Back to Journals » ImmunoTargets and Therapy » Volume 15
A Retrospective Study on the Clinical Characteristics and Management of Immune-Related Adverse Events in Gynecologic Cancer Patients Treated with Immune Checkpoint Inhibitors
Authors Xia Y, Gao S, Wei Q, Gu W, Li X ![]() , Qu H
, Qu H
Received 14 September 2025
Accepted for publication 1 January 2026
Published 21 January 2026 Volume 2026:15 566542
DOI https://doi.org/10.2147/ITT.S566542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Yu Xia,1,* Song Gao,1,* Qianxue Wei,1,* Wen Gu,2,* Xiuqin Li,1 Hui Qu1
1Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of Oncology, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiuqin Li, Email [email protected] Hui Qu, Email [email protected]
Purpose: This study aimed to characterize the clinical profile, risk factors, and management of immune-related adverse events (irAEs) in patients with gynecologic cancers treated with immune checkpoint inhibitors (ICIs).
Methods: In this single-center retrospective study, we analyzed data from 626 gynecologic cancer patients who received ICIs at our institution between January 2019 and July 2024. Data on the occurrence, grading, organ involvement, management, and potential risk factors of irAEs were collected and analyzed using binary logistic regression.
Results: Of the 626 patients, 136 (21.7%) developed irAEs. The most commonly affected systems were endocrine (11.7%), cardiac (3.2%), and skin (2.6%). The incidence of grade 1– 2 and grade 3– 4 irAEs was 17.7% and 3.99%, respectively. The median time to irAE onset was 9 weeks (after 3 treatment cycles). Binary logistic regression analysis revealed that anti-PD-1/CTLA-4 bispecific antibody was a significant risk factor for irAEs (OR = 2.874, p < 0.0001), whereas a higher number of treatment cycles and combination immunotherapy regimens were protective factors. Most irAEs were managed with intravenous methylprednisolone daily. No irAE-related deaths occurred.
Conclusion: In this cohort of gynecologic cancer patients receiving ICIs, our findings suggest a considerable prevalence of endocrine and cardiac irAEs and identify several treatment-related factors associated with irAE risk. The results may underscore the potential importance of timely glucocorticoid initiation, and could support the consideration of empirical steroid therapy in critically ill patients when diagnostic confirmation is difficult. These findings point to the potential importance of organ-specific monitoring and provide insights that could inform the development of management strategies for this population.
Keywords: immunotherapy, immune-related adverse events, cardiac toxicity, gynecologic cancer, glucocorticoids, methylprednisolone
Introduction
Immune checkpoint inhibitors (ICIs) have revolutionized cancer therapy,1–5 inducing durable responses across various solid tumors by enhancing antitumor T-cell activity.6 These agents primarily target CTLA-4 and PD-1/PD-L1 pathways, with their applications expanding from initial success in melanoma3 to now encompass gynecologic malignancies.5,7–10
The unique mechanism of ICI-mediated T-cell activation leads to a distinct spectrum of immune-related adverse events (irAEs)11,12 that differ fundamentally from conventional chemotherapy toxicities. Since T-cell are ubiquitous, irAEs can affect virtually any organ system,12–15 with incidence and severity influenced by both drug class and tumor type. Epidemiological data show that CTLA-4 inhibitors are associated with higher rates of severe (grade 3/4) irAEs than PD-1/PD-L1 agents (31% vs 10%).16 In contrast, PD-1 blockade is more frequently linked to pneumonitis and endocrine dysfunction.
Despite established knowledge of irAE patterns in melanoma and lung cancers, a significant gap exists in gynecologic oncology. Current literature lacks comprehensive, real-world characterization of irAE profiles specific to endometrial and cervical cancer patients receiving ICIs. This is particularly relevant given the unique tumor microenvironment and antigenic landscape of gynecologic malignancies.
To address this gap, we conducted a detailed analysis of irAE characteristics in gynecologic cancer patients treated with ICIs at our institution. This study aims to: (1) define the incidence, spectrum, and timing of irAEs in this population; (2) identify organ-specific patterns distinct from those observed in other tumor types; (3) explore risk factors associated with the development of irAEs; and (4) synthesize management experience to inform clinical practice. Our findings provide novel insights into irAE manifestations in gynecologic cancers and support the development of tailored monitoring and management strategies.
Materials and Methods
Study Design and Patient Characteristics
We conducted a retrospective cohort study at the Department of Gynecologic Oncology, Shengjing Hospital of China Medical University. We enrolled 626 patients with gynecologic cancers who received immune checkpoint inhibitors (ICIs) between January 2019 and July 2024.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows:
- Histologically confirmed cervical, ovarian, vulvar, or vaginal cancer, uterine malignancies, or gestational trophoblastic neoplasia;
- Receipt of at least one cycle of ICI therapy;
- Availability of complete medical records for review.
Patients were excluded from the analysis if they:
- Had a diagnosis of another active malignancy;
- Had inadequate follow-up data;
- Were lost to follow-up within the first month after ICI initiation.
Data Collection Procedures
Data were systematically extracted from electronic medical records through a structured abstraction process. Two independent researchers reviewed all patient records using a standardized data collection form. Collected variables included: (1) demographic and clinical characteristics; (2) ICI treatment details (agent, dosage, frequency, combination therapies); (3) laboratory parameters (complete blood count, liver and renal function tests, thyroid function, cardiac biomarkers, and other organ-specific parameters as clinically indicated); (4) radiological findings; (5) irAE occurrence, including type, severity, and timing; and (6) management strategies and outcomes. Any discrepancies in data abstraction were resolved through consensus with a third senior investigator.
The cohort included patients diagnosed with cervical cancer, uterine malignancies, vulvar cancer, vaginal cancer, and gestational trophoblastic neoplasia. ICI treatment was administered either as monotherapy or in combination with chemotherapy, radiotherapy, or targeted therapy. All patients received at least one cycle of intravenous ICI, with a median follow-up of 19 months (range: 1–52).
Sample Size Consideration
Given the comprehensive nature of our institutional database and the study’s exploratory aim to characterize irAE patterns in gynecologic cancers, we included all eligible patients treated during the specified period rather than conducting a pre-specified power calculation. This approach allowed for maximal capture of irAE events, though we acknowledge that the modest number of irAE cases may limit subgroup analyses. The immunotherapeutic agents included in this study included the following three classes of immune checkpoint inhibitors, namely anti-PD-1 monoclonal antibodies, anti-PD-L1 monoclonal antibodies, and anti-PD-1/anti-CTLA-4 bispecific antibodies.
The collected clinical data encompassed the types of ICIs administered, the incidence and severity of irAEs, the median time to irAE onset, and the median number of treatment cycles. irAEs were categorized based on the affected organ systems and graded according to the Common Terminology Criteria for Adverse Events (CTCAE, version 5.0). Analysis focused on the spectrum, frequency, and severity of irAEs, along with the median time to onset and median number of treatment cycles prior to occurrence. Additionally, we evaluated the management strategies employed for irAEs, their clinical outcomes, and the feasibility of rechallenging with ICIs.
Diagnosis of Immune-Related Adverse Events
The diagnosis of irAEs was based on established clinical guidelines and required a comprehensive assessment to exclude alternative causes before attributing manifestations to immunotherapy. It is crucial to note that clinical diagnosis does not rely on a single immunological biomarker. Detailed diagnostic criteria for specific irAEs are provided in Supplementary Table 1.
The diagnostic assessment incorporated the following key components:
- A temporal association with ICI initiation.
- Exclusion of alternative causes (eg, disease progression, infection, or other drug-related effects).
