Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
A Risk Prediction Model for MDR Acinetobacter baumannii Pneumonia in Cerebral Hemorrhage Patients Based on Inflammatory Markers from Peripheral Blood Cell Counts
Authors Min J, Tian W, Hu H, Zhao Y
Received 7 September 2025
Accepted for publication 8 January 2026
Published 20 January 2026 Volume 2026:19 561364
DOI https://doi.org/10.2147/JMDH.S561364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Charles V Pollack
Jie Min,1,* Wei Tian,1,* Hang Hu,1 Yongfeng Zhao2
1Neurointensive Care Unit, The First Affiliated Hospital of Yangtze University, Jingzhou, 434000, People’s Republic of China; 2Department of Hematology, The First Affiliated Hospital of Yangtze University, Jingzhou, 434000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongfeng Zhao, Email [email protected] Jie Min, Email [email protected]
Background: Acinetobacter baumannii (A. baumannii) is one of the most common pathogens in pneumonia patients with cerebral hemorrhage. Exploring objective predictors of pneumonia due to multidrug-resistant (MDR) A. baumannii is of great significance for infection prevention and control.
Objective: To construct a risk prediction model for MDR A. baumannii pneumonia in cerebral hemorrhage patients based on inflammatory markers from peripheral blood cell counts.
Methods: A retrospective study was carried out in cases with pneumonia due to A. baumannii among patients with cerebral hemorrhage from January 2021 to December 2024. The baseline data and peripheral blood cell counts were used for analysis. The risk factors for pneumonia due to MDR A. baumannii were obtained through univariate and multivariate analyses.
Results: Among the 182 patients included, there were 79 cases with pneumonia due to MDR A. baumannii and 103 cases with pneumonia due to sensitive A. baumannii. The level of systemic immune-inflammation index (SII) at admission in patients with pneumonia due to MDR A. baumannii was significantly higher than sensitive A. baumannii. The result of multivariate logistic regression analysis showed that SII level (≥ 1851.91 × 109/L), tracheotomy duration (≥ 6 days) and Glasgow coma scale score (< 11) were risk factors for pneumonia due to MDR A. baumannii. The Area Under Curve (AUC) of the multivariate logistic regression model was 0.755, the sensitivity and specificity were 86.1% and 55.3%, respectively.
Conclusion: Longer duration of tracheotomy, lower GCS score and higher SII at admission were possibly associated with pneumonia due to MDR A. baumannii in cerebral hemorrhage patients. For high-risk patients, taking timely preventive and control measures against MDR A. baumannii pneumonia infections is crucial.
Keywords: Acinetobacter baumannii, systemic immune-inflammation index, multidrug-resistant, pneumonia, neutrophil-lymphocyte ratio
Introduction
Due to consciousness disorders, swallowing difficulties, and bed rest in patients with cerebral hemorrhage, pneumonia has become one common complication of cerebral hemorrhage. The incidence of pneumonia in patients with cerebral hemorrhage was over 40% in the Intensive Care Unit.1,2 Pneumonia has seriously affected the prognosis and mortality of stroke patients.3,4
A. baumannii became the most common pathogen in patients with cerebral hemorrhage complicated with pneumonia.1 Moreover, A. baumannii is a special pathogen with great ability to survive in vitro for a long time and is prone to clonal dissemination.5 Multidrug-resistant and pan-drug-resistant A. baumannii have become global epidemic6 and are the most important pathogens causing hospital acquired infections in China. They could cause respiratory tract infections, bacteremia, urinary tract infections, meningitis, surgical site infections, etc.7 They also increased the risk of death.8 In one systematic review including 27 studies, the overall mortality rate of patients with MDR A. baumannii pneumonia could reach 42.6%.9
Pneumonia due to MDR A. baumannii mainly occurred in patients with mechanical ventilation in the Intensive Care Unit.10,11 Tracheotomy was widely recognized as a risk factor for A. baumannii pneumonia.12 Recent surgery (within 1 mo) and invasive interventions were also identified as risk factors related to pneumonia-related A. baumannii bacteremia.13 Patients with stroke were prone to infections caused by MDR A. baumannii due to tracheotomy and prolonged use of antibiotics, which could increase the cost and prolong the hospital stay. Therefore, exploring objective predictors of pneumonia due to MDR A. baumannii is of great significance for infection prevention and control.
Current research generally agreed that the development of MDR A. baumannii pneumonia resulted from the combined effects of a patient’s baseline condition, specific healthcare exposures, and laboratory indicators. Advanced age, critical illness, or being immunocompromised are significant baseline risk factors. Meanwhile, ICU admission, invasive procedures such as mechanical ventilation and central venous catheterization, as well as prior exposure to carbapenem antibiotics constitute key healthcare-related drivers.14–16
However, these factors are largely static or retrospective in nature, lacking the ability to reflect the patient’s dynamic immune-inflammatory status. In recent years, systemic inflammatory markers, such as the neutrophil-to-lymphocyte ratio (NLR), system inflammation response index (SIRI), and C-reactive protein have garnered significant attention due to their easy accessibility, dynamic monitorability, and objective reflection of infection and immune balance. Theoretically, the dynamic changes in these indicators can delineate the host’s immune response intensity to pathogens and may even predict the risk of specific pathogen infections. However, existing research primarily focuses on the value of these indicators in distinguishing infection from non-infectious states or assessing prognosis,17,18 whereas their investigation as early and specific predictive tools for MDR A. baumannii pneumonia remains limited. Therefore, this study aims to construct a risk prediction model based on dynamic inflammatory markers by systematically analyzing serial inflammatory marker data throughout the patient’s disease course.
Methods
Study Design
A retrospective study was conducted in the Neurosurgery Department and Neurointensive care unit of the First Affiliated Hospital of Yangtze University from January 2021 to December 2024. The inclusion criteria were as follows: intracranial hemorrhage confirmed by Computed Tomography (CT); new or progressive infiltrates and consolidations in the lungs confirmed by CT after 72 hours of surgery; A. baumannii found in sputum or pulmonary alveolar lavage fluid by bacterial culture or the next generation sequencing after 72 hours of surgery; undergoing surgeries after admission. The exclusion criteria were as follows: death within 48 hours of admission; pneumonia before admission; severe hematological disorders or immune deficiency affecting blood cell counts. This study was approved by the Institutional Review Board of the First Affiliated Hospital of Yangtze University (KY2025-022-01), and the requirement for informed patient consent was waived owing to its retrospective nature. All data were anonymized and handled with strict confidentiality to ensure compliance with the Declaration of Helsinki. A detailed flowchart is provided in Figure 1.
 |
Figure 1 Flowchart of the study. |
Diagnosis of pneumonia followed the diagnosis and treatment guidelines for hospital-acquired pneumonia in Chinese adults,19 depending on lower respiratory tract symptoms (eg, fever or chills, cough, or shortness of breath) and new focal chest signs coinciding with the onset or progressive pulmonary infiltrates on chest radiography. Except for the abnormal lesions identified by CT or chest X-ray, two or more of the following symptoms were also needed: fever with a body temperature over 38 degree Celsius; purulent airway secretions; leukocytes over 10×109/L or less than 4 ×109/L. The diagnosis required the joint judgment of two experienced doctors.
Data Collection
All clinical data were extracted from the Hospital Information System by two independent reviewers (JM and WT) to ensure accuracy. Any controversies were resolved by a third reviewer (HH). The following data were collected from the enrolled patients: demographic characteristics; Glasgow coma scale (GCS) score at admission; combined baseline lung diseases (including rib fracture, emphysema, and bronchiectasis); combined hypertension, diabetes mellitus, and hypoproteinemia; duration of invasive procedures including urinary catheter, central venous catheterization (CVC), tracheotomy, and gastric tube; duration of antibiotics. Neutrophils, lymphocytes, monocytes, and platelets at admission, on the first and third postoperative days needed to be collected. Neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), Systemic Immune-Inflammation Index (SII), and system inflammation response index (SIRI) were calculated. SII=(neutrophil×platelet)/lymphocyte; SIRI =(neutrophil×monocyte)/lymphocyte.
This retrospective study analyzed microbiological data from the Department of Clinical Laboratory at the First Affiliated Hospital of Yangtze University. Within the routine diagnostic pipeline, definitive identification of bacterial isolates was achieved through matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Antimicrobial susceptibility testing was performed concurrently. The entire workflow was conducted following the guidelines of the Clinical and Laboratory Standards Institute (CLSI), ensuring consistency with the standard practices at the time of isolation.
Statistical Analysis
Statistical analysis were performed by SPSS 23.0 (SPSS Inc., Chicago, IL, USA) software. The univariate analysis of qualitative variables were conducted by Pearson Chi-Square, Continuity Correction, or Fisher’s Exact Test. The univariate analysis of quantitative variables were conducted by independent sample t-test, corrected t-test, or Mann–Whitney U-test according to the distribution and homogeneity characteristics. A multivariate logistic regression model was established to obtain the factors that could predict pneumonia due to MDR A. baumannii in patients with cerebral hemorrhage. The variables with p-values less than 0.05 in univariate analysis were regarded as covariates in the multivariate logistic regression analysis. The receiver operating characteristic curve (ROC) was used for the cut-off value of the quantitative variable with P-value less than 0.05. All P-values were bilateral, and considered statistically significant with P <0.05. GraphPad Prism version 9.4.1 (GraphPad Software, San Diego, CA, USA) was used for drawing figures. A post hoc power analysis was conducted using G*Power (version 3.1.9.7), based on the total sample size and an alpha level of 0.05. The analysis revealed a statistical power of 91.8%.
Results
Among all enrolled (182) patients with pneumonia due to A. baumannii, the median age was 59 years, with 139 males and 43 females. There were 127 cases with GCS score <11, 45 cases with intraventricular hemorrhage, 99 cases with hypertension, 17 cases with diabetes, and 83 cases with hypoproteinemia. The median duration for antibiotics before detection of A. baumannii was 10 days, for urinary catheterization was 9 days, for central venous catheterization was 5 days, for gastric catheterization was 9 days, and for tracheotomy was 6 days (Table 1). The NLR levels at admission, on the first and third postoperative days were 8.97 ± 9.32, 11.95 ± 6.94, and 7.71 ± 5.88, respectively. The PLR levels were 156.22 ± 203.20, 169.84 ± 153.85, and 216.03 ± 149.20, respectively. The MLR levels were 0.55 ± 0.64, 0.96 ± 0.64, and 0.74 ± 0.75, respectively. The SII levels were (1742.19 ± 2362.65) × 109/L, (1677.94 ± 1717.77) × 109/L, and (1690.63 ± 1715.53) × 109/L, respectively. The SIRI levels were (5.92 ± 9.79) × 109/L, (9.43 ± 9.53) × 109/L, and (6.24 ± 5.37) × 109/L, respectively (Table 2).
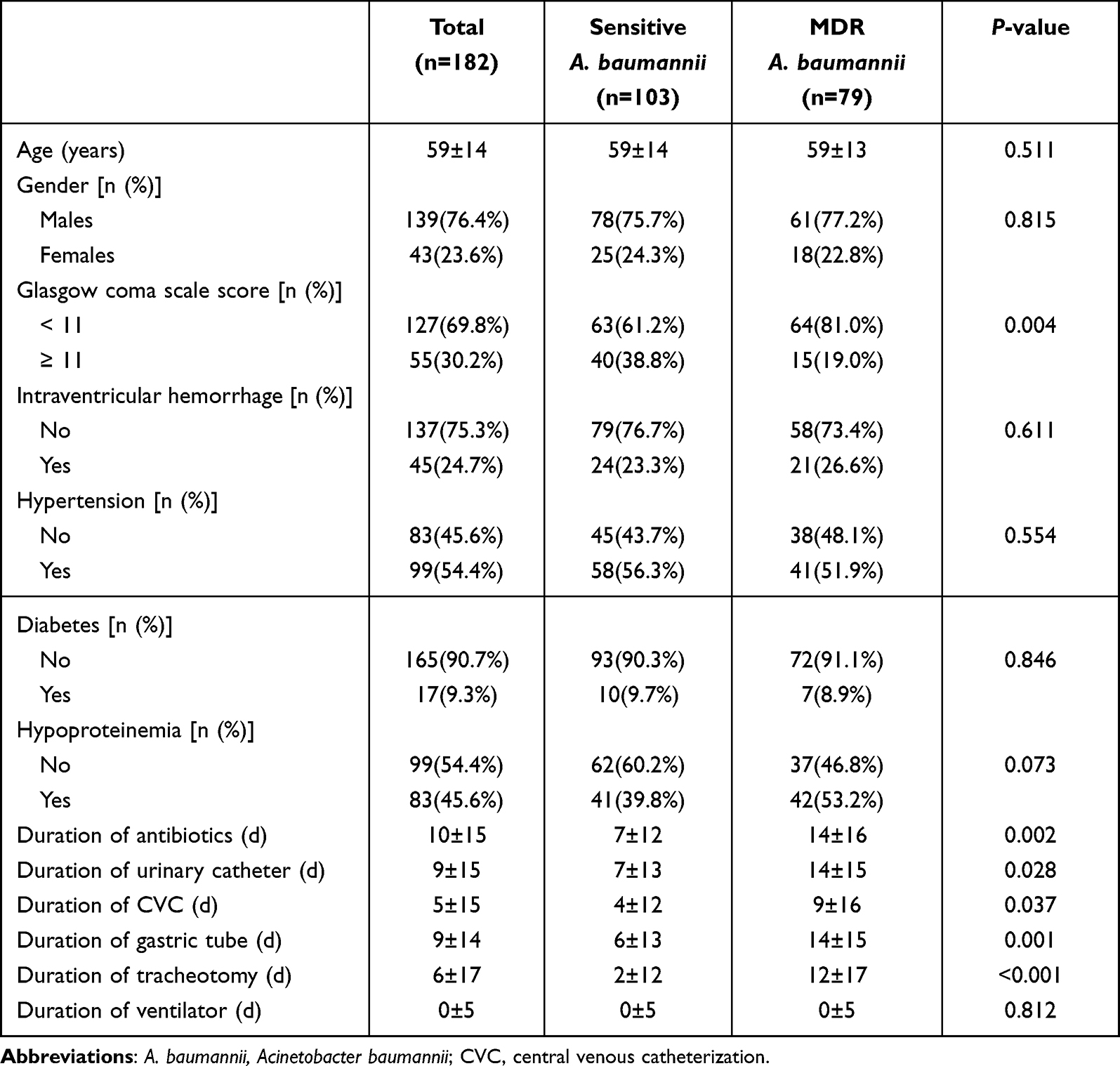 |
Table 1 Differences of Characteristics Between Cases with Pneumonia Due to Multidrug-Resistant (MDR) A. baumannii and Sensitive A. baumannii in Cerebral Hemorrhage Patients |
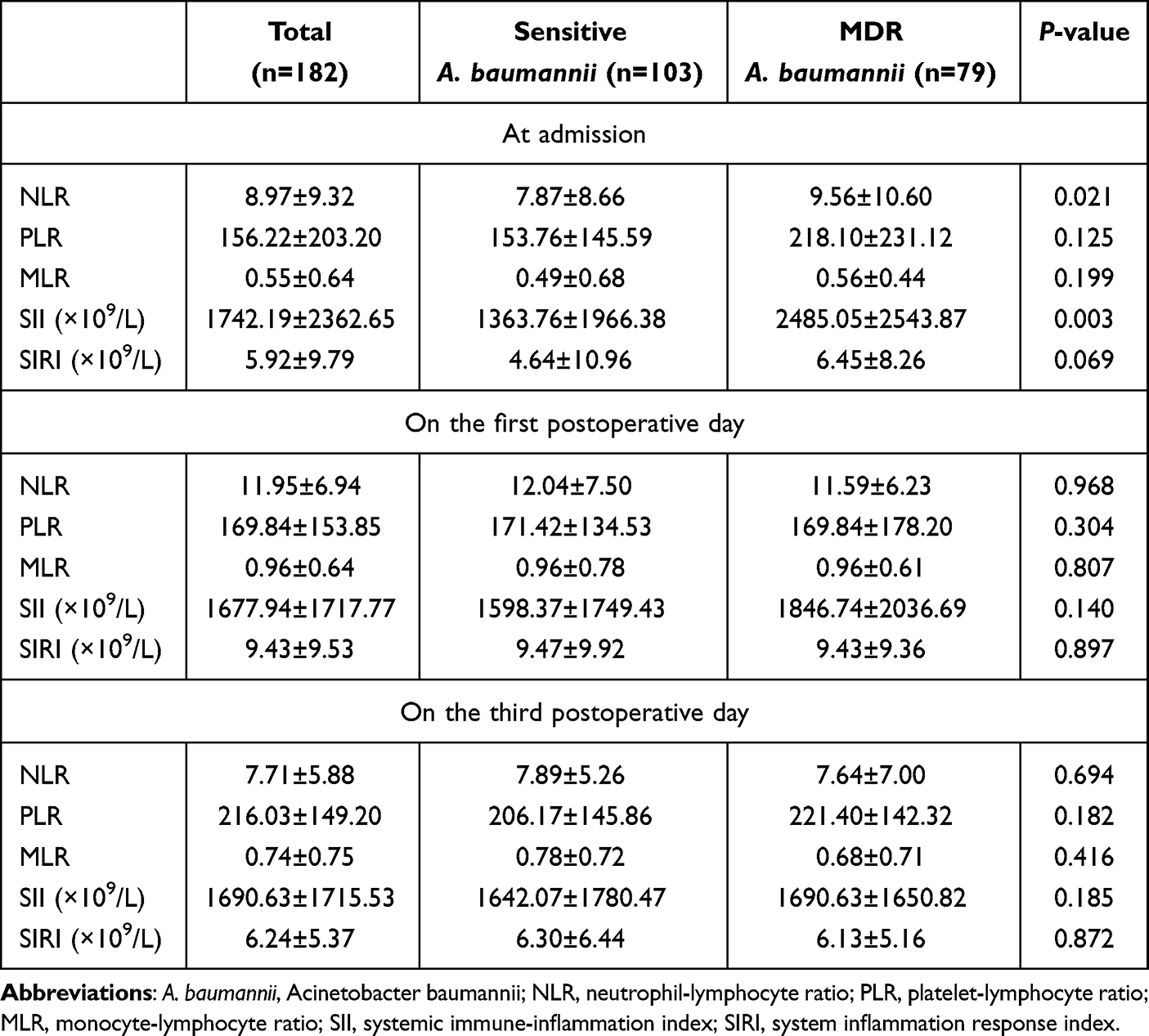 |
Table 2 Differences of Inflammatory Markers Between Cases with Pneumonia Due to Multidrug-Resistant (MDR) A. baumannii and Sensitive A. baumannii in Cerebral Hemorrhage Patients |
The proportion of cases with GCS score <11 in patients with pneumonia due to MDR A. baumannii was 81.0%, significantly higher than patients with pneumonia due to sensitive A. baumannii (61.2%), P = 0.004. The median duration for antibiotics (14 ± 16 days vs 7 ± 12 days, P = 0.002), for tracheotomy (12 ± 17 days vs 2 ± 12 days, P < 0.001), for gastric catheterization (14 ± 15 days vs 6 ± 13 days, P = 0.001), for urinary catheterization (14 ± 15 days vs 7 ± 13 days, P = 0.028), and for central venous catheterization (9 ± 16 days vs 4 ± 12 days, P = 0.037) in patients with pneumonia due to MDR A. baumannii were all significantly longer than that in patients with pneumonia due to sensitive A. baumannii. There were no significant differences in age (P = 0.511), sex (P = 0.815), proportions of combined intraventricular hemorrhage (P = 0.611), hypertension (P = 0.554), diabetes (P = 0.846), and hypoproteinemia (P = 0.073) (Table 1).
The NLR level at admission in pneumonia patients due to MDR A. baumannii was 9.56 ± 10.60, significantly higher than that in pneumonia patients due to sensitive A. baumannii (7.87 ± 8.66), P = 0.021. The SII level at admission was also significantly higher [(2485.05 ± 2543.87) × 109/L vs (1363.76 ± 1966.38) × 109/L], P = 0.003. There were no significant differences in PLR (P = 0.125), MLR (P = 0.199), and SIRI levels (P = 0.069) at admission between patients with MDR and sensitive A. baumannii pneumonia. In addition, there were also no significant differences in all inflammatory markers on the first and third postoperative days, P > 0.05 (Table 2).
The cut-off value of tracheotomy duration for predicting pneumonia due to MDR A. baumannii was 6 days (AUC = 0.674, 95% CI: 0.595–0.753, Youden index = 0.340, P < 0.001). The sensitivity and specificity were 70.9% and 63.1%, respectively (Figure 2A). The cut-off value of NLR at admission for predicting pneumonia due to MDR A. baumannii was 6.90 (AUC = 0.600, 95% CI: 0.517–0.682, Youden index = 0.238, P = 0.021). The sensitivity and specificity were 77.2% and 46.6%, respectively (Figure 2B). The cut-off value of SII at admission for predicting pneumonia due to MDR A. baumannii was 1851.91 × 109/L (AUC = 0.628, 95% CI: 0.545–0.711, Youdenindex = 0.232, P = 0.003). The sensitivity and specificity were 62.0% and 61.2%, respectively (Figure 2C).
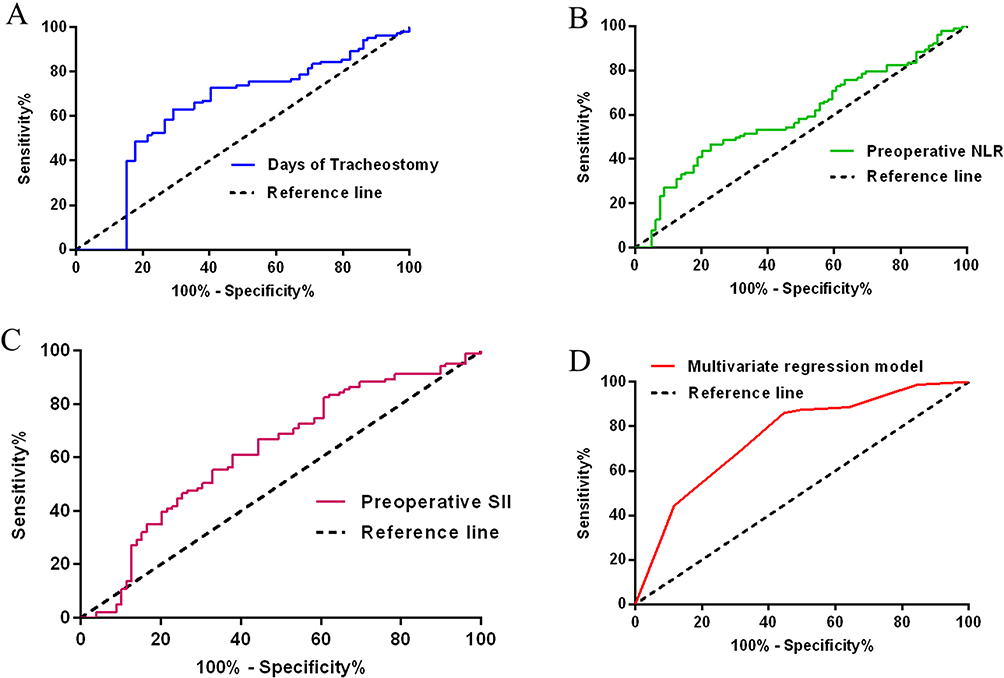 |
Figure 2 Receiver operating characteristic curves of tracheotomy duration (A), NLR at admission (B), SII at admission (C), and the multivariate logistic regression model (D) for predicting pneumonia due to multidrug-resistant A. baumanni. |
The variables included in the multivariate logistic regression analysis were GCS score, duration of urinary catheter, central venous catheterization, tracheotomy, gastric tube, and antibiotics, NLR and SII levels at admission. The AUC of multivariate logistic regression model was 0.755 (95% CI: 0.685–0.826, Youden index = 0.414, p < 0.001). The sensitivity and specificity were 86.1% and 55.3%, respectively (Figure 2D). The result of multivariate logistic regression analysis showed that SII level (≥1851.91 × 109/L) (OR: 3.494, 95% CI: 1.749–6.978, P < 0.001), tracheotomy duration (≥6 days) (OR: 4.209, 95% CI: 2.145–8.261, P < 0.001) and GCS score (<11) (OR: 3.176, 95% CI: 1.450–6.956, P = 0.004) were risk factors for pneumonia due to MDR A. baumannii (Figure 3).
 |
Figure 3 Forest plot of the multivariate logistic regression model. |
Discussion
Our research demonstrated that tracheotomy duration, GCS score and SII level at admission could be associated with pneumonia due to MDR A. baumannii. The GCS score reflects eye opening response, language response, and limb movement in patients with cerebral hemorrhage. GCS score was considered to be associated with prognosis of patients with cerebral hemorrhage.20 Lower GCS score also possibly increased the incidence of acute kidney injury, gastrointestinal bleeding, and pneumonia in patients with cerebral hemorrhage.1,20,21 The association of lower GCS score with pneumonia due to MDR A. baumannii in our study may originate from disorders of consciousness. In addition, our study also confirmed the association of longer tracheotomy duration with pneumonia due to MDR A. baumannii. The opening of respiratory tract caused by tracheotomy may become one of the pathways for pathogen invasion. However, the two factors of GCS score and tracheotomy duration are largely static in nature, lacking the ability to reflect the patient’s dynamic immune-inflammatory status.
So we specifically explored the relationship between inflammatory markers at different time points and pneumonia due to MDR A. baumannii in the study. The results confirmed the relationship between SII at admission and pneumonia due to MDR A. baumannii. SII is a comprehensive reflection of the levels of neutrophils, lymphocytes, and platelets, and reflects the balance of inflammation and immunity in the body. SII has shown important clinical relevance and predictive value in various infections and pneumonia related diseases. In different infection models such as diabetes foot infection, urinary tract infection and chronic kidney disease patients with COVID-19, SII also showed significant diagnostic and prognostic differentiation ability, which can effectively identify infection severity, organ involvement risk and hospital death probability.22–24 In addition, researches have shown that elevated levels of SII were independently associated with poor prognosis (such as increased risk of long-term mortality) in patients with stroke associated pneumonia and severe community-acquired pneumonia. Its predictive performance can be enhanced by combining it with traditional scoring systems or with prognostic nutritional index.25–27 These pieces of evidence collectively indicate that SII is an easily accessible and widely applicable inflammatory biomarker that can aid in early risk stratification and prognostic assessment of patients with infections and related pulmonary complications.
The relationship between SII and pneumonia due to MDR A. baumannii could be attributed to inflammatory response. The relationship between inflammatory response and MDR infection has been confirmed in other studies. Patients with catheter-related bloodstream infections caused by MDR bacteria had a higher procalcitonin level and a longer time for the procalcitonin level to return to normal than patients with infections caused by sensitive bacteria.28 Procalcitonin is associated with systemic inflammatory response in bacterial infection. This study implied a stronger inflammatory response in patients with MDR bacterial infections. Moreover, MDR bacterial infections are difficult to control, and the inflammatory response may persist, which could lead to prolonged high levels of inflammatory markers. In patients with MDR A. baumannii infection, the inflammatory response also may be stronger. Neutrophils played an important role in drug-resistant A. baumannii respiratory infections.29 The inflammatory response is significantly altered after a stroke. For example, interleukin-6 and C-reactive protein can serve as predictors of outcome in stroke patients.30,31 Additionally, the activation of the sympathetic nervous system following a stroke may mediate systemic immunosuppression, which in turn contributes to an increased risk of infection.32,33
In our research, the relationship between SII and MDR A. baumannii infection was confirmed, indicating a stronger inflammatory response or immune suppression in patients with stroke. Higher SII possibly indicated excessive inflammatory response or immune imbalance, which was associated with the risk of MDR A. baumannii. So SII could serve as a rapid, economical biomarker to help assess the risk of pneumonia due to MDR A. baumannii, further providing a new perspective for the drug-resistant mechanism of bacteria, helping to guide individualized anti-infection and immunomodulatory therapy. However, the correlation between elevated SII levels and MDR A. baumannii pneumonia is worth noting, which may be influenced by other confounding factors. For example, patients with greater bleeding may have more severe systemic inflammatory responses. It is worth acknowledging that the clinical model based on the duration of tracheotomy, lower GCS score and higher SII showed the highest predictive performance, with an AUC value of 0.755, significantly better than the model using any single predictive factor. But in the end, the AUC value of this model was not high enough.
This study has several limitations. First, the inclusion of only patients who underwent surgical treatment rather than all patients with intracerebral hemorrhage introduced significant selection bias. This severely limited the generalizability of the study findings. Second, the sample size of MDR A. baumannii infections was small, which possibly reduced the statistical power and missed weak but important associations. Third, this study did not compare SII with other inflammatory markers including procalcitonin, interleukin-6 and C-reactive protein. Future studies will expand the sample size through a multicenter, prospective design, and validate the combination of SII with other inflammatory markers.
Conclusion
Our study revealed a possible correlation of longer duration of tracheotomy, lower GCS score and higher SII at admission with the risk of MDR A. baumannii pneumonia, providing valuable predictive clues for early identification of high-risk patients. However, its core value lies in enabling “early risk warning” rather than directly guiding treatment decisions. It must be emphasized that the model currently only reveals a statistical association, and its clinical applicability must be validated through prospective, multi-center studies. External validation studies are also needed. Before obtaining high-level evidence support, we recommend using the model prediction results as a trigger to initiate a comprehensive prevention and control plan. Once a patient is identified as high-risk, microbiological specimen testing, strictly implementing contact isolation and environmental disinfection, strictly reviewing and implementing Ventilator-Associated Pneumonia bundling strategies, early removal of non essential invasive devices, and clinical sign monitoring are very necessary.
Data Sharing Statement
The data which was used and/or analyzed during this study is available from the corresponding author (Jie Min) on reasonable request.
Ethics Approval and Informed Consent
The study was approved by and complied with the requirements of the Ethics Committee of the First Affiliated Hospital of Yangtze University (KY2025-022-01). The Ethics Committee waived the requirement for patient informed consent due to the nature of retrospective study. The confidentiality of information was protected according to the Helsinki Declaration.
Acknowledgments
We are thankful to all the medical staff in the Neurointensive Care Unit and the department of Neurosurgery, The First Affiliated Hospital of Yangtze University.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xue LY, Gaowa S, Wang W, et al. Ventilator-associated pneumonia in patients with cerebral hemorrhage: impact on mortality and microbiological characterization. Med Clin. 2020;154(10):400–10. doi:10.1016/j.medcli.2020.01.003
2. Chang L, Dong Y, Zhou P. Investigation on risk factors of ventilator-associated pneumonia in acute cerebral hemorrhage patients in intensive care unit. Can Respir J. 2017;2017:7272080. doi:10.1155/2017/7272080
3. Heuschmann PU, Kolominsky-Rabas PL, Misselwitz B, et al. Predictors of in-hospital mortality and attributable risks of death after ischemic stroke: the german stroke registers study group. Arch Intern Med. 2004;164(16):1761–1768. doi:10.1001/archinte.164.16.1761
4. Koennecke HC, Belz W, Berfelde D, et al. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology. 2011;77(10):965–972. doi:10.1212/WNL.0b013e31822dc795
5. Zhou H, Yang Q, Yu YS, et al. Clonal spread of imipenem-resistant acinetobacter baumannii among different cities of China. J Clin Microbiol. 2007;45(12):4054–4057. doi:10.1128/JCM.00343-07
6. Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev. 2008;21(3):538–582. doi:10.1128/CMR.00058-07
7. Fournier PE, Richet H, Weinstein RA. The epidemiology and control of Acinetobacter baumannii in health care facilities. Clin Infect Dis. 2006;42(5):692–699. doi:10.1086/500202
8. Dijkshoorn L, Nemec A, Seifert H. An increasing threat in hospitals: multidrug-resistant Acinetobacter baumannii. Nat Rev Microbiol. 2007;5(12):939–951. doi:10.1038/nrmicro1789
9. Mohd Sazlly Lim S, Zainal Abidin A, Liew SM, et al. The global prevalence of multidrug-resistance among Acinetobacter baumannii causing hospital-acquired and ventilator-associated pneumonia and its associated mortality: a systematic review and meta-analysis. J Infect. 2019;79(6):593–600. doi:10.1016/j.jinf.2019.09.012
10. Munoz-Price LS, Weinstein RA. Acinetobacter infection. N Engl J Med. 2008;358(12):1271–1281. doi:10.1056/NEJMra070741
11. Alsumrain M, Melillo N, Debari VA, et al. Predictors and outcomes of pneumonia in patients with spontaneous intracerebral hemorrhage. J Intensive Care Med. 2013;28(2):118–123. doi:10.1177/0885066612437512
12. Huang Q, Zhou Q, Ju T, et al. Meropenem and amikacin for management of post-neurosurgical infections from Acinetobacter baumannii. Surg Infect. 2019;20(4):292–297. doi:10.1089/sur.2018.242
13. Lan M, Dongmei K, Guodong S, et al. Risk factors for bacteremic pneumonia and mortality (28-day mortality) in patients with Acinetobacter baumannii bacteremia. BMC Infect Dis. 2024;24(1):448. doi:10.1186/s12879-024-09335-8
14. Garnacho-Montero J, Ortiz-Leyba C, Fernández-Hinojosa E, et al. Acinetobacter baumannii ventilator-associated pneumonia: epidemiological and clinical findings. Intensive Care Med. 2005;31(5):649–655. doi:10.1007/s00134-005-2598-0
15. Wang Z, Huang Y, Liu X, et al. Development of a model to predict the risk of multi-drug resistant organism infections in ruptured intracranial aneurysms patients with hospital-acquired pneumonia in the neurological intensive care unit. Clin Neurol Neurosurg. 2024;246:108568. doi:10.1016/j.clineuro.2024.108568
16. Vasudevan A, Mukhopadhyay A, Li J, et al. A prediction tool for nosocomial multi-drug resistant gram-negative bacilli infections in critically ill patients - prospective observational study. BMC Infect Dis. 2014;14(1):615. doi:10.1186/s12879-014-0615-z
17. Wang RH, Wen WX, Jiang ZP, et al. The clinical value of neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR) and systemic inflammation response index (SIRI) for predicting the occurrence and severity of pneumonia in patients with intracerebral hemorrhage. Front Immunol. 2023;14:1115031. doi:10.3389/fimmu.2023.1115031
18. Yu T, Liu H, Liu Y, et al. Inflammatory response biomarkers nomogram for predicting pneumonia in patients with spontaneous intracerebral hemorrhage. Front Neurol. 2023;13:1084616. doi:10.3389/fneur.2022.1084616
19. Shi Y, Huang Y, Zhang TT, et al. Chinese guidelines for the diagnosis and treatment of hospital-acquired pneumonia and ventilator-associated pneumonia in adults (2018 Edition). J Thorac Dis. 2019;11(6):2581–2616. doi:10.21037/jtd.2019.06.09
20. Wang Q, Li S, Sun M, et al. Systemic immune-inflammation index may predict the acute kidney injury and prognosis in patients with spontaneous cerebral hemorrhage undergoing craniotomy: a single-center retrospective study. BMC Nephrol. 2023;24(1):73. doi:10.1186/s12882-023-03124-2
21. Zou Y, Zhang W, Huang C, et al. Clinical significance of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in acute cerebral hemorrhage with gastrointestinal hemorrhage, and logistic regression analysis of risk factors. Exp Ther Med. 2019;18(3):1533–1538. doi:10.3892/etm.2019.7778
22. Ozer Balin S, Ozcan EC, Uğur K. A new inflammatory marker of clinical and diagnostic importance in diabetic foot infection: systemic immune-inflammation index. Int J Low Extrem Wounds. 2025;24(4):1003–1009. doi:10.1177/15347346221130817
23. Kocaaslan R, Dilli D, Çitli R. Diagnostic value of the systemic immune-inflammation index in newborns with urinary tract infection. Am J Perinatol. 2024;41(S 01):e719–e727. doi:10.1055/s-0042-1757353
24. Ozdemir A, Kocak SY, Karabela SN, et al. Can systemic immune inflammation index at admission predict in-hospital mortality in chronic kidney disease patients with SARS-CoV-2 infection? Nefrologia. 2022;42(5):549–558. doi:10.1016/j.nefroe.2021.09.009
25. Xie M, Yuan K, Zhu X, et al. Systemic immune-inflammation index and long-term mortality in patients with stroke-associated pneumonia. J Inflamm Res. 2023;16:1581–1593. doi:10.2147/JIR.S399371
26. Chen X, Hao L, Zhou Y, et al. Combined systemic immune-inflammation index-prognostic nutritional index score in evaluating the prognosis of patients with severe community-acquired pneumonia. J Inflamm Res. 2025;18:7105–7114. doi:10.2147/JIR.S521440
27. Zheng Z, Yu M, Peng G, et al. Systemic immune inflammation index (SII) and prognostic nutritional index (PNI) associated with prolonged intensive care unit (ICU) stay in patients with pneumonia complicated with respiratory failure. Int J Gen Med. 2025;18:1765–1776. doi:10.2147/IJGM.S510659
28. Huespe I, Prado E, Staneloni I, et al. Cinética de procalcitonina en infecciones causadas por bacterias multirresistentes [Kinetics of procalcitonin in infections caused by multidrug-resistant bacteria]. Medicina. 2020;80(6):599–605.
29. Breslow JM, Meissler JJ, Hartzell RR, et al. Innate immune responses to systemic Acinetobacter baumannii infection in mice: neutrophils, but not interleukin-17, mediate host resistance. Infect Immun. 2011;79(8):3317–3327. doi:10.1128/IAI.00069-11
30. Bustamante A, Sobrino T, Giralt D, et al. Prognostic value of blood interleukin-6 in the prediction of functional outcome after stroke: a systematic review and meta-analysis. J Neuroimmunol. 2014;274(1–2):215–224. doi:10.1016/j.jneuroim.2014.07.015
31. VanGilder RL, Davidov DM, Stinehart KR, et al. C-reactive protein and long-term ischemic stroke prognosis. J Clin Neurosci. 2014;21(4):547–553. doi:10.1016/j.jocn.2013.06.015
32. Prass K, Meisel C, Höflich C, et al. Stroke-induced immunodeficiency promotes spontaneous bacterial infections and is mediated by sympathetic activation reversal by poststroke T helper cell type 1-like immunostimulation. J Exp Med. 2003;198(5):725–736. doi:10.1084/jem.20021098
33. Westendorp WF, Nederkoorn PJ, Vermeij JD, et al. Post-stroke infection: a systematic review and meta-analysis. BMC Neurol. 2011;11(1):110. doi:10.1186/1471-2377-11-110
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prediction of Antibiotic Efficacy in Cerebral Hemorrhage-Associated Pneumonia Using Inflammatory Hematological Indices: A Retrospective Study
Wang X, Yang X, Yao Y, Hu H, Zhao Y, Zhu Z
Journal of Inflammation Research 2025, 18:13763-13772
Published Date: 4 October 2025
Comparison of Two Different Doses of Ampicillin-Sulbactam as Part of Combination Therapy in the Treatment of Multidrug Resistant Acinetobacter baumannii Ventilator Associated Pneumonia: A Randomized Clinical Trial
Niknami E, Alavi Darazam I, Mahboubi A, Shabani M, Salamzadeh J, Sahraei Z
Infection and Drug Resistance 2026, 19:584186
Published Date: 20 February 2026