Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
A Real-World Data Retrospective Cohort Study of Low Estrogen Receptor-Positive Early Breast Cancer: Natural History and Treatment Outcomes
Authors Bari S, Boulware D, Li J, Loftus L, Soyano Muller A, Jameel Z, Khong H, Czerniecki BJ, Costa RLB
Received 4 May 2022
Accepted for publication 30 July 2022
Published 6 August 2022 Volume 2022:14 Pages 199—210
DOI https://doi.org/10.2147/BCTT.S371975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Shahla Bari,1 David Boulware,2 Jiannong Li,2 Loretta Loftus,3 Aixa Soyano Muller,3 Zena Jameel,4 Hung Khong,3 Brian J Czerniecki,3 Ricardo LB Costa3
1Department of Hematology/Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 2Department of Biostatistics, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 3Department of Breast Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 4Department of Anatomic and Clinical Pathology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA
Correspondence: Ricardo LB Costa, Department of Breast Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA, Tel +813 745 3806, Fax +813 745 7287, Email [email protected]
Purpose: Estrogen receptor-positive (ER+) breast cancer (BC) is a heterogeneous disease, and there is an ongoing debate regarding the optimal cut point for clinically relevant ER expression. We used a real-world database to assess the prognostic and predictive values of lower ER expression levels on treatment outcomes with endocrine therapy.
Methods: We used a nationwide electronic health record database. Descriptive statistics were used to evaluate the association between ER expression, tumor characteristics, and treatment patterns among patients with early-stage BC. We used Kaplan–Meier survival curves to estimate recurrence-free survival (RFS) and overall survival (OS). We assessed associations between an alternative ER expression-level cut point and clinical outcomes.
Results: Among 4697 patients with early-stage HER2-negative BC, 83 (2.04%) had ER+-low BC (ER expression, 1– 9.99%) and 36 (0.88%) had ER+-intermediate BC (10– 19.9%). ER+-low tumors were associated with higher tumor grade, larger size, and higher axillary tumor burden than ER+-high tumors (≥ 20% ER expression). African Americans had a higher prevalence of both triple-negative BC (TNBC) and ER+-low BC than ER+-high BC. Patients with ER+-low and ER+-intermediate tumors had survival outcomes similar to patients with TNBC and worse survival outcomes than patients with ER+-high tumors (P < 0.001). Tumors with < 20% ER expression were associated with worse outcomes.
Conclusion: In our cohort, patients with BCs with ER expression levels < 20% had poor clinical outcomes similar to those of patients with TNBC.
Keywords: breast cancer, estrogen receptor, low-positive, recurrence-free survival
Introduction
Breast cancer (BC) is the most common malignancy worldwide. Each year, an estimated 270 000 new cases are diagnosed in the United States alone.1 Hormone receptor– (HR-) positive (HR+) BC is the most common subset (~60% of cases) and is defined by the 2010 American Society of Clinical Oncology (ASCO) and College of American Pathology (CAP) guidelines as a tumor with at least 1% of cancer nuclei that stain positive for HRs for estrogen or progesterone by immunohistochemistry.2 Notwithstanding the clinical importance of pathological assessments of both HRs, decisions pertaining to endocrine therapy (ET) are largely based on expression levels of estrogen receptors (ERs), and progesterone receptors are largely accepted as a prognostic biomarker.
