Back to Journals » Infection and Drug Resistance » Volume 16
A Scoring System Based on Laboratory Parameters and Clinical Features to Predict Unfavorable Treatment Outcomes in Multidrug- and Rifampicin-Resistant Tuberculosis Patients
Authors Yan J, Luo H, Nie Q, Hu S, Yu Q, Wang X
Received 12 November 2022
Accepted for publication 23 December 2022
Published 10 January 2023 Volume 2023:16 Pages 225—237
DOI https://doi.org/10.2147/IDR.S397304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jisong Yan,1 Hong Luo,1 Qi Nie,1 Shengling Hu,2 Qi Yu,2 Xianguang Wang1
1Department of Respiratory and Critical Care Medicine, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, 430023, People’s Republic of China; 2Department of Infectious Diseases, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, 430023, People’s Republic of China
Correspondence: Qi Yu, Department of Infectious Diseases, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, 430023, People’s Republic of China, Email [email protected] Xianguang Wang, Department of Respiratory and Critical Care Medicine, Wuhan Jinyintan Hospital, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, 430023, People’s Republic of China, Email [email protected]
Background: The growth of antibiotic resistance to Mycobacterium TB represents a major barrier to the goal of “Ending the global TB epidemics”. This study aimed to develop and validate a simple clinical scoring system to predict the unfavorable treatment outcomes (UTO) in multidrug- and rifampicin-resistant tuberculosis (MDR/RR-TB) patients.
Methods: A total of 333 MDR/RR-TB patients were recruited retrospectively. The clinical, radiological and laboratory features were gathered and selected by lasso regression. These variables with area under the receiver operating characteristic curve (AUC)> 0.6 were subsequently submitted to multivariate logistic analysis. The binomial logistic model was used for establishing a scoring system based on the nomogram at the training set (N = 241). Then, another independent set was used to validate the scoring system (N = 92).
Results: The new scoring system consists of age (8 points), education level (10 points), bronchiectasis (4 points), red blood cell distribution width-coefficient of variation (RDW-CV) (7 points), international normalized ratio (INR) (7 points), albumin to globulin ratio (AGR) (5 points), and C-reactive protein to prealbumin ratio (CPR) (6 points). The scoring system identifying UTO has a discriminatory power of 0.887 (95% CI=0.835– 0.939) in the training set, and 0.805 (95% CI=0.714– 0.896) in the validation set. In addition, the scoring system is used exclusively to predict the death of MDR/RR-TB and has shown excellent performance in both training and validation sets, with AUC of 0.930 (95% CI=0.872– 0.989) and 0.872 (95% CI=0.778– 0.967), respectively.
Conclusion: This novel scoring system based on seven accessible predictors has exhibited good predictive performance in predicting UTO, especially in predicting death risk.
Keywords: multidrug- and rifampicin-resistant tuberculosis, treatment outcome, laboratory parameters, scoring system
Introduction
Currently, MDR/RR-TB remains a significant challenge in the global TB control process. The growth of antibiotic resistance to Mycobacterium TB also represents a major barrier to the goal of “Ending the global TB epidemics”.1,2 According to the World Health Organization (WHO) Global TB report in 2022, 0.45 million new cases were diagnosed as RR-TB, including 141,953 cases of MDR-TB and 25,038 cases of pre-XDR-TB or XDR-TB. However, only about one-third of patients diagnosed with MDR/RR-TB are admitted to treatment each year. The MDR/RR-TB therapy success rate was about 60%. The global DR-TB epidemic has been exacerbated by poor treatment results and limited access to MDR/RR-TB therapy.
China is one of the nations with a high prevalence of MDR/RR-TB, and the epidemic of MDR/RR-TB is very serious. Although the cumulative number of MDR/RR-TB individuals enrolled in treatment rank first in the world, the average success rate of treatment in China is only 54% due to high costs, prolonged treatment regimens and drug adverse events, far below the WHO’s target of at least 75% recovery rate.3
In recent years, to improve the success rate of treatment, some studies have attempted to identify the poor prognosis of individuals with MDR-TB by constructing predictive models,4–6 but the predictive performance was moderate. In addition to the regional variability of study participants, these clinical studies have not created a quick and user-friendly scoring system for physicians to utilize in clinical settings. Thus, it is essential to design a simple and practical approach for early identifying individuals with poor prognoses in the treatment of MDR/RR-TB.
Based on the situation of MDR/RR-TB treatment success rate and shortcomings in previous studies, our goal in this study was to establish an efficient scoring system to predict the UTO of MDR/RR-TB patients. Considering that some laboratory parameters often available in clinical practice (eg C-reactive protein(CRP), hemoglobin(Hb), albumin(Alb), RDW-CV, AGR, etc.) have proven to be valuable in the prediction of TB activity7 and prognosis8–12 in previous studies. Additionally, the coagulation function in TB is receiving more and more attention.13–15 The interaction between the coagulation system and inflammation is ultimately associated with increased mycobacterium tuberculosis replication.14 In this study, these laboratory parameters potentially relevant to treatment outcomes were the first time incorporated to develop the scoring system. Moreover, we exclusively apply the scoring system to predict death risk in MDR/RR-TB patients.
