and use. In addition, the majority of Veterans indicated that, if the process were repeated, a preference for the pamphlet format. Further, research will be required to understand the barriers that contributed to the poor adherence of the video-based aid. However, it is likely that there were significant barriers around access to internet and technological literacy that contributed to low usage of the online video-based aid.
All participating Veterans reported a positive or neutral experience using decision aids, with no reported deficits in comprehension and positive effects on consultation preparedness and reduced pre-consultation anxiety. Similarly, the majority of the veterans felt the decision aids contained an appropriate amount of information regarding treatment options. Overall, the use of decision aids was well accepted by the cohort of Veterans in this study, suggesting that the use of decision aids is a promising avenue for improving patient-centered care in VA.
This pilot study was not powered to compare decision aid influence on patient knowledge. When aggregated, however, the average knowledge score in this study was 56%, which compares favorably to previous findings where Veterans with osteoarthritis and no decision aid exposure had an average knowledge score of 45%.4 These findings indicate that decision aids are effective for Veterans, although non-Veteran patients exposed to decision aids had an average knowledge score of 68%, suggesting that decision aids alone may not be sufficient to optimize patient knowledge.4 Additional work is required to identify and remove barriers to providing a truly patient-centered care model for Veterans, which should in turn be implemented as policy to extend benefits across VA. Because of its ubiquity, relative surgical indications, and treatment equipoise, knee osteoarthritis is an ideal disease in which to study this important question.
This study has several limitations. First, the small overall sample size prohibited formal statistical analysis about decision aid effectiveness and acceptability. As a pilot study, the goal was not to generate robust data for statistical analysis but to assess the feasibility of the study and identify areas of improvement in methodology in preparation for a larger study.17 According to the recommendations by Thabane et al on pilot study design, sample size is less important than the sample being representative of the target study population, and “should be large enough to provide useful information about the aspects that are being assessed for feasibility”, both of which are accomplished here.17 Second, there was a high attrition rate in this study. The higher attrition rate in the group that received only the video-based decision aid makes it difficult to compare across the three decision aid groups and also imparts some selection bias. While these factors limit the strength of the conclusions we can draw from these preliminary data, they present areas for improvement in the methodology for a subsequent study.
The limitations of this pilot study, including small size and high attrition rate, present opportunities to modify the methodology for the future study. With over 9 thousand Veterans undergoing total knee replacement annually,15 there is ample opportunity for a large number of patients enrolled in a relatively short period of time, depending on the number of treatment centers involved. The high attrition rate should be taken into account when selecting the size of the enrollment group and when considering distribution of the decision aids and questionnaires. There was a higher attrition rate in the video-based decision aid group, which could be addressed by having the patients view the decision aid in the office just prior to their appointment. However, part of this higher attrition rate is due to lack of internet or computer access at home. Eliminating this barrier would limit the generalizability to the Veteran population for widespread, in-home use. The attrition rate could be improved by increasing the in-office completion of pre- and post-visit questionnaires by checking for their completion at surgical consultation appointment check in and check out. Despite these limitations, the results of this pilot study are promising and confirm that further work is warranted to determine how to best implement decision aids in the Veteran population.
Conclusion
In this sample of Veterans considering treatment for knee osteoarthritis, we found that Veterans are well prepared to engage in a patient-centered care experience. None of the patients in this study preferred the decision-making responsibility to be placed entirely on the physician and the majority of patients preferred to share the responsibility equally with their physician. Similarly, the majority of patients felt comfortable questioning their physician about treatment recommendations. Decision aids helped Veterans feel more informed about their treatment options and better engage in discussion with their physician. Pamphlet-based aids were utilized at a higher rate than online video-based aids. Further research is needed to fully understand best practice for decision aid deployment in the Veteran population and understand the effect on patient knowledge.
Funding
This study was funded by the VA Early Career Development Award (V1CDA2015-34). The sponsor had no involvement in any of the stages from study design to submission of the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maya H. Patient-physician relationships in the military. Heal Law Policy. 2008;2(1):8.