- A clinical presentation consistent with known irAE phenotypes.
- Supportive diagnostic findings (eg, from laboratory tests, imaging, or histopathology).
- Response to immunosuppressive treatment when applicable.
These criteria were applied in an organ-specific manner. For instance:
- Endocrine irAEs were diagnosed based on characteristic symptom profiles and hormone abnormalities (eg, TSH, free T4, cortisol), after excluding metastases and other causes.
- Cardiac irAEs (eg, myocarditis) required a combination of suggestive symptoms, elevated cardiac biomarkers (troponin, CK-MB), electrocardiographic (ECG) abnormalities, and supportive echocardiographic findings.
For all other irAEs, diagnosis rested upon the consistent application of these core principles: evaluation of organ-specific clinical features, utilization of relevant diagnostic tests, and rigorous exclusion of competing etiologies.
Statistical Analysis
Statistical analyses were performed using SPSS (version 28.0) and GraphPad Prism (version 5.01). Descriptive statistics were used to summarize patient characteristics, with continuous variables presented as median (range) and categorical variables as frequency (percentage).
Independent factors associated with irAE development were identified by multivariable binary logistic regression. The model incorporated age, number of treatment cycles, class of ICI, treatment regimen (monotherapy vs combination), treatment stage, and tumor type as covariates. Categorical variables were appropriately dummy-coded for analysis (eg, with the most common category serving as the reference). The results are presented as adjusted odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Model fit was evaluated by the Likelihood Ratio Test, pseudo-R2 statistics, and the Hosmer-Lemeshow test. Statistical significance was defined as a two-sided p-value < 0.05.
Results
Epidemiology and Clinical Characteristics of irAEs
Incidence Spectrum of irAEs
Among the 626 patients with gynecologic cancers treated with ICIs, the overall incidence of irAEs was 21.7% (136/626). The median age of the entire cohort was 55 years (range: 20–83), and there was no significant difference in age between patients who developed irAEs (58 years; range: 30–80) and those who did not (56 years; range: 20–83; p = 0.348).
IrAEs involved ten organ systems, with the endocrine system being the most frequently affected (11.66%, 73/626). Among endocrine irAEs, hypothyroidism was predominant (61 cases, 83.6%), followed by thyroiditis (n=5), hyperthyroidism (n=3), immune-related diabetes mellitus (n=2, one presenting with ketoacidosis), and adrenal insufficiency (n=2). Notably, two patients with pre-existing autoimmune thyroiditis and normal baseline function developed acute thyroiditis as an irAE.
Cardiac events were the second most common (3.19%, 20/626), with all cases diagnosed as myocarditis. Three of these patients had pre-existing cardiac conditions, including a history of myocardial infarction with stenting (n=2) or atrial arrhythmias (n=1).
The incidence and manifestations of irAEs in other organ systems are summarized in Table 1 and Figure 1:
- Dermatologic: 2.55% (16/626), primarily presenting as cutaneous capillary hyperplasia (n=10) and other cutaneous manifestations (n=6).
- Pulmonary: 1.76% (11/626) with pneumonitis.
- Gastrointestinal: 1.28% (8/626) with colitis.
- Musculoskeletal: 1.12% (7/626) with myositis.
- Hepatic: 0.80% (5/626) with hepatitis.
- Neurological: 0.48% (3/626) with peripheral neuritis.
- Hematological: 0.32% (2/626) with thrombocytopenia.
- Pancreatic: 0.16% (1/626) with pancreatitis.
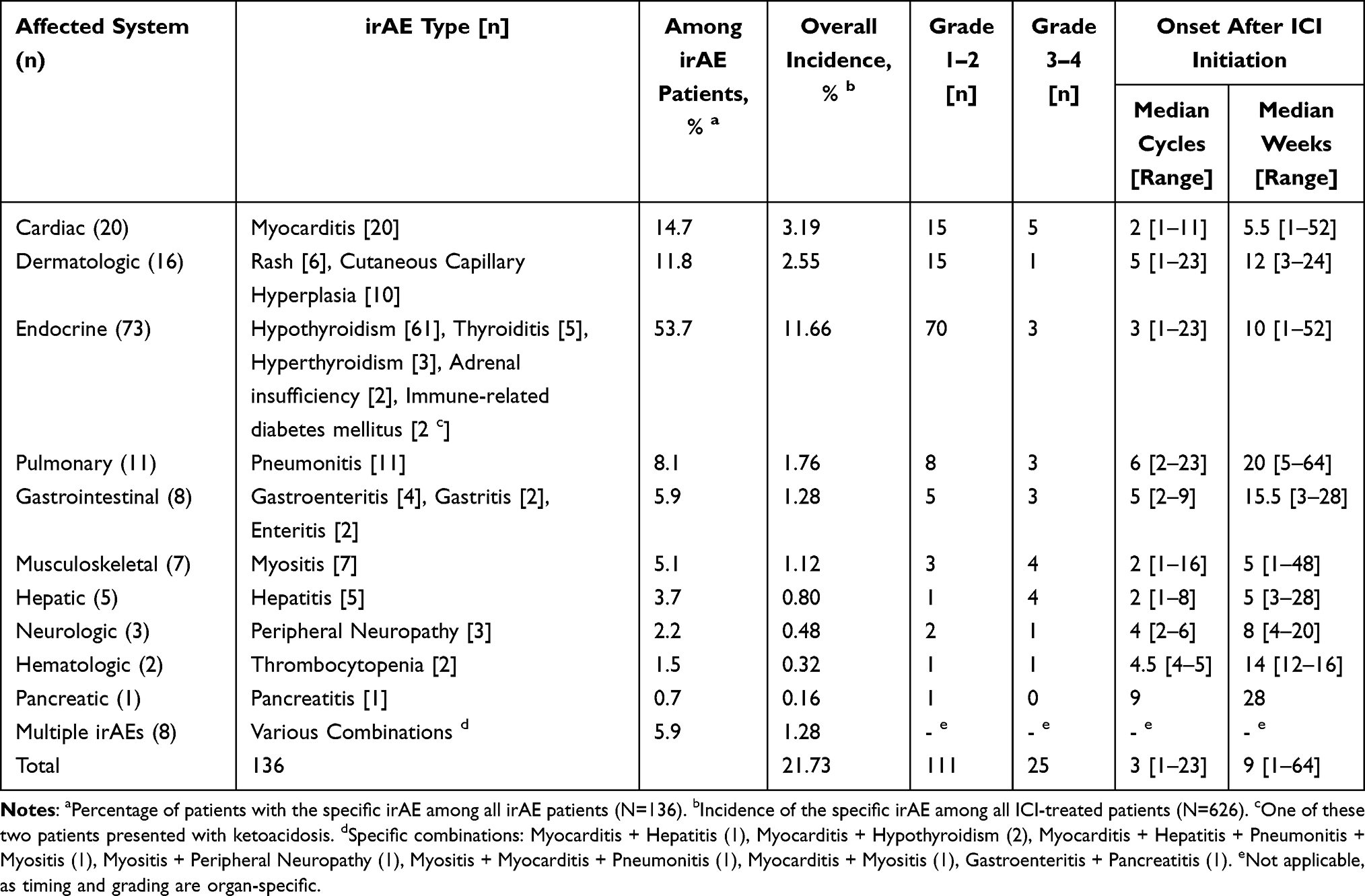 |
Table 1 Spectrum and Characteristics of Immune-Related Adverse Events (irAEs) |
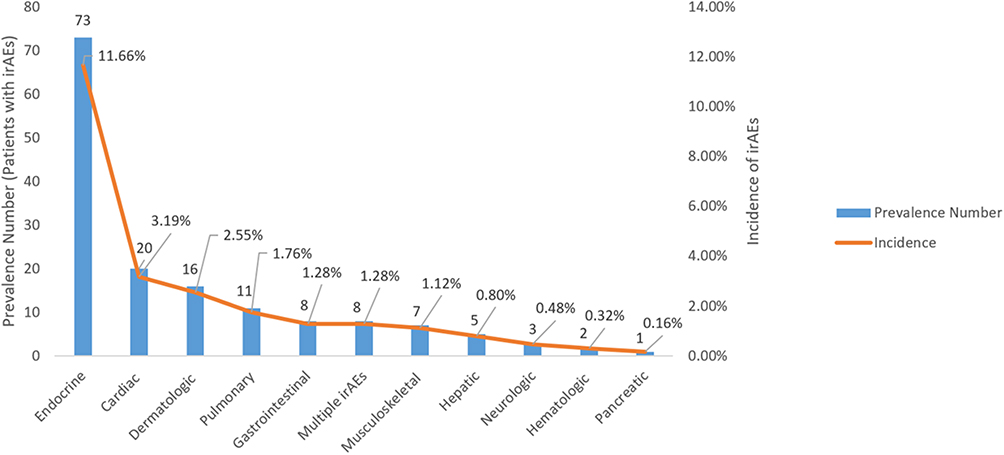 |
Figure 1 Organ-Specific Distribution of irAEs. |
Multi-organ irAEs occurred in eight patients. Representative clinical images, including CT scans and physical findings for pneumonitis, thyroiditis, and dermatological irAEs, are provided in Supplementary Figures 1–6.
