Back to Journals » Journal of Pain Research » Volume 14
A Systematic Review and Meta-Analysis of Randomized Controlled Trials of Labor Epidural Analgesia Using Moderately High Concentrations of Plain Local Anesthetics versus Low Concentrations of Local Anesthetics with Opioids
Authors Zhang L ![]() , Hu Y
, Hu Y ![]() , Wu X, Paglia MJ, Zhang X
, Wu X, Paglia MJ, Zhang X ![]()
Received 8 February 2021
Accepted for publication 19 April 2021
Published 21 May 2021 Volume 2021:14 Pages 1303—1313
DOI https://doi.org/10.2147/JPR.S305838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Li Zhang,1,* Yirui Hu,2,* Xianren Wu,1 Michael J Paglia,3 Xiaopeng Zhang1
1Department of Anesthesiology, Geisinger Medical Center, Danville, PA, USA; 2Population Health Sciences, Geisinger Medical Center, Danville, PA, USA; 3Department of Obstetrics and Gynecology, Geisinger Medical Center, Danville, PA, USA
*These authors contributed equally to this work
Correspondence: Li Zhang
Department of Anesthesiology, Geisinger Medical Center, 100 North Academy Avenue, Danville, PA, 17822, USA
Tel +1-570-271-6587
Fax +1-570-271-6762
Email [email protected]
Xiaopeng Zhang
Department of Anesthesiology, Geisinger Medical Center, 100 North Academy Avenue, Danville, PA, 17822, USA
Tel +1-570-2710-6849
Email [email protected]
Purpose: Compared to low concentrations of local anesthetics with opioids for labor epidural analgesia, very high concentrations of local anesthetics are associated with an increased risk of assisted vaginal delivery. We aimed to investigate if moderately high concentrations of plain local anesthetics are also associated with this risk.
Methods: We searched for published randomized controlled trials that compared moderately high concentrations of plain local anesthetics (> 0.1% but ≤ 0.125% bupivacaine, > 0.1% but ≤ 0.125% levobupivacaine, or > 0.17% but ≤ 0.2% ropivacaine) to low concentrations of local anesthetics (≤ 0.1% bupivacaine, ≤ 0.1% levobupivacaine, or ≤ 0.17% ropivacaine) with opioids for labor analgesia. Meta-analyses were performed to compare the risk of assisted vaginal delivery and other perinatal outcomes between these two groups.
Results: We identified nine randomized controlled trials with a total of 1334 participants. Meta-analysis of these nine trials showed no differences in the risks of assisted vaginal delivery (odds ratio [OR] = 1.18; 95% confidence interval [CI], 0.93– 1.49) or Cesarean delivery (OR = 0.96; 95% CI, 0.71– 1.29) between the two groups. The incidence of motor block was higher in the group of moderately high concentrations (OR = 4.05; 95% CI, 2.19– 7.48), while the incidence of pruritus was lower (OR = 0.07; 95% CI, 0.03– 0.16).
Conclusion: This systematic review and meta-analysis suggests that the current evidence is inadequate to support that moderately high concentrations of plain local anesthetics increase the risk of assisted vaginal delivery compared to low concentrations of local anesthetics with opioids.
Keywords: assisted vaginal delivery, epidural, labor analgesia, local anesthetics, meta-analysis
Introduction
Neuraxial techniques are the most effective methods for providing intrapartum pain relief. A combination of low concentrations of local anesthetics with opioids is currently the standard for labor epidural analgesia.1 Compared with high concentrations of local anesthetics, low concentrations of local anesthetics combined with opioids are believed to reduce the incidence of assisted vaginal delivery while providing adequate labor analgesia.
Current definition of low concentrations of local anesthetics for labor epidural analgesia is ≤0.1% bupivacaine, ≤0.1% levobupivacaine, or ≤ 0.17% ropivacaine.2,3 The most recent meta-analysis compared low concentrations versus high concentrations of local anesthetics (> 0.1% bupivacaine or > 0.17% ropivacaine) for labor analgesia and concluded that high concentrations of local anesthetics increase the incidence of assisted vaginal delivery.2 The conclusion from this meta-analysis was based on the comparison of low concentrations of local anesthetics with multiple different high concentrations of local anesthetics. Previous studies suggested that at a very high concentration, ie, > 0.125% bupivacaine, > 0.125% levobupivacaine, or > 0.2% ropivacaine, epidural local anesthetics with or without opioids were associated with an increased risk of assisted vaginal delivery.4,5 However, it is uncertain if current evidence also supports that at moderately high concentrations, ie, > 0.1% but ≤ 0.125% bupivacaine, > 0.1% but ≤0.125% levobupivacaine, or > 0.17% but ≤ 0.2% ropivacaine, plain local anesthetics are also associated with such risk. Some studies suggested that plain local anesthetics at a moderately high concentration did not increase the risk of assisted vaginal delivery and provided adequate labor epidural analgesia similar to the standard mixture of low concentration local anesthetics with opioids.6,7 We carried out a systematic review and meta-analysis to investigate the existing evidence on this question.
Methods
Definitions of Low, Moderately High, and Very High Concentrations of Local Anesthetics
Low concentrations of local anesthetics were defined as ≤0.1% bupivacaine, ≤0.1% levobupivacaine, or ≤0.17% ropivacaine.2,3 The moderately high concentrations of local anesthetics were defined as >0.1% but ≤0.125% bupivacaine, >0.1% but ≤0.125% levobupivacaine, or >0.17% but ≤ 0.2% ropivacaine, ie, within 25% above the upper limit of low concentrations of local anesthetics. The very high concentrations of local anesthetics were defined as >0.125% bupivacaine, >0.125% levobupivacaine, or > 0.2% ropivacaine.
