Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
A Real-World Study on the Day and Night-Time Symptoms Among Greek COPD Patients Who Recently Initiated Treatment with Dual Bronchodilation: The DANICO Study
Authors Kostikas K ![]() , Dimakou K
, Dimakou K ![]() , Gourgoulianis K, Gaga M, Papapetrou D, Tsoukalas G, Chatziapostolou P, Antoniadis A, Meletis G, Evangelopoulou E, Styliara P, Karypidou I, Gogali A
, Gourgoulianis K, Gaga M, Papapetrou D, Tsoukalas G, Chatziapostolou P, Antoniadis A, Meletis G, Evangelopoulou E, Styliara P, Karypidou I, Gogali A ![]() , Kalafatakis K, Tzanakis N
, Kalafatakis K, Tzanakis N
Received 23 March 2022
Accepted for publication 21 July 2022
Published 1 September 2022 Volume 2022:17 Pages 2027—2041
DOI https://doi.org/10.2147/COPD.S367553
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Konstantinos Kostikas,1 Katerina Dimakou,2 Konstantinos Gourgoulianis,3 Mina Gaga,4 Dimosthenis Papapetrou,5 Georgios Tsoukalas,6 Panagiotis Chatziapostolou,7 Antonios Antoniadis,8 Georgios Meletis,9 Efstathia Evangelopoulou,10 Panagiota Styliara,11 Ilektra Karypidou,12 Athena Gogali,1 Konstantinos Kalafatakis,13,14 Nikolaos Tzanakis15
1Respiratory Medicine Department, University Hospital of Ioannina, Ioannina, Greece; 2 5th Respiratory Medicine Department, General Hospital for Chest Diseases of Athens “SOTIRIA”, Athens, Greece; 3Department of Respiratory Medicine, University of Thessaly, Larissa, Greece; 4 7th Respiratory Medicine Department, General Hospital for Chest Diseases of Athens “SOTIRIA”, Athens, Greece; 5Iatriko Athinon, Paleo Faliro, Attiki, Greece; 6 4th Respiratory Medicine Department, General Hospital for Chest Diseases of Athens “SOTIRIA”, Athens, Greece; 7Department of Pulmonary Medicine, Euromedica General Clinic, Thessaloniki, Greece; 8Department of Pulmonary Medicine, General Hospital of Serres, Serres, Greece; 9Department of Pulmonary Medicine, General Hospital of Heraklion “VENIZELEIO”, Heraklion, Greece; 10Respiratory Medicine Department, General Hospital of Nikaia “ST. PANTELEIMON”, Piraeus, Greece; 11Menarini Hellas, Athens, Greece; 12Department of Pulmonary Medicine, General Hospital of Thessaloniki “GEORGIOS PAPANIKOLAOU”, Thessaloniki, Greece; 13Department of Informatics & Telecommunications, University of Ioannina, Arta, Greece; 14Barts and the London School of Medicine & Dentistry, Queen Mary University of London (Malta Campus), Victoria, Gozo, Malta; 15Department of Respiratory Medicine, University General Hospital of Heraklion, Heraklion, Greece
Correspondence: Konstantinos Kostikas, Respiratory Medicine & Head of Respiratory Medicine Department, University Hospital of Ioannina, Ioannina, Greece, Tel +30-2651007536 ; +30-6944780616, Email [email protected]; [email protected]
Purpose: The rationale of this study was to investigate the prevalence of daily and night symptoms and quality of sleep in Greek COPD patients as a means to evaluate their response to treatment with the fixed dose combination of aclidinium/formoterol (administered through the Genuair® device).
Patients and Methods: This study was a multicenter, nationwide, non-interventional, observational study in 2105 patients suffering from COPD, who have recently started treatment with aclidinium/formoterol. Patients were attending to two visits, one baseline and a final visit, 3 months later. Different variables have been collected on either the baseline or the final visit or both: demographics, vital sign measurements, COPD-related medical history parameters, comorbidities, COPD assessment test (CAT), COPD severity based on spirometry measurements, COPD stage based on the ABCD assessment approach proposed by the 2019 Global Initiative for Chronic Obstructive Lung Disease (GOLD), COPD treatment report, and severity of early-morning, daytime and night-time COPD-related symptoms. Reasons for prescribing aclidinium/formoterol, satisfaction of patients to the treatment, as well as their compliance have also been recorded.
Results: After 3 months on aclidinium/formoterol, 50.1% of the patients experienced an improvement in their early-morning symptoms. Furthermore, 49.9% of them experienced an improvement in their daily symptoms, 44.9% improved their night-time symptoms and 43.2% reduced the frequency of overnight sleep disruptions due to COPD symptoms. These favorable outcomes apply mainly to GOLD Groups B–D. Treatment with aclidinium/formoterol improved on average the pre-bronchodilation FEV1% pred by 3.18%, the post-bronchodilation FEV1% pred by 2.78% and reduced CAT score by 5.22 points. Satisfaction with using aclidinium/formoterol across patients was high, as well as compliance to therapy.
Conclusion: Aclidinium/formoterol provided significant benefits on the quality of life of COPD patients by reducing the morning, daytime and the night-time symptoms and symptom burden in GOLD Groups B–D, and activity impairment under real-life conditions in all GOLD ABCD groups.
Keywords: COPD, dual-bronchodilation therapy, aclidinium/formoterol, daytime and night-time symptoms, GOLD ABCD classification
Introduction
Chronic obstructive pulmonary disease (COPD), one of the leading causes of morbidity and mortality worldwide, presents challenges in properly evaluating its personalised severity (a multifactorial variable where, besides pulmonary functional capacity, other factors play crucial role, such as type and intensity/duration of symptoms, frequency of exacerbations, presence of comorbidities) and subsequently recommending the most suitable for each case therapeutic strategies. In this context, current Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations rely on the “ABCD” assessment tool for estimating COPD severity and issuing pharmacological interventions;1 this approach is being periodically revised in accordance with newer clinical evidence.
A particularly challenging domain, regarding accurately estimating the disease burden for each patient (to come to meaningful clinical decisions), relates to the fact that daytime and nighttime symptoms might differ (in type, intensity, or duration), leading to notable differences in the quality of life among COPD patients with the same attributable disease severity. For instance, nighttime symptoms may lead to sleep disturbances, affecting bodily circadian rhythms, resulting in neuropsychiatric comorbidities, such as sleep disorders, anxiety, or depression.2,3 Therefore, a more detailed approach regarding the appropriate classification of COPD patients and their treatment beyond the GOLD recommendations seems necessary and this notion is increasingly discussed among COPD specialists worldwide.4
Some recently published controlled trials in COPD patients have shown that dual bronchodilation therapy with long-acting muscarinic antagonists (LAMA) and long-acting β2-agonists (LABA) is superior to mono-components and fixed dose combinations of inhaled corticosteroids with LABA (ICS/LABA) in both improving the symptoms of the patients and reducing the rate of COPD exacerbations.5–10 However, it has been also reported that not all patients respond to a given treatment in the same way, and efforts have been made to characterise the types of patients who respond to certain types of treatments, like LAMA/LABA.11 The latter (combination of a LABA with a long-acting muscarinic receptor antagonist LAMA) is proposed by the GOLD recommendations as first-line treatment in patients with more severe COPD (group D), as a step-up treatment from mono-bronchodilators (in patients still symptomatic in these treatments), and for de-escalation of ICS from ICS/LABA treatment or triple therapy with LABA+LAMA+ICS (in patients with pneumonia, inappropriate initial indication or lack of response to ICS).
