Back to Journals » Patient Preference and Adherence » Volume 16
A Systematic Review of Patient Preferences, Expectations, and Values for the Management and Treatment of Hypertension
Authors Xu X, Guo T ![]() , Liu Z, Chen P, Zhang Y, Ji Q, Xie H
, Liu Z, Chen P, Zhang Y, Ji Q, Xie H
Received 1 September 2022
Accepted for publication 12 October 2022
Published 20 October 2022 Volume 2022:16 Pages 2867—2876
DOI https://doi.org/10.2147/PPA.S388356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Xianpeng Xu,1 Tao Guo,1 Zifeng Liu,1 Peng Chen,1 Ying Zhang,1 Qingjie Ji,2 Hui Xie1
1Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Quzhou Hospital of Traditional Chinese Medicine, Quzhou, People’s Republic of China
Correspondence: Hui Xie, Hospital of Chengdu University of Traditional Chinese Medicine, No. 39 Shi-er-qiao Road, Chengdu, 610072, Sichuan Province, People’s Republic of China, Email [email protected]
Objective: To comprehensively summarize the evidence on the preferences, expectations, and values of hypertension management and treatment in hypertensive patients.
Methods: From inception through January 2022, PubMed, Embase, Web of Science, EBSCO, and China National Knowledge Infrastructure were searched for studies with hypertension value, preference, or expectation. A qualitative retrospective analysis was performed.
Results: A total of 24 studies involving 8701 participants were included. Although studies on the preferences of hypertensive patients are difficult to standardize, considerable convergence has occurred: 1) Patients preferred treatment regimens with lower incidence of comorbidities, faster response, lower cost, more frequent blood pressure monitoring, fewer side effects, and more convenient medication. 2) Patients have a crucial role in the treatment, and their physicians are expected to develop a shared patient-centered decision-making model.
Conclusion: The results of this systematic review demonstrated that side effects, cost, and convenience are important factors for patients when selecting a treatment regimen for hypertension. Patients often obtain hypertension information from their physicians and prefer shared patient-centered decision-making.
Keywords: patient preferences, hypertension, hypertension management, systematic review
Introduction
Hypertension is a critical risk factor for cardiovascular and cerebrovascular disease, affecting the heart, brain, kidneys, and other human organs.1 The high prevalence and low control rate of hypertension in the United States are worrying, and the global trend is not optimistic, particularly in low- and middle-income countries.2 Effective antihypertensive treatment can reduce all-cause and cardiovascular mortality, as well as the risk of cardiovascular events, including coronary heart disease (CHD), stroke, and heart failure.3 Although hypertension is a preventable and controllable condition, its outcomes are largely dependent on government disease control measures, doctor treatment strategies, patient adherence, and family member help.4 Furthermore, most hypertensive patients are asymptomatic and may be unaware of the need for treatment since they have no symptoms that compel them to seek treatment, even if they have mild clinical symptoms.5
Although definitions of hypertension vary among guidelines, the indications and treatment regimens for antihypertensive treatment are relatively similar. Currently, the major treatment options for hypertension are divided into non-pharmacological (including lifestyle interventions and various device-based therapies) and pharmacological management. Based on the recommended guidelines, ACEI inhibitors, Angiotensin Receptor Blockers (ARBs), calcium channel blockers, and thiazide or thiazide-like diuretics are usually selected as the first-line agents, and β-blockers as first-line therapy in patients with severe comorbidities.6,7 Despite the well-established treatment options for hypertension, the actual awareness, treatment, and control rates of hypertension are disappointingly low, necessitating urgent improvements in patient screening, diagnosis, treatment, and follow-up.8 Hence, it becomes even more essential to consider that patient values and treatment preferences positively impact the management and treatment of hypertension.
In the medical process, patient preferences and values are increasingly considered critical components of evidence-based medicine. Simultaneously, when making decisions, the patient’s voice should be fully considered.9 Although the skillful application of guidelines can help clinicians make easier, faster, and better decisions about the diagnosis and treatment of disease, guidelines cannot replace clinicians’ compassionate and mindful engagement with the patients in shared decision-making when patient preferences and values are important.10 Due to differences in patients’ backgrounds, goals, and values, it is difficult for clinicians to effectively understand each patient’s preferences. Clinicians’ diagnosis and treatment conceptions may be inconsistent with patients’ preferences and values. Investigating the preferences, expectations, and values of hypertensive patients helps manage and treat hypertension. In this study, a systematic literature review was conducted to comprehensively summarize the evidence.