The current definition of ER positivity (ER+) presents an obvious caveat, as it does not encompass the biological heterogeneity inherent to the wide distribution of ER expression levels between tumors. Moreover, it suggests that patients with BCs with varying levels of ER expression have similar natural histories and derive similar benefits from approved and developing ETs. This is an incorrect premise. Data show that patients with tumors harboring lower levels of ERs have poor prognoses similar to those of patients with strictly defined triple-negative BC (TNBC); patients with TNBC have a 3-year absolute risk of BC recurrence of 30%, despite multimodality therapy.3–5 The results of a meta-analysis of 21,457 patients with early-stage BC showed that ER+-low status (ie, ligand-based assay, HR <10 fmol/mg cytosol protein) was not significantly associated with clinical benefit from adjuvant ET.6 Current guidelines for ER testing for BCs, published by ASCO and CAP, define ER+-low tumors as cancer with 1% to 10% staining for ERs and affirm the optimal cut point for ER positivity using the universally adopted immunohistochemistry scoring system.7 It is noticeable that this revision recognizes that most of the trials supporting the benefit of adjuvant ET for early ER+ BC conducted in the 1990s used quantitative measures of HRs that are no longer routinely used in clinical practice.
Despite the poor prognoses associated with ER+-low BC and the apparent inefficacy of ETs for these cancers, treatment development for ER+-low BC has been stagnant because these patients are not allowed to participate in clinical trials for patients with TNBC under the questionable assumption that these patients will experience better outcomes and benefit from ETs. This is important, as developmental therapeutics have gained momentum and treatments targeted at strictly defined subsets of BCs (eg, TNBC vs ER+ BCs) continue to be developed. This is evidenced by a new surge in clinical trials that assess the efficacy of new agents targeting ERs (eg, selective estrogen receptor modulators [SERMs] and degraders [SERDs]).8
We conducted a large real-world retrospective study of patients with early-stage BC to improve our current understanding of the prevalence and the natural history of tumors with lower levels of ER expression while also describing real-world treatment patterns for patients with this disease. Moreover, we retrospectively assessed the prognostic and predictive values of an alternative definition of ER+-low BC in relation to both natural history and treatment outcomes with ET.
Materials and Methods
Data Source
This retrospective cohort study used the nationwide Flatiron Health Electronic Health Record (FEHR) database, a real-world longitudinal database comprising deidentified patient-level structured and unstructured data curated via technology-enabled abstraction.9,10 The database originated from approximately 280 US cancer clinics (~800 sites of care). The majority of patients were from community oncology settings, and relative community/academic proportions may vary depending on the study cohort.
Our cohort (N = 9386) included patients with early-stage BC diagnosed between January 2011 and May 2020. Institutional Review Board approval of the study was obtained prior to study conduct and included a waiver for informed consent. The data were deidentified and subjected to obligations to prevent reidentification and protect patient confidentiality. The dataset included patient-related and tumor-related variables, including epidemiological, clinical, and pathological data, as well as age at diagnosis, race, ethnicity, menopausal status, tumor size, grade, Ki-67 (%) score, number of lymph nodes involved, chemotherapy history, and ET history. Expression of HRs and human epidermal growth factor receptor 2 (HER2) expression was assessed locally in accordance with standard immunohistochemistry nuclei staining by a local pathologist. Expression of HRs and HER2 was measured as the percent of nuclei staining and membrane staining, respectively. HER2 amplification was assessed according to locally assessed fluorescent in situ hybridization.
Recurrence-free survival (RFS) was defined as the time in months from the date of first treatment to the date of diagnosis of metastasis, first local recurrence, or death, whichever occurred first; patients without these data were censored at the last date known alive. Overall survival (OS) was defined as the time from the date of first treatment to the date of death; patients without these data were censored at the last date known alive.
Real-World Cohort Key Inclusion and Exclusion Criteria
The inclusion criteria used to select cases from the FEHR BC cohort included having a diagnosis of histologically proven stage I through III BC and receiving surgical treatment for BCs with curative intent. The exclusion criteria were having carcinoma in situ, metastatic BC, or HER2+ BC. Patients who received chemotherapy before or after surgical treatment were classified as having received perioperative chemotherapy. Information on perioperative chemotherapy, ET, and radiation therapy was abstracted. Because of the variation in the number of chemotherapy regimens, these regimens were classified as anthracycline- and taxane-combination, anthracycline-only, taxane-only regimens, and others. Anastrozole, exemestane, letrozole, and tamoxifen were classified as ET. Patients were followed from the date of resection (index date) to the date of biopsy-proven tumor recurrence, death, or last follow-up. Patients with >90 days between diagnosis and first Flatiron Health–reported structured activity were excluded to avoid missing treatment data. Furthermore, any patient with <90 days of follow-up from the index date was excluded.