Among other LAMA/LABA combinations, the one administered through the Genuair® device contains two active substances, aclidinium bromide (LAMA) and formoterol fumarate dihydrate (LABA) and was granted a marketing authorisation valid throughout the European Union by the European Commission since 19 November 2014.12 Aclidinium/formoterol is available as an inhalation powder in a portable DPI device. The inhaler delivers 340 μg of aclidinium bromide and 12 μg of formoterol fumarate dihydrate for each inhalation. The recommended dose is one inhalation twice a day. Since today, no real-world studies have provided any form of evidence (a) on the use of aclidinium/formoterol by the respiratory medicine physicians in the context of managing COPD in Greek patients, (b) on patient-centric (subjective) and clinical (objective) markers of its therapeutic efficacy and (c) on patients’ clinical features and compliance. Taking these parameters into consideration, the rationale of this non-interventional study was to investigate the prevalence of daily and night symptoms in Greek COPD patients with different levels of disease severity according to the latest GOLD recommendations, as a means to evaluate their response to the fixed dose combination of aclidinium/formoterol.
Materials and Methods
Study Overview, Structure, and Workflow
This study was a multicenter, nationwide, non-interventional, observational study in patients suffering from COPD and recently started treatment with aclidinium/formoterol according to the locally approved summary of product characteristics. The decision to treat the patient with aclidinium/formoterol was taken by the treating physician, independently of participation in this study as per his/her medical judgement and was made before participation being considered. Patients with COPD diagnosed by a pulmonologist and stable disease were enrolled consecutively and were followed over an observational period of 3 months on average (Figure 1). In total, 205 sites (pulmonologists in private practice and hospitals) participated in the study ensuring a proper geographical representation among Greece. Patients were examined at baseline (Visit 1) and at follow-up (Visit 2). At Visit 1, the following parameters were measured or acquired (from previous measurements) as per routine clinical practice: demographics, medical and family history, concomitant diseases, prior COPD medication, concomitant COPD medication, vital signs, body weight and height, spirometric values, COPD early-morning and night-time symptoms questionnaire, COPD Assessment Test (CAT), exacerbations in the past year. Also, the physician provided the reason he/she decided to prescribe a LAMA/LABA combination (aclidinium/formoterol). At Visit 2, concomitant COPD medication, newer spirometric values, COPD early-morning and night-time symptoms questionnaire and CAT were re-acquired, and drug compliance, exacerbations since last visit and patient’s satisfaction with the Genuair device were additionally assessed. The evaluations during visit 2 (either self-evaluations of patients or evaluations by physicians) were performed without any of the involved parties having access to the initial measurements at visit 1.
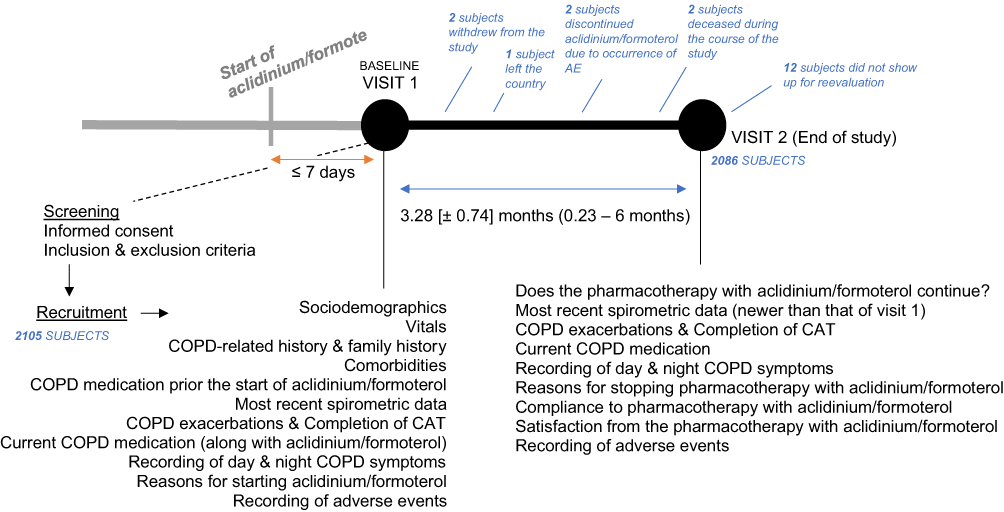 |
Figure 1 Overview of the DANICO study. Abbreviations: CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease. |
Bioethical Considerations
The study was conducted according to the provisions of Good Clinical Practice (GCP), local laws, EU-Directive 2001/20, and the International Conference on Harmonization and the World Medical Association Declaration of Helsinki guidelines. Prior to study initiation, study protocol and all relevant documentation was submitted to and approved by the Institutional Review Board/Ethics Committees (IRB/EC) of the following institutions: General Hospital of Thorax diseases “SOTIRIA” (Athens), General Hospital of Nikaia (Athens), General Hospital of Thessaloniki “G. PAPANIKOLAOU”, General Hospital of Serres, University Hospital of Larissa, University Hospital of Ioannina and University Hospital of Heraklion “PAGNI” (Crete). Given the sensitive nature of data processed in the frame of the study, all parties involved undertook adequate safety measures (physical, logical, organisational, technical, etc.) to warrant that data would always be processed safely and in compliance with the EU Data Privacy Directive 95/46/EC.
Written informed consent was obtained from each subject prior to evaluations performed for eligibility and any study-related procedures by the Investigator or its authorized delegate. In the patient information section, patients were given information and fully comprehensive explanation in easily understandable terms of the study procedures, regarding the benefits, restrictions, discomforts, and risks in taking part in the study. Subjects were also informed about the measures taken to ensure their confidentiality according to the current legislation. Subjects were given adequate time to review the information in the informed consent form and were allowed to ask, and have answered, questions concerning all portions of the conduct of the study. Subjects were able to withdraw from the study at any time without explanation and without losing the right to receive medical care. Management of adverse events (AEs) was handled according to the protocol and as per drug safety regulations in Greece and the European Union.
Participants
Patients fulfilled the following inclusion criteria for inclusion in the study: (a) age ≥40 years, (b) current or ex-smoker with a smoking history of at least 10 pack-years, (c) established diagnosis of COPD according to the 2019 GOLD recommendations, (d) recent initiation of treatment with aclidinium/formoterol (for no more than 1 week), (e) no exacerbations in the previous 6 weeks, and (f) patients able and willing to sign informed consent and to comply with study procedures. The following exclusion criteria were applied: (a) undergoing pregnancy or lactation (for women); (b) history of a previous diagnosis of asthma, sleep apnea syndrome or other chronic respiratory disease different from COPD; (c) an acute or chronic condition that, in the investigator’s opinion, would limit the patient’s ability to complete questionnaires or participate in this study; and (d) participation in another study.
Study Objectives
The primary objective of the present study was to determine (a) the frequency and severity of early-morning, day- and night-time symptoms related to COPD at baseline (visit 1) and (b) the frequency and severity of early-morning, day- and night-time symptoms related to COPD after the end of the observational period (3 months on average), coinciding with undergoing therapy with aclidinium/formoterol. The secondary objectives of the present study were (a) to evaluate the association between early-morning and night-time symptoms and disease severity; (b) to evaluate the extent of satisfaction of patients when using the aclidinium/formoterol inhalation device, as well as the association between the perceived satisfaction of the device and the GOLD stage in COPD; and (c) to characterise the treatment pathways of COPD patients starting therapy with aclidinium/formoterol (years of disease, type of previous therapy, comorbidities and reason for the physicians’ decision for the prescription).
Study Assessments
Demographics: Age, body weight, height, and gender of the participants was recorded (visit 1).
Vital sign measurements: Diastolic and systolic blood pressure along with heart rate have been measured and recorded by the responsible physicians (visit 1).
COPD medical history: during visit 1, patients were asked to provide information regarding their COPD medical history. This included the time of first diagnosis and their family history of COPD, asthma, lung cancer or occupational hazardous exposure.