Materials and Methods
Patients and Study Design
MDR/RR-TB cases with long-course treatment were enrolled retrospectively at the Wuhan Jinyintan Hospital, Tongji Medical College, Huazhong University of Science and Technology (Infectious Disease Hospital). The inclusion criteria were: (1) Mycobacterium tuberculosis culture positive or nucleic acid amplification (NAA) assays (such as PCR and GeneXpert MTB/RIF) positive; (2) rifampin resistance as confirmed by a drug susceptibility testing (DST) or GeneXpert MTB/RIF, includes rifampin-resistant (RR-TB), multidrug-resistant tuberculosis (MDR-TB), and extensively drug‑resistant tuberculosis (XDR-TB). The exclusionary criteria were as follows: (1) patients with MDR-TB who had died before receiving MDR therapy; (2) non-tuberculous mycobacteria infection; (3) Patients receiving short courses of treatment; (4) lost to follow-up or missing information.
According to the treatment recommendations and guidelines for drug-resistant TB,16 drug-resistant TB experts prescribe treatment regimens based on drug sensitivity results, financial situation, and treatment history. These regimens are constructed utilizing a hierarchy of suggested medications, with a minimum number of medications thought to be effective. The duration of the treatment program varies between 18 and 24 months, depending on the clinical outcome and results of follow-up cultures.
All participants were split into training and validation cohorts in a 2:1 ratio using SPSS software (version 20.0; IBM, Chicago, IL, USA). 33.3% of those with MDR/RR-TB are in the validation cohort, while 66.7% are in the training cohort. In the training cohort, a prediction model and scoring system for MDR/RR-TB treatment outcomes were developed. The score system’s predictive capabilities were subsequently confirmed in a validation cohort.
Data Collection
Baseline data of each individual was extracted through the Electronic Medical Record System before treatment began as follows: demographic characteristics (age, gender, education level, etc.), radiological features (bronchiectasis, pulmonary cavity, pleural effusion) and laboratory indexes. Moreover, several ratios, including C-reactive protein to prealbumin ratio (CPR), platelet to lymphocyte ratio (PLR), and albumin to globulin ratio (AGR) were calculated and incorporated in this study. Treatment outcomes of DR-TB patients were obtained at the national electronic case registry.
Definition
Determination of the end-of-treatment outcomes followed WHO classification of outcomes.17 Unfavorable treatment outcomes (UTO) were defined as death and treatment failure. Favorable treatment outcomes (FTO) were defined as being cured or having completed treatment. Other definitions were shown in the Supplementary Materials.
Statistical Analysis
77 variables were enrolled after excluding those with more than 10% lacking values (Supplementary Table 1). The remaining missing values were imputed with the missForest algorithm. Categorical variables were presented as a number with percentages and compared with Chi-square test and Fisher’s exact test. The continuous variables were presented as the mean with standard deviation or median (interquartile range, IQR) and compared with Student’s t-test or Mann–Whitney U-test. The steps to construct the model are as follows: (1) Variables transformation: Continuous variables in the training set were converted into binary variables using the cut-off values found in receiver operating characteristic (ROC) curves. (2) Variables selection: ①To avoid co-linearity and over-fitting, Least Absolute Shrinkage and Selection Operator (LASSO) regression was performed to find optimal variables for constructing the model; ②Optimal variables with an AUC≥0.6 were regarded as candidate variables for the model. (3) Nomogram construction: The candidate variables were submitted to multivariate logistic analysis to develop a prediction model. Then, the prediction model was transformed into a nomogram using the “rms package” of R studio software (version 4.20). (4) Scoring system construction: A scoring system was built according to the regression coefficient of each parameter in the multivariate logistic analysis. The scores of each variable were obtained by the following methods: ①Variables scoring: the variable in the logistic regression analysis with the highest coefficient was defined as 10 points (education level in this study). Scores for the other variables were determined by equating, with final rounding to integers. ②Patients scoring: the scores of each patient were the sum of the scores of all variables in the scoring system (points= age*8+education level*10 +bronchiectasis*4 +RDW-CV*7 +INR*7+AGR*5+ CPR*6). (5) Evaluation of the scoring system: ROC analysis, calibration curve, and decision curve analysis (DCA) were used for evaluating the predictive power of the scoring system. (6) Determining the cut-off value of the scoring system: The ROC analysis was used to find the optimal cut-off score, corresponding to the highest Youden index, to distinguish FTO from UTO.
All the statistical analysis was conducted by SPSS (version 20.0; IBM, Chicago, IL, USA) and R software version 4.20 (http://www.rproject.org). Two-sided P <0.05 was considered statistically significant.
Result
Study Population
A total of 470 participants from Wuhan Jinyintan Hospital were diagnosed with MDR/RR-TB. 333 MDR/RR-TB patients complied with the eligibility standards, including 68 RR-TB patients, 252 MDR-TB patients and 13 XDR-TB patients. Of the 333 cases, 50 showed treatment failure, 42 died, 122 were cured, and 119 completed their treatment. Furthermore, the training set was randomly assigned to about 66.7% of the participants (N = 241), while the validation set was given to the remaining patients (N = 92). Figure 1 lists a detailed flowchart of the participant selection process. As shown in Table 1, there is no significant differences in the sociodemographic characteristics (such as age and education levels), radiological features (such as bronchiectasis) and treatment outcomes between the training and validation sets. In addition, the distribution of the laboratory indicators in the model between the training and validation sets is shown in Supplementary Table 2. The results indicate that our randomly assigned data sets are mutually independent.