Statistical Methods
Of the 9386 early-stage BC patients, 3490 had missing or incomplete ER, progesterone receptor (PR), or HER2 status and/or did not have at least 90 days of follow-up. Further 1299 patients had HER2+ BC and were also excluded from the final analysis, leaving 4697 evaluable patients (634 with TNBC and 4063 with ER+ BC). Descriptive characteristics were described by using means (standard deviations) and medians (ranges) for continuous variables and frequencies for categorical variables.
A training dataset and a test dataset were established by dividing the ER+ dataset into two-thirds training and one-third test data. The range of ER percent staining values was divided into 10 levels of 10% increments. A cut-point sensitivity analysis was performed on the training dataset using the Contal and O’Quigley method,11 which enabled us to assess the optimum cut point of ER+ staining; this was then correlated with RFS using Cox proportional hazards regression. The analysis did not identify a cut point that adequately and significantly differentiated RFS from other cut points, so we conservatively defined new exploratory ER+ cut point (ie, 1–19.9% vs ≥20%) and cohorts were compared using the Kruskal–Wallis test for continuous variables and Fisher's exact test for categorical variables.
We then constructed Kaplan–Meier curves for RFS and OS for both the training and test sets. A multivariable Cox proportional hazards survival analysis was used on the training set and adjusted for age, radiotherapy, and ET. This model was then used on the test set, and the c-statistic was used to check for model fit. Hazard ratios and 95% confidence intervals are reported. Subsequently, we further defined tumor ER expression levels into 3 distinct exploratory groups: (i) ER+-low (1–9.99%), (ii) ER+-intermediate (10–19.99%), and (iii) ER+-high (≥20%). Univariate analyses were performed to assess the effect of ET treatment on patients with ER+-low and ER+-intermediate BC. All analyses were performed in SAS v 9.4 (Cary, NC).
Results
Of the total cohort of 9386 patients with early-stage BC, only 4697 were evaluable (634 with TNBC and 4063 with ER+ BCs). Only 83 cases were classified as ER+-low (ie, ER expression 1–9.99%). Median follow-up was 36 months (range, 17–60 months).
Baseline Demographics and Clinical, Treatment, and Outcome Patterns
The majority (66.6%) of patients were White, and African Americans represented 9.2% of the cohort analyzed. There were 38 males in this dataset. Median age in years at diagnosis of BC was 63, and most women (72.4%) were postmenopausal. Regarding types of BC, 81.5% of patients had invasive ductal carcinomas, 12.3% had lobular carcinomas, and 47.8% had grade 2 tumors. Up to 63.6% of patients with early-stage BC received adjuvant radiation therapy, 31.4% received adjuvant chemotherapy, and 61.4% underwent mastectomies (Table 1). Patients with ER+ tumors had significantly longer RFS and OS than patients with TNBC (Figure 1).