Spirometric measurements and disease severity: lung function (spirometric) data from each patient’s latest measurements were recorded by the investigator during both study visits by means of FEV1 (forced expiratory volume in 1 sec) and FVC (forced vital capacity), pre- and post-bronchodilation, according to common clinical practice, and the severity of airflow limitation was determined as mild (post-bronchodilation FEV1 ≥80% of predicted), moderate (post-bronchodilation FEV1 = 50–79% predicted), severe (post-bronchodilation FEV1 = 30–49% predicted) and very severe (post-bronchodilation FEV1 <30% of predicted).
Comorbidities: Comorbidities were recorded as reported by the patient and/or as recorded in the national electronic prescription system (available for each patient) during Visit 1.
COPD Assessment Test (CAT): The patients were asked to fill a CAT questionnaire onsite during both study visits. The CAT consists of eight items (cough, phlegm, chest tightness, breathlessness, limited activities, confidence leaving home, sleeplessness, and energy). Item scores range from 0 to 5 points resulting in a CAT total score ranging from 0 to 40 points. The minimal clinically important difference of the CAT is 2 points.13
Classification of subjects based on the GOLD ABCD classification: during visit 1, patients were asked about their disease exacerbation history (frequency, severity) over the previous 12 months, and were subsequently classified as belonging to Group A (CAT score <10, up to one exacerbation not leading to hospitalization), B (CAT score ≥10, up to one exacerbation not leading to hospitalization), C (CAT score <10, 2+ exacerbations or any leading to hospitalization) or D (CAT score ≥10, 2+ exacerbations or any leading to hospitalization) of the ABCD assessment tool suggested by GOLD guidelines. During visit 2, patients were asked to update their disease exacerbation history for the period succeeding study visit 1.
COPD treatment report: a detailed database for all COPD-related drugs that every patient was taking before and after the start of aclidinium/formoterol has been created during study visit 1. Similarly, a detailed database for all COPD-related drugs that every patient was taking at the time of the second study visit has been developed.
COPD early-morning and night symptoms questionnaire: this tool was designed to measure the occurrence and severity of early-morning (wake up) and night symptoms in patients with COPD. The questionnaire was asking the physician to document, during both study visits, how often the patient wakes up at night due to the symptoms and score the symptom severity using a 5-point Likert-type scale, ranging from no symptoms (0) to very severe symptoms (4), and frequency using an 11-point Likert-type scale, ranging from never (0) to more than once every night (10). The tool also records any COPD symptoms that the patient experienced after waking up in the morning, namely cough, wheezing, shortness of breath and difficulty bringing up the phlegm as well as the severity of each symptom using a 5-point Likert-type scale, ranging from no symptoms (0) to very severe symptoms (4). Finally, the physician was also asked to document the extent of limitation of the patient’s daily activities due to COPD symptoms using a 5-point Likert-type scale, ranging from “not at all” (0) to “a very large extent” (4).14–16
Reasons for prescribing aclidinium/formoterol: during the visit 1, the treating physician reported the reason for having taken the medical decision to initiate treatment with aclidinium/formoterol as part of the therapeutic approach of COPD for every given study participant.
Patients’ satisfaction with the Genuair inhalation device: at visit 2 patients were asked to confirm that they continue their treatment with aclidinium/formoterol, record the reason if not, state how often they omit any dose of the drug (ie, compliance to treatment), reasons for that, express any concerns from the use of aclidinium/formoterol, and rate their satisfaction with the inhalation device in a scale from 1 to 100 with higher scores indicating higher satisfaction.
AEs recording: All reported AEs received through the study regardless of whether the event was serious, labeled, or attributed to aclidinium/formoterol were reported to regulatory authorities in accordance with Regulation (EC) No. 726/2004 and Directive 2001/89/E as amended and Volume 9a of the Rules Governing Medicinal Products in the European Union in the E.U. The crude incidence of treatment emergent adverse events (ie, events started after the first dose of study treatment and after the informed consent form signature) has been reported. As per protocol provisions, all participating investigators (treating respiratory medicine physicians) collected and assessed any occurred subjective and objective AEs during each study visit. In addition, AEs communicated by patients or relatives or delegates via the phone or emails have been also recorded, and if incomplete, the remaining pieces of information (including diagnostic measures conducted in healthcare facilities) were followed up by the investigators promptly.
Statistical Analysis
All variables were summarized by frequency distribution tables (categorical variable) or are expressed as in the number of cases. Their median, mean, standard deviation (SD), or range for continuous variables, has been calculated. Missing values have not been replaced, and all analyses are based on the number of existing values from any part of the sample. Any missing values occurred in a random manner, ie, could not introduce a systematic bias into the study. The Wilcoxon signed-rank test has been utilized to determine whether there is a median difference between paired observations (prior and after the start of aclidinium/formoterol) of the ordinal variables constructed by the output of the questionnaires used in the study. In these cases, the symmetry of the distribution of the differences between the two related groups has been confirmed. Moreover, a two-way repeated measures analysis of variance (ANOVA) was run to determine the effect of the averagely 3-month treatment period with aclidinium/formoterol on spirometric parameters, pre- and post-bronchodilation. In this case, the number of outliers has been determined, as well as the normality in the distribution of the dependent variable in the two levels of the within-subjects’ factors. Finally, a paired-samples t-test was used to determine whether there was a statistically significant mean difference between the CAT score of the study participants before and after being treated with aclidinium/formoterol. In this case, the presence of as few outliers as possible and the normality in the distribution of the differences of the dependent variable are also important and confirmed. All tests were 2-sided, and the significance level p was set to 0.05. Bonferroni correction has been applied to account for multiple comparisons, wherever applicable. As a measure of the effect size, partial eta squared (η2) was used in the ANOVA, and Cohen’s d was used in the Student’s t-test.
Results
Study Sample Characteristics
A total of 2105 patients were enrolled in this study from May 2019 to November 2019. Nineteen patients discontinued from the study; 15 subjects did not show for reevaluation, 2 subjects stopped the study treatment due to adverse events and 2 were deceased (see below). Almost three-quarters of the patient sample were male with a mean age of 68 years (± 9.6). Most patients were either overweight or obese (Supplementary Table 1). The mean time-since-initial-diagnosis of the patient sample was 5.8 years (± 5.4), and only 11% of them had a family history of COPD. Most patients (61%) were classified to Group B, according to the GOLD recommendations. Almost half of the patients suffered from comorbidities, which mainly involved cardiovascular disorders, diabetes mellitus and metabolic syndrome (Supplementary Table 2). Half of the total study sample had also suffered at baseline from at least one COPD exacerbation over the previous year, and about a quarter of these patients were referred at least once to the emergency room of a hospital for such as reason (Supplementary Figure 1).
Characterization of Treatment Pathways
From the total patient sample that completed the study (2086 patients), 2063 patients were still on aclidinium/formoterol by visit 2, and 23 patients completely discontinued COPD medications (including aclidinium/formoterol). Prior to being prescribed with aclidinium/formoterol, more than a third of study participants (35%) were receiving a LABA/ICS, about a sixth (18%) was taking monotherapy with a LAMA and another sixth (17%) no medication at all. Less frequent options were administering three different medications (LABA + LAMA + ICS), LABA monotherapy or a combination of LABA/LAMA other than aclidinium/formoterol. After being prescribed with aclidinium/formoterol, the great majority of patients were receiving the latter as a monotherapy during visit 1 (79%) as well as visit 2 (86%). In most of the remaining cases, aclidinium/formoterol was combined with either one or two other pharmaceutical agents, including ICS, a short-acting β adrenoreceptor agonist and/or LABA/ICS (Figure 2).