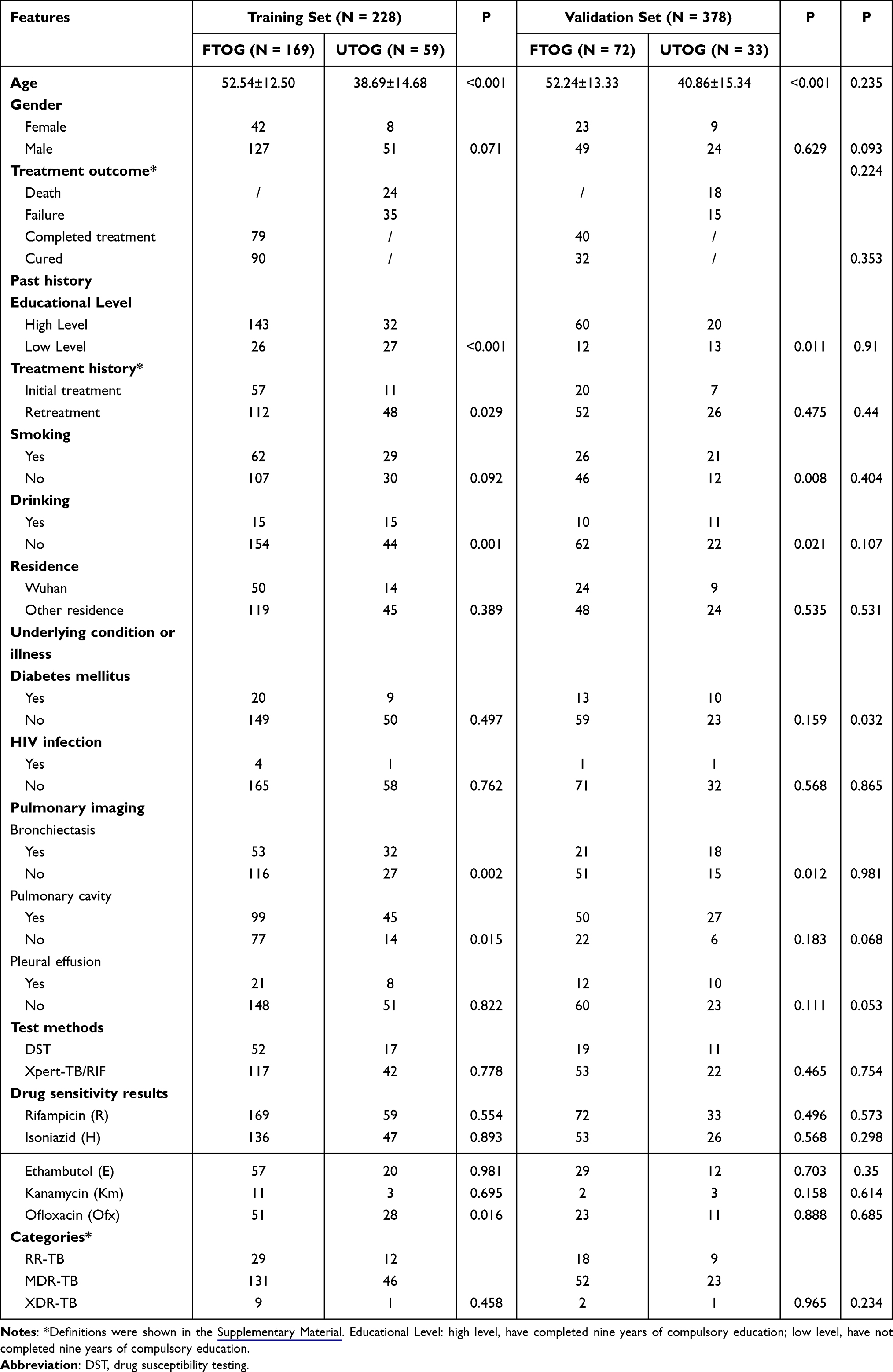 |
Table 1 Comparisons of Sociodemographic Characteristics and Radiological Features in Training and Validation Sets |
 |
Figure 1 Flowchart of participant selection and the performance of the steps. Abbreviations: MDR/RR-TB, multidrug- and rifampicin-resistant tuberculosis; UTO, unfavorable treatment outcomes; LASSO, least absolute shrinkage and selection operator; AUC, area under curve. |
Construction of a Nomogram and Scoring System
A total of 14 variables were selected After performing LASSO regression (Figure 2). 13 variables with AUC of more than 0.6 were submitted to multivariate regression analysis to build a highly accurate prediction model (Supplementary Table 3). Seven key variables (Age, education levels, bronchiectasis, RDW-CV, INR, AGR, CPR) were chosen to construct the prediction model (Table 2). Incorporating these predictive markers, the nomogram was built based on multivariate regression analysis (Figure 3A). Drawing a vertical line straight up from the matching value of the predictive factor to an axis labeled “Points” would reveal the risk point for each factor in the nomogram. The predictive nomogram demonstrated high discrimination (AUC = 0.888; 95% CI: 0.836–0.940) (Figure 3B) and reliable calibration (Figure 3C). The nomogram’s net benefit and predictive power were assessed using the decision curve analysis and calibration curves. As shown in Figure 3D, MDR/RR-TB patients would benefit from using this predictive nomogram with a threshold probability 0.26.
