Back to Journals » Patient Preference and Adherence » Volume 19
A Systematic Review of Patient Preferences, Expectations, and Values for the Management and Treatment of Graves Disease
Authors Chen Y ![]() , Ren Z, Zhou X
, Ren Z, Zhou X ![]() , Gao P
, Gao P ![]()
Received 4 June 2025
Accepted for publication 13 September 2025
Published 19 September 2025 Volume 2025:19 Pages 2949—2957
DOI https://doi.org/10.2147/PPA.S540261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Yingjie Chen,1,* Zonghao Ren,2,* Xiujuan Zhou,3 Peiyang Gao3
1School of Clinical Medicine, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Department of Endocrinology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 3Department of Critical Care Medicine, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peiyang Gao, Department of Critical Care Medicine, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected] Xiujuan Zhou, Department of Critical Care Medicine, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected]
Objective: To systematically synthesize evidence on treatment preferences, values, and expectations among patients with Graves’ disease (GD), in order to understand the disease’s impact on quality of life and inform clinical decision-making..
Methods: PubMed, Embase, Web of Science, and Cochrane Library were searched for articles about GD, patient preferences, and expectations from database inception to December 2024. Studies included in the review must report raw data on patient-reported outcomes, preferences or experiences relating to GD, and must undergo quality assessment according to the Agency for Healthcare Research and Quality (AHRQ).
Results: Twenty-one studies involving patients with GD were included. Although preferences varied, several trends emerged: 1) Most patients reported that GD significantly disrupted their quality of life and social functioning, with 60% experiencing severe discomfort. 2) Antithyroid drugs (ATD) was the most preferred initial treatment (64%), followed by surgery (25%) and radioactive iodine therapy (RAI) (11%), with concerns about radioactivity and surgical complications influencing decisions. 3) Key factors affecting treatment choices included remission rates, recovery time, impact on daily life, and physician recommendations. 4) Graves’ ophthalmopathy (GO) patients faced additional challenges, including social withdrawal and appearance-related distress, with female patients expressing greater concern about disfigurement.
Conclusion: This systematic review indicates that GD, particularly GO, significantly impairs patients’ self-confidence, quality of life, and social functioning. Treatment choices are influenced by expected outcomes, personal circumstances, psychological concerns, and economic factors. ATD remains the preferred first-line treatment, though individual preferences vary significantly, emphasizing the importance of personalized approaches and decision aids.
Keywords: graves disease, patient preferences, shared decision-making, treatment expectations, graves ophthalmopathy, systematic review
Introduction
Graves Disease (GD) is a complex immune-mediated disease caused by autoantibodies. Autoantibodies activate thyroid-stimulating hormone receptors, stimulating the synthesis and secretion of thyroid hormone and thyroid growth.1 GD induces a hyperthyroid state marked by thyrotoxicosis, triggering multisystem manifestations. Neuromuscular disturbances (tremors, irritability, insomnia), metabolic dysregulation (unintentional weight loss, heat intolerance), and cardiopulmonary sequelae (tachycardia, dyspnea, atrial fibrillation) are pathognomonic, often accompanied by goitrous thyroid enlargement.2 A cohort study of 500,000 people showed that the incidence of atrial fibrillation in patients with thyrotoxicosis over the age of 65 was approximately 13%.3 In addition, Graves Ophthalmopathy (GO) is also a common complication of GD, with an incidence of 25%-50%, causing great damage to the patient’s vision and even the risk of vision loss.4,5
The current treatments for GD mainly include antithyroid drugs (ATD), radioactive iodine therapy (RAI), and thyroidectomy.6 Because the treatment methods are controversial, treatment selection is challenging for both patients and doctors.7 In addition, as a chronic disease, long-term management of the disease is also a continuous physical and mental burden for patients. Current clinical decision-making focuses on achieving biochemical targets for thyroid function and controlling complications, but pays insufficient attention to patients’ subjective treatment experience, quality of life needs, and value trade-offs.8 The purpose of this study is to systematically summarize evidence on treatment options and clinical outcome determinants for Graves’ disease (GD). The study also aims to resolve controversies between various therapies and identify unmet needs of GD patients, with the ultimate goal of optimizing personalized treatment choices.