Factors Associated with irAE Risk
A total of 626 patients were included in the analysis. Of these, 136 (21.73%) developed immune-related adverse events (irAEs), while 490 (78.27%) did not. Supplementary Table 2 summarizes the incidence of irAEs across different patient subgroups.
To identify factors associated with the risk of irAEs, a binary logistic regression was performed. The overall model was statistically significant (χ2 = 51.440, df = 12, p < 0.0001). The Cox & Snell R2 and Nagelkerke R2 values were 0.079 and 0.122, respectively, indicating that the model explained a partial but limited proportion of the variance. The Hosmer-Lemeshow test indicated a good model fit (χ2 = 13.051, df = 8, p = 0.110). Detailed results of the regression analysis, including coefficients, odds ratios, and confidence intervals for all variables, are presented in Table 2.
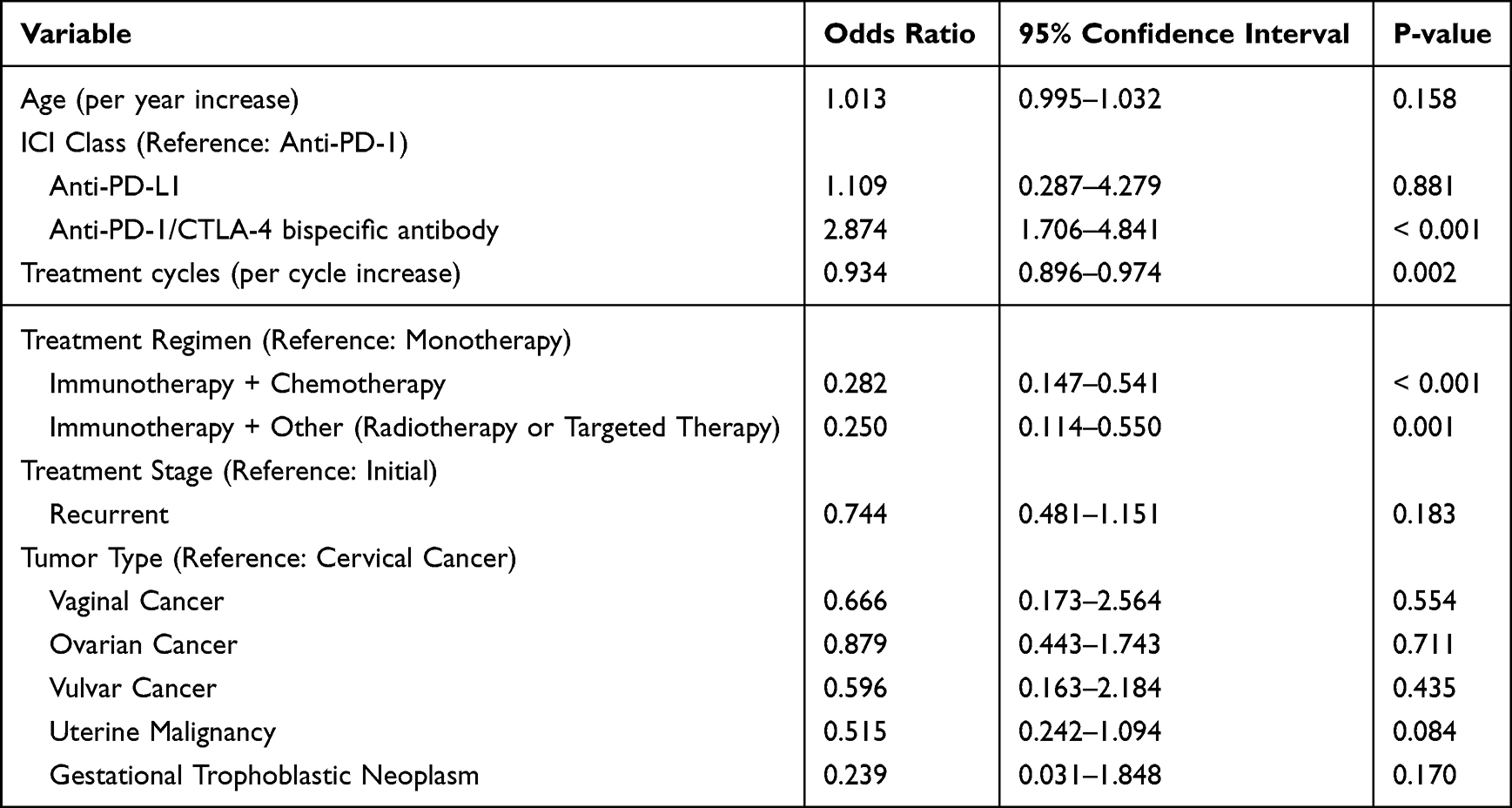 |
Table 2 Multivariable Logistic Regression Analysis of Factors Associated with Immune-Related Adverse Event (irAE) Risk |
In summary, the analysis identified several significant predictors. The use of an anti-PD-1/CTLA-4 bispecific antibody was associated with a significantly increased risk of irAEs (OR = 2.874, 95% CI: 1.706–4.841, p < 0.001) compared to PD-1 inhibitors. Conversely, an increased number of treatment cycles (OR = 0.934, 95% CI: 0.896–0.974, p = 0.002) and treatment with immunotherapy combination regimens—either Immunotherapy + Chemotherapy (OR = 0.282, 95% CI: 0.147–0.541, p < 0.001) or Immunotherapy + Other (OR = 0.250, 95% CI: 0.114–0.550, p = 0.001)—were significant protective factors. No significant associations were found for age, treatment stage, or specific tumor types.
Severity and Time to Onset of irAEs
Among the 626 gynecologic cancer patients treated with ICIs, the overall incidence of irAEs was 21.73%. Grade 1–2 irAEs occurred in 17.73% (111/626) of patients, while grade 3–4 irAEs were observed in 3.99% (25/626). No grade 5 irAE-related fatalities were reported. Of the 136 patients who developed irAEs, 81.62% (111/136) experienced grade 1–2 events, and 18.38% (25/136) had grade 3–4 events. The organ-specific severity distribution of irAEs is detailed in Table 1.