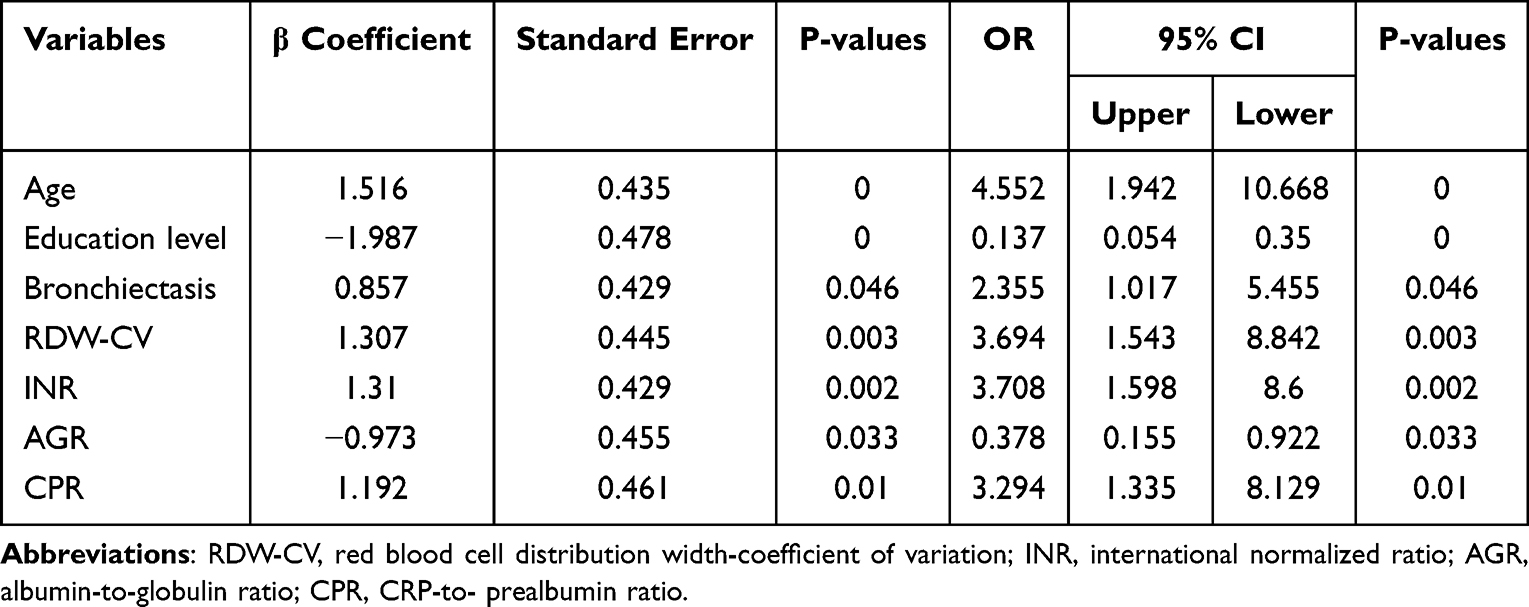 |
Table 2 Multivariate Regression Analysis of Significant Parameters in the Training Set |
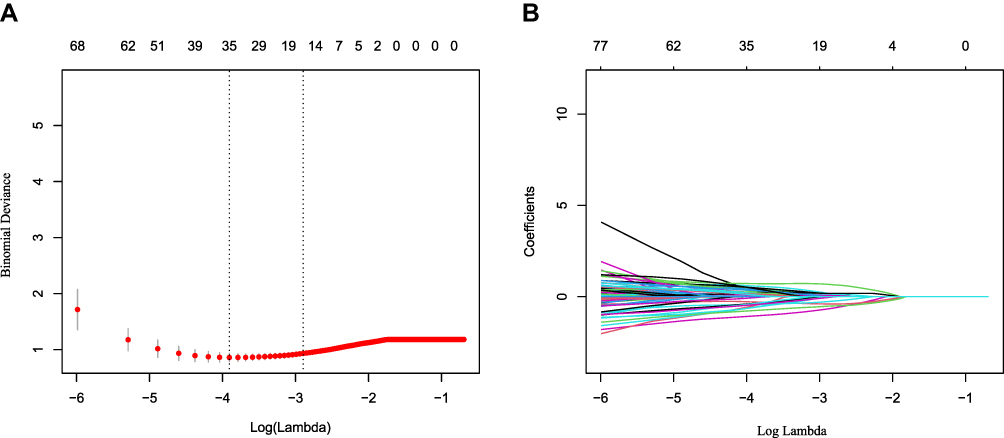 |
Figure 2 Variables selection using the LASSO regression analysis with 10-fold cross-validation. Abbreviations: LASSO, least absolute shrinkage and selection operator; SE, standard error. Notes: (A) Tuning parameter (lambda) selection of deviance in the LASSO regression based on the minimum criteria (left dotted line) and the 1-SE criteria (right dotted line). (B) A coefficient profile plot was created against the log (lambda) sequence. In the present study, Variable’s selection was according to the 1-SE criteria. |
 |
Figure 3 Calibration and clinical use of a nomogram for the prediction of UTO in MDR/RR-TB. Abbreviations: UTO, unfavorable treatment outcomes; MDR/RR-TB, multidrug- and rifampicin-resistant tuberculosis. Notes: (A) Nomogram for predicting UTO in MDR/RR-TB. (B) ROC curve of the nomogram. (C) Calibration curve of the nomogram. (D) DCA of the nomogram. |
Considering the clinical application, we established a novel scoring system based on this well-performing nomogram with integer points: age (8 points), education level (10 points), bronchiectasis (4 points), RDW-CV (7 points), INR (7 points), AGR (5 points) and CPR (6 points) (Table 3).