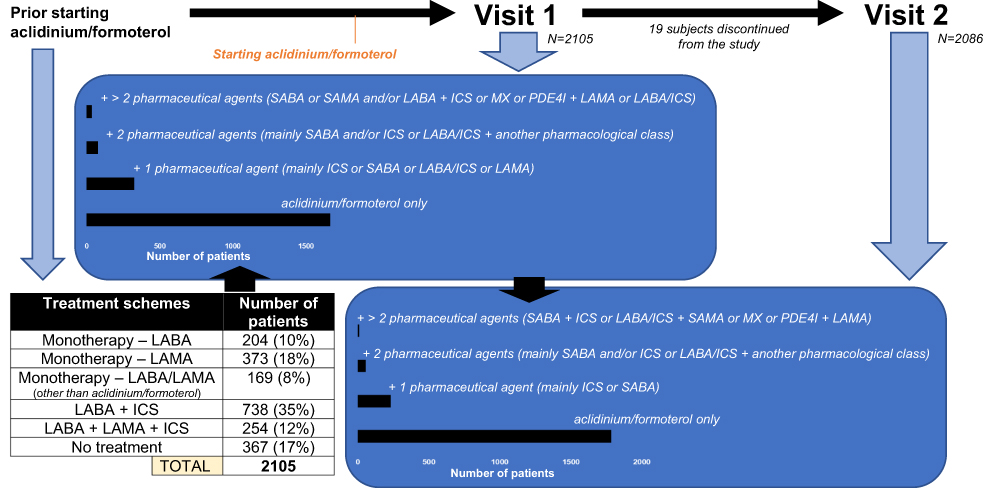 |
Figure 2 Summary of the different treatment pathways that were followed by the study participants, either before being prescribed with aclidinium/formoterol, at visit 1 and visit 2 of the study. Abbreviations: ICS, inhaled corticosteroids; LABA, long-acting β adrenoreceptor agonists; LAMA, long-acting muscarinic receptor antagonists; MX, methylxanthines; PDE4I, phosphodiesterase-4 inhibitors; SABA, short-acting β adrenoreceptor agonists; SAMA, short-acting muscarinic receptor antagonists. |
Evolution of Early-Morning Symptoms
The use of aclidinium/formoterol correlates with significant alterations in the burden of early-morning, daily and night-time symptoms. The severity of early-morning symptoms was significantly reduced at follow-up visit (p<0.001) (Figure 3A) with the probability of having less severe early-morning symptoms at this visit being 4.537 (95% CI 3.197–6.438) times greater as compared to baseline. Overall, 1039 patients (50.1%) experienced an improvement in their early-morning symptoms, over 908 who remained stable and 126 whose symptoms deteriorated (49.9%). The favorable results of using aclidinium/formoterol are more distinct in the GOLD Groups B–D, while in Group A, the favorable outcome was smaller (Supplementary Figure 2). In terms of specific early-morning symptoms, the presence of cough, wheezing, dyspnea or mucus clearance difficulties was significantly reduced at the follow-up visit (p<0.001), with the corresponding probability of these symptoms being the most disturbing early-morning symptom at that visit being decreased by 45% [OR 0.55 (95% CI 0.495–0.611)], 59% [OR 0.41 (95% CI 0.368–0.450)], 53% [OR 0.47 (95% CI 0.421–0.513)] and 54% [OR 0.46 (95% CI 0.414–0.509)] respectively (Figure 3B). Again, these favorable results are more evident in the GOLD Groups B–D, rather than in Group A (Supplementary Figure 2).
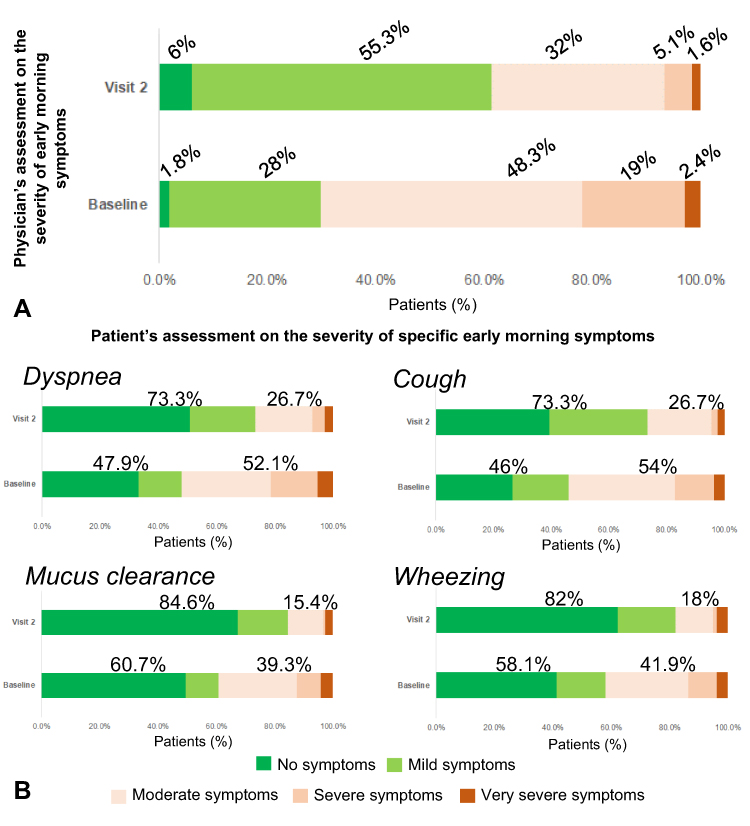 |
Figure 3 (A) Patient distribution according to the physician-assessed severity of early-morning at baseline and at the follow-up visit (visit 2). Numbers indicate the percentages of patients. (B) Patient distribution according to the severity of specific early-morning symptoms as perceived by the patients at baseline and at the follow-up visit (visit 2). Numbers indicate the percentages of patients. |
Evolution of the Daytime and Night-Time Symptoms, and COPD Symptom-Related Nocturnal Awakenings
At baseline visit, 69% of the patients reported being at least moderately impaired in the performance of their daily activities due to their COPD symptoms, with this percentage decreasing to 41.6% at the follow-up visit (Figure 4A). Moreover, the severity of night-time symptoms was significantly reduced at the follow-up visit (p<0.001), with the probability of having less severe night-time symptoms being 2.906 (95% CI 2.353–3.597) times greater as compared to baseline (Figure 4B). Finally, over 40% of the patients, for which data were available, showed a reduction in the frequency of their nocturnal awakenings due to COPD symptoms (Figure 4C). Once more, these favorable results are more evident in the GOLD Groups B–D, rather than in Group A (Supplementary Figure 3).