The time to irAE onset varied widely. The median time to irAE onset was 9 weeks (range: 1–64), which corresponded to a median of 3 treatment cycles (range: 1–23), as summarized in Table 1. The longest interval was 64 weeks, observed in a case of pneumonitis. Among the various types of irAEs reported, muscular and hepatic irAEs had the shortest median time to onset, at 5 weeks.
Spectrum and Risk Factors of Cardiac irAEs
Cardiac events represented the second most common category of irAEs, occurring in 3.19% (20/626) of patients, with all cases diagnosed as myocarditis. Of the 20 patients with cardiac events, 15 (75%) were in the combination therapy group (ICI plus chemotherapy). Notably, all 15 of these patients received a taxane-based chemotherapeutic regimen. A subgroup analysis based on ICI type showed a higher incidence of cardiac events in patients receiving anti-PD-1 and anti-CTLA-4 antibodies (5/81, 6.17%) compared to those on anti-PD-1 monotherapy (15/530, 2.83%). Furthermore, the onset of these cardiac events was notably early (median of 2 cycles), preceding the median onset for all irAEs in our cohort (3 cycles). Additionally, 6 of the 20 patients with myocarditis experienced a recurrence of symptoms during corticosteroid taper. Among the 20 patients with myocarditis, three patients had pre-existing cardiac conditions: two with a history of myocardial infarction and stenting, and one with frequent atrial premature contractions and brief episodes of atrial tachycardia.
Management Strategies for irAEs
Apart from specific endocrine immune-related adverse events (such as thyroid hormone replacement therapy for hypothyroidism), all other types of immune-related adverse events (irAEs) are primarily managed with glucocorticoids as first-line treatment (Table 3). Among glucocorticoid agents, methylprednisolone is the preferred clinical choice. Dosage regimens are strictly determined in accordance with authoritative domestic and international guidelines, including relevant management consensus and guidelines issued by the Toxicity Management Working Group of the Society for Immunotherapy of Cancer (SITC).
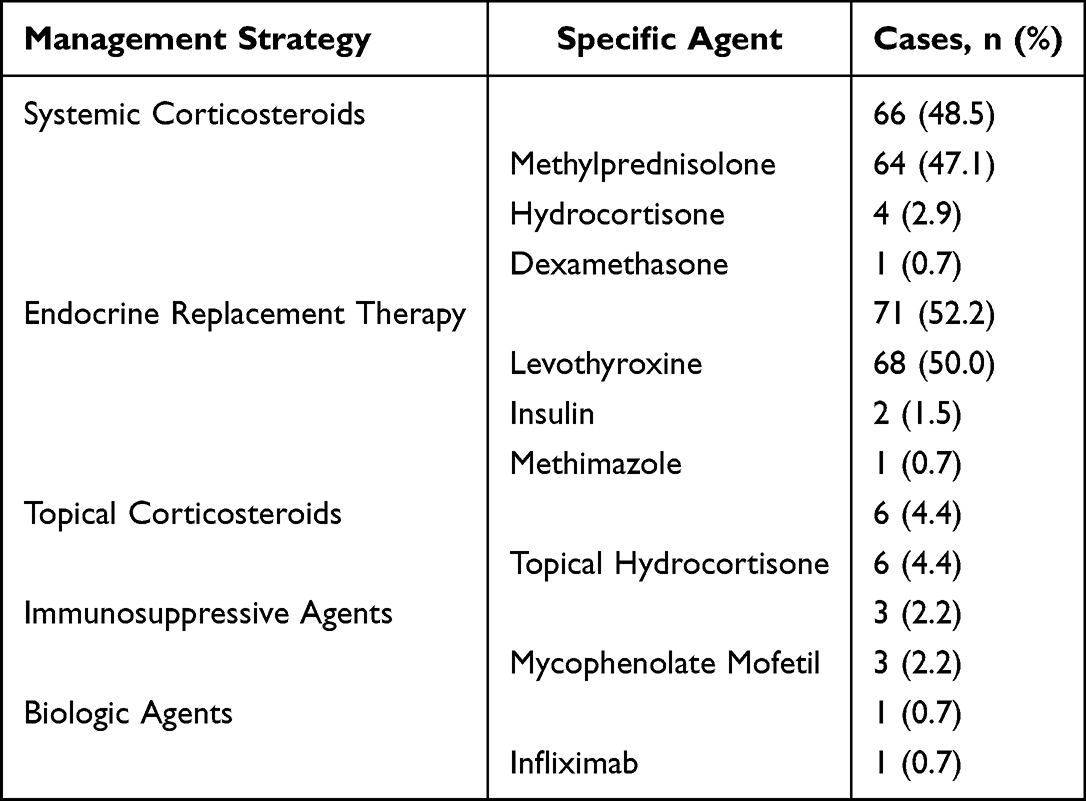 |
Table 3 Management Strategies for Immune-Related Adverse Events (N=136) |
Outcomes of irAEs and ICI Rechallenge
Among the 136 patients who developed irAEs, 126 achieved complete recovery after treatment, including 20 who experienced transient clinical worsening during therapy but eventually attained complete resolution. Seven patients were still undergoing active treatment for their irAEs at the time of analysis. Three patients discontinued treatment and were discharged from the hospital after the onset of irAEs. Five patients required admission to the intensive care unit (ICU) due to severe irAEs; all were successfully treated with high-dose intravenous methylprednisolone and discharged. All five of these ICU patients had myocarditis, with one case presenting as part of a multi-organ involvement syndrome (which also included pneumonia, myositis, and hepatitis). A detailed analysis of the five patients with myocarditis who required ICU admission revealed a distinct and severe clinical phenotype. These events occurred early in the treatment course, after a median of 2 cycles of immunotherapy. All patients presented with a dramatic elevation in cardiac biomarkers. All five cases were high-grade (Grade 3–4) adverse events, and all exhibited hemodynamic involvement, including arrhythmias or impaired left ventricular function. No deaths were observed in this study.
ICI rechallenge was performed in nine patients (6.62%), all of whom had experienced initial irAEs of grade 1–2 severity. Upon rechallenge, one patient experienced a recurrence of myocarditis.
Discussion
The expanding indications for immune checkpoint inhibitors (ICIs) have firmly established their role in the first-line treatment of gynecologic cancers, particularly cervical and endometrial cancer. This increasing utilization has consequently heightened the clinical focus on the management of irAEs, making their identification, management, and monitoring a critical aspect of clinical practice. As a retrospective observational study, we aimed to characterize the clinical landscape and management of irAEs in a real-world cohort of gynecologic cancer patients, thereby generating hypotheses for future research.
IrAEs are notably characterized by their highly individualized manifestations, clinical complexity, and unpredictability. To address the challenges these features pose and to optimize patient outcomes, we conducted a detailed retrospective analysis of patients who developed irAEs at our institution.