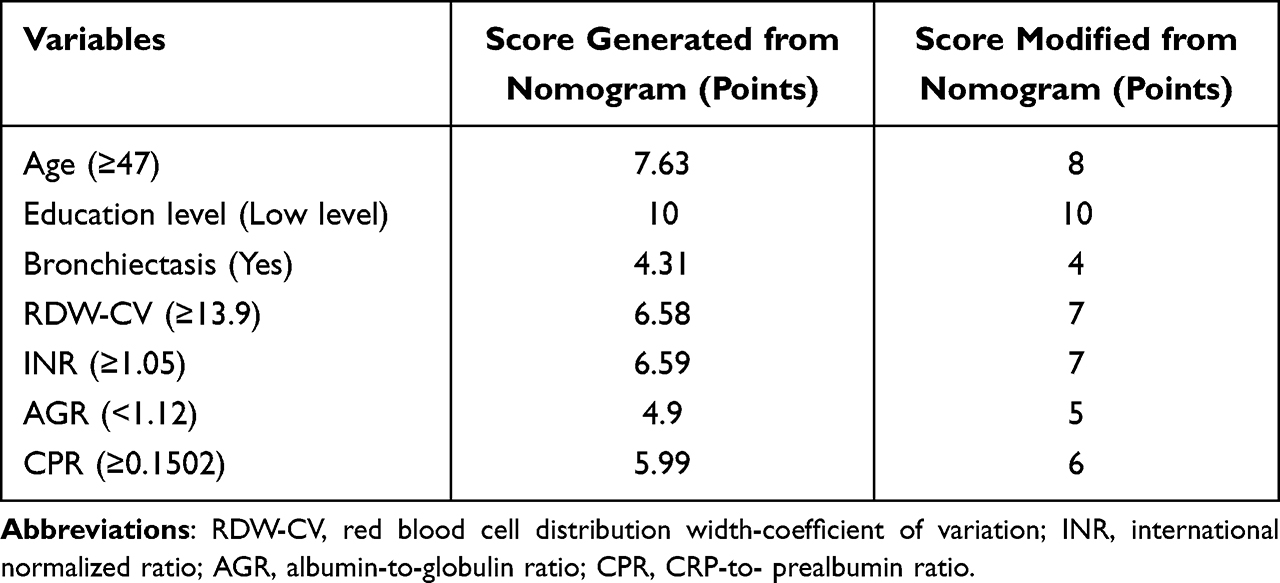 |
Table 3 A Scoring System Developed from a Nomogram of the Training Set |
Predictive Performance of the Scoring System in the Training Set and Validation Set
We obtain the appropriate cut-off points through the maximum Youden index. When the total points ≥19 points, drug-resistant TB patients were more likely to have a poor prognosis after treatment. And the sensitivity and specificity of the scoring system were 0.831 and 0.834(Supplementary Table 4). Additionally, the AUC values of this scoring system for predicting UTO were 0.887 (95% CI=0.835–0.939) in the training set, 0.805 (95% CI=0.714–0.896) in the validation set (Figure 4A). Furthermore, this scoring system also demonstrated satisfactory calibration in the training set (Figure 4B) and validation set (Figure 4C), indicating that there was no discernible discrepancy between the expected probability and the actual probability.
 |
Figure 4 Discrimination and calibration of the scoring system for the prediction of UTO in MDR/RR-TB. Abbreviations: UTO, unfavorable treatment outcomes; MDR/RR-TB, drug-resistant tuberculosis. Notes: ROC curves of the scoring system in the training set (A) and validation set (B). Calibration curves of the scoring system in the training set (C) and validation set (D). |
Predictive Performance of the Scoring System for Predicting the Death of MDR/RR-TB Patients
As clinicians are often concerned about the death of MDR/RR-TB patients, we applied the scoring system to analyze this particular subgroup. Satisfyingly, this scoring model showed good discriminatory power to predict the occurrence of death with the AUC 0.930 (95% CI= 0.872–0.989) in the training set (Figure 5A) and 0.872 (95% CI=0.778–0.967) in the validation set (Figure 5B). In addition, the scoring system also showed a good calibration to the predict death risk of DR-TB in two sets (Figure 5C and D).
 |
Figure 5 Discrimination and calibration of the scoring system for the prediction of death in MDR/RR-TB. Abbreviations: UTO, unfavorable treatment outcomes; MDR/RR-TB, multidrug- and rifampicin-resistant tuberculosis. Notes: ROC curves of the scoring system in the training set (A) and validation set (B). Calibration curves of the scoring system in the training set (C) and validation set (D). |
Discussion
MDR/RR-TB is one of the most difficult barriers to ending TB worldwide. Early identification and intervention of individuals with drug-resistant TB at high risk of poor prognosis can help avoid unfavorable treatment outcomes to achieve the WHO goal of ending TB. In this study, the success rate of ATT for MDR/RR-TB is approximately 69%, which is similar to the reports in Xi’an18 and Zhejiang,19 China.
In the present studies, LASSO regression and ROC analysis were used to screen the variables. After multivariate logistic regression analysis, seven effective predictors (age, education levels, bronchiectasis, RDW-CV, INR, AGR, CPR) were further selected to build the model, which allowed a potentially robust and reliable model to be developed.