Literature Search Strategies and Data Extraction
This systematic review and meta-analysis were conducted based on criteria of the Preferred Reporting Items for Systemic Reviews and Meta-analysis (PRISMA) statement. The registration number with PROSPERO is CRD42019145888. We systematically searched Ovid Medline, Cochrane CENTRAL, PubMed, CINAHL and Google Scholars for randomized controlled trials (RCTs) that compared moderately high concentrations of plain local anesthetics versus low concentrations of local anesthetics with opioids for maintenance of labor epidural analgesia.
Search terms included epidural analgesia, epidural anesthesia, labor, delivery, obstetrics, bupivacaine, levobupivacaine, ropivacaine, randomized, trial (see Appendix 1 for database search strategy for Ovid Medline). We also manually searched for studies listed in the references of included papers, in case there were potential studies not captured by the database search strategy. There was no limitation on language.
We included original full-text articles that were: (1) RCTs published in peer-reviewed journals from 1946 (the earliest year that publications are searchable in the online databases) to April 2020, (2) compared epidural infusion of moderately high concentrations of plain local anesthetics versus low concentrations of local anesthetics with opioids, (3) assessed outcomes including spontaneous delivery, assisted vaginal delivery (vaginal delivery with the help of forceps or a vacuum device), cesarean delivery, duration of labor, analgesia effect, motor block, nausea, vomiting, maternal hypotension, pruritus, urinary retention, neonatal Apgar scores, and umbilical blood pH. If there were several studies based on the same cohort, the studies with the most recent and relevant results were included.
Study selection was conducted in three screening steps. The first screening of titles was independently reviewed by two reviewers (LZ, XZ) by reviewing the titles identified from the literature search. The second screening of study abstracts that remained from the initial title screening were then reviewed by three reviewers, among whom disagreements were reconciled (LZ, XZ and XW). In the third screening, full-text studies that met the above inclusion criteria were included for final systematic review and meta-analyses. Data were collected and verified from included studies by two reviewers (LZ, XZ) independently.
Characteristics of each study, including study design, patient baseline information, procedural details and above-mentioned outcomes, were extracted into Microsoft-Excel file. Figure 1 summarized the complete process of paper study enrollment according to the PRISMA statement.
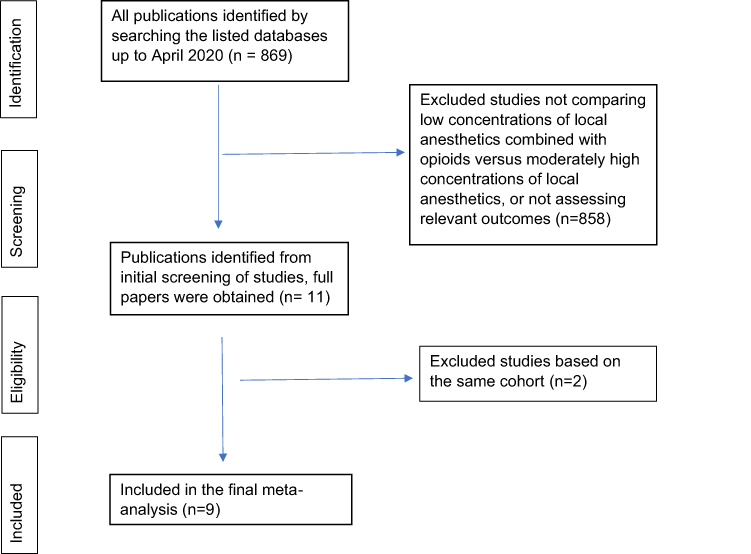 |
Figure 1 Flow chart for literature enrollment from identification to final synthesis according to the PRISMA protocol. Abbreviation: PRISMA, Preferred Reporting Items for Systemic Reviews and Meta-analysis. |
Quality Assessment
The included studies were independently evaluated by two reviewers (LZ, XZ) using the Cochrane risk of bias assessment tool,8,9 which evaluated 6 domains including random sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other sources of bias.
Statistical Analyses
The primary outcome was the incidence of assisted vaginal delivery. Secondary outcomes included (1) obstetric outcomes (incidence of cesarean delivery, incidence of spontaneous vaginal delivery, duration of first stage of labor, duration of second stage of labor); (2) analgesic effect (pain scores); (3) maternal side effects (motor block (no motor block is defined as a Bromage grade = I), pruritus, nausea, vomiting, maternal hypotension, and urinary retention); (4) neonatal outcomes (neonatal Apgar scores < 7 at one and five minutes, and umbilical arterial blood pH).
Random-effects meta-analyses were performed for each included outcome. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for binary outcomes, while mean differences (MDs) and 95% CIs were estimated for continuous outcomes. The pooled OR is considered statistically significant if the 95% CI did not contain 1, and the pooled MD is considered statistically significant if the 95% CI did not contain 0. Each included study’s pooled estimates and measures of variability were used to generate forest plots. If meta-analysis was not possible for an outcome, the data from individual studies were reported qualitatively. Heterogeneity was assessed using the I2 statistic. The I2 statistic was calculated to quantify the proportion of between-study heterogeneity attributable to variability in the association rather than sampling variation. The p value was calculated based on the heterogeneity test (I2), where a high p value (≥≥0.05) indicated that the heterogeneity was insignificant. All analyses were conducted using RStudio (Version 1.0.136; The R Foundation, Vienna, Austria) using the “Meta” and “Metafor” package.