Methods
Selection Criteria
This systematic review was registered in PROSPERO (CRD42024614238) and employed a structured literature search focusing on three core aspects: adult populations with GD, research exploring patient-centred outcomes (such as preferences, expectations and values in disease management), factors influencing treatment decision-making. Exclusions included topics unrelated to GD, publications in languages other than English, and non-primary research formats (eg reviews, letters, posters).
Data Sources and Search Strategy
Four electronic databases (PubMed, Embase, Web of Science and Cochrane Library) were systematically queried from their respective inception dates until December 2024. In order to comprehensively retrieve relevant literature, a strategy combining MeSH terms and keyword searching was employed, with PubMed being used as a case. The initial literature search on GD was conducted using MeSH terms, followed by keyword searches in the title or abstract using terms such as “Graves” disease’, “hyperthyroidism”, and so forth. These searches were subsequently merged. The same approach was applied to the literature search, with a focus on “patient preference”, “patient compliance” or “patient values”. The results of the disease and patient preference components were then combined. Table 1 shows the PubMed search strategy. Equivalent syntax adaptations were applied to other platforms based on their respective indexing systems.
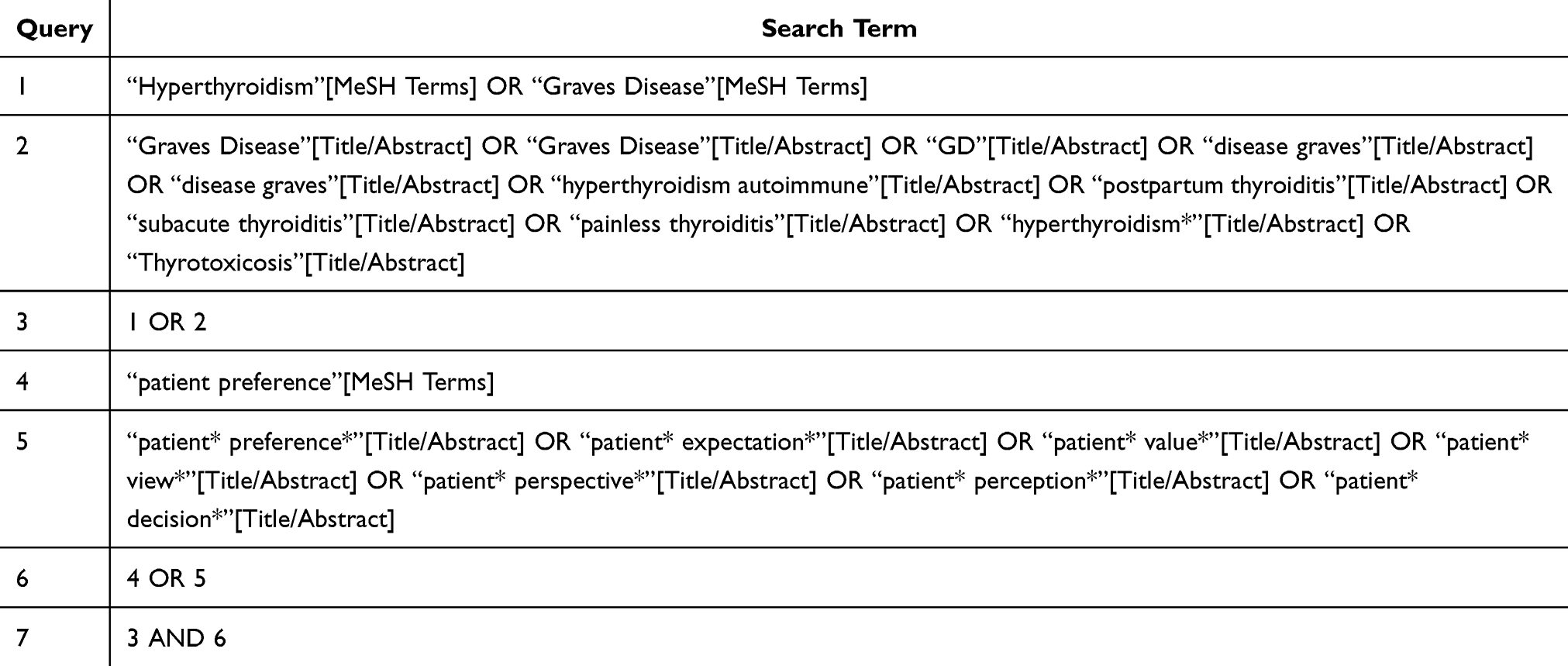 |
Table 1 Search Strategy for PubMed |
Data Extraction and Quality Assessment
The process of literature review entailed independent screening of studies by two authors based on established inclusion and exclusion criteria. The initial screening process was conducted on the basis of a title and abstract review. Disagreements were addressed through discussion or correspondence with the corresponding authors. Data extraction for study type, study design, sample size, etc. was conducted independently by two reviewers, with guidance provided by the Agency for Healthcare Research and Quality (AHRQ).9 This scale, a standard tool for evaluating observational studies, employs an 11-point checklist with “Yes” (1 point), “No” (0 points), and “Uncertain” (0 points) as potential responses. The evaluation of studies was conducted using a structured grading system, categorizing them as low (0–3), moderate (4–7), or high (8–11) quality based on their scores. As illustrated in Figure 1, the flow diagram delineates the systematic review process.
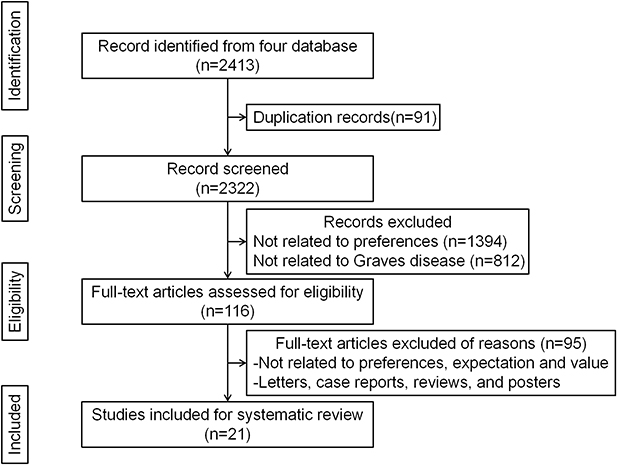 |
Figure 1 Flow diagram of the systematic literature review process. From an initial 2413 records identified from four databases, 91 duplicates were removed. The remaining 2322 records were screened, leading to the exclusion of 2206 records (1394 not related to preferences and 812 not related to Graves’ disease). The remaining 116 full-text articles were assessed for eligibility, of which 95 were excluded for various reasons (not related to preferences, expectations, and values; or being letters, case reports, reviews, or posters). This resulted in a final selection of 21 studies included for the systematic review. |
Result
Characteristics of Included Studies
A total of 2413 articles were included in the four databases. After deduplication and browsing the title and abstracts, 116 articles were found. After reading the full text, 21 articles met the inclusion criteria. Studies on patients’ cognition and preferences for hyperthyroidism were mainly distributed in the United Kingdom (n=6), the United States (n=6), New Zealand (n=4), Sweden (n=1), Italy (n=1), Denmark (n=1), Czech Republic (n=1) and Australia (n=1). The time span of the included literature was from 1998 to 2024. The time span of the included literature was from 1998 to 2024. Despite the age of some of the literature, its systematic reporting of patients’ views of GD, the factors influencing their choice of treatment plan, and the results of their final choice renders it relevant for inclusion. Table 2 provides a summary of the 21 studies, including sample size, study type, study description and the most important research results.