Age with 8 points is an important parameter in our model. In the present study, MDR-TB patients older than 45 years old were more likely to have a poor treatment outcome, suggesting that we need to pay attention to the management of other diseases in elderly patients during the treatment process. These results are consistent with previous studies that have shown a higher probability of comorbid disease, adverse effects and death with increasing age.18–22 In addition, our study pointed out that patients with lower levels of education (10 points) had the greatest risk of UTO during treatment. The possible reason for this is that treatment of drug-resistant TB requires more financial support, and financial status is correlated with education level,23,24 which is higher in those who have completed education than in those who have not. In addition, patients with higher levels of education can gain more knowledge about TB and improve treatment adherence.25,26 Radiological data such as chest Computed Tomography (CT) can provide important evidence for the diagnosis of TB patients, and we set bronchiectasis as one of the variables to predict treatment outcomes. In the Asia-Pacific region, infections such as tuberculosis are the main cause of bronchiectasis,27 which would lead to the progression of the disease owing to combined Pseudomonas aeruginosa infection and reduced microflora diversity.28
In order to further improve the predictive accuracy, in the present study, 60 laboratory markers were evaluated, including major parameters often used in clinical settings and efficient ratio indicators, such as CPR and NLR. Recently, CPR and NLR are newly discovered markers of inflammation that are simpler, easier to measure, and relatively stable compared to other inflammatory markers. Recent research has also demonstrated that CPR and NLR could predict the prognosis of COVID-19.29 And higher levels of CPR in gastric cancer patients after radical resection had a higher risk for recurrence.30 It is worth noting that there is no study focusing on CPR in TB patients. Our study revealed that CPR and NLR had great predictive power for UTO, as evidenced by AUC values of 0.730 and 0.680, respectively. Lou et al showed that prealbumin and C-reactive protein had significant associations with poor prognosis in anemic TB patients,12 which was roughly consistent with our research. Additionally, prealbumin could be a sensitive indicator of anemia and malnutrition,31,32 and C-reactive protein has also been discovered to be an effective biomarker for TB-HIV screening.33
In addition to inflammation-related indicators, parameters related to anemia (RDW-CV), malnutrition (AGR), and coagulation (INR) are also included in the scoring system. RDW-CV was proven to have significant associations with poor prognosis in anemic TB patients.12 Moreover, the lower albumin to globulin ratio (AGR) may be used to predict unfavorable outcomes due to the links between immunoreactivity and malnutrition.11 The role of coagulation function in TB has attracted increasing attention. Wang et al found that aspirin enhanced the clinical benefit of the treatment in patients with tuberculosis combined with type 2 diabetes mellitus.34 Previous studies have suggested that the levels of APTT and Fbg in TB patients are higher than those in the control group.13 Even, decreased Fbg values were observed after the anti-tuberculosis therapy.13 In addition, Fbg could evaluate early treatment response in HIV/MDR-TB coinfection patients.35 In the present study, we first found that INR could predict the UTO of MDR/RR-TB, and the AUC value was 0.630.
Finally, to develop a scoring system, we transformed the model into a scoring system and created a user-friendly clinical tool. Compared with clinical features, laboratory examination indicators can not only explain the possible underlying mechanisms but also greatly improve predictive efficiency. Our scoring system predicted UTO (AUC=0.887, 95% CI =0.835–0.939) and death (AUC=0.930, 95% CI=0.872–0.989) with high accuracy. MDR/RR-TB patients could get improved risk classification. And according to the performance of clinical decision curves, predictive models can help clinicians make better decisions. Generally, the indicators involved in the scoring system are easy to obtain at the designated specialist hospital for tuberculosis and the cost is acceptable. We recommend the use of our scoring system in primary TB hospitals because of its simplicity and practicality. Through this user-friendly model, clinicians can quantitatively determine individual prognoses, provide personalized guidance and treatment, and improve the success rate of treatment for MDR/RR-TB patients. In particular, to our knowledge, this is the first predictive scoring model for the treatment outcomes of MDR/RR-TB patients.
In recent years, with the development of analytical approaches, the construction of mathematical models based on multiple markers has been increasingly applied in the field of
medicine. Khan et al developed artificial neural networks to predict tuberculosis disease.36 As for drug-resistant tuberculosis, clinical mutants such as RpsA-S324F could offer valuable information for better management of drug-resistant tuberculosis.37 However, single mutants provide less information, and are inconvenient and expensive to use in clinical settings. In addition, limited studies attempt to help clinicians make decisions by developing a prediction model to predict poor treatment outcomes of DR-TB patients. Denekew et al4 developed a nomogram to predict UTO in MDR-TB patients based on anemia, adverse events, comorbidity, age, marriage status, and treatment supporter. The AUC of the nomogram was 0.753 (95% CI=0.708–0.798). Similarly, Luiz et al5 also used clinical features to establish a nomogram to identify death, default, and failure in MDR-TB patients. However, the AUC of the nomogram was unsatisfactory. In addition to the exploration of UTO in DR-TB patients, Indian researchers constructed a model to forecast poor treatment outcomes in TB-HIV co-infection patients, with an AUC of 0.78. Treatment history, TB type (pulmonary or extrapulmonary or both), and baseline smear results (negative or positive) were enrolled in the model. Unfortunately, Although the clinical characteristics and parameters required by the above methods are readily available, further applications are limited by suboptimal predictive power.
Compared with other models, our scoring system has several advantages. Firstly, in previous studies, most models included only clinical feature variables (eg, adverse events, comorbidities, age, marital status, and treatment supporters) and thus obtained moderate predictive power. As the results showed, our predictive scoring system is more accurate than previous studies. Secondly, in addition to some clinical and radiological features, the predictive scoring system innovatively incorporates laboratory indicators (inflammatory, nutritional and coagulation indicators). These indicators of the scoring system provide a more comprehensive indication of the baseline status of MDR/RR-TB patients, thus providing targeted guidance to the patients. For example, we can optimize nutritional status and improve hyperinflammatory states, thereby minimizing mortality in MDR/RR-TB patients. Thirdly, our scoring system facilitates clinical use by calculating scores, especially in economically poor areas or primary hospitals. Last but not least, our scoring system has a remarkable performance power in predicting death due to MDR/RR-TB. When patients are at greater risk of UTO, especially death, they should be advised to go to a high-level hospital for further treatment, which will reduce the mortality rate, time cost and financial loss, and improve the treatment success.
However, the current study is not exempt from some limitations. Firstly, the sample size of our studies was relatively small for objective reasons, and future studies will require larger and multicenter sets to further improve the model. Additionally, some studies showed that culture conversion status may be a potential factor related to the treatment outcomes,38,39 but we did not include the variable because of the extensive absence of cultivation information.