Methods
Eligibility Criteria
The study included systematic literature searches meeting the following criteria: 1) The study population was adult patients with hypertension, including patients with normal hypertension and resistant hypertension; 2) The research content was associated with the patient preferences, expectations, and values for the management and treatment of hypertension; 3) To study the decision-making of hypertensive patients to receive hypertension treatment and the factors that influence the patient’s choice. The exclusion criteria were as follows: 1) Not related to hypertension or patient preferences, expectations, and values; 2) Letters, reviews, case reports, and posters.
Data Sources and Search Strategy
From their inception to January 2022, five electronic databases were systematically searched (PubMed, Embase, Web of Science, EBSCO, and China National Knowledge Infrastructure). Key phrases included “hypertension”, “high blood pressure”, or “blood pressure” in combination with “preferences”, “expectations”, or “values”. We searched the PubMed database for MeSH terms as well as all relevant search terms to find potential articles that used the terms “hypertension” in combination with “patient preference”. Table 1 represents the search strategy for PubMed, and Figure 1 depicts the specific systematic literature screening process.
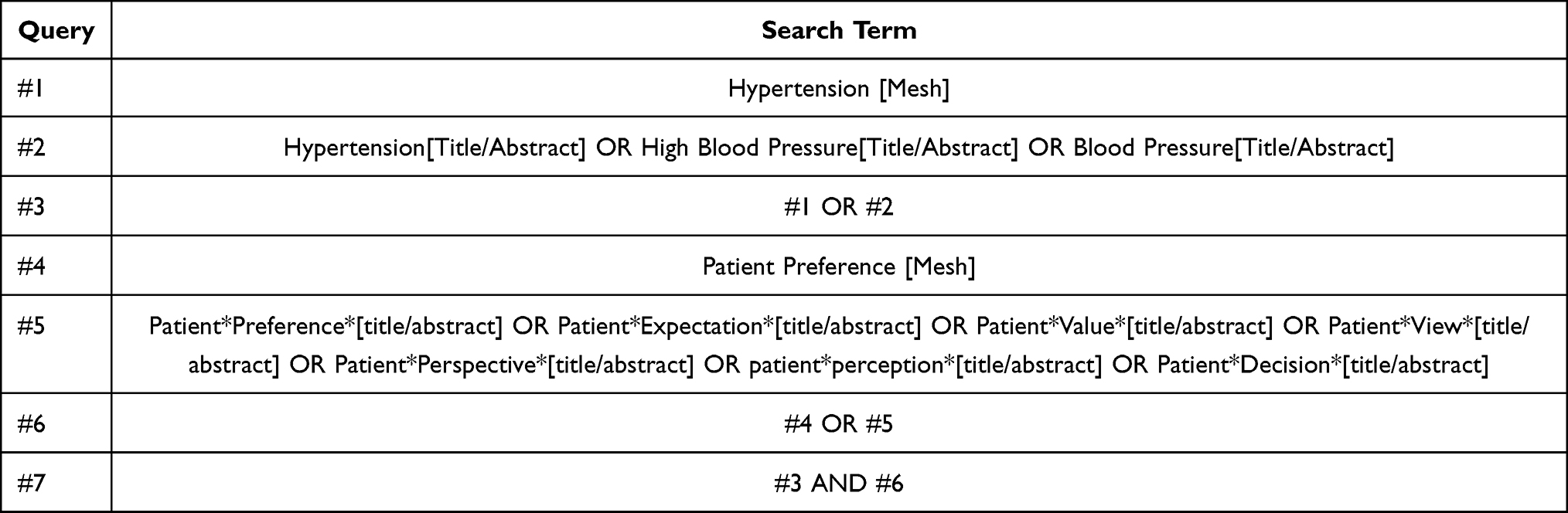 |
Table 1 Search Strategy for PubMed |
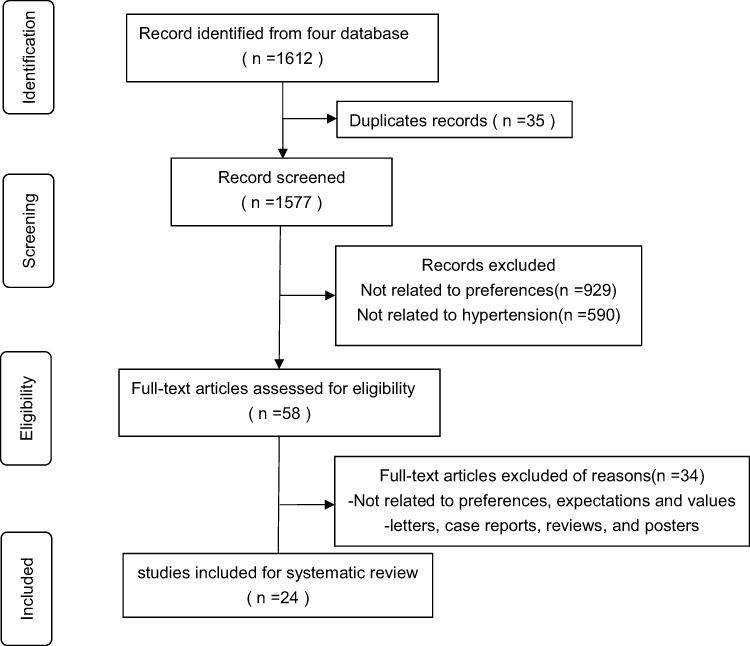 |
Figure 1 Flow diagram of the selection process. |
Data Extraction and Quality Assessment
Two reviewers independently conducted the literature screening and information extraction, and any discrepancies were resolved through discussion. Data on the first author, date of publication, sample size, study design, study description, results, and demographics were extracted by the reviewers.
The quality of the literature was independently assessed by two independent reviewers using instruments recommended by the Agency for Healthcare Research and Quality (AHRQ),11 and the disagreement was resolved through a third-party discussion. The AHRQ checklist is a commonly used tool for evaluating observational studies, consisting of 11 items that are answered with “yes” (scored 1), “no” (scored 0),) and “unclear” (scored 0). The quality was classified into three levels: low quality = 0–3; moderate quality = 4–7; high quality = 8–11.