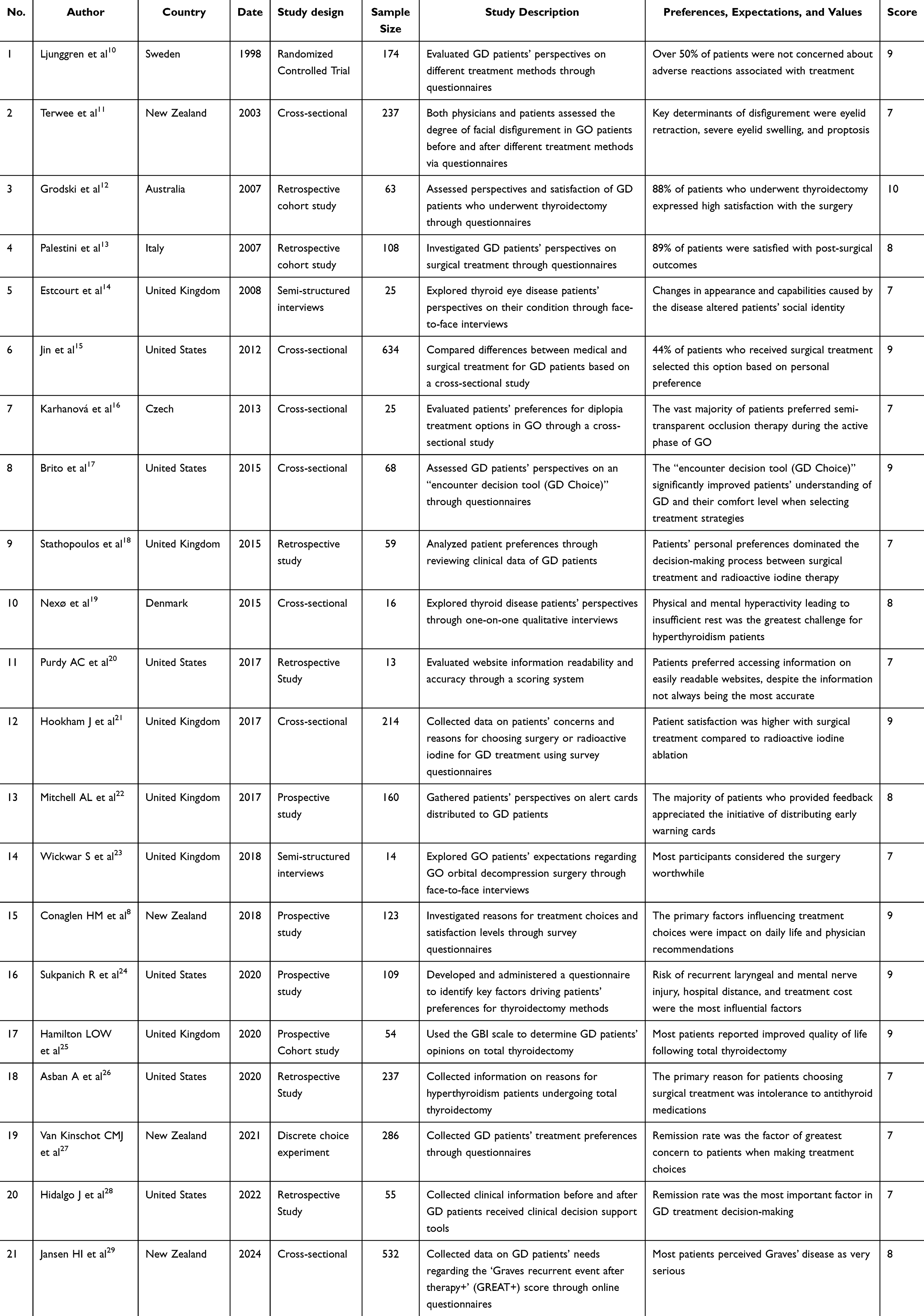 |
Table 2 Characteristics of Included Studies and Summary of Results |
Quality of Life and Social Functioning Impairment in Patients with GD
Patients with GD frequently experience significant disruption to their quality of life and social functioning. Ljunggren et al reported that 60% of GD patients experienced severe discomfort, with 66% acknowledging that the disease impaired their social interactions.10 In a similar vein, Palestini et al found that 66% of GD patients perceived the disease as detrimental to their normal daily activities, although 89% did not consider medication treatment and regular examinations burdensome.13 Nexø et al highlighted a common challenge where patients struggled to distinguish whether their symptoms were disease-related, leading to delayed diagnosis; additionally, most participants expressed a desire for greater recognition of their disease status from others.19 Regarding information-seeking behaviors, Purdy et al observed that patients preferred accessing private websites with lower readability barriers, despite these sources having lower accuracy rates compared to academic, governmental, and nonprofit websites which offered more accurate information but presented higher barriers to comprehension.20
Patterns and Drivers of Treatment Preferences: Multidimensional Concerns and Heterogeneity in Patient Choices
Treatment preferences among GD patients vary considerably and are influenced by multiple factors. Ljunggren et al noted that over 92% of patients expressed satisfaction with their chosen treatment, although dissatisfaction events were more frequent in the surgical group compared to the medication group; notably, patients’ primary concern regarding RAI treatment stemmed from fear of radioactive isotopes.10 Grodski et al reported that one-third of patients opted for surgery as their definitive treatment despite the absence of specific indications,12 while Jin et al identified economic factors as crucial determinants in patients’ decisions between surgical versus medical treatment.15 Decision-making tools such as “GD Choice” were found by Brito et al to effectively enhance patients’ understanding and decision-making regarding GD treatment options.17 According to Stathopoulos et al, patients typically preferred surgical intervention over RAI therapy after failed medical treatment, primarily due to radiophobia.18
Patient concerns regarding specific treatment modalities have been well-documented in the literature. Hookham et al discovered that common reasons for refusing surgery included concerns about general anesthesia, scarring, and voice changes, while RAI was often rejected due to risks of close contact restrictions and disease exacerbation; significantly, 92% of patients found physician discussions beneficial for decision-making.21 Conaglen et al reported treatment distribution as: 64% receiving ATD, 11% RAI, and 25% surgery, with recovery time and impact on daily life being patients’ primary concerns when making treatment decisions.8 Age-related preferences were noted by Sukpanich et al, with patients ≤60 years more accepting of “TransOral Endoscopic Thyroidectomy - Vestibular Approach (TOETVA)”, while those >60 years preferred traditional incisions.24 Hamilton et al found that most patients could tolerate only minor post-surgical side effects such as weight gain and mood changes.25