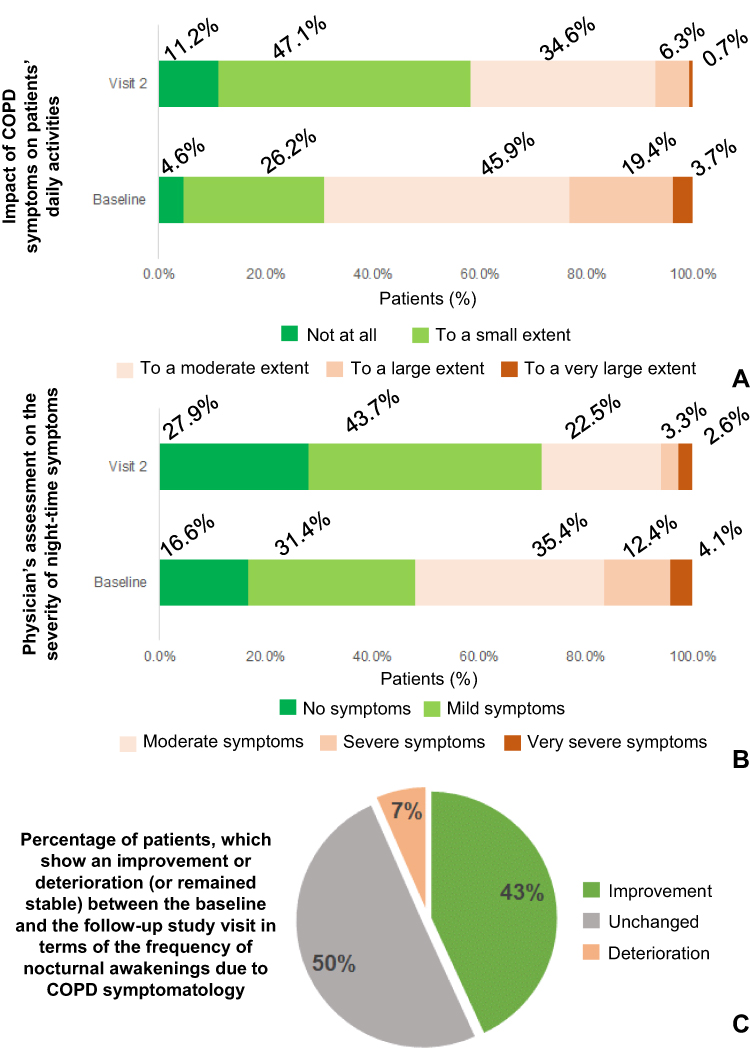 |
Figure 4 (A) Patient distribution according to the impact of daily COPD-related symptoms on the patients’ daily activities at baseline and at the follow-up visit (visit 2). Numbers indicate the percentages of patients. (B) Patient distribution according to the physician-assessed severity of night-time symptoms at baseline and at the follow-up visit (visit 2). Numbers indicate the percentages of patients. (C) Patient distribution according to whether the frequency of their nocturnal awakenings was reduced (improvement), increased (deterioration) or remained unchanged between the baseline and follow-up visit. Numbers indicate the percentages of patients. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Evolution of Spirometric Parameters
The use of aclidinium/formoterol correlates with significant improvement in the FEV1% pred of COPD patients, in all GOLD ABCD groups. Nevertheless, that improvement was the least notable in Group A (either pre- or post-bronchodilation) and the most in Group D. In Group A, an improvement of 1.74% in pre-bronchodilation FEV1% pred and 0.95% in post-bronchodilation FEV1% pred on average has been observed (mean ± standard deviation, pre-bronchodilation FEV1% pred visit 1 vs visit 2: 65.93 ± 13.61 vs 67.67 ± 13.37, and post-bronchodilation FEV1% pred visit 1 vs visit 2: 67.99 ± 13.62 vs 68.94 ± 13.20). The corresponding values for Group B were 3.43% and 3.17% (58.45 ± 14.83 vs 61.89 ± 14.92 and 60.20 ± 14.91 vs 63.38 ± 14.93 respectively), for Group C 2.89% and 2.10% (51.56 ± 13.64 vs 54.45 ± 12.88, and 53.65 ± 13.85 vs 55.75 ± 13.69 respectively), and for Group D 4.36% and 4.18% (47.35 ± 14.89 vs 51.71 ± 15.09, and 49.43 ± 15.12 vs 53.61 ± 15.32 respectively). Significant interactions have been observed by repeated measures ANOVA between the study visit and the state of bronchodilation (pre-/post-), and a significant main effect of the study visit on the %predicted FEV1 of patients within each of the Groups A–C (F1,226 = 5.73, p = 0.018, partial η2 = 0.025, F1,1239 = 7.09, p = 0.008, partial η2 = 0.006, and F1,199 = 7.73, p = 0.006, partial η2 = 0.037, respectively), and also, a significant main effect of the study visit on the %predicted FEV1 of patients within Group D has been also identified (Figure 5, upper panel).
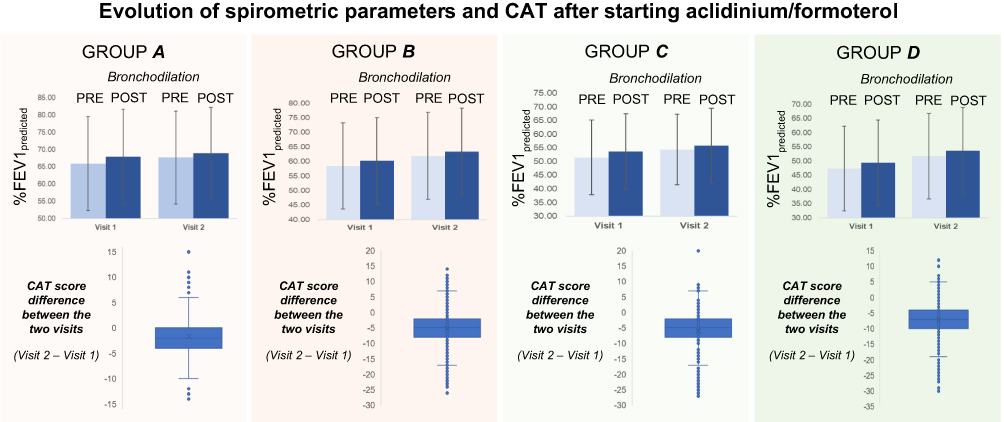 |
Figure 5 (Spirometric parameters - Upper panel in each ABCD group) Data shown are mean ± standard deviation. There was a statistically significant interaction between the state of bronchodilation and visit (before and after being treated with Aclidinium/formoterol) on %FEV1predicted in patients of GOLD Groups A–C (F1,226 = 5.73, p = 0.018, partial η2 = 0.025, F1,1239 = 7.09, p = 0.008, partial η2 = 0.006, and F1,199 = 7.73, p = 0.006, partial η2 = 0.037, respectively). Ιn Group A, pre-bronchodilation %FEV1predicted increased on average by 1.74%, and post-bronchodilation by 0.95%. In Group B, the corresponding percentages were 3.43% and 3.17%. In Group C, 2.9% and 2.1%. In Group D, no interaction between the study visits and the state of bronchodilation has been determined. (CAT – Lower panel in each ABCD group) Data shown are mean difference ± standard deviation. Participants on average were scoring lower to CAT in their second study visit compared to their first one, a statistically significant decrease across all GOLD ABCD groups (−1.69 with 95% CI [−2.16 to −1.21], t234 = −6.94, p < 0.001, d = 0.45 for Group A, −5.2 with 95% CI [−5.47 to −4.93], t1271 = −37.84, p < 0.001, d = 1.06 for Group B, −5.93 with 95% CI [−6.91 to −4.96], t208 = −11.99, p < 0.001, d = 0.83 for Group C and −7.15 with 95% CI [−7.78 to −6.52], t369 = −22.25, p < 0.001, d = 1.16 for Group D). Abbreviations: CAT, COPD assessment test; CI, confidence intervals; COPD, chronic obstructive pulmonary disease; %FEV1predicted, forced Expiratory Volume in 1 sec expressed as percentage of the predicted (based on age, height, and race); FI, functional impairment; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ME, magnitude of effort; MT, magnitude of task. |
Evolution of CAT Score
The use of aclidinium/formoterol was also associated with significant improvement (ie, reduction) in the CAT score of COPD patients, in all GOLD ABCD groups. The higher the group the greater the mean observed improvement (−1.69 points with 95% CI [−2.16 to −1.21], t234 = −6.94, p < 0.001, d = 0.45 for Group A, −5.2 points with 95% CI [−5.47 to −4.93], t1271 = −37.84, p < 0.001, d = 1.06 for Group B, −5.93 points with 95% CI [−6.91 to −4.96], t208 = −11.99, p < 0.001, d = 0.83 for Group C and −7.15 points with 95% CI [−7.78 to −6.52], t369 = −22.25, p < 0.001, d = 1.16 for Group D) (Figure 5, lower panel). The summary statistics of the CAT score (overall and subscores) before and after 3 months (on average) receiving aclidinium/formoterol are presented in Supplementary Table 3.