Results
Study Characteristics and Risk of Bias Assessment
The database started with a total of 869 citations. Of these, 858 studies were excluded due to irrelevant topics, assessment of exposure and outcomes not meeting the inclusion criteria. The remaining 11 studies were retrieved in full-text to be examined in more details. Three studies7,10,11 were based on the same cohort and the study with the most recent and relevant results was included,7 resulting in a total of 9 studies included in the systematic review and meta-analysis (Figure 1). Table 1 presents study characteristics of included studies. There are 9 RCTs and a total of 1334 patients included.6,7,12–18 Basal infusion was used for labor epidural analgesia in all but one RCT.18 Sample size ranged from 32 to 587, with median being 80. The risk of bias assessment is shown in Appendix 2.
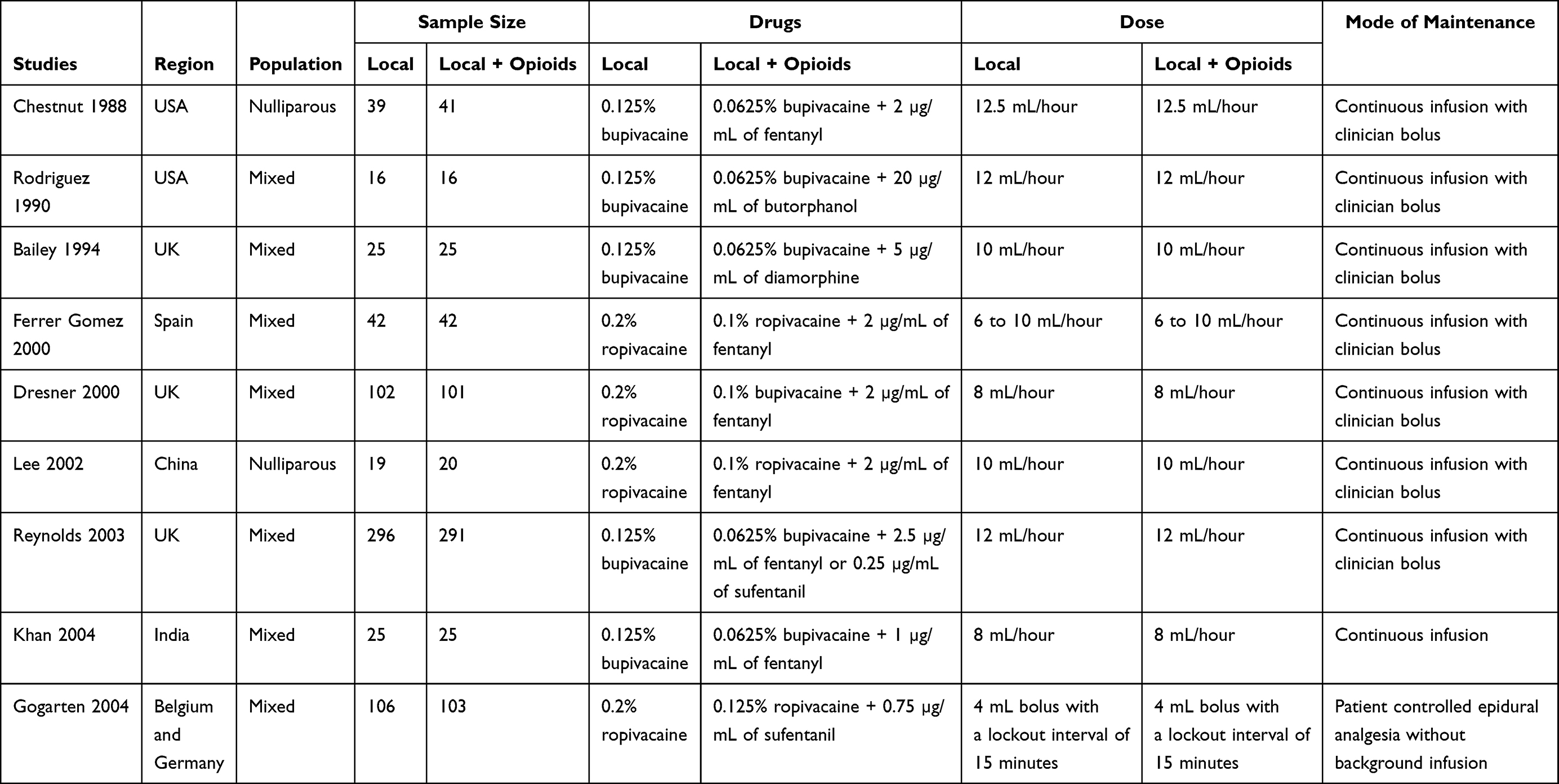 |
Table 1 Baseline Characteristics of Included Clinical Trials |
Meta-Analyses
Mode of Delivery
Nine studies with 1334 participants compared the mode of delivery between the group of moderately high concentrations of plain local anesthetics and the group of low concentrations of local anesthetics with opioids. There were no significant differences in the odds of assisted vaginal delivery (OR = 1.18; 95% CI, 0.93–1.49; I2 = 0%, p = 0.67), Cesarean delivery (OR = 0.96; 95% CI, 0.71–1.29; I2 = 0%, p = 0.78), or spontaneous vaginal delivery (OR = 0.89; 95% CI, 0.71–1.11; I2 = 0%, p = 0.89) (Figure 2).