The Landscape of irAEs in Gynecologic Cancers
Incidence and Associated Factors of irAEs in Gynecologic Cancer
Previous studies have reported a broad spectrum of incidence rates for irAEs associated with immune checkpoint inhibitors (ICIs). The overall incidence of irAEs ranges from 29% to 43.3%.17–21 Specifically, irAEs related to PD-1 antibodies occur in approximately 18.49% to 20% of cases, whereas CTLA-4 antibodies are associated with a higher incidence—exceeding 75% in some studies.22 Moreover, the incidence of severe irAEs (grade 3–4) is significantly greater with CTLA-4 antibodies (ranging from 34% to 41.6%) compared to PD-1/PD-L1 inhibitors (less than 20%).17,18,23–25 These variations in reported incidence rates may arise from differences in ICI regimens, tumor types, patient characteristics, and study designs. These factors collectively complicate the accurate estimation of irAE incidence and epidemiological profiles in clinical trials.23 The observed variations in reported incidence rates may be attributed to differences in the types of ICIs administered, tumor types, patient demographics, and study designs. These factors collectively pose challenges for deriving accurate incidence rates and reliable epidemiological data on irAEs from clinical trials. In this study, the overall incidence of irAEs among gynecologic cancer patients was 21.73%, which is comparatively lower than certain previously reported figures. Specifically, the incidence of grade 1–2 irAEs in this study was 17.73%, which is lower than the approximately 40.0% reported in the literature, while the incidence of grade 3–4 events was 3.99%, consistent with the reported grade 3–5 incidence of approximately 3.0% in existing literature.19,26–28 Overall, the total incidence of irAEs identified in this study remains lower than that documented in several other studies.
This study serves as a preliminary exploratory analysis aimed at identifying clinical factors potentially associated with the risk of irAEs. Using binary logistic regression, we observed several suggestive associations. These descriptive findings provide initial clues and direction for further investigation but do not establish definitive causal relationships. The most pronounced finding was the strong association between the use of an anti-PD-1/CTLA-4 bispecific antibody and an elevated risk of irAEs (OR=2.874). We speculate that this observation aligns with the pharmacological rationale for immune checkpoint inhibitors, whereby simultaneous blockade of both PD-1 and CTLA-4 pathways is likely to induce more robust T-cell activation. This finding places our results in the context of prior knowledge, as substantial evidence has established that combination therapy with separate PD-1 and CTLA-4 inhibitory antibodies carries a higher toxicity profile than PD-1 inhibitor monotherapy.4,29–31 However, as an exploratory analysis, this study cannot definitively establish causality, and unmeasured confounding factors (eg, differences in patient selection, tumor burden, or pre-existing conditions) may have influenced the results. Nonetheless, this key finding provides an important descriptive signal for clinicians, highlighting the need for heightened vigilance and proactive management when using this potent class of therapeutics.
Conversely, our analysis suggested potential protective associations that warrant careful scrutiny. The observed inverse relationship between the number of treatment cycles and irAE risk (OR=0.934) aligns with reports from large studies indicating that most irAEs occur during the initial phases of treatment.32,33 A plausible explanation for this is the “survivor cohort” effect, whereby patients who are less tolerant of therapy or prone to irAEs discontinue treatment early, leaving a population receiving more cycles that is inherently at lower risk for subsequent irAEs.32 Alternatively, this phenomenon might reflect dynamic adaptations of the immune system, where persistent antigen exposure could potentially lead to immune tolerance, reducing the propensity to attack normal tissues.34 Thus, this association likely reflects the combined effect of a selected patient population and potential immune adaptation.
Similarly, the notably lower irAE risk associated with immunotherapy combination regimens—both with chemotherapy (OR=0.282) and with radiotherapy/targeted therapy (OR=0.250)—is a compelling finding. This counterintuitive observation may stem from multiple factors. From a biological perspective, certain chemotherapeutic agents are not merely immunosuppressive but can “remodel” the tumor immune microenvironment, for instance by depleting immunosuppressive cells, potentially directing immune attack more specifically toward the tumor rather than normal tissues.35 Likewise, radiotherapy, as a localized modality, might help guide the immune response more specifically against the tumor.36 However, when interpreting these results, potential confounding must be rigorously considered. Large retrospective analyses have confirmed that poorer baseline performance status (ECOG PS) is an independent risk factor for severe irAEs.16 In clinical practice, patients with better performance status and potentially lower tumor burden are typically selected for aggressive combination therapies. Therefore, the observed associations are likely significantly influenced by this “patient selection bias”16 Future prospective studies or meticulously designed analyses using propensity score matching are needed to discern whether this protective effect truly stems from the treatment modality itself or from the characteristics of the selected patient population.
It is noteworthy that factors such as age, treatment stage, and specific tumor types did not show significant associations with irAE risk in our dataset. This might suggest that the specific therapeutic agents and regimens themselves are more influential determinants, but it could also reflect limitations of our study, such as sample size, population heterogeneity, or other unmeasured variables.
Our model identified several meaningful and significant influencing factors, but it falls short of encompassing all causes contributing to the occurrence of irAEs. The limited explanatory variance (as indicated by the R2 values) is a common characteristic of exploratory studies in this field and helps define the current boundaries of our understanding. In summary, the value of this study lies in its preliminary description of potential factors associated with irAE risk using existing clinical data, identifying several signals worthy of attention. These findings do not provide conclusive answers but lay the groundwork for subsequent, more targeted prospective studies or research integrating multi-omics data to more comprehensively elucidate the mechanisms underlying irAEs.
Types of irAEs in Gynecologic Cancer
The mechanism of immune checkpoint inhibitors (ICIs) involves activating T cells to target and eliminate tumor cells. However, this activation can also trigger irAEs due to off-target bystander effects or the presence of antigens shared between tumor and normal tissues.37,38 Since T cells are distributed throughout all tissues and organs, irAEs have the potential to affect virtually any organ system. irAEs are generally classified into two categories: common toxicities—affecting the skin, gastrointestinal tract, endocrine system, lungs, and musculoskeletal system—and less frequent toxicities involving the cardiovascular system, liver, blood, kidneys, nervous system, and eyes.12,39 The specific T cell subsets (CD4+/CD8+) targeted by different ICIs can influence both the incidence and organ distribution of irAEs. For example, a large meta-analysis revealed that colitis and hypophysitis occur more frequently with CTLA-4 inhibitors, while diabetes and pneumonia are more commonly associated with anti-PD-1/PD-L1 agents.18 In melanoma patients, gastrointestinal and cutaneous toxicities are more prevalent, whereas pneumonia is relatively uncommon. However, reports specifically addressing irAEs in gynecologic cancers remain limited.
In this study, we analyzed 136 gynecologic cancer patients who developed irAEs. The most frequently affected organ system was the endocrine system (11.66%), which is consistent with existing guidelines. Among endocrine irAEs, thyroid dysfunction was the most common, primarily presenting as hypothyroidism. Thyroiditis and hyperthyroidism frequently progress to hypothyroidism over time, which aligns with previous literature reports.33,40–42 This distinctive susceptibility is determined by a confluence of unique anatomical, molecular, and immunological features specific to the thyroid. Firstly, the thyroid is one of the most highly vascularized organs in the human body per unit mass. This rich blood supply provides an efficient conduit for the trafficking and infiltration of activated T cells into the thyroid parenchyma, facilitating immune attack. Secondly, the constitutive expression of relatively high levels of PD-L1 on thyroid cells serves as a key molecular basis for its targeting.43 Finally, the thyroid possesses highly specific autoantigens, primarily thyroid peroxidase and thyroglobulin. The exposure of these antigens to the immune system, followed by their recognition by activated T cells, leads to a destructive thyroiditis.44
In this study, two patients diagnosed with thyroiditis tested positive for anti-thyroid antibodies prior to ICI initiation. Pre-existing anti-thyroid antibodies prior to ICI treatment have been linked to an increased risk of developing thyroid irAEs.45,46 Other frequently observed endocrine irAEs included secondary adrenal insufficiency and diabetes.30,39 Notably, ICI-induced diabetes may present as diabetic ketoacidosis. Although endocrine irAEs can generally be managed with hormone replacement and symptomatic therapy, baseline screening for endocrine abnormalities—beyond thyroid function tests—is not routinely performed in all patients. Moreover, empirical glucocorticoid treatment for suspected irAEs may confound subsequent endocrine test results, thereby complicating the diagnostic process.