Treatment selection patterns and long-term considerations also emerged as important themes. Asban et al observed that most patients initially preferred ATD treatment, considering surgery only after developing drug intolerance, resistance, or obstructive symptoms.26 Van Kinschot et al determined that ATD remained patients’ most preferred treatment option, with generally negative attitudes toward RAI compared to surgery.27 Hidalgo et al noted patients’ unwillingness to commit to long-term ATD therapy.28 Finally, Jansen et al reported that the “Graves recurrent event after therapy+ (GREAT+)” score effectively predicted individual recurrence probability after ATD discontinuation, with 55% of patients choosing RAI or thyroidectomy when facing higher recurrence probabilities.29
Psychosocial Burden, Social Dysfunction and Multidimensional Interventions in Patients with GO
GO presents unique challenges that influence patient management approaches and outcomes. Estcourt et al suggested that non-face-to-face communication methods, such as internet and telephone consultations, might be more suitable for GO patients.14 Terwee et al discovered that GD patients typically overestimated the severity of disfigurement caused by GO, with female patients expressing greater concern about appearance-related changes.11 The psychosocial impact was highlighted by Estcourt et al, who noted that GO led to significant changes in patients’ daily lives, resulting in social withdrawal.14 Regarding management strategies, Karhanová et al recommended semi-transparent occlusion for patients during the active phase of GO and while awaiting surgery.16 Mitchell et al found that distributing GO warning cards helped improve patients’ understanding of the condition and increased GO diagnosis rates.22 Post-surgical perspectives were examined by Wickwar et al, who reported that patients generally experienced improvements in appearance and health status following orbital decompression surgery, though dissatisfaction commonly stemmed from issues related to surgical care and rehabilitation processes.23
Discussion
GD is the most common cause of thyrotoxicosis, affecting approximately 3% of women and 0.5% of men over their lifetime.30 Conventional treatment options of ATD, RAI, or thyroidectomy have remained largely unchanged for many years, although most patients relapse after a course of ATD or require lifelong thyroid hormone replacement therapy after RAI or surgery.31 Each treatment approach has its limitations. ATDs are non-invasive and do not require surgery or radiation, but their disadvantages may be the need for long-term medication and possible side effects such as liver damage and neutropenia.32 RAI has the advantage of being a one-time treatment, but its disadvantages are permanent hypothyroidism and the possibility of relapse after treatment.33 Thyroidectomy can quickly and more completely relieve the disease, but there are risks such as lifelong hypothyroidism and nerve damage.34 Understanding the preferences and treatment expectations of GD patients can help patients and clinicians make more personalized decisions and improve patient well-being and compliance.