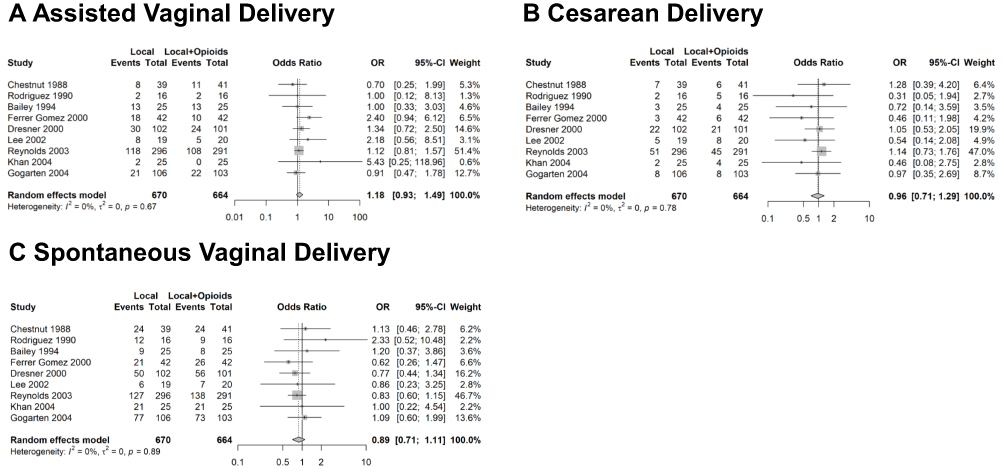 |
Figure 2 Forest plot of odds of assisted vaginal delivery (A), Cesarean delivery (B), and spontaneous vaginal delivery (C). There are no significant differences between the group of moderately high concentrations of plain local anesthetics and the group of low concentrations of local anesthetics with opioids. Abbreviations: OR, odds ratio; CI, confidence interval. |
Duration of Labor
Four studies with 926 participants reported outcomes for the duration of the first stage of labor, and four studies with 389 participants presented outcomes for the duration of the second stage of labor. Meta-analysis indicated that the duration of the first stage of labor was shorter in the group of moderately high concentrations of plain local anesthetics (MD = −32.84 minutes; 95% CI, −63.81 – −1.87 minutes; I2 = 0%, p = 0.54), while the duration of the second stage of labor was not significantly different between two groups (MD = 0.87 minutes; 95% CI, −5.02–6.76 minutes; I2 = 6%, p = 0.36) (Figure 3).
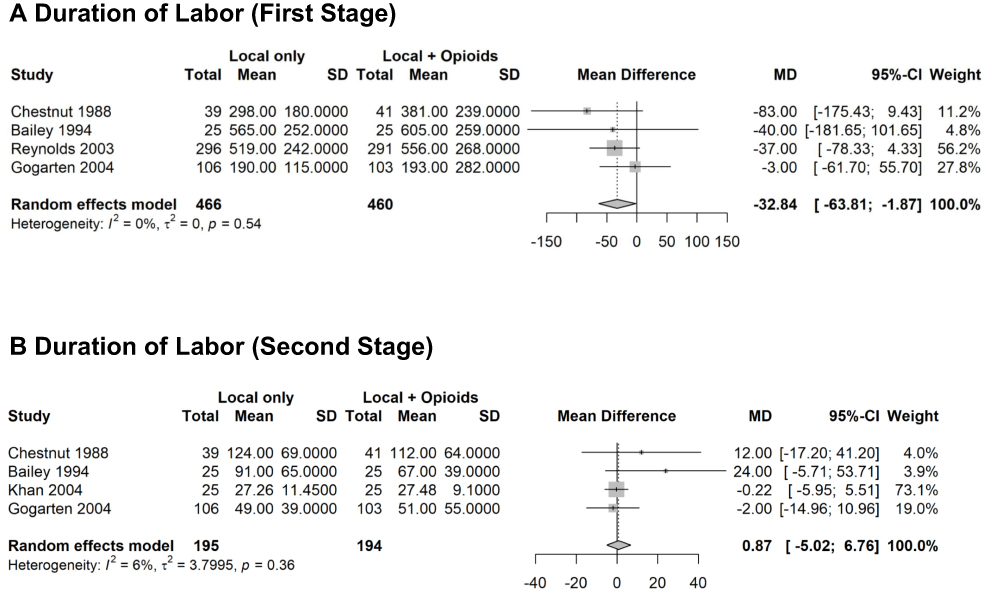 |
Figure 3 Forest plot of duration of first stage (A) and second stage of labor (B). Moderately high concentrations of local anesthetics are associated with a small but significant decrease in the duration of first stage of labor but no significant change in the duration of second stage of labor. Abbreviations: MD, mean difference; CI, confidence interval. |
Analgesic Effect
Eight studies with 747 participants compared pain scores between the two groups (Table 2). A variety of methods were used to report pain scores in those studies, which made it unfeasible to perform a meta-analysis. Among these eight studies, six studies with 613 participants reported no significant difference in pain scores between the two groups. One study with 50 participants17 reported a slightly lower pain score at 30 minutes in the group of moderately high concentration of local anesthetics, while another study14 with 84 participants reported a slightly higher pain score at 15 minutes, 30 minutes, 60 minutes, and 90 minutes in the group of moderately high concentration of local anesthetics. Nevertheless, in both studies, pain scores were not significantly different between the two groups at other times of assessment. Three studies with 315 participants reported pain relief assessed either by patients6,12 or midwives.15 No significant difference in pain relief was found between the two groups.