In this study, we also observed irAEs involving critical organs, including multi-organ dysfunction, myocarditis, pneumonia, colitis, hepatitis, and rare instances of pancreatitis. No fatal outcomes were reported. Through ongoing clinical reflection, we have identified several critical aspects for managing patients and irAEs during ICI treatment.
Detailed Analysis of Cardiac irAEs
In our cohort, cardiac irAEs emerged as the second most common type (3.19%) in our cohort, accounting for 14.70% of all irAE cases (20/136). This incidence, with a mean time to onset of 5.5 weeks, notably diverges from guideline-based expectations which estimate such events to be relatively uncommon (less than 1%).47 This finding underscores the significant clinical burden of cardiac irAEs in the gynecologic oncology population. Several key observations from our analysis merit emphasis. First, the association observed between myocarditis and combination immunochemotherapy, particularly taxane-based regimens, suggests a potential synergistic toxicity; taxanes are known to have cardiovascular effects, and their combination with ICIs may potentially precipitate an exaggerated inflammatory response in the myocardium. Second, the markedly higher incidence with anti-PD-1/CTLA-4 bispecific antibodies compared to anti-PD-1 monotherapy aligns with the established paradigm that enhanced T-cell activation from combined immune checkpoint blockade increases the risk of severe irAEs.48
Furthermore, our data highlight substantial clinical challenges. The recurrence of myocarditis in a subset of patients (6/20) despite standard corticosteroid treatment is particularly concerning. The challenge of recurrence calls for further investigation into the mechanisms of irAE persistence and more robust treatment protocols. Additionally, the onset of these severe cardiac events was notably early (median of 2 cycles). This early onset (median of 2 cycles) is consistent with previous reports of ICI-related myocarditis48,49 and highlights the initial treatment period as being of particular risk for cardiotoxicity. Given that cardiac toxicity represents the second most common cause of fatal irAEs, maintaining a high level of clinical vigilance is imperative. Early symptoms may be nonspecific, yet significant elevations in cardiac enzymes and troponin I levels are often detectable Consistent with the observational design of our study, the relationships discussed here indicate association rather than causation.
In our limited cohort of severe myocarditis cases requiring ICU admission, the observed clinical presentation generally included early onset following immunotherapy initiation, markedly elevated cardiac biomarkers, high-grade severity, and hemodynamic compromise. Drawing from our experience and supported by existing literature on high-risk ICI-myocarditis,49 this constellation of features could potentially be regarded as clinically significant indicators warranting enhanced suspicion. We suggest that the emergence of such features might reasonably prompt consideration of intensified monitoring and earlier implementation of interventional measures, which could contribute to mitigating the risk of adverse outcomes.
Management of irAEs: Insights from a Descriptive Study
The following management recommendations are derived from our retrospective clinical experience and descriptive analysis. They represent practical approaches formulated in response to the irAE patterns observed in our cohort, rather than protocols validated by prospective or controlled studies.
Patient and Healthcare Provider Education
The unpredictable nature and potential severity of irAEs present considerable challenges in clinical practice. Since irAEs can involve virtually any tissue or organ, many healthcare providers—including internists and emergency physicians—may lack sufficient experience or knowledge to promptly recognize and manage these complications. Strict adherence to conventional examination and diagnostic pathways may delay the timely initiation of appropriate irAE-directed therapy, which can in turn lead to serious clinical outcomes.
Literature reports emphasize that the time interval between symptom onset and the initiation of treatment for irAEs is critical for patient outcomes. Studies have shown that patients who receive glucocorticoid therapy within 5 days of symptom onset exhibit improved prognosis. It is recommended that the time from emergency department presentation to glucocorticoid administration should not exceed 12 hours. Delays in treatment—particularly when the interval from symptom onset to glucocorticoid initiation exceeds 5 days—may significantly compromise final treatment efficacy.50,51
Therefore, enhancing awareness of irAEs among medical staff is critically important.52 Oncology teams should receive targeted training to improve their ability to recognize and manage these adverse events, including identifying early signs and symptoms of irAEs and initiating timely treatment. Equally essential is patient education. Patients and their families should be advised that any new or worsening symptoms occurring during immune checkpoint inhibitor (ICI) therapy must be reported promptly to their primary oncology team, rather than first seeking evaluation in other specialty clinics. The treating oncologist can then assess whether the symptoms are irAE-related and coordinate multidisciplinary consultations as needed. This strategy helps prevent treatment delays caused by a lack of familiarity with irAEs among non-oncology specialists.
Baseline Assessment Before ICIs Administration
A comprehensive evaluation of the patient’s medical history and biochemical profile is essential prior to initiating immune checkpoint inhibitor (ICI) therapy. This assessment should include a detailed review of any subclinical immune-related abnormalities observed in biochemical tests—such as thyroiditis, rheumatoid arthritis, and other autoimmune disorders—as these conditions have been reported in the literature to potentially increase the risk of immune-related adverse events (irAEs) during ICI treatment.
Clear and thorough communication with the patient and their family is imperative. They should be adequately informed about the potential risks of complications or irAEs associated with pre-existing conditions. Obtaining informed consent from both the patient and their family is mandatory before commencing ICI treatment. This process ensures that healthcare providers and patients share a clear understanding of the potential benefits and risks involved in ICI therapy.
Standardized Monitoring and Timely Glucocorticoid Intervention
Standardized biochemical monitoring should be performed before each administration of immune checkpoint inhibitors (ICIs), especially when ICIs are used in combination with chemotherapy or targeted therapies. Any new or atypical symptoms that differ from those typically observed in previous treatment cycles should be promptly evaluated as potential immune-related adverse events (irAEs). Given the diverse and nonspecific clinical manifestations of irAEs, maintaining a high level of vigilance is essential to facilitate early detection and intervention.
In cases of severe involvement of critical organs—such as the heart or lungs—where the diagnosis remains uncertain, empirical glucocorticoid therapy at an appropriate dose should be initiated without delay. This strategy serves two key purposes:
Halting Immune-Mediated Organ Damage
If the manifestations are confirmed to be irAEs, early glucocorticoid intervention can promptly suppress immune-mediated injury, thereby reducing the risk of irreversible organ damage.
Supporting Diagnostic Confirmation
If clinical symptoms improve rapidly following glucocorticoid administration, this response can serve as an important diagnostic indicator, supporting the recognition of irAEs.
Institutional Experience with Glucocorticoid Management of irAEs
In this study, intravenous methylprednisolone served as the cornerstone of irAE management, and no irAE-related fatalities were observed. Based on our descriptive findings, our clinical experience with glucocorticoid therapy is summarized as follows:
Adequate Initial Dosing
The initial glucocorticoid dose must be sufficient to effectively control the irAE. Dosing should be individualized according to the severity (grade) of the irAE and the organ system involved, in accordance with established domestic and international guidelines, such as those provided by the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. Glucocorticoids are typically administered once daily. For grade 3 or 4 irAEs affecting critical organs—such as the heart, lungs, or liver—high-dose methylprednisolone pulse therapy (500–1000 mg) for 3 days is essential to rapidly mitigate immune-mediated damage and prevent clinical deterioration.