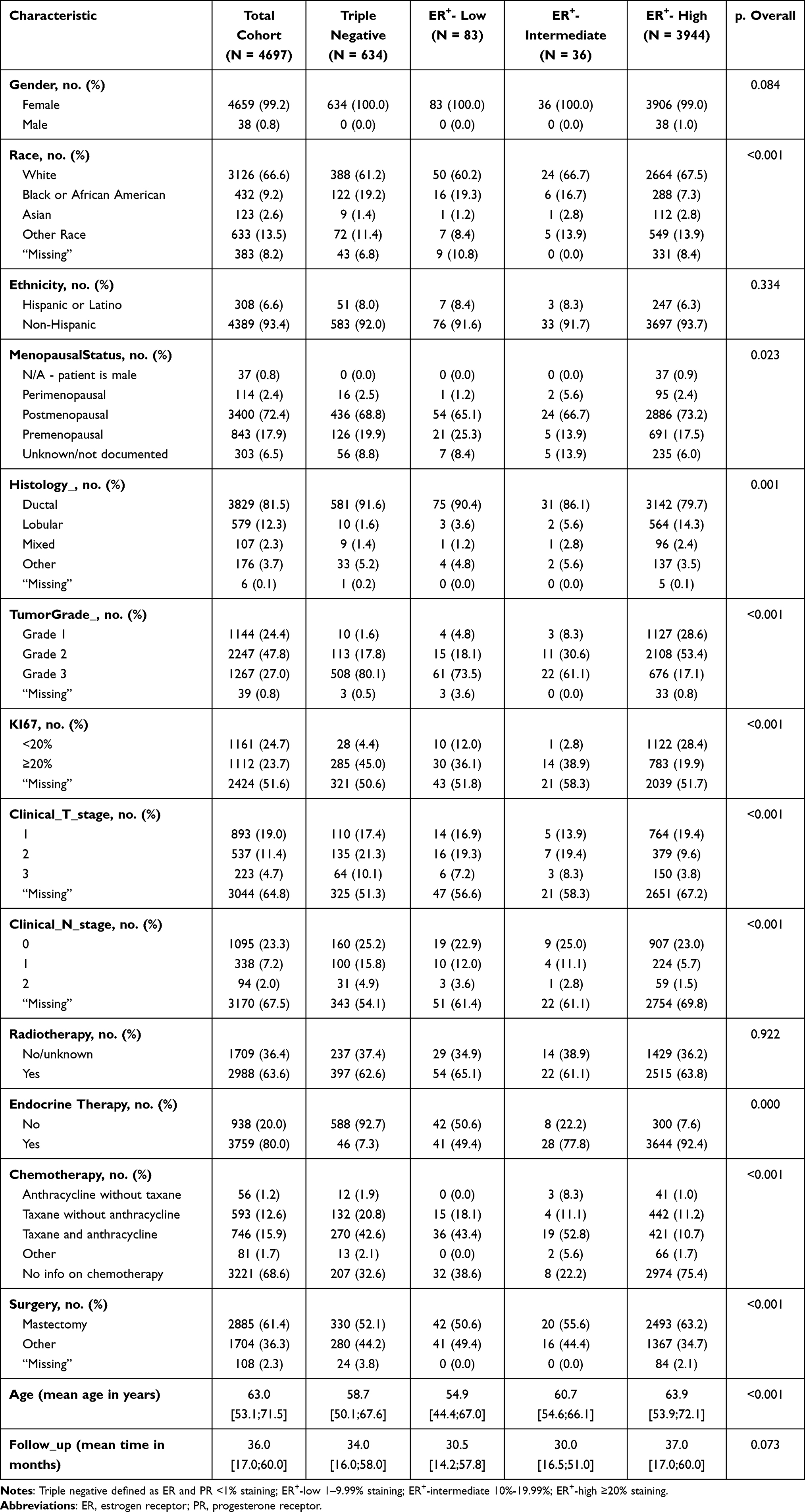 |
Table 1 Cohort Description |
 |
Figure 1 Clinical outcomes of patients with ER+ and TNBC BCs. Triple negative was defined as ER/PR < 1% staining and HER2- (ie, IHC 0/1+ and non-amplified); ER+ ≥ 1% staining. Panel (A) shows recurrence-free survival; panel (B) shows overall survival. Abbreviations: BC, breast cancer; CI, confidence interval; ER, estrogen receptor; HR, hormone receptor; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; PR, progesterone receptor, NE, not estimated. |
Distribution of ER Expression and Pathological Characteristics
Of the total 4063 patients with ER+/HER2− early-stage BC included in our analysis, 83 (2.04%) had ER+-low (ER staining 1–9.99%) BC, 36 (0.88%) had ER+-intermediate (ER staining 10–19.99%) BC, and 3944 (97.07%) had ER+-high BC. Both TNBC and ER+-low tumors were more commonly observed among patients <60 years of age. Patients with higher ER expression were typically older. Compared with Whites, African American patients had a higher frequency of both TNBC (28.2% vs 12.41%) and ER+-low (3.7% vs 1.59%) BC and lower frequency of ER+-high 66.7 vs 85.2%) tumors. The majority of ER+-high tumors had low to intermediate histological grades, whereas most tumors with lower levels of ER expression were grade 3 (Table 1). Patients with ER+-high tumors were also more commonly diagnosed with smaller tumors and lower axillary tumor burden than those with ER+-low tumors.