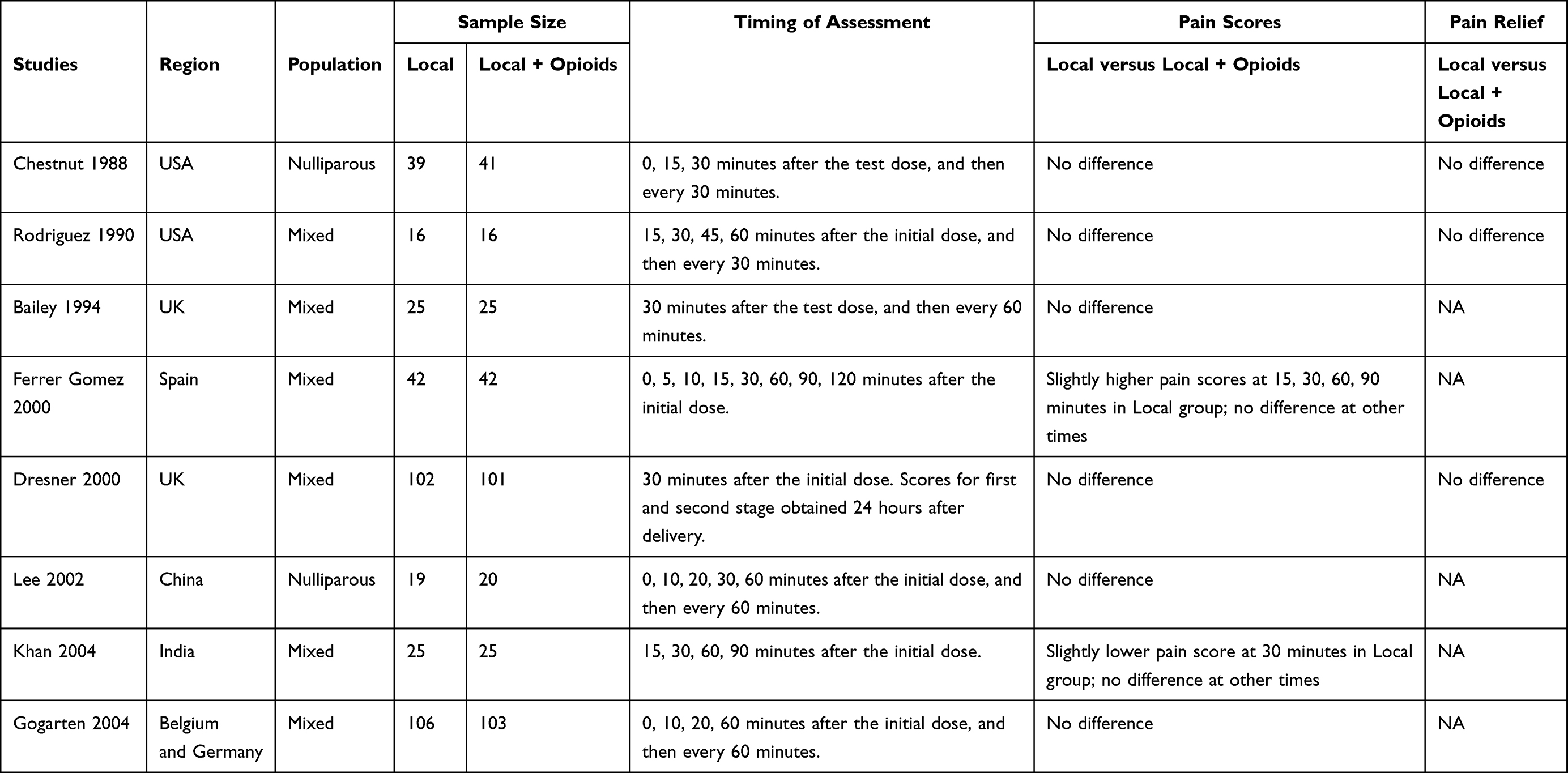 |
Table 2 Maternal Pain Score and Pain Relief |
Maternal Side Effects
Nine studies with 1215 participants presented results for motor block. The group of moderate high concentrations of local anesthetics was associated with higher odds of motor block (OR = 4.05; 95% CI, 2.19–7.48; I2 = 60%, p = 0.01) (Figure 4A). Six studies with 460 participants reported results for pruritus. The group of moderate high concentrations of local anesthetics was associated with lower odds of pruritus (OR = 0.07; 95% CI, 0.03–0.16; I2 = 2%, p = 0.38) (Figure 4B). The odds of nausea (OR = 0.98; 95% CI, 0.59–1.60; I2 = 0%, p = 0.62), vomiting (OR = 1.01; 95% CI, 0.57–1.80; I2 = 0%, p = 0.91), maternal hypotension (OR = 0.74; 95% CI, 0.15–3.70; I2 = 59%, p = 0.06), and urinary retention (OR = 0.94; 95% CI, 0.30–2.90; I2 = 51%, p = 0.13) were not significantly different between the two groups (Figure 4C–F).