Conclusion
Our findings suggest that age, education level, bronchiectasis, RDW-CV, INR, AGR and CPR were valuable to predict unfavorable treatment outcomes in DR-TB patients, especially in predicting death risk. The use of our scoring system in clinical practice will help identify these populations for tailored management to prevent poor events.
Data Sharing Statement
The datasets used in this study are obtainable from the corresponding author on reasonable request.
Ethics Statement
The Declaration of Helsinki was followed in the conduct of this study. The Huazhong University of Science and Technology’s Tongji Medical College’s ethics committee at Wuhan Jinyintan Hospital gave its approval to the study protocol (KY-2022-06.01). Personal identifiers were not provided to maintain privacy. In accordance with the national legislation and institutional standards, informed consent from the study participants was not necessary.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lange C, Chesov D, Heyckendorf J, Leung CC, Udwadia Z, Dheda K. Drug-resistant tuberculosis: an update on disease burden, diagnosis and treatment. Respirology. 2018;23(7):656–673. doi:10.1111/resp.13304
2. Knight GM, McQuaid CF, Dodd PJ, Houben RMGJ. Global burden of latent multidrug-resistant tuberculosis: trends and estimates based on mathematical modelling. Lancet Infect Dis. 2019;19(8):903–912. doi:10.1016/S1473-3099(19)30307-X
3. World Health Organization. Global Tuberculosis Report 2021. World Health Organization; 2021.
4. Anley DT, Akalu TY, Merid MW, Tsegaye T. Development and validation of a nomogram for the prediction of unfavorable treatment outcome among multi-drug resistant tuberculosis patients in North West Ethiopia: an application of prediction modelling. Infect Drug Resist. 2022;15:3887–3904. doi:10.2147/IDR.S372351
5. Arroyo LH, Ramos ACV, Yamamura M, et al. Predictive model of unfavorable outcomes for multidrug-resistant tuberculosis. Rev Saude Publica. 2019;53:77. doi:10.11606/s1518-8787.2019053001151
6. Madan C, Chopra KK, Satyanarayana S, et al. Developing a model to predict unfavourable treatment outcomes in patients with tuberculosis and human immunodeficiency virus co-infection in Delhi, India. PLoS One. 2018;13(10):e0204982. doi:10.1371/journal.pone.0204982
7. Yu Q, Yan J, Tian S, et al. A scoring system developed from a nomogram to differentiate active pulmonary tuberculosis from inactive pulmonary tuberculosis. Front Cell Infect Microbiol. 2022;12:947954. doi:10.3389/fcimb.2022.947954
8. Tang S, Tan S, Yao L, et al. Risk factors for poor treatment outcomes in patients with MDR-TB and XDR-TB in China: retrospective multi-center investigation. PLoS One. 2013;8(12):e82943. doi:10.1371/journal.pone.0082943
9. Kuaban A, Balkissou AD, Ekongolo MCE, Nsounfon AW, Pefura-Yone EW, Kuaban C. Incidence and factors associated with unfavourable treatment outcome among patients with rifampicin-resistant pulmonary tuberculosis in Yaoundé, Cameroon. Pan Afr Med J. 2021;38:229. doi:10.11604/pamj.2021.38.229.28317
10. Alemu A, Bitew ZW, Worku T. Poor treatment outcome and its predictors among drug-resistant tuberculosis patients in Ethiopia: a systematic review and meta-analysis. Int J Infect Dis. 2020;98:420–439. doi:10.1016/j.ijid.2020.05.087
11. Li K, Tang H, Yang Y, et al. Clinical features, long-term clinical outcomes, and prognostic factors of tuberculous meningitis in West China: a multivariate analysis of 154 adults. Expert Rev Anti Infect Ther. 2017;15(6):629–635. doi:10.1080/14787210.2017.1309974
12. Luo M, Liu M, Wu X, et al. Impact of anemia on prognosis in tuberculosis patients. Ann Transl Med. 2022;10(6):329. doi:10.21037/atm-22-679
13. Verma R, Mahapatro S, Kumar A, et al. Platelet dysfunction and coagulation assessment in patients of tuberculous meningitis. Neurol Sci. 2020;41(8):2103–2110. doi:10.1007/s10072-020-04299-4
14. Caccamo N, Dieli F. Inflammation and the coagulation system in tuberculosis: tissue Factor leads the dance. Eur J Immunol. 2016;46(2):303–306. doi:10.1002/eji.201546225
15. Jin H. Effect of big data analysis-based remote management combined with yangyin runfei decoction on coagulation function, pulmonary function, and quality of life of pulmonary tuberculosis patients. Comput Intell Neurosci. 2022;2022:1708133. doi:10.1155/2022/1708133
16. World Health Organization. WHO Consolidated Guidelines on Drug-Resistant Tuberculosis Treatment. World Health Organization; 2019.
17. World Health Organization. Definitions and Reporting Framework for Tuberculosis – 2013 Revision: Updated December 2014 and January 2020. World Health Organization; 2013.