Clinical Outcomes of Patients with ER+-Low and ER+-Intermediate Early-Stage BCs
There were no statistically significant differences in the epidemiological, clinical, and pathological characteristics of patients with ER+-low and ER+-intermediate tumors (Table 2). Surgical and radiation treatment patterns were similar between these 2 groups. More patients in the ER+-intermediate group received adjuvant ET (unadjusted P = 0.007) and adjuvant chemotherapy with both anthracycline- and taxane-containing perioperative regimens (unadjusted, P = 0.004) than those in the ER+-low group. In univariate analyses, patients with ER+-low and ER+-intermediate tumors had poor OS and RFS rates, which were similar to those of patients with TNBCs (Figure 2). The low number of patients in the ER+-low and ER+-intermediate groups precluded multivariate analyses.
 |
Table 2 Comparison Between ER+-Low and ER+-Intermediate Groups |
 |
Figure 2 Clinical outcomes of patients with TN, ER+-low, ER+-intermediate, and ER+-high BCs. Triple negative was defined as ER and PR < 1% staining,; ER+-low, 1–9.99% staining; ER+-intermediate, 10–19.99%; ER+-high ≥ 20% staining. Panel (A) shows recurrence-free survival; panel (B) shows overall survival. Abbreviations: BC, breast cancer; CI, confidence interval; ER, estrogen receptor; HR, hormone receptor; HER2, human epidermal growth factor receptor 2; NE, not estimated; TN, triple negative. |
Sensitivity Analyses of ER Cut Point
Kaplan–Meier survival curves for both RFS and OS showed that patients with tumors harboring ER expression levels from 1% to 19.9% had significantly poorer outcomes than patients with expression rates ≥20% (Figure 3). Furthermore, multivariable Cox proportional survival analyses were performed on the training set and showed a statistically significant association between higher expression of ERs (≥20%) and improved RFS (hazard ratio, 0.55; 95% CI, 0.33–0.96; P = 0.02) and OS (hazard ratio, 0.5; 95% CI, 0.27–0.9; P = 0.02; Harrell’s c statistics, 0.677 for RFS and 0.698 for OS) (Table 3). Univariate analyses showed no significant differences in the treatment effect of ET on RFS and OS when comparing patients with ER+-low (1–9.99%) and ER+-intermediate tumors (10–19.99%) (Table 4), suggesting that these populations experience similar outcomes when ET is given. Finally, patients with ER+-low BC who were treated with ET had numerically improved RFS; in-between cohort differences were not statistically tested because there were too few patients in each cohort (Supplementary Figure 1).