Results
Characteristics of Included Studies
A total of 1612 articles were obtained with electronic search, of which 58 full-text studies were selected after the screening of the title and abstract. The full text of the remaining 58 articles was then screened, and finally, 24 articles meeting the inclusion criteria were selected (Figure 1). Most studies on patient preferences in patients with hypertension were conducted in patients from American (n = 7), Europe (n = 6), Asia (n = 5), Africa (n = 3), and Canada (n = 3). Table 2 provides an overview of the research, including the date of the study, sample size, study design, study description, preferences, and methodological quality.
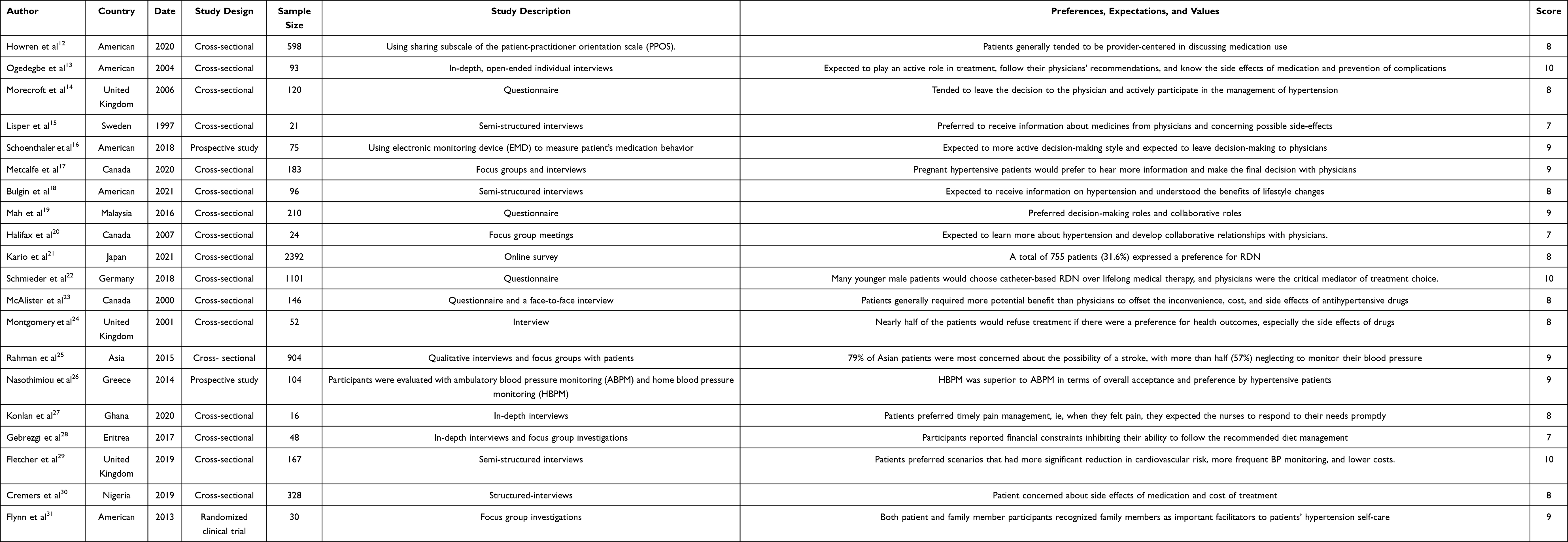 |
Table 2 Characteristics of Included Studies and Summary of Results |
The Preferences and Expectations for Decision-Making
The preferences and expectations for decision-making were reported in nine studies. Most patients knowing they had hypertension, anticipated an essential role in their treatment. They expected their physicians to develop a patient-centric model of shared decision-making. At the same time, because most patients lacked pertinent knowledge on hypertension, they anticipated learning more about it from doctors during the diagnostic and treatment processes, including treatment courses, side effects of medication and complications, etc. Patients usually let doctors make the final call in the end.
Howren et al examined patient preference data from a randomized clinical trial designed to test the efficacy of a patient activation intervention in encouraging the prescribing of thiazides to uncontrolled hypertensive patients. They found that those who were provider-centric in the most intensive intervention sectors started discussing thiazides more than others.12 According to a different study,13 patients expected their physicians to educate them about hypertension treatments and the medications that would decrease their blood pressure and protect them from heart attacks, strokes, and kidney failure. In this study, 27% of patients to anticipated actively