Reasons for Initiating Treatment with Aclidinium/Formoterol
The dominant reason for the treating physicians to prescribe aclidinium/formoterol was the unsatisfactory control of the disease; with the previous treatment scheme, COPD was either symptomatic or progressing (to more severe spirometric stages) or patients were experiencing exacerbations. Another reason included the inappropriate previous use of ICS. In 121 cases (5.8%), aclidinium/formoterol was prescribed as the initiation therapy. The mean satisfaction expressed by patients across the GOLD ABCD groups was exceeding 80. More than three-quarters of the study sample (77%) was perfectly compliant in receiving the daily doses of aclidinium/formoterol. Another 12% was occasionally missing a dose (up to once every month) and the last 11% was more systematically missing doses (once or more every week). The main reasons for the missing doses included the fact that patients decided not to use inhalers when feeling better and in cases of polypharmacy, ie, in patients who require to take multiple drugs on a daily basis for a number of different health problems (Figure 6).
 |
Figure 6 (A) Reasons for prescribing Aclidinium/formoterol by the treating physicians. (B) Satisfaction of patients using Aclidinium/formoterol per GOLD ABCD group. (C) Compliance to the treatment scheme with Aclidinium/formoterol, and reasons for missing doses. Abbreviations: AEs, adverse events; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids. |
AEs Reporting
There were six cases of adverse events occurring during the study (Table 1); two of them, which led to death, were not related to COPD therapy, and for another one it was unlikely that the study medication (or the COPD therapy in general) was involved in the occurrence. Three cases of adverse events were probable or likely to be related to aclidinium/formoterol therapy (one incident of nasal bleeding, one incident of agitation a few days after starting pharmacotherapy with aclidinium/formoterol, and another incident of dysuria/difficulties in urination which also started acutely after initiation of aclidinium/formoterol therapy); in the latter two cases, patients discontinued aclidinium/formoterol, as well as the study.
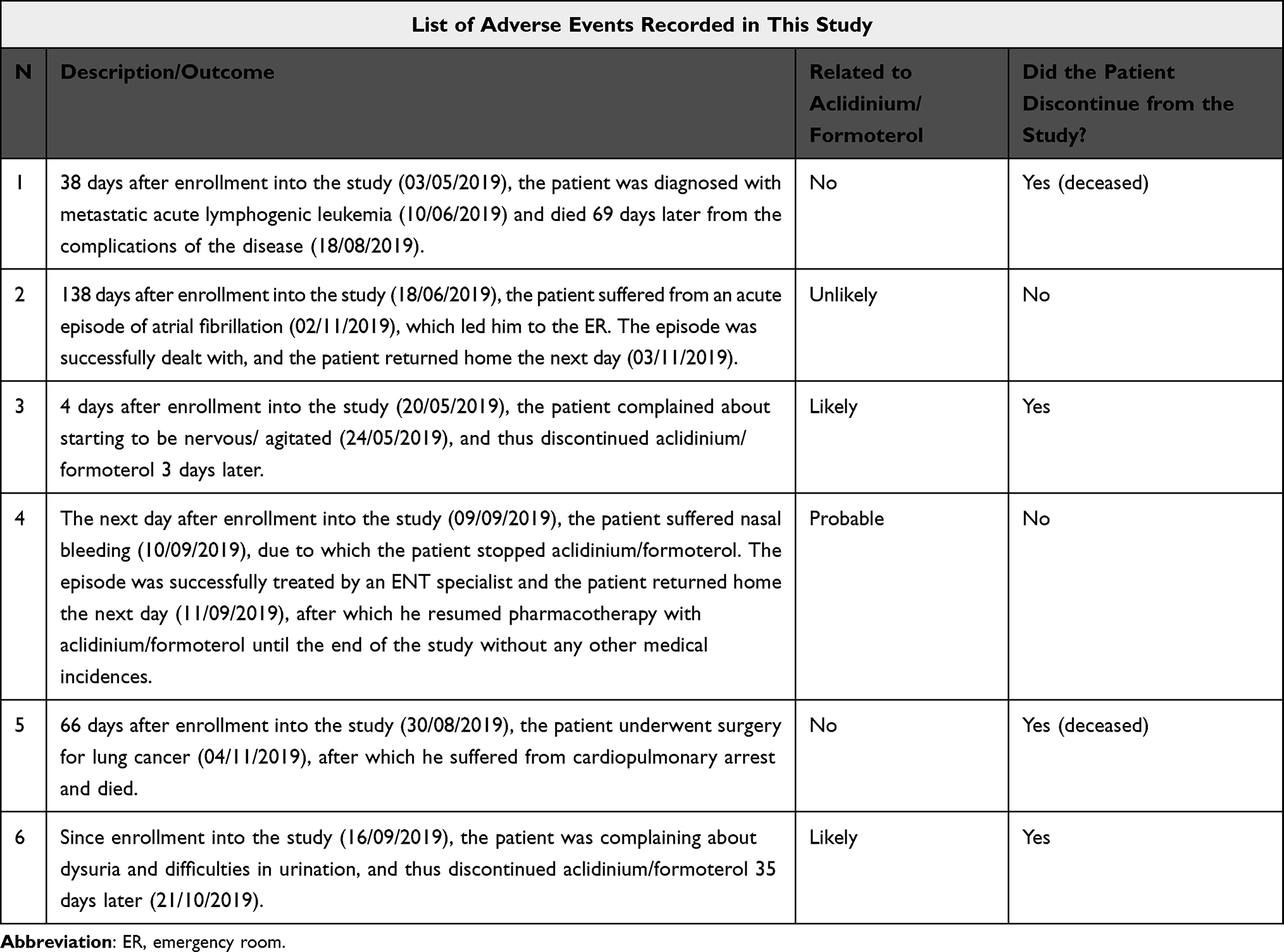 |
Table 1 The 6 Cases of Adverse Events Having Occurred During the Observational Study |
Discussion
Overall, a total of 2105 patients were enrolled in the DΑNΙCO study and were deemed eligible for participation (and thus included in the main analysis; FAS population) of which 2086 completed the study, whereas 19 discontinued from the study, mostly due to loss to follow-up. The features of our population sample show similarities to other large epidemiological studies conducted in Greece and abroad.17–21 In almost half of the cases (48.6%), the treating physician decided to prescribe aclidinium/formoterol due to the fact that patients were still symptomatic while on previous treatment (including lack of efficacy of ICS-containing approaches). Other common reasons included disease progression and thus choice of aclidinium/formoterol as an add-on therapy, occurrence of exacerbations while on previous treatment, or inappropriate use of ICS. Satisfaction with using aclidinium/formoterol across patients was high (the mean rating was exceeding 80 out of 100), independent of the GOLD ABCD group they belonged to. Compliance to the treatment was also satisfactory, with 89% of the population sample showing either perfect (no missing doses) or very good compliance (missing about one dose monthly).
After averagely 3 months on aclidinium/formoterol, 1039 (50.1%) patients experienced an improvement in their early-morning symptoms (over 908 who remained stable and 126 whose symptoms deteriorated). These favorable outcomes apply mainly to GOLD Groups B–D. Moreover, when patients are asked about specific early-morning symptoms (such as cough, wheezing, dyspnea or mucus clearance), again, there are more patients claiming having experienced an improvement compared to those with opposite outcome. This dynamic is again clearer in Groups B-D, rather than A. Treatment with aclidinium/formoterol seems to also exert favorable outcomes to COPD symptomatology throughout the day, at night-time and during night sleep. These improvements are again clearer for Groups B-D and less clear for Group A. Similarly, improvements have been also observed on average in the pre-bronchodilation FEV1% pred (by 3.18%) and the post-bronchodilation FEV1% pred (by 2.78%), which though are less evident in Group A and more evident in Group D. Similarly, a mean reduction in the CAT score by 5.22 points has been recorded; the higher the group (from A to D) the higher the observed reduction.