 |
Table 3 Cox Proportional Hazards Regression -Comparative Analysis of Recurrence-Free Survival (RFS) and Overall Survival of ER+-1–19.9% Vs ER+-≥20% Staining |
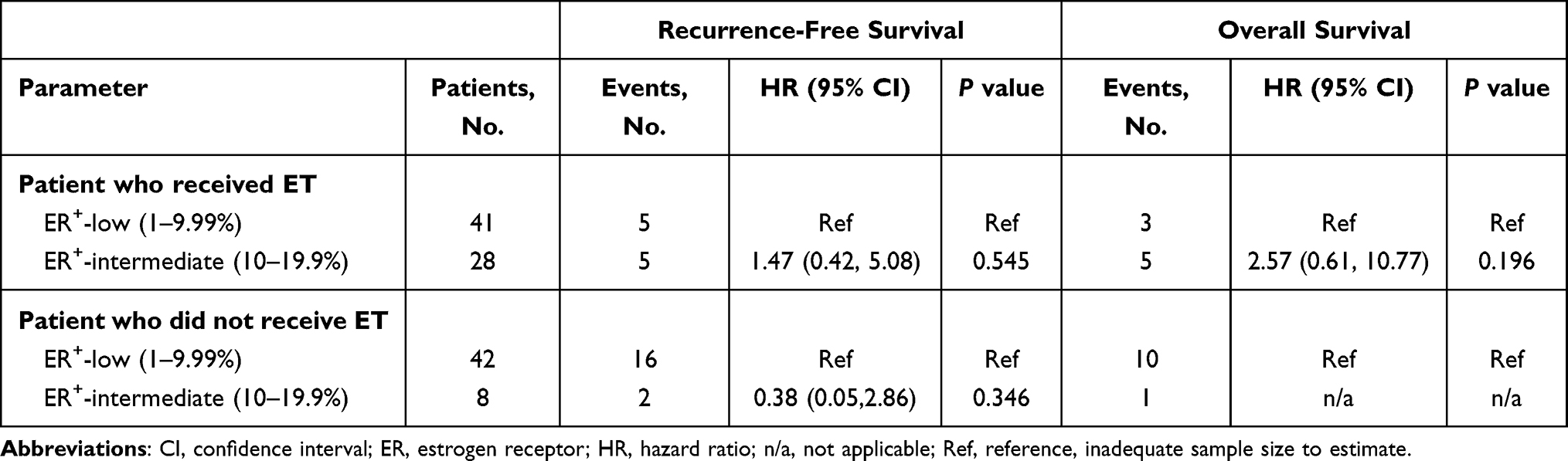 |
Table 4 Endocrine Therapy Treatment Effect (Univariate Analysis) |
 |
Figure 3 Clinical outcomes of patients ER+-1–19.9% staining and ER+-≥ 20% staining. Panel (A) shows recurrence-free survival for the training set, which includes two-thirds of evaluable patients; panel (B) shows recurrence-free survival for the test set, which includes one-third of evaluable patients; panel (C) shows overall survival. For the training set; panel (D) shows overall survival for the test set. Abbreviations: BC, breast cancer; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NE, not estimated; TN, triple negative. |
Discussion
ER+ BC is a heterogenous disease in both its natural history and its wide distribution of ER expression levels between tumors; cases of low expression represent a small proportion of BCs. The optimal cut point that indicates reliable prognostic ER expression and predictive information of ET benefit remains to be determined. Historically, any level of ER expression has been considered to be positive, which is counterintuitive and misleading because tumors harboring lower levels of ERs will likely not respond to ET. In parallel, tumors with low expression rates of ERs are universally excluded from contemporary clinical trials for patients with TNBC. As a corollary, ER+-low BC remains an orphan disease not only because of its low frequency but also because of lack of knowledge about its natural history. Indeed, others have confirmed that ER+-low BC represents a rare subset of the disease associated with poor outcomes and aggressive clinicopathological characteristics.12,13 With an increasing number of clinical trials aiming to develop new ETs (eg, SERDs and SERMs), a better understanding of the natural history of and the possible benefit from developing ETs remains an unmet need for patients with this rare subset of BC.
We conducted a large real-world retrospective cohort study of 4697 participants with early-stage ER+ BCs or TNBCs. In this cohort, the natural history of patients with early-stage BCs was similar to previously published literature.14 Our results suggest that ER+-low BCs (expression, 1–9.99%) represent a small subset (1.8%) of ER+ BC cases. These tumors presented with pathological features and prognoses similar to those of patients with TNBC. We observed a continuous association between ER expression in 10% increments and improved clinical outcomes. Our sensitivity analyses did not allow for the distinction of higher ER cut point. Therefore, we conservatively chose 20% as a clinically reasonable cut point for further analyses; based on this, we defined an ER+-intermediate group (ie, 10–19.9%).