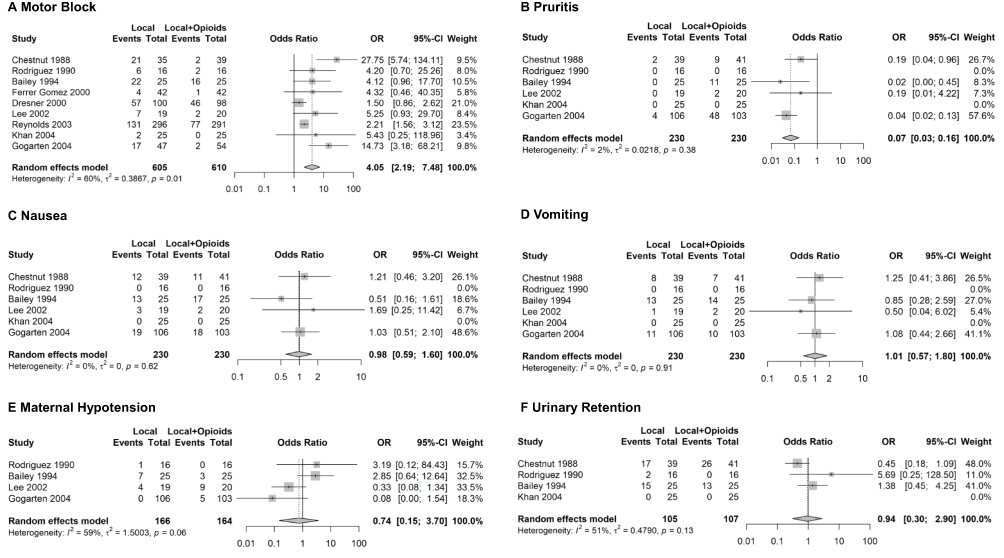 |
Figure 4 Forest plot of maternal side effects including motor block (A), pruritus (B), nausea (C), vomiting (D), maternal hypotension (E) and urinary retention (F). Moderately high concentrations of local anesthetics are associated with increased odds of motor block but decreased odds of pruritus. There are no significant differences in nausea, vomiting, maternal hypotension or urinary retention between the two groups. Abbreviations: OR, odds ratio; CI, confidence interval. |
Neonatal Outcomes
Five studies with 788 participants compared neonatal Apgar scores at one minute and five minutes between the group of moderately high concentrations of plain local anesthetics and the group of low concentrations of local anesthetics with opioids. There were no significant differences in the odds of neonatal Apgar scores < 7 at one minute (OR = 0.93; 95% CI, 0.61–1.41; I2 = 0%, p = 0.88), or five minutes (OR = 2.50; 95% CI, 0.33–18.70; I2 = 20%, p = 0.29) (Figure 5A and B). Three studies with 751 participants compared umbilical arterial blood pH between the two groups. There were no significant differences (MD = - 0.01; 95% CI, - 0.02–0.01; I2 = 45%, p = 0.16) (Figure 5C).
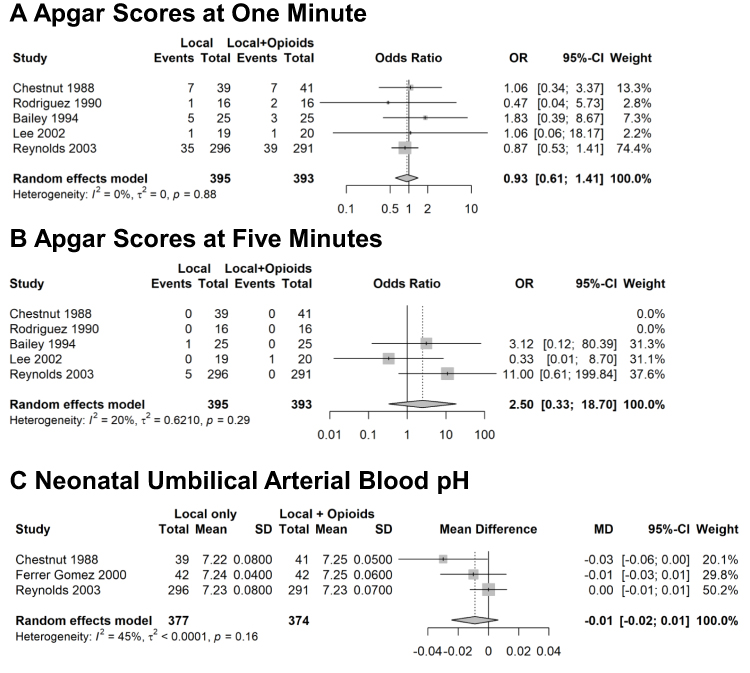 |
Figure 5 Forest plot of neonatal Apgar scores at one minute (A) and five minutes (B), and neonatal umbilical arterial blood pH (C). There are no significant differences in Apgar scores or umbilical arterial blood pH between the two groups. Abbreviations: OR, odds ratio; MD, mean difference; CI, confidence interval. |
Discussion
The combination of low concentrations of local anesthetics with opioids has been commonly used for labor epidural analgesia.1 This combination is widely accepted as the standard mixture partially due to its suggested benefits to decrease the risk of assisted vaginal delivery while providing adequate labor analgesia.2,4 Although previous studies suggested that at a very high concentration, epidural local anesthetics with or without opioids increased the risk of assisted vaginal delivery,4,5 our systemic review and meta-analysis demonstrated that current evidence is inadequate to support the assumption that at moderately high concentrations, plain local anesthetics also increase such risk. Findings from this meta-analysis suggested that, compared to low concentrations of local anesthetics with opioids, moderately high concentrations of plain local anesthetics provided effective labor analgesia without increasing the risk of assisted vaginal delivery. This might not be surprising as none of included trials showed a significant difference in mode of delivery between the two groups.
Our findings are different from those of a previous meta-analysis comparing low concentrations of local anesthetics to high concentrations of local anesthetics for labor analgesia.2 In that meta-analysis, low concentrations of local anesthetics were associated with a decreased risk of assisted vaginal delivery. The definition of low concentrations of local anesthetics in that meta-analysis was the same as ours, ie, ≤ 0.1% bupivacaine or ≤ 0.17% ropivacaine. However, in that meta-analysis, they included both moderately high concentrations of local anesthetics and very high concentrations of local anesthetics in a single group. In this meta-analysis, we separated them and focused only on moderately high concentrations. It is likely that very high concentrations of local anesthetics increase the risk of assisted vaginal delivery, but moderately high concentrations might not.