This study included 21 articles, summarizing GD patients’ views on the disease, their expectations for treatment, and their views and treatment preferences for GO. The results showed that most GD patients believed that the disease affected their normal lives, especially those with GO, and they were eager to get help. However, there are currently limited channels for obtaining popular science knowledge about graves, and there are problems such as high barriers to access and insufficient accuracy. Therefore, more accessible and understandable channels must be established through official outlets for the prevention and treatment of Graves’ disease. These channels could include regular community education, science popularization websites, and early warning cards. Clinicians should also help patients cope with the psychological stress caused by the disease.
This study showed that most patients prefer ATD treatment due to fear of radioactive substances and surgery as well as economic factors. Although current studies have shown that ATD treatment is effective and safe, the adverse reactions and compliance issues of the drug are still not suitable for some Graves patients.35 Therefore, clinicians can use predictive tools to improve risk assessment, identify patient preferences, strengthen communication with patients to clarify their core demands, and develop individualized treatment for each Graves patient.
Limitations
This study was a qualitative retrospective analysis, and some of the included literature was not precise enough about the preferences and expectations of GD patients. In addition, there was no precise and standardized information to quantify patients’ preferences, expectations, and values. The methods used to review the literature and summarize the research results were somewhat empirical and subjective, which may lead to biased results.
Conclusion
This systematic review demonstrates that the disease significantly impairs quality of life and social functioning of GD patients, especially GO patients. Treatment choices are influenced by expected outcomes, personal circumstances, psychological concerns, and economic factors. ATD remains the preferred first-line treatment. However, individual preferences vary significantly, which emphasizes the importance of personalized approaches and decision aids. Additionally, establishing effective communication channels is crucial to helping GD patients better understand the indications and prognosis of RAI, and thyroidectomy, as well as for making shared decisions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoang TD, Stocker DJ, Chou EL, et al. 2022 update on clinical management of graves disease and thyroid eye disease. Endocrinol Metab Clinics North Am. 2022;51(2):287–304. doi:10.1016/j.ecl.2021.12.004
2. Viola N, Colleo A, Casula M, et al. Graves’ disease: is it time for targeted therapy? A narrative review. Medicina. 2025;61(3):500. doi:10.3390/medicina61030500
3. Selmer C, Olesen JB, Hansen ML, et al. The spectrum of thyroid disease and risk of new onset atrial fibrillation: a large population cohort study. BMJ. 2012;345(nov27 1):e7895. doi:10.1136/bmj.e7895
4. Cui X, Wang F, Liu C. A review of TSHR- and IGF-1R-related pathogenesis and treatment of graves’ orbitopathy. Front Immunol. 2023;14:1062045. doi:10.3389/fimmu.2023.1062045
5. Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European group on graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43–G67. doi:10.1530/EJE-21-0479
6. Sundaresh V, Brito JP, Wang Z, et al. Comparative effectiveness of therapies for graves’ hyperthyroidism: a systematic review and network meta-analysis. J Clin Endocrinol Metab. 2013;98(9):3671–3677. doi:10.1210/jc.2013-1954
7. Taprogge J, Gape PMD, Carnegie-Peake L, et al. A systematic review and meta-analysis of the relationship between the radiation absorbed dose to the thyroid and response in patients treated with radioiodine for graves’ disease. Thyroid. 2021;31(12):1829–1838. doi:10.1089/thy.2021.0302
8. Conaglen HM, Tamatea JAU, Conaglen JV, et al. Treatment choice, satisfaction and quality of life in patients with graves’ disease. Clin Endocrinol. 2018;88(6):977–984. doi:10.1111/cen.13611
9. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
10. Ljunggren JG, Törring O, Wallin G, et al. Quality of life aspects and costs in treatment of graves’ hyperthyroidism with antithyroid drugs, surgery, or radioiodine: results from a prospective, randomized study. Thyroid. 1998;8(8):653–659. doi:10.1089/thy.1998.8.653
11. Terwee CB, Dekker FW, Bonsel GJ, et al. Facial disfigurement: is it in the eye of the beholder? A study in patients with graves’ ophthalmopathy. Clin Endocrinol. 2003;58(2):192–198. doi:10.1046/j.1365-2265.2003.01695.x
12. Grodski S, Stalberg P, Robinson BG, et al. Surgery versus radioiodine therapy as definitive management for graves’ disease: the role of patient preference. Thyroid. 2007;17(2):157–160. doi:10.1089/thy.2006.0141
13. Palestini N, Grivon M, Durando R, et al. Thyroidectomy for graves’ hyperthyroidism. retrospective study of patients’ appreciation. Ann Ital Chir. 2007;78(5):405–412.