We observed that ER expression <20% was associated with poor RFS and OS (Figure 3). In our cohort, patients with tumors harboring ER expression rates between 10% and 19.9% (intermediate levels) presented similar clinicopathological features, natural histories, and treatment patterns to those with ER+-low BCs (1–9.99%); however, anthracycline- and taxane-containing chemotherapy regimens were more commonly administered to patients with tumors with ER+-intermediate tumors. Moreover, ER+-intermediate patients had similar RFS as ER+-low patients, but the ER+-low group seemed to still derive benefit from adjuvant ET. We observed that an incremental expression of ER is associated with improved outcomes, further suggesting that the binary categorization of ER expression represents a simplification of continuous biological phenomena. Based on our findings, a balanced discussion should be conducted among patients with ER+-low and ER+-intermediate BC when making a decision on adjuvant ET, as possible benefits need to be weighed against toxicities, including arthralgia, thrombosis, osteoporosis, and fatigue.15 If patient and physician collaboratively decide to forego adjuvant ET, these patients should be informed about the possible higher risk of cancer recurrence and closely monitored.
Our study has limitations inherent to real-world retrospective cohort studies and the very small number of patients with ER+-low and ER+-intermediate tumors. There were missing data preventing us from including important variables, such as chemotherapy and nodal staging, into our analyses. Assessments of ER expression were not centrally reviewed, so it is uncertain whether all sites that contributed data followed strictly ASCO-CAP guidelines for ER, PR, and HER2 testing.7 Additionally, there were very few patients with ER+-low and ER+-intermediate, limiting exploratory statistical comparisons and multivariable adjustments. Further, data on ET compliance and genomic markers (eg, Oncotype Dx scores) in this real-world database were not available for most patients; therefore, we were unable to assess for possible interactions between those data and ER levels. In addition, the Flatiron database lacks information on histological features of BC recurrences; these data would have allowed for differentiation between invasive and non-invasive recurrences, which would have been ideal.
Nonetheless, this was a large retrospective study that uses real-world data, thereby increasing the external validity of our hypothesis-generating findings. Given the low frequency of ER+-low tumors,16 the conduction of large prospective studies assessing the prognostic and predictive values of lower ER expression is practically unfeasible. However, retrospective analyses of prospectively collected tumor samples and data from large phase 3 trials assessing the efficacy of adjuvant ET may be feasible and favored to address this unmet need. This study therefore fills an important gap in our knowledge of the natural history of ER+-low and ER+-intermediate tumors.
Conclusions
Findings from this real-world retrospective study suggest that patients in this cohort with ER expression rates <20% have poor outcomes; however, given that few patients had lower tumor expression of ERs in our cohort, our findings need to be validated in future studies.
Data Sharing Statement
The data that support the findings of this study have been originated by Flatiron Health, Inc. These de-identified data may be available upon request and are subject to a license agreement with Flatiron Health; interested researchers should contact [email protected] to determine licensing terms.
Ethical Approval
Institutional Review Board (IRB) approval of the study protocol was obtained from Western Copernicus Group (WCG) IRB prior to study conduct and included a waiver of informed consent.
Informed Consent
This article does not contain any studies with human participants which would require informed consent.
Acknowledgments
Editorial assistance was provided by the Moffitt Cancer Center’s Office of Scientific Writing by Dr. Paul Fletcher, Daley Drucker, and Mikael Michalik. No compensation was given beyond their regular salaries. This work has been supported in part by the Biostatistics & Bioinformatics Shared Resource at the H. Lee Moffitt Cancer Center & Research Institute, a comprehensive cancer center designated by the National Cancer Institute and funded in part by Moffitt’s Cancer Center Support Grant (P30-CA076292).