Over the last decade, the efficacy of aclidinium/formoterol in COPD patients has been accessed under different study designs. In the ACTIVATE study, treatment with aclidinium/formoterol (400/12 μg) improved lung hyperinflation and physical activity in patients with moderate-to-severe COPD compared to placebo-treated controls.22 In the AFFIRM COPD study, a 24-week, double-blind, double-dummy, active-controlled study, where patients were randomised (1:1) between aclidinium/formoterol (400/12 μg) twice-daily via Genuair/Pressair or salmeterol/fluticasone (50/500 μg) twice-daily via Accuhaler, the former regimen achieved a significant improvement in peak FEV1, an improvement of the transition dyspnea index by 1.5 points (compared to baseline) at 12 weeks and almost 2 points at 24 weeks, as well as a reduction in the CAT score by almost 2 points (compared to baseline) at 12 weeks and more than 2.5 points at 24 weeks.23 Other studies have also shown that aclidinium/formoterol (400/12 μg twice daily) may provide greater airway stability and fewer exacerbations or deteriorations in lung function, health status, or dyspnea compared with placebo or monotherapies.24 Our study, which relied on real-world data and recruited both patient-centric (subjective) as well as objective outcome measures, and additionally stratified patients based on the GOLD ABCD classification system, reports stronger reductions in the CAT score 3 months post-treatment initiation with aclidinium/formoterol, similar improvements in the spirometric parameters and a notable self-determined improvement in the morning-, day- and night-time symptoms of Group B-D COPD patients.
Our study confirms, under conditions of real practice, the results from the two pivotal Phase III clinical trials, the ACLIFORM COPD and AUGMENT COPD, in which aclidinium/formoterol demonstrated improvements in both early-morning and night-time symptom overall scores and their individual domain scores (cough, wheezing, shortness of breath, and difficulty bringing up phlegm) versus placebo, and early-morning and night-time symptom overall score versus both monotherapies.7,25 The results of our study are also aligned with another recently conducted, 12-month-long observational study on COPD patients in Germany, although the authors of that study show the evolution of the early-morning symptoms, using as a starting point 3 months after initiating aclidinium/formoterol (in our case this was the end point). The authors of that study also used a different approach for modelling the corresponding data.10 Finally, our results support up to a certain degree the suggestions of DACCORD observational study on the validity of switching to LABA/LAMA fixed-dose combination for patients either (a) symptomatic as first maintenance therapy, or (b) symptomatic and not well controlled with a mono-bronchodilator or LABA/ICS, or (c) as a “step down” strategy from triple therapy (LAMA+LABA+ICS).26
This study was based on the GOLD guidelines of 2019, which have not been changed by the latest GOLD recommendations. Potential limitations of this study relate to its non-interventional nature. One such limitation is the lack of a control group. Moreover, in this study, there was an apparent presence of comorbidities as well as of concomitant use of other COPD medications that may act as potential confounders. However, this limitation was addressed by evaluating any potential association of such comorbidities with the study outcomes, although this was not the case in terms of other COPD medications, especially those with a potential synergistic effect or a similar mechanism of action. Moreover, patients of different GOLD ABCD groups were included in the study, with considerably more patients in group B than in the other groups at baseline. Therefore, improvements in the symptoms of these patients should be interpreted with caution, although the type of group was taken into account during the analyses of the study outcomes. Another potential bias may arise from the use of self-reported questionnaires, which here could be influenced by the patient’s condition and mood at the time of the interview or his/her desire to please the physician, or just be prone to recall bias. Although, in general, improvement reported by patients seems to be overestimated compared to improvement measured objectively (and to some extent might reflect the Hawthorne effect), it successfully provides a more realistic and practical view of how the patient feels and functions, which for many pharmacological therapies (including the one assessed by this study) represents the optimal goal. It should be mentioned though that this study aimed at capturing both patient’s and physician’s perspectives of early-morning, daytime and night-time symptoms. In addition, given that the observational period lasted for averagely 3 months, long-lasting therapeutic effects could not be assessed. An important limitation of our spirometric data is the fact that only % predicted values of FEV1 and FVC were collected and analyzed. This was due to the fact that the DANICO study focused on the improvement of patient-reported outcomes in a real-life setting, rather than on lung function improvement, that is a well-established outcome for dual bronchodilation. It should also be noted that, since the frequency and severity of symptoms between the 2 visits were not recorded, trends cannot be established. Finally, the study included a single LAMA/LABA combination, that of aclidinium/formoterol. The scope of the study was to monitor the use and therapeutic impact of aclidinium/formoterol per se in the Greek population of COPD patients, and therefore we cannot comparative any evidence in relation to other LAMA/LABA combinations.
This study was conducted under conditions of everyday clinical practice. Notably, real-world studies, rather than implementing strict inclusion and exclusion criteria (resulting in highly selective populations like those in randomized controlled clinical trials), adopt pragmatic care settings and procedures in non-selected patients, including even those with comorbidities or concomitant medications, thus providing high external validity.27 Consistently, this study used only a very limited number of inclusion/exclusion criteria, with no restrictions regarding comorbidities or concomitant medications, and patient enrolment was performed consecutively as per medical judgement of the treating physician. Moreover, all decisions regarding treatment, as well as all medical examinations and procedures, were also exclusively based on the treating physician’s judgement and thus reflect the usual procedures followed in routine care. Finally, in this study, external validity was further enhanced by the geographical distribution (nation-wide) of sites enrolling patients, leading to a study population as representative of the general Greek COPD population as possible.
Conclusions
Taken together, the DANICO study has demonstrated that aclidinium/formoterol, administered through the Genuair® device, confers significant benefits on the quality of life of COPD patients by reducing the morning, daytime and the night-time and symptom burden in GOLD Groups B–D, and activity impairment under real-life conditions in all GOLD ABCD groups. Considering current evidence, and according to GOLD recommendations, aclidinium/formoterol should be considered an effective treatment option for symptomatic patients with COPD of various stages.
Data Sharing Statement
All data of this study are contained in this manuscript and Supplementary Materials.
Ethics Approval and Informed Consent
Please refer to the Materials and Methods section (Bioethical Considerations subsection) for full details.
Acknowledgments
Moreover, the authors would like to express their gratitude to Diamantis Chloros (Pulmonary Department, Aristotle University of Thessaloniki, “G. Papanikolaou” Hospital, Exohi, Greece), Georgatou Niki (Lung Specialist, Director, Iatriko Athinon, Areos 41, Paleo Faliro), Pechlivanidou Rouzana (Pulmonary Department, General Hospital of Serres, Serres, Greece), Emmanouil Ferdoutsis (Department of Pneumonology, Medical School University of Crete, Crete, Greece), Antonia Digalaki (5th Respiratory Medicine Department, General Hospital for Chest Diseases “SOTIRIA”, Athens, Greece), who significantly assisted in data collection, and Ioannis Violaris and Alexandros Tzallas (Department of Informatics & Telecommunications, School of Informatics & Telecommunications, University of Ioannina), who supported data analysis.
Author Contributions
K.KO, K.D., K.G. and N.T. conceived, designed and coordinated the study, and assisted in manuscript preparation. M.G., D.P., G.T. and P.C. coordinated data collection and processing, performed quality controls during the study execution, and assisted in manuscript preparation. A.A., G.M., E.E. and P.S. performed data collection, and assisted in data analysis and manuscript preparation. I.K., A.G. and K.KA. performed the data analysis, interpretation and wrote the main manuscript text. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The DANICO study has been sponsored by Menarini Hellas S.A.