Our meta-analysis has several limitations. First, due to the limited number of available RCTs, we had to pool all low concentrations of local anesthetics into one group, and did not divide different low concentrations or different local anesthetics into different groups. However, this limitation might not affect our analysis significantly. Moderately high concentrations of plain local anesthetics were compared to very low concentrations of local anesthetics in the majority of the included trials – 0.0625% bupivacaine was used in five trials and 0.1% ropivacaine was used in the other two trials. The increased risk of assisted vaginal delivery was not detected in any of these seven trials. Second, all but one clinical trial included in this meta-analysis used the method of continuous infusion instead of intermittent bolus for epidural analgesia. It is unclear if moderately high concentrations of local anesthetics, when given as intermittent bolus, would increase the risk of assisted vaginal delivery. The only available trial included in this meta-analysis suggested that they did not. However, more trials are needed to clarify this question. Third, we did not compare moderately high concentrations of plain local anesthetics with low concentrations of plain local anesthetics. Although low concentrations of plain local anesthetics might be able to decrease the incidence of assisted vaginal delivery, previous studies suggested that they are unlikely able to provide adequate labor epidural analgesia.19,20 Fourth, all the available studies included in this meta-analysis are old with the most recent one being published in 2004. Maintenance regimens in the included studies likely differ from those employed in contemporary practice. None of the studies except one used patient controlled epidural analgesia (PCEA), which is a standard practice in many institutions currently. In addition, we could not pool the results for pain scores because a variety of methods were used to report pain scores in the included studies. We also did not report on need for physician interventions as such information was absent in most of the included studies. Future studies utilizing contemporary regimens for labor epidural analgesia and reporting pain scores with a standard method will help address this limitation.
One disadvantage of the current standard mixture which includes opioids is the iatrogenic exposure of parturients to opioids. Although such exposure may not increase the risk of opioid addiction, it is associated with opioid-induced side effects such as itching. Furthermore, the opioid epidemic has been getting worse, and the prevalence of opioid abuse or dependence during pregnancy also increased significantly in recent years.21,22 To deal with the worsening opioid epidemic and prevent opioid diversion, many hospitals are implementing more restricted policies on handling opioid-containing medications and wastes. This results in additional financial burdens, time consumption, and potential documentation errors for using epidural cartridges containing opioids. A variety of adjunct agents have been studied to replace opioids for labor epidural analgesia,23–26 however, none of them have been widely accepted by obstetric anesthesiologists or pharmaceutical companies as a replacement for the current standard mixture that contains opioids. This is either due to unclear superiority of those agents over opioids or uncertain profits for producing non-standard epidural mixtures in a large scale. If future trials with larger sample sizes could demonstrate that moderately high concentrations of plain local anesthetic are safe and effective for labor epidural analgesia, one solution might be to remove opioids and use moderately high concentrations of plain local anesthetics for labor epidural analgesia.
Conclusion
In conclusion, this systematic review and meta-analysis suggested current evidence is inadequate to support the assumption that moderately high concentrations of plain local anesthetics increase the risk of assisted vaginal delivery compared to standard mixture of low concentrations of local anesthetics with opioids.
Acknowledgments
The authors thank Joy Zhang for help with Spanish translation.
Disclosure
Li Zhang, Yirui Hu, Xianren Wu, Michael J. Paglia, Xiaopeng Zhang report no conflicts of interest in this work.
References
1. Apfelbaum JL, Hawkins JL, Agarkar Met al. Practice guidelines for obstetric anesthesia: an updated report by the American society of anesthesiologists task force on obstetric anesthesia and the society for obstetric anesthesia and perinatology. Anesthesiology. 2016;124(2):270–300. doi:10.1097/ALN.0000000000000935
2. Sultan P, Murphy C, Halpern S, Carvalho B. The effect of low concentrations versus high concentrations of local anesthetics for labour analgesia on obstetric and anesthetic outcomes: a meta-analysis. Can J Anaesth. 2013;60(9):840–854. doi:10.1007/s12630-013-9981-z
3. Wang TT, Sun S, Huang SQ. Effects of epidural labor analgesia with low concentrations of local anesthetics on obstetric outcomes: a systematic review and meta-analysis of randomized controlled trials. Anesth Analg. 2017;124(5):1571–1580. doi:10.1213/ANE.0000000000001709
4. Comparative Obstetric Mobile Epidural Trial Study Group, UK. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial. Lancet. 2001;358(9275):19–23. doi:10.1016/S0140-6736(00)05251-X
5. James KS, McGrady E, Quasim I, Patrick A. Comparison of epidural bolus administration of 0.25% bupivacaine and 0.1% bupivacaine with 0.0002% fentanyl for analgesia during labour. Br J Anaesth. 1998;81(4):507–510. doi:10.1093/bja/81.4.507
6. Chestnut DH, Owen CL, Bates JN, Ostman LG, Choi WW, Geiger MW. Continuous infusion epidural analgesia during labor: a randomized, double-blind comparison of 0.0625% bupivacaine/0.0002% fentanyl versus 0.125% bupivacaine. Anesthesiology. 1988;68(5):754–759. doi:10.1097/00000542-198805000-00013
7. Reynolds F, Russell R, Porter J, Smeeton N. Does the use of low dose bupivacaine/opioid epidural infusion increase the normal delivery rate? Int J Obstet Anesth. 2003;12(3):156–163. doi:10.1016/S0959-289X(03)00008-6
8. Higgins JP, Altman DG, Gotzsche PC, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:5928. doi:10.1136/bmj.d5928
9. Hao Q, Hu Y, Zhang L, et al. A systematic review and meta-analysis of clinical trials of neuraxial, intravenous, and inhalational anesthesia for external cephalic version. Anesth Analg. 2020;131(6):1800–1811. doi:10.1213/ANE.0000000000004795
10. Russell R, Quinlan J, Reynolds F. Motor block during epidural infusions for nulliparous women in labour: a randomized double-blind study of plain bupivacaine and low dose bupivacaine with fentanyl. Int J Obstet Anesth. 1995;4(2):82–88. doi:10.1016/0959-289X(95)82997-O
11. Russell R, Reynolds F. Epidural infusion of low-dose bupivacaine and opioid in labour. does reducing motor block increase the spontaneous delivery rate? Anaesthesia. 1996;51(3):266–273. doi:10.1111/j.1365-2044.1996.tb13645.x
12. Rodriguez J, Abboud TK, Reyes A, et al. Continuous infusion epidural anesthesia during labor: a randomized, double-blind comparison of 0.0625% bupivacaine/0.002% butorphanol and 0.125% bupivacaine. Reg Anesth. 1990;15(6):300–303.