2. Defense D of, ed. The FDA may decide that potential recipients of a drug under an emergency use authorization should have the option to refuse it. The president may waive this option for military personnel; 2014. Army Regul.
3. Defense D of, ed. A soldier on active duty or active duty for training will usually be required to submit to medical care considered necessary to preserve his or her life, alleviate undue suffering, or protect of maintain the health of others; 2014. Army Regul.
4. Henderson ER, Titus AJ, Keeney BJ, Goodney PP, Lurie JD, Ibrahim SA. Military service and decision quality in the management of knee osteoarthritis. Mil Med. 2018;183(7–8):e208–e213. doi:10.1093/milmed/usy104
5. Mazur DJ, Hickam DH. Patients’ preferences for risk disclosure and role in decision making for invasive medical procedures. J Gen Intern Med. 1997;12(2):114–117. doi:10.1007/s11606-006-5006-8
6. Bozic KJ, Chiu V. Emerging ideas: shared decision making in patients with osteoarthritis of the Hip and knee. Clin Orthop Relat Res. 2011;469(7):2081–2085. doi:10.1007/s11999-010-1740-7
7. Bozic KJ, Lau E, Kurtz S, et al. Patient-related risk factors for periprosthetic joint infection and postoperative mortality following total Hip arthroplasty in Medicare patients. J Bone Jt Surg Am. 2012;94(9):794–800. doi:10.2106/JBJS.K.00072
8. Sepucha KR, Fowler FJ, Mulley AG. Policy support for patient-centered care: the need for measurable improvements in decision quality. Health Aff. 2004;23(Suppl2):VAR-54-VAR–62. doi:10.1377/hlthaff.var.54
9. Strull WM, Lo B, Charles G. Do patients want to participate in medical decision making? JAMA. 1984;252(21):2990–2994. doi:10.1001/jama.1984.03350210038026
10. Sabatino MJ, Reilly CA, Kunkel ST, et al. Duration of military service is associated with decision quality in Veterans considering total knee replacement: case series. Patient Relat Outcome Meas. 2019;10:209–215. doi:10.2147/PROM.S163691
11. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017. doi:10.1002/14651858.CD001431.pub5
12. Wennberg JE. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ. 2002;325(7370):961–964. doi:10.1136/bmj.325.7370.961
13. O’Connor AM, Llewellyn-Thomas HA, Flood AB. Modifying unwarranted variations in health care: shared decision making using patient decision aids. Heal Aff. 2004;23(Suppl2):VAR63–VAR72. doi:10.1377/hlthaff.var.63
14. Slover J, Shue J, Koenig K. Shared decision-making in orthopaedic surgery. Clin Orthop Relat Res. 2012;470(4):1046–1053. doi:10.1007/s11999-011-2156-8
15. Department of Veterans Affairs- National Surgery Office. Q1 FY15 VA National Surgery Office Quarterly Report. Department of Veterans Affairs- National Surgery Office; 2015.
16. Losina E, Walensky RP, Kessler CL, et al. Cost-effectiveness of Total Knee Arthroplasty in the United States. Arch Intern Med. 2009;169(12):1113. doi:10.1001/archinternmed.2009.136
17. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. 2010;10(1). doi:10.1186/1471-2288-10-1
18. Emmi Solutions. Patient engagement programs. Available from: https://www.emmisolutions.com/.
19. EBSCO Health. Option grid decision aids. Available from: https://health.ebsco.com/products/option-grid.
20. HealthMeasures PROMIS. Available from: www.healthmeasures.net/PROMIS.
21. Sepucha KR, Stacey D, Clay CF, et al. Decision quality instrument for treatment of Hip and knee osteoarthritis: a psychometric evaluation. BMC Musculoskelet Disord. 2011;12:149. doi:10.1186/1471-2474-12-149
22. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development, Validity, and Reliability of Three Instruments to Assess Holistic Care from Different Perspectives

Fang CK, Pi SH, Li IF
Journal of Multidisciplinary Healthcare 2025, 18:3647-3671
Published Date: 24 June 2025