Disclosure
The Respiratory Medicine Department (Konstantinos Kostikas) and the Department of Informatics and Telecommunications (Konstantinos Kalafatakis and Ioannis Violaris) of the University of Ioannina have received funding from Menarini Hellas S.A. Dr Konstantinos Kostikas reports grants, personal fees from AstraZeneca, grants, personal fees from Boehringer Ingelheim, personal fees from CSL Behring, grants, personal fees from Chiesi, grants, personal fees from ELPEN, personal fees from GILEAD, grants, personal fees from GSK, grants, personal fees from Menarini, grants, personal fees from Novartis, grants, personal fees from Sanofi, grants from NuvoAir, outside the submitted work. Dr Panagiota Styliara reports they are an employee of Menarini Hellas that conducted the study, during the conduct of the study. Dr Athena Gogali reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GSK, Novartis, outside the submitted work. Dr Konstantinos Kalafatakis reports grants from MENARINI HELLAS S.A., during the conduct of the study. Professor Nikolaos Tzanakis reports grants, personal fees from GSK, AstraZeneca, Novartis, Boehringer Ingelheim, ELPEN, MENARINI and NYCOMED; personal fees from PHARMATEN, INOVIS and GILEAD outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. GOLD. Global initiative for chronic obstructive lung disease; 2019. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf.
2. Agusti A, Hedner J, Marin JM, Barbé F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183–194. doi:10.1183/09059180.00004311
3. Price D, Small M, Milligan G, Higgins V, Gil EG, Estruch J. Impact of night-time symptoms in COPD: a real-world study in five European countries. Int J Chron Obstruct Pulmon Dis. 2013;8:595–603. doi:10.2147/COPD.S48570
4. Scichilone N, Incalzi RA, Blasi F, et al. Circadian rhythm of COPD symptoms in clinically based phenotypes. Results from the STORICO Italian observational study. BMC Pulm Med. 2019;19(1):171. doi:10.1186/s12890-019-0935-2
5. Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14:178. doi:10.1186/1471-2466-14-178
6. D’Urzo AD, Rennard SI, Kerwin EM, et al. Efficacy and safety of fixed-dose combinations of aclidinium bromide/formoterol fumarate: the 24-week, randomized, placebo-controlled AUGMENT COPD study. Respir Res. 2014;15(1):123. doi:10.1186/s12931-014-0123-0
7. Bateman ED, Chapman KR, Singh D, et al. Aclidinium bromide and formoterol fumarate as a fixed-dose combination in COPD: pooled analysis of symptoms and exacerbations from two six-month, multicentre, randomised studies (ACLIFORM and AUGMENT). Respir Res. 2015;16(1):92. doi:10.1186/s12931-015-0250-2
8. Miravitlles M, Chapman K, Chuecos F, Ribera A, Gil EG. The efficacy of aclidinium/formoterol on lung function and symptoms in patients with COPD categorized by symptom status: a pooled analysis. Int J Chron Obstr Pulm Dis. 2016;11:2041–2053. doi:10.2147/COPD.S114566
9. Ni H, Moe S, Soe Z, Myint KT, Viswanathan KN. Combined aclidinium bromide and long-acting beta2-agonist for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2018;12(12):CD011594. doi:10.1002/14651858.CD011594.pub2
10. Plate T, Friedrich FW, Beier J. Effectiveness and tolerability of LABA/LAMA fixed-dose combinations aclidinium/formoterol, glycopyrronium/indacaterol and umeclidinium/vilanterol in the treatment of COPD in daily practice - results of the non-interventional DETECT study. Int J Chron Obstruct Pulmon Dis. 2020;15:1335–1347. doi:10.2147/COPD.S252354
11. Matsunaga K, Oishi K, Miravitlles M, Anzueto A. Time to revise COPD treatment algorithm. Int J Chron Obstruct Pulmon Dis. 2019;14:2229–2234. doi:10.2147/COPD.S219051
12. Summary of the European Public Assessment Report (EPAR) for Brimica Genuair. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/brimica-genuair.
13. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
14. Mocarski M, Zaiser E, Trundell D, Make BJ, Hareendran A. Evaluation of the psychometric properties of the nighttime symptoms of COPD instrument. Int J Chron Obstruct Pulmon Dis. 2015;10:475–487. doi:10.2147/COPD.S75776
15. Garrow AP, Khan N, Tyson S, Vestbo J, Singh D, Yorke J. The development and first validation of the Manchester Early Morning Symptoms Index (MEMSI) for patients with COPD. Thorax. 2015;70(8):757–763. doi:10.1136/thoraxjnl-2014-206410
16. Hareendran A, Palsgrove AC, Mocarski M, et al. The development of a patient-reported outcome measure for assessing nighttime symptoms of chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2013;11:104. doi:10.1186/1477-7525-11-104
17. Kourlaba G, Hillas G, Vassilakopoulos T, Maniadakis N. The disease burden of chronic obstructive pulmonary disease in Greece. Int J Chron Obstruct Pulmon Dis. 2016;11(1):2179–2189. doi:10.2147/COPD.S110373
18. Mitsiki E, Bania E, Varounis C, Gourgoulianis KI, Alexopoulos EC. Characteristics of prevalent and new COPD cases in Greece: the GOLDEN study. Int J Chron Obstruct Pulmon Dis. 2015;10:1371–1382. doi:10.2147/COPD.S81468
19. Kostikas K, Vassilakopoulos TI, Tzanakis N, et al. A real-world observational study examining the impact of aclidinium bromide therapy on the quality of life, symptoms, and activity impairment of patients with chronic obstructive pulmonary disease: the Greek ON-AIR study. Int J Chron Obstruct Pulmon Dis. 2020;15:515–526. doi:10.2147/COPD.S239044
20. Tzanakis N, Koulouris N, Dimakou K, et al. Classification of COPD patients and compliance to recommended treatment in Greece according to GOLD 2017 report: the RELICO study. BMC Pulm Med. 2021;21(1):216. doi:10.1186/s12890-021-01576-6
21. Koulouris N, Dimakou K, Gourgoulianis K, et al. Self-perceived quality of sleep among COPD patients in Greece: the SLEPICO study. Sci Rep. 2022;12:540. doi:10.1038/s41598-021-04610-z
22. Watz H, Troosters T, Beeh KM, et al. ACTIVATE: the effect of aclidinium/formoterol on hyperinflation, exercise capacity, and physical activity in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2545–2558. doi:10.2147/COPD.S143488
23. Claus Vogelmeier C, Paggiaro PL, Dorca J, et al. Efficacy and safety of aclidinium/formoterol versus salmeterol/fluticasone: a Phase 3 COPD study. Eur Respir J. 2016;48(4):1030–1039. doi:10.1183/13993003.00216-2016
24. Singh D, D’Urzo AD, Chuecos F, Muñoz A, Gil EG. Reduction in clinically important deterioration in chronic obstructive pulmonary disease with Aclidinium/formoterol. Respir Res. 2017;18(1):106. doi:10.1186/s12931-017-0583-0
25. D’Urzo AD, Singh D, Donohue JF, Chapman KR. Aclidinium bromide in fixed-dose combination with formoterol fumarate in the management of COPD: an update on the evidence base. Ther Adv Respir Dis. 2019;13:1753466619850725. doi:10.1177/1753466619850725
26. Worth H, Buhl R, Criée CP, Kardos P, Lossi NS, Vogelmeier CF. GOLD 2017 treatment pathways in ‘real life’: an analysis of the DACCORD observational study. Respir Med. 2017;131:77–84. doi:10.1016/j.rmed.2017.08.008
27. Saturni S, Bellini F, Braido F, et al. Randomized controlled trials and real life studies. Approaches and methodologies: a clinical point of view. Pulm Pharmacol Ther. 2014;27(2):129–138. doi:10.1016/j.pupt.2014.01.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.