13. Bailey CR, Ruggier R, Findley IL. Diamorphine-bupivacaine mixture compared with plain bupivacaine for analgesia. Br J Anaesth. 1994;72(1):58–61. doi:10.1093/bja/72.1.58
14. Ferrer Gomez C, Saludes Serra J, Tello Galindo I, Gomez Montemayor E, Bella Romera S, Cuenca Pena J. [0.2% ropivacaine vs. 0.1% ropivacaine plus fentanyl in obstetric epidural analgesia]. Rev Esp Anestesiol Reanim. 2000;47(8):332–336. Spanish.
15. Dresner M, Freeman J, Calow C, Quinn A, Bamber J. Ropivacaine 0.2% versus bupivacaine 0.1% with fentanyl: a double blind comparison for analgesia during labour. Br J Anaesth. 2000;85(6):826–829. doi:10.1093/bja/85.6.826
16. Lee BB, Ngan Kee WD, Lau WM, Wong ASY. Epidural infusions for labor analgesia: a comparison of 0.2% ropivacaine, 0.1% ropivacaine, and 0.1% ropivacaine with fentanyl. Reg Anesth Pain Med. 2002;27(1):31–36. doi:10.1053/rapm.2002.27836
17. Khan MAH, Pillai A, Dave NM, Kamdar BM. Epiudral analgesia during labour-comparison of continuous infusion of 0.125% bupivacaine v/s 0.0625% bupivacaine/0.0001% fentanyl. J Anaesthesiol Clin Pharmacol. 2004;20(3):267–271.
18. Gogarten W, Van de Velde M, Soetens F, et al. A multicentre trial comparing different concentrations of ropivacaine plus sufentanil with bupivacaine plus sufentanil for patient-controlled epidural analgesia in labour. Eur J Anaesthesiol. 2004;21(1):38–45. doi:10.1097/00003643-200401000-00007
19. Polley LS, Columb MO, Naughton NN, Wagner DS, van de Ven CJ, Goralski KH. Relative analgesic potencies of levobupivacaine and ropivacaine for epidural analgesia in labor. Anesthesiology. 2003;99(6):1354–1358. doi:10.1097/00000542-200312000-00017
20. Carvalho B, Hilton G, Wen L, Weiniger CF. Prospective longitudinal cohort questionnaire assessment of labouring women’s preference both pre- and post-delivery for either reduced pain intensity for a longer duration or greater pain intensity for a shorter duration. Br J Anaesth. 2014;113(3):468–473. doi:10.1093/bja/aeu149
21. Maeda A, Bateman BT, Clancy CR, Creanga AA, Leffert LR. Opioid abuse and dependence during pregnancy: temporal trends and obstetrical outcomes. Anesthesiology. 2014;121(6):1158–1165. doi:10.1097/ALN.0000000000000472
22. Committee opinion no. 711 summary: opioid use and opioid use disorder in pregnancy. Obstet Gynecol. 2017;130(2):488–489. doi:10.1097/AOG.0000000000002229
23. Boogmans T, Vertommen J, Valkenborgh T, Devroe S, Roofthooft E, Van de Velde M. Epidural neostigmine and clonidine improves the quality of combined spinal epidural analgesia in labour: a randomised, double-blind controlled trial. Eur J Anaesthesiol. 2014;31(4):190–196. doi:10.1097/EJA.0b013e32836249e9
24. Booth JL, Ross VH, Nelson KE, Harris L, Eisenach JC, Pan PH. Epidural neostigmine versus fentanyl to decrease bupivacaine use in patient-controlled epidural analgesia during labor: a randomized, double-blind, controlled study. Anesthesiology. 2017;127(1):50–57. doi:10.1097/ALN.0000000000001669
25. Cheng Q, Bi X, Zhang W, Lu Y, Tian H. Dexmedetomidine versus sufentanil with high- or low-concentration ropivacaine for labor epidural analgesia: a randomized trial. J Obstet Gynaecol Res. 2019;45(11):2193–2201. doi:10.1111/jog.14104
26. Roelants F, Lavand’homme P. Clonidine versus sufentanil as an adjuvant to ropivacaine in patient-controlled epidural labour analgesia: a randomised double-blind trial. Eur J Anaesthesiol. 2015;32(11):805–811. doi:10.1097/EJA.0000000000000347
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.