participating in their treatment, and 57% expected to be aware of the benefits, risks, and potential problems of their blood pressure medications. According to Morecroft et al,14 patients needed to believe that their general practitioner was in charge of their treatment and that decision-making on what blood pressure level is considered appropriate should be left to them. Lisper et al15 revealed that the patients preferred to get information about their medications from their physicians, and they reported a desire to do so before starting their pharmaceutical regimen, particularly about potential adverse effects. As per Schoenthaler et al,16 over two-thirds of patients (57.3%) preferred to participate in shared decision-making (SDM) during the clinic visit, which involved making a choice together and considering the doctor’s advice. In another study,17 most of the pregnant hypertensive patients said they would prefer information about pregnancy hypertension from their physicians (79%), and nearly 82% wanted this information when they were at risk for pregnancy hypertension before they experienced hypertension. According to Bulgin et al,18 patients were expected to learn about hypertension and comprehend the advantages of making lifestyle adjustments. According to the research by Mah et al,19 51.4% of patients chose a collaborative role with a doctor, 44.8% preferred a passive role, and only 1.9% preferred an active role. In preferred decision-making roles. In another study,20 patients stated that they lacked a working knowledge of the most fundamental terms related to hypertension and the health effects of high or low blood pressure. However, they acknowledged that they were responsible for their health, made responsible choices, and developed physician partnerships.
The Preferences and Expectations for Management and Treatment
The preferences and expectations for management and treatment were reported in ten studies. In terms of management and treatment, regimens that that decrease the incidence of comorbidities, respond quicker, are less expensive, monitor blood pressure more frequently, have fewer side effects, and make medication more convenient are preferred, with side effects being a consideration for the vast majority of patients.