The abstract of this paper was presented at the American Society of Clinical Oncology Conference in 2021 as a poster presentation with interim findings. The poster’s abstract was published in “Meeting Abstracts” in Journal of Clinical Oncology 39, no. 15_suppl (May 20, 2021) 525–525.
Funding
Shula’s Foundation.
Disclosure
R. L. B. Costa received honorarium from Bristol Meyers Squib, Pfizer, Athenex Oncology, Daiichi Sankyo and Astra Zeneca. All other authors declare no conflicts of interest.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch Pathol Lab Med. 2010;134(7):e48–72. doi:10.5858/134.7.e48
3. Landmann A, Farrugia DJ, Zhu L, et al. Low Estrogen Receptor (ER)-positive breast cancer and neoadjuvant systemic chemotherapy: is response similar to typical ER-positive or ER-negative disease? Am J Clin Pathol. 2018;150(1):34–42. doi:10.1093/ajcp/aqy028
4. Prabhu JS, Korlimarla A, Desai K, et al. A majority of low (1–10%) ER positive breast cancers behave like hormone receptor negative tumors. J Cancer. 2014;5(2):156–165. doi:10.7150/jca.7668
5. Raghav KP, Hernandez-Aya LF, Lei X, et al. Impact of low estrogen/progesterone receptor expression on survival outcomes in breast cancers previously classified as triple negative breast cancers. Cancer. 2012;118(6):1498–1506. doi:10.1002/cncr.26431
6. Davies C, Godwin J, Gray R, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–784.
7. Allison KH, Hammond MEH, Dowsett M, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol. 2020;38(12):1346–1366. doi:10.1200/JCO.19.02309
8. Howell SJ, Johnston SR, Howell A. The use of selective estrogen receptor modulators and selective estrogen receptor down-regulators in breast cancer. Best Pract Res Clin Endocrinol Metab. 2004;18(1):47–66. doi:10.1016/j.beem.2003.08.002
9. Ma X, Long L, Moon S, Adamson BJS, Baxi SS. Comparison of population characteristics in real-world clinical oncology databases in the US: flatiron health, SEER, and NPCR. medRxiv. 2020. doi:10.1101/2020.03.16.20037143
10. Benjamin Birnbaum NN, Seidl-Rathkopf K, Agrawal M, et al. Model-assisted cohort selection with bias analysis for generating large-scale cohorts from the EHR for oncology research; 2020. Available from: https://arxiv.org/abs/2001.09765.
11. Tunes-da-Silva G, Klein JP. Cutpoint selection for discretizing a continuous covariate for generalized estimating equations. Comput Stat Data Anal. 2011;55(1):226–235. doi:10.1016/j.csda.2010.02.016
12. Luo C, Zhong X, Fan Y, Wu Y, Zheng H, Luo T. Clinical characteristics and survival outcome of patients with estrogen receptor low positive breast cancer. Breast. 2022;63:24–28. doi:10.1016/j.breast.2022.03.002
13. Fei F, Siegal GP, Wei S. Characterization of estrogen receptor-low-positive breast cancer. Breast Cancer Res Treat. 2021;188(1):225–235. doi:10.1007/s10549-021-06148-0
14. Liedtke C, Mazouni C, Hess KR, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–1281. doi:10.1200/JCO.2007.14.4147
15. Berkowitz MJ, Thompson CK, Zibecchi LT, et al. How patients experience endocrine therapy for breast cancer: an online survey of side effects, adherence, and medical team support. J Cancer Surviv. 2021;15(1):29–39. doi:10.1007/s11764-020-00908-5
16. Yi M, Huo L, Koenig KB, et al. Which threshold for ER positivity? A retrospective study based on 9639 patients. Ann Oncol. 2014;25(5):1004–1011. doi:10.1093/annonc/mdu053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.