18. Ma J-B, Zeng L-C, Ren F, et al. Treatment outcomes and risk factors of multidrug-resistant tuberculosis patients in Xi’an China, a retrospective cohort study. Infect Drug Resist. 2022;15:4947–4957. doi:10.2147/IDR.S376177
19. Zhang L, Meng Q, Chen S, et al. Treatment outcomes of multidrug-resistant tuberculosis patients in Zhejiang, China, 2009–2013. Clin Microbiol Infect. 2018;24(4):381–388. doi:10.1016/j.cmi.2017.07.008
20. Van LH, Phu PT, Vinh DN, et al. Risk factors for poor treatment outcomes of 2266 multidrug-resistant tuberculosis cases in Ho Chi Minh City: a retrospective study. BMC Infect Dis. 2020;20(1):164. doi:10.1186/s12879-020-4887-1
21. Sharma N, Khanna A, Chandra S, et al. Trends & treatment outcomes of multidrug-resistant tuberculosis in Delhi, India (2009–2014): a retrospective record-based study. Indian J Med Res. 2020;151(6):598–603. doi:10.4103/ijmr.IJMR_1048_18
22. Hannah HA, Miramontes R, Gandhi NR. Sociodemographic and clinical risk factors associated with tuberculosis mortality in the United States, 2009–2013. Public Health Rep. 2017;132(3):366–375. doi:10.1177/0033354917698117
23. Becerra MC, Huang -C-C, Lecca L, et al. Transmissibility and potential for disease progression of drug resistant: prospective cohort study. BMJ. 2019;367:l5894. doi:10.1136/bmj.l5894
24. Wang S, Tu J. Nomogram to predict multidrug-resistant tuberculosis. Ann Clin Microbiol Antimicrob. 2020;19(1):27. doi:10.1186/s12941-020-00369-9
25. Tupasi TE, Garfin AMCG, Kurbatova EV, et al. Factors associated with loss to follow-up during treatment for multidrug-resistant tuberculosis, the Philippines, 2012–2014. Emerg Infect Dis. 2016;22(3):491–502. doi:10.3201/eid2203.151788
26. Abdelbary BE, Garcia-Viveros M, Ramirez-Oropesa H, Rahbar MH, Restrepo BI. Predicting treatment failure, death and drug resistance using a computed risk score among newly diagnosed TB patients in Tamaulipas, Mexico. Epidemiol Infect. 2017;145(14):3020–3034. doi:10.1017/S0950268817001911
27. Chandrasekaran R, Mac Aogáin M, Chalmers JD, Elborn SJ, Chotirmall SH. Geographic variation in the aetiology, epidemiology and microbiology of bronchiectasis. BMC Pulm Med. 2018;18(1):83. doi:10.1186/s12890-018-0638-0
28. Dicker AJ, Lonergan M, Keir HR, et al. The sputum microbiome and clinical outcomes in patients with bronchiectasis: a prospective observational study. Lancet Respir Med. 2021;9(8):885–896. doi:10.1016/S2213-2600(20)30557-9
29. Karimi A, Shobeiri P, Kulasinghe A, Rezaei N. Novel systemic inflammation markers to predict COVID-19 prognosis. Front Immunol. 2021;12:741061. doi:10.3389/fimmu.2021.741061
30. Lu J, Xu B-B, Zheng Z-F, et al. CRP/prealbumin, a novel inflammatory index for predicting recurrence after radical resection in gastric cancer patients: post hoc analysis of a randomized Phase III trial. Gastric Cancer. 2019;22(3):536–545. doi:10.1007/s10120-018-0892-0
31. Luo Y, Xue Y, Yuan X, et al. Combination of prealbumin and tuberculosis-specific antigen/phytohemagglutinin ratio for discriminating active tuberculosis from latent tuberculosis infection. Int J Clin Pract. 2021;75(4):e13831. doi:10.1111/ijcp.13831
32. Cunningham LL, Madsen MJ, Van Sickels JE. Using prealbumin as an inflammatory marker for patients with deep space infections of odontogenic origin. J Oral Maxillofac Surg. 2006;64(3):375–378. doi:10.1016/j.joms.2005.11.008
33. Yoon C, Semitala FC, Atuhumuza E, et al. Point-of-care C-reactive protein-based tuberculosis screening for people living with HIV: a diagnostic accuracy study. Lancet Infect Dis. 2017;17(12):1285–1292. doi:10.1016/S1473-3099(17)30488-7
34. Wang W, Du Z, Ni M, et al. Aspirin enhances the clinical efficacy of anti-tuberculosis therapy in pulmonary tuberculosis in patients with type 2 diabetes mellitus. Infect Dis. 2020;52(10):721–729. doi:10.1080/23744235.2020.1778177
35. Cudahy PGT, Warren JL, Cohen T, Wilson D. Trends in C-reactive protein, D-dimer, and fibrinogen during therapy for HIV-associated multidrug-resistant tuberculosis. Am J Trop Med Hyg. 2018;99(5):1336–1341. doi:10.4269/ajtmh.18-0322
36. Khan MT, Kaushik AC, Ji L, Malik SI, Ali S, Wei D-Q. Artificial neural networks for prediction of tuberculosis disease. Front Microbiol. 2019;10:395. doi:10.3389/fmicb.2019.00395
37. Khan MT, Rehaman AU, Junaid M, Malik SI, Wei D-Q. Insight into novel clinical mutants of RpsA-S324F, E325K, and G341R of associated with pyrazinamide resistance. Comput Struct Biotechnol J. 2018;16:379–387. doi:10.1016/j.csbj.2018.09.004
38. Günther G, Lange C, Alexandru S, et al. Treatment outcomes in multidrug-resistant tuberculosis. N Engl J Med. 2016;375(11):1103–1105. doi:10.1056/NEJMc1603274
39. Kurbatova EV, Cegielski JP, Lienhardt C, et al. Sputum culture conversion as a prognostic marker for end-of-treatment outcome in patients with multidrug-resistant tuberculosis: a secondary analysis of data from two observational cohort studies. Lancet Respir Med. 2015;3(3):201–209. doi:10.1016/S2213-2600(15)00036-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.