In a countrywide survey of Japanese patients, the Kario et al 2022 study looked into patients’ preferences for renal denervation.21 The study discovered that nearly one-third of the patients preferred RDN, among which patients with resistant hypertension, poor adherence to antihypertensive medications, younger patients, and patients with side effects during antihypertensive treatment were more likely to prefer RDN.21 A similar study conducted in Germany22 revealed that RDN was favored by 38.2% of individuals who were not already taking medicine and by 28.2% of those who were. Patients’ preferences were found to be influenced by antihypertensive effects, the experience of side effects, and medication adherence. The study by McAlister et al showed that patients generally needed greater potential benefits than physicians to make up for the difficulty, expense, and side effects of antihypertensive medications.23 The study by Montgomery et al found that among patients with a 5-year absolute risk of >10% and those with systolic blood pressure greater than 160 mmHg, nearly half would avoid treatment if the patient’s preference for health outcomes, particularly drug side effects and complications, was taken into consideration.24 In the study by Rahman et al, 79% of Asian patients were concerned about the possibility of a stroke, with more than half (57%) neglecting monitoring their blood pressure.25 AAs per the study by Nasothimiou et al,26 which compared the patients’ preferences for ambulatory blood pressure monitoring and home blood pressure monitoring, discovered that HBPM significantly performed better than ABPM in terms of overall patient acceptance and preference, with broad availability, lower cost, and higher patient acceptance, and should be the process of choice for out-of-office blood pressure assessment in most patients in clinical practice. A 2020 in-depth interview by Konlan et al stated that when patients were enquired about their expectations for care prior to admission, patients reported that they expected nurses to be very responsive to their needs and should proactively meet those needs, to treat pain as an emergency, and comfort them when they are in pain.27
A study by Gebrezgi et al found that a patient’s economic status can affect the management of hypertension in different ways. Eritrea provides antihypertensive medications free of charge, and economic status does not appear to affect patients’ adherence to antihypertensive medications. However, financial status affects patients’ adherence to lifestyle changes, such as dietary management and purchasing blood pressure management devices.28 The study by Fletcher et al29 in the UK found that patients preferred options with a greater reduction in cardiovascular risk, more frequent blood pressure monitoring, and lower cost, revealing that cost is an important factor influencing patient preference even in developed countries. A mixed methods research found that half of the patients face financial constraints and sometimes difficulties in purchasing medicines, with the economic downturn significantly impacting patients’ ability to afford medicines.30
Additional Perspectives on Patients’ Preferences
Flynn et al compared urban African American patients and family members’ perceptions of facilitators and barriers to hypertension self-management and found that both patient and family member participants believed family members were essential facilitators of patients’ hypertension self-care factors.31 The study by Gibson et al32 showed that there are significant information gaps in the short-term and long-term benefits of hypertensive medication usage in hypertensive patients. However, the most important advantage of these drugs was a reduction in the risk of long-term complications due to improved disease control; nonetheless, these benefits were mentioned by less than half of patients with hypertension.32 The majority of the participants believed that strengthening lifestyle changes would enable them to stop the medication, avoid additional medication, or cure their hypertension. These participants were quite optimistic about their ability to improve their lifestyle, attributing their expectations to scientific progress, good social and medical support, and stress relief.33 In another study, from the patient’s point of view, patients generally did not perceive high blood pressure as a chronic disease requiring adherence to treatment recommendations but rather as a primarily stress-related health condition with no consequences if left untreated.34 In a study by Nishigaki et al,35 33.5% of patients reported no changes in their diet or exercise regimen since diagnosis, 29.1% believed that hypertension could be treated casually, and 10–15% believed that there is no need to take antihypertensive medications or inform their physicians when they are asymptomatic or have stable blood pressure.
Discussion
This systematic literature review involving 24 publications summarizes the preferences, values, and expectations of hypertensive patients in managing and treating hypertension. Both patients and physicians should focus on patient preferences, values, and expectations because they can help determine the trade-offs between the benefits and harms associated with various treatment options, allowing the patient to select the optimal treatment regimen at a particular level.36 Controlling blood pressure levels is the primary objective of hypertension management and treatment. In the absence of novel antihypertensive medications, it is critical that healthcare providers focus on how to use the medications better.37 Patient refusal and non-adherence to treatment for hypertension appear to be a common phenomenon, indicating conscious choices made by patients based on their knowledge and perceptions of their medical condition and its treatment.
People’s understanding of health and disease is limited to their bodies or personal experiences; thus, during their visits, patients seek as much information on hypertension as possible from healthcare professionals. In a study, most of the patients looked to healthcare professionals as sources of information on hypertension, expecting them to inform about the side effects of antihypertensive medications and their mechanisms of action and learn about the physiology of antihypertensive medications and the prevention of complications.13 In clinical exposure reports, patients with shared decision-making were more likely to have positive health outcomes, such as improved self-reported health status, self-management behaviors, emotional well-being, fewer referrals for diagnostic tests, nursing satisfaction, adherence to treatment plans, less invasive treatment options, and shorter hospital stays.16 SDM is a patient-centered care model in which patient-provider information on available options is shared, preferences and goals for the possible outcomes of a decision are expressed, and physicians and patients collaborate in making the final decision, discussing various treatment options to meet patient priorities and health care needs.38,39 The patient-centered decision-making model did not completely transform the passive position of the patient in decision-making, suggesting that even with sufficient information about hypertension, the patient may consider the provider’s recommendations while participating in shared decision-making.16 A study found that patients’ preference for shared decision-making was significantly related to their age and education level, with younger and more educated patients preferring SDM.19
Furthermore, the findings of this study suggest that patients’ preferences and expectations for the management and treatment of hypertension are diverse, and different patient groups have different preferences for treatment options. Patients usually prefer treatment options with fewer comorbidities, faster responses, lower costs, more frequent blood pressure monitoring, fewer side effects, and easier medication administration. Age and gender differences are crucial for hypertension management and treatment preferences, and there are significant age and gender differences in the acceptance of management and treatment methods.21,23 After decades of development, despite its clinical efficacy data have been mixed, renal denervation (RDN) has emerged as a potential emerging treatment modality, with catheter-based RDN being one of the important options for patients with resistant hypertension.40–42 In a study where approximately one-third of the patients surveyed expressed a preference for RDN, younger patients were more likely to prefer RDN than older patients, and patients who experienced side effects during antihypertensive treatment were more likely to prefer RDN.21 A project evaluating the use of RDN as a treatment option in hypertensive patients in Germany revealed that younger men are more likely to receive RDN, which may be related to the fact that men are more likely to take risks than women, and younger individuals are more likely to take risks than older.
Moreover, a significant issue is that many patients usually do not believe that high blood pressure is a chronic disease that requires adherence to treatment recommendations. On the contrary, they believe that improving lifestyles such as diet and exercise can avoid taking antihypertensive drugs or even cure the disease. How to change the concept of these patients and improve their understanding of the risk of hypertension is also a significant issue for medical personnel.33–35
Limitations
This qualitative review analysis has some limitations. First, only a few studies fully met the inclusion criteria for this review. Some studies met the inclusion criteria for this review but did not provide sufficient detail regarding patient preferences, expectations, and values, which may have influenced our analysis. Second, there is currently a lack of standardized reporting and evidence for determining patient preferences for the definitions of preferences, expectations, and values. Systematic literature review approaches to summarizing the evidence are tentative and empirical, therefore, outcomes may be variable.
Conclusions
In summary, the present systematic review demonstrated that side effects, cost, and convenience are major factors for patients when selecting a treatment regimen for hypertension. For hypertension treatment decisions, patients often obtain hypertension information from their physicians and prefer shared patient-centered decision-making.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. McManus RJ, Little P, Stuart B, et al. Home and online management and evaluation of blood pressure (HOME BP) using a digital intervention in poorly controlled hypertension: randomised controlled trial. BMJ. 2021;372. doi:10.1136/bmj.m4858
2. Qamar A, Braunwald E. Treatment of hypertension: addressing a global health problem. JAMA. 2018;320(17):1751–1752. doi:10.1001/jama.2018.16579
3. Brunström M, Carlberg B. Association of blood pressure lowering with mortality and cardiovascular disease across blood pressure levels: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(1):28–36. doi:10.1001/jamainternmed.2017.6015
4. Mancia G, Rea F, Corrao G, Grassi G. Two-drug combinations as first-step antihypertensive treatment. Circ Res. 2019;124(7):1113–1123. doi:10.1161/CIRCRESAHA.118.313294
5. Musinguzi G, Anthierens S, Nuwaha F, Van Geertruyden JP, Wanyenze RK, Bastiaens H. Factors influencing compliance and health seeking behaviour for hypertension in Mukono and Buikwe in Uganda: a qualitative study. Int J Hypertens. 2018;2018:8307591. doi:10.1155/2018/8307591
6. Williams B, Mancia G, Spiering W, et al. 2018 practice guidelines for the management of arterial hypertension of the European society of cardiology and the European society of hypertension ESC/ESH task force for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. doi:10.1093/eurheartj/ehy339
7. Whelton PK, Carey RM, Aronow WS, et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017;2018(71):e127–e248.
8. Brouwers S, Sudano I, Kokubo Y, Sulaica EM. Arterial hypertension. Lancet. 2021;398(10296):249–261. doi:10.1016/S0140-6736(21)00221-X
9. Swift JK, Mullins RH, Penix EA, Roth KL, Trusty WT. The importance of listening to patient preferences when making mental health care decisions. World Psychiatry. 2021;20(3):316–317. doi:10.1002/wps.20912
10. Montori VM, Brito JP, Murad MH. The optimal practice of evidence-based medicine: incorporating patient preferences in practice guidelines. JAMA. 2013;310(23):2503–2504. doi:10.1001/jama.2013.281422
11. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-2
12. Howren MB, Vander Weg MW, Christensen AJ, Kaboli PJ. Association of patient preferences on medication discussion in hypertension: results from a randomized clinical trial. Soc Sci Med. 2020;262:113244. doi:10.1016/j.socscimed.2020.113244
13. Ogedegbe G, Mancuso CA, Allegrante JP. Expectations of blood pressure management in hypertensive African-American patients: a qualitative study. J Natl Med Assoc. 2004;96(4):442–449.
14. Morecroft C, Cantrill J, Tully MP. Individual patient’s preferences for hypertension management: a Q-methodological approach. Patient Educ Couns. 2006;61(3):354–362. doi:10.1016/j.pec.2005.04.011
15. Lisper L, Isacson D, Sjödén PO, Bingefors K. Medicated hypertensive patients views and experience of information and communication concerning antihypertensive drugs. Patient Educ Couns. 1997;32(3):147–155. doi:10.1016/s0738-3991(97)00033-5
16. Schoenthaler A, Rosenthal DM, Butler M, Jacobowitz L. Medication adherence improvement similar for shared decision-making preference or longer patient-provider relationship. J Am Board Fam Med. 2018;31(5):752–760. doi:10.3122/jabfm.2018.05.180009
17. Metcalfe RK, Harrison M, Hutfield A, et al. Patient preferences and decisional needs when choosing a treatment approach for pregnancy hypertension: a stated preference study. Can J Cardiol. 2020;36(5):775–779. doi:10.1016/j.cjca.2020.02.090
18. Bulgin D, Biola HR, Whitney CA, et al. Patient expectations and preferences for community-based hypertension classes with implications for action. Worldviews Evid Based Nurs. 2022;19(1):42–46. doi:10.1111/wvn.12550
19. Mah HC, Muthupalaniappen L, Chong WW. Perceived involvement and preferences in shared decision-making among patients with hypertension. Fam Pract. 2016;33(3):296–301. doi:10.1093/fampra/cmw012
20. Halifax NV, Cafazzo JA, Irvine MJ, et al. Telemanagement of hypertension: a qualitative assessment of patient and physician preferences. Can J Cardiol. 2007;23(7):591–594. doi:10.1016/s0828-282x(07)70807-3
21. Kario K, Kagitani H, Hayashi S, Hanamura S, Ozawa K, Kanegae H. A Japan nationwide web-based survey of patient preference for renal denervation for hypertension treatment. Hypertens Res. 2022;45(2):232–240. doi:10.1038/s41440-021-00760-9
22. Schmieder RE, Högerl K, Jung S, Bramlage P, Veelken R, Ott C. Patient preference for therapies in hypertension: a cross-sectional survey of German patients. Clin Res Cardiol. 2019;108(12):1331–1342. doi:10.1007/s00392-019-01468-0
23. McAlister FA, O’Connor AM, Wells G, Grover SA, Laupacis A. When should hypertension be treated? The different perspectives of Canadian family physicians and patients. CMAJ. 2000;163(4):403–408.