14. Estcourt S, Vaidya B, Quinn A, et al. The impact of thyroid eye disease upon patients’ wellbeing: a qualitative analysis. Clin Endocrinol. 2008;68(4):635–639. doi:10.1111/j.1365-2265.2007.03087.x
15. Jin J, Sandoval V, Lawless ME, et al. Disparity in the management of graves’ disease observed at an urban county hospital: a decade-long experience. Am J Surg. 2012;204(2):199–202. doi:10.1016/j.amjsurg.2011.10.010
16. Karhanová M, Kalitová J, Vláčil O, et al. Conservative management options for thyroid disease induced diplopia. Cesk Slov Oftalmol. 2013;69(5):220–224. Czech.
17. Brito JP, Castaneda-Guarderas A, Gionfriddo MR, et al. Development and pilot testing of an encounter tool for shared decision making about the treatment of graves’ disease. Thyroid. 2015;25(11):1191–1198. doi:10.1089/thy.2015.0277
18. Stathopoulos P, Gangidi S, Kotrotsos G, et al. Graves’ disease: a review of surgical indications, management, and complications in a cohort of 59 patients. Int J Oral Maxillofac Surg. 2015;44(6):713–717. doi:10.1016/j.ijom.2015.02.007
19. Nexø MA, watt T, Cleal B, et al. Exploring the experiences of people with hypo- and hyperthyroidism. Qual Health Res. 2015;25(7):945–953. doi:10.1177/1049732314554093
20. Purdy AC, Idriss A, Ahern S, et al. Dr Google: the readability and accuracy of patient education websites for graves’ disease treatment. Surgery. 2017;162(5):1148–1154. doi:10.1016/j.surg.2017.07.011
21. Hookham J, Truran P, Allahabadia A, et al. Patients’ perceptions and views of surgery and radioiodine ablation in the definitive management of graves’ disease. Postgrad Med J. 2017;93(1099):266–270. doi:10.1136/postgradmedj-2015-133756
22. Mitchell AL, Hickey J, Vaidya B, et al. Raising awareness of graves’ orbitopathy with early warning cards. Clin Endocrinol. 2017;87(6):853–859. doi:10.1111/cen.13438
23. Wickwar S, McBain H, Edmunds MR, et al. Patients’ expectations for the functional and psychosocial outcomes of orbital decompression surgery for thyroid eye disease: a qualitative study. Psychol Health Med. 2018;23(4):475–484. doi:10.1080/13548506.2017.1356930
24. Sukpanich R, Sanglestsawai S, Seib CD, et al. The influence of cosmetic concerns on patient preferences for approaches to thyroid lobectomy: a discrete choice experiment. Thyroid. 2020;30(9):1306–1313. doi:10.1089/thy.2019.0821
25. Hamilton LOW, Lim AE, Clark LJ. Total thyroidectomy for graves’ disease-what do our patients think? A qualitative cohort study to evaluate the surgical management of graves’ disease. Surgeon. 2020;18(4):193–196. doi:10.1016/j.surge.2019.09.005
26. Asban A, Anue A, Xie R, et al. Increasing use of thyroidectomy as definitive treatment for hyperthyroidism. J Surg Res. 2020;246:435–441. doi:10.1016/j.jss.2019.09.020
27. van Kinschot CMJ, Soekhai VR, de Bekker-Grob EW, et al. Preferences of patients and clinicians for treatment of graves’ disease: a discrete choice experiment. Eur J Endocrinol. 2021;184(6):803–812. doi:10.1530/EJE-20-1490