Gradual Tapering Regimen
Unlike conventional autoimmune disorders, irAEs often involve more intense and sustained inflammatory responses. Therefore, glucocorticoid tapering should be gradual, with longer maintenance periods at each reduced dosage. The total treatment duration may extend from 4 to 8 weeks or longer. Abrupt or rapid dose reduction increases the risk of irAE recurrence, underscoring the importance of a carefully managed and prolonged tapering schedule.
Management of ICI-Induced Endocrine Dysfunction (Diabetes)
ICI-induced diabetes results from immune-mediated destruction of insulin-secreting beta cells. Therefore, contrary to the management of conventional diabetes, the cornerstone of treatment for this specific irAE is prompt immunosuppression with glucocorticoids to halt the autoimmune attack on pancreatic islets. The goal is to preserve residual beta-cell function and potentially reduce long-term insulin dependence. This approach aims to preserve and recover endogenous insulin secretion, potentially reducing long-term dependence on exogenous insulin. Given the hyperglycemic effects of methylprednisolone and dexamethasone, hydrocortisone may be considered as a preferable alternative in such scenarios due to its milder impact on blood glucose and electrolyte balance.
In summary, the management strategies outlined above are merely a descriptive summary of our institutional practice, stemming from the irAE profile observed in this study. While they suggest potential clinical relevance, their efficacy requires further validation in prospective studies.
Limitations
Although our study offers valuable insights and practical guidance for clinical practice, several limitations should be acknowledged:
1. First, the retrospective and observational design of this study is inherently suited for characterizing the real-world spectrum of irAEs, not for investigating their mechanistic basis. Therefore, the associations between treatment factors and irAEs uncovered here must be interpreted as suggestive and necessitate confirmation through prospective research.
2. Population Specificity: This study was conducted exclusively in a gynecologic cancer population, which may restrict the generalizability of our findings to other cancer types or demographic groups. Future research should evaluate similar interventions in broader and more diverse cohorts to enhance the external validity of the results.
3. Need for Further Research on Cardiac Toxicity: Cardiac toxicity emerged as a notable concern in our analysis. More extensive studies are warranted to refine the identification, diagnosis, and detailed management strategies for this particular irAE. A deeper understanding of its mechanisms and clinical course may lead to improved patient outcomes.
4. Follow-Up Duration: Although the follow-up period was sufficient for assessing primary outcomes, a longer observation time could yield further insights into the long-term effects of both irAEs and their treatments. Extended longitudinal monitoring may help elucidate the sustained impact of immune-related toxicities and the durability of management approaches.
Conclusions
In conclusion, by applying a consistent clinical framework for diagnosis, our study confirms the diverse spectrum of irAEs and underscores that cardiac events represent a more prevalent challenge in our real-world gynecologic oncology cohort than previously documented. Our study preliminarily links irAE risk to specific treatments, such as bispecific antibodies (higher risk) and combination regimens (lower risk). However, these non-causal, exploratory findings require confirmation in future investigations. While most irAEs in this cohort were controlled with guideline-directed glucocorticoid therapy, we noted that refractory cases occasionally required combination with additional immunosuppressive agents—an anomaly that warrants further investigation. The association observed between prompt glucocorticoid intervention and favorable outcomes suggests that vigilant monitoring and early treatment are critical; however, given the observational nature of our data, these therapeutic strategies should be viewed as supportive evidence for established protocols rather than as definitive causal proof.
Therefore, future prospective studies with standardized monitoring are needed to validate these findings, elucidate the underlying biology of irAEs, and inform long-term survivor care.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and ethical restrictions, but are available from the corresponding author (Hui Qu) on reasonable request.
Ethical Approval
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shengjing Hospital of China Medical University (Approval Number: 2024PS1636K). The need for informed consent was waived by the ethics committee due to the retrospective nature of the study and the use of anonymized patient data. All patient information was kept strictly confidential and was used solely for the purposes of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Oliveira G, Wu CJ. Dynamics and specificities of T cells in cancer immunotherapy. Nat Rev Cancer. 2023;23(5):295–15. doi:10.1038/s41568-023-00560-y
2. Sharma P, Allison JP. Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential. Cell. 2015;161(2):205–214. doi:10.1016/j.cell.2015.03.030
3. Ma W, Xue R, Zhu Z, et al. Increasing cure rates of solid tumors by immune checkpoint inhibitors. Exp Hematol Oncol. 2023;12(1):10. doi:10.1186/s40164-023-00372-8
4. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
5. Makker V, Colombo N, Casado Herraez A, et al. Lenvatinib plus pembrolizumab for advanced endometrial cancer. N Engl J Med. 2022;386(5):437–448. doi:10.1056/NEJMoa2108330
6. Lebbe C, Weber JS, Maio M, et al. Survival follow-up and ipilimumab retreatment of patients with advanced melanoma who received ipilimumab in prior Phase II studies. Ann Oncol. 2014;25(11):2277–2284. doi:10.1093/annonc/mdu441
7. Emens LA, Romero PJ, Anderson AC, et al. Challenges and opportunities in cancer immunotherapy: a society for immunotherapy of cancer (SITC) strategic vision. J Immunother Cancer. 2024;12(6):e009063. doi:10.1136/jitc-2024-009063
8. Oaknin A, Tinker AV, Gilbert L, et al. Clinical activity and safety of the anti-programmed death 1 monoclonal antibody dostarlimab for patients with recurrent or advanced mismatch repair-deficient endometrial cancer: a nonrandomized phase 1 clinical trial. JAMA Oncol. 2020;6(11):1766–1772. doi:10.1001/jamaoncol.2020.4515
9. Marabelle A, Fakih M, Lopez J, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, Phase 2 KEYNOTE-158 study. Lancet Oncol. 2020;21(10):1353–1365. doi:10.1016/S1470-2045(20)30445-9
10. Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med. 2021;385(20):1856–1867. doi:10.1056/NEJMoa2112435
11. Molina GE, Zubiri L, Cohen JV, et al. Temporal trends and outcomes among patients admitted for immune-related adverse events: a single-center retrospective cohort study from 2011 to 2018. Oncologist. 2021;26(6):514–522. doi:10.1002/onco.13740
12. Brahmer JR, Abu-Sbeih H, Ascierto PA, et al. Society for immunotherapy of cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2021;9(6):e002435. doi:10.1136/jitc-2021-002435
13. Bonanno L, Lorenzi M, Massa D, et al. Immune-related diarrhea and colitis in non-small cell lung cancers: impact of multidisciplinary management in a real-world setting. Oncologist. 2024;29(1):e118–e30. doi:10.1093/oncolo/oyad238
14. Haanen J, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv264–iv66. doi:10.1093/annonc/mdy162
15. Poto R, Troiani T, Criscuolo G, et al. Holistic approach to immune checkpoint inhibitor-related adverse events. Front Immunol. 2022;13:804597. doi:10.3389/fimmu.2022.804597