24. Montgomery AA, Harding J, Fahey T. Shared decision making in hypertension: the impact of patient preferences on treatment choice. Fam Pract. 2001;18(3):309–313. doi:10.1093/fampra/18.3.309
25. Rahman AR, Wang JG, Kwong GM, et al. Perception of hypertension management by patients and doctors in Asia: potential to improve blood pressure control. Asia Pac Fam Med. 2015;14(1):2. doi:10.1186/s12930-015-0018-3
26. Nasothimiou EG, Karpettas N, Dafni MG, Stergiou GS. Patients’ preference for ambulatory versus home blood pressure monitoring. J Hum Hypertens. 2014;28(4):224–229. doi:10.1038/jhh.2013.104
27. Konlan KD, Armah-Mensah M, Aryee R, Appiah TA. Expectation and satisfaction with nursing care among hypertensives receiving care at a resource-constrained hospital in Ghana. Nurs Res Pract. 2020;2020:6094712. doi:10.1155/2020/6094712
28. Gebrezgi MT, Trepka MJ, Kidane EA. Barriers to and facilitators of hypertension management in Asmara, Eritrea: patients’ perspectives. J Health Popul Nutr. 2017;36(1):11. doi:10.1186/s41043-017-0090-4
29. Fletcher B, Hinton L, McManus R, Rivero-Arias O. Patient preferences for management of high blood pressure in the UK: a discrete choice experiment. Br J Gen Pract. 2019;69(686):e629–e637. doi:10.3399/bjgp19X705101
30. Cremers AL, Alege A, Nelissen HE, et al. Patients’ and healthcare providers’ perceptions and practices regarding hypertension, pharmacy-based care, and mHealth in Lagos, Nigeria: a mixed methods study. J Hypertens. 2019;37(2):389–397. doi:10.1097/HJH.0000000000001877
31. Flynn SJ, Ameling JM, Hill-Briggs F, et al. Facilitators and barriers to hypertension self-management in urban African Americans: perspectives of patients and family members. Patient Prefer Adherence. 2013;7:741–749. doi:10.2147/PPA.S46517
32. Gibson DS, Nathan AG, Quinn MT, Laiteerapong N. Patient expectations of hypertension and diabetes medication: excessive focus on short-term benefits. SAGE Open Med. 2018;6:2050312118821119. doi:10.1177/2050312118821119
33. Fairchild PC, Nathan AG, Quinn M, Huang ES, Laiteerapong N. Patients’ future expectations for diabetes and hypertension treatments: ”Through the Diet… I Think This is Going to Go Away”. J Gen Intern Med. 2017;32(1):49–55. doi:10.1007/s11606-016-3871-3
34. Anthony H, Valinsky L, Inbar Z, Gabriel C, Varda S. Perceptions of hypertension treatment among patients with and without diabetes. BMC Fam Pract. 2012;13:24. doi:10.1186/1471-2296-13-24
35. Nishigaki N, Shimasaki Y, Yoshida T, Hasebe N. Physician and patient perspectives on hypertension management and factors associated with lifestyle modifications in Japan: results from an online survey. Hypertens Res. 2020;43(5):450–462. doi:10.1038/s41440-020-0398-0
36. Herzog TJ, Armstrong DK, Brady MF, et al. Ovarian cancer clinical trial endpoints: society of gynecologic oncology white paper. Gynecol Oncol. 2014;132(1):8–17. doi:10.1016/j.ygyno.2013.11.008
37. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
38. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
39. Murray E, Pollack L, White M, Lo B. Clinical decision-making: patients’ preferences and experiences. Patient Educ Couns. 2007;65(2):189–196. doi:10.1016/j.pec.2006.07.007
40. Bhatt DL, Kandzari DE, O’Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393–1401. doi:10.1056/NEJMoa1402670
41. Esler MD, Krum H; Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376(9756):1903–1909. doi:10.1016/S0140-6736(10)62039-9
42. Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275–1281. doi:10.1016/S0140-6736(09)60566-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient Preference Studies for Advanced Prostate Cancer Treatment Along the Medical Product Life Cycle: Systematic Literature Review
Menges D, Piatti MC, Cerny T, Puhan MA
Patient Preference and Adherence 2022, 16:1539-1557
Published Date: 28 June 2022
Preferences and Adherence of People with Prediabetes for Disease Management and Treatment: A Systematic Review
Ren Z, Xu X, Yue R
Patient Preference and Adherence 2023, 17:2981-2989
Published Date: 15 November 2023
A Systematic Review of Patient Preferences, Expectations, and Values for the Management and Treatment of Graves Disease
Chen Y, Ren Z, Zhou X, Gao P
Patient Preference and Adherence 2025, 19:2949-2957
Published Date: 19 September 2025