28. Hidalgo J, Vallejo S, El Kawkgi OM, et al. Individualized graves’ disease remission rates conversations: a videographic analysis of medical encounters. Endocrine. 2022;76(1):237–239. doi:10.1007/s12020-022-02989-x
29. Jansen HI, Heuveling van Beek C, Bisschop PH, et al. The need for the GREAT+ score to predict relapse in Graves’ disease: a questionnaire among patients and internal medicine specialists. J Endocrinol Invest. 2024;47(10):2499–2505. doi:10.1007/s40618-024-02358-7
30. Lane LC, Wood CL, Cheetham T. Graves’ disease: moving forwards. Arch Dischildhood. 2023;108(4):276–281. doi:10.1136/archdischild-2022-323905
31. Azizi F, Mehran L, Abdi H, et al. Approach to the patient considering long-term antithyroid drug therapy for graves’ disease. J Clin Endocrinol Metab. 2024;109(10):e1881–e1888. doi:10.1210/clinem/dgae456
32. Kim KJ, Choi J, Kim KJ, et al. Cancer risk in graves disease with radioactive (131)I treatment: a nationwide cohort study. J Nucl Med. 2024;65(5):693–699. doi:10.2967/jnumed.123.266531
33. Schiavone D, Crimì F, Cabrelle G, et al. Role of lugol solution before total thyroidectomy for graves’ disease: randomized clinical trial. Br J Surg. 2024;111(8):znae196. doi:10.1093/bjs/znae196
34. Meling Stokland A-E, Austdal M, Nedrebø BG, et al. Outcomes of patients with graves disease 25 years after initiating antithyroid drug therapy. J Clin Endocrinol Metab. 2024;109(3):827–836. doi:10.1210/clinem/dgad538
35. Grixti L, Lane LC, Pearce SH. The genetics of graves’ disease. Rev Endocr Metab Disord. 2024;25(1):203–214. doi:10.1007/s11154-023-09848-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient Preference Studies for Advanced Prostate Cancer Treatment Along the Medical Product Life Cycle: Systematic Literature Review
Menges D, Piatti MC, Cerny T, Puhan MA
Patient Preference and Adherence 2022, 16:1539-1557
Published Date: 28 June 2022
A Systematic Review of Patient Preferences, Expectations, and Values for the Management and Treatment of Hypertension
Xu X, Guo T, Liu Z, Chen P, Zhang Y, Ji Q, Xie H
Patient Preference and Adherence 2022, 16:2867-2876
Published Date: 20 October 2022
Preferred Conversation Topics with Respect to Treatment Decisions Among Individuals with Type 2 Diabetes
Tichler A, Hertroijs DFL, Ruwaard D, Brouwers MCGJ, Hiligsmann M, de Jong JD, Elissen AMJ
Patient Preference and Adherence 2023, 17:719-729
Published Date: 17 March 2023
Preferences and Adherence of People with Prediabetes for Disease Management and Treatment: A Systematic Review
Ren Z, Xu X, Yue R
Patient Preference and Adherence 2023, 17:2981-2989
Published Date: 15 November 2023
Patients’ Preferences for Attributes of Oral vs Injectable Androgen Deprivation Therapy in Prostate Cancer: A Discrete Choice Experiment

Collins SP, Hong A, Hauber B, Flanders SC, Will O, Maculaitis MC, Gatoulis SC, Chakoian M, Thorley J
Patient Preference and Adherence 2025, 19:1397-1409
Published Date: 9 May 2025