16. Khoja L, Day D, Wei-Wu Chen T, et al. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–2385. doi:10.1093/annonc/mdx286
17. Eggermont AM, Chiarion-Sileni V, Grob JJ, et al. Prolonged survival in stage III melanoma with ipilimumab adjuvant therapy. N Engl J Med. 2016;375(19):1845–1855. doi:10.1056/NEJMoa1611299
18. Arnaud-Coffin P, Maillet D, Gan HK, et al. A systematic review of adverse events in randomized trials assessing immune checkpoint inhibitors. Int J Cancer. 2019;145(3):639–648. doi:10.1002/ijc.32132
19. Li L, Li G, Rao B, et al. Landscape of immune checkpoint inhibitor-related adverse events in Chinese population. Sci Rep. 2020;10(1):15567. doi:10.1038/s41598-020-72649-5
20. Maillet D, Corbaux P, Stelmes JJ, et al. Association between immune-related adverse events and long-term survival outcomes in patients treated with immune checkpoint inhibitors. Eur J Cancer. 2020;132:61–70. doi:10.1016/j.ejca.2020.03.017
21. Holstead R, Kartolo A, Baetz T. Emergency department utilization for patients receiving immune checkpoint inhibitors: a retrospective analysis of identification and outcomes for those presenting for immune-related adverse events. Curr Oncol. 2020;28(1):52–59. doi:10.3390/curroncol28010007
22. Bertrand A, Kostine M, Barnetche T, et al. Immune related adverse events associated with anti-CTLA-4 antibodies: systematic review and meta-analysis. BMC Med. 2015;13(1):211. doi:10.1186/s12916-015-0455-8
23. Maughan BL, Bailey E, Gill DM, et al. Incidence of immune-related adverse events with program death receptor-1- and program death receptor-1 ligand-directed therapies in genitourinary cancers. Front Oncol. 2017;7:56. doi:10.3389/fonc.2017.00056
24. Villadolid J, Amin A. Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities. Transl Lung Cancer Res. 2015;4(5):560–575. doi:10.3978/j.issn.2218-6751.2015.06.06
25. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–2454. doi:10.1056/NEJMoa1200690
26. Moey MYY, Gougis P, Goldschmidt V, et al. Increased reporting of fatal pneumonitis associated with immune checkpoint inhibitors: a WHO pharmacovigilance database analysis. Eur Respir J. 2020;55(6):2000038. doi:10.1183/13993003.00038-2020
27. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378(2):158–168. doi:10.1056/NEJMra1703481
28. Pillai RN, Behera M, Owonikoko TK, et al. Comparison of the toxicity profile of PD-1 versus PD-L1 inhibitors in non-small cell lung cancer: a systematic analysis of the literature. Cancer. 2018;124(2):271–277. doi:10.1002/cncr.31043
29. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373(1):23–34. doi:10.1056/NEJMoa1504030
30. Wang Y, Zhou S, Yang F, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol. 2019;5(7):1008–1019. doi:10.1001/jamaoncol.2019.0393
31. Hammers HJ, Plimack ER, Infante JR, et al. Safety and efficacy of nivolumab in combination with ipilimumab in metastatic renal cell carcinoma: the CheckMate 016 study. J Clin Oncol. 2017;35(34):3851–3858. doi:10.1200/JCO.2016.72.1985
32. Weber JS, Hodi FS, Wolchok JD, et al. Safety profile of nivolumab monotherapy: a pooled analysis of patients with advanced melanoma. J Clin Oncol. 2017;35(7):785–792. doi:10.1200/JCO.2015.66.1389
33. Osorio JC, Ni A, Chaft JE, et al. Antibody-mediated thyroid dysfunction during T-cell checkpoint blockade in patients with non-small-cell lung cancer. Ann Oncol. 2017;28(3):583–589. doi:10.1093/annonc/mdw640
34. Schadendorf D, Hodi FS, Robert C, et al. Pooled analysis of long-term survival data from Phase II and Phase III trials of ipilimumab in unresectable or metastatic melanoma. J Clin Oncol. 2015;33(17):1889–1894. doi:10.1200/JCO.2014.56.2736
35. Galluzzi L, Humeau J, Buque A, et al. Immunostimulation with chemotherapy in the era of immune checkpoint inhibitors. Nat Rev Clin Oncol. 2020;17(12):725–741. doi:10.1038/s41571-020-0413-z
36. Weichselbaum RR, Liang H, Deng L, et al. Radiotherapy and immunotherapy: a beneficial liaison? Nat Rev Clin Oncol. 2017;14(6):365–379. doi:10.1038/nrclinonc.2016.211
37. Le Burel S, Champiat S, Mateus C, et al. Prevalence of immune-related systemic adverse events in patients treated with anti-programmed cell Death 1/anti-programmed cell death-Ligand 1 agents: a single-centre pharmacovigilance database analysis. Eur J Cancer. 2017;82:34–44. doi:10.1016/j.ejca.2017.05.032
38. Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. 2016;54:139–148. doi:10.1016/j.ejca.2015.11.016
39. Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the society for immunotherapy of cancer (SITC) toxicity management working group. J Immunother Cancer. 2017;5(1):95. doi:10.1186/s40425-017-0300-z
40. de Filette J, Jansen Y, Schreuer M, et al. Incidence of thyroid-related adverse events in melanoma patients treated with pembrolizumab. J Clin Endocrinol Metab. 2016;101(11):4431–4439. doi:10.1210/jc.2016-2300
41. Elia G, Ferrari SM, Galdiero MR, et al. New insight in endocrine-related adverse events associated to immune checkpoint blockade. Best Pract Res Clin Endocrinol Metab. 2020;34(1):101370. doi:10.1016/j.beem.2019.101370
42. Barroso-Sousa R, Barry WT, Garrido-Castro AC, et al. Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens: a systematic review and meta-analysis. JAMA Oncol. 2018;4(2):173–182. doi:10.1001/jamaoncol.2017.3064
43. Tanaka R, Fujisawa Y, Maruyama H, et al. Nivolumab-induced thyroid dysfunction. Jpn J Clin Oncol. 2016;46(6):575–579. doi:10.1093/jjco/hyw036
44. Del Rivero J, Cordes LM, Klubo-Gwiezdzinska J, et al. Endocrine-related adverse events related to immune checkpoint inhibitors: proposed algorithms for management. Oncologist. 2020;25(4):290–300. doi:10.1634/theoncologist.2018-0470
45. Toi Y, Sugawara S, Kawashima Y, et al. Association of immune-related adverse events with clinical benefit in patients with advanced non-small-cell lung cancer treated with nivolumab. Oncologist. 2018;23(11):1358–1365. doi:10.1634/theoncologist.2017-0384
46. Toi Y, Sugawara S, Sugisaka J, et al. Profiling preexisting antibodies in patients treated with anti-PD-1 therapy for advanced non-small cell lung cancer. JAMA Oncol. 2019;5(3):376–383. doi:10.1001/jamaoncol.2018.5860
47. Johnson DB, Balko JM, Compton ML, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375(18):1749–1755. doi:10.1056/NEJMoa1609214
48. Moslehi JJ, Salem JE, Sosman JA, et al. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet. 2018;391(10124):933. doi:10.1016/S0140-6736(18)30533-6
49. Salem JE, Manouchehri A, Moey M, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018;19(12):1579–1589. doi:10.1016/S1470-2045(18)30608-9
50. Skribek M, Rounis K, Afshar S, et al. Effect of corticosteroids on the outcome of patients with advanced non-small cell lung cancer treated with immune-checkpoint inhibitors. Eur J Cancer. 2021;145:245–254. doi:10.1016/j.ejca.2020.12.012
51. Petrelli F, Signorelli D, Ghidini M, et al. Association of steroids use with survival in patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Cancers. 2020;12(3):546. doi:10.3390/cancers12030546
52. Yeung SJ, Qdaisat A, Chaftari P, et al. Diagnosis and management of immune-related adverse effects of immune checkpoint therapy in the emergency department. J Am Coll Emerg Physicians Open. 2020;1(6):1637–1659. doi:10.1002/emp2.12209
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy and Low Adverse Events of Methylprednisolone Pulses Combined to Low-Dose Glucocorticoids for Systemic Sclerosis: A Retrospective Clinical Study of 10 Years’ Follow-Up
Cheng H, Yu Z, Yan CL, Yang HD, Gao C, Wen HY
Journal of Inflammation Research 2022, 15:4421-4433
Published Date